Lutathera®: The First FDA- and EMA-Approved Radiopharmaceutical for Peptide Receptor Radionuclide Therapy



Abstract
1. Introduction
2. Chemical Overview
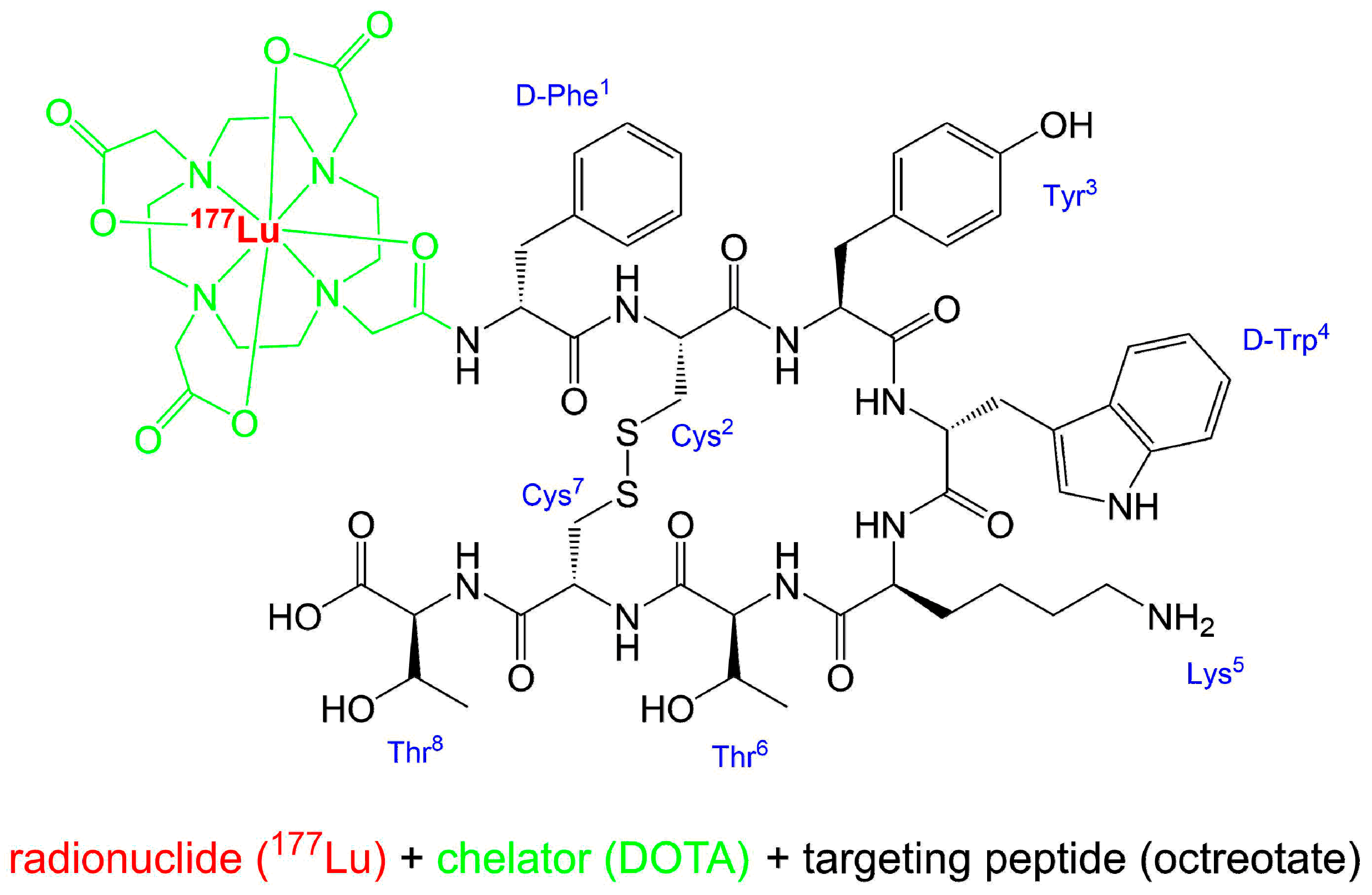
2.1. Names and Structure
2.2. Lutetium-177
2.3. Manufacturing and Quality Criteria
3. Medicinal and Pharmaceutical Overview
3.1. Clinical Indication
3.2. Application
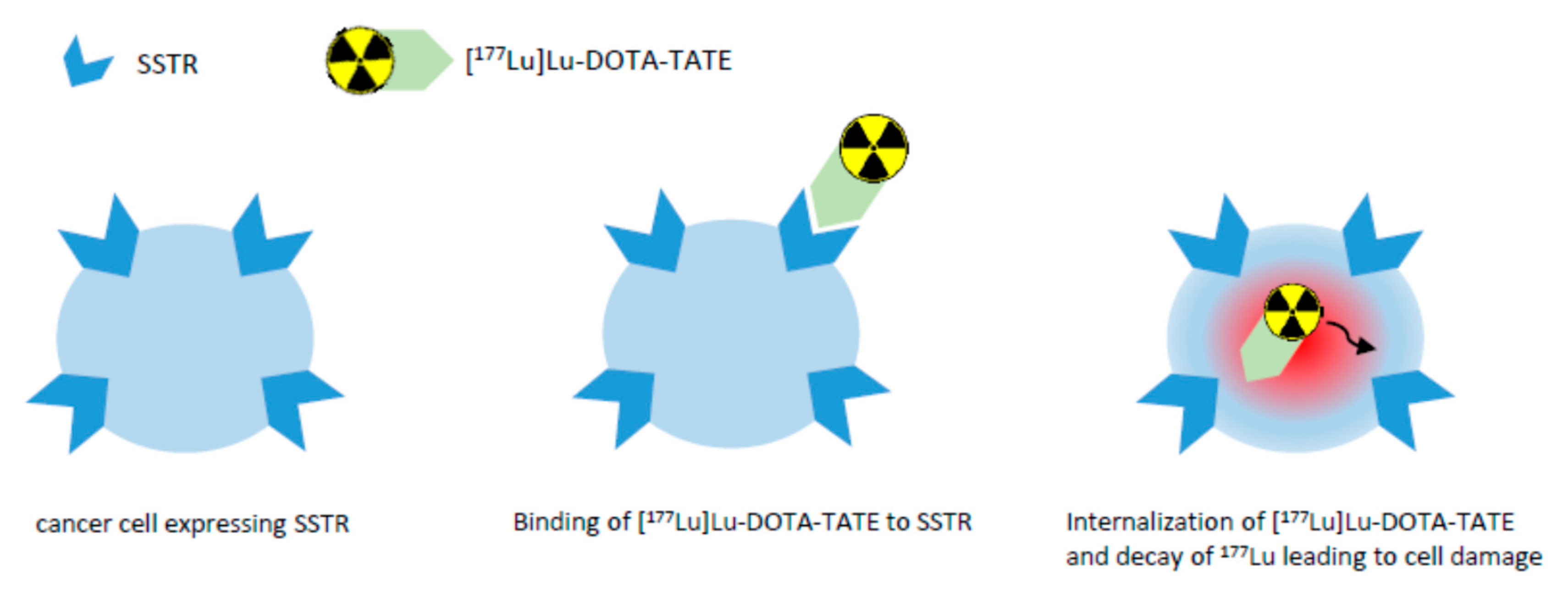
3.3. Pharmacology and Pharmacokinetics
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Coenen, H.H.; Gee, A.D.; Adam, M.; Antoni, G.; Cutler, C.S.; Fujibayashi, Y.; Jeong, J.M.; Mach, R.H.; Mindt, T.L.; Pike, V.W.; et al. Consensus nomenclature rules for radiopharmaceutical chemistry – Setting the record straight. Nucl. Med. Biol. 2017, 55, v. [Google Scholar] [CrossRef] [PubMed]
- Coenen, H.H.; Gee, A.D.; Adam, M.; Antoni, G.; Cutler, C.S.; Fujibayashi, Y.; Jeong, J.M.; Mach, R.H.; Mindt, T.L.; Pike, V.W.; et al. Open letter to journal editors: International consensus radiochemistry nomenclature guidelines. J. Label. Compd. Radiopharm. 2018, 61, 402–404. [Google Scholar] [CrossRef] [PubMed]
- FDA Letter of Approval for LUTATHERA®. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/appletter/2018/208700Orig1s000ltr.pdf (accessed on 23 April 2019).
- Authorization details for Lutathera® in Europe. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/lutathera#authorisation-details-section (accessed on 23 April 2019).
- Authorization details for Lutathera® in Canada. Available online: https://hpr-rps.hres.ca/reg-content/regulatory-decision-summary-detail.php?linkID = RDS00480 (accessed on 23 April 2019).
- Turner, J.H. An introduction to the clinical practice of theranostics in oncology. Br. J. Radiol. 2018, 91, 20180440. [Google Scholar] [CrossRef] [PubMed]
- Dash, A.; Chakraborty, S.; Pillai, M.R.A.; Knapp, F.F., Jr. Peptide Receptor Radionuclide Therapy: An Overview. Cancer Biother. Radiopharm. 2015, 30, 47–71. [Google Scholar] [CrossRef] [PubMed]
- Product Monograph LUTATHERA®. Available online: https://www.samnordic.se/wp-content/uploads/2018/05/LUTATHERA-MONOGRAPH-120218.pdf (accessed on 18 April 2019).
