
Characterization of Upper Extremity Kinematics Using Virtual Reality Movement Tasks and Wearable IMU Technology

 ,
, 
 , and
, and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Equipment/Software
2.2. Description of Movement Levels and Movement Tasks
2.3. Data Collection Procedure
2.4. Data Analysis
3. Results
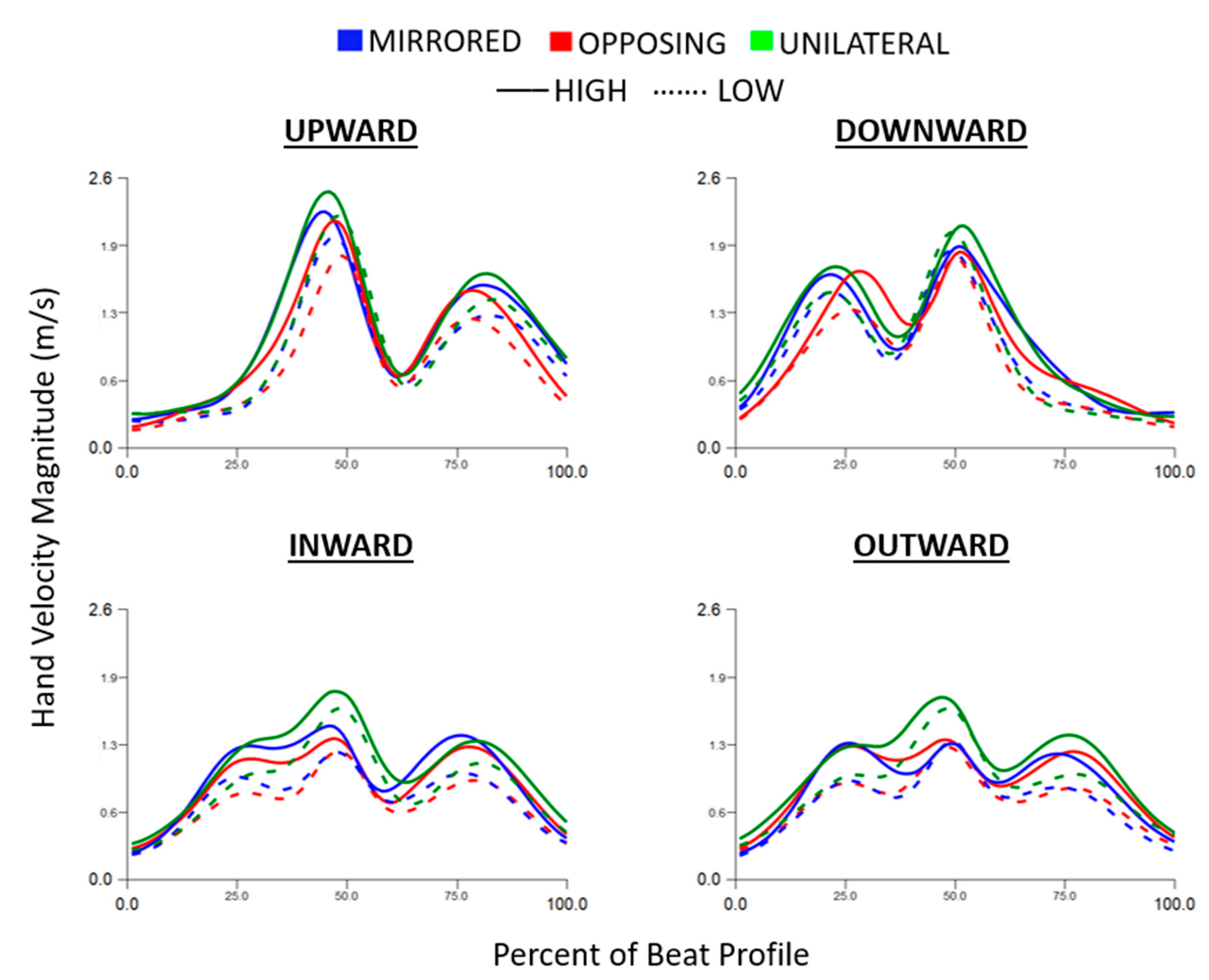
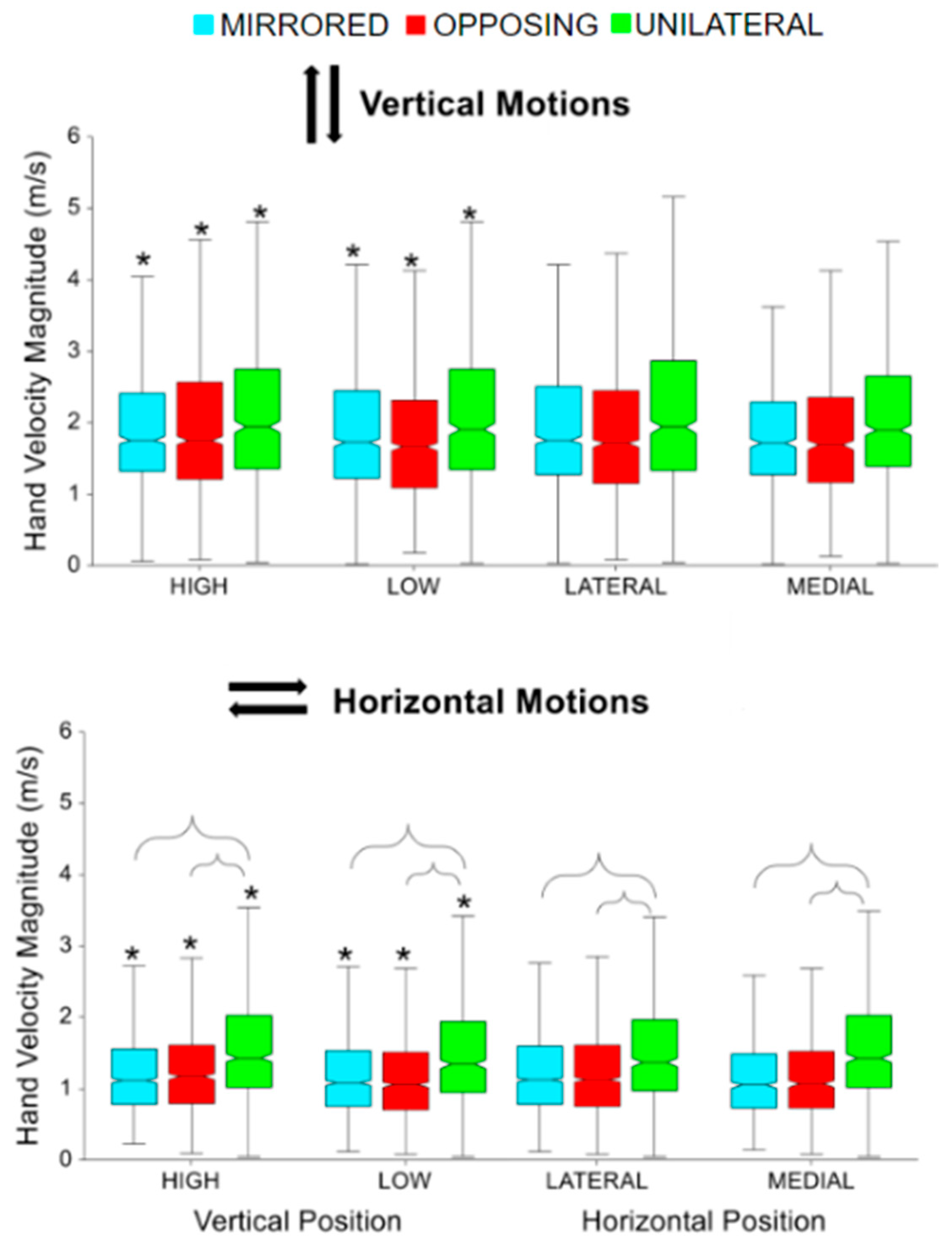
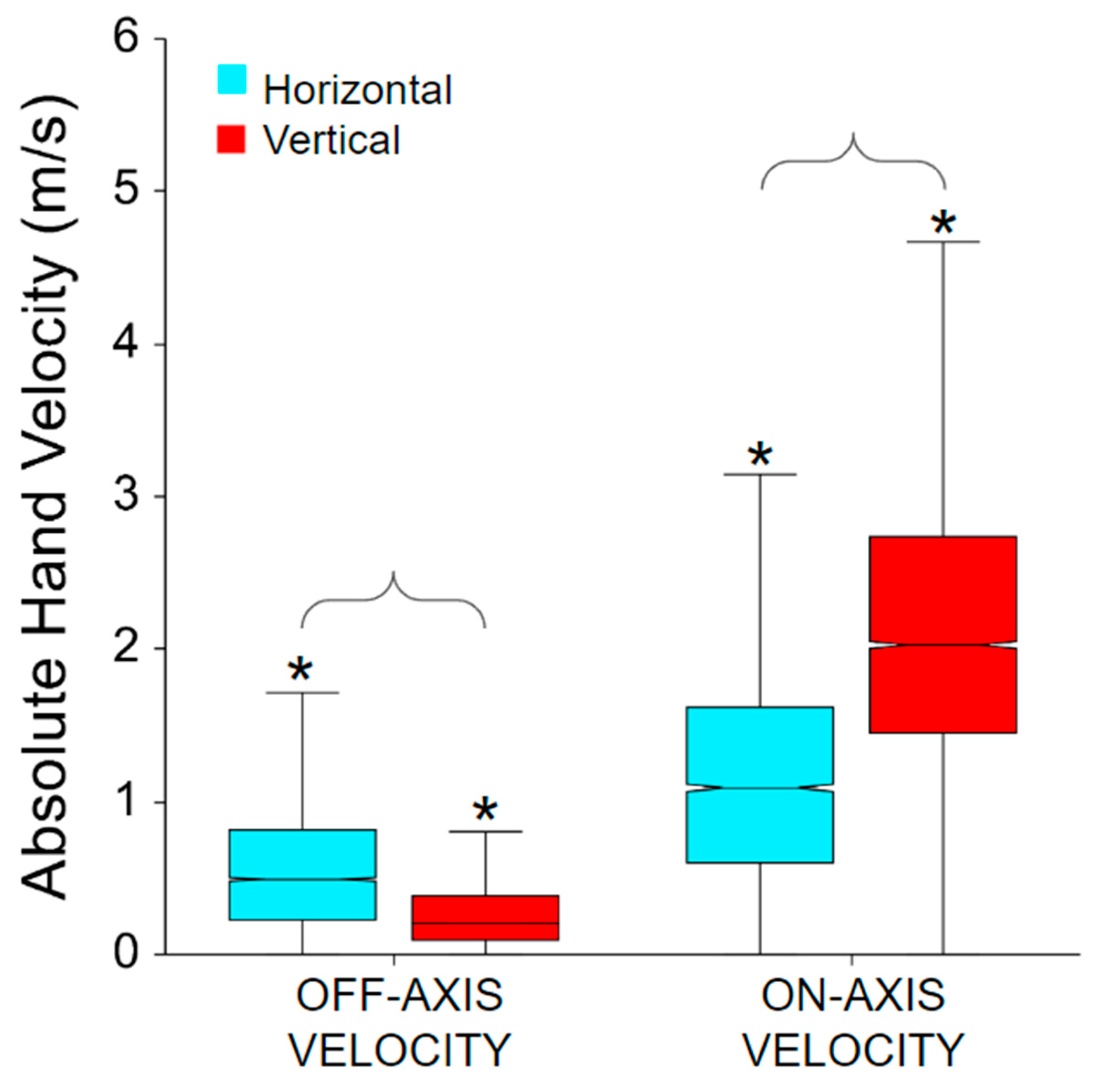
3.1. Hand Velocity
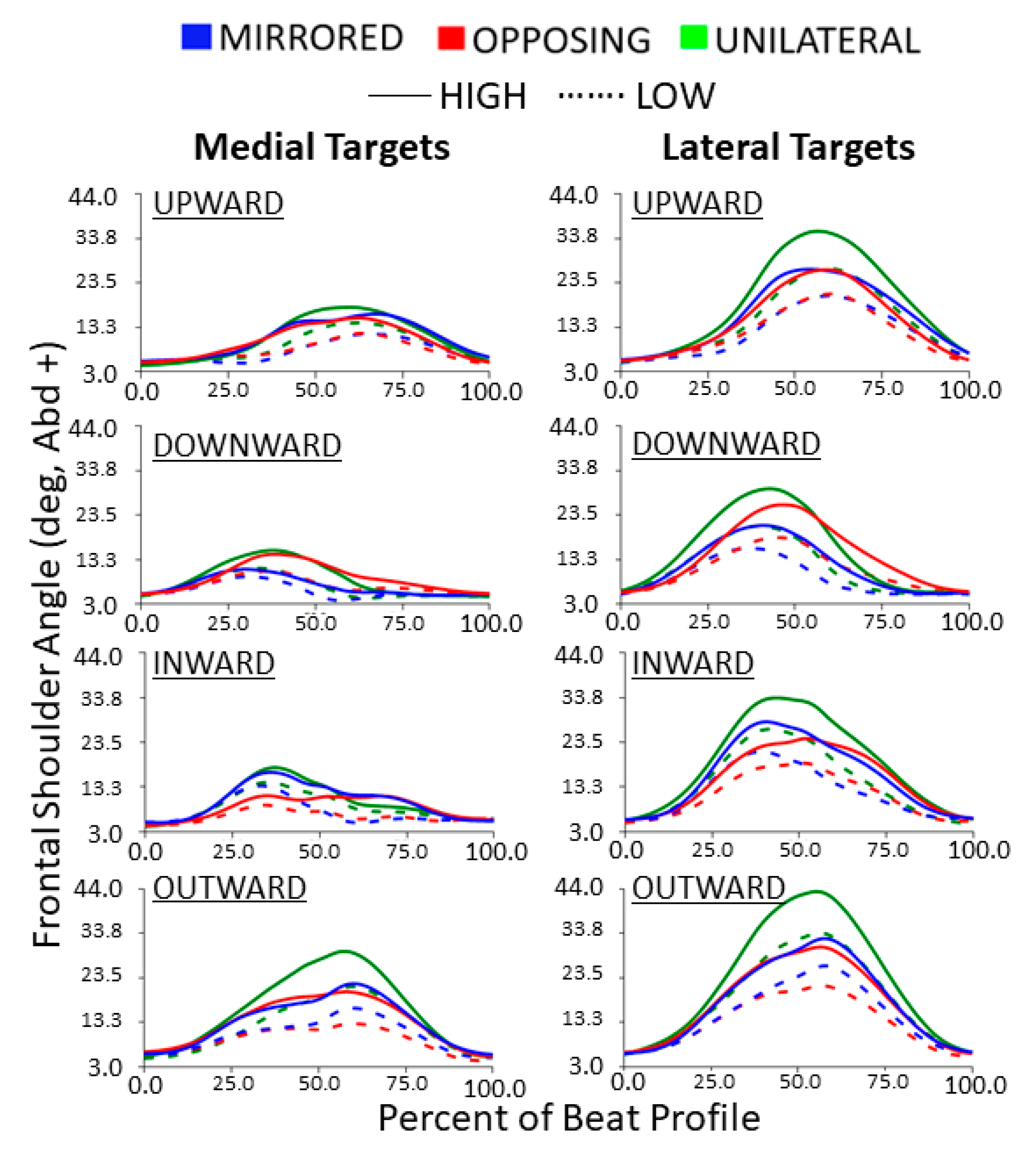
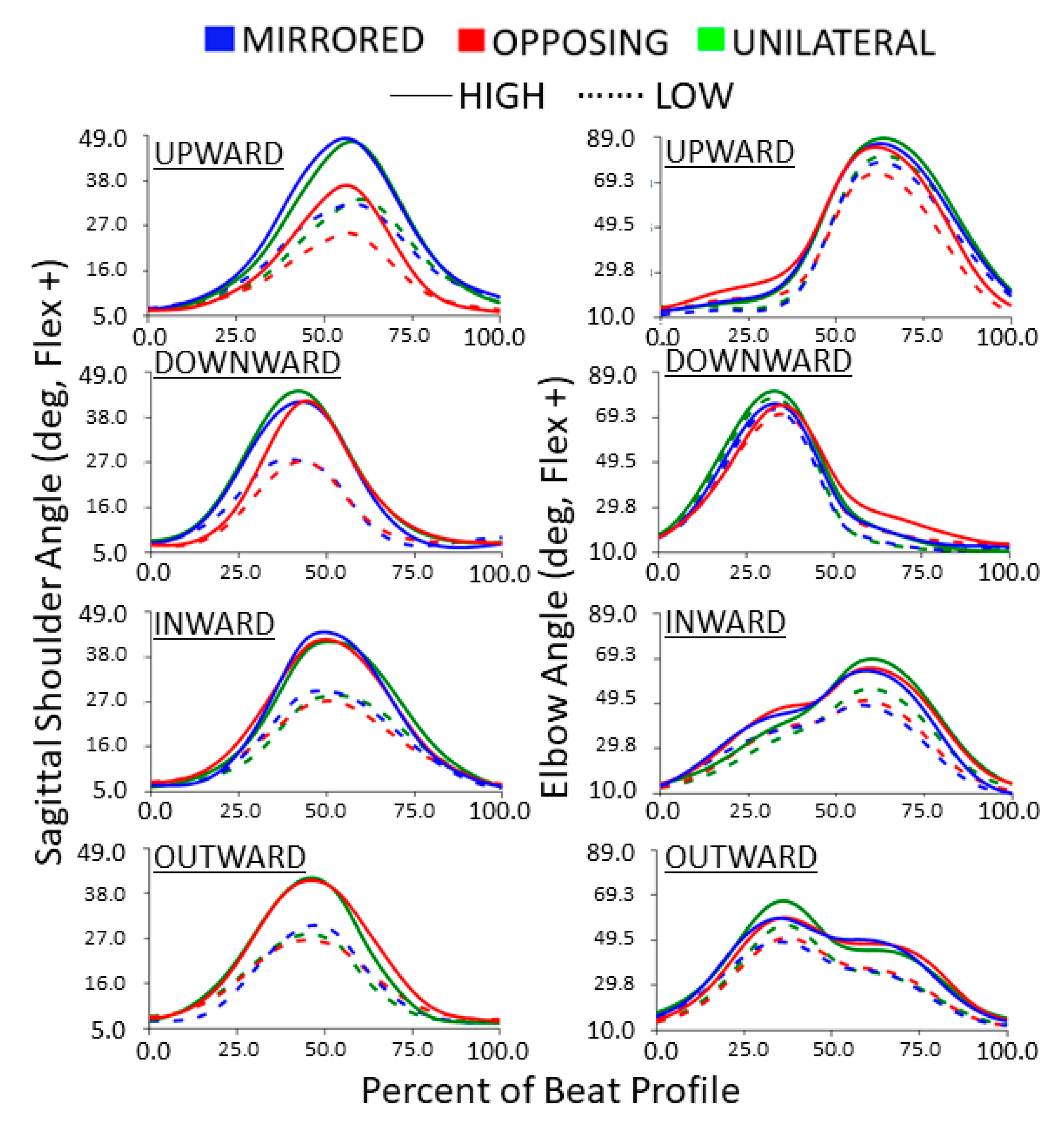
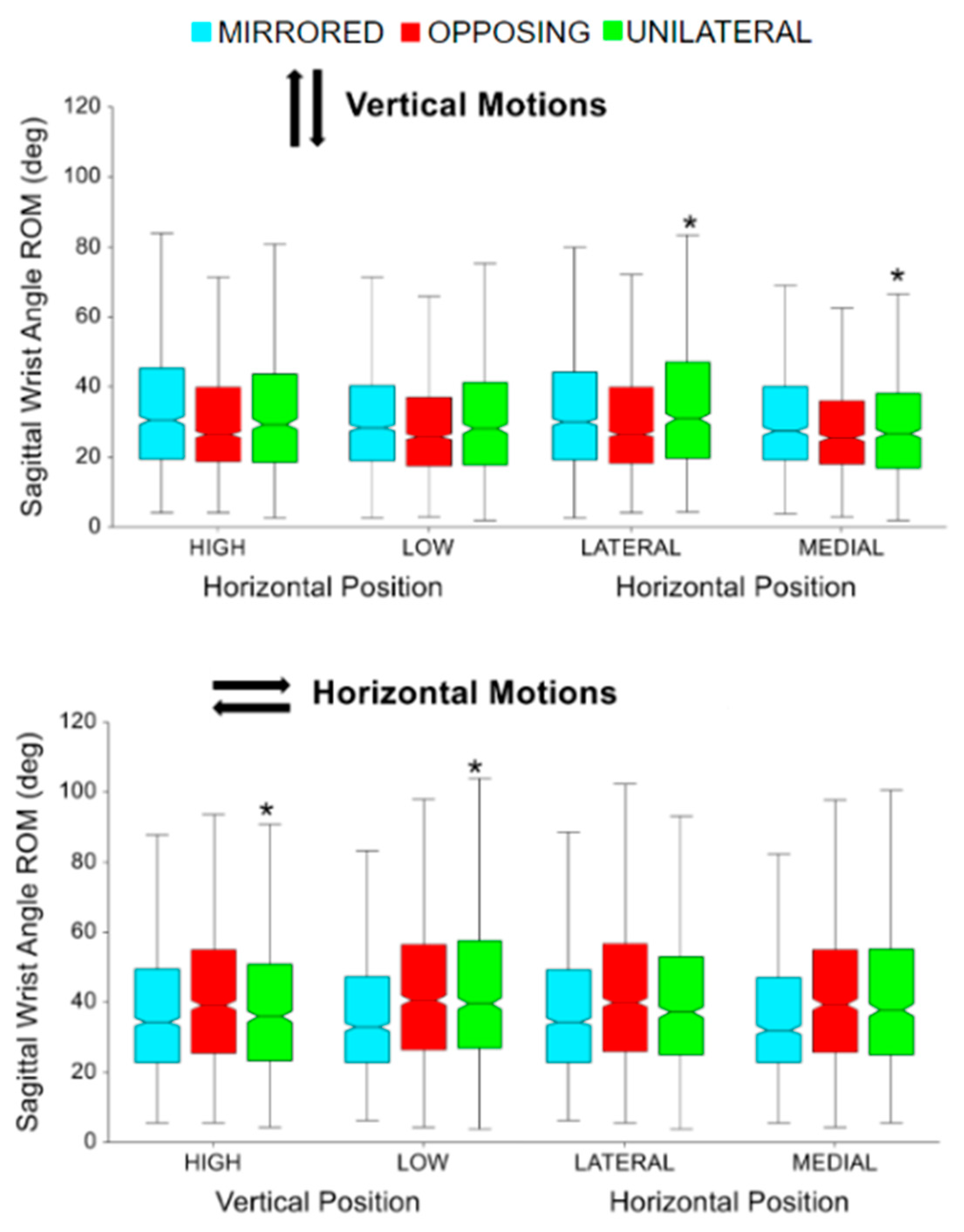
3.2. Joint Angles
4. Discussion
4.1. Task Validation
4.2. Impact of Movement Levels
4.3. Cardinal Movement Task Direction
4.4. Task Position
4.5. Collision Constraint and Controller Hand Position
4.6. Limitations and Future Work
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hubbard, I.J.; Parsons, M.W.; Neilson, C.; Carey, L.M. Task-specific training: Evidence for and translation to clinical practice. Occup. Ther. Int. 2009, 16, 175–189. [Google Scholar] [CrossRef] [PubMed]
- Bayona, N.A.; Bitensky, J.; Salter, K.; Teasell, R. The Role of Task-Specific Training in Rehabilitation Therapies. Top. Stroke Rehabil. 2005, 12, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Waddell, K.J.; Birkenmeier, R.L.; Moore, J.L.; Hornby, T.G.; Lang, C.E. Feasibility of High-Repetition, Task-Specific Training for Individuals with Upper-Extremity Paresis. Am. J. Occup. Ther. 2014, 68, 444–453. [Google Scholar] [CrossRef] [PubMed]
