
Soft Transducer for Patient’s Vitals Telemonitoring with Deep Learning-Based Personalized Anomaly Detection

 ,
, 
 , ,
, ,  and
and
Abstract
:1. Introduction
2. Related Work
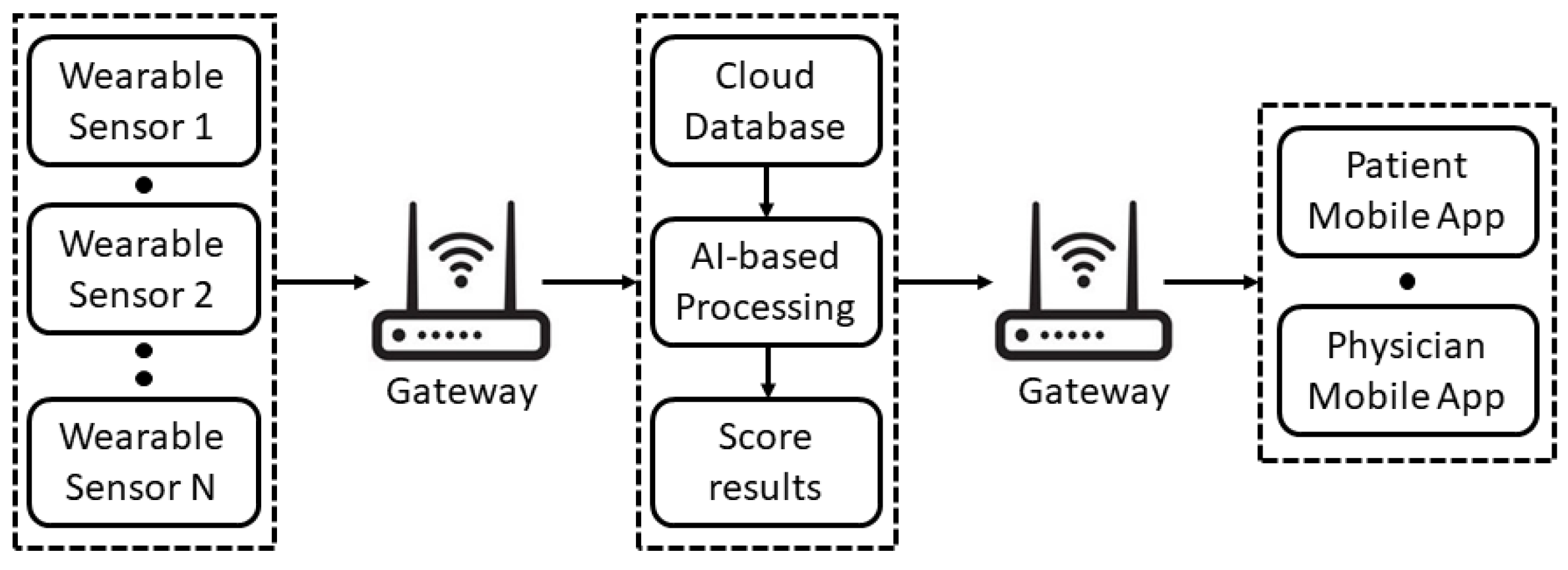
3. Design and Overall Architecture
- The patient uses wearable sensors to measure the vitals.
- The measured data are sent to a cloud database and are made available through a mobile application for the patient and the remote physician.
- The data on the cloud are processed by means of a DL algorithm, which is trained on the basis of preliminary measurements of the patient vitals.
- If the patient’s vitals exceed a certain threshold, an alert is sent to the physician and to the patient.
- Patient registration;
- Vitals measurements;
- Management of the patient’s Medical History;
- Remote Vitals visualization;
- AI processing;
- Delivery of the Score results to the patient and the physician.
4. Implementation
4.1. Wearable Sensing Platform
4.2. Mobile Application
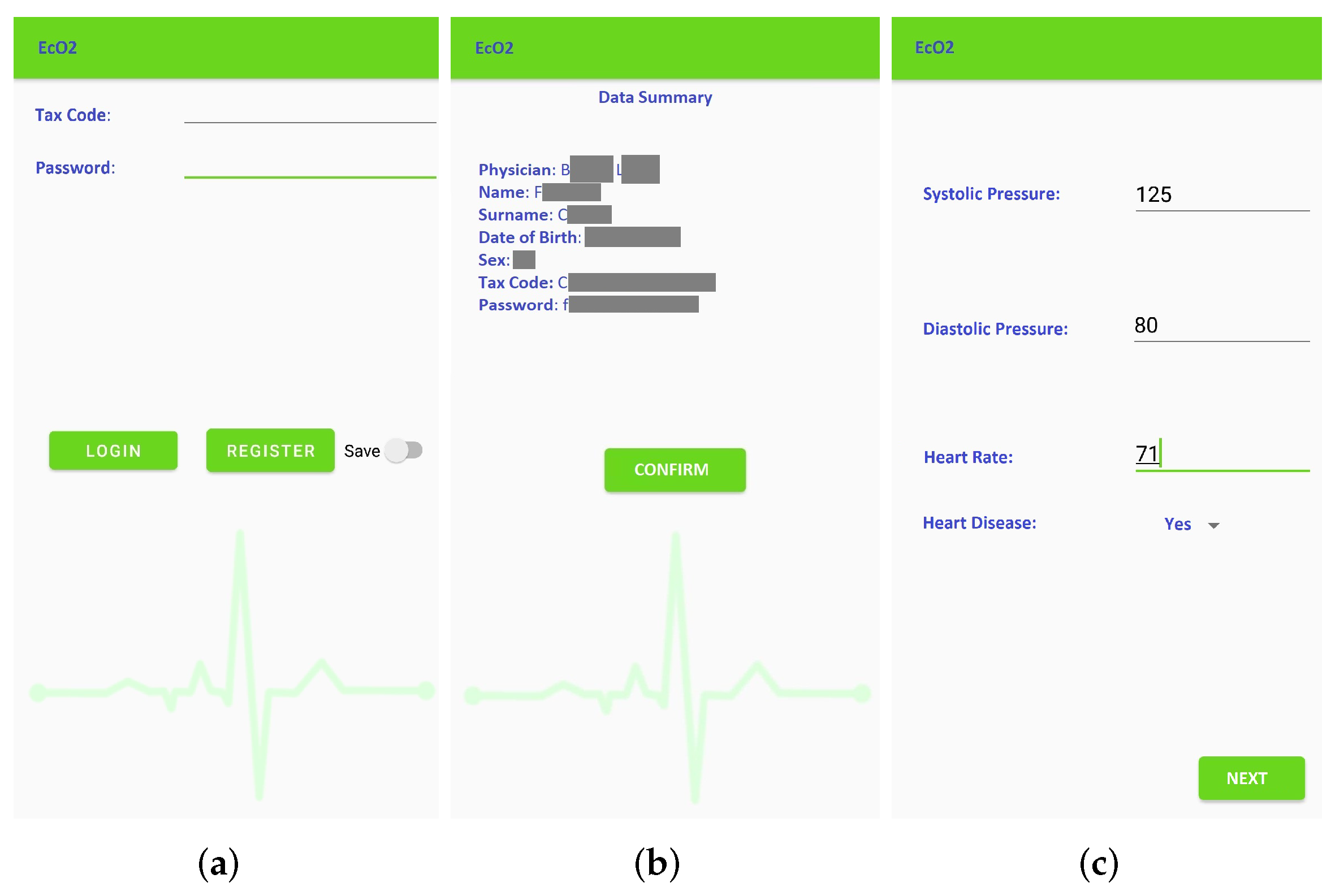
- Patient registration: Figure 4 shows the window for registration and/or log in. During registration, the patient inserts their tax code (which is automatically verified), and the patient is associated to the reference physician. The user also enters additional personal information (such as name, surnames, date of birth). The association to the wearable measurement devices is carried out by scanning a QR code generated specifically for a