Highlights
What are the main findings?
- Heart rate measurements from a commercially wearable device placed over tattoo skin were inaccurate, especially during rest, with error decreasing as exercise intensity increased.
- Skin tone was a significant predictor of measurement error during rest and walking, while tattoo characteristics, such as age and intensity, did not significantly affect heart rate accuracy.
What are the implications of the main findings?
- Wearable device manufacturers should consider skin tone and tattoo presence when designing and calibrating sensors, as these factors can introduce bias and reduce measurement accuracy.
- Excluding tattooed individuals from research studies may compromise generalizability and equity, highlighting the need for inclusive methodologies and improved sensor technologies.
Abstract
This study evaluated the accuracy of heart rate (HR) measures of a commercial wearable device on tattooed skin and assessed tattoo characteristics associated with HR accuracy. Participants (n = 25) wore a chest strap HR monitor (criterion) and an armband HR monitor (experimental) during rest and self-paced walking and running. Conditions with the experimental device on tattooed and non-tattooed sections of skin were completed, and HR was collected every second and compared via Lin’s correlation (CCC) and the mean absolute percent error (MAPE). Skin tone and tattoo age and intensity were evaluated with HR accuracy. HR from tattooed skin was not accurate during rest (MAPE = 22.9%; CCC = 0.25), walking (MAPE = 7.5%; CCC = 0.68), or running (MAPE = 5.1%; CCC = 0.83). Measures taken on non-tattooed skin were within acceptable standards for accuracy throughout all three conditions (MAPE < 5%; CCC > 0.90). Skin tone was the only characteristic found to contribute to HR accuracy during rest (p = 0.046) and walking (p = 0.045). No variables loaded for running. The presence of arm tattoos affected HR readings, with the greatest inaccuracy occurring at rest. Specific tattoo characteristics did not statistically contribute to HR accuracy, as shown by the regression analysis. More research is needed to clarify how the varied tattoo characteristics affect HR devices.
1. Introduction
Obtaining a tattoo for indigenous peoples was less about artistic practice and more about becoming integrated into the community by providing outward evidence of shared societal values [1,2]. As a result, many tattoo experts were religious leaders who had proven themselves to be worthy of respect [2,3]. Despite the religious and cultural tradition, the practice transformed to carry a stigma in certain countries because tattoos were perceived by people as being associated with criminality and deviant behavior [4,5]. However, the popularity of tattoos tends to fluctuate across time and age demographics [4]. In 2012, it was reported that 38% of 30–39 year olds had a tattoo [6], and this value rose to 46% in the same age group in a 2023 poll [7]. It is presently apparent that the popularity of tattooing has increased, with an estimated 32% of the overall U.S. population having at least one tattoo [7].
Another popular practice is the use of wearable technology, which consists of devices worn on the body and capable of returning metrics such as heart rate, step count, or energy expenditure [8]. From 2016 to the present, wearable technology has been listed among the top world-wide fitness trends [9,10]. With respect to physiological metrics returned from wearable devices, heart rate is generally the most accurate, while energy expenditure is the least, and step count falls in between [8,11]. However, heart rate, particularly when used in an applied setting, may be affected by a number of factors such as device placement, motion artifact, and the influence of ambient light [12,13,14].
One factor that may affect heart rate accuracy returned from wearable devices is the presence of tattoos. Because heart rate in wearable devices are obtained through photoplethysmography-reliant (PPG) technology, the signal may be affected by permanent ink deposited into the skin. While recent guidelines have alluded to the possibility that tattoos may affect the PPG signal of wearable devices [15,16,17,18,19], to our knowledge, no direct investigation has evaluated the effect on heart rate accuracy. Perhaps due to the aforementioned recommendations, some research has begun excluding participants who have tattoos from investigations that utilize wearable devices for obtaining metrics [20,21]. This may be problematic, as excluding individuals from research studies can create bias and compromise the generalizability of the results [22].
To date, no direct investigation has been conducted to determine the effect of tattoos on the accuracy of PPG-based heart rate measurements. Our aim was to systematically determine what effect the presence of a tattoo on the arm would have on heart rate validity measures compared to an electrocardiogram-based criterion measure, as well as a sensor of the same make placed over an area of open skin. We hypothesized, based on the literature, that the sensor placed over a tattooed area would result in less valid measurements, while the sensor placed over the open skin would produce valid heart rate measurements. Additionally, we aimed to determine whether certain tattoo characteristics were associated with heart rate accuracy. We hypothesized that the characteristics of some types of tattoos (color, intensity) would be associated with decreased validity measurements, while other characteristics would not.