- Fong, K.N.K.; Tang, Y.M.; Sie, K.; Yu, A.K.H.; Lo, C.C.W.; Ma, Y.W.T. Task-specific virtual reality training on hemiparetic upper extremity in patients with stroke. Virtual Real. 2021, 26, 453–464. [Google Scholar] [CrossRef]
- Toovey, R.A.M.; Harvey, A.R.; McGinley, J.L.; Lee, K.J.; Shih, S.T.F.; Spittle, A.J. Task-specific training for bicycle-riding goals in ambulant children with cerebral palsy: A randomized controlled trial. Dev. Med. Child Neurol. 2022, 64, 243–252. [Google Scholar] [CrossRef] [PubMed]
- Dorsch, S.; Carling, C.; Cao, Z.; Fanayan, E.; Graham, P.L.; McCluskey, A.; Schurr, K.; Scrivener, K.; Tyson, S. Bobath therapy is inferior to task-specific training and not superior to other interventions in improving arm activity and arm strength outcomes after stroke: A systematic review. J. Physiother. 2023, 69, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Rozevink, S.G.; Hijmans, J.M.; Horstink, K.A.; van der Sluis, C.K. Effectiveness of task-specific training using assistive devices and task-specific usual care on upper limb performance after stroke: A systematic review and meta-analysis. Disabil. Rehabil. Assist. Technol. 2023, 18, 1245–1258. [Google Scholar] [CrossRef]
- Afsar, S.I.; Mirzayev, I.; Yemisci, O.U.; Saracgil, S.N.C. Virtual Reality in Upper Extremity Rehabilitation of Stroke Patients: A Randomized Controlled Trial. J. Stroke Cerebrovasc. Dis. 2018, 27, 3473–3478. [Google Scholar] [CrossRef]
- Ho, T.-H.; Yang, F.-C.; Lin, R.-C.; Chien, W.-C.; Chung, C.-H.; Chiang, S.-L.; Chou, C.-H.; Tsai, C.-K.; Lin, Y.-K.; Lee, J.-T. Impact of virtual reality-based rehabilitation on functional outcomes in patients with acute stroke: A retrospective case-matched study. J. Neurol. 2019, 266, 589–597. [Google Scholar] [CrossRef]