single device. These sensitive data are treated in full compliance with anonymity requirements. In fact, only when an anomaly is detected, the doctor is warned and is able to trace the patient’s identity. Figure 4b shows the window that summarizes the user’s data before they are sent to the cloud database, which checks the data and sends a feedback on the correct registration. Once the registration phase is completed, the patient is brought back to the log-in window to make the first log in. Furthermore, at this stage, there is a check with the database to verify that the password and tax code entered are correct.
- Vitals measurement: To allow the successive automated estimation of the systolic and diastolic pressure, a preliminary calibration procedure has to be carried out. In particular, the patient uses a sphygmomanometer to measure the systolic and diastolic pressure values, while the wearable sensing platform sensor is measuring HR and SpO2. Then, the patient manually enters these data in the application (Figure 4c). This phase, which has to be carried out only once, is necessary to identify the parameters that will subsequently allow the soft transducer to estimate the pressure. After the calibration, the patient can start using the soft transducer.
- Management of the patient’s Medical History: The management of the patient’s medical history is conducted by: (a) showing the daily progress by a graph of the measurements made, (b) reporting the symptoms during the day and (c) indicating any symptoms not present to study a certain correspondence. The cloud database is updated in real-time after each measurement session.
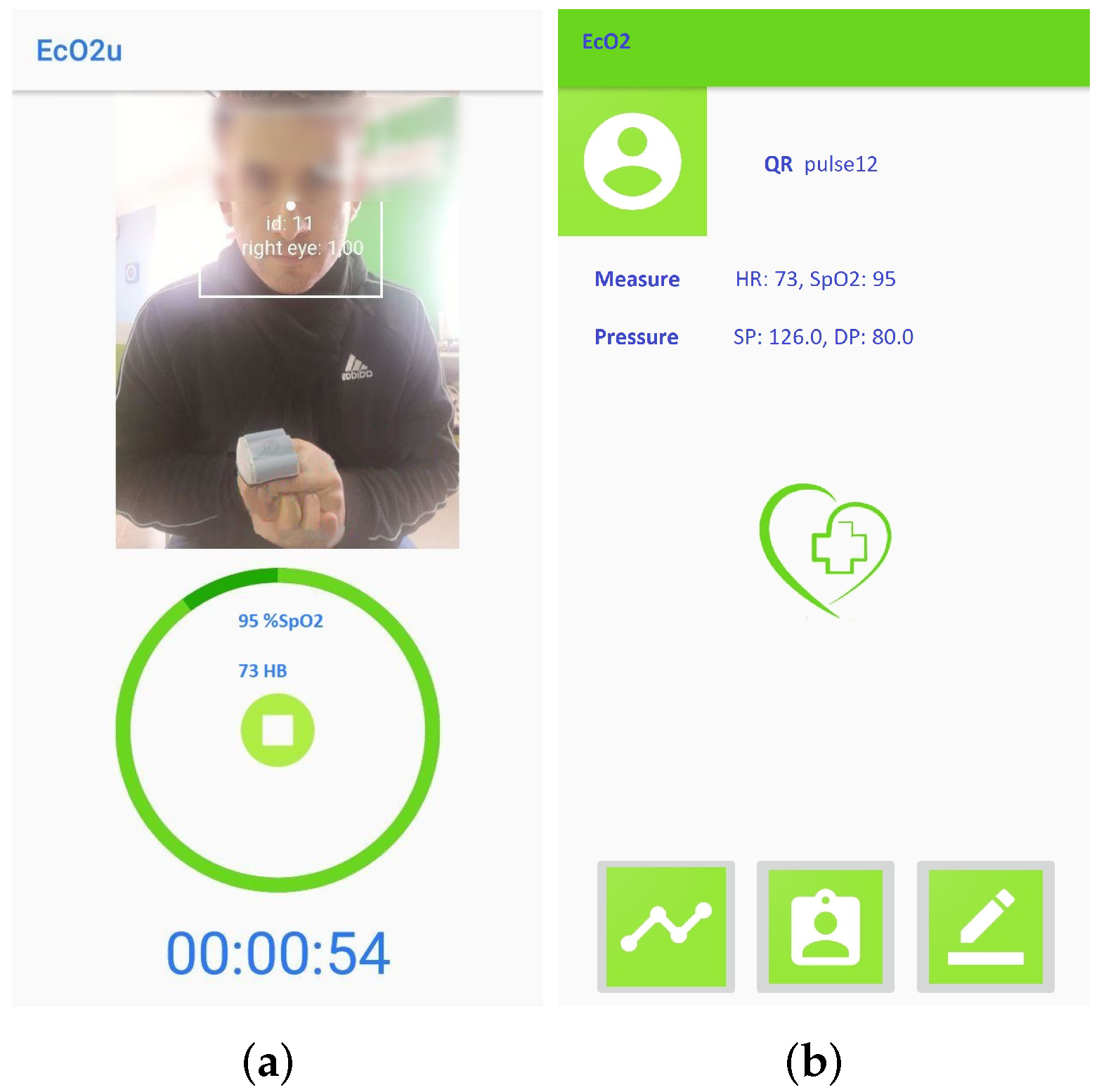
- Remote Vitals Visualization: The physician can access the EcO2u mobile application with the master credentials to view their patient list; after selecting the specific patient, the physician can display the most recent medical parameters, the graph of past trends and the list of notes, which can be also entered by the patient, in order to see if there is an onset of new symptoms that require a change in therapy (see Figure 5b).
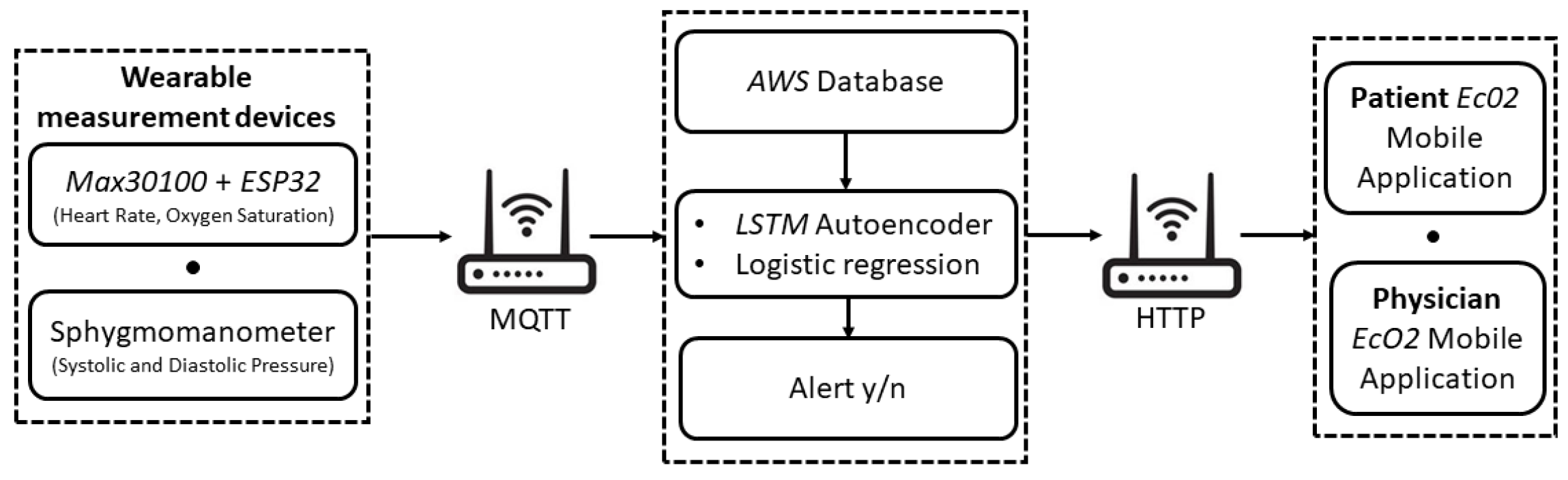
- AI processing: The AI-based processing of the acquired vitals provides a diagnostic tool to detect anomalies in real-time. In particular, as detailed in the following section, a multivariate linear regression is used to estimate the value of SP and DP, starting from the HR and SpO2 values coming from the MAX30100 and taking into account the age and the presence of diabetes for each patient, while a DL algorithm, based on an LSTM Autoencoder, is used to process the entire set of obtained data (HR, SpO2, SP, DP).
- Delivery of the Score result: The Score result is a synthetic quantity that indicates if an anomaly is detected based on the patient’s history and current data. In that case, the physician and the patient are immediately warned about the patient’s condition.