- Xu, C.; Zhang, H. Somatostatin Receptor Based Imaging and Radionuclide Therapy. BioMed Res. Int. 2015, 2015, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Brazeau, P.; Vale, W.; Burgus, R.; Ling, N.; Butcher, M.; Rivier, J.; Guillemin, R. Hypothalamic Polypeptide That Inhibits the Secretion of Immunoreactive Pituitary Growth Hormone. Science 1973, 179, 77–79. [Google Scholar] [CrossRef] [PubMed]
- Kwekkeboom, D.J.; Kam, B.L.; van Essen, M.; Teunissen, J.J.M.; van Eijck, C.H.J.; Valkema, R.; de Jong, M.; de Herder, W.W.; Krenning, E.P. Somatostatin receptor-based imaging and therapy of gastroenteropancreatic neuroendocrine tumors. Endocr. Relat. Cancer 2010, 17, R53–R73. [Google Scholar] [CrossRef] [PubMed]
- Krenning, E.P.; Bakker, W.H.; Breeman, W.A.; Koper, J.W.; Kooij, P.P.; Ausema, L.; Lameris, J.S.; Reubi, J.C.; Lamberts, S.W. Localization of endocrine related tumors with radioiodinated analogue of somatostatin. Lancet 1989, 1, 242–245. [Google Scholar] [CrossRef]
- Erion, J.L.; Bugaj, J.E.; Schmidt, M.A.; Wilhelm, R.R.; Srivanasan, A. High radiotherapeutic efficacy of [Lu-177]-DOTA-Y3-octreotate in a rat tumor model [abstract]. J. Nucl. Med. 1999, 40, 223. [Google Scholar]
- Levine, R.; Krenning, E.P. Clinical History of the Theranostic Radionuclide Approach to Neuroendocrine Tumors and Other Types of Cancer: Historical Review Based on an Interview of Eric P. Krenning by Rachel Levine. J. Nucl. Med. 2017, 58, 3S–9S. [Google Scholar] [CrossRef] [PubMed]
- Lutathera® Summary of Product Characteristics. Available online: https://www.ema.europa.eu/en/documents/product-information/lutathera-epar-product-information_en.pdf (accessed on 23 April 2019).
- Strosberg, J.; El-Haddad, G.; Wolin, E.; Hendifar, A.; Yao, J.; Chasen, B.; Mittra, E.; Kunz, P.L.; Kulke, M.H.; Jacene, H.; et al. NETTER-1 Trial Investigators. Phase 3 trial of 177Lu-dotatate for midgut neuroendocrine tumors. N. Engl. J. Med. 2017, 376, 125–135. [Google Scholar] [CrossRef] [PubMed]
- Aime, S.; Barge, A.; Botta, M.; Fasano, M.; Ayala, J.D.; Bombieri, G. Crystal structure and solution dynamics of the lutetium(III) chelate of DOTA. Inorg. Chim. Acta 1996, 246, 423–426. [Google Scholar] [CrossRef]
- Nomenclature of Inorganic Chemistry, IUPAC Recommendations 2005, IR-9 Coordination Compounds. Available online: https://iupac.org/wp-content/uploads/2016/07/Red_Book_2005.pdf (accessed on 23 July 2019).
- Decay Characteristics of 177Lu. Available online: https://www.nndc.bnl.gov/nudat2/dec_searchi.jsp (accessed on 18 April 2019).
- Zalutsky, M.R. Radionuclide Therapy. In Handbook of Nuclear Chemistry; Vértes, A., Nagy, S., Klencsár, Z., Eds.; Springer US: Heidelberg, Germany, 2004; Volume 4, pp. 315–342. [Google Scholar]
- Kim, Y.C.; Kim, Y.H.; Um, S.H.; Seo, Y.S.; Park, E.K.; Oh, S.Y.; Han, Y.M.; Choe, J.-G. Usefullness of Bremsstrahlung Images after Intra-Arterial Resin Y90 Microsphere Radioembolization for Hepatic Tumors. Nucl. Med. Mol. Imaging 2011, 45, 59–64. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Elschot, M.; Vermolen, B.J.; Lam, M.E.G.H.; de Keizer, B.; van den Bosch, M.A.A.J.; de Jong, H.W.A.M. Quantitative Comparison of PET and Bremsstrahlung SPECT for Imaging the in vivo Yttrium-90 Microsphere Distribution after Liver Radioembolization. PLoS ONE 2013, 8, e55742. [Google Scholar] [CrossRef] [PubMed]
- Aslani, A.; Snowdon, G.M.; Bailey, D.L.; Schembri, G.P.; Bailey, E.A.; Pavlakis, N.; Roach, P.J. Lutetium-177 DOTATATE Production with an Automated Radiopharmaceutical Synthesis System. Asia Ocean. J. Nucl. Med. Biol. 2015, 3, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Lutathera® EPAR. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/lutathera (accessed on 23 April 2019).
