
Machine Learning for Renal Pathologies: An Updated Survey

 ,
,  , ,
, ,  ,
,  and
and 
Abstract
:1. Introduction
- -
- segmentation and identification of the anatomy of interest within the diagnostic images (e.g., kidney masses such as tumors, cysts, etc.);
- -
- classification of a kidney mass type, or of the stage in which a specific tumor is found;
- -
- prediction of the evolution of kidney functionality, which can highlight the presence of pathologies.
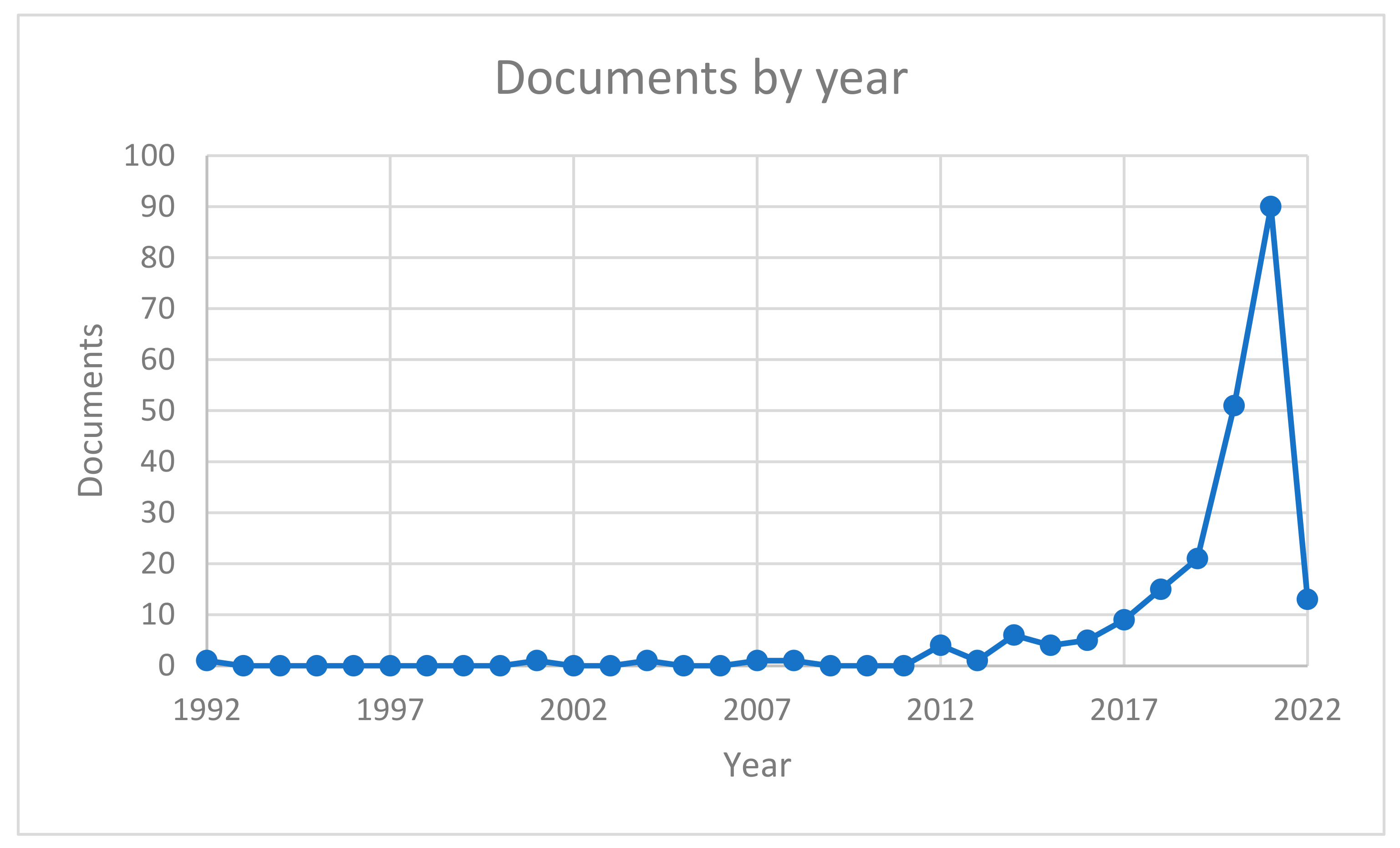
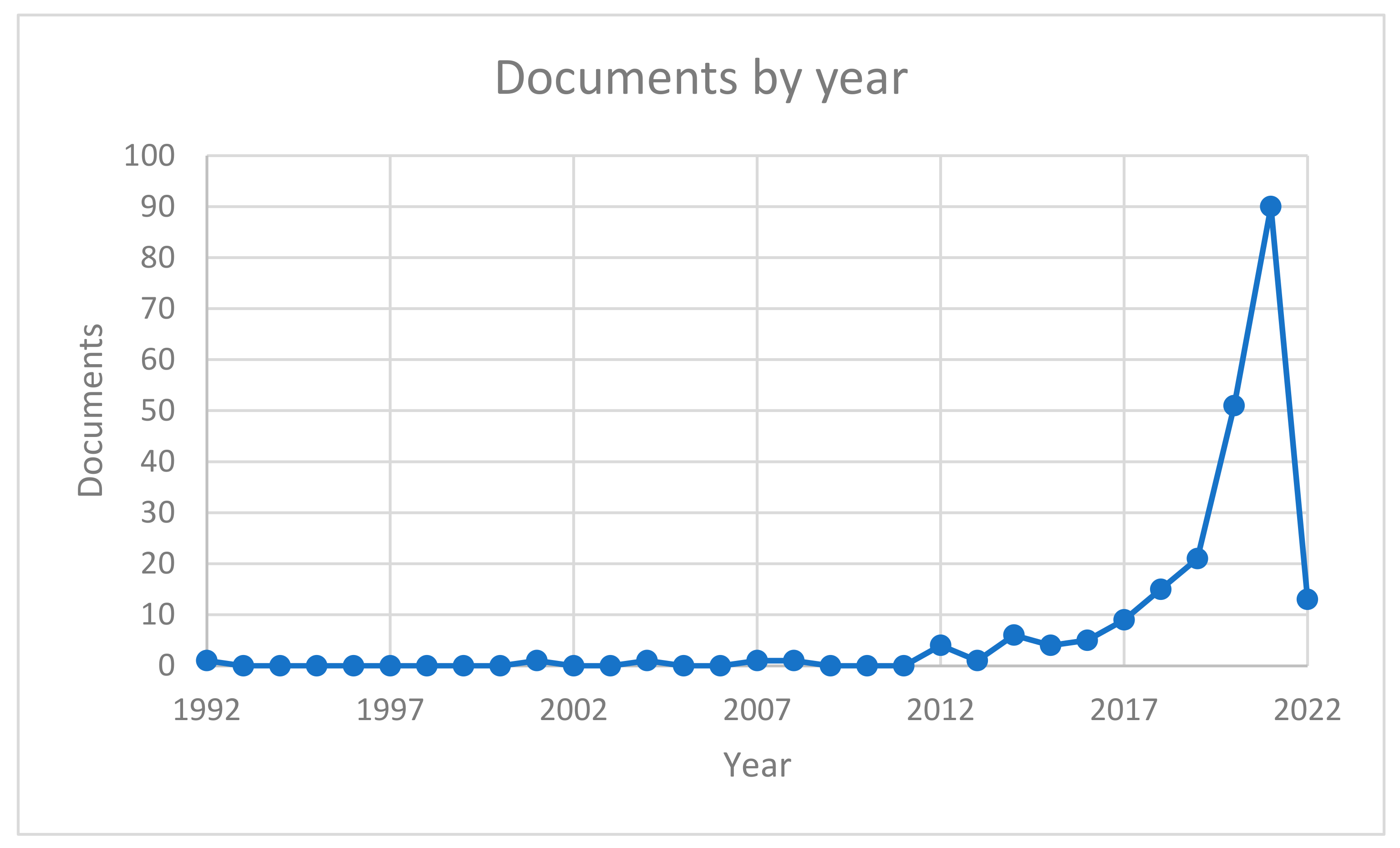
2. Article Selection
AND
KEY (artificial AND intelligence AND machine AND learning AND kidney)
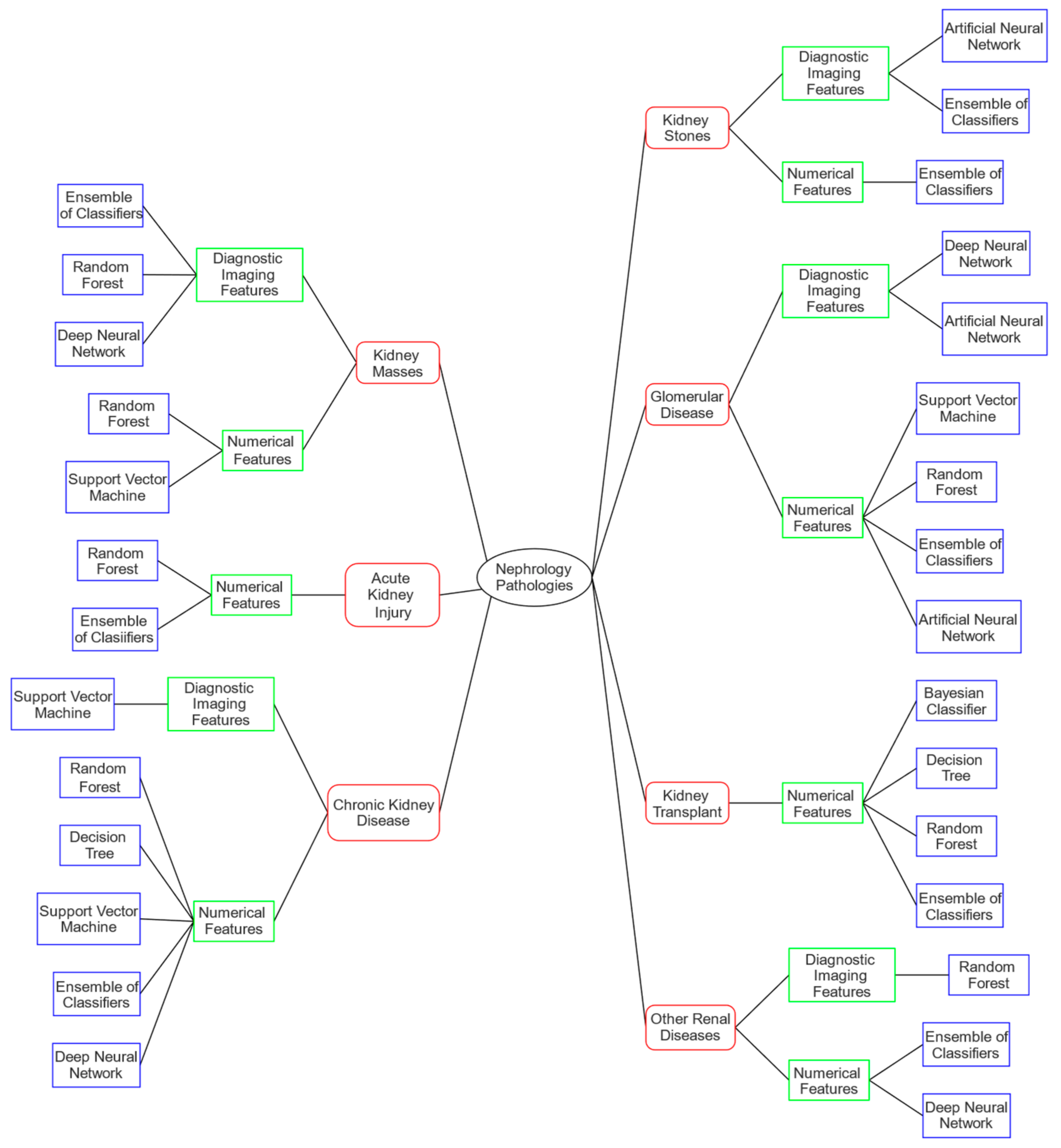
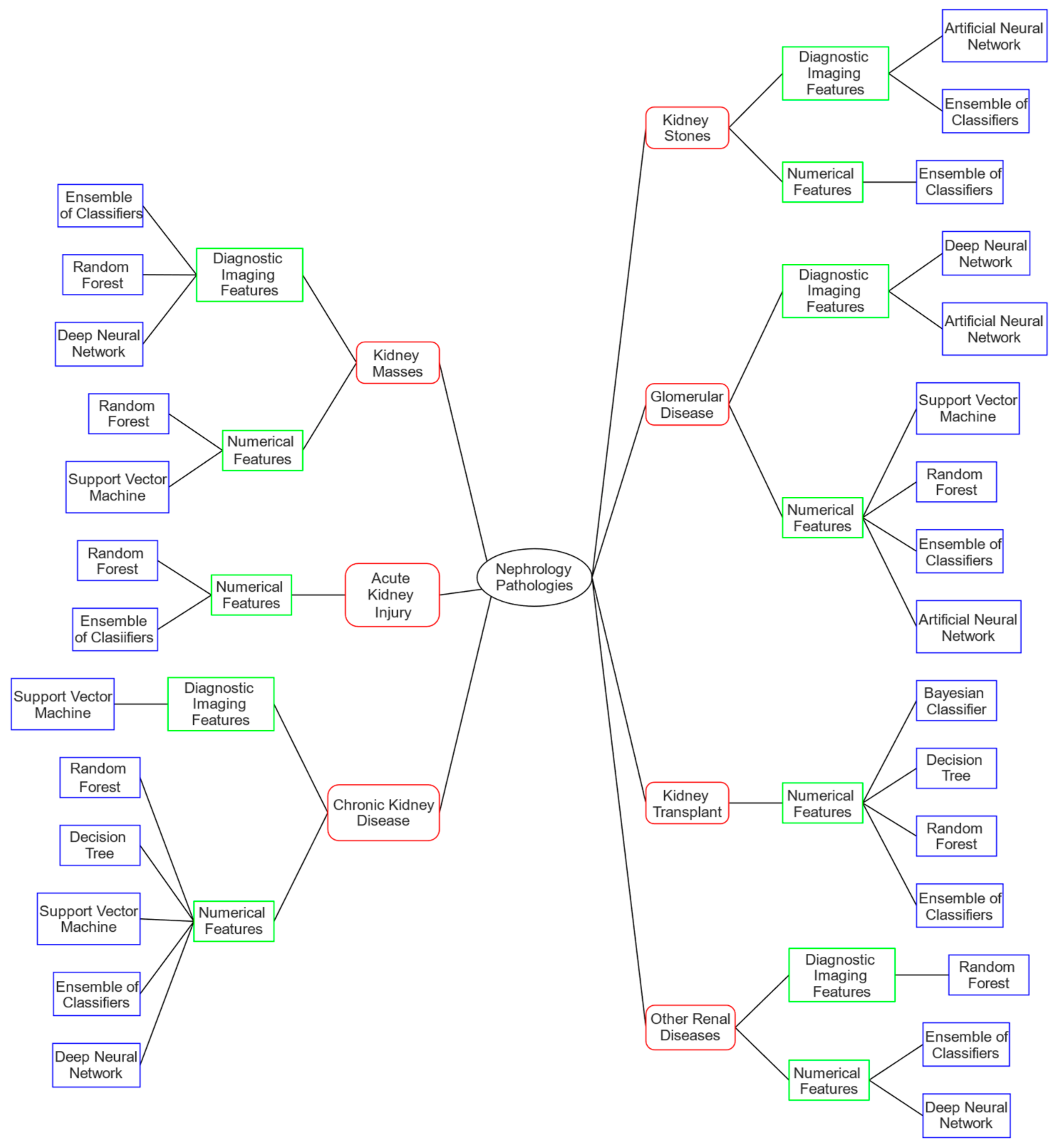
3. Machine Learning Approaches for Nephrology
- (1)
- segmentation and identification, which intends to analyze diagnostic images with the purpose of highlighting or detecting one or more specific elements;
- (2)
- classification, which aims to perform a diagnosis or to determine the degree of severity of disease;
- (3)
- prediction, which aims to prevent or forecast some future event, e.g., predict either the degeneration of a disease or the outcome of a specific therapy.
3.1. Kidney Masses
3.2. Acute Kidney Injury
3.3. Chronic Kidney Disease
3.4. Kidney Stone
3.5. Glomerular Diseases
3.6. Kidney Transplant
3.7. Other Renal Diseases
4. Databases Used in Reviewed Research