4.3. Deep Learning Algorithm for Anomaly Detection
- Data Set Creation: First, the reference data set for the anomaly detection was imported from [41]. The 50 subjects included are 80% men (40) and 20% women (10), with an age range ranging from 26 to 35 years old. Oxygen saturation, heart rate and identification are indicated for each user.
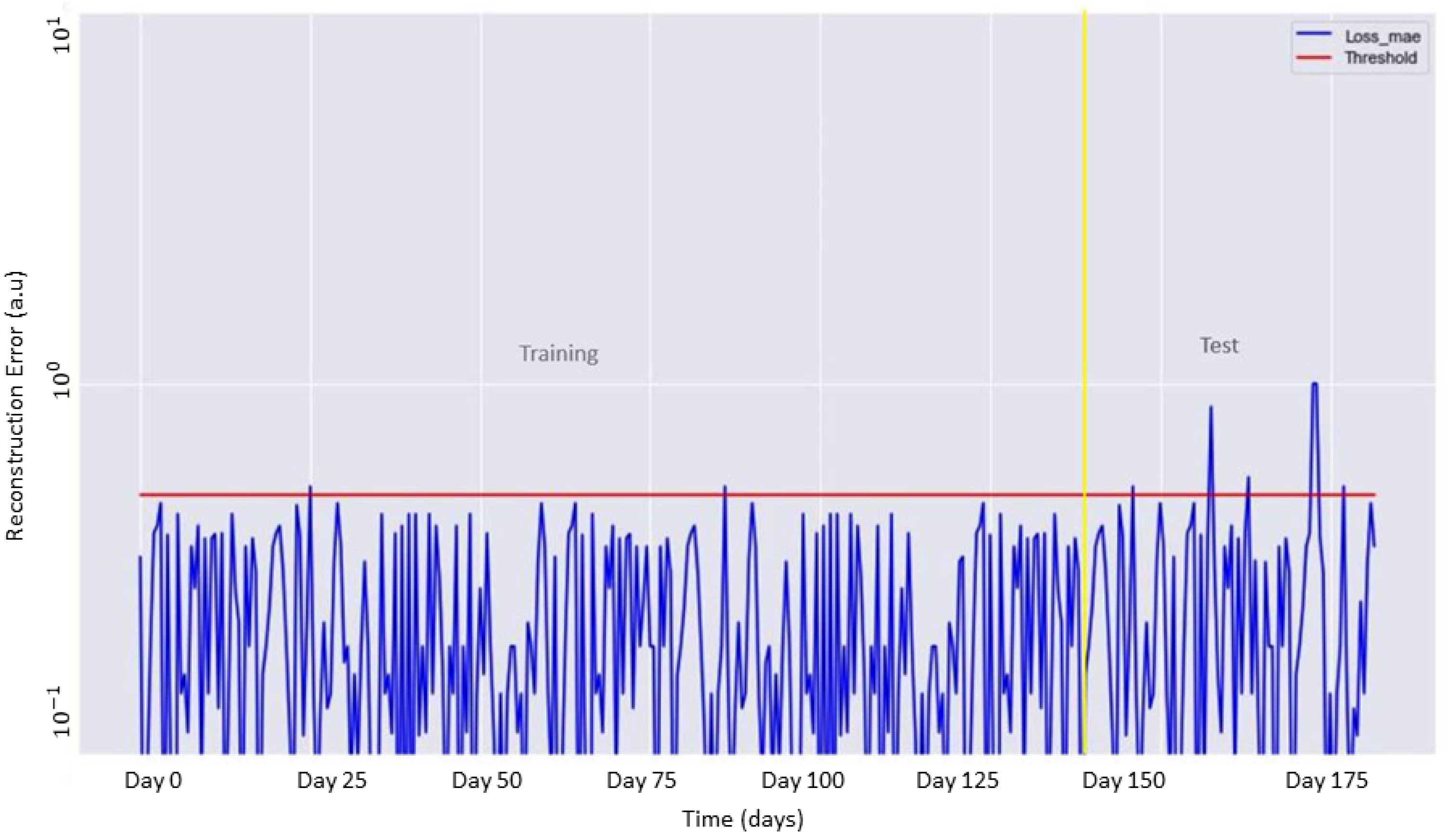
- Model Identification and Training: The second phase consisted of the construction of a normal behavior model using 80% of the imported data set as training data. The identification of this model is necessary to allow the subsequent classification of anomalies when they occur. The model chosen was the LSTM Autoencoder. This structure is characterized by an Encoder, which learns to generate an internal, compressed representation of input data, and a Decoder, which tries to reconstruct the original input on the basis of this internal representation. The Autoencoder was developed with an LSTM neural network. This choice was dictated by the fact that LSTM is the most suitable approach to process data when effects from past events need to be taken into account, differently from CNN, which does not depend on any previous information for prediction since it only uses the current window [42]. The LSTM requires pre-processing the data based on a three-dimensional array that contains the number of observations, the time window and the relevant information. To determine the LSTM architecture, it was considered that the number of layers and the corresponding number of neurons should be high enough to avoid underfitting but, at the same time, should be as low as possible to avoid both overfitting and high computational complexity. Therefore, an input level with 16 nodes, 2 hidden layers with 4 nodes each, and an output level with 16 nodes was chosen. The number of epochs was set to 100 and the batch size to 10. The model was trained by minimizing the reconstruction error, defined as the average absolute difference between the original input and the rebuilt output produced by the decoder.
