
Development Technologies for the Monitoring of Six-Minute Walk Test: A Systematic Review

 ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Methodology
2.1. Six-Minute Walk Test Protocol
2.2. Research Questions
2.3. Inclusion Criteria
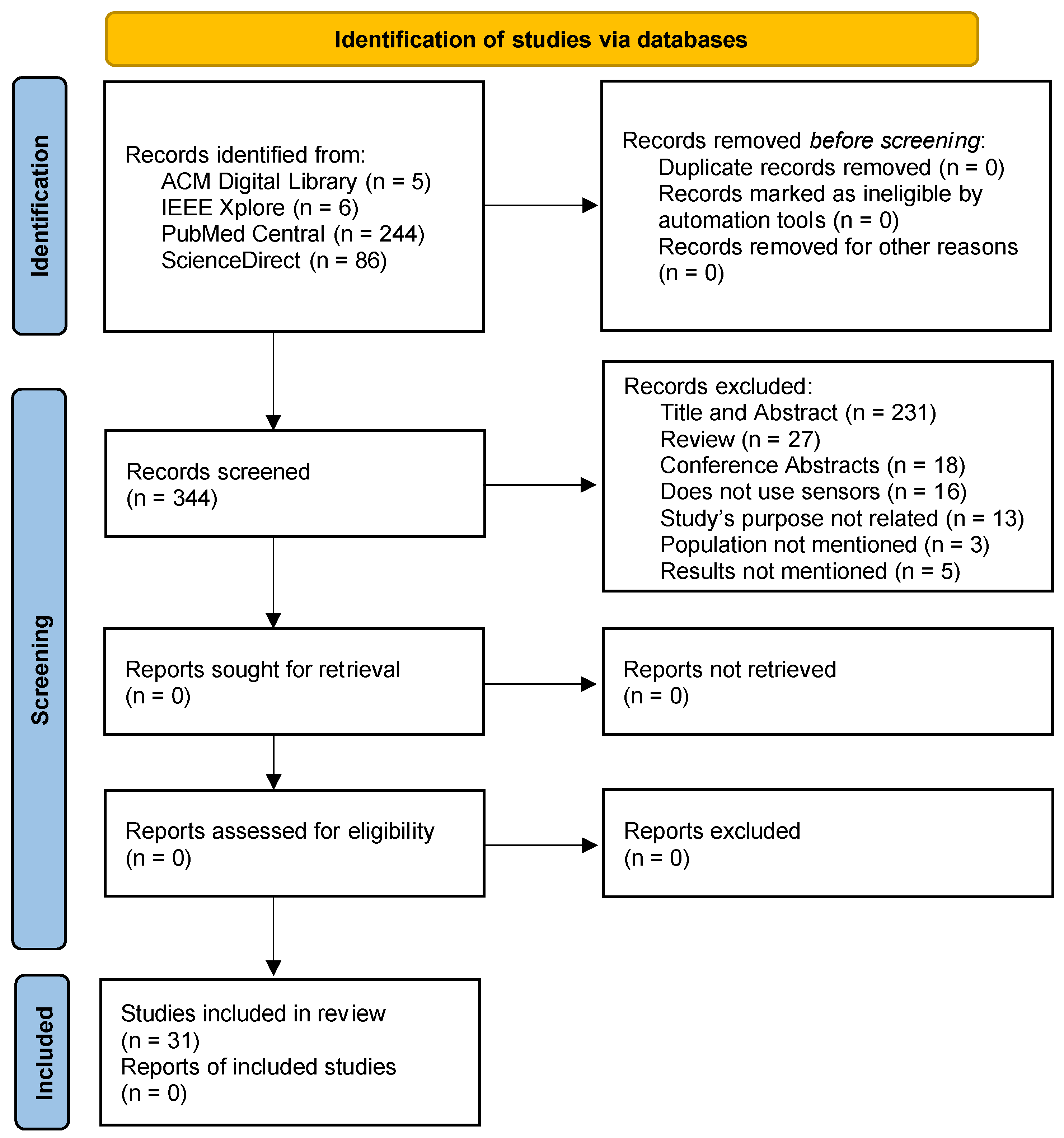
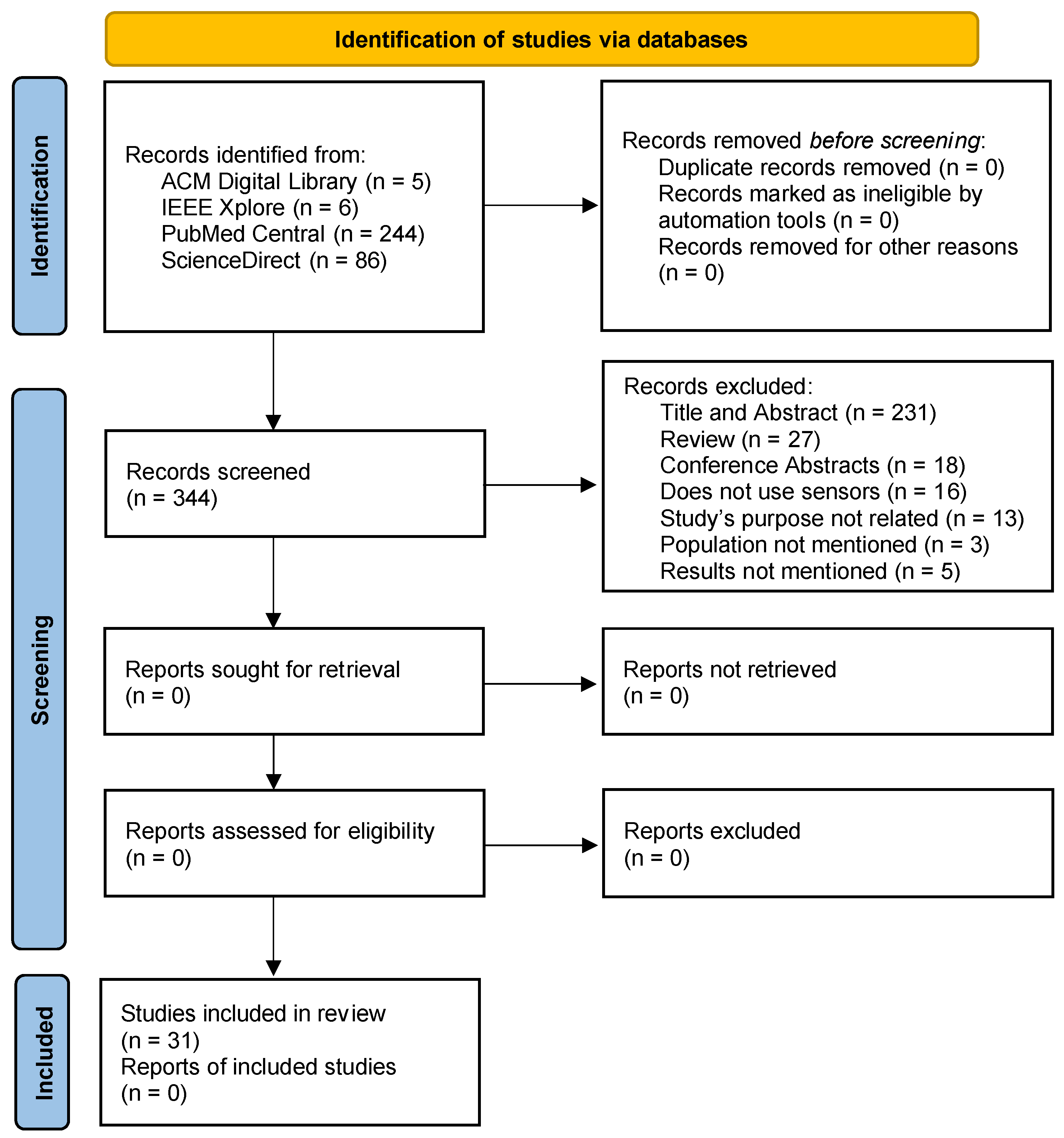
2.4. Search Strategy
2.5. Extraction of Study Characteristics
3. Results
4. Discussion
4.1. Interpretation of the Results
4.2. Validity and Reliability
4.3. Comparison of the Different Studies Analyzed
4.4. Final Remarks
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef]
- Bradley, P.S.; Mohr, M.; Bendiksen, M.; Randers, M.B.; Flindt, M.; Barnes, C.; Hood, P.; Gomez, A.; Andersen, J.L.; Di Mascio, M.; et al. Sub-maximal and maximal Yo–Yo intermittent endurance test level 2: Heart rate response, reproducibility and application to elite soccer. Eur. J. Appl. Physiol. 2011, 111, 969–978. [Google Scholar] [CrossRef]
- Daines, K.J.F.; Baddour, N.; Burger, H.; Bavec, A.; Lemaire, E.D. Fall risk classification for people with lower extremity amputations using random forests and smartphone sensor features from a 6-minute walk test. PLoS ONE 2021, 16, e0247574. [Google Scholar] [CrossRef] [PubMed]
- Drover, D.; Howcroft, J.; Kofman, J.; Lemaire, E. Faller Classification in Older Adults Using Wearable Sensors Based on Turn and Straight-Walking Accelerometer-Based Features. Sensors 2017, 17, 1321. [Google Scholar] [CrossRef]
- Kennedy, R.; Carroll, K.; Paterson, K.L.; Ryan, M.M.; McGinley, J.L. Deterioration in gait and functional ambulation in children and adolescents with Charcot–Marie–Tooth disease over 12 months. Neuromuscul. Disord. 2017, 27, 658–666. [Google Scholar] [CrossRef]
- Thygesen, K.; Mair, J.; Giannitsis, E.; Mueller, C.; Lindahl, B.; Blankenberg, S.; Huber, K.; Plebani, M.; Biasucci, L.M.; Tubaro, M.; et al. How to use high-sensitivity cardiac troponins in acute cardiac care. Eur. Heart J. 2012, 33, 2252–2257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kimberlin, C.L.; Winterstein, A.G. Validity and reliability of measurement instruments used in research. Am. J. Health Syst. Pharm. 2008, 65, 2276–2284. [Google Scholar] [CrossRef]
- Cousins, S.O.B. Exercise, Aging and Health: Overcoming Barriers to an Active Old Age; Taylor & Francis: London, UK, 2014; ISBN 978-1-317-76346-8. [Google Scholar]
- Granger, C.L.; McDonald, C.F.; Parry, S.M.; Oliveira, C.C.; Denehy, L. Functional capacity, physical activity and muscle strength assessment of individuals with non-small cell lung cancer: A systematic review of instruments and their measurement properties. BMC Cancer 2013, 13, 135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kennedy-Malone, L. Central and Peripheral Nervous System Disorders. Adv. Pract. Nurs. Care Older Adults 2018, 328. [Google Scholar]
- Volkers, K.M.; Scherder, E.J. The effect of regular walks on various health aspects in older people with dementia: Protocol of a randomized-controlled trial. BMC Geriatr. 2011, 11, 38. [Google Scholar] [CrossRef] [Green Version]
- Qureshi, A.; Brandt-Pearce, M.; Goldman, M.D. Relationship between gait variables and domains of neurologic dysfunction in multiple sclerosis using six-minute walk test. In Proceedings of the 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 4959–4962. [Google Scholar]
- Storm, F.A.; Cesareo, A.; Reni, G.; Biffi, E. Wearable Inertial Sensors to Assess Gait during the 6-Minute Walk Test: A Systematic Review. Sensors 2020, 20, 2660. [Google Scholar] [CrossRef]
- PRISMA-P Group; Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Zdravevski, E.; Lameski, P.; Trajkovik, V.; Chorbev, I.; Goleva, R.; Pombo, N.; Garcia, N.M. Automation in Systematic, Scoping and Rapid Reviews by an NLP Toolkit: A Case Study in Enhanced Living Environments. In Enhanced Living Environments; Ganchev, I., Garcia, N.M., Dobre, C., Mavromoustakis, C.X., Goleva, R., Eds.; Lecture Notes in Computer Science; Springer International Publishing: Cham, Switzerland, 2019; Volume 11369, pp. 1–18. ISBN 978-3-030-10751-2. [Google Scholar]
- Cochen de Cock, V.; Dotov, D.; Damm, L.; Lacombe, S.; Ihalainen, P.; Picot, M.C.; Galtier, F.; Lebrun, C.; Giordano, A.; Driss, V.; et al. BeatWalk: Personalized Music-Based Gait Rehabilitation in Parkinson’s Disease. Front. Psychol. 2021, 12, 655121. [Google Scholar] [CrossRef] [PubMed]
- Hadouiri, N.; Monnet, E.; Gouelle, A.; Decavel, P.; Sagawa, Y. Evaluation of Prolonged Walking in Persons with Multiple Sclerosis: Reliability of the Spatio-Temporal Walking Variables during the 6-Minute Walk Test. Sensors 2021, 21, 3075. [Google Scholar] [CrossRef] [PubMed]
- Marin, L.; Vandoni, M.; Zaza, G.; Febbi, M.; Pedrotti, L.; Chiodaroli, M.; Lovecchio, N.; Manzoni, F. The Effects of Insole-Based Visual Feedback on Weight-Bearing in Patients Undergoing Total Hip Replacement. Int. J. Environ. Res. Public Health 2021, 18, 3346. [Google Scholar] [CrossRef]
- Sagawa, Y.; Watelain, E.; Moulin, T.; Decavel, P. Physical Activity during Weekdays and Weekends in Persons with Multiple Sclerosis. Sensors 2021, 21, 3617. [Google Scholar] [CrossRef]
- Salvi, D.; Poffley, E.; Tarassenko, L.; Orchard, E. App-Based Versus Standard Six-Minute Walk Test in Pulmonary Hypertension: Mixed Methods Study. JMIR mHealth uHealth 2021, 9, e22748. [Google Scholar] [CrossRef]
- Tan, A.Q.; Sohn, W.J.; Naidu, A.; Trumbower, R.D. Daily acute intermittent hypoxia combined with walking practice enhances walking performance but not intralimb motor coordination in persons with chronic incomplete spinal cord injury. Exp. Neurol. 2021, 340, 113669. [Google Scholar] [CrossRef]
- Caronni, A.; Gervasoni, E.; Ferrarin, M.; Anastasi, D.; Brichetto, G.; Confalonieri, P.; Di Giovanni, R.; Prosperini, L.; Tacchino, A.; Solaro, C.; et al. Local Dynamic Stability of Gait in People with Early Multiple Sclerosis and No-to-Mild Neurological Impairment. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 1389–1396. [Google Scholar] [CrossRef]
- Gulart, A.A.; Munari, A.B.; Klein, S.R.; Venâncio, R.S.; Alexandre, H.F.; Mayer, A.F. The London Chest Activity of Daily Living scale cut-off point to discriminate functional status in patients with chronic obstructive pulmonary disease. Braz. J. Phys. Ther. 2020, 24, 264–272. [Google Scholar] [CrossRef]