5. Discussion
6. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Sutherland, S.M.; Goldstein, S.L.; Bagshaw, S.M. Leveraging Big Data and Electronic Health Records to Enhance Novel Approaches to Acute Kidney Injury Research and Care. Blood Purif. 2017, 44, 68–76. [Google Scholar] [CrossRef] [PubMed]
- Thongprayoon, C.; Kaewput, W.; Kovvuru, K.; Hansrivijit, P.; Kanduri, S.R.; Bathini, T.; Chewcharat, A.; Leeaphorn, N.; Gonzalez-Suarez, M.L.; Cheungpasitporn, W. Promises of Big Data and Artificial Intelligence in Nephrology and Transplantation. J. Clin. Med. 2020, 9, 1107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zitt, E.; Pscheidt, C.; Concin, H.; Kramar, R.; Peter, R.S.; Beyersmann, J.; Lhotta, K.; Nagel, G. Long-Term Risk for End-Stage Kidney Disease and Death in a Large Population-Based Cohort. Sci. Rep. 2018, 8, 7729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, R.; Kanso, A.; Sedor, J.R. Chronic Kidney Disease and Its Complications. Prim. Care-Clin. Off. Pract. 2008, 35, 329–344. [Google Scholar] [CrossRef] [Green Version]
- Thompson, S.; James, M.; Wiebe, N.; Hemmelgarn, B.; Manns, B.; Klarenbach, S.; Tonelli, M. Cause of Death in Patients with Reduced Kidney Function. J. Am. Soc. Nephrol. 2015, 26, 2504–2511. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.K.; Knicely, D.H.; Grams, M.E. Chronic Kidney Disease Diagnosis and Management: A Review. J. Am. Med. Assoc. 2019, 322, 1294–1304. [Google Scholar] [CrossRef]