- Janeh, O.; Bruder, G.; Steinicke, F.; Gulberti, A.; Poetter-Nerger, M. Analyses of Gait Parameters of Younger and Older Adults During (Non-)Isometric Virtual Walking. IEEE Trans. Vis. Comput. Graph. 2017, 24, 2663–2674. [Google Scholar] [CrossRef]
- Kannape, O.A.; Smith, E.J.; Moseley, P.; Roy, M.P.; Lenggenhager, B. Experimentally induced limb-disownership in mixed reality. Neuropsychologia 2019, 124, 161–170. [Google Scholar] [CrossRef] [PubMed]
- Lupu, R.G.; Botezatu, N.; Ungureanu, F.; Ignat, D.; Moldoveanu, A. Virtual reality based stroke recovery for upper limbs using leap motion. In Proceedings of the 2016 20th International Conference on System Theory, Control and Computing (ICSTCC), Sinaia, Romania, 13–15 October 2016; pp. 295–299. [Google Scholar]
- Vaughan, N.; Gabrys, B. Scoring and assessment in medical VR training simulators with dynamic time series classification. Eng. Appl. Artif. Intell. 2020, 94, 103760. [Google Scholar] [CrossRef]
- Shahmoradi, L.; Almasi, S.; Ahmadi, H.; Bashiri, A.; Azadi, T.; Mirbagherie, A.; Ansari, N.N.; Honarpishe, R. Virtual reality games for rehabilitation of upper extremities in stroke patients. J. Bodyw. Mov. Ther. 2020, 26, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Jung, H.; Yun, S.J.; Oh, B.; Gil Seo, H. Upper Extremity Rehabilitation Using Fully Immersive Virtual Reality Games with a Head Mount Display: A Feasibility Study. PM&R 2020, 12, 257–262. [Google Scholar] [CrossRef]