- Paradiso, C.; Colino, F.; Liu, S. The Validity and Reliability of the Mi Band Wearable Device for Measuring Steps and Heart Rate. Int. J. Exerc. Sci. 2020, 13, 689–701. [Google Scholar]
- Plotnik, M.; Wagner, J.M.; Adusumilli, G.; Gottlieb, A.; Naismith, R.T. Gait asymmetry, and bilateral coordination of gait during a six-minute walk test in persons with multiple sclerosis. Sci. Rep. 2020, 10, 12382. [Google Scholar] [CrossRef] [PubMed]
- Schubert, C.; Archer, G.; Zelis, J.M.; Nordmeyer, S.; Runte, K.; Hennemuth, A.; Berger, F.; Falk, V.; Tonino, P.A.L.; Hose, R.; et al. Wearable devices can predict the outcome of standardized 6-minute walk tests in heart disease. NPJ Digit. Med. 2020, 3, 92. [Google Scholar] [CrossRef]
- Yeo, S.S.; Kwon, J.W.; Cho, I.H. Associations between Age-Related Changes in the Core Vestibular Projection Pathway and Balance Ability: A Diffusion Tensor Imaging Study. Behav. Neurol. 2020, 2020, 2825108. [Google Scholar] [CrossRef] [Green Version]
- Zeitlberger, A.M.; Sosnova, M.; Ziga, M.; Steinsiepe, V.; Gautschi, O.P.; Stienen, M.N.; Maldaner, N. Smartphone-Based Self-Assessment of Objective Functional Impairment (6-Minute Walking Test) in Patients Undergoing Epidural Steroid Injection. Neurospine 2020, 17, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Beausoleil, S.; Miramand, L.; Turcot, K. Evolution of gait parameters in individuals with a lower-limb amputation during a six-minute walk test. Gait Posture 2019, 72, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Bertuletti, S.; Salis, F.; Cereatti, A.; Angelini, L.; Buckley, E.; Nair, K.P.S.; Mazza, C.; Croce, U.D. Inter-leg Distance Measurement as a Tool for Accurate Step Counting in Patients with Multiple Sclerosis. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 6413–6417. [Google Scholar]
- Camp, P.G.; Sima, C.A.; Kirkham, A.; Inskip, J.A.; Parappilly, B. The de Morton mobility index is a feasible and valid mobility assessment tool in hospitalized patients with an acute exacerbation of chronic obstructive pulmonary disease. Chron. Respir. Dis. 2019, 16, 147997311987297. [Google Scholar] [CrossRef] [Green Version]
- Moumdjian, L.; Moens, B.; Maes, P.-J.; van Geel, F.; Ilsbroukx, S.; Borgers, S.; Leman, M.; Feys, P. Continuous 12 min walking to music, metronomes and in silence: Auditory-motor coupling and its effects on perceived fatigue, motivation and gait in persons with multiple sclerosis. Mult. Scler. Relat. Disord. 2019, 35, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Taborri, J.; Studer, V.; Grossi, P.; Brambilla, L.; Ferro, M.T.; Mantegazza, R.; Rossi, S. Measuring changes in gait kinematics due to walking-related fatigue in patients with Multiple Sclerosis. In Proceedings of the 2019 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Istanbul, Turkey, 26–28 June 2019; pp. 1–6. [Google Scholar]
- Tousignant, M.; Mampuya, W.M.; Bissonnette, J.; Guillemette, E.; Lauriault, F.; Lavoie, J.; St-Laurent, M.-E.; Pagé, C. Telerehabilitation with live-feed biomedical sensor signals for patients with heart failure: A pilot study. Cardiovasc. Diagn. Ther. 2019, 9, 319–327. [Google Scholar] [CrossRef]
- Acuña, S.A.; Tyler, M.E.; Danilov, Y.P.; Thelen, D.G. Abnormal muscle activation patterns are associated with chronic gait deficits following traumatic brain injury. Gait Posture 2018, 62, 510–517. [Google Scholar] [CrossRef]
- Byrnes, S.K.; Nüesch, C.; Loske, S.; Leuenberger, A.; Schären, S.; Netzer, C.; Mündermann, A. Inertial Sensor-Based Gait and Attractor Analysis as Clinical Measurement Tool: Functionality and Sensitivity in Healthy Subjects and Patients with Symptomatic Lumbar Spinal Stenosis. Front. Physiol. 2018, 9, 1095. [Google Scholar] [CrossRef] [Green Version]
- D’Alessandro, C.; Piccoli, G.; Barsotti, M.; Tassi, S.; Giannese, D.; Morganti, R.; Cupisti, A. Prevalence and Correlates of Sarcopenia among Elderly CKD Outpatients on Tertiary Care. Nutrients 2018, 10, 1951. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hadouiri, N.; Feuvrier, D.; Pauchot, J.; Decavel, P.; Sagawa, Y. Donor site morbidity after vascularized fibula free flap: Gait analysis during prolonged walk conditions. Int. J. Oral Maxillofac. Surg. 2018, 47, 309–315. [Google Scholar] [CrossRef] [PubMed]
- El Hosainy, A.; Kaddah, S.; Saied, M.; Ibrahim, A.; Darwish, R. Preliminary study of the anabolic/catabolic balance in patients with interstitial pulmonary fibrosis. Egypt. J. Chest Dis. Tuberc. 2017, 66, 497–503. [Google Scholar] [CrossRef]
- Moon, Y.; McGinnis, R.S.; Seagers, K.; Motl, R.W.; Sheth, N.; Wright, J.A.; Ghaffari, R.; Sosnoff, J.J. Monitoring gait in multiple sclerosis with novel wearable motion sensors. PLoS ONE 2017, 12, e0171346. [Google Scholar] [CrossRef]
- Toosizadeh, N.; Berry, C.; Bime, C.; Najafi, B.; Kraft, M.; Mohler, J. Assessing upper-extremity motion: An innovative method to quantify functional capacity in patients with chronic obstructive pulmonary disease. PLoS ONE 2017, 12, e0172766. [Google Scholar] [CrossRef] [Green Version]
- Cheng, Q.; Juen, J.; Bellam, S.; Fulara, N.; Close, D.; Silverstein, J.C.; Schatz, B. Classification Models for Pulmonary Function using Motion Analysis from Phone Sensors. AMIA Annu. Symp. Proc. AMIA Symp. 2016, 2016, 401–410. [Google Scholar]
- Cheng, Q.; Shang, J.; Juen, J.; Han, J.; Schatz, B. Mining Discriminative Patterns to Predict Health Status for Cardiopulmonary Patients. In Proceedings of the 7th ACM International Conference on Bioinformatics, Computational Biology, and Health Informatics, Seattle, WA, USA, 2–5 October 2016; pp. 41–49. [Google Scholar]
- Kalron, A. Construct validity of the walk ratio as a measure of gait control in people with multiple sclerosis without mobility aids. Gait Posture 2016, 47, 103–107. [Google Scholar] [CrossRef]
- Resnik, L.; Borgia, M. Reliability of outcome measures for people with lower-limb amputations: Distinguishing true change from statistical error. Phys. Ther. 2011, 91, 555–565. [Google Scholar] [CrossRef]
- Pera, M.C.; Luigetti, M.; Pane, M.; Coratti, G.; Forcina, N.; Fanelli, L.; Mazzone, E.S.; Antonaci, L.; Lapenta, L.; Palermo, C. 6MWT can identify type 3 SMA patients with neuromuscular junction dysfunction. Neuromuscul. Disord. 2017, 27, 879–882. [Google Scholar] [CrossRef]
