

mmWave-RM: A Respiration Monitoring and Pattern Classification System Based on mmWave Radar

Abstract
1. Introduction
2. Related Work
3. Proposed System
3.1. Respiratory Signal Modelling
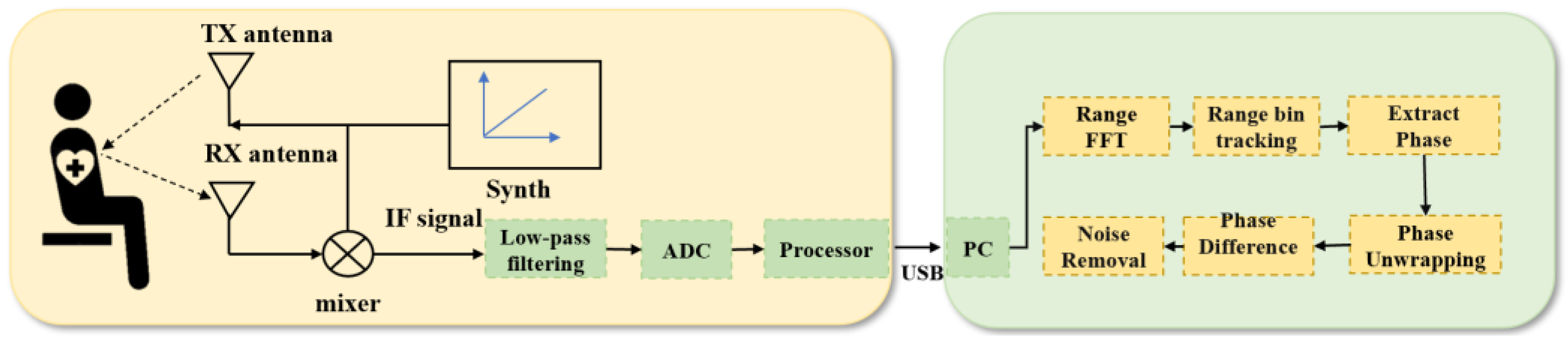
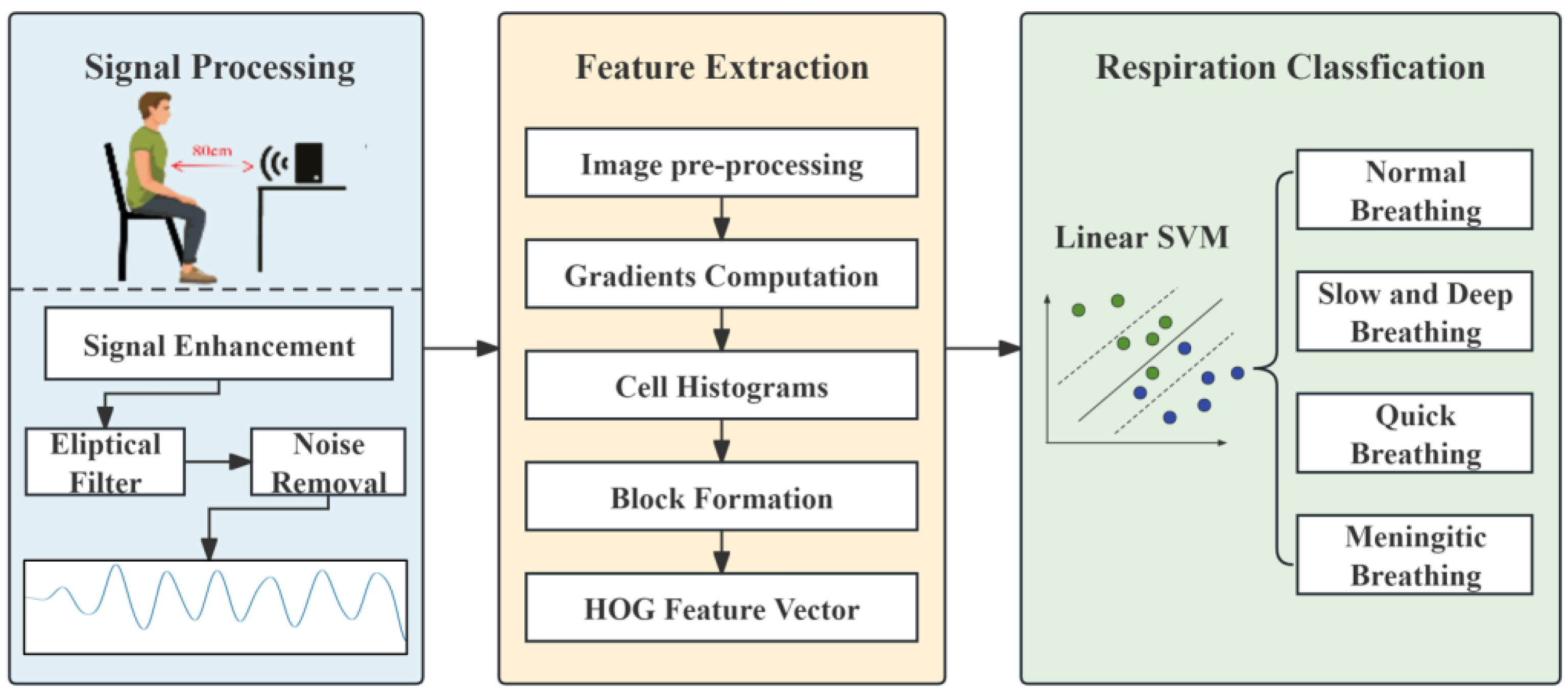
3.2. System Overview
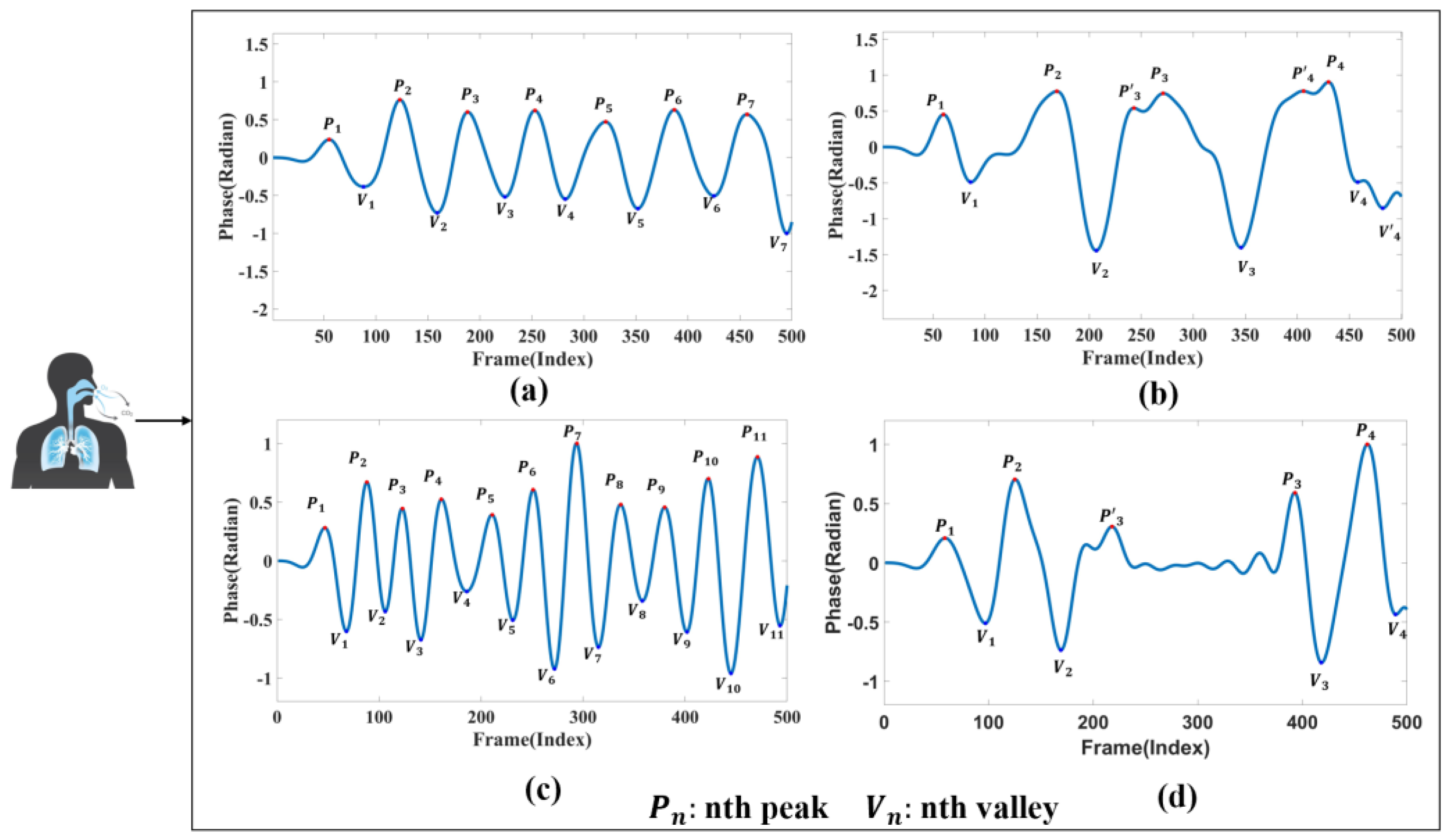
3.3. Breathing Pattern Definition
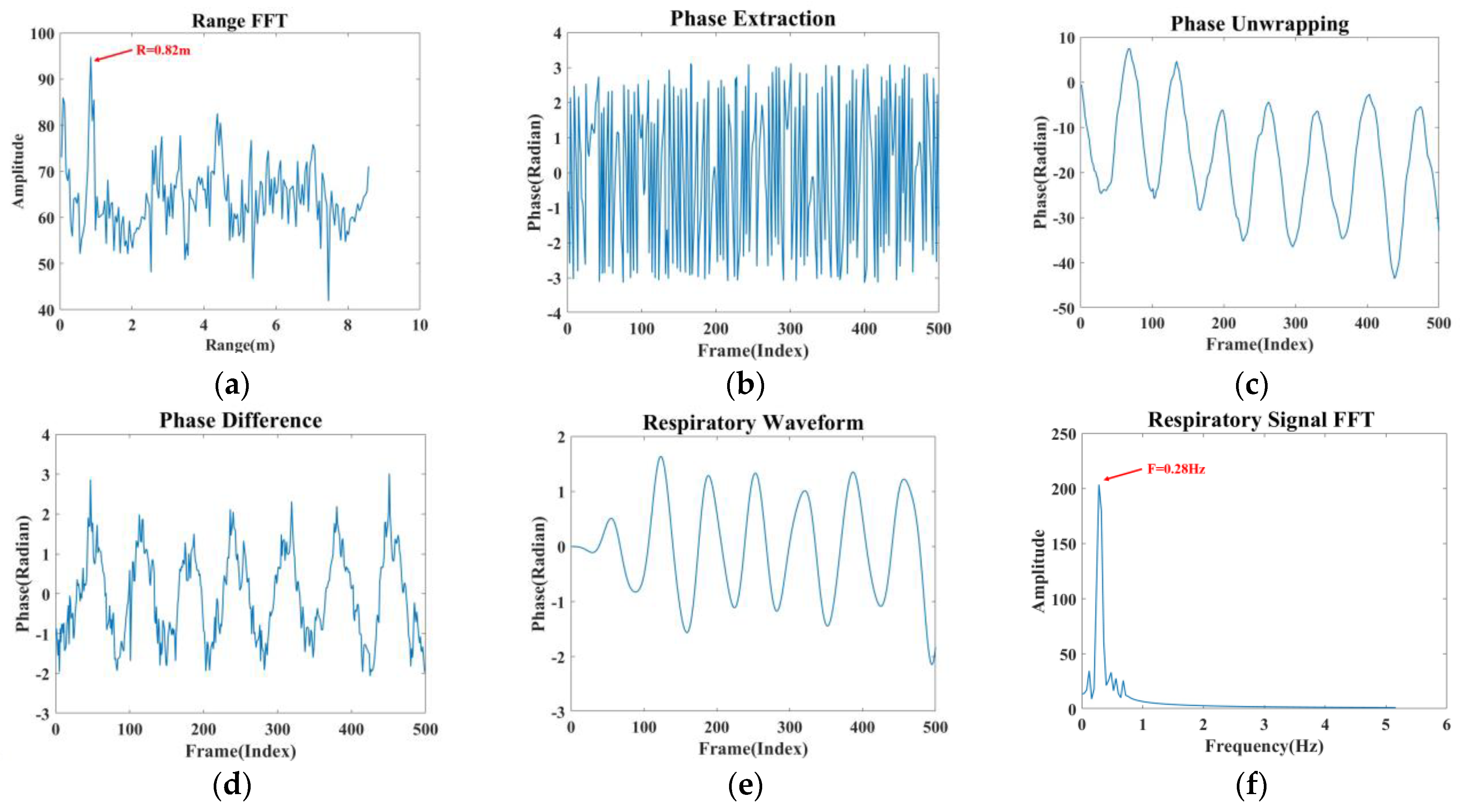
3.4. Signal Processing Module
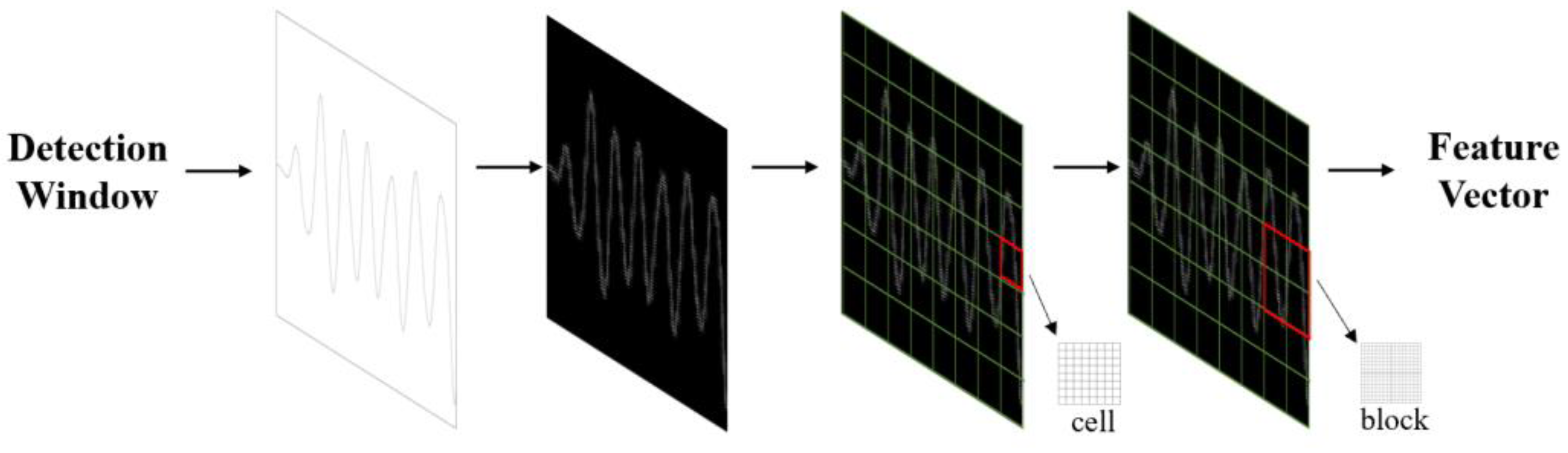
3.5. Feature Extraction Module
3.6. Breathing Pattern Classification Module
| Algorithm 1: Steps of FMCW-RM |
| Input: Dataset (Mi,Ni)(i = 1,2,⋯⋯,n) Output: Classification accuracy 1. img=resize(img,(256,256)) 2. G_magnitude = sqrt(power(Gx, 2) + power(Gy, 2))//Calculate gradient value 3. G_angle =arctan2(Gx, Gy) 4. bins=Get_bins(G_magnitude, G_angle, cell_size, bin_count)// Calculate the histogram of the gradient 5. function Block_Vector(bins, cell_x, cell_y, bin_count) 6. For i in range(0, self.cell_x − 1): 7. For j in range(0, self.cell_y − 1): 8. magnitude =mag(feature)// calculates the magnitude of feature 9. end for 10. end for 11. return block_vector 12. end function 13. clf = svm.SVC( )//model training 14. clf.fit(train_data, train_target) 15. pred = clf.predict(test_data)// model prediction 16. accuracy = calculate_accuracy(test_target, pred) 17. return accuracy |
4. Experimentation and Evaluation
4.1. Experimental Parameters and Environment Settings
4.2. Reliability Validation of Millimetre Wave Radar Measurement Methods
4.3. Physical Environment Analysis