- Ijaz, K.; Ahmadpour, N.; Wang, Y.; Calvo, R.A. Player Experience of Needs Satisfaction (PENS) in an Immersive Virtual Reality Exercise Platform Describes Motivation and Enjoyment. Int. J. Hum.–Comput. Interact. 2020, 36, 1195–1204. [Google Scholar] [CrossRef]
- Jaspers, E.; Desloovere, K.; Bruyninckx, H.; Molenaers, G.; Klingels, K.; Feys, H. Review of quantitative measurements of upper limb movements in hemiplegic cerebral palsy. Gait Posture 2009, 30, 395–404. [Google Scholar] [CrossRef] [PubMed]
- Culmer, P.R.; Levesley, M.C.; Mon-Williams, M.; Williams, J.H. A new tool for assessing human movement: The Kinematic Assessment Tool. J. Neurosci. Methods 2009, 184, 184–192. [Google Scholar] [CrossRef]
- Khurelbaatar, T.; Kim, K.; Lee, S.; Kim, Y.H. Consistent accuracy in whole-body joint kinetics during gait using wearable inertial motion sensors and in-shoe pressure sensors. Gait Posture 2015, 42, 65–69. [Google Scholar] [CrossRef]
- Cerfoglio, S.; Capodaglio, P.; Rossi, P.; Conforti, I.; D’angeli, V.; Milani, E.; Galli, M.; Cimolin, V. Evaluation of Upper Body and Lower Limbs Kinematics through an IMU-Based Medical System: A Comparative Study with the Optoelectronic System. Sensors 2023, 23, 6156. [Google Scholar] [CrossRef]
- Teufl, W.; Miezal, M.; Taetz, B.; Fröhlich, M.; Bleser, G. Validity of inertial sensor based 3D joint kinematics of static and dynamic sport and physiotherapy specific movements. PLoS ONE 2019, 14, e0213064. [Google Scholar] [CrossRef]