- Zdravevski, E.; Lameski, P.; Kulakov, A.; Kalajdziski, S. Transformation of nominal features into numeric in supervised multi-class problems based on the weight of evidence parameter. In Proceedings of the 2015 Federated Conference on Computer Science and Information Systems (FedCSIS), Lodz, Poland, 13–16 September 2015; pp. 169–179. [Google Scholar]
- Zdravevski, E.; Lameski, P.; Apanowicz, C.; Ślȩzak, D. From Big Data to business analytics: The case study of churn prediction. Appl. Soft Comput. 2020, 90, 106164. [Google Scholar] [CrossRef]
- Grzegorowski, M.; Zdravevski, E.; Janusz, A.; Lameski, P.; Apanowicz, C.; Ślęzak, D. Cost Optimization for Big Data Workloads Based on Dynamic Scheduling and Cluster-Size Tuning. Big Data Res. 2021, 25, 100203. [Google Scholar] [CrossRef]
- Zdravevski, E.; Lameski, P.; Kulakov, A.; Filiposka, S.; Trajanov, D.; Jakimovski, B. Parallel computation of information gain using Hadoop and MapReduce. In Proceedings of the 2015 Federated Conference on Computer Science and Information Systems (FedCSIS), Lodz, Poland, 13–16 September 2015; pp. 181–192. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Paper | Year | Location | Population | Purpose of Study | Sensors Used | Include Medical Collaboration | Type of Methods | Diseases |
|---|---|---|---|---|---|---|---|---|
| De Cock et al. [16] | 2021 | Montpellier (France) | 45 Parkinson’s disease patients | Investigating the observance, safety, tolerance, usability, and enjoyment of a smartphone application | Ankle-worn, accelerometer, gyroscope, and magnetometer sensors | Yes | Statistical | Parkinson’s disease |
| Hadouiri et al. [17] | 2021 | Besançon (France) | 45 multiple sclerosis patients and 24 healthy subjects | Measuring the performance of the inverted pendulum algorithm, and an adaptation correcting for lateral step movement | GAITRite walkway system composed of accelerometer, gyroscope, and magnetometer sensors | Yes | Statistical | multiple sclerosis |
| Marin et al. [18] | 2021 | Pavia (Italy) | 19 Total Hip Replacement and 21 healthy patients | Investigating the visual biofeedback effect of a sensorized system for plantar pressure dynamic evaluation | sensorized insoles composed of accelerometer, gyroscope, and magnetometer sensors | Yes | Statistical | Total Hip Replacement |
| Sagawa et al. [19] | 2021 | Besançon (France) | 41 multiple sclerosis patients and 16 healthy subjects | Measuring the level of activity during weekdays and weekends, and its correlation with clinical parameters | accelerometer | Yes | Statistical | multiple sclerosis |
| Salvi et al. [20] | 2021 | Oxford (United Kingdom) | 33 pulmonary hypertension patients | Assessing the accuracy of the indoor clinical settings, validity, and test-retest reliability of outdoor performance in the community, compliance, usability, and acceptance of the mobile application, and feasibility of pulse oximetry | accelerometer, gyroscope, magnetometer, Global Positioning System (GPS), and Bluetooth pulse oximeter | Yes | Statistical | pulmonary hypertension |
| Tan et al. [21] | 2021 | Atlanta (United States of America) | 11 spinal cord injuries patients | Analyzing the daily acute intermittent hypoxia combined with walking practice | optical motion capture system composed by accelerometer, gyroscope, and magnetometer | Yes | Statistical | spinal cord injuries |
| Carommi et al. [22] | 2020 | Milan (Italy), Moncrivello—Vercelli (Italy), and Genova (Italy) | 80 multiple sclerosis patients with no clinal evidence | Researching the presence of poor Local Dynamic Stability of gait | accelerometer, gyroscope, and magnetometer | Yes | Statistical | multiple sclerosis |
| Gulart et al. [23] | 2020 | Santa Catarina (Brazil) | 61 chronic obstructive pulmonary disease patients | Determining the cut-off point for the London Chest Activity of Daily Living scale and the scores associated with clinical outcomes of a pulmonary rehabilitation program | Accelerometer | Yes | Statistical | chronic obstructive pulmonary disease |
| Paradiso et al. [24] | 2020 | Victoria (Canada) | 14 individuals | Evaluating the measurement of steps and the assessment of the validity and reliability of the monitor to measure heart rate during rest and exercise | Mi Band device composed by accelerometer and heart rate sensors | No | Statistical | N/D |
| Plotnik et al. [25] | 2020 | Washington (United States of America) | 92 multiple sclerosis patients | Assessing gait asymmetry and bilateral coordination of gait (BCG), and their association with disease severity | Opal motion sensor-based gait analysis system composed by accelerometer, gyroscope, and magnetometer | Yes | Statistical | multiple sclerosis |
| Schubert et al. [26] | 2020 | Berlin (Germany) and Sheffield (United Kingdom) | 107 heart disease patients | Measuring the distances in patients with different stages of mitral and aortic valve disease | accelerometer, gyroscope, magnetometer, and heart rate sensors | Yes | Statistical | heart disease |
| Yeo et al. [27] | 2020 | Daegu (Korea) | 11 older adults and 12 young people | Investigating the changes of the vestibulospinal tract, and parietoinsular vestibular cortex | Diffusion Tensor Imaging | Yes | Statistical | N/D |
| Zeitlberger et al. [28] | 2020 | St. Gallen (Switzerland) | 3 lumbar degenerative disc disease patients | Assessment of the discrimination between Epidural steroid injection responders and non-responders | Global Positioning System (GPS) | Yes | Statistical | lumbar degenerative disc disease |
| Beausoleil et al. [29] | 2019 | Quebec (Canada) | 15 lower-limb amputation patients | Quantification of the evolution of gait parameters | accelerometer, gyroscope, magnetometer, and heart rate sensors | Yes | Statistical | lower-limb amputation |
| Bertuletti et al. [30] | 2019 | Sheffield (United Kingdom) | 13 multiple sclerosis patients | Testing and validation of a step counter method based on the direct measurement of inter-leg distance | SWING wearable multi-sensor system composed of accelerometer, gyroscope, magnetometer, and time-of-flight distance sensors | No | Statistical | multiple sclerosis |
| Camp et al. [31] | 2019 | Vancouver (Canada) | 22 acute exacerbation of chronic obstructive pulmonary disease patients | Assessing convergent, discriminant, and known-group validity and floor/ceiling effects of the de Morton Mobility Index | accelerometer | Yes | Statistical | chronic obstructive pulmonary disease |