2. Materials and Methods
2.1. Participants
Participants were recruited for this study via convenience sampling. Inclusion criteria were that they had to pass the health screening, have a tattoo on either arm, and have an open skin section on the same arm as the tattoo because of potential interindividual blood flow differences between arms [23]. Participants who were screened and deemed not to require medical clearance to complete exercise according to the American College of Sports Medicine preparticipation health screening recommendations [24] continued with the investigation. Twenty-five adult participants (female n = 10, male n = 12, gender diverse [transgender MTF, transgender FTM, genderqueer, gender nonconforming, neither exclusively female nor male] n = 3) were selected for this study after completing an informed consent form that was approved by the Institutional Review Board (IRB approval #UNLV-2024-528). Gender and ethnicity were obtained using a self-reported questionnaire (Qualtrics, Provo, UT, USA). The number of gender diverse participants were combined (rather than reported individually) to protect confidentiality.
Our previous work using the same devices to evaluate heart rate validity revealed actual power ranging from 0.8034 to 0.9168 with accompanying sample sizes between 5 and 12 participants [25]. To be conservative, we aimed to test a greater number of participants. Demographic characteristics of participants were as follows: age = 33.7 ± 11.4 yrs; height = 170.7 ± 11.9 cm; mass = 82.8 ± 15.6 kg; age of tattoo = 7.7 ± 8.5 yrs. Self-reported race/ethnicity of participants were as follows: Asian n = 2, Black or African American n = 2, Hispanic, Latino, or Spanish n = 6, Multiracial n = 1, Native Hawaiian or other Pacific Islander n = 2, White n = 11, White, some other race, ethnicity, origin n = 1.
2.2. Protocol
The study consisted of a single day of testing with acute measurements obtained during rest, self-paced walking, and self-paced jogging. Participants were outfitted with a Polar H10 chest strap heart rate monitor (Polar Electro Inc., Kempele, Finland; sampling frequency 1000 Hz), which served as the criterion measure because this family of devices is both valid [26] and reliable [27] at the exercise intensities employed in the current investigation. The experimental devices used in this investigation were the Polar Verity Sense armbands (Polar Electro Inc., Kempele, Finland; sampling frequency 135 Hz). The Polar Verity Sense was chosen because it has shown them to be valid and reliable in a variety of use cases [11,25,28] and it allowed us to place the sensors directly over any tattooed area on the upper or lower arm. All devices (Polar H10, Polar Verity Sense tattoo, Polar Verity Sense open skin) were connected to the PerformTek Data Collector application (Valencell, Inc. Raleigh, NC, USA), which collected the data into a single .csv file per trial and returned heart rate measurements each second.
In this intra-subject design, the criterion device was secured around the chest (see Figure 1). One experimental device was placed over an area of skin at what was perceived by researchers to be the greatest amount of tattoo coverage (see Figure 1). The other experimental device was placed over an area of the skin on the same arm that had no tattoo coverage, as close as possible to the tattooed area to account for potential differences in skin thickness and vascularization (see Figure 1). Once the criterion and experimental devices were secured, the researchers assured all were connected via Bluetooth to the PerformTek Data Collector application, and 5 min of seated rest was completed. Participants then determined their preferred treadmill speeds (WOODWAY 4Front, Waukesha, WI, USA) for walking and running consisting of three self-paced trials per exercise type [29]. During each trial, participants were blinded to the speed displayed on the treadmill and instructed to gradually increase it to a pace they deemed comfortable and sustainable for 5 min of walking or running. The speed was recorded and the procedure repeated three times for walking and three times for running. The speeds from the three trials were averaged to determine individualized self-preferred walking and running speeds. The sample mean speeds were 56.1 ± 18.2 m·min−1 for walking and 110.5 ± 25.7 m·min−1 for running. Participants completed one 5-min bout of self-paced walking followed by one 5-min bout of self-paced running.
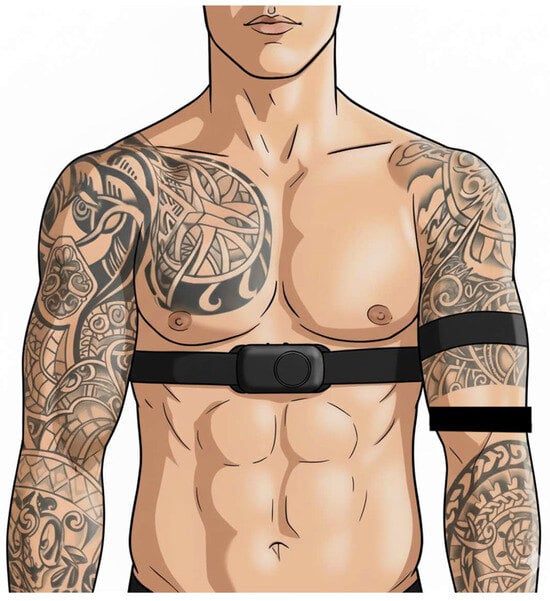
Figure 1.
Example schematic of sensor set up. Polar H10 chest strap was placed around the chest. One Polar Verity Sense was placed around the arm over tattooed skin. The other Polar Verity Sense was placed around the same arm on an area of open skin near the sensor over the tattoo.