- Wu, Y.; Tao, K.; Chen, Q.; Tian, Y.; Sun, L. A Comprehensive Analysis of the Validity and Reliability of the Perception Neuron Studio for Upper-Body Motion Capture. Sensors 2022, 22, 6954. [Google Scholar] [CrossRef] [PubMed]
- Held, J.P.O.; Klaassen, B.; Eenhoorn, A.; van Beijnum, B.-J.F.; Buurke, J.H.; Veltink, P.H.; Luft, A.R. Inertial Sensor Measurements of Upper-Limb Kinematics in Stroke Patients in Clinic and Home Environment. Front. Bioeng. Biotechnol. 2018, 6, 27. [Google Scholar] [CrossRef] [PubMed]
- Voss, S.; Joyce, J.; Biskis, A.; Parulekar, M.; Armijo, N.; Zampieri, C.; Tracy, R.; Palmer, A.S.; Fefferman, M.; Ouyang, B.; et al. Normative database of spatiotemporal gait parameters using inertial sensors in typically developing children and young adults. Gait Posture 2020, 80, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Reyes-Guzmán, A.d.L.; Dimbwadyo-Terrer, I.; Trincado-Alonso, F.; Monasterio-Huelin, F.; Torricelli, D.; Gil-Agudo, A. Quantitative assessment based on kinematic measures of functional impairments during upper extremity movements: A review. Clin. Biomech. 2014, 29, 719–727. [Google Scholar] [CrossRef] [PubMed]
- Aizawa, J.; Masuda, T.; Koyama, T.; Nakamaru, K.; Isozaki, K.; Okawa, A.; Morita, S. Three-dimensional motion of the upper extremity joints during various activities of daily living. J. Biomech. 2010, 43, 2915–2922. [Google Scholar] [CrossRef] [PubMed]
