
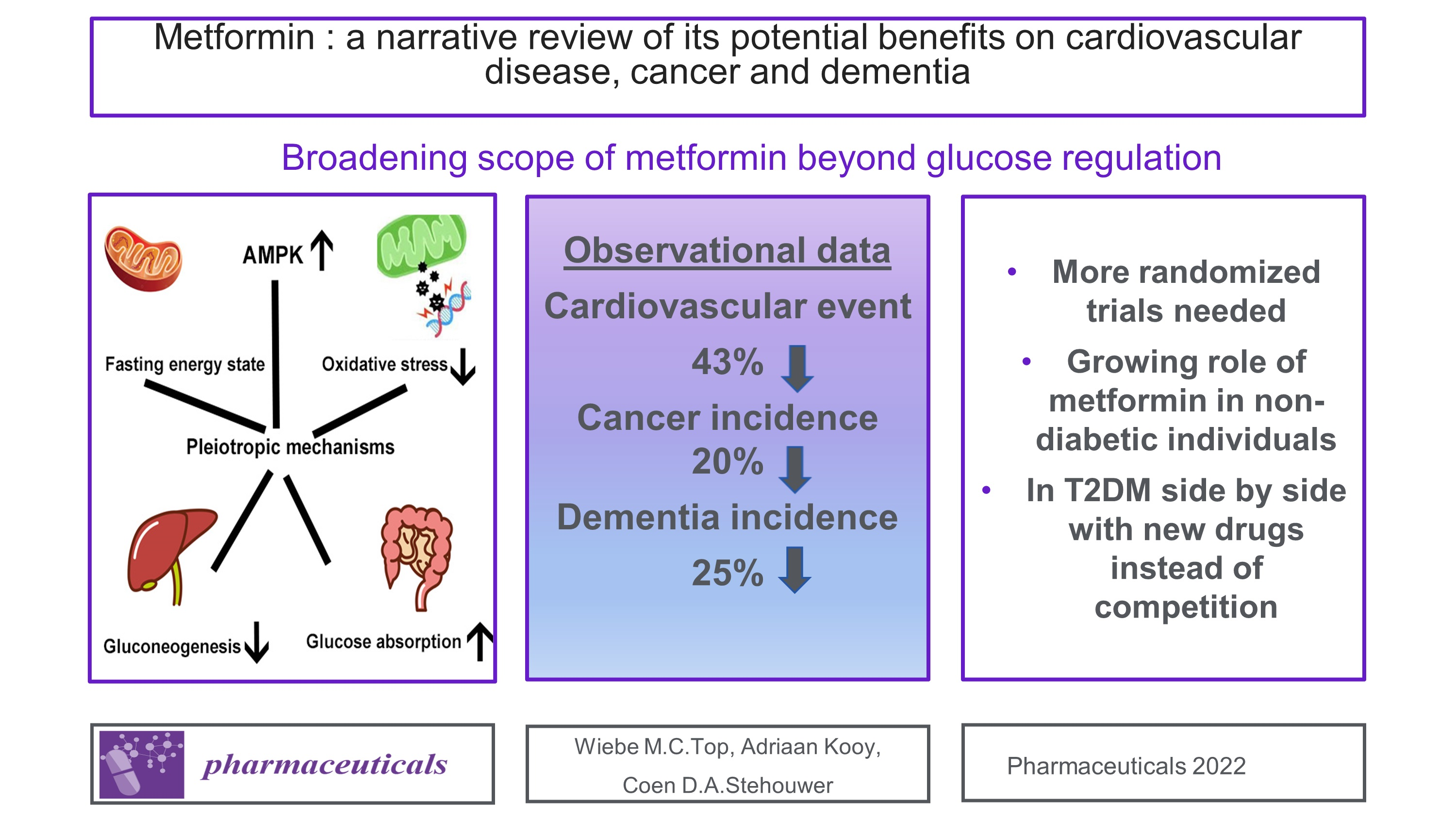
Metformin: A Narrative Review of Its Potential Benefits for Cardiovascular Disease, Cancer and Dementia


Abstract
:
1. Introduction
2. Metformin
2.1. Biguanides
2.2. Glucose Lowering Mechanisms
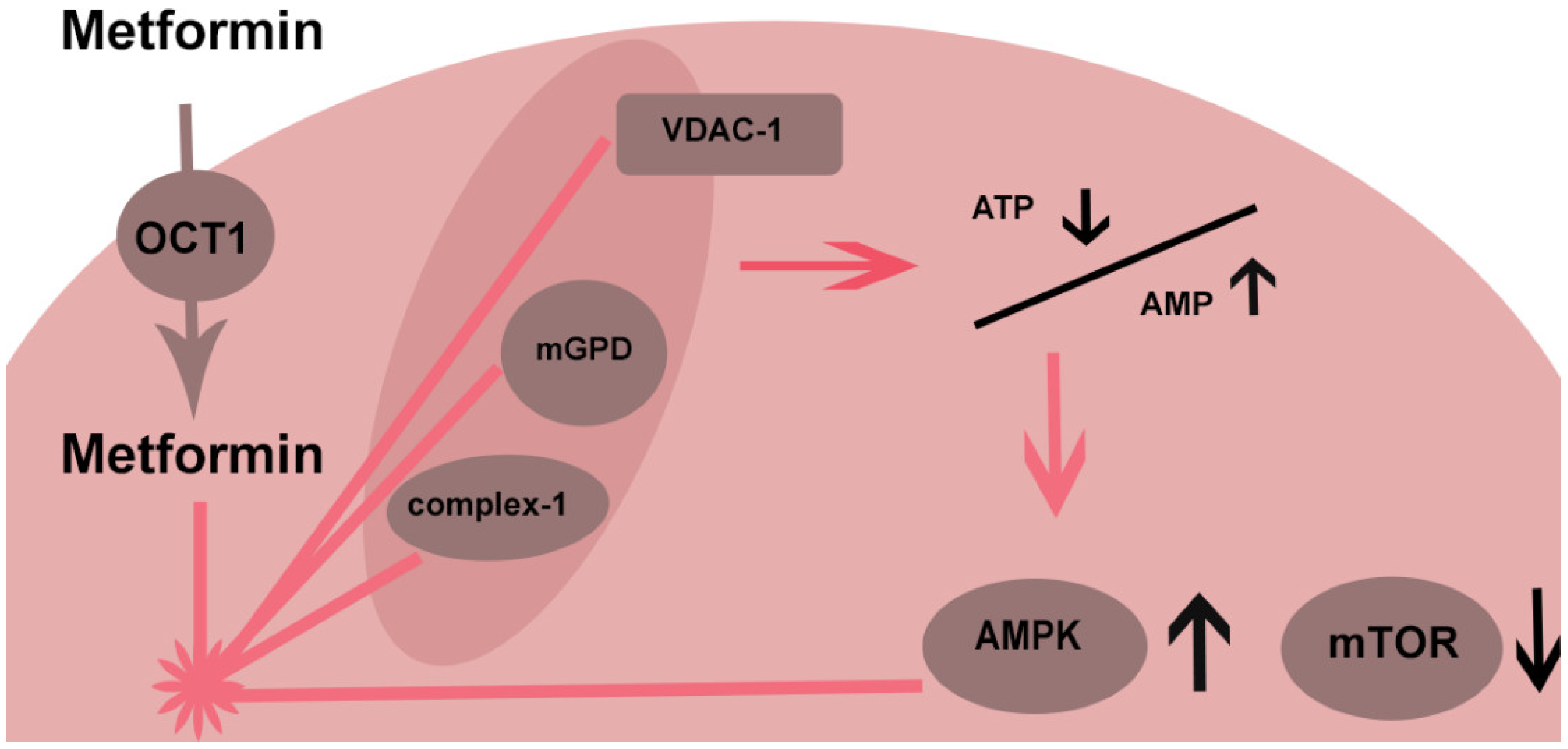
2.3. Cellular Mechanisms
2.4. Mitochondrial Pathways
2.5. AMPK
2.6. AMPK-Independent Effects
3. Cardiovascular Effects
3.1. UKPDS
3.2. HOME
3.3. SPREAD-DIMCAD
3.4. Other Relevant Trials and Meta-Analyses
3.5. Observational Data
3.6. SGLT2 Inhibitors and GLP-1 Receptor Agonists
4. Cancer
4.1. Breast Cancer
4.2. Colorectal Cancer
4.3. Lung Cancer
5. Cognitive Function
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Werner, E.A.; Bell, J. CCXIV.—The preparation of methylguanidine, and of ββ-dimethylguanidine by the interaction of dicyanodiamide, and methylammonium and dimethylammonium chlorides respectively. J. Chem. Soc. Trans. 1922, 121, 1790–1794. [Google Scholar] [CrossRef]
- Cryer, D.R.; Nicholas, S.P.; Henry, D.H.; Mills, D.J.; Stadel, B.V. Comparative outcomes study of metformin intervention versus conventional approach. Diabetes Care 2005, 28, 539–543. [Google Scholar] [CrossRef] [Green Version]
- Holman, R.R.; Paul, S.K.; Bethel, M.A.; Matthews, D.R.; Neil, H.A.W. 10-Year Follow-up of Intensive Glucose Control in Type 2 Diabetes. N. Engl. J. Med. 2008, 359, 1577–1589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buse, J.B.; Wexler, D.J.; Tsapas, A.; Rossing, P.; Mingrone, G.; Mathieu, C.; D’Alessio, D.A.; Davies, M.J. 2019 Update to: Management of Hyperglycemia in Type 2 Diabetes, 2018. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2019, 43, 487–493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ala, M.; Ala, M. Metformin for Cardiovascular Protection, Inflammatory Bowel Disease, Osteoporosis, Periodontitis, Polycystic Ovarian Syndrome, Neurodegeneration, Cancer, Inflammation and Senescence: What Is Next? ACS Pharmacol. Transl. Sci. 2021, 4, 1747–1770. [Google Scholar] [CrossRef] [PubMed]
- Kathuria, D.; Raul, A.D.; Wanjari, P.; Bharatam, P.V. Biguanides: Species with versatile therapeutic applications. Eur. J. Med. Chem. 2021, 219, 113378. [Google Scholar] [CrossRef]
- Garcia, E.Y. Flumamine, a new synthetic analgesic and anti-flu drug. J. Philipp. Med. Assoc. 1950, 26, 287–293. [Google Scholar]
- Sterne, J. Du nouveau dans les antidiabetiques. La NN dimethylamine guanyl guanide (NNDG). Maroc Med. 1957, 36, 1295–1296. [Google Scholar]
- Bridges, H.R.; Sirviö, V.A.; Agip, A.N.A.; Hirst, J. Molecular features of biguanides required for targeting of mitochondrial respiratory complex I and activation of AMP-kinase. BMC Biol. 2016, 14, 65. [Google Scholar] [CrossRef] [Green Version]
- Dujic, T.; Zhou, K.; Yee, S.W.; van Leeuwen, N.; de Keyser, C.E.; Javorský, M.; Goswami, S.; Zaharenko, L.; Hougaard Christensen, M.M.; Out, M.; et al. Variants in Pharmacokinetic Transporters and Glycemic Response to Metformin: A Metgen Meta-Analysis. Clin. Pharmacol. Ther. 2017, 101, 763–772. [Google Scholar] [CrossRef] [Green Version]
- Jeong, Y.S.; Jusko, W.J. Meta-assessment of metformin absorption and disposition pharmacokinetics in nine species. Pharmaceuticals 2021, 14, 545. [Google Scholar] [CrossRef]
- Lamoia, T.E.; Shulman, G.I. Cellular and Molecular Mechanisms of Metformin Action. Endocr. Rev. 2021, 42, 77–96. [Google Scholar] [CrossRef]
- Natali, A.; Ferrannini, E. Effects of metformin and thiazolidinediones on suppression of hepatic glucose production and stimulation of glucose uptake in type 2 diabetes: A systematic review. Diabetologia 2006, 49, 434–441. [Google Scholar] [CrossRef] [Green Version]
- Gormsen, L.C.; Søndergaard, E.; Christensen, N.L.; Brøsen, K.; Jessen, N.; Nielsen, S. Metformin increases endogenous glucose production in non-diabetic individuals and individuals with recent-onset type 2 diabetes. Diabetologia 2019, 62, 1251–1256. [Google Scholar] [CrossRef] [Green Version]
- Koffert, J.P.; Mikkola, K.; Virtanen, K.A.; Andersson, A.M.D.; Faxius, L.; Hällsten, K.; Heglind, M.; Guiducci, L.; Pham, T.; Silvola, J.M.U.; et al. Metformin treatment significantly enhances intestinal glucose uptake in patients with type 2 diabetes: Results from a randomized clinical trial. Diabetes Res. Clin. Pract. 2017, 131, 208–216. [Google Scholar] [CrossRef] [Green Version]