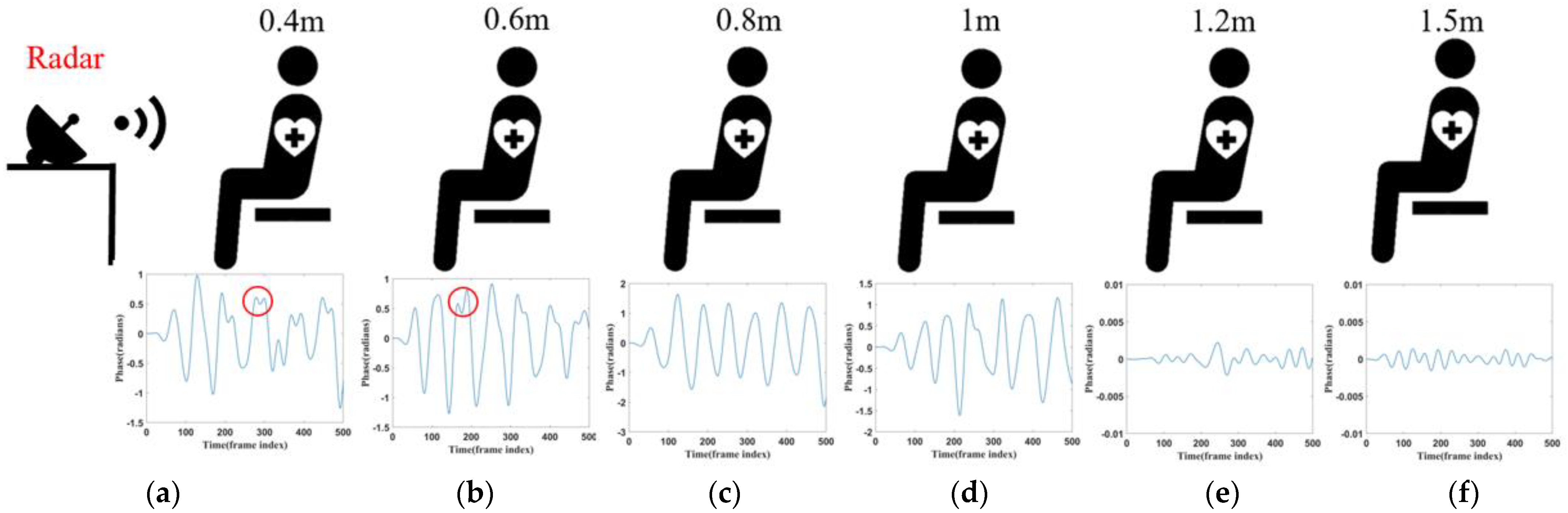
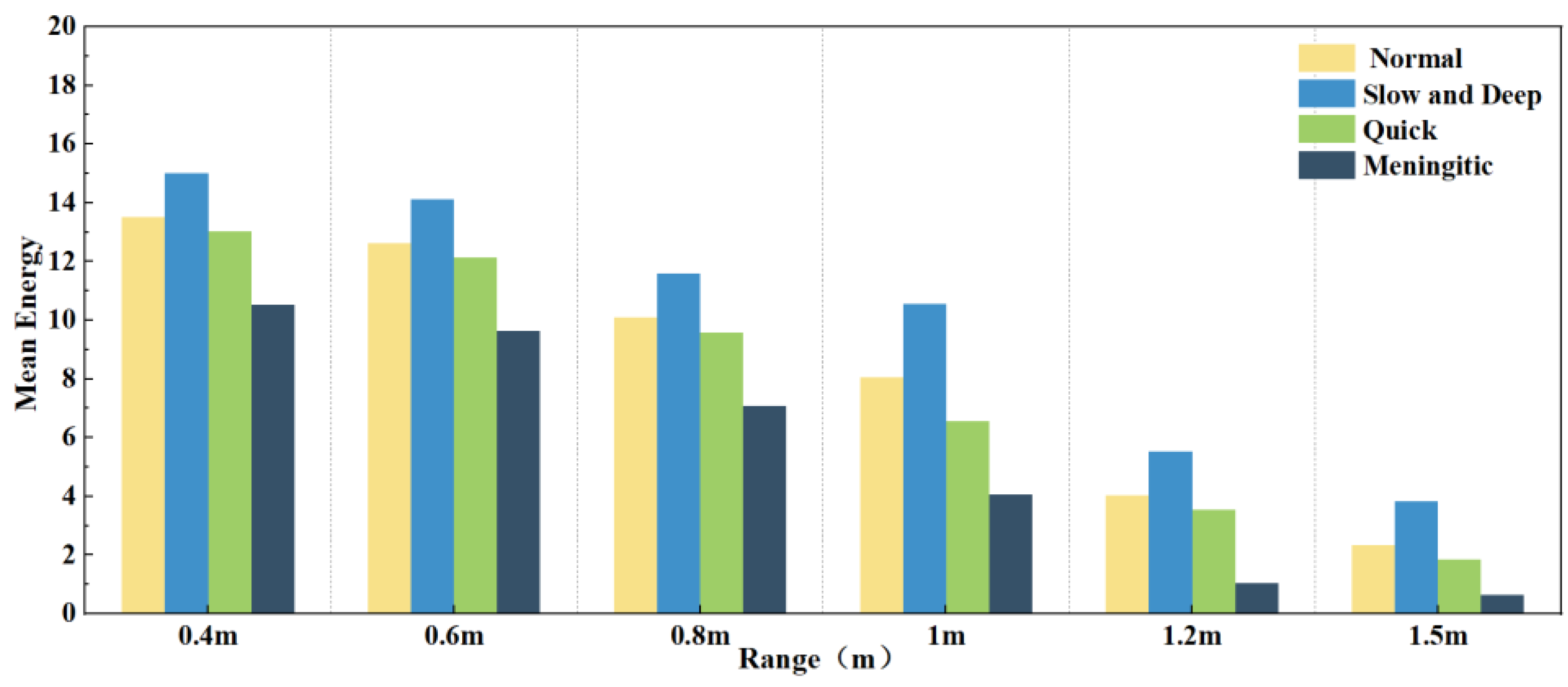
4.3.1. Distance Analysis
4.3.2. Analysis of Diversity in Personnel Status
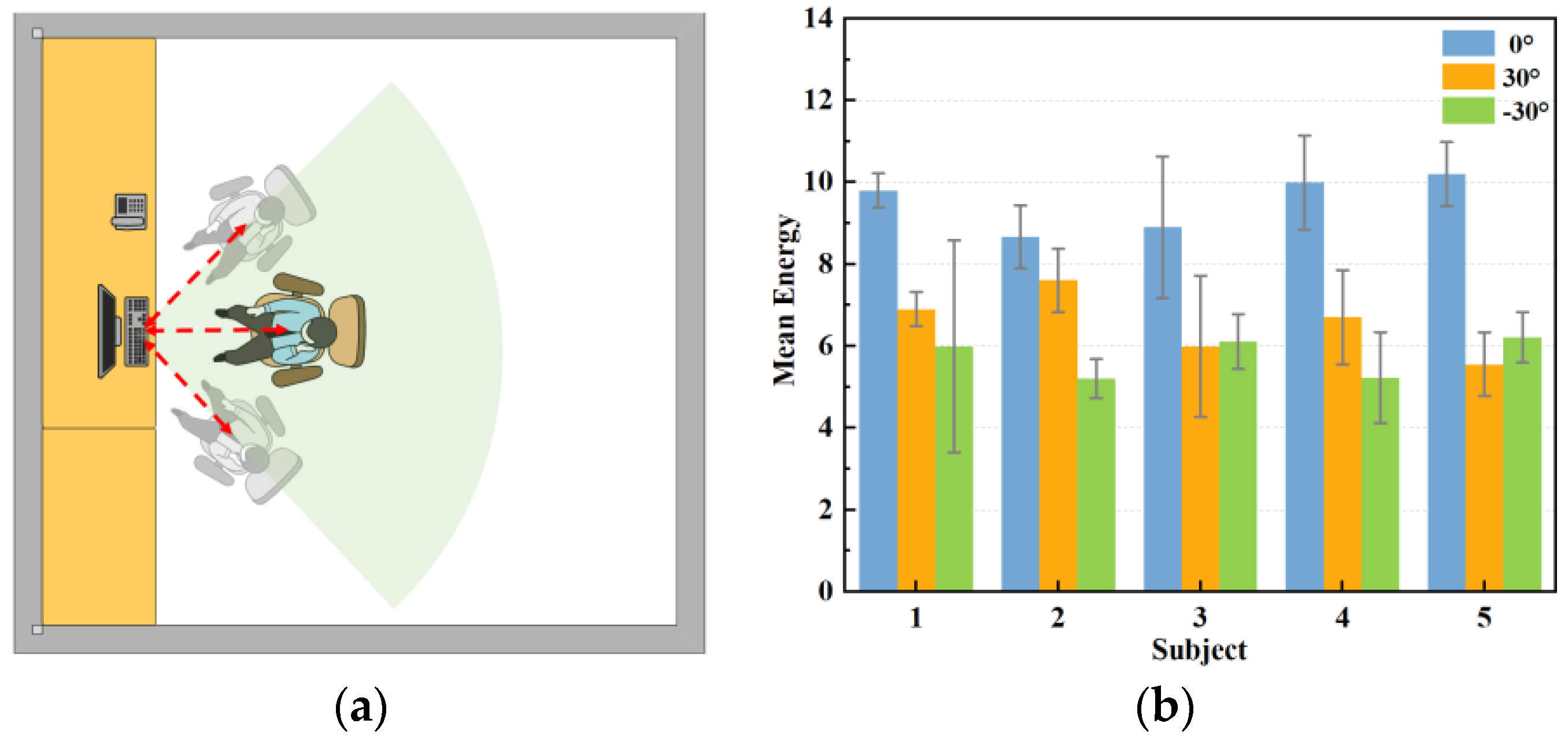
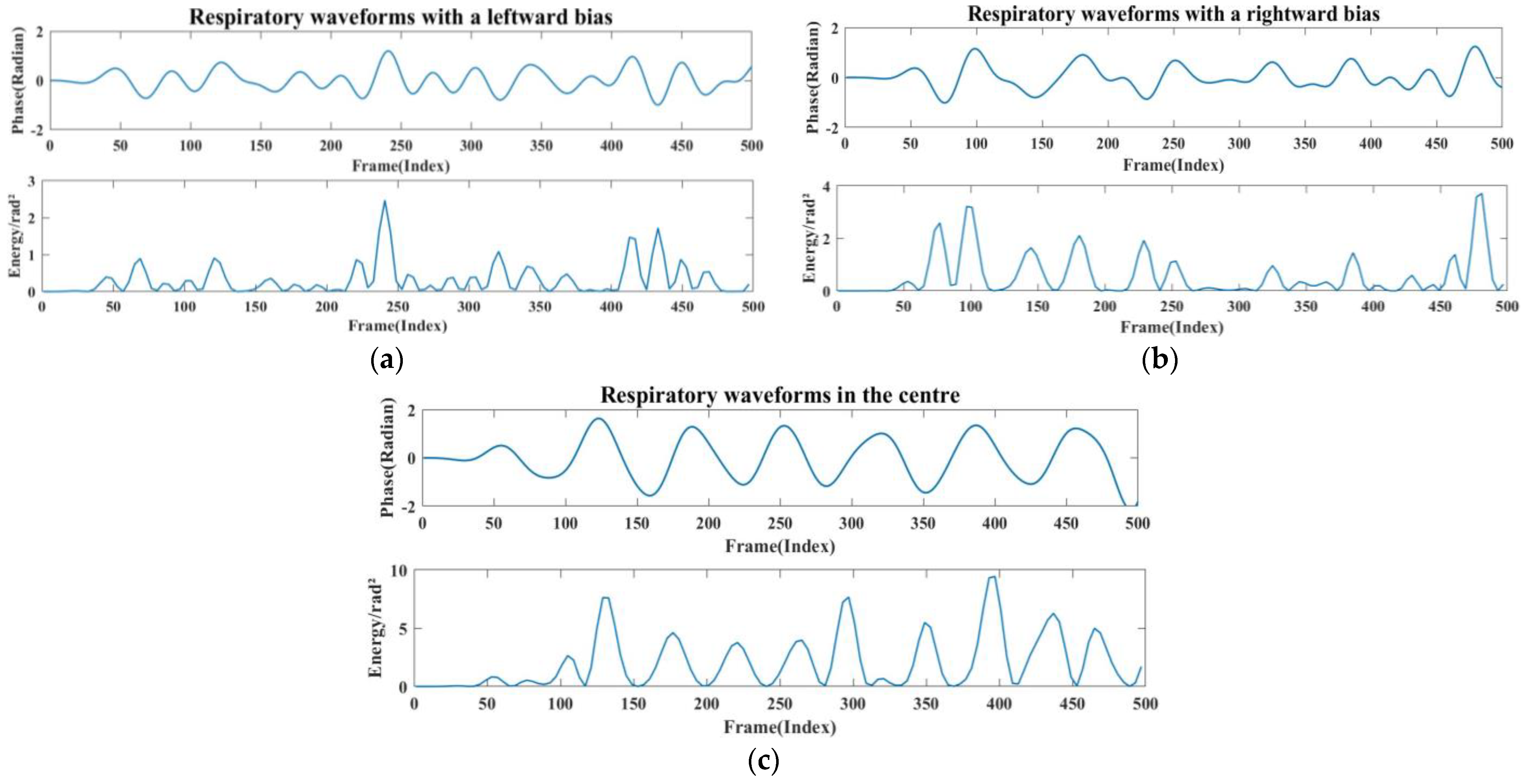
4.3.3. Perspective Analysis
4.3.4. Analysis of Different Experimental Environments
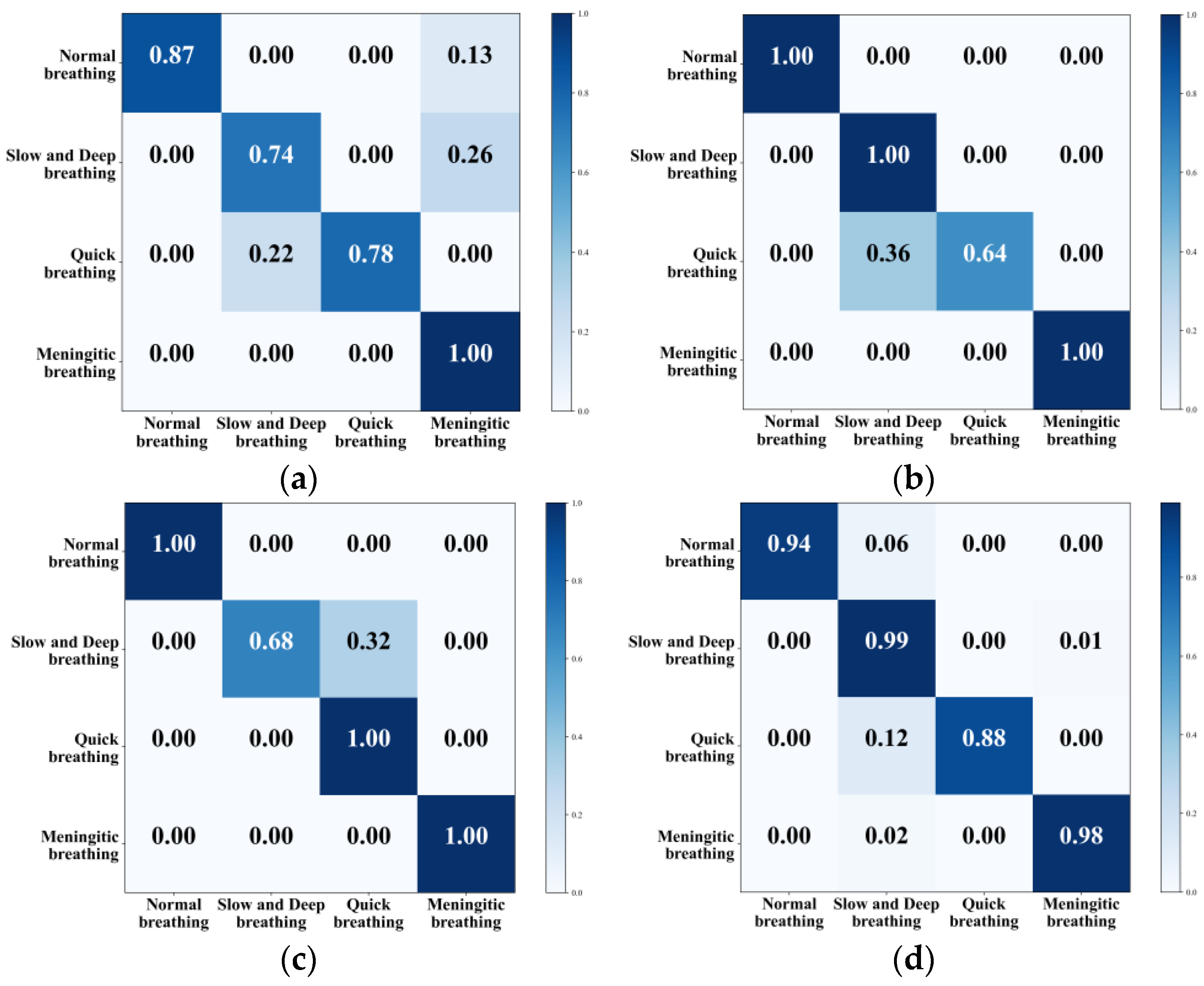
4.4. Classification Results
4.5. Comparison with Recent Research Work
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- West, J.B. Respiratory Physiology: The Essentials; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2012. [Google Scholar]
- Bousquet, J.; Dahl, R.; Khaltaev, N. Global alliance against chronic respiratory diseases. Eur. Respir. J. 2007, 29, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Olaithe, M.; Bucks, R.S. Executive dysfunction in OSA before and after treatment: A meta-analysis. Sleep 2013, 36, 1297–1305. [Google Scholar] [CrossRef]
- Jin, F.; Zhang, R.; Sengupta, A.; Cao, S.; Hariri, S.; Agarwal, N.K.; Agarwal, S.K. Multiple patients behavior detection in real-time using mmWave radar and deep CNNs. In Proceedings of the 2019 IEEE Radar Conference (RadarConf), Boston, MA, USA, 22–26 April 2019; pp. 1–6. [Google Scholar]
- Adib, F.; Mao, H.; Kabelac, Z. Smart homes that monitor breathing and heart rate. In Proceedings of the 33rd Annual ACM Conference on Human Factors in Computing Systems, Seoul, Republic of Korea, 18–23 April 2015; pp. 837–846. [Google Scholar]
- Vapnik, V. The Nature of Statistical Learning Theory; Springer Science & Business Media: New York, NY, USA, 2013. [Google Scholar]