- Murphy, M.A.; Willén, C.; Sunnerhagen, K.S. Kinematic variables quantifying upper-extremity performance after stroke during reaching and drinking from a glass. Neurorehabil. Neural Repair 2011, 25, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Renner, C.I.; Brendel, C.; Hummelsheim, H. Bilateral Arm Training vs Unilateral Arm Training for Severely Affected Patients with Stroke: Exploratory Single-Blinded Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2020, 101, 1120–1130. [Google Scholar] [CrossRef]
- Chen, P.-M.; Kwong, P.W.; Lai, C.K.; Ng, S.S.M. Comparison of bilateral and unilateral upper limb training in people with stroke: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0216357. [Google Scholar] [CrossRef]
- Summers, J.J.; Kagerer, F.A.; Garry, M.I.; Hiraga, C.Y.; Loftus, A.; Cauraugh, J.H. Bilateral and unilateral movement training on upper limb function in chronic stroke patients: A TMS study. J. Neurol. Sci. 2007, 252, 76–82. [Google Scholar] [CrossRef]
- Richardson, M.C.; Tears, C.; Morris, A.; Alexanders, J. The Effects of Unilateral Versus Bilateral Motor Training on Upper Limb Function in Adults with Chronic Stroke: A Systematic Review. J. Stroke Cerebrovasc. Dis. 2021, 30, 105617. [Google Scholar] [CrossRef]
- Hung, C.-S.; Lin, K.-C.; Chang, W.-Y.; Huang, W.-C.; Chang, Y.-J.; Chen, C.-L.; Yao, K.G.; Lee, Y.-Y. Unilateral vs Bilateral Hybrid Approaches for Upper Limb Rehabilitation in Chronic Stroke: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2019, 100, 2225–2232. [Google Scholar] [CrossRef] [PubMed]
- Bartur, G.; Pratt, H.; Frenkel-Toledo, S.; Soroker, N. Neurophysiological effects of mirror visual feedback in stroke patients with unilateral hemispheric damage. Brain Res. 2018, 1700, 170–180. [Google Scholar] [CrossRef] [PubMed]