- Alarm Value Identification: The third phase consisted of the identification of threshold values in order to mark the data as standard or anomalous. These thresholds were determined by the reconstruction errors that the Autoencoder performs in the training phase. An anomaly occurs if the obtained reconstruction error exceeds that threshold; in that case, the corresponding data are marked as anomalous.
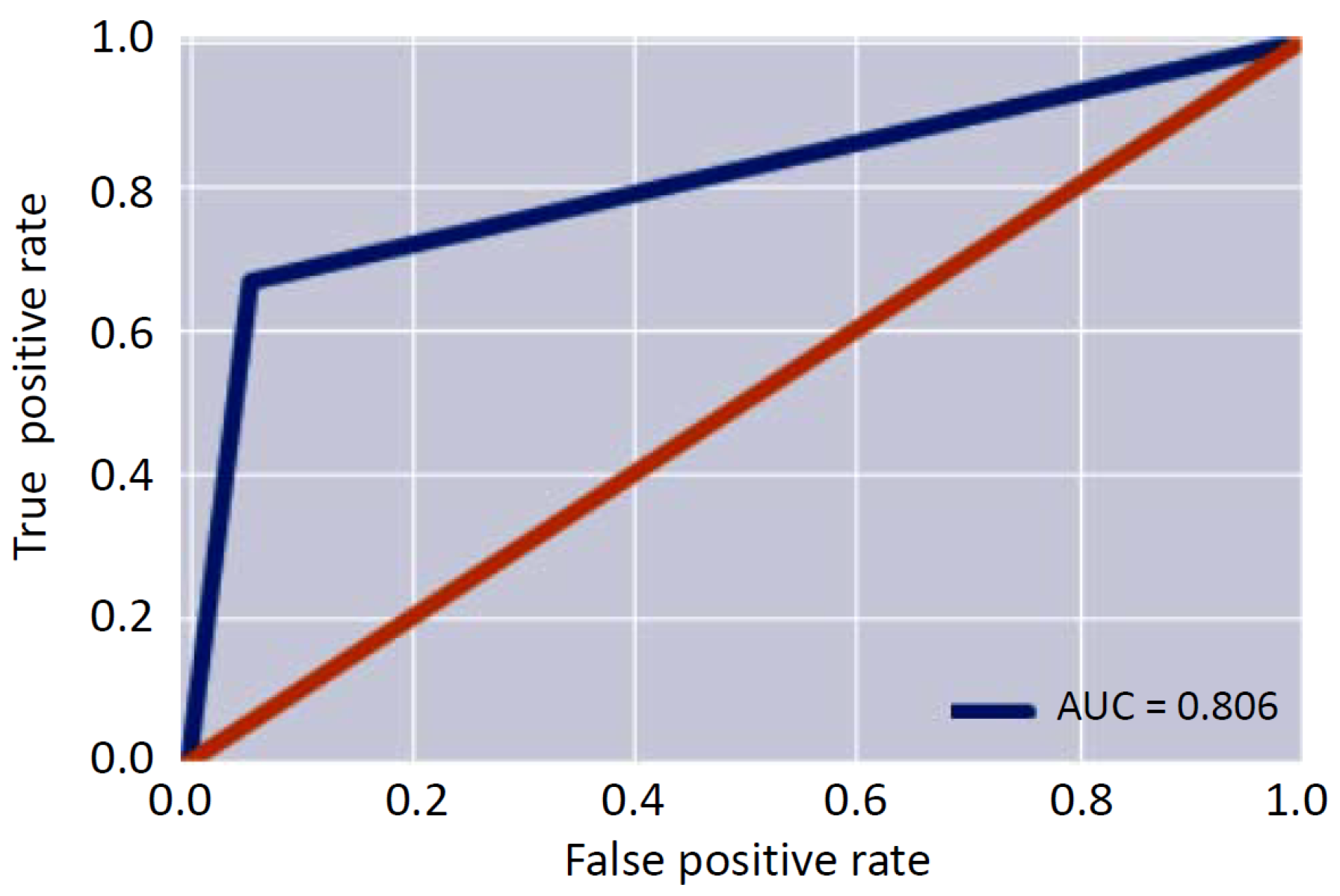
- Test Validation: The fourth phase allowed the validation of the threshold identified in the previous step. At this stage, the Autoencoder was provided with labeled data containing two anomalies to be identified. These test data are made up of the remaining 20% of the imported data set. The identification of an anomaly can be seen as a binary classification problem that provides a prediction score as output. The score indicates the certainty of the system that a given observation belongs to the standard class or that there is an anomaly.To this aim, the assessment of the obtained model was carried out using three figures of merit: the Area Under Curve-Receiving Operating Characteristic (AUC-ROC) curve; the F1 score; and the Binary Accuracy.
- The ROC curve is plotted following two metrics: True Positive Rate (also known as Sensivity) and False Positive Rate. The True Positive Rate is defined as the number of true positive results divided by the number of all samples that should have been identified as positive. On the other hand, the False Positive Rate is defined as the ratio between the number of negative results wrongly categorized as positive (false positives) and the total number of actual negative results. The ROC curve shows the relationship between the True Positive Rate and the False Positive Rate. The closer Area Under Curve (AUC) is to 1, the more accurate is the model.
- The score is calculated based on two metrics: Precision and Recall (also known as Sensivity or True Positive Rate and already defined in the previous item). The Precision is defined as the number of true positive results divided by the number of all positive results, including those not identified correctly. The score is obtained as the harmonic mean of the Precision and Recall, and it is a indication of the test’s accuracy.