- Product Quality Review Application Number 208700Orig1s000. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2018/208700Orig1s000ChemR.pdf (accessed on 23 April 2019).
- Label LUTATHERA®. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/208700s000lbl.pdf (accessed on 23 April 2019).
- Product Monograph for LUTATHERATM for Canada. Available online: https://pdf.hres.ca/dpd_pm/00049099.pdf (accessed on 23 April 2019).
- Krenning Score of Neuroendocrine Tumour Uptake. Available online: https://radiopaedia.org/articles/krenning-score-of-neuroendocrine-tumour-uptake (accessed on 25 June 2019).
- Reubi, J.C.; Schär, J.-C.; Waser, B.; Wenger, S.; Heppeler, A.; Schmitt, J.S.; Mäcke, H.R. Affinity profiles for human somatostatin receptor subtypes SST1–SST5 of somatostatin radiotracers selected for scintigraphic and radiotherapeutic use. Eur. J. Nucl. Med. 2000, 27, 273–282. [Google Scholar] [CrossRef] [PubMed]
- Brechbiel, M.W. Targeted α-therapy–past, present, future? Dalton Trans. 2007, 43, 4918–4928. [Google Scholar] [CrossRef] [PubMed]
- Haberkorn, U.; Giesel, F.; Morgenstern, A.; Kratochwil, C. The Future of Radioligand Therapy: α, β, or Both? J. Nucl. Med. 2017, 58, 1017–1018. [Google Scholar] [CrossRef] [PubMed]
- Milenic, D.E.; Brady, E.D.; Brechbiel, M.W. Antibody-Targeted Radiation Cancer Therapy. Nat. Rev. Drug Discov. 2004, 3, 488–498. [Google Scholar] [CrossRef]
- Abuqbeitah, M.; Demir, M.; Uslu-Beşli, L.; Yeyin, N.; Sönmezoğlu, K. Blood clearance and occupational exposure for 177Lu-DOTATATE compared to 177Lu-PSMA radionuclide therapy. Radiat. Environ. Biophys. 2018, 57, 55–61. [Google Scholar] [CrossRef]
- De Jong, M.; Rolleman, E.J.; Bernard, B.F.; Visser, T.J.; Bakker, W.H.; Breeman, W.A.P.; Krenning, E.P. Inhibition of Renal Uptake of Indium-111-DTPAOctreotide. J. Nucl. Med. 1996, 37, 1388–1392. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Organ | Absorbed Dose Per Unit Activity / Gy/GBq n = 20) | Calculated Absorbed Dose for 4 × 7.4 GBq (29.6 GBq Cumulative Activity) / Gy | ||
|---|---|---|---|---|
| Mean | SD | Mean | SD | |
| Adrenals | 0.037 | 0.016 | 1.1 | 0.5 |
| Breast | 0.027 | 0.016 | 0.8 | 0.5 |
| Heart wall | 0.032 | 0.015 | 0.9 | 0.4 |
| Kidneys | 0.654 | 0.295 | 19.4 | 8.7 |
| Liver * | 0.299 | 0.226 | 8.9 | 6.7 |
| Lungs | 0.031 | 0.015 | 0.9 | 0.4 |
| Muscle | 0.029 | 0.015 | 0.8 | 0.4 |
| Pancreas | 0.038 | 0.016 | 1.1 | 0.5 |
| Red Marrow | 0.035 | 0.029 | 1.0 | 0.8 |
| Spleen | 0.846 | 0.804 | 25.1 | 23.8 |
| Thymus | 0.028 | 0.015 | 0.8 | 0.5 |
| Urinary Bladder Wall | 0.437 | 0.176 | 12.8 | 5.3 |
| Total Body | 0.052 | 0.027 | 1.6 | 0.8 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hennrich, U.; Kopka, K. Lutathera®: The First FDA- and EMA-Approved Radiopharmaceutical for Peptide Receptor Radionuclide Therapy. Pharmaceuticals 2019, 12, 114. https://doi.org/10.3390/ph12030114
Hennrich U, Kopka K. Lutathera®: The First FDA- and EMA-Approved Radiopharmaceutical for Peptide Receptor Radionuclide Therapy. Pharmaceuticals. 2019; 12(3):114. https://doi.org/10.3390/ph12030114
Chicago/Turabian StyleHennrich, Ute, and Klaus Kopka. 2019. "Lutathera®: The First FDA- and EMA-Approved Radiopharmaceutical for Peptide Receptor Radionuclide Therapy" Pharmaceuticals 12, no. 3: 114. https://doi.org/10.3390/ph12030114
APA StyleHennrich, U., & Kopka, K. (2019). Lutathera®: The First FDA- and EMA-Approved Radiopharmaceutical for Peptide Receptor Radionuclide Therapy. Pharmaceuticals, 12(3), 114. https://doi.org/10.3390/ph12030114