- Yang, H.C.; Zuo, Y.; Fogo, A.B. Models of Chronic Kidney Disease. Drug Discov. Today Dis. Model. 2010, 7, 13–19. [Google Scholar] [CrossRef] [Green Version]
- Thompson, R.H.; Kurta, J.M.; Kaag, M.; Tickoo, S.K.; Kundu, S.; Katz, D.; Nogueira, L.; Reuter, V.E.; Russo, P. Tumor Size Is Associated With Malignant Potential in Renal Cell Carcinoma Cases. J. Urol. 2009, 181, 2033–2036. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Remulla, D.; Nguyen, J.H.; Aastha, D.; Liu, Y.; Dasgupta, P.; Hung, A.J. Current Status of Artificial Intelligence Applications in Urology and Their Potential to Influence Clinical Practice. BJU Int. 2019, 124, 567–577. [Google Scholar] [CrossRef]
- Rashidi, H.H.; Tran, N.K.; Betts, E.V.; Howell, L.P.; Green, R. Artificial Intelligence and Machine Learning in Pathology: The Present Landscape of Supervised Methods. Acad. Pathol. 2019, 6, 2374289519873088. [Google Scholar] [CrossRef]
- Zaidi, S.S.A.; Ansari, M.S.; Aslam, A.; Kanwal, N.; Asghar, M.; Lee, B. A Survey of Modern Deep Learning Based Object Detection Models. Digit. Signal Process. Rev. J. 2022, 126, 103514. [Google Scholar] [CrossRef]
- Papastratis, I. Speech Recognition: A Review of the Different Deep Learning Approaches. Available online: https://theaisummer.com/speech-recognition/ (accessed on 7 June 2022).