- Bahne, E.; Sun, E.W.L.; Young, R.L.; Hansen, M.; Sonne, D.P.; Hansen, J.S.; Rohde, U.; Liou, A.P.; Jackson, M.L.; de Fontgalland, D.; et al. Metformin-induced glucagon-like peptide-1 secretion contributes to the actions of metformin in type 2 diabetes. JCI Insight 2018, 3, e93936. [Google Scholar] [CrossRef] [Green Version]
- Horakova, O.; Kroupova, P.; Bardova, K.; Buresova, J.; Janovska, P.; Kopecky, J.; Rossmeisl, M. Metformin acutely lowers blood glucose levels by inhibition of intestinal glucose transport. Sci. Rep. 2019, 9, 6156. [Google Scholar] [CrossRef]
- Buse, J.B.; DeFronzo, R.A.; Rosenstock, J.; Kim, T.; Burns, C.; Skare, S.; Baron, A.; Fineman, M. The primary glucose-lowering effect of metformin resides in the gut, not the circulation: Results from short-term pharmacokinetic and 12-week dose-ranging studies. Diabetes Care 2016, 39, 198–205. [Google Scholar] [CrossRef] [Green Version]
- Sum, C.F.; Webster, J.M.; Johnson, A.B.; Catalano, C.; Cooper, B.G.; Taylor, R. The effect of intravenous metformin on glucose metabolism during hyperglycaemia in type 2 diabetes. Diabet. Med. 1992, 9, 61–65. [Google Scholar] [CrossRef]
- Bouchoucha, M.; Uzzan, B.; Cohen, R. Metformin and digestive disorders. Diabetes Metab. 2011, 37, 90–96. [Google Scholar] [CrossRef]
- Yang, M.; Darwish, T.; Larraufie, P.; Rimmington, D.; Cimino, I.; Goldspink, D.A.; Jenkins, B.; Koulman, A.; Brighton, C.A.; Ma, M.; et al. Inhibition of mitochondrial function by metformin increases glucose uptake, glycolysis and GDF-15 release from intestinal cells. Sci. Rep. 2021, 11, 2529. [Google Scholar] [CrossRef]
- Polianskyte-Prause, Z.; Tolvanen, T.A.; Lindfors, S.; Dumont, V.; Van, M.; Wang, H.; Dash, S.N.; Berg, M.; Naams, J.B.; Hautala, L.C.; et al. Metformin increases glucose uptake and acts renoprotectively by reducing SHIP2 activity. FASEB J. 2019, 33, 2858–2869. [Google Scholar] [CrossRef] [Green Version]
- Auger, C.; Sivayoganathan, T.; Abdullahi, A.; Parousis, A.; Pang, B.W.; Jeschke, M.G. Metformin adapts its cellular effects to bioenergetic status in a model of metabolic dysfunction. Sci. Rep. 2018, 8, 5646. [Google Scholar] [CrossRef]
- El-Mir, M.Y.; Detaille, D.; R-Villanueva, G.; Delgado-Esteban, M.; Guigas, B.; Attia, S.; Fontaine, E.; Almeida, A.; Leverve, X. Neuroprotective role of antidiabetic drug metformin against apoptotic cell death in primary cortical neurons. J. Mol. Neurosci. 2008, 34, 77–87. [Google Scholar] [CrossRef]
- Hu, M.; Ye, P.; Liao, H.; Chen, M.; Yang, F. Metformin Protects H9C2 Cardiomyocytes from High-Glucose and Hypoxia/Reoxygenation Injury via Inhibition of Reactive Oxygen Species Generation and Inflammatory Responses: Role of AMPK and JNK. J. Diabetes Res. 2016, 2016, 2961954. [Google Scholar] [CrossRef] [Green Version]
- Cheng, G.; Li, L. High-glucose-induced apoptosis, ROS production and pro-inflammatory response in cardiomyocytes is attenuated by metformin treatment via PP2A activation. J. Biosci. 2020, 45, 126. [Google Scholar] [CrossRef]
- Kukidome, D.; Nishikawa, T.; Sonoda, K.; Imoto, K.; Fujisawa, K.; Yano, M.; Motoshima, H.; Taguchi, T.; Matsumura, T.; Araki, E. Activation of AMP-activated protein kinase reduces hyperglycemia-induced mitochondrial reactive oxygen species production and promotes mitochondrial biogenesis in human umbilical vein endothelial cells. Diabetes 2006, 55, 120–127. [Google Scholar] [CrossRef]
- Algire, C.; Moiseeva, O.; Deschênes-Simard, X.; Amrein, L.; Petruccelli, L.; Birman, E.; Viollet, B.; Ferbeyre, G.; Pollak, M.N. Metformin reduces endogenous reactive oxygen species and associated DNA damage. Cancer Prev. Res. 2012, 5, 536–543. [Google Scholar] [CrossRef] [Green Version]
- Bai, B.; Chen, H. Metformin: A Novel Weapon against Inflammation. Front. Pharmacol. 2021, 12, 622262. [Google Scholar] [CrossRef]
- Davis, B.J.; Xie, Z.; Viollet, B.; Zou, M. Drug Metformin Stimulates Nitric Oxide Synthesis In Vivo and Endothelial Nitric Oxide Synthase. Diabetes 2006, 55, 496–505. [Google Scholar] [CrossRef] [Green Version]
- Bellin, C.; De Wiza, D.H.; Wiernsperger, N.F.; Rösen, P. Generation of reactive oxygen species by endothelial and smooth muscle cells: Influence of hyperglycemia and metformin. Horm. Metab. Res. 2006, 38, 732–739. [Google Scholar] [CrossRef] [PubMed]