The validity of the Fitzpatrick Skin Phototype scale has been questioned in individuals with darker skin tone [30] because it does not account for the diversity of skin tones in people of color [31]. The Monk Skin Tone Scale, a 10-shade scale, was used to reduce artificial intelligence bias for users with colored skin [32]. A digital picture of both the tattooed skin area and the non-tattooed skin area was obtained using an Apple iPhone (16e, iOS Version 18.6.2, Cupertino, CA, USA). The images were evaluated using open-source ImageJ software (version 1.54g) [33]. Briefly, the oval selection option was used to click and drag inside the indentation area left by the Polar Verity Sense (see Figure 2), then the mean gray setting was used to obtain values for mean, minimum (min), and maximum (max) intensity scores. Skin tone was determined using the following procedures: the non-tattooed picture was opened in iOS, and the Digital Color Meter was opened concurrently using the hexadecimal view. The Monk Skin Tone Swatches were visually compared to the hexadecimal displayed, opting for the closest swatch.
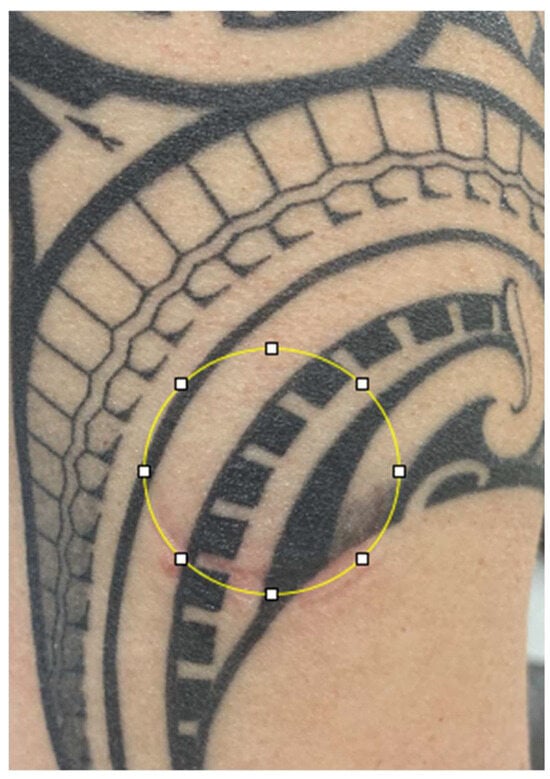
Figure 2.
Example of ImageJ procedure on tattooed skin area. Artist attribution: Kiwi Burt.
2.3. Data Analysis
Data were downloaded from the PerformTek application and copied into a spreadsheet in Google Sheets (Google, LLC, Mountain View, CA, USA) with calculations for the statistical tests noted below. Error analysis was tested via mean absolute percentage error (MAPE). Linearity was assessed via Pearson’s Product Moment Correlation Coefficient (r), and Lin’s Concordance Correlation Coefficient (CCC). Bland–Altman plots were generated with mean bias and 95% confidence intervals and limits of agreement reported. Predetermined thresholds of ≤5% for MAPE [12,34], and ≥0.90 for CCC [12,28] were used. Prediction equations were derived using the Linear Regression function in SPSS (Version 29.0.2.0, IBM Corporation, Armonk, NY, USA) to perform stepwise multiple regression with the predictors of participant mean absolute percentage error being Monk Skin Tone, age of the tattoo, mean intensity of the tattooed area, min intensity of the tattooed area, and max intensity of the tattooed area. The following assumptions were determined: linearity, independence of observations, homoscedasticity, normality of residuals, and multicollinearity. If any of the assumptions were violated, the appropriate action was taken before performing the stepwise multiple regression (i.e., transformation of data, removal of collinear variables).
3. Results
The sensor placed over non-tattooed skin did not function properly in one participant during rest (resulting in 7291 data points rather than 7591, see Table 1). Heart rate validity measures did not meet the threshold for any condition (rest, walk, run) on tattooed skin (see Table 1). Variability in validity measures tended to decrease in tattooed skin as the exercise intensity level increased (see Figure 3, Figure 4 and Figure 5 for a depiction of the Pearson Product Moment Correlation). On the other hand, agreement (in the form of the bias measurement) was narrower during the walk, overestimating heart rate (HR) by nearly 2 beats per minute (bpm), while becoming wider during the run, underestimating HR by 6 bpm. In all cases, the sensor placed over non-tattooed skin met the predetermined validity thresholds (see Table 1).

Table 1.
Validity measures associated with sensors placed over tattooed and non-tattooed skin during rest, walking, and running conditions.
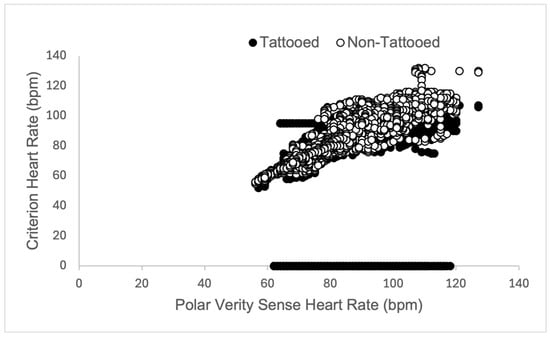
Figure 3.