- He, S.; Han, Z.; Iglesias, C.; Mehta, V.; Bolic, M. A real-time respiration monitoring and classification system using a depth camera and radars. Front. Physiol. 2022, 13, 799621. [Google Scholar] [CrossRef] [PubMed]
- Alizadeh, M.; Shaker, G. Remote monitoring of human vital signs using mm-wave FMCW radar. IEEE Access 2019, 7, 54958–54968. [Google Scholar] [CrossRef]
- Kiyokawa, H.; Greenberg, M.; Shirota, K.; Pasterkamp, H. Auditory detection of simulated crackles in breath sounds. Chest 2001, 119, 1886–1892. [Google Scholar] [CrossRef] [PubMed]
- Andreozzi, E.; Fratini, A.; Esposito, D.; Naik, G.; Polley, C.; Gargiulo, G.D.; Bifulco, P. Forcecardiography: A novel technique to measure heart mechanical vibrations onto the chest wall. Sensors 2020, 20, 3885. [Google Scholar] [CrossRef] [PubMed]
- Inan, O.T.; Migeotte, P.F.; Park, K.S.; Etemadi, M.; Tavakolian, K.; Casanella, R.; Di Rienzo, M. Ballistocardiography and seismocardiography: A review of recent advances. IEEE J. Biomed. Health Inform. 2014, 19, 1414–1427. [Google Scholar] [CrossRef]
- Sieciński, S.; Kostka, P.S.; Tkacz, E.J. Gyrocardiography: A review of the definition, history, waveform description, and applications. Sensors 2020, 20, 6675. [Google Scholar] [CrossRef]
- Liu, H.; Allen, J.; Zheng, D.; Chen, F. Recent development of respiratory rate measurement technologies. Physiol. Meas. 2019, 40, 07TR01. [Google Scholar] [CrossRef]