- De Jager, J.; Kooy, A.; Schalkwijk, C.; van der Kolk, J.; Lehert, P.; Bets, D.; Wulffelé, M.G.; Donker, A.J.; Stehouwer, C.D.A. Long-term effects of metformin on endothelial function in type 2 diabetes: A randomized controlled trial. J. Intern. Med. 2014, 275, 59–70. [Google Scholar] [CrossRef] [PubMed]
- Giaccari, A.; Solini, A.; Frontoni, S.; Prato, S. Del Metformin benefits: Another example for alternative energy substrate mechanism? Diabetes Care 2021, 44, 647–654. [Google Scholar] [CrossRef] [PubMed]
- Leng, W.; Jiang, J.; Chen, B.; Wu, Q. Metformin and malignant tumors: Not over the hill. Diabetes Metab. Syndr. Obes. Targets Ther. 2021, 14, 3673–3689. [Google Scholar] [CrossRef]
- Pollak, M. Insulin and insulin-like growth factor signalling in neoplasia. Nat. Rev. Cancer 2008, 8, 915–928, Erratum in Nat. Rev. Cancer 2009, 9, 224. [Google Scholar] [CrossRef]
- Pimentel, I.; Chen, B.E.; Lohmann, A.E.; Ennis, M.; Ligibel, J.; Shepherd, L.; Hershman, D.L.; Whelan, T.; Stambolic, V.; Mayer, I.; et al. The Effect of Metformin vs Placebo on Sex Hormones in Canadian Cancer Trials Group MA.32. J. Natl. Cancer Inst. 2021, 113, 192–198. [Google Scholar] [CrossRef]
- Salani, B.; Del Rio, A.; Marini, C.; Sambuceti, G.; Cordera, R.; Maggi, D. Metformin, cancer and glucose metabolism. Endocr. Relat. Cancer 2014, 21, R461–R471. [Google Scholar] [CrossRef] [Green Version]
- Müller, S.; Versini, A.; Sindikubwabo, F.; Belthier, G.; Niyomchon, S.; Pannequin, J.; Grimaud, L.; Cañeque, T.; Rodriguez, R. Metformin reveals a mitochondrial copper addiction of mesenchymal cancer cells. PLoS ONE 2018, 13, e0208213. [Google Scholar] [CrossRef] [Green Version]
- Ma, R.; Yi, B.; Riker, A.I.; Xi, Y. Metformin and cancer immunity. Acta Pharmacol. Sin. 2020, 41, 1403–1409. [Google Scholar] [CrossRef]
- Rotermund, C.; Machetanz, G.; Fitzgerald, J.C. The therapeutic potential of metformin in neurodegenerative diseases. Front. Endocrinol. 2018, 9, 400. [Google Scholar] [CrossRef]
- Gupta, A.; Bisht, B.; Dey, C.S. Peripheral insulin-sensitizer drug metformin ameliorates neuronal insulin resistance and Alzheimer’s-like changes. Neuropharmacology 2011, 60, 910–920. [Google Scholar] [CrossRef]
- Kickstein, E.; Krauss, S.; Thornhill, P.; Rutschow, D.; Zeller, R.; Sharkey, J.; Williamson, R.; Fuchs, M.; Köhler, A.; Glossmann, H.; et al. Biguanide metformin acts on tau phosphorylation via mTOR/protein phosphatase 2A (PP2A) signaling. Proc. Natl. Acad. Sci. USA 2010, 107, 21830–21835. [Google Scholar] [CrossRef] [Green Version]
- Kodali, M.; Attaluri, S.; Madhu, L.N.; Shuai, B.; Upadhya, R.; Gonzalez, J.J.; Rao, X.; Shetty, A.K. Metformin treatment in late middle age improves cognitive function with alleviation of microglial activation and enhancement of autophagy in the hippocampus. Aging Cell 2021, 20, e13277. [Google Scholar] [CrossRef]
- Chen, Y.; Zhao, S.; Fan, Z.; Li, Z.; Zhu, Y.; Shen, T.; Li, K.; Yan, Y.; Tian, J.; Liu, Z.; et al. Metformin attenuates plaque-associated tau pathology and reduces amyloid-β burden in APP/PS1 mice. Alzheimer’s Res. Ther. 2021, 13, 40. [Google Scholar] [CrossRef]
- Owen, M.R.; Doran, E.; Halestrap, A.P. Evidence that metformin exerts its anti-diabetic effects through inhibition of complex 1 of the mitochondrial respiratory chain. Biochem. J. 2000, 348 Pt 3, 607–614. [Google Scholar] [CrossRef]
- He, L.; Wondisford, F.E. Metformin action: Concentrations matter. Cell Metab. 2015, 21, 159–162. [Google Scholar] [CrossRef] [Green Version]
- Shoshan-Barmatz, V.; Anand, U.; Nahon-Crystal, E.; Di Carlo, M.; Shteinfer-Kuzmine, A. Adverse Effects of Metformin from Diabetes to COVID-19, Cancer, Neurodegenerative Diseases, and Aging: Is VDAC1 a Common Target? Front. Physiol. 2021, 12, 730048. [Google Scholar] [CrossRef]
- Muller, S.; Denet, S.; Candiloros, H.; Barrois, R.; Wiernsperger, N.; Donner, M.; Drouin, P. Action of metformin on erythrocyte membrane fluidity in vitro and in vivo. Eur. J. Pharmacol. 1997, 337, 103–110. [Google Scholar] [CrossRef]
- Vytla, V.S.; Ochs, R.S. Metformin increases mitochondrial energy formation in L6 muscle cell cultures. J. Biol. Chem. 2013, 288, 20369–20377. [Google Scholar] [CrossRef] [Green Version]