- Magherini, R.; Mussi, E.; Servi, M.; Volpe, Y. Emotion Recognition in the Times of COVID 19: Coping with Face Masks. Intellingent Syst. Appl. 2022, 200094. [Google Scholar] [CrossRef]
- Wankhade, M.; Rao, A.C.S.; Kulkarni, C. A Survey on Sentiment Analysis Methods, Applications, and Challenges; Springer: Amasterdam, The Netherlands, 2022; ISBN 0123456789. [Google Scholar]
- Ligthart, A.; Catal, C.; Tekinerdogan, B. Systematic Reviews in Sentiment Analysis: A Tertiary Study; Springer: Amasterdam, The Netherlands, 2021; Volume 54, ISBN 1046202109973. [Google Scholar]
- Hardy, M.; Harvey, H. Artificial Intelligence in Diagnostic Imaging: Impact on the Radiography Profession. Br. J. Radiol. 2020, 93, 20190840. [Google Scholar] [CrossRef]
- Jvion. Healthcare & Clinical AI Platform. Available online: https://jvion.com/ (accessed on 7 June 2022).
- Wellframe. Digital Health Management. Available online: www.wellframe.com (accessed on 7 June 2022).
- Enlitic. Healthcare Information Technology with Enlitic. Available online: https://www.enlitic.com/ (accessed on 7 June 2022).
- Johnson, K.B.; Wei, W.Q.; Weeraratne, D.; Frisse, M.E.; Misulis, K.; Rhee, K.; Zhao, J.; Snowdon, J.L. Precision Medicine, AI, and the Future of Personalized Health Care. Clin. Transl. Sci. 2021, 14, 86–93. [Google Scholar] [CrossRef] [PubMed]
- GNS Health Care. Available online: www.gnshealthcare.com (accessed on 7 June 2022).
- Oncora Medical: Real World Data to Fight Cancer. Available online: www.oncora.ai (accessed on 7 June 2022).
- Zakipoint Health. Available online: www.zakipointhealth.com (accessed on 7 June 2022).
- Khan, Z.F.; Alotaibi, S.R. Applications of Artificial Intelligence and Big Data Analytics in M-Health: A Healthcare System Perspective. J. Healthc. Eng. 2020, 2020, 8894694. [Google Scholar] [CrossRef] [PubMed]
- Ballard, B.D.; Guzman, N. Renal Mass. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Chen, C.J.; Pai, T.W.; Fujita, H.; Lee, C.H.; Chen, Y.T.; Chen, K.S.; Chen, Y.C. Stage diagnosis for chronic kidney disease based on ultrasonography. In Proceedings of the International Conference on Fuzzy Systems and Knowledge Discovery (FSKD), Xiamen, China, 19–21 August 2014; pp. 525–530. [Google Scholar] [CrossRef]
- Lee, Y.; Kim, N.; Cho, K.S.; Kang, S.H.; Dae, Y.K.; Yoon, Y.J.; Kim, J.K. Bayesian Classifier for Predicting Malignant Renal Cysts on MDCT: Early Clinical Experience. Am. J. Roentgenol. 2009, 193, 106–111. [Google Scholar] [CrossRef]
- Kunapuli, G.; Varghese, B.A.; Ganapathy, P.; Desai, B.; Cen, S.; Aron, M.; Gill, I.; Duddalwar, V. A Decision-Support Tool for Renal Mass Classification. J. Digit. Imaging 2018, 31, 929–939. [Google Scholar] [CrossRef]
- Erdim, C.; Yardimci, A.H.; Bektas, C.T.; Kocak, B.; Koca, S.B.; Demir, H.; Kilickesmez, O. Prediction of Benign and Malignant Solid Renal Masses: Machine Learning-Based CT Texture Analysis. Acad. Radiol. 2020, 27, 1422–1429. [Google Scholar] [CrossRef]
- Kocak, B.; Ates, E.; Durmaz, E.S.; Ulusan, M.B.; Kilickesmez, O. Influence of Segmentation Margin on Machine Learning–Based High-Dimensional Quantitative CT Texture Analysis: A Reproducibility Study on Renal Clear Cell Carcinomas. Eur. Radiol. 2019, 29, 4765–4775. [Google Scholar] [CrossRef]
- Kocak, B.; Durmaz, E.S.; Kaya, O.K.; Kilickesmez, O. Machine Learning-Based Unenhanced CT Texture Analysis for Predicting BAP1 Mutation Status of Clear Cell Renal Cell Carcinomas. Acta Radiol. 2019, 61, 856–864. [Google Scholar] [CrossRef]
- Cui, E.; Li, Z.; Ma, C.; Li, Q.; Lei, Y.; Lan, Y.; Yu, J.; Zhou, Z.; Li, R.; Long, W.; et al. Predicting the ISUP Grade of Clear Cell Renal Cell Carcinoma with Multiparametric MR and Multiphase CT Radiomics. Eur. Radiol. 2020, 30, 2912–2921. [Google Scholar] [CrossRef]
- Bektas, C.T.; Kocak, B.; Yardimci, A.H.; Turkcanoglu, M.H.; Yucetas, U.; Koca, S.B.; Erdim, C.; Kilickesmez, O. Clear Cell Renal Cell Carcinoma: Machine Learning-Based Quantitative Computed Tomography Texture Analysis for Prediction of Fuhrman Nuclear Grade. Eur. Radiol. 2018, 29, 1153–1163. [Google Scholar] [CrossRef] [PubMed]
- Azuaje, F.; Kim, S.-Y.; Perez Hernandez, D.; Dittmar, G. Connecting Histopathology Imaging and Proteomics in Kidney Cancer through Machine Learning. J. Clin. Med. 2019, 8, 1535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, B.; Mukherjee, S.; Jain, M. A New Method Using Multiphoton Imaging and Morphometric Analysis for Differentiating Chromophobe Renal Cell Carcinoma and Oncocytoma Kidney Tumors. Multiphot. Microsc. Biomed. Sci. XVI 2016, 9712, 179–186. [Google Scholar] [CrossRef]
- Singh, N.P.; Bapi, R.S.; Vinod, P.K. Machine Learning Models to Predict the Progression from Early to Late Stages of Papillary Renal Cell Carcinoma. Comput. Biol. Med. 2018, 100, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Alonso-Betanzos, A.; Bolón-Canedo, V.; Morán-Fernández, L.; Sánchez-Maroño, N. A Review of Microarray Datasets: Where to Find Them and Specific Characteristics; Methods in Molecular Biology Series; Humana Press: Totowa, NJ, USA, 2019; Volume 1986, pp. 65–85. ISBN 9781493994427. [Google Scholar]