- Vanegas, E.; Igual, R.; Plaza, I. Piezoresistive breathing sensing system with 3d printed wearable casing. J. Sens. 2019, 2019, 2431731. [Google Scholar] [CrossRef]
- Mah, A.J.; Nguyen, T.; Ghazi Zadeh, L.; Shadgan, A.; Khaksari, K.; Nourizadeh, M.; Zaidi, A.; Park, S.; Gandjbakhche, A.H.; Shadgan, B. Optical Monitoring of breathing patterns and tissue oxygenation: A potential application in COVID-19 screening and monitoring. Sensors 2022, 22, 7274. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Park, S.; Nguyen, T. Simulated Breathing Patterns Classification Using Convolutional Neural Network with Deep Embedded Features. In Proceedings of the 2024 IEEE International Conference on Consumer Electronics (ICCE), Las Vegas, NV, USA, 6–8 January 2024; pp. 1–3. [Google Scholar]
- Ceniccola, G.D.; Castro, M.G.; Piovacari, S.M.F. Current technologies in body composition assessment: Advantages and disadvantages. Nutrition 2019, 62, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Lin, Z.Q.; Wong, A. Covid-net: A tailored deep convolutional neural network design for detection of COVID-19 cases from chest x-ray images. Sci. Rep. 2020, 10, 19549. [Google Scholar] [CrossRef] [PubMed]
- Armenta-Garcia, J.A.; Gonzalez-Navarro, F.F.; Caro-Gutierrez, J. Mining Wi-Fi Channel State Information for breathing and heart rate classification. Pervasive Mob. Comput. 2023, 91, 101768. [Google Scholar] [CrossRef]
- Kontou, P.; Smida, S.B.; Anagnostou, D.E. Contactless Respiration Monitoring using Wi-Fi and Artificial Neural Network Detection Method. IEEE J. Biomed. Health Inform. 2023, 28, 1297–1308. [Google Scholar] [CrossRef] [PubMed]