- Zhang, C.S.; Li, M.; Ma, T.; Zong, Y.; Cui, J.; Feng, J.W.; Wu, Y.Q.; Lin, S.Y.; Lin, S.C. Metformin Activates AMPK through the Lysosomal Pathway. Cell Metab. 2016, 24, 521–522. [Google Scholar] [CrossRef] [Green Version]
- Kalender, A.; Selvaraj, A.; Kim, S.Y.; Gulati, P.; Brûlé, S.; Viollet, B.; Kemp, B.E.; Bardeesy, N.; Dennis, P.; Schlager, J.J.; et al. Metformin, independent of AMPK, inhibits mTORC1 in a rag GTPase-dependent manner. Cell Metab. 2010, 11, 390–401. [Google Scholar] [CrossRef] [Green Version]
- Foretz, M.; Hébrard, S.; Leclerc, J.; Zarrinpashneh, E.; Soty, M.; Mithieux, G.; Sakamoto, K.; Andreelli, F.; Viollet, B. Metformin inhibits hepatic gluconeogenesis in mice independently of the LKB1/AMPK pathway via a decrease in hepatic energy state. J. Clin. Investig. 2010, 120, 2355–2369. [Google Scholar] [CrossRef] [Green Version]
- Miller, R.A.; Birnbaum, M.J. An energetic tale of AMPK-independent effects of metformin. J. Clin. Investig. 2010, 120, 2267–2270. [Google Scholar] [CrossRef] [Green Version]
- Kristófi, R.; Eriksson, J.W. Metformin as an anti-inflammatory agent: A short review. J. Endocrinol. 2021, 251, R11–R22. [Google Scholar] [CrossRef]
- Moiseeva, O.; Deschênes-Simard, X.; St-Germain, E.; Igelmann, S.; Huot, G.; Cadar, A.E.; Bourdeau, V.; Pollak, M.N.; Ferbeyre, G. Metformin inhibits the senescence-associated secretory phenotype by interfering with IKK/NF-κB activation. Aging Cell 2013, 12, 489–498. [Google Scholar] [CrossRef]
- Abdelrahman, S.; Alghrably, M.; Campagna, M.; Hauser, C.A.E.; Jaremko, M.; Lachowicz, J.I. Metal complex formation and anticancer activity of cu(I) and cu(ii) complexes with metformin. Molecules 2021, 26, 4730. [Google Scholar] [CrossRef]
- Lamanna, C.; Monami, M.; Marchionni, N.; Mannucci, E. Effect of metformin on cardiovascular events and mortality: A meta-analysis of randomized clinical trials. Diabetes. Obes. Metab. 2011, 13, 221–228. [Google Scholar] [CrossRef]
- Boussageon, R.; Supper, I.; Bejan-Angoulvant, T.; Kellou, N.; Cucherat, M.; Boissel, J.P.; Kassai, B.; Moreau, A.; Gueyffier, F.; Cornu, C. Reappraisal of metformin efficacy in the treatment of type 2 diabetes: A meta-analysis of randomised controlled trials. PLoS Med. 2012, 9, e1001204. [Google Scholar] [CrossRef] [Green Version]
- Griffin, S.J.; Leaver, J.K.; Irving, G.J. Impact of metformin on cardiovascular disease: A meta-analysis of randomised trials among people with type 2 diabetes. Diabetologia 2017, 60, 1620–1629. [Google Scholar] [CrossRef] [Green Version]
- Gnesin, F.; Thuesen, A.C.B.; Kähler, L.K.A.; Madsbad, S.; Hemmingsen, B. Metformin monotherapy for adults with type 2 diabetes mellitus. Cochrane Database Syst. Rev. 2020, 2020, CD012906. [Google Scholar] [CrossRef] [Green Version]
- UK Prospective Diabetes Study (UKPDS) Group. Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). Lancet 1998, 352, 854–865. [Google Scholar] [CrossRef]
- Kooy, A.; de Jager, J.; Lehert, P.; Bets, D.; Wulffele, M.G.; Donker, A.J.M.; Stehouwer, C.D.A. Long-term effects of metformin on metabolism and microvascular and macrovascular disease in patients with type 2 diabetes mellitus. Arch. Intern. Med. 2009, 169, 616–625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, J.; Zhang, Y.; Lai, S.; Lv, A.; Su, Q.; Dong, Y.; Zhou, Z.; Tang, W.; Zhao, J.; Cui, L.; et al. Effects of metformin versus glipizide on cardiovascular outcomes in patients with type 2 diabetes and coronary artery disease. Diabetes Care 2013, 36, 1304–1311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monami, M.; Candido, R.; Pintaudi, B.; Targher, G.; Mannucci, E.; Delle Monache, L.; Gallo, M.; Giaccari, A.; Masini, M.L.; Mazzone, F.; et al. Effect of metformin on all-cause mortality and major adverse cardiovascular events: An updated meta-analysis of randomized controlled trials. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 699–704. [Google Scholar] [CrossRef]
- Holman, R.R. Post trial monitoring results of the UKPDS sulfonylurea plus metformin substudy. In Proceedings of the 49th Annual Meeting of the European Association for the Study of Diabetes, Barcelona, Spain, 23–27 September 2013; Available online: http://www.easdvirtualmeeting.org/re (accessed on 9 February 2022).