| Moumdjian et al. [32] | 2019 | Hasselt (Belgium) | 31 multiple sclerosis patients and 30 healthy subjects | Investigating the effects on perceived physical and cognitive fatigue, motivation, and gait | OPAL wearable sensors are composed of an accelerometer, gyroscope, and magnetometer | Yes | Statistical | multiple sclerosis |
| Taborri et al. [33] | 2019 | Crema (Italy) | 9 multiple sclerosis patients and 26 healthy subjects | Measuring changes in gait kinematics due to fatigue | wireless inertial sensors MIMUs composed by accelerometer, gyroscope, and magnetometer | Yes | Statistical | multiple sclerosis |
| Tousignant et al. [34] | 2019 | Quebec (Canada) | 4 heart failure patients | Measuring the feasibility and usefulness of biomedical sensors in telerehabilitation | Electrocardiography (ECG) signal, oxygen saturation, and heart rate | Yes | Statistical | heart disease |
| Acuña et al. [35] | 2018 | Wisconsin–Madison (United States of America) | 44 traumatic brain injury patients | Assessment of the relationship between lower limb muscle activation patterns and chronic gait deficits | Accelerometer and Electromyography (EMG) sensors | Yes | Statistical | traumatic brain injury |
| Byrnes et al. [36] | 2018 | Basel (Switzerland) | 24 healthy individuals and 19 Symptomatic Lumbar Spinal Stenosis patients | Assessing the effects of the attractor for acceleration gait data, the exercise-induced changes in the attractor in patients with symptomatic lumbar spinal stenosis, and the exercise-induced changes in the attractor after surgical treatment. | accelerometer, gyroscope, and magnetometer | Yes | Statistical | Symptomatic Lumbar Spinal Stenosis |
| D’Alessando et al. [37] | 2018 | Le Mans (France) | 40 chronic kidney disease patients | Assessment of the prevalence and correlation of sarcopenia | accelerometer, gyroscope, and magnetometer sensors | Yes | Statistical | chronic kidney disease |
| Hadouiri et al. [38] | 2018 | Besançon (France) | 11 vascularized fibula free flap patients and 30 healthy subjects | Determination of the effect of vascularized fibula free flap harvesting on temporal-spatial gait variables | GAITRite walkway system composed of accelerometer, gyroscope, and magnetometer sensors | Yes | Statistical | vascularized fibula free flap |
| El Hosainy et al. [39] | 2017 | Cairo (Egypt) | 22 healthy individuals and two groups of 22 interstitial pulmonary fibrosis patients | Assessment of the metabolic disturbance and its reflection on the muscular state | spirometry | Yes | Statistical | interstitial pulmonary fibrosis |
| Kennedy et al. [5] | 2017 | Parkville (Australia) | 27 children | Investigating the change in spatiotemporal gait parameters and functional ambulation | GAITRite walkway system composed of accelerometer, gyroscope, and magnetometer sensors | No | Statistical | N/D |
| Moon et al. [40] | 2017 | Illinois (United States of America) | 45 multiple sclerosis patients and 15 healthy subjects | Examining gait characteristics under controlled conditions remotely | accelerometer, gyroscope, and magnetometer sensors | No | Statistical | multiple sclerosis |
| Toosizadeh et al. [41] | 2017 | Tucson (United States of America) | 49 chronic obstructive pulmonary disease patients | Evaluating an upper-extremity function test to assess functional capacity | accelerometer, gyroscope, and magnetometer sensors | Yes | Statistical | chronic obstructive pulmonary disease |
| Cheng et al. [42] | 2016 | Illinois (United States of America) | 24 pulmonary disease patients | Measuring pulmonary functions | accelerometer | Yes | Machine Learning | pulmonary disease |
| Cheng et al. [43] | 2016 | Illinois (United States of America) | 55 pulmonary patients and 11 healthy subjects | Tracking cardiopulmonary conditions | accelerometer | Yes | Machine Learning | pulmonary disease |
| Kalron [44] | 2016 | Tel Hashomer (Israel) | 229 multiple sclerosis patients | Measuring the relationship between the walk ratio and other theoretically related constructs | GAITRite walkway system composed of accelerometer, gyroscope, and magnetometer sensors | Yes | Statistical | multiple sclerosis |
| Qureshi et al. [12] | 2016 | Virginia (United States of America) | 28 multiple sclerosis patients | Inferring changes in gait speed and gait cycle length variance over six minutes, and the relationships between these variables and other assessments, including functional systems scores, modified fatigue impact scale, and multiple sclerosis walking scale | BSN platform composed by accelerometer, gyroscope, and magnetometer | No | Statistical | multiple sclerosis |
| Study | Sensors | Diseases | ||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ankle-Worn | Accelerometer | Gyroscope | Magnetometer | GPS | Bluetooth Pulse Oximeter | Heart rate | Diffusion Tensor Imaging | Time-of-Flight Distance | ECG | Oxygen Saturation | EMG | Spirometry | Parkinson | Multiple Sclerosis | Total Hip Replacement | Pulmonary Diseases | Spinal Cord Injuries | Chronic Obstructive Pulmonary | Lumbar Degenerative disc | Lower-limb Amputation | Traumatic Brain Injury | Symptomatic Lumbar Spinal Stenosis | Chronic Kidney Disease | Vascularized Fibula Free Flap | Charcot–Marie–Tooth | Heart Disease | N/D | |
| De Cock et al. [16] | x | x | x | x | x | |||||||||||||||||||||||
| Hadouiri et al. [17] | x | x | x | x | ||||||||||||||||||||||||
| Marin et al. [18] | x | x | x | x | ||||||||||||||||||||||||
| Sagawa et al. [19] | x | x | ||||||||||||||||||||||||||
| Salvi et al. [20] | x | x | x | x | x | x | ||||||||||||||||||||||
| Tan et al. [21] | x | x | x | x | ||||||||||||||||||||||||
| Carommi et al. [22] | x | x | x | x | ||||||||||||||||||||||||
| Gulart et al. [23] | x | x | ||||||||||||||||||||||||||
| Paradiso et al. [24] | x | x | x | |||||||||||||||||||||||||
| Plotnik et al. [25] | x | x | x | x | ||||||||||||||||||||||||
| Schubert et al. [26] | x | x | x | x | x | |||||||||||||||||||||||
| Yeo et al. [27] | x | x | ||||||||||||||||||||||||||
| Zeitlberger et al. [28] | x | x | ||||||||||||||||||||||||||
| Beausoleil et al. [29] | x | x | x | x | x | |||||||||||||||||||||||
| Bertuletti et al. [30] | x | x | x | x | x | |||||||||||||||||||||||
| Camp et al. [31] | x | x | ||||||||||||||||||||||||||