Graphical representation of Pearson Product Moment Correlation heart rate (measured in beats per minute, bpm) returned from the criterion sensor (Polar H10 chest strap) and experimental sensors (Polar Verity Sense) placed over tattooed skin (closed circles) and non-tattooed skin (open circles) on the upper or lower arm during a 5-min rest period in adult participants (N = 25).
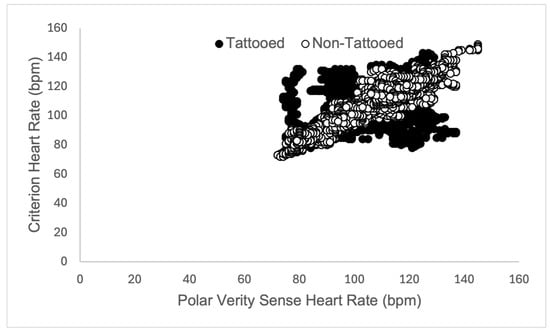
Figure 4.
Graphical representation of Pearson Product Moment Correlation heart rate (measured in beats per minute, bpm) returned from the criterion sensor (Polar H10 chest strap) and experimental sensors (Polar Verity Sense) placed over tattooed skin (closed circles) and non-tattooed skin (open circles) on the upper or lower arm during a 5-min self-paced walk in adult participants (N = 25).
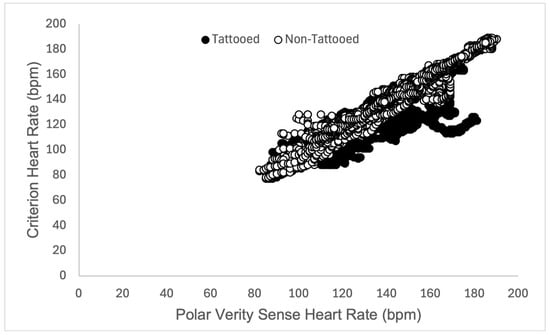
Figure 5.
Graphical representation of Pearson Product Moment Correlation heart rate (measured in beats per minute, bpm) returned from the criterion sensor (Polar H10 chest strap) and experimental sensors (Polar Verity Sense) placed over tattooed skin (closed circles) and non-tattooed skin (open circles) on the upper or lower arm during a 5-min self-paced run in adult participants (N = 25).
Closer inspection of the data revealed that in 9 participants, sensor readings were obtained but dropped out to zero at various points during the tattooed skin resting condition. Because of this, the bias in the resting condition was 16.7 bpm lower than the criterion measure. When these 1486 data points were removed, the tattooed skin resting condition did meet validity thresholds (MAPE = 4.2%, CCC = 0.91, r = 0.92, R2 = 0.84, bias = 0.6 [0.5 to 0.8], and limits of agreement = −11.5 to 12.7).
There was an attempt to determine whether certain tattoo characteristics were associated with heart rate accuracy utilizing individual MAPE percentage over the duration of each trial, and the results of the stepwise multiple regression are shown in Table 2, Table 3 and Table 4. Tattoo characteristics are shown in Table 5. The only significant variable was skin tone in the resting and walking conditions (see Table 2 and Table 3). No significant predictors were noted in the running condition (see Table 4).
Table 2.
Multiple regression model for MAPE (%) in the resting condition.
Table 3.
Multiple regression model for MAPE (%) in the walking condition.
Table 4.
Multiple regression model for MAPE (%) in the running condition.
Table 5.
Tattoo characteristics associated with participants.
4. Discussion
The purpose of this study was to utilize an intra-subject design to determine the extent to which tattoos on the arms affected heart rate readings obtained from wearable technology devices. We hypothesized that the sensor placed over a tattooed area would result in less valid measurements, while the sensor placed over the open skin would produce valid heart rate measurements. Additionally, we hypothesized that the characteristics of some types of tattoos (color, intensity) would be associated with decreased validity measurements, while other characteristics would not. Our main findings, using unfiltered second-by-second data, are that resting measurements of the tattooed area appear to be the least valid, followed by the walking condition (did not meet the 5% MAPE or 0.9 Lin’s threshold), and that the self-paced running condition was least affected (barely did not meet MAPE threshold, and not Lin’s). In all conditions, sensors placed over open skin yielded measurements that met all predetermined validity thresholds. Our second hypothesis was incorrect, as we were unable to derive a regression equation that predicted how tattoos would affect heart rate validity during exercise.