- Guo, Z.; Yuan, W.; Gui, L. BreatheBand: A fine-grained and robust respiration monitor system using WiFi signals. ACM Trans. Sens. Netw. 2023, 19, 1–18. [Google Scholar] [CrossRef]
- Ji, S.; Wen, H.; Wu, J.; Zhang, Z.; Zhao, K. Systematic heartbeat monitoring using a FMCW mm-wave radar. In Proceedings of the 2021 IEEE International Conference on Consumer Electronics and Computer Engineering (ICCECE), Guangzhou, China, 15–17 January 2021; pp. 714–718. [Google Scholar]
- Abdul-Atty, M.M.; Mabrouk, M.; Elramly, S. Design and implementation of a low cost FMCW radar with configurable signal processor for human movement and breathing detection. In Proceedings of the Research World International Conference, Saint Petersburg, Russia, 7–8 September 2019; pp. 5–10. [Google Scholar]
- Avian, C.; Leu, J.S.; Ali, E.; Putro, N.A.S. Non-contact Breathing Patterns Recognition with FMCW Radar by Processing Temporal Information using Transformer Network. In Proceedings of the 2023 Asia-Pacific Microwave Conference (APMC), Taipei, Taiwan, 5–8 December 2023; pp. 420–422. [Google Scholar]
- Wang, Y.; Liu, H.; Xiang, W.; Shui, Y. A Novel Non-contact Respiration and Heartbeat Detection Method Using Frequency-Modulated Continuous Wave Radar. IEEE Sens. J. 2024, 24, 10434–10446. [Google Scholar] [CrossRef]
- Miao, D.; Zhao, H.; Hong, H. Doppler radar-based human breathing patterns classification using Support Vector Machine. In Proceedings of the 2017 IEEE radar conference (RadarConf), Seattle, WA, USA, 8–12 May 2017; pp. 0456–0459. [Google Scholar]