| Moumdjian et al. [32] | x | x | x | x | ||||||||||||||||||||||||
| Taborri et al. [33] | x | x | x | x | ||||||||||||||||||||||||
| Tousignant et al. [34] | x | x | x | x | ||||||||||||||||||||||||
| Acuña et al. [35] | x | x | x | |||||||||||||||||||||||||
| Byrnes et al. [36] | x | x | x | x | ||||||||||||||||||||||||
| D’Alessando et al. [37] | x | x | x | x | ||||||||||||||||||||||||
| Hadouiri et al. [38] | x | x | x | |||||||||||||||||||||||||
| El Hosainy et al. [39] | x | x | ||||||||||||||||||||||||||
| Kennedy et al. [5] | x | x | x | x | ||||||||||||||||||||||||
| Moon et al. [40] | x | x | x | x | ||||||||||||||||||||||||
| Toosizadeh et al. [41] | x | x | x | x | ||||||||||||||||||||||||
| Cheng et al. [42] | x | x | ||||||||||||||||||||||||||
| Cheng et al. [43] | x | x | ||||||||||||||||||||||||||
| Kalron [44] | x | x | x | x | ||||||||||||||||||||||||
| Qureshi et al. [12] | x | x | x | x | ||||||||||||||||||||||||
| Study | Results and Benefits | Limitations |
|---|---|---|
| De Cock et al. [16] | Results demonstrated that musical application (BeatWalk) for individualized gait rehabilitation in Parkinson’s is a safe, user-friendly, and enjoyable solution displaying good observance. The rehabilitation program using BeatWalk motivated patients to go outside, walk alone, and enjoy physical activity for almost eight and a half hours. | N/D |
| Hadouiri et al. [17] | The results demonstrate that Spatio-temporal (ST) variables analyzed during specific 6MWT intervals are reliable for assessing the physical management in multiple sclerosis. This process could be used in clinical practice or medical treatments during the intervals of a 6MWT. | The measurement of ST variables during the 6MWT was not continuous and depended on the length of the GAITRite instrumented walkway. Therefore, only ST variables were used to assess walking in this study, and only two tests were performed. |
| Marin et al. [18] | The results demonstrated improved weight-bearing distribution for the experimental group compared to the control group. This process may facilitate the performance of the rehabilitation activities magnifying the peripherical nervous system caption. | N/D |
| Sagawa et al. [19] | The results showed that, during the week, multiple sclerosis (PwMS) performed less activity than their healthy peers. In addition, multiple Sclerosis had a stable level of activity throughout the week, contrary to healthy persons whose average and peak values increased on Saturdays. | The first limitation concerns the wear time of accelerometers by PwMS. PwMS wore accelerometers on average one hour less than their healthy peers during weekdays. Second, the seven-day evaluation was a good compromise between the representativeness and feasibility of accelerometer measures. Third, it is essential to note that the analysis was done from a physical point of view and does not consider the physiological demands of groups. Finally, these results correspond to those obtained in a relatively small French population. |
| Salvi et al. [20] | The results demonstrated that app-based outdoor 6MWTs in community settings are valid, repeatable, and well accepted by patients. Its use should be made explicit to patients to increase their engagement, and it could complement or potentially substitute conventional 6MWTs in clinics. | This pilot study involved 30 patients and was not aimed at obtaining statistical significance. However, it is also important to observe that the manual data quality assurance strategy was inconsistent. As a result, an underestimated number of outdoor tests performed in the wrong conditions were included in the statistics. |
| Tan et al. [21] | The results indicated that five consecutive days of acute intermittent hypoxia (AIH) + WALK improved walking performance in persons with chronic, incomplete spinal cord injuries (SCI). The most significant change in performance occurred in persons who walk overground using bilateral arm-driven walking aids. | Many study limitations were due to the inherent heterogeneity of spinal cord injury in humans and the small sample size that precluded the generalization of the current findings. In addition, it focused on intralimb assessments of only the more impaired lower-limb and did not assess the less impaired lower-limb or interlimb coordination. Confounding factors likely contribute to the variability in responsiveness to AIH. Factors such as pre-existing medical conditions and delivery methods may influence the dose and timing of AIH. |
| Carommi et al. [22] | Results demonstrated that maximum gait speed is slightly lower in non-disabled people with multiple sclerosis (PWMS) than controls and that this finding is associated with poorer stability of gait, as indicated by a more significant local dynamic stability (LDS, e.g., short-term Lyapunov’s exponents, sLyEs) of gait. Furthermore, the correlation between vertical, mediolateral, and anteroposterior acceleration (sLyEAP) and the clinical measures of gait, balance, and fatigue suggests that sLyEAP could represent a measure of the stability of gait in PWMS valid from a clinical point of view. | sLyEVT and sLyEML (local dynamic stability was quantified by computing the short-term Lyapunov exponent (sLyE) from the trunk (i.e., lower back) anteroposterior (AP), mediolateral (ML), and vertical (VT) accelerations) are different in patients and controls. Still, neither is associated with any clinical measure of balance, gait, or impact of the disease. Moreover, lower trunk acceleration along the mediolateral axis is often proposed as a marker of gait impairment, and it might thus surprise that sLyEML does not correlate with clinical measures. However, sLyEs of acceleration provides different information (focused on local dynamic stability and amplitude) than the acceleration itself. |
| Gulart et al. [23] | Results demonstrated that the cut-off point of 28% was sensitive and specific to discriminate the functional status of patients with chronic obstructive pulmonary disease (COPD). Therefore, the %total score of the London Chest Activity of Daily Living (LCADL) reflects better outcomes of chronic obstructive pulmonary disease when compared to the total score. | One limitation is the lack of significance in the receiver operating characteristic curve analysis using the 6MWT as the anchor. In addition, some analyses have presented low statistical power, especially for the subgroups, since a sample estimation was not conducted for this purpose. |