- The Binary Accuracy represents how well a classification test correctly identifies or excludes a condition. Then, it is defined as the proportion of correct predictions among the total number of cases examined.
- Readjustment: Once the model is validated, it is readjusted after 30 days with further measurements provided by the user. The readjustment aims to identify customized threshold values for the personalized patient care.
5. Experimental Results and Discussion
5.1. Experimental Validation of the Telemonitoring System
5.2. Experimental Validation of the Developed DL Algorithm
Patient-Specific Customization and Validation of The Soft Transducer
- The user employed the soft transducer for 30 days. The acquisition of their vitals (twice a day) also included abnormal values, which were emulated by placing him/her under stress conditions (e.g., a short run).
- The obtained data set (60 samples) was split into 80% training (48 samples) and 20% test (12 samples). Therefore, the LSTM Autoencoder was re-trained in order to identify the patient specific threshold value
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Veenis, J.F.; Radhoe, S.P.; Hooijmans, P.; Brugts, J.J. Remote Monitoring in Chronic Heart Failure Patients: Is Non-Invasive Remote Monitoring the Way to Go? Sensors 2021, 21, 887. [Google Scholar] [CrossRef]
- Silva, A.F.; Tavakoli, M. Domiciliary Hospitalization through Wearable Biomonitoring Patches: Recent Advances, Technical Challenges, and the Relation to Covid-19. Sensors 2020, 20, 6835. [Google Scholar] [CrossRef] [PubMed]
- Khan, F.; Ghaffar, A.; Khan, N.; Cho, S.H. An Overview of Signal Processing Techniques for Remote Health Monitoring Using Impulse Radio UWB Transceiver. Sensors 2020, 20, 2479. [Google Scholar] [CrossRef] [PubMed]
- Schiavoni, R.; Monti, G.; Piuzzi, E.; Tarricone, L.; Tedesco, A.; De Benedetto, E.; Cataldo, A. Feasibility of a wearable reflectometric system for sensing skin hydration. Sensors 2020, 20, 2833. [Google Scholar] [CrossRef] [PubMed]
- Arquilla, K.; Webb, A.K.; Anderson, A.P. Textile electrocardiogram (ECG) electrodes for wearable health monitoring. Sensors 2020, 20, 1013. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Li, C.; Liu, W.; Wang, J.; Zhou, J.; Wang, S. A Multi-Sensor Wearable System for the Quantitative Assessment of Parkinson’s Disease. Sensors 2020, 20, 6146. [Google Scholar] [CrossRef]
- Kumar, S.; Buckley, J.L.; Barton, J.; Pigeon, M.; Newberry, R.; Rodencal, M.; Hajzeraj, A.; Hannon, T.; Rogers, K.; Casey, D.; et al. A wristwatch-based wireless sensor platform for IoT health monitoring applications. Sensors 2020, 20, 1675. [Google Scholar] [CrossRef] [Green Version]
- Corchia, L.; Monti, G.; De Benedetto, E.; Cataldo, A.; Angrisani, L.; Arpaia, P.; Tarricone, L. Fully-textile, wearable chipless tags for identification and tracking applications. Sensors 2020, 20, 429. [Google Scholar] [CrossRef] [Green Version]
- Schiavoni, R.; Monti, G.; Tedesco, A.; Tarricone, L.; Piuzzi, E.; De Benedetto, E.; Masciullo, A.; Cataldo, A. Microwave Wearable System for Sensing Skin Hydration. In Proceedings of the Conference Record—IEEE Instrumentation and Measurement Technology Conference, Glasgow, UK, 17–20 May 2021; Volume 2021. [Google Scholar] [CrossRef]
- Harb, H.; Mansour, A.; Nasser, A.; Cruz, E.M.; de la Torre Díez, I. A Sensor-Based Data Analytics for Patient Monitoring in Connected Healthcare Applications. IEEE Sens. J. 2021, 21, 974–984. [Google Scholar] [CrossRef]
- Yeh, K. A Secure IoT-Based Healthcare System With Body Sensor Networks. IEEE Access 2016, 4, 10288–10299. [Google Scholar] [CrossRef]
- Donati, M.; Celli, A.; Ruiu, A.; Saponara, S.; Fanucci, L. A telemedicine service platform exploiting BT/BLE wearable sensors for remote monitoring of chronic patients. In Proceedings of the 2018 7th International Conference on Modern Circuits and Systems Technologies (MOCAST), Thessaloniki, Greece, 7–9 May 2018; pp. 1–4. [Google Scholar]
- Rohmetra, H.; Raghunath, N.; Narang, P.; Chamola, V.; Guizani, M.; Lakkaniga, N.R. AI-enabled remote monitoring of vital signs for COVID-19: Methods, prospects and challenges. Computing 2021, 1–27. [Google Scholar] [CrossRef]
- Kumar, A.; Krishnamurthi, R.; Nayyar, A.; Sharma, K.; Grover, V.; Hossain, E. A Novel Smart Healthcare Design, Simulation, and Implementation Using Healthcare 4.0 Processes. IEEE Access 2020, 8, 118433–118471. [Google Scholar] [CrossRef]
- Rodrigues, J.J.P.C.; De Rezende Segundo, D.B.; Junqueira, H.A.; Sabino, M.H.; Prince, R.M.; Al-Muhtadi, J.; De Albuquerque, V.H.C. Enabling Technologies for the Internet of Health Things. IEEE Access 2018, 6, 13129–13141. [Google Scholar] [CrossRef]