- Top, W.M.C.; Lehert, P.; Schalkwijk, C.G.; Stehouwer, C.D.A.; Kooy, A. Metformin and N-terminal pro B-type natriuretic peptide in type 2 diabetes patients, a post-hoc analysis of a randomized controlled trial. PLoS ONE 2021, 16, e0247939. [Google Scholar] [CrossRef]
- Kahn, S.E.; Haffner, S.M.; Heise, M.A.; Herman, W.H.; Holman, R.R.; Jones, N.P.; Kravitz, B.G.; Lachin, J.M.; O’Neill, M.C.; Zinman, B.; et al. Glycemic Durability of Rosiglitazone, Metformin, or Glyburide Monotherapy. N. Engl. J. Med. 2006, 355, 2427–2443. [Google Scholar] [CrossRef] [Green Version]
- Rachmani, R.; Slavachevski, I.; Levi, Z.; Zadok, B.S.; Kedar, Y.; Ravid, M. Metformin in patients with type 2 diabetes mellitus: Reconsideration of traditional contraindications. Eur. J. Intern. Med. 2002, 13, 428–433. [Google Scholar] [CrossRef]
- Li, T.; Providencia, R.; Mu, N.; Yin, Y.; Chen, M.; Wang, Y.; Liu, M.; Yu, L.; Gu, C.; Ma, H. Association of metformin monotherapy or combined therapy with cardiovascular risks in patients with type 2 diabetes mellitus. Cardiovasc. Diabetol. 2021, 20, 30. [Google Scholar] [CrossRef]
- Zhang, K.; Yang, W.; Dai, H.; Deng, Z. Cardiovascular risk following metformin treatment in patients with type 2 diabetes mellitus: Results from meta-analysis. Diabetes Res. Clin. Pract. 2020, 160, 108001. [Google Scholar] [CrossRef]
- Campbell, J.M.; Bellman, S.M.; Stephenson, M.D.; Lisy, K. Metformin reduces all-cause mortality and diseases of ageing independent of its effect on diabetes control: A systematic review and meta-analysis. Ageing Res. Rev. 2017, 40, 31–44. [Google Scholar] [CrossRef]
- Han, Y.; Xie, H.; Liu, Y.; Gao, P.; Yang, X.; Shen, Z. Effect of metformin on all-cause and cardiovascular mortality in patients with coronary artery diseases: A systematic review and an updated meta-analysis. Cardiovasc. Diabetol. 2019, 18, 96. [Google Scholar] [CrossRef] [Green Version]
- Hu, Y.; Lei, M.; Ke, G.; Huang, X.; Peng, X.; Zhong, L.; Fu, P. Metformin Use and Risk of All-Cause Mortality and Cardiovascular Events in Patients with Chronic Kidney Disease—A Systematic Review and Meta-Analysis. Front. Endocrinol. 2020, 11, 559446. [Google Scholar] [CrossRef]
- Harrington, J.L.; de Albuquerque Rocha, N.; Patel, K.V.; Verma, S.; McGuire, D.K. Should Metformin Remain First-Line Medical Therapy for Patients with Type 2 Diabetes Mellitus and Atherosclerotic Cardiovascular Disease? An Alternative Approach. Curr. Diabetes Rep. 2018, 18, 64. [Google Scholar] [CrossRef]
- Pearson-Stuttard, J.; Bennett, J.; Cheng, Y.J.; Vamos, E.P.; Cross, A.J.; Ezzati, M.; Gregg, E.W. Trends in predominant causes of death in individuals with and without diabetes in England from 2001 to 2018: An epidemiological analysis of linked primary care records. Lancet Diabetes Endocrinol. 2021, 9, 165–173. [Google Scholar] [CrossRef]
- Wu, H.; Lau, E.S.H.; Ma, R.C.W.; Kong, A.P.S.; Wild, S.H.; Goggins, W.; Chow, E.; So, W.-Y.; Chan, J.C.N.; Luk, A.O.Y. Secular trends in all-cause and cause-specific mortality rates in people with diabetes in Hong Kong, 2001–2016: A retrospective cohort study. Diabetologia 2020, 63, 757–766. [Google Scholar] [CrossRef]
- Tsilidis, K.K.; Kasimis, J.C.; Lopez, D.S.; Ntzani, E.E.; Ioannidis, J.P.A. Type 2 diabetes and cancer: Umbrella review of meta-analyses of observationlal studies. BMJ 2015, 350, g7607. [Google Scholar] [CrossRef] [Green Version]
- Libby, G.; Donnelly, L.A.; Donnan, P.T.; Alessi, D.R.; Morris, A.D.; Evans, J.M.M. New users of metformin are at low risk of incident cancer: A cohort study among people with type 2 diabetes. Diabetes Care 2009, 32, 1620–1625. [Google Scholar] [CrossRef] [Green Version]
- Rey-Reñones, C.; Baena-Díez, J.M.; Aguilar-Palacio, I.; Miquel, C.; Grau, M. Type 2 diabetes mellitus and cancer: Epidemiology, physiopathology and prevention. Biomedicines 2021, 9, 1429. [Google Scholar] [CrossRef]
- Zhang, K.; Bai, P.; Dai, H.; Deng, Z. Metformin and risk of cancer among patients with type 2 diabetes mellitus: A systematic review and meta-analysis. Prim. Care Diabetes 2021, 15, 52–58. [Google Scholar] [CrossRef]
- Tseng, C.-H. Metformin may reduce breast cancer risk in Taiwanese women with type 2 diabetes. Breast Cancer Res. Treat. 2014, 145, 785–790. [Google Scholar] [CrossRef]
- Chen, L.; Chubak, J.; Boudreau, D.M.; Barlow, W.E.; Weiss, N.S.; Li, C.I. Diabetes treatments and risks of adverse breast cancer outcomes among early-stage breast cancer patients: A SEER-medicare analysis. Cancer Res. 2017, 77, 6033–6041. [Google Scholar] [CrossRef] [Green Version]
- Hui, T.; Shang, C.; Yang, L.; Wang, M.; Li, R.; Song, Z. Metformin improves the outcomes in Chinese invasive breast cancer patients with type 2 diabetes mellitus. Sci. Rep. 2021, 11, 10034. [Google Scholar] [CrossRef]
- Wang, Q.; Shi, M. Effect of metformin use on the risk and prognosis of colorectal cancer in diabetes mellitus. Anticancer. Drugs 2021, 33, 191–199. [Google Scholar] [CrossRef]