- Isensee, F.; Maier-Hein, K.H. An Attempt at Beating the 3D U-Net. arXiv 2019, arXiv:1908.02182. [Google Scholar] [CrossRef] [Green Version]
- Hou, X.; Xie, C.; Li, F.; Nan, Y. Cascaded Semantic Segmentation for Kidney and Tumor. Submiss. 2019 Kidney Tumor Segm. Chall. KiTS19 2019, 2–6. [Google Scholar] [CrossRef] [Green Version]
- Mu, G.; Lin, Z.; Han, M.; Yao, G.; Gao, Y. Segmentation of Kidney Tumor by Multi-Resolution VB-Nets. Submiss. 2019 Kidney Tumor Segm. Chall. KiTS19 2019, 1–5. [Google Scholar] [CrossRef] [Green Version]
- National Cancer Institute. Clinical Proteomic Tumor Analysis Consortium (CPTAC) Radiology Data from the Clinical Proteomic Tumor Analysis Consortium Clear Cell Renal Cell Carcinoma CPTAC-CCRCC Collection. 2018. Available online: https://wiki.cancerimagingarchive.net/display/Public/CPTAC-CCRCC (accessed on 7 June 2022).
- National Cancer Institute GDC Data Portal. Genes. Available online: https://portal.gdc.cancer.gov/genes/ENSG00000143294 (accessed on 7 June 2022).
- Yang, X.J.; Tan, M.-H.; Kim, H.L.; Ditlev, J.A.; Betten, M.W.; Png, C.E.; Kort, E.J.; Futami, K.; Furge, K.A.; Takahashi, M.; et al. A Molecular Classification of Papillary Renal Cell Carcinoma. Cancer Res. 2005, 65, 5628–5637. [Google Scholar] [CrossRef] [Green Version]
- KiTS19—Grand Challenge. Available online: https://kits19.grand-challenge.org/home (accessed on 7 June 2022).
- Sanchez-Pinto, L.N.; Venable, L.R.; Fahrenbach, J.; Churpek, M.M. Comparison of Variable Selection Methods for Clinical Predictive Modeling. Int. J. Med. Inform. 2018, 116, 10–17. [Google Scholar] [CrossRef]
- Penny-Dimri, J.C.; Bergmeir, C.; Reid, C.M.; Williams-Spence, J.; Cochrane, A.D.; Smith, J.A. Machine Learning Algorithms for Predicting and Risk Profiling of Cardiac Surgery-Associated Acute Kidney Injury. Semin. Thorac. Cardiovasc. Surg. 2021, 33, 735–745. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Yang, D.; Liu, Z.; Chen, C.; Ge, M.; Li, X.; Luo, T.; Wu, Z.; Shi, C.; Wang, B.; et al. An Explainable Supervised Machine Learning Predictor of Acute Kidney Injury after Adult Deceased Donor Liver Transplantation. J. Transl. Med. 2021, 19, 321. [Google Scholar] [CrossRef] [PubMed]
- Tran, N.K.; Sen, S.; Palmieri, T.L.; Lima, K.; Falwell, S.; Wajda, J.; Rashidi, H.H. Artificial Intelligence and Machine Learning for Predicting Acute Kidney Injury in Severely Burned Patients: A Proof of Concept. Burns 2019, 45, 1350–1358. [Google Scholar] [CrossRef] [PubMed]
- Fix, E.; Hodges, J.L. Discriminatory Analysis. Nonparametric Discrimination: Consistency Properties. Int. Stat. Rev. Rev. Int. Stat. 1989, 57, 238. [Google Scholar] [CrossRef]
- Ibrahim, N.E.; McCarthy, C.P.; Shrestha, S.; Gaggin, H.K.; Mukai, R.; Magaret, C.A.; Rhyne, R.F.; Januzzi, J.L. A Clinical, Proteomics, and Artificial Intelligence-Driven Model to Predict Acute Kidney Injury in Patients Undergoing Coronary Angiography. Clin. Cardiol. 2019, 42, 292–298. [Google Scholar] [CrossRef] [Green Version]
- Tseng, P.Y.; Chen, Y.T.; Wang, C.H.; Chiu, K.M.; Peng, Y.S.; Hsu, S.P.; Chen, K.L.; Yang, C.Y.; Lee, O.K.S. Prediction of the Development of Acute Kidney Injury Following Cardiac Surgery by Machine Learning. Crit. Care 2020, 24, 478. [Google Scholar] [CrossRef]
- Azzalini, L.; Candilio, L.; McCullough, P.A.; Colombo, A. Current Risk of Contrast-Induced Acute Kidney Injury After Coronary Angiography and Intervention: A Reappraisal of the Literature. Can. J. Cardiol. 2017, 33, 1225–1228. [Google Scholar] [CrossRef]
- Connell, A.; Montgomery, H.; Martin, P.; Nightingale, C.; Sadeghi-Alavijeh, O.; King, D.; Karthikesalingam, A.; Hughes, C.; Back, T.; Ayoub, K.; et al. Evaluation of a Digitally-Enabled Care Pathway for Acute Kidney Injury Management in Hospital Emergency Admissions. NPJ Digit. Med. 2019, 2, 67. [Google Scholar] [CrossRef] [Green Version]
- Scanlon, L.A.; O’hara, C.; Garbett, A.; Barker-Hewitt, M.; Barriuso, J. Developing an Agnostic Risk Prediction Model for Early Aki Detection in Cancer Patients. Cancers 2021, 13, 4182. [Google Scholar] [CrossRef]
- Song, X.; Yu, A.S.L.; Kellum, J.A.; Waitman, L.R.; Matheny, M.E.; Simpson, S.Q.; Hu, Y.; Liu, M. Cross-Site Transportability of an Explainable Artificial Intelligence Model for Acute Kidney Injury Prediction. Nat. Commun. 2020, 11, 5668. [Google Scholar] [CrossRef]
- Kursa, M.B.; Jankowski, A.; Rudnicki, W.R. Boruta—A System for Feature Selection. Fundam. Inform. 2010, 101, 271–285. [Google Scholar] [CrossRef]
- Churpek, M.M.; Yuen, T.C.; Winslow, C.; Robicsek, A.A.; Meltzer, D.O.; Gibbons, R.D.; Edelson, D.P. Multicenter Development and Validation of a Risk Stratification Tool for Ward Patients. Am. J. Respir. Crit. Care Med. 2014, 190, 649–655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanchez-Pinto, L.N.; Khemani, R.G. Development of a Prediction Model of Early Acute Kidney Injury in Critically Ill Children Using Electronic Health Record Data. Pediatr. Crit. Care Med. 2016, 17, 508–515. [Google Scholar] [CrossRef] [PubMed]
- National Database|ANZSCTS. Available online: https://anzscts.org/database (accessed on 17 February 2022).