The finding that heart rate validity did not meet predetermined thresholds in the resting condition comes with a caveat. We observed dropouts (i.e., zero bpm heart rate readings) in 9 of 25 participants (36%). When these readings were removed from the analysis, the sensor placed over tattooed skin performed similarly to the sensor on non-tattooed skin (meeting the thresholds for all validity measurements) in the resting condition. The only significant predictor of HR validity during rest and walking was skin tone, with darker skin tones associated with worse validity measurements. A similar phenomenon has been described in the literature on pulse oximeters [35,36,37], where darker skin tone is reported to increase the variability of accuracy measurements. Additionally, emerging evidence suggests the technology found in consumer wearable heart rate device sensors may suffer from the same limitations [16]. It is encouraging to note that recently a smartphone adapter was developed, which offers a recalibration to avoid skin tone bias with the aim of overcoming the variation in blood oxygen saturation observed when oximeters are used on darker skin [38]. We suggest a similar effort be applied to consumer grade wearable devices that return a heart rate measurement, accounting for not only skin tone, but also the presence of tattoos. This is important, as health-related research transitions to greater reliance on data provided by consumer grade wearables, and if uncorrected may exacerbate structural health disparities for people with darker skin tones [39], and also for people with tattoos according to the current research findings.
Wearable device manufacturers including Apple, Garmin, and Biovotion, have acknowledged various factors that may affect the heart rate readings, and one factor is the presence of arm tattoos [40]. While many authors have suggested tattoos may affect heart rate measures obtained from wearable devices [15,16,17,18,19], this is the first study to collect experimental data to address the possibility. The Polar Verity Sense was used because we have shown it to have greater accuracy than other wearable devices in a variety of use cases including trail running [25], overground skipping [11], and simulated pickleball [28]. Other authors have reported the Polar Verity Sense to be accurate during high-intensity interval training [41], while performing tactically relevant movements [42], and during laboratory-based and free-living activities [43]. Thus, we supposed that any variation observed in the accuracy was due to the presence and nature of the tattoo. During the exercising conditions, the presence of a tattoo appeared to affect accuracy to a greater degree during the lower intensity activity (walking), than when a higher intensity activity (running) was performed. This phenomenon is counter to what has been reported in studies utilizing non-tattooed individuals, where an increase in intensity results in worsening heart rate measurement error [44,45,46], and appears to be exacerbated in people with darker skin tones [47]. While more research is needed to elucidate the effect of increasing exercise intensity on heart rate accuracy in people with tattoos, we propose the current observations may be due to an increased ability of the sensor to obtain measures through tattooed skin at increased blood flow rates.
This investigation is not without limitations. While every attempt was made to place the sensors over a tattooed area and open skin area in close proximity, this was not possible on every occasion. Future studies should measure and report the absolute and relative positions of each sensor on the arm to determine whether such differences may contribute to the differences observed in the current study. We acknowledge the INTERLIVE recommendations for heart rate-based studies to test at least 45 participants [48]. The current study tested fewer participants, although effect sizes from a previous investigation with the same device suggest a lower number may be appropriate when second-by-second heart rate data are used [25]. Future studies should aim to include an appropriate number of tattooed participants across skin tone categories. Another limitation is the methodology used to determine the skin tones of participants. Photographs were obtained of the participants’ skin were obtained using a cellular phone after exercise, both of which may have impacted the evaluation. Additionally, while the hexadecimal view on the Digital Color Meter allowed for some degree of confidence, a subjective determination using the Monk Skin Tone swatches ultimately had to be made, as the colors did not exactly match what was presented on the scale. Future research using a wider representation of skin tones and more sensitive methodology may be useful as the entire range of the Monk Skin Tone Scale was not represented in the current investigation. As noted previously, future study is needed to determine the mechanism of action for why heart rate accuracy measures appear to improve on tattooed skin as exercise intensity increases.
In conclusion, these findings indicate that the presence of arm tattoos has an effect on heart rate readings obtained from commercial wearable technology device sensors, with the greatest effect observed at rest and variation decreasing as exercise intensity increases. It should be noted that not all tattoos had an impact on heart rate validity measures. In many individual instances, the presence of an arm tattoo did not affect the heart rate validity measurement at all. Thus, care should be taken when excluding participants based on the presence of tattoos. While tattoos affect the validity of heart rate readings obtained via wearable sensors, more research is needed to elucidate the underlying mechanisms, as well as the effect varied characteristics of the tattoo may have (ink color, ink composition, how deep into the epidermis the tattoo is embedded, saturation of the tattooed area, evidence or not of scarring from the tattoo, etc.).