- Riddell, M.; Kuo, H.; Zewdie, E.; Kirton, A. Mirror movements in children with unilateral cerebral palsy due to perinatal stroke: Clinical correlates of plasticity reorganization. Dev. Med. Child Neurol. 2019, 61, 943–949. [Google Scholar] [CrossRef] [PubMed]
- Tosi, G.; Romano, D.; Maravita, A. Mirror Box Training in Hemiplegic Stroke Patients Affects Body Representation. Front. Hum. Neurosci. 2018, 11, 617. [Google Scholar] [CrossRef]
- Rossiter, H.E.; Borrelli, M.R.; Borchert, R.J.; Bradbury, D.; Ward, N.S. Cortical Mechanisms of Mirror Therapy After Stroke. Neurorehabilit. Neural Repair 2015, 29, 444–452. [Google Scholar] [CrossRef]
- MVN User Manual. Movella. 2021. Available online: https://www.xsens.com/hubfs/Downloads/usermanual/MVN_User_Manual.pdf (accessed on 16 November 2023).
- Vox, J.P.; Weber, A.; Wolf, K.I.; Izdebski, K.; Schüler, T.; König, P.; Wallhoff, F.; Friemert, D. An Evaluation of Motion Trackers with Virtual Reality Sensor Technology in Comparison to a Marker-Based Motion Capture System Based on Joint Angles for Ergonomic Risk Assessment. Sensors 2021, 21, 3145. [Google Scholar] [CrossRef]
- Pataky, T.C. One-dimensional statistical parametric mapping in Python. Comput. Methods Biomech. Biomed. Eng. 2012, 15, 295–301. [Google Scholar] [CrossRef]
- Vijayan, V.; Fang, S.; Reissman, T.; Reissman, M.E.; Kinney, A.L. How Does Added Mass Affect the Gait of Middle-Aged Adults? An Assessment Using Statistical Parametric Mapping. Sensors 2022, 22, 6154. [Google Scholar] [CrossRef]