- Feng, C.; Zhao, H.; Liu, Q. Implementation of radar-based breathing disorder recognition using FPGA. In Proceedings of the 2019 IEEE MTT-S International Microwave Biomedical Conference (IMBioC), Nanjing, China, 6–8 May 2019; Volume 1, pp. 1–3. [Google Scholar]
- Cinyol, F.; Baysal, U.; Köksal, D.; Babaoğlu, E. Incorporating support vector machine to the classification of respiratory sounds by Convolutional Neural Network. Biomed. Signal Process. Control 2023, 79, 104093. [Google Scholar] [CrossRef]
- Hong, J.W.; Kim, S.H.; Han, G.T. Detection of multiple respiration patterns based on 1D SNN from continuous human breathing signals and the range classification method for each respiration pattern. Sensors 2023, 23, 5275. [Google Scholar] [CrossRef]
- Wang, Q.; Dong, Z.; Liu, D.; Cao, T.; Zhang, M.; Liu, R.; Sun, J. Frequency-modulated continuous wave radar respiratory pattern detection technology based on multifeature. J. Healthc. Eng. 2021, 2021, 9376662. [Google Scholar] [CrossRef]
- Li, Z.; Jin, T.; Dai, Y.; Song, Y. Motion-Robust Contactless Heartbeat Sensing Using 4D Imaging Radar. IEEE Trans. Instrum. Meas. 2023, 72, 1–10. [Google Scholar]
- Guyton, A.C. Text Book of Medical Physiology; Elsevier Saunders: Philadelphia, PA, USA, 2006. [Google Scholar]
- Yuan, G.; Drost, N.A.; McIvor, R.A. Respiratory rate and breathing pattern. McMaster Univ. Med. J. 2013, 10, 23–25. [Google Scholar]