- Omboni, S.; Panzeri, E.; Campolo, L. E-health in hypertension management: An insight into the current and future role of blood pressure telemonitoring. Curr. Hypertens. Rep. 2020, 22, 1–13. [Google Scholar] [CrossRef]
- Koshimizu, H.; Kojima, R.; Kario, K.; Okuno, Y. Prediction of blood pressure variability using deep neural networks. Int. J. Med. Inform. 2020, 136, 104067. [Google Scholar] [CrossRef]
- Lee, S.; Chang, J.H. Deep learning ensemble with asymptotic techniques for oscillometric blood pressure estimation. Comput. Methods Prog. Biomed. 2017, 151, 1–13. [Google Scholar] [CrossRef]
- Koren, G.; Nordon, G.; Radinsky, K.; Shalev, V. Machine learning of big data in gaining insight into successful treatment of hypertension. Pharmacol. Res. Perspect. 2018, 6, e00396. [Google Scholar] [CrossRef] [Green Version]
- Tzafestas, S.G. Synergy of IoT and AI in modern society: The robotics and automation case. Robot. Autom. Eng. J. 2018, 31, 1–15. [Google Scholar] [CrossRef]
- Knickerbocker, J.U.; Budd, R.; Dang, B.; Chen, Q.; Colgan, E.; Hung, L.; Kumar, S.; Lee, K.; Lu, M.; Nah, J.; et al. Heterogeneous integration technology demonstrations for future healthcare, IoT, and AI computing solutions. In Proceedings of the 2018 IEEE 68th Electronic Components and Technology Conference (ECTC), San Diego, CA, USA, 29 May–1 June 2018; pp. 1519–1528. [Google Scholar]
- Johnson, K.W.; Torres Soto, J.; Glicksberg, B.S.; Shameer, K.; Miotto, R.; Ali, M.; Ashley, E.; Dudley, J.T. Artificial intelligence in cardiology. J. Am. Coll. Cardiol. 2018, 71, 2668–2679. [Google Scholar] [CrossRef]
- Rajkomar, A.; Dean, J.; Kohane, I. Machine learning in medicine. N. Engl. J. Med. 2019, 380, 1347–1358. [Google Scholar] [CrossRef]
- Hijazi, S.; Page, A.; Kantarci, B.; Soyata, T. Machine learning in cardiac health monitoring and decision support. Computer 2016, 49, 38–48. [Google Scholar] [CrossRef]
- Arefa, I.; Alam, M.; Siddiquee, I.; Siddique, N. Performance Analysis of Machine Learning Algorithms for Hypertension Decision Support System. In Proceedings of the 2019 IEEE International Conference on Robotics, Automation, Artificial-intelligence and Internet-of-Things (RAAICON), Automation, Dhaka, Bangladesh, 29 November–1 December 2019; pp. 15–20. [Google Scholar]
- Huang, S.; Xu, Y.; Yue, L.; Wei, S.; Liu, L.; Gan, X.; Zhou, S.; Nie, S. Evaluating the risk of hypertension using an artificial neural network method in rural residents over the age of 35 years in a Chinese area. Hypertens. Res. 2010, 33, 722–726. [Google Scholar] [CrossRef]
- Youssef Ali Amer, A.; Wouters, F.; Vranken, J.; de Korte-de Boer, D.; Smit-Fun, V.; Duflot, P.; Beaupain, M.H.; Vandervoort, P.; Luca, S.; Aerts, J.M.; et al. Vital Signs Prediction and Early Warning Score Calculation Based on Continuous Monitoring of Hospitalised Patients Using Wearable Technology. Sensors 2020, 20, 6593. [Google Scholar] [CrossRef]
- Aileni, R.M.; Pasca, S.; Florescu, A. EEG-Brain Activity Monitoring and Predictive Analysis of Signals Using Artificial Neural Networks. Sensors 2020, 20, 3346. [Google Scholar] [CrossRef]
- Uddin, M.Z.; Hassan, M.M.; Alsanad, A.; Savaglio, C. A body sensor data fusion and deep recurrent neural network-based behavior recognition approach for robust healthcare. Inf. Fusion 2020, 55, 105–115. [Google Scholar] [CrossRef]
- Munir, M.; Siddiqui, S.A.; Dengel, A.; Ahmed, S. DeepAnT: A deep learning approach for unsupervised anomaly detection in time series. IEEE Access 2018, 7, 1991–2005. [Google Scholar] [CrossRef]
- Fitriyani, N.L.; Syafrudin, M.; Alfian, G.; Rhee, J. Development of disease prediction model based on ensemble learning approach for diabetes and hypertension. IEEE Access 2019, 7, 144777–144789. [Google Scholar] [CrossRef]
- Saleh, H.; Younis, E.M.; Sahal, R.; Ali, A.A. Predicting Systolic Blood Pressure in Real-Time Using Streaming Data and Deep Learning. Mob. Netw. Appl. 2020, 26, 326–335. [Google Scholar] [CrossRef]
- Hazari, S. Usability Factors to Consider When Developing Apps for Senior Citizen Population. Available online: http://appsusability.com/2012/06/20/elder/ (accessed on 12 November 2021).
- MAX30100 Technical Specification. Available online: https://www.maximintegrated.com/en/products/sensors/MAX30100.html?utm_source=google&utm_campaign=corp-sensors&s_kwcid=AL!8732!3!517495051369!b!!g!!&gclid=CjwKCAjwzt6LBhBeEiwAbPGOgU6XlnaLwAiRQZfmrDWlxDbKuBd9_edSl_jfpszGaTb4nB7qWRj94RoCXpIQAvD_BwE (accessed on 12 November 2021).