- Xiao, K.; Liu, F.; Liu, J.; Xu, J.; Wu, Q.; Li, X. The effect of metformin on lung cancer risk and survival in patients with type 2 diabetes mellitus: A meta-analysis. J. Clin. Pharm. Ther. 2020, 45, 783–792. [Google Scholar] [CrossRef]
- Park, Y.M.M.; Bookwalter, D.B.; O’Brien, K.M.; Jackson, C.L.; Weinberg, C.R.; Sandler, D.P. A prospective study of type 2 diabetes, metformin use, and risk of breast cancer. Ann. Oncol. 2021, 32, 351–359. [Google Scholar] [CrossRef]
- Al-Ghalib, H.A.; Al-Otaibi, A.D.; Al Tulaihi, B.; Al-Ghaleb, S. The anti-proliferative role of metformin in non-diabetic female patients with breast cancer: Systematic review and meta-analysis of randomized control trials. Clin. Diabetol. 2021, 10, 252–260. [Google Scholar] [CrossRef]
- Morio, K.; Kurata, Y.; Kawaguchi-Sakita, N.; Shiroshita, A.; Kataoka, Y. Efficacy of Metformin in Patients With Breast Cancer Receiving Chemotherapy or Endocrine Therapy: Systematic Review and Meta-analysis. Ann. Pharmacother. 2022, 56, 245–255. [Google Scholar] [CrossRef]
- Lusica, P.M.M.; Eugenio, K.P.Y.; Sacdalan, D.B.L.; Jimeno, C.A. A systematic review and meta-analysis on the efficacy and safety of metformin as adjunctive therapy among women with metastatic breast cancer. Cancer Treat. Res. Commun. 2021, 29, 100457. [Google Scholar] [CrossRef]
- Wang, Q.; Ma, X.; Long, J.; Du, X.; Pan, B.; Mao, H. Metformin and survival of women with breast cancer: A meta-analysis of randomized controlled trials. J. Clin. Pharm. Ther. 2021, in press. [Google Scholar] [CrossRef]
- Yang, W.T.; Yang, H.J.; Zhou, J.G.; Liu, J. Le Relationship between metformin therapy and risk of colorectal cancer in patients with diabetes mellitus: A meta-analysis. Int. J. Colorectal Dis. 2020, 35, 2117–2131. [Google Scholar] [CrossRef]
- Ng, C.A.W.; Jiang, A.A.; Toh, E.M.S.; Ng, C.H.; Ong, Z.H.; Peng, S.; Tham, H.Y.; Sundar, R.; Chong, C.S.; Khoo, C.M. Metformin and colorectal cancer: A systematic review, meta-analysis and meta-regression. Int. J. Colorectal Dis. 2020, 35, 1501–1512. [Google Scholar] [CrossRef] [PubMed]
- Higurashi, T.; Hosono, K.; Takahashi, H.; Komiya, Y.; Umezawa, S.; Sakai, E.; Uchiyama, T.; Taniguchi, L.; Hata, Y.; Uchiyama, S.; et al. Metformin for chemoprevention of metachronous colorectal adenoma or polyps in post-polypectomy patients without diabetes: A multicentre double-blind, placebo-controlled, randomised phase 3 trial. Lancet Oncol. 2016, 17, 475–483. [Google Scholar] [CrossRef]
- Bragagnoli, A.C.; Araujo, R.L.C.; Ferraz, M.W.; dos Santos, L.V.; Abdalla, K.C.; Comar, F.; Santos, F.A.; Oliveira, M.A.; Carvalheira, J.B.C.; Cárcano, F.M.; et al. Metformin plus lrinotecan in patients with refractory colorectal cancer: A phase 2 clinical trial. Br. J. Cancer 2021, 124, 1072–1078. [Google Scholar] [CrossRef] [PubMed]
- Miranda, V.C.; Braghiroli, M.I.; Faria, L.D.; Bariani, G.; Alex, A.; Bezerra Neto, J.E.; Capareli, F.C.; Sabbaga, J.; Lobo dos Santos, J.F.; Hoff, P.M.; et al. Phase 2 Trial of Metformin Combined With 5-Fluorouracil in Patients with Refractory Metastatic Colorectal Cancer. Clin. Colorectal Cancer 2016, 15, 321–328.e1. [Google Scholar] [CrossRef] [PubMed]
- Skinner, H.D.; Crane, C.H.; Garrett, C.R.; Eng, C.; Chang, G.J.; Skibber, J.M.; Rodriguez-Bigas, M.A.; Kelly, P.; Sandulache, V.C.; Delclos, M.E.; et al. Metformin use and improved response to therapy in rectal cancer. Cancer Med. 2013, 2, 99–107. [Google Scholar] [CrossRef]
- Oh, B.Y.; Park, Y.A.; Huh, J.W.; Cho, Y.B.; Yun, S.H.; Lee, W.Y.; Park, H.C.; Choi, D.H.; Park, Y.S.; Kim, H.C. Metformin enhances the response to radiotherapy in diabetic patients with rectal cancer. J. Cancer Res. Clin. Oncol. 2016, 142, 1377–1385. [Google Scholar] [CrossRef]
- Brancher, S.; Ribeiro, A.E.; Toporcov, T.N.; Weiderpass, E. The role of metformin on lung cancer survival: The first systematic review and meta-analysis of observational studies and randomized clinical trials. J. Cancer Res. Clin. Oncol. 2021, 147, 2819–2836. [Google Scholar] [CrossRef]
- Luo, X.; Chen, X.; Wang, L.; Yang, B.; Cai, S. Metformin Adjunct With Antineoplastic Agents for the Treatment of Lung Cancer: A Meta-Analysis of Randomized Controlled Trials and Observational Cohort Studies. Front. Pharmacol. 2021, 12, 639016. [Google Scholar] [CrossRef]
- Arrieta, O.; Barrón, F.; Padilla, M.Á.S.; Avilés-Salas, A.; Ramírez-Tirado, L.A.; Arguelles Jiménez, M.J.; Vergara, E.; Zatarain-Barrón, Z.L.; Hernández-Pedro, N.; Cardona, A.F.; et al. Effect of Metformin Plus Tyrosine Kinase Inhibitors Compared with Tyrosine Kinase Inhibitors Alone in Patients with Epidermal Growth Factor Receptor-Mutated Lung Adenocarcinoma: A Phase 2 Randomized Clinical Trial. JAMA Oncol. 2019, 5, e192553. [Google Scholar] [CrossRef]
- Arrieta, O.; Zatarain-Barrón, Z.L.; Turcott, J.G.; Barrón, F.; Yendamuri, S.; Cardona, A.F.; Rosell, R. Association of BMI with Benefit of Metformin Plus Epidermal Growth Factor Receptor-Tyrosine Kinase Inhibitors in Patients with Advanced Lung Adenocarcinoma: A Secondary Analysis of a Phase 2 Randomized Clinical Trial. JAMA Oncol. 2022. [Google Scholar] [CrossRef]