- ClinicalTrials.Gov. The CASABLANCA Study: Catheter Sampled Blood Archive in Cardiovascular Diseases—Full Text View—ClinicalTrials.Gov. Available online: https://clinicaltrials.gov/ct2/show/study/NCT00842868 (accessed on 16 March 2022).
- Waitman, L.R.; Aaronson, L.S.; Nadkarni, P.M.; Connolly, D.W.; Campbell, J.R. The Greater Plains Collaborative: A PCORnet Clinical Research Data Network. J. Am. Med. Inform. Assoc. 2014, 21, 637–641. [Google Scholar] [CrossRef] [Green Version]
- Facts about Chronic Kidney Disease. Available online: https://www.kidney.org/news/newsroom/fsindex (accessed on 9 May 2022).
- Botev, R.; Mallié, J.-P. Reporting the EGFR and Its Implication for CKD Diagnosis. Clin. J. Am. Soc. Nephrol. 2008, 3, 1606–1607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dua, D.; Graff, C. UCI Machine Learning Repository. Available online: http://archive.ics.uci.edu/ml (accessed on 7 June 2022).
- Salekin, A.; Stankovic, J. Detection of chronic kidney disease and selecting important predictive attributes. In Proceedings of the 2016 IEEE International Conference on Healthcare Informatics (ICHI), Chicago, IL, USA, 4–7 October 2016; pp. 262–270. [Google Scholar] [CrossRef]
- Boukenze, B.; Haqiq, A.; Mousannif, H. Predicting Chronic Kidney Failure Disease Using Data Mining Techniques. Lect. Notes Electr. Eng. 2017, 397, 701–712. [Google Scholar] [CrossRef]
- Charleonnan, A.; Fufaung, T.; Niyomwong, T.; Chokchueypattanakit, W.; Suwannawach, S.; Ninchawee, N. Predictive analytics for chronic kidney disease using machine learning techniques. In Proceedings of the Management and Innovation Technology International Conference (MITicon 2016), Bang-Saen, Thailand, 12–14 October 2016; pp. MIT80–MIT83. [Google Scholar] [CrossRef]
- Wibawa, M.S.; Maysanjaya, I.M.D.; Putra, I.M.A.W. Boosted classifier and features selection for enhancing chronic kidney disease diagnose. In Proceedings of the International Conference on Cyber and IT Service Management (CITSM), Denpasar, Indonesia, 8–10 August 2017. [Google Scholar] [CrossRef]
- Subasi, A.; Alickovic, E.; Kevric, J. Diagnosis of Chronic Kidney Disease by Using Random Forest; IFMBE Proceedings Book Series; Springer: Berlin/Heidelberg, Germany, 2017; pp. 589–594. [Google Scholar]
- Aljaaf, A.J.; Al-Jumeily, D.; Haglan, H.M.; Alloghani, M.; Baker, T.; Hussain, A.J.; Mustafina, J. Early prediction of chronic kidney disease using machine learning supported by predictive analytics. In Proceedings of the 2018 IEEE Congress on Evolutionary Computation (CEC 2018), Rio de Janeiro, Brazil, 8–13 July 2018. [Google Scholar] [CrossRef]
- Vanaja, R.; Mukherjee, S. Novel Wrapper-Based Feature Selection for Efficient Clinical Decision Support System. Commun. Comput. Inf. Sci. 2018, 941, 113–129. [Google Scholar] [CrossRef]
- Rady, E.H.A.; Anwar, A.S. Prediction of Kidney Disease Stages Using Data Mining Algorithms. Inform. Med. Unlocked 2019, 15, 100178. [Google Scholar] [CrossRef]
- Senan, E.M.; Al-Adhaileh, M.H.; Alsaade, F.W.; Aldhyani, T.H.H.; Alqarni, A.A.; Alsharif, N.; Uddin, M.I.; Alahmadi, A.H.; Jadhav, M.E.; Alzahrani, M.Y. Diagnosis of Chronic Kidney Disease Using Effective Classification Algorithms and Recursive Feature Elimination Techniques. J. Healthc. Eng. 2021, 2021, 1004767. [Google Scholar] [CrossRef]
- Wickramasinghe, M.P.N.M.; Perera, D.M.; Kahandawaarachchi, K.A.D.C.P. Dietary prediction for patients with chronic kidney disease (CKD) by considering blood potassium level using machine learning algorithms. In Proceedings of the IEEE Lifesciences Conference—IEEE LSC 2018, Sydney, Australia, 13–15 December 2017; pp. 300–303. [Google Scholar] [CrossRef]