| Paradiso et al. [24] | Results demonstrated that the Mi Band 2 is a suitable tool to measure steps at a moderate pace in healthy adults. However, the Mi Band device underestimates steps at lower speeds and heart rate during exercise. | First, the sample size of this study is restricted to healthy adults; thus, this limited the generalizability of their findings. Second, it assessed the Mi Band device under rest and exercise conditions in controlled laboratory settings. Still, it did not measure the device’s accuracy and reliability in free-living conditions. Last, the measured reliability between devices worn on the left and right wrists, but it did not measure reliability over time. |
| Plotnik et al. [25] | Results show that gait is more asymmetric and less coordinated as the disease progresses. Participants with mild multiple sclerosis (MS) showed significantly better bilateral coordination of gait (BCG) as reflected by lower e phase coordination index (PCI) values in comparison to the other two MS severity groups. BCG shows weaker clinical MS status associations than those observed between functional and subjective gait assessments and MS status. Like different neurological cohorts, BCG could be necessary to assess and target interventions among pwMS. | While providing data from a relatively large cohort of pwMS, the small number of participants in the severe group should be acknowledged as it limits the external validity of the findings. Additionally, gait asymmetry (GA) and BCG are worse in pwMS who have more disability and disease progression than those with mild to moderate disability. |
| Schubert et al. [26] | Results indicate that solely determining overall physical activity is not sufficient to predict exercise capacity. Only with quantification of the specific time spent in moderate activity, six-minute walk test outcomes were effectively predicted. | In this study, to determine resting heart rate, activity sensors data of the device were used. The paroxysmal occurrence of tachycardic atrial fibrillation, widespread in the older population, could potentially influence the heart rate-based analysis of activity. In addition, the influence of age, medication, and physical fitness on the resting heart rate could be a limitation for categorizing activity based on heart rate data. |
| Yeo et al. [27] | Results obtained indicate changes in diffusion tensor imaging (DTI) parameters in the vestibular neural pathway and are associated with age-related reductions in balance ability. The study provides primary data that could be used to plan exercise programs designed to mitigate fall risk. | The first limitation of this study is that the small number of subjects recruited limits the generalizability of its findings. Second, it was challenging to locate regions of interest precisely because of the diminutive sizes of vestibular nuclei. Third, it was not considered neuroplasticity because the subjects of this study were healthy adults. |
| Zeitlberger et al. [28] | Results of three cases of this study demonstrated that the 6WT is a helpful tool to assess outcome and monitor a patient’s functional walking capacity before and after lumbar epidural steroid injection (ESI). It further demonstrates that self-measurements of the 6WT are feasible in clinical practice and are well-accepted by patients. | The main limitation of this study is that the case series had a small sample size, which prevents meaningful statistical analysis. Therefore, further investigations to assess the validity and sensitivity of the 6MWT and the 6MWT’s ability to detect changes in the functional capacity of patients undergoing spine surgery or ESI are warranted inadequately powered studies. |
| Beausoleil et al. [29] | Results indicated that minimum toe clearance (MinTC) and stance phase variability along the 6MWT were significantly different. In addition, cadence variability and speed variation were significantly different between both feet (amputated and non-amputated leg). The increased variability in gait parameters along the 6MWT suggests a greater risk of future mobility problems following a return in the community. The data provided by the inertial sensors (IMUs) reflect the potential of the clinical rehabilitation program and could, therefore, help clinicians refine their interventions. | The small number of participants and the heterogeneity of the sample relating to age, sex, level, cause of amputation, and the number of days spent in a rehabilitation program limit the possibility of generalizing those outcomes. |
| Bertuletti et al. [30] | Results showed good accuracy in detecting steps with half the errors in detecting the step of the instrumented side compared to the non-instrumented. This test is the suggested configuration for patients walking with a large base of support | N/D |
| Camp et al. [31] | This study showed moderate to strong validity with measures of physical function, specifically 6MWD and gait velocity. In this study of chronic obstructive pulmonary disease patients, the Morton Mobility Index (DEMMI) was found to have good convergent, discriminant, and known-group validity related to measures of observed physical function and is an appropriate measure of mobility for physiotherapists’ and other healthcare professionals use in the acute care setting. | This study was conducted with younger patients (mean age 60 years) than typical AECOPD populations. Although the mean DEMMI score was like other reports, this younger group may be more mobile than older patients, and a sampling bias may be present. In addition, some patients who met the initial criteria of the study were discharged before day 3, also indicating a less severe AECOPD cohort. The sample size was calculated based on the validity analysis, which required a sample of 19 individuals for adequate power. However, the possibility of a DEMMI ceiling effect in this group could not be confirmed or denied in this study. |