- Poor, S.R.; Ettcheto, M.; Cano, A.; Sanchez-Lopez, E.; Manzine, P.R.; Olloquequi, J.; Camins, A.; Javan, M. Metformin a potential pharmacological strategy in late onset Alzheimer’s disease treatment. Pharmaceuticals 2021, 14, 890. [Google Scholar] [CrossRef]
- De la Monte, S.M.; Wands, J.R. Alzheimer’s disease is type 3 diabetes-evidence reviewed. J. Diabetes Sci. Technol. 2008, 2, 1101–1113. [Google Scholar] [CrossRef] [Green Version]
- Mattishent, K.; Loke, Y.K. Meta-Analysis: Association Between Hypoglycemia and Serious Adverse Events in Older Patients Treated With Glucose-Lowering Agents. Front. Endocrinol. 2021, 12, 571568. [Google Scholar] [CrossRef]
- Sheen, Y.J.; Sheu, W.H.H. Association between hypoglycemia and dementia in patients with type 2 diabetes. Diabetes Res. Clin. Pract. 2016, 116, 279–287. [Google Scholar] [CrossRef]
- Silbert, R.; Salcido-Montenegro, A.; Rodriguez-Gutierrez, R.; Katabi, A.; McCoy, R.G. Hypoglycemia Among Patients with Type 2 Diabetes: Epidemiology, Risk Factors, and Prevention Strategies. Curr. Diab. Rep. 2018, 18, 53. [Google Scholar] [CrossRef]
- Campbell, J.M.; Stephenson, M.D.; De Courten, B.; Chapman, I.; Bellman, S.M.; Aromataris, E. Metformin Use Associated with Reduced Risk of Dementia in Patients with Diabetes: A Systematic Review and Meta-Analysis. J. Alzheimer’s Dis. 2018, 65, 1225–1236. [Google Scholar] [CrossRef] [Green Version]
- Ping, F.; Jiang, N.; Li, Y. Association between metformin and neurodegenerative diseases of observational studies: Systematic review and meta-analysis. BMJ Open Diabetes Res. Care 2020, 8, e001370. [Google Scholar] [CrossRef]
- Qin, X.; Zhang, X.; Li, P.; Wang, M.; Yan, L.; Bao, Z.; Liu, Q. Association Between Diabetes Medications and the Risk of Parkinson’s Disease: A Systematic Review and Meta-Analysis. Front. Neurol. 2021, 12, 678649. [Google Scholar] [CrossRef]
- Zhou, J.B.; Tang, X.; Han, M.; Yang, J.; Simó, R. Impact of antidiabetic agents on dementia risk: A Bayesian network meta-analysis. Metabolism 2020, 109, 154265. [Google Scholar] [CrossRef]
- Samaras, K.; Makkar, S.; Crawford, J.D.; Kochan, N.A.; Wen, W.; Draper, B.; Trollor, J.N.; Brodaty, H.; Sachdev, P.S. Metformin use is associated with slowed cognitive decline and reduced incident dementia in older adults with type 2 diabetes: The Sydney memory and ageing study. Diabetes Care 2020, 43, 2691–2701. [Google Scholar] [CrossRef]
- Luchsinger, J.A.; Perez, T.; Chang, H.; Mehta, P.; Steffener, J.; Pradabhan, G.; Ichise, M.; Manly, J.; Devanand, D.P.; Bagiella, E. Metformin in amnestic mild cognitive impairment: Results of a pilot randomized placebo controlled clinical trial. J. Alzheimer’s Dis. 2016, 51, 501–514. [Google Scholar] [CrossRef] [Green Version]
- Koenig, A.M.; Mechanic-Hamilton, D.; Xie, S.X.; Combs, M.F.; Cappola, A.R.; Xie, L.; Detre, J.A.; Wolk, D.A.; Arnold, S.E. Effects of the Insulin Sensitizer Metformin in Alzheimer Disease: Pilot Data From a Randomized Placebo-controlled Crossover Study. Alzheimer’s Dis. Assoc. Disord. 2017, 31, 107–113. [Google Scholar] [CrossRef]
- De Jager, J.; Kooy, A.; Lehert, P.; Wulffelé, M.G.; Van Der Kolk, J.; Bets, D.; Verburg, J.; Donker, A.J.M.; Stehouwer, C.D.A. Long term treatment with metformin in patients with type 2 diabetes and risk of vitamin B-12 deficiency: Randomised placebo controlled trial. BMJ 2010, 340, 1177. [Google Scholar] [CrossRef] [Green Version]
- McCarter, S.J.; Teigen, L.M.; McCarter, A.R.; Benarroch, E.E.; St. Louis, E.K.; Savica, R. Low Vitamin B12 and Parkinson Disease: Potential Link to Reduced Cholinergic Transmission and Severity of Disease. Mayo Clin. Proc. 2019, 94, 757–762. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
| Physiological Mechanism | Molecular Mechanism | Target Tissue |
|---|---|---|
| Glucose metabolism | ||
| Decreased gluconeogenesis | Allosteric enzyme inhibition, redox state, complex 1 inhibition, AMPK activation | Liver [12] |
| Increased glucose uptake muscles | Increase in glucose transporters by SHIP2 inhibition | Skeletal muscles [22] |
| Increased gastrointestinal glucose uptake | Mitochondrial inhibition | Enterocyte [21] |
| GLP-1 secretion | AMPK | Enteroendocrine L cell [16] |
| Vascular | ||
| Anti-inflammatory | Decrease NFkB | Macrophage [29] |
| Endothelial NO increase | AMPK | Endothelial cell [30] |
| Decrease oxidative stress | Mitochondrial ion channels and AMPK | Endothelial cell [31] |
| Hemostasis and leucocyte adhesion | Decrease in vWf and sVCAM-1 | Endothelial cell [32] |
| Alternative energy substrate | Elevated lactate | Cardiomyocytes [33] |
| Decrease oxidative stress | AMPK and PP2A | Cardiomyocytes [25,26] |
| Antineoplastic | ||
| Antiproliferation | Decrease mTOR | Tumor cells [34] |
| Decreased insulin and free IGF-1 fraction | Tumor cells [34,35] | |
| Reducing estrogen | Inhibition aromatase activity | Estrogen sensitive tumors [36] |
| Inhibition of glycolysis | Hexokinase2 inhibition | Tumor cells [37] |