- Adrogué, H.J.; Madias, N.E. Management of life-threatening acid–base disorders. N. Engl. J. Med. 1998, 338, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Rehman, M.; Shah, R.A.; Khan, M.B. Improving machine learning classification accuracy for breathing abnormalities by enhancing dataset. Sensors 2021, 21, 6750. [Google Scholar] [CrossRef]
- Hao, Z.; Yan, H.; Dang, X.; Ma, Z.; Ke, W.; Jin, P. RMVS: Remote Monitoring of Vital Signs with mm-Wave Radar. In Proceedings of the 1st ACM Workshop on AI Empowered Mobile and Wireless Sensing, Sydney, NSW, Australia, 21 October 2022; pp. 1–6. [Google Scholar]
- Dalal, N.; Triggs, B. Histograms of oriented gradients for human detection. In Proceedings of the 2005 IEEE Computer Society Conference on Computer Vision and Pattern Recognition (CVPR’05), San Diego, CA, USA, 20–25 June 2005; pp. 886–893. [Google Scholar]
- Purnomo, A.T.; Lin, D.B.; Adiprabowo, T. Non-contact monitoring and classification of breathing pattern for the supervision of people infected by COVID-19. Sensors 2021, 21, 3172. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Value |
|---|---|
| Start Frequency | 77 GHZ |
| Bandwidth | 4 GHZ |
| Number of Transmitting Antennas | 1 |
| Number of Receiving Antennas | 4 |
| Samples Per-Chirp | 200 |
| Chirp Duration | 50 μs |
| Frame Duration | 50 ms |
| Number of Chirps per Frame | 2 |
| Subject Number | Sex | Height (cm) | Weight (kg) |
|---|---|---|---|
| 1 | male | 172 | 60 |
| 2 | male | 185 | 75 |
| 3 | male | 178 | 71 |
| 4 | female | 163 | 47 |
| 5 | female | 170 | 61 |
| Number | Millimeter-Wave Radar (Breaths Times) | HUAWEI WATCH GT2 (Breaths Times) |
|---|---|---|
| 1 | 10 | 9 |