| Moumdjian et al. [32] | Results demonstrated that all participants synchronized to both stimuli, yet multiple sclerosis (PwMS) synchronized better to music. Overall, participants had lower cadence, speed, and stride length overall conditions, except for HC, with increasing cadence during the music condition. In addition, PwMS perceived less cognitive fatigue, no difference in perceived physical fatigue, and a higher motivation walking to music than metronomes and silence. | One of the methodological limitations was that the walking track was 4.5 by 6 m square, and it is considered a limitation to this study as it induced many turns. |
| Taborri et al. [33] | This paper proposed synthetic indices to objectively measure the effects of prolonged walking on gait kinematics when multiple sclerosis patients performed prolonged walking. Proposed indices reveal themselves as reliable and repeatable both intra-day and inter-day. This fundamental metrological aspect allows assessing the evolution of a range of motion, gait variability, and gait asymmetry during a 6MWT as useful indices for monitoring gait deterioration. | N/D |
| Tousignant et al. [34] | Results demonstrated that most participants tended to improve their physical capacities such as walking distance and lower limb muscular strength. In addition, the use of sensors allowed a safe environment for the patient and an adequate and personalized exercise prescription. | The small number of participants is a weakness and a reality in pilot studies: no generalization is allowed. |
| Acuña et al. [35] | Results demonstrated considerable heterogeneity in performance on clinical balance and gait assessments. Abnormal muscle activation patterns were significantly correlated with variations in the dynamic gait index among the traumatic brain injury (TBI) subjects. Individuals who have experienced a prior TBI exhibit characteristic changes in the temporal coordination of select lower extremity muscles, which may contribute to impairments during challenging walking tasks. | The first limitation of this study is that the healthy controls were not matched for age, height, or weight. It could not be excluded that these differences may account for some of the observed differences between the TBI and healthy control subjects. Second, here was used the ensemble average muscle activation obtained over multiple strides, rather than individual stride data. Lastly, this study analyzed the activation of each muscle independently. |
| Byrnes et al. [36] | Results showed that the attractor for acceleration gait data varies largely among healthy subjects, and hence a reference attractor cannot be defined. Moreover, the change in the attractor and its variability during the 6MWT differed between patients and elderly healthy persons but not between repeated assessments. Attractor based on low-pass filtered signals could reflect pathology-specific differences in gait characteristics but does not appear to be sufficiently sensitive to serve as outcome parameter of decompression surgery in patients with symptomatic lumbar spinal stenosis. | A lack of statistically significant differences in exercise-induced changes in acceleration patterns and variability over time may be attributed to the heterogeneity of our patient population. |
| D’Alessando et al. [37] | Results demonstrated that older seniors showed lower serum albumin, hand-grip strength, body mass index (BMI), skeletal muscle mass, and resting energy expenditure. Protein intake was significantly lower in older seniors, whereas energy intake was similar. Average daily physical activity was lower in the older seniors than in the younger ones. Sarcopenia was more prevalent in older than in younger seniors. Among older seniors, sarcopenic and non-sarcopenic ones differed in age and performance on the six-minute walk test. In contrast, the estimated glomerular filtration rate (eGFR), biochemistry, dietary protein, and energy intakes were similar. | This study has several limitations: it is based upon a convenience sample of relatively limited size and involves only males. Another limit is choosing a creatinine-based formula (CKD-EPI) for estimated glomerular filtration rate calculation. The use of cystatin C-based eGFR might be preferable in this setting, avoiding an overestimation of eGFR in sarcopenic subjects. |
| Hadouiri et al. [38] | Results showed that after vascularized fibula free flap (VFFF) harvesting, patients have an altered walking capacity during prolonged walking conditions, which could be associated in part with the VFFF harvesting. The VFFF group in this study walked a reduced distance in the 6MWT, had an increased toe in/out angle on the operated side, and demonstrated altered physical exercise management during this lengthy walk task. | The main limitation is that the functional alterations observed in the VFFF group may have resulted from the VFFF. In addition, eight of the 11 patients in this study came from a typical population of smokers (including four with a drinker profile) who presented with maxillofacial or oral cancer. Another limitation concerns the small size of the study population. |
| El Hosainy et al. [39] | This study found a marked increase in serum lactate dehydrogenase levels associated with a significant decrease in serum creatine phosphokinase levels in idiopathic pulmonary fibrosis (IPF) patients compared to the control subjects that may reveal the presence of adaptive mechanisms in those patients to prevent muscle pain and fatigue. Additionally, a marked decrease in the mean of the serum IGF-1 levels in the newly diagnosed IPF patients compared to the control group, while the mean of the serum IGF-1 Levels in the previously diagnosed IPF patients was non-significant when compared to the other two groups. It may suggest a functional improvement with the start of steroid treatment. | N/D |