- ESP32 Technical Specification. Available online: https://www.espressif.com/en/products/socs/esp32 (accessed on 12 November 2021).
- Lazazzera, R.; Belhaj, Y.; Carrault, G. A new wearable device for blood pressure estimation using photoplethysmogram. Sensors 2019, 19, 2557. [Google Scholar] [CrossRef] [Green Version]
- Hsieh, Y.Y.; Wu, C.D.; Lu, S.S.; Tsao, Y. A linear regression model with dynamic pulse transit time features for noninvasive blood pressure prediction. In Proceedings of the 2016 IEEE Biomedical Circuits and Systems Conference (BioCAS), Shanghai, China, 17–19 October 2016; pp. 604–607. [Google Scholar] [CrossRef]
- Haddad, S.; Boukhayma, A.; Caizzone, A. Continuous PPG-Based Blood Pressure Monitoring Using Multi-Linear Regression. IEEE J. Biomed. Health Inform. 2021. aheadofprint. [Google Scholar] [CrossRef]
- Khalid, S.G.; Zhang, J.; Chen, F.; Zheng, D. Blood pressure estimation using photoplethysmography only: Comparison between different machine learning approaches. J. Healthc. Eng. 2018, 2018, 1548647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, B.; Ren, H.; Huang, G.; Cheng, Y.; Hu, C. Predicting blood pressure from physiological index data using the SVR algorithm. BMC Bioinform. 2019, 20, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Kaggle. Available online: https://www.kaggle.com/datasets (accessed on 13 June 2021).
- Selvin, S.; Vinayakumar, R.; Gopalakrishnan, E.A.; Menon, V.K.; Soman, K.P. Stock price prediction using LSTM, RNN and CNN-sliding window model. In Proceedings of the 2017 International Conference on Advances in Computing, Communications and Informatics (ICACCI), Udupi, India, 13–16 September 2017; pp. 1643–1647. [Google Scholar] [CrossRef]
- Arpaia, P.; De Benedetto, E.; Duraccio, L. Design, implementation, and metrological characterization of a wearable, integrated AR-BCI hands-free system for health 4.0 monitoring. Measurement 2021, 177, 109280. [Google Scholar] [CrossRef]
- Cattari, N.; Condino, S.; Cutolo, F.; Ferrari, M.; Ferrari, V. In situ visualization for 3d ultrasound-guided interventions with augmented reality headset. Bioengineering 2021, 8, 131. [Google Scholar] [CrossRef]
- Condino, S.; Montemurro, N.; Cattari, N.; D’Amato, R.; Thomale, U.; Ferrari, V.; Cutolo, F. Evaluation of a Wearable AR Platform for Guiding Complex Craniotomies in Neurosurgery. Ann. Biomed. Eng. 2021, 49, 2590–2605. [Google Scholar] [CrossRef]
- Viglialoro, R.; Condino, S.; Turini, G.; Carbone, M.; Ferrari, V.; Gesi, M. Augmented reality, mixed reality, and hybrid approach in healthcare simulation: A systematic review. Appl. Sci. 2021, 11, 2338. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject | HR (Bpm) 1st Session | HR (Bpm) 2nd Session | SP/DP (mmHg) 1st Session | SP/DP (mmHg) 2nd Session |
|---|---|---|---|---|
| #1 | 85 ± 3 | 82 ± 2 | 112/80 ± 2 | 112/79 ± 2 |
| #2 | 71 ± 2 | 68 ± 2 | 130/82 ±1 | 128/82 ± 2 |
| #3 | 88 ± 4 | 85 ± 4 | 125/85 ± 2 | 124/84 ± 1 |
| #4 | 75 ± 1 | 73 ± 2 | 126/84 ± 2 | 125/84 ± 1 |
| #5 | 70 ± 2 | 67 ± 1 | 136/82 ± 1 | 134/82 ± 2 |
| Metric | Result |
|---|---|
| True Positive | 68 |
| False Positive | 1 |
| False Negative | 4 |
| True Negative | 2 |
| True Positive Rate | 0.94 |
| False Positive Rate | 0.33 |
| Precision | 0.99 |
| Area Under Curve | 0.81 |
| F1 Score | 0.96 |
| Binary Accuracy | 0.93 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arpaia, P.; Crauso, F.; De Benedetto, E.; Duraccio, L.; Improta, G.; Serino, F. Soft Transducer for Patient’s Vitals Telemonitoring with Deep Learning-Based Personalized Anomaly Detection. Sensors 2022, 22, 536. https://doi.org/10.3390/s22020536
Arpaia P, Crauso F, De Benedetto E, Duraccio L, Improta G, Serino F. Soft Transducer for Patient’s Vitals Telemonitoring with Deep Learning-Based Personalized Anomaly Detection. Sensors. 2022; 22(2):536. https://doi.org/10.3390/s22020536
Chicago/Turabian StyleArpaia, Pasquale, Federica Crauso, Egidio De Benedetto, Luigi Duraccio, Giovanni Improta, and Francesco Serino. 2022. "Soft Transducer for Patient’s Vitals Telemonitoring with Deep Learning-Based Personalized Anomaly Detection" Sensors 22, no. 2: 536. https://doi.org/10.3390/s22020536
APA StyleArpaia, P., Crauso, F., De Benedetto, E., Duraccio, L., Improta, G., & Serino, F. (2022). Soft Transducer for Patient’s Vitals Telemonitoring with Deep Learning-Based Personalized Anomaly Detection. Sensors, 22(2), 536. https://doi.org/10.3390/s22020536