Author Contributions
Conceptualization, J.W.N.; methodology, J.W.N.; experiments, J.W.N., O.R.P., and R.M.; validation and formal analysis, J.W.N.; investigation, J.W.N., O.R.P., and R.M.; data curation, J.W.N.; writing—original draft preparation, J.W.N. and J.A.B.; writing—review and editing, J.W.N., O.R.P., R.M., and J.A.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of the University of Nevada, Las Vegas (protocol code: UNLV-2024-528, date of approval: 27 November 2024).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Acknowledgments
University of Nevada, Las Vegas (UNLV) is situated on the traditional homelands of Indigenous groups, including the Nuwu or Nuwuvi, Southern Paiute People, descendants of the Tudinu, or Desert People.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| CCC | Lin’s Concordance Correlation Coefficient |
| MAPE | Mean Absolute Percentage Error |
| PPG | Photoplethysmography |
| r | Pearson’s Product-Moment Correlation Coefficient |
References
- Krutak, L. Tattoo Traditions of Native North America: Ancient and Contemporary Expressions of Identity; Stichting LM Publishers: Edam, The Netherlands, 2014. [Google Scholar]
- Krutak, L. The cultural heritage of tattooing: A brief history. Curr. Probl. Dermatol. 2015, 48, 1–5. [Google Scholar]
- Togafau, K. Tatau: A History of Sāmoan Tattooing by Sean Mallon and Sébastien Galliot; University of Hawai’i Press: Honolulu, HI, USA, 2020; pp. 299–301. [Google Scholar]
- Fisher, A.J. Tattooing the Body, Marking Culture. Body Soc. 2002, 8, 91–107. [Google Scholar] [CrossRef]
- Broussard, A.K.; Harton, C.H. Tattoo or taboo? Tattoo stigma and negative attitudes toward tattooed individuals. J. Soc. Psychol. 2018, 158, 521–540. [Google Scholar] [CrossRef]
- Braverman, S. One in Five US Adults Now Has a Tattoo; Harris Poll: New York, NY, USA; Chicago, IL, USA, 2012; pp. 1–6. [Google Scholar]
- Schaeffer, K.; Dinesh, S. 32% of Americans have a tattoo, including 22% who have more than one. Pew Research Center, 15 August 2023. [Google Scholar]
- Bunn, J.; Navalta, W.J.; Fountaine, J.C.; Reece, J. Current State of Commercial Wearable Technology in Physical Activity Monitoring 2015–2017. Int. J. Exerc. Sci. 2018, 11, 503–515. [Google Scholar] [CrossRef]
- Thompson, R.W. Worldwide Survey of Fitness Trends for 2017. ACSM’S Health Fit. J. 2016, 20, 8–17. [Google Scholar] [CrossRef]
- Newsome, M.A.N.; Batrakoulis, A.; Camhi, M.S.; Mcavoy, C.; Sansone, S.J.; Reed, R. 2025 ACSM Worldwide Fitness Trends: Future Directions of the Health and Fitness Industry. ACSM’S Health Fit. J. 2024, 28, 11–25. [Google Scholar] [CrossRef]
- Navalta, W.J.; Davis, W.D.; Carrier, B.; Malek, M.E.; Vargas, N.; Rodriguez, P.J.; Weyers, B.; Carlos, K.; Peck, M. Validity and Reliability of Wearable Devices during Self-Paced Walking, Jogging and Overground Skipping. Sport Mont 2023, 21, 23–29. [Google Scholar] [CrossRef]
- Navalta, W.J.; Montes, J.; Bodell, G.N.; Salatto, W.R.; Manning, W.J.; Debeliso, M. Concurrent heart rate validity of wearable technology devices during trail running. PLoS ONE 2020, 15, e0238569. [Google Scholar] [CrossRef]
- Estepp, R.J.; Blackford, B.E.; Meier, M.C. Recovering pulse rate during motion artifact with a multi-imager array for non-contact imaging photoplethysmography. In Proceedings of the 2014 IEEE International Conference on Systems, Man, and Cybernetics (SMC) 2014, San Diego, CA, USA, 5–8 October 2014. [Google Scholar] [CrossRef]
- Trivedi, S.N.; Ghouri, F.A.; Shah, K.N.; Lai, E.; Barker, J.S. Effects of motion, ambient light, and hypoperfusion on pulse oximeter function. J. Clin. Anesth. 1997, 9, 179–183. [Google Scholar] [CrossRef]
- Nelson, W.B.; Low, A.C.; Jacobson, N.; Areán, P.; Torous, J.; Allen, B.N. Guidelines for wrist-worn consumer wearable assessment of heart rate in biobehavioral research. npj Digit. Med. 2020, 3, 90. [Google Scholar] [CrossRef]
- Koerber, D.; Khan, S.; Shamsheri, T.; Kirubarajan, A.; Mehta, S. Accuracy of Heart Rate Measurement with Wrist-Worn Wearable Devices in Various Skin Tones: A Systematic Review. J. Racial Ethn. Health Dispar. 2023, 10, 2676–2684. [Google Scholar] [CrossRef]
- Weiler, D.T.; Villajuan, S.O.; Edkins, L.; Cleary, S.; Saleem, J.J. Wearable heart rate monitor technology accuracy in research: A comparative study between PPG and ECG technology. Proc. Hum. Factors Ergon. Soc. Annu. Meet. 2017, 61, 1292–1296. [Google Scholar] [CrossRef]
- Teixeira, E.; Fonseca, H.; Diniz-Sousa, F.; Veras, L.; Boppre, G.; Oliveira, J.; Pinto, D.; Alves, J.A.; Barbosa, A.; Mendes, R.; et al. Wearable Devices for Physical Activity and Healthcare Monitoring in Elderly People: A Critical Review. Geriatrics 2021, 6, 38. [Google Scholar] [CrossRef]
- Scardulla, F.; Cosoli, G.; Spinsante, S.; Poli, A.; Iadarola, G.; Pernice, R.; Busacca, A.; Pasta, S.; Scalise, L.; D’Acquisto, L. Photoplethysmograhic sensors, potential and limitations: Is it time for regulation? A comprehensive review. Measurement 2023, 218, 113150. [Google Scholar] [CrossRef]
- Icenhower, A.; Murphy, C.; Brooks, K.A.; Irby, M.; N’Dah, K.; Robison, J.; Fanning, J. Investigating the accuracy of Garmin PPG sensors on differing skin types based on the Fitzpatrick scale: Cross-sectional comparison study. Front. Digit. Health 2025, 7, 1553565. [Google Scholar] [CrossRef] [PubMed]
- Sameer, K. Health Electronic Assessment of Risks and Trends Using Biometric Equipment and Technology. Available online: https://tulane.trialstoday.org/trial/NCT06753045 (accessed on 23 April 2025).