| Decrease inflammation | Decrease NFkB | Macrophage [29] |
| Decrease antioxidative stress | Mitochondrial ion channels | Epithelial cells [28] |
| Inhibition of mesenchymal transition | Mitochondrial binding of copper | Tumor cells [38] |
| Improving immune response | AMPK and AMPK independent changes in tumor microenvironment | Immune cells [39] |
| CNS protection | ||
| Decrease antioxidative stress | Mitochondrial | Microglia and neurons [24,40] |
| Increase insulin sensitivity | AMPK | Neurons [41] |
| Dephosphorylation proteins | AMPK and PP2A | Neurons [42] |
| Increase autophagy | Decrease mTOR | Hippocampus microglia [43,44] |
| Decrease inflammation | Decrease NFkB | Neurons [29] |
| Study (Reference) | Participants | Comparator | Endpoint | RR/HR/OR (95% CI) |
|---|---|---|---|---|
| Individual Trial | ||||
| UKPDS 1998 [61] | Newly diagnosed T2DM, n = 753 | Diet | All-cause mortality | 0.64 (0.45–0.91) |
| Any diabetes related endpoint | 0.68 (0.53–0.87) | |||
| UKPDS 2008 [3] | Newly diagnosed T2DM, n = 753 | Diet | All-cause mortality | 0.73 (0.59–0.89) |
| Any diabetes related endpoint | 0.79 (0.66–0.95) | |||
| HOME 2009 [62] | Insulin using T2DM, n = 390 | Placebo | Macrovascular aggregate score | 0.61 (0.40–0.94) |
| SPREAD-DIMCAD 2013 [63] | T2DM with coronary artery disease, n = 304 | Sulfonylurea | Macrovascular aggregate score | 0.54 (0.30–0.90) |
| Meta analysis | Trials | |||
| Lamanna 2011 [57] | 10 | No therapy, placebo, active comparators | All-cause mortality | 1.10 (0.80–1.51) |
| 12 | Cardiovascular events | 0.94 (0.82–1.07) | ||
| Boussageon 2012 [58] | 11 | Diet, placebo, no treatment, metformin add-on, metformin withdrawal | All-cause mortality | 0.99 (0.75–1.31) |
| 10 | Myocardial infarction | 0.90 (0.74–1.09) | ||
| Griffin 2017 [59] | 13 | Diet, lifestyle, placebo | All-cause mortality | 0.96 (0.84–1.09) |
| 7 | Myocardial infarction | 0.89 (0.75–1.06) | ||
| Monami 2021 [64] | 13 | Placebo/no therapy, active comparators | All-cause mortality | 0.80 (0.60–1.07) |
| 2 | MACE | 0.52 (0.37–0.73) |
| Mortality | T2DM Relative Risk (95% CI) |
|---|---|
| Breast cancer | 1.24 (0.95–1.62) |
| Colorectal cancer | 1.20 (1.03–1.40) |
| Endometrial cancer | 1.23 (0.78–1.93) |
| Hepatocellular carcinoma | 2.43 (1.67–3.55) |
| Total cancer mortality | 1.16 (1.04–1.30) |
| Incidence | |
| Breast cancer | 1.20 (1.12–1.28) |
| Colorectal cancer | 1.27 (1.21–1.34) |
| Endometrial cancer | 1.97 (1.71–2.27) |
| Hepatocellular carcinoma | 2.31 (1.87–2.84) |
| Intrahepatic cholangiocarcinoma | 1.97 (1.57–2.46) |
| Pancreatic cancer | 1.95 (1.66–2.28) |
| Total cancer incidence | 1.10 (1.04–1.17) |
| Study (Reference) | Measure | Number of Cases | Breast Cancer | Colorectal Cancer | Lung Cancer |
|---|---|---|---|---|---|
| Tseng 2014 [81] | Incidence | ~500k | 0.63 (0.60–0.67) | ||
| Libby 2009 [78] | Incidence | ~8000 | 0.60 (0.32–1.10) | 0.60 (0.38–0.94) | 0.70 (0.43–1.15) |
| Chen 2017 [82] | Incidence | ~45k | 0.86 (0.70–1.05) ER− 1.25 (0.84–1.88) ER+ | ||
| Hui 2021 [83] | Mortality OS * | ~4000 | 0.39 (0.25–0.60) | ||
| Wang 2021 [84] | Incidence | ~2 million | 0.71 (0.64–0.80) | ||
| Mortality OS | 0.72 (0.62–0.83) | ||||
| Mortality CRC specific | 0.80 (0.70–0.92) | ||||
| Xiao 2020 [85] | Incidence | ~200k | 0.78 (0.70–0.86) | ||
| Mortality OS | 0.65 (0.55–0.77) |
| Study (Reference) | Participants | Comparator | Endpoint | OR/HR (95% CI) |
|---|---|---|---|---|
| Individual trial | ||||
| Samaras 2020 [111] | N = 1037 | Non-metformin T2DM treatment | Dementia | 0.19 (0.04–0.85) |
| Meta analysis | Trials | |||
| Campbell 2018 [107] | 3 | Non-metformin T2DM treatment | Cognitive impairment | 0.55 (0.38–0.78) |
| 6 | Dementia | 0.76 (0.60–0.97) | ||
| Ping 2020 [108] | 23 | Non-metformin T2DM treatment | Overall neurodegenerative disease | 1.04 (0.92–1.17) |
| 17 | Dementia | 0.96 (0.85–1.08) | ||
| 3 | Parkinsons disease | 1.66 (1.14–2.42) | ||
| Zhou 2020 [110] | 9 | Diet | Dementia | 0.75 (0.63–0.86) |
| 14 | Dementia | 0.86 (0.74–1.00) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Top, W.M.C.; Kooy, A.; Stehouwer, C.D.A. Metformin: A Narrative Review of Its Potential Benefits for Cardiovascular Disease, Cancer and Dementia. Pharmaceuticals 2022, 15, 312. https://doi.org/10.3390/ph15030312
Top WMC, Kooy A, Stehouwer CDA. Metformin: A Narrative Review of Its Potential Benefits for Cardiovascular Disease, Cancer and Dementia. Pharmaceuticals. 2022; 15(3):312. https://doi.org/10.3390/ph15030312
Chicago/Turabian StyleTop, Wiebe M. C., Adriaan Kooy, and Coen D. A. Stehouwer. 2022. "Metformin: A Narrative Review of Its Potential Benefits for Cardiovascular Disease, Cancer and Dementia" Pharmaceuticals 15, no. 3: 312. https://doi.org/10.3390/ph15030312
APA StyleTop, W. M. C., Kooy, A., & Stehouwer, C. D. A. (2022). Metformin: A Narrative Review of Its Potential Benefits for Cardiovascular Disease, Cancer and Dementia. Pharmaceuticals, 15(3), 312. https://doi.org/10.3390/ph15030312