| 2 | 7 | 7 |
| 3 | 8 | 8 |
| 4 | 8 | 7 |
| 5 | 7 | 8 |
| 6 | 9 | 8 |
| 7 | 10 | 9 |
| 8 | 7 | 7 |
| 9 | 11 | 10 |
| 10 | 9 | 8 |
| Average | 8.6 | 8.1 |
| Method | Accuracy |
|---|---|
| KNN | 84.75% |
| SVM | 91% |
| CNN+LSTM | 92% |
| G-SVM | 94.75% |
| Method | Denoising Technology | Features | Model | Accuracy |
|---|---|---|---|---|
| [15] | Polynomial fit | Respiratory interval | Random Forest | 87% |
| [7] | Differencing | MFCC | XGBoost | 87% |
| [38] | Singular value decomposition | Time-domain features | Random Forest | 90% |
| [16] | Not mentioned | Embedded features | CNN | 92.34% |
| This Work | Signal overlay | HOG | SVM | 94.75% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hao, Z.; Wang, Y.; Li, F.; Ding, G.; Gao, Y. mmWave-RM: A Respiration Monitoring and Pattern Classification System Based on mmWave Radar. Sensors 2024, 24, 4315. https://doi.org/10.3390/s24134315
Hao Z, Wang Y, Li F, Ding G, Gao Y. mmWave-RM: A Respiration Monitoring and Pattern Classification System Based on mmWave Radar. Sensors. 2024; 24(13):4315. https://doi.org/10.3390/s24134315
Chicago/Turabian StyleHao, Zhanjun, Yue Wang, Fenfang Li, Guozhen Ding, and Yifei Gao. 2024. "mmWave-RM: A Respiration Monitoring and Pattern Classification System Based on mmWave Radar" Sensors 24, no. 13: 4315. https://doi.org/10.3390/s24134315
APA StyleHao, Z., Wang, Y., Li, F., Ding, G., & Gao, Y. (2024). mmWave-RM: A Respiration Monitoring and Pattern Classification System Based on mmWave Radar. Sensors, 24(13), 4315. https://doi.org/10.3390/s24134315