- Lohner, V.; Enkirch, J.S.; Hattingen, E.; Stöcker, T.; Breteler, B.M.M. Safety of Tattoos, Permanent Make-Up, and Medical Implants in Population-Based 3T Magnetic Resonance Brain Imaging: The Rhineland Study. Front. Neurol. 2022, 13, 795573. [Google Scholar] [CrossRef] [PubMed]
- Essa, A.R.; Ahmed, K.S. Prevalence of inter-arm blood pressure difference among young healthy adults: Results from a large cross-sectional study on 3235 participants. Ann. Med. Surg. 2022, 77, 103631. [Google Scholar] [CrossRef]
- Riebe, D.; Franklin, A.B.; Thompson, D.P.; Garber, E.C.; Whitfield, P.G.; Magal, M.; Pescatello, S.L. Updating ACSM’s Recommendations for Exercise Preparticipation Health Screening. Med. Sci. Sports Exerc. 2015, 47, 2473–2479. [Google Scholar] [CrossRef]
- Navalta, W.J.; Davis, W.D.; Malek, M.E.; Carrier, B.; Bodell, G.N.; Manning, W.J.; Cowley, J.; Funk, M.; Lawrence, M.M.; Debeliso, M. Heart rate processing algorithms and exercise duration on reliability and validity decisions in biceps-worn Polar Verity Sense and OH1 wearables. Sci. Rep. 2023, 13, 11736. [Google Scholar] [CrossRef]
- Schaffarczyk, M.; Rogers, B.; Reer, R.; Gronwald, T. Validity of the Polar H10 Sensor for Heart Rate Variability Analysis during Resting State and Incremental Exercise in Recreational Men and Women. Sensors 2022, 22, 6536. [Google Scholar] [CrossRef]
- Montes, J.; Navalta, W.J. Reliability of the Polar T31 Uncoded Heart Rate Monitor in Free Motion and Treadmill Activities. Int. J. Exerc. Sci. 2019, 12, 69–76. [Google Scholar] [CrossRef]
- Navalta, J.; Carrier, B.; Blank, M.; Zarei, S.; Davis, D.; Craig, M.; Perez, O.; Baca, J.; Sweder, T.; Carballo, T.; et al. Validity and Reliability of Wearable Technology Devices during Simulated Pickleball Game Play. Sports 2024, 12, 234. [Google Scholar] [CrossRef] [PubMed]
- Mercer, A.M.; Stone, M.T.; Young, C.J.; Mercer, A.J. Running Economy While Running in Shoes Categorized as Maximal Cushioning. Int. J. Exerc. Sci. 2018, 11, 1031–1040. [Google Scholar] [CrossRef]
- Sommers, S.M.; Fargo, D.J.; Regueira, Y.; Brown, M.K.; Beacham, L.B.; Perfetti, R.A.; Everett, S.J.; Margolis, J.D. Are the Fitzpatrick Skin Phototypes Valid for Cancer Risk Assessment in a Racially and Ethnically Diverse Sample of Women? Ethn. Dis. 2019, 29, 505–512. [Google Scholar] [CrossRef]
- Wilkes, M.; Wright, Y.C.; Plessis, D.L.J.; Reeder, A. Fitzpatrick Skin Type, Individual Typology Angle, and Melanin Index in an African Population. JAMA Dermatol. 2015, 151, 902. [Google Scholar] [CrossRef]
- Monk, E. The Monk Skin Tone Scale. 2023. Available online: https://skintone.google (accessed on 15 December 2024).