| Kennedy et al. [5] | Results indicated that children with Charcot–Marie–Tooth (CMT) were less active than typically developing (TD) controls. The children with CMT had a moderate disability and reduced ambulatory capacity in a six-minute walk test. Physical activity correlated with more significant disability and normalized six-minute walk distance-related disability affects physical activity and gait-related function in children and adolescents with CMT compared to TD peers. In addition, reduced physical activity adversely affects function across the timespan of childhood and adolescence into adulthood in people with CMT. | The limitations of this study included the relatively small participant numbers, broad age range, and mix of CMT subtypes which may have increased the variability of the results. Given the small sample numbers, it could not demonstrate differences in gait speed between CMT subtypes. Further, while lower limb surgery and injury over the 12-month interval were accounted for, physical activity levels and the occurrence of physiotherapy were not documented and may have influenced change over time. Low physical activity and exercise levels may contribute to gait and physical function deterioration and should be addressed in future studies. |
| Moon et al. [40] | Results demonstrated that BioStampRC sensors accurately and precisely measure gait parameters in multiple sclerosis (PwMS) across diverse walking impairment levels and detected differences in gait characteristics by disability level in PwMS. This technology can provide granular monitoring of gait both inside and outside the clinic. | A primary limitation is that 6MW trials were conducted on a motorized treadmill. It is established that treadmill walking is distinct from overground walking. The treadmill was utilized to maintain gait speed within a given trial. Additionally, while the inertial sensors provide tri-axial angular velocity and acceleration data, the study only utilized angular velocity data to analyze temporal gait parameters. Further, the different devices used were not attached to the body’s exact location. While this helped minimize interference between devices, there might be some errors due to the other attachment locations. |
| Toosizadeh et al. [41] | Results show promise of a quick upper-extremity measure of functional capacity in patients with chronic obstructive pulmonary disease (COPD, and as an outcome measure in clinical COPD trials. Speed, power, and moment upper-extremity function parameters were independently associated with 6MWD when controlling for age, gender, and body mass index. In addition, elbow moment showed significant Pearson correlations with all pulmonary function measures and maximal inspiratory/expiratory pressure measures. | As with measurement limitations for gait-based measures, upper-extremity disability or injury may limit upper-extremity function (UEF) measurement. Further, due to the small sample size, current results should be considered preliminary and need further validation among larger samples. Additionally, a small percentage of participants were at the severe COPD stage, and therefore, the current sample may not adequately represent those with functional/gait impairments. Also, the study lacks intra- and inter-rater reliability assessments. Lastly, although a strong correlation was observed between UEF and 6MWD tests, the association between UEF outcomes and long-term prospective clinical measures, including the risk of exacerbations, hospitalization, and mortality, should be assessed. |
| Cheng et al. [42] | Results showed that every patient now has correct modeling of GOLD level, even sample by sample (10 s), not only walk test by walk test (6 min). Measuring motion is a potential solution for passive monitoring, distinguishing this work from the phone applications measuring pulmonary functions with the microphone. A passive monitor has compliance advantages over active phone applications. The patient simply uses their phone as usual during daily activities. No particular actions or special experts are necessary. | N/D |
| Cheng et al. [43] | Results demonstrated that a universal model, trained with about sixty patients 6MWT data, has perfect accuracy at detecting all statuses from GOLD 0 to GOLD 3. In addition, it gives a way to interpret better how the predictive model works and how the input features, containing demographics and gait features, interact with each other. | N/D |
| Kalron [44] | Results demonstrated that the walk ratio discriminates between multiple sclerosis (MS) fallers and non-fallers and between different neurological disability levels. In addition, the consistency of the walk ratio results between the instrumental and manual measurements is encouraging due to the measurement’s clinical feasibility and applicability that can be provided either with or without instrumental gait measurement devices. | Walk ratio was not sensitive to asymmetries between left and proper steps. The impact of gait asymmetry on the walk ratio measure is unclear in the neurological population. The study did not provide data on the walk ratio application in MS using a walking assistive device. All outcome scores were based on a single measurement session, preventing from concluding the reproducibility of the walk ratio measure over time. |
| Qureshi et al. [12] | Results illustrated that the variables from a severely impacted gait stand out as a subject completes the test. Minute-based extension of the feature space is promising for personalized signal processing by letting physicians observe changes in gait parameters over time instead of actual values to remove inter-patient variability. | N/D |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pires, I.M.; Denysyuk, H.V.; Villasana, M.V.; Sá, J.; Marques, D.L.; Morgado, J.F.; Albuquerque, C.; Zdravevski, E. Development Technologies for the Monitoring of Six-Minute Walk Test: A Systematic Review. Sensors 2022, 22, 581. https://doi.org/10.3390/s22020581
Pires IM, Denysyuk HV, Villasana MV, Sá J, Marques DL, Morgado JF, Albuquerque C, Zdravevski E. Development Technologies for the Monitoring of Six-Minute Walk Test: A Systematic Review. Sensors. 2022; 22(2):581. https://doi.org/10.3390/s22020581
Chicago/Turabian StylePires, Ivan Miguel, Hanna Vitaliyivna Denysyuk, María Vanessa Villasana, Juliana Sá, Diogo Luís Marques, José Francisco Morgado, Carlos Albuquerque, and Eftim Zdravevski. 2022. "Development Technologies for the Monitoring of Six-Minute Walk Test: A Systematic Review" Sensors 22, no. 2: 581. https://doi.org/10.3390/s22020581
APA StylePires, I. M., Denysyuk, H. V., Villasana, M. V., Sá, J., Marques, D. L., Morgado, J. F., Albuquerque, C., & Zdravevski, E. (2022). Development Technologies for the Monitoring of Six-Minute Walk Test: A Systematic Review. Sensors, 22(2), 581. https://doi.org/10.3390/s22020581