- Nüesch, C.; Roos, E.; Egloff, C.; Pagenstert, G.; Mündermann, A. The effect of different running shoes on treadmill running mechanics and muscle activity assessed using statistical parametric mapping (SPM). Gait Posture 2019, 69, 1–7. [Google Scholar] [CrossRef]
- Andersson, J.L.R.; Jenkinson, M.; Smith, S. Non-Linear Registration aka Spatial Normalisation; FMRIB Technial Report TR07JA2; FMRIB Centre: Oxford, UK, 2007. [Google Scholar]









Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barclay, S.A.; Klausing, L.N.; Hill, T.M.; Kinney, A.L.; Reissman, T.; Reissman, M.E. Characterization of Upper Extremity Kinematics Using Virtual Reality Movement Tasks and Wearable IMU Technology. Sensors 2024, 24, 233. https://doi.org/10.3390/s24010233
Barclay SA, Klausing LN, Hill TM, Kinney AL, Reissman T, Reissman ME. Characterization of Upper Extremity Kinematics Using Virtual Reality Movement Tasks and Wearable IMU Technology. Sensors. 2024; 24(1):233. https://doi.org/10.3390/s24010233
Chicago/Turabian StyleBarclay, Skyler A., Lanna N. Klausing, Tessa M. Hill, Allison L. Kinney, Timothy Reissman, and Megan E. Reissman. 2024. "Characterization of Upper Extremity Kinematics Using Virtual Reality Movement Tasks and Wearable IMU Technology" Sensors 24, no. 1: 233. https://doi.org/10.3390/s24010233
APA StyleBarclay, S. A., Klausing, L. N., Hill, T. M., Kinney, A. L., Reissman, T., & Reissman, M. E. (2024). Characterization of Upper Extremity Kinematics Using Virtual Reality Movement Tasks and Wearable IMU Technology. Sensors, 24(1), 233. https://doi.org/10.3390/s24010233