- Mitch, W.E.; Remuzzi, G. Diets for Patients with Chronic Kidney Disease, Should We Reconsider? BMC Nephrol. 2016, 17, 80. [Google Scholar] [CrossRef] [Green Version]
- Hayashi, Y.; Nakajima, K.; Nakajima, K. A Rule Extraction Approach to Explore the Upper Limit of Hemoglobin during Anemia Treatment in Patients with Predialysis Chronic Kidney Disease. Inform. Med. Unlocked 2019, 17, 100262. [Google Scholar] [CrossRef]
- Liu, K.; Xu, S.; Feng, N. A Radial Basis Probabilistic Process Neural Network Model and Corresponding Classification Algorithm. Appl. Intell. 2019, 49, 2256–2265. [Google Scholar] [CrossRef]
- Han, H.; Segal, A.M.; Seifter, J.L.; Dwyer, J.T. Nutritional Management of Kidney Stones (Nephrolithiasis). Clin. Nutr. Res. 2015, 4, 137. [Google Scholar] [CrossRef] [Green Version]
- Yarnell, J.; O’Reilly, D. Epidemiology and Disease Prevention, 2nd ed.; Oxford University Press: London, UK, 2013. [Google Scholar]
- Miernik, A.; Hein, S.; Wilhelm, K.; Schoenthaler, M. Harnsteindiagnostik—Was Bringt Uns Die Zukunft? Aktuelle Urol. 2017, 48, 127–131. [Google Scholar] [CrossRef] [PubMed]
- Große Hokamp, N.; Lennartz, S.; Salem, J.; Pinto dos Santos, D.; Heidenreich, A.; Maintz, D.; Haneder, S. Dose Independent Characterization of Renal Stones by Means of Dual Energy Computed Tomography and Machine Learning: An Ex-Vivo Study. Eur. Radiol. 2019, 30, 1397–1404. [Google Scholar] [CrossRef]
- De Perrot, T.; Hofmeister, J.; Burgermeister, S.; Martin, S.P.; Feutry, G.; Klein, J.; Montet, X. Differentiating Kidney Stones from Phleboliths in Unenhanced Low-Dose Computed Tomography Using Radiomics and Machine Learning. Eur. Radiol. 2019, 29, 4776–4782. [Google Scholar] [CrossRef]
- Aminsharifi, A.; Irani, D.; Pooyesh, S.; Parvin, H.; Dehghani, S.; Yousofi, K.; Fazel, E.; Zibaie, F. Artificial Neural Network System to Predict the Postoperative Outcome of Percutaneous Nephrolithotomy. J. Endourol. 2017, 31, 461–467. [Google Scholar] [CrossRef]
- Shabaniyan, T.; Parsaei, H.; Aminsharifi, A.; Movahedi, M.M.; Jahromi, A.T.; Pouyesh, S.; Parvin, H. An Artificial Intelligence-Based Clinical Decision Support System for Large Kidney Stone Treatment. Australas. Phys. Eng. Sci. Med. 2019, 42, 771–779. [Google Scholar] [CrossRef]
- Yang, S.W.; Hyon, Y.K.; Na, H.S.; Jin, L.; Lee, J.G.; Park, J.M.; Lee, J.Y.; Shin, J.H.; Lim, J.S.; Na, Y.G.; et al. Machine Learning Prediction of Stone-Free Success in Patients with Urinary Stone after Treatment of Shock Wave Lithotripsy. BMC Urol. 2020, 20, 88. [Google Scholar] [CrossRef]
- National Kidney Foundation. Understanding Glomerular Diseases. Available online: https://www.kidney.org/atoz/content/understanding-glomerular-diseases (accessed on 20 April 2022).
- Leung, R.K.K.; Wang, Y.; Ma, R.C.W.; Luk, A.O.Y.; Lam, V.; Ng, M.; So, W.Y.; Tsui, S.K.W.; Chan, J.C.N. Using a Multi-Staged Strategy Based on Machine Learning and Mathematical Modeling to Predict Genotype-Phenotype Risk Patterns in Diabetic Kidney Disease: A Prospective Case-Control Cohort Analysis. BMC Nephrol. 2013, 14, 162. [Google Scholar] [CrossRef]
- Dagliati, A.; Marini, S.; Sacchi, L.; Cogni, G.; Teliti, M.; Tibollo, V.; De Cata, P.; Chiovato, L.; Bellazzi, R. Machine Learning Methods to Predict Diabetes Complications. J. Diabetes Sci. Technol. 2018, 12, 295–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bennett, C.C. Artificial Intelligence for Diabetes Case Management: The Intersection of Physical and Mental Health. Inform. Med. Unlocked 2019, 16, 100191. [Google Scholar] [CrossRef]
- Schena, F.P.; Nistor, I. Epidemiology of IgA Nephropathy: A Global Perspective. Semin. Nephrol. 2018, 38, 435–442. [Google Scholar] [CrossRef] [PubMed]
- National Kidney Foundation. IgA Nephropathy. Available online: https://www.kidney.org/atoz/content/iganeph (accessed on 7 June 2022).