- Abràmoff, M.D.; Magalhães, P.J.; Ram, S.J. Image processing with ImageJ. Biophotonics Int. 2004, 11, 36–42. [Google Scholar]
- Navalta, W.J.; Ramirez, G.G.; Maxwell, C.; Radzak, N.K.; Mcginnis, R.G. Validity and Reliability of Three Commercially Available Smart Sports Bras during Treadmill Walking and Running. Sci. Rep. 2020, 10, 7397. [Google Scholar] [CrossRef] [PubMed]
- Bickler, E.P.; Feiner, R.J.; Severinghaus, W.J. Effects of Skin Pigmentation on Pulse Oximeter Accuracy at Low Saturation. Anesthesiology 2005, 102, 715–719. [Google Scholar] [CrossRef] [PubMed]
- Feiner, R.J.; Severinghaus, W.J.; Bickler, E.P. Dark Skin Decreases the Accuracy of Pulse Oximeters at Low Oxygen Saturation: The Effects of Oximeter Probe Type and Gender. Anesth. Analg. 2007, 105, S18–S23. [Google Scholar] [CrossRef]
- Sjoding, W.M.; Dickson, P.R.; Iwashyna, J.T.; Gay, E.S.; Valley, S.T. Racial Bias in Pulse Oximetry Measurement. N. Engl. J. Med. 2020, 383, 2477–2478. [Google Scholar] [CrossRef]
- Adams, T.A.; Mandel, I.; Gao, Y.; Heckman, W.B.; Nandakumar, R.; Choudhury, T. Equity-Driven Sensing System for Measuring Skin Tone–Calibrated Peripheral Blood Oxygen Saturation (OptoBeat): Development, Design, and Evaluation Study. JMIR Biomed. Eng. 2022, 7, e34934. [Google Scholar] [CrossRef]
- Colvonen, J.P.; Deyoung, N.P.; Bosompra, A.N.-O.; Owens, L.R. Limiting racial disparities and bias for wearable devices in health science research. Sleep 2020, 43, zsaa159. [Google Scholar] [CrossRef]
- Bent, B.; Goldstein, A.B.; Kibbe, A.W.; Dunn, P.J. Investigating sources of inaccuracy in wearable optical heart rate sensors. npj Digit. Med. 2020, 3, 18. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Barker, R.A.; Li, M.; Gu, Y.; Williams, A.C. Validation of polar verity sense for heart rate monitoring during school-based high-intensity interval training in adolescents. J. Sports Sci. 2025, 43, 1076–1084. [Google Scholar] [CrossRef]
- Merrigan, J.J.; Stovall, H.J.; Stone, D.J.; Stephenson, M.; Finomore, S.V.; Hagen, A.J. Validation of Garmin and Polar Devices for Continuous Heart Rate Monitoring During Common Training Movements in Tactical Populations. Meas. Phys. Educ. Exerc. Sci. 2023, 27, 234–247. [Google Scholar] [CrossRef]
- Neudorfer, M.; Kumar, D.; Smeddinck, D.J.; Kulnik, T.S.; Niebauer, J.; Treff, G.; Sareban, M. Validity of Four Consumer-Grade Optical Heart Rate Sensors for Assessing Volume and Intensity Distribution of Physical Activity. Scand. J. Med. Sci. Sports 2024, 34, e14756. [Google Scholar] [CrossRef] [PubMed]
- Muggeridge, J.D.; Hickson, K.; Davies, V.A.; Giggins, M.O.; Megson, L.I.; Gorely, T.; Crabtree, R.D. Measurement of Heart Rate Using the Polar OH1 and Fitbit Charge 3 Wearable Devices in Healthy Adults During Light, Moderate, Vigorous, and Sprint-Based Exercise: Validation Study. JMIR mHealth uHealth 2021, 9, e25313. [Google Scholar] [CrossRef] [PubMed]
- Montalvo, S.; Martinez, A.; Arias, S.; Lozano, A.; Gonzalez, P.M.; Dietze-Hermosa, S.M.; Boyea, L.B.; Dorgo, S. Commercial Smart Watches and Heart Rate Monitors: A Concurrent Validity Analysis. J. Strength Cond. Res. 2023, 37, 1802–1808. [Google Scholar] [CrossRef]
- Støve, P.M.; Haucke, E.; Nymann, L.M.; Sigurdsson, T.; Larsen, T.B. Accuracy of the wearable activity tracker Garmin Forerunner 235 for the assessment of heart rate during rest and activity. J. Sports Sci. 2019, 37, 895–901. [Google Scholar] [CrossRef]
- Hung, H.S.; Serwa, K.; Rosenthal, G.; Eng, J.J. Validity of heart rate measurements in wrist-based monitors across skin tones during exercise. PLoS ONE 2025, 20, e0318724. [Google Scholar] [CrossRef]
- Mühlen, M.J.; Stang, J.; Skovgaard, L.E.; Judice, B.P.; Molina-Garcia, P.; Johnston, W.; Sardinha, B.L.; Ortega, B.F.; Caulfield, B.; Bloch, W.; et al. Recommendations for determining the validity of consumer wearable heart rate devices: Expert statement and checklist of the INTERLIVE Network. Br. J. Sports Med. 2021, 55, 767–779. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).