- Takahashi, K.; Kitamura, S.; Fukushima, K.; Sang, Y.; Tsuji, K.; Wada, J. The Resolution of Immunofluorescent Pathological Images Affects Diagnosis for Not Only Artificial Intelligence but Also Human. J. Nephropathol. 2021, 10, e26. [Google Scholar] [CrossRef]
- Schena, F.P.; Anelli, V.W.; Trotta, J.; Di Noia, T.; Manno, C.; Tripepi, G.; D’Arrigo, G.; Chesnaye, N.C.; Russo, M.L.; Stangou, M.; et al. Development and Testing of an Artificial Intelligence Tool for Predicting End-Stage Kidney Disease in Patients with Immunoglobulin A Nephropathy. Kidney Int. 2021, 99, 1179–1188. [Google Scholar] [CrossRef] [PubMed]
- Konieczny, A.; Stojanowski, J.; Krajewska, M.; Kusztal, M. Machine Learning in Prediction of Iga Nephropathy Outcome: A Comparative Approach. J. Pers. Med. 2021, 11, 312. [Google Scholar] [CrossRef] [PubMed]
- Agar, J.W.M.; Webb, G.I. Application of Machine Learning to a Renal Biopsy Database. Nephrol. Dial. Transplant. 1992, 7, 472–478. [Google Scholar] [CrossRef]
- Iakovidis, D.K.; Goudas, T.; Smailis, C.; Maglogiannis, I. Ratsnake: A Versatile Image Annotation Tool with Application to Computer-Aided Diagnosis. Sci. World J. 2014, 2014, 312. [Google Scholar] [CrossRef]
- Aldeman, N.L.S.; de Sá Urtiga Aita, K.M.; Machado, V.P.; da Mata Sousa, L.C.D.; Coelho, A.G.B.; da Silva, A.S.; da Silva Mendes, A.P.; de Oliveira Neres, F.J.; do Monte, S.J.H. Smartpathk: A Platform for Teaching Glomerulopathies Using Machine Learning. BMC Med. Educ. 2021, 21, 248. [Google Scholar] [CrossRef]
- Niel, O.; Bastard, P.; Boussard, C.; Hogan, J.; Kwon, T.; Deschênes, G. Artificial Intelligence Outperforms Experienced Nephrologists to Assess Dry Weight in Pediatric Patients on Chronic Hemodialysis. Pediatr. Nephrol. 2018, 33, 1799–1803. [Google Scholar] [CrossRef]
- Higgins, R.; Hathaway, M.; Lowe, D.; Lam, F.; Kashi, H.; Tan, L.C.; Imray, C.; Fletcher, S.; Zehnder, D.; Chen, K.; et al. Blood Levels of Donor-Specific Human Leukocyte Antigen Antibodies After Renal Transplantation: Resolution of Rejection in the Presence of Circulating Donor-Specific Antibody. Transplantation 2007, 84, 876–884. [Google Scholar] [CrossRef] [PubMed]
- Gloor, J.M.; Stegall, M.D. ABO Incompatible Kidney Transplantation. Curr. Opin. Nephrol. Hypertens. 2007, 16, 529–534. [Google Scholar] [CrossRef] [PubMed]
- Khovanova, N.; Daga, S.; Shaikhina, T.; Krishnan, N.; Jones, J.; Zehnder, D.; Mitchell, D.; Higgins, R.; Briggs, D.; Lowe, D. Subclass Analysis of Donor HLA-Specific IgG in Antibody-Incompatible Renal Transplantation Reveals a Significant Association of IgG4 with Rejection and Graft Failure. Transpl. Int. 2015, 28, 1405–1415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greco, R.; Papalia, T.; Lofaro, D.; Maestripieri, S.; Mancuso, D.; Bonofiglio, R. Decisional Trees in Renal Transplant Follow-Up. Transplant. Proc. 2010, 42, 1134–1136. [Google Scholar] [CrossRef]
- Brown, T.S.; Elster, E.A.; Stevens, K.; Graybill, J.C.; Gillern, S.; Phinney, S.; Salifu, M.O.; Jindal, R.M. Bayesian Modeling of Pretransplant Variables Accurately Predicts Kidney Graft Survival. Am. J. Nephrol. 2012, 36, 561–569. [Google Scholar] [CrossRef]
- Topuz, K.; Zengul, F.D.; Dag, A.; Almehmi, A.; Yildirim, M.B. Predicting Graft Survival among Kidney Transplant Recipients: A Bayesian Decision Support Model. Decis. Support Syst. 2017, 106, 97–109. [Google Scholar] [CrossRef]
- Shaikhina, T.; Lowe, D.; Daga, S.; Briggs, D.; Higgins, R.; Khovanova, N. Decision Tree and Random Forest Models for Outcome Prediction in Antibody Incompatible Kidney Transplantation. Biomed. Signal Process. Control 2017, 52, 456–462. [Google Scholar] [CrossRef]
- Elihimas Júnior, U.F.; Couto, J.P.; Pereira, W.; Barros De Oliveira Sá, M.P.; Tenório De França, E.E.; Aguiar, F.C.; Cabral, D.B.C.; Alencar, S.B.V.; Feitosa, S.J.D.C.; Claizoni Dos Santos, T.O.; et al. Logistic Regression Model in a Machine Learning Application to Predict Elderly Kidney Transplant Recipients with Worse Renal Function One Year after Kidney Transplant: Elderly KTbot. J. Aging Res. 2020, 2020, 118–128. [Google Scholar] [CrossRef]
- Shih, D.T.; Kim, S.B.; Chen, V.C.P.; Rosenberger, J.M.; Pilla, V.L. Efficient Computer Experiment-Based Optimization through Variable Selection. Ann. Oper. Res. 2014, 216, 287–305. [Google Scholar] [CrossRef]
- Martínez-Martínez, J.M.; Escandell-Montero, P.; Barbieri, C.; Soria-Olivas, E.; Mari, F.; Martínez-Sober, M.; Amato, C.; Serrano López, A.J.; Bassi, M.; Magdalena-Benedito, R.; et al. Prediction of the Hemoglobin Level in Hemodialysis Patients Using Machine Learning Techniques. Comput. Methods Programs Biomed. 2014, 117, 208–217. [Google Scholar] [CrossRef]
- Stopper, A.; Amato, C.; Gioberge, S.; Giordana, G.; Marcelli, D.; Gatti, E. Managing Complexity at Dialysis Service Centers across Europe. Blood Purif. 2007, 25, 77–89. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Jia, Z.; Zeng, X.; Feng, C.; Lu, X.; Duan, H.; Li, H. Renal Biopsy Recommendation Based on Text Understanding. Stud. Health Technol. Inform. 2019, 264, 689–693. [Google Scholar] [CrossRef] [PubMed]
- Kanda, E.; Epureanu, B.I.; Adachi, T.; Tsuruta, Y.; Kikuchi, K.; Kashihara, N.; Abe, M.; Masakane, I.; Nitta, K. Application of Explainable Ensemble Artificial Intelligence Model to Categorization of Hemodialysis-Patient and Treatment Using Nationwide-Real-World Data in Japan. PLoS ONE 2020, 15, e0233491. [Google Scholar] [CrossRef] [PubMed]
- Aalamifar, F.; Rivaz, H.; Cerrolaza, J.J.; Jago, J.; Safdar, N.; Boctor, E.M.; Linguraru, M.G. Classification of Kidney and Liver Tissue Using Ultrasound Backscatter Data. Med. Imaging 2015 Ultrason. Imaging Tomogr. 2015, 9419, 192–199. [Google Scholar] [CrossRef]
- Singh, A.; Nadkarni, G.; Gottesman, O.; Ellis, S.B.; Bottinger, E.P.; Guttag, J.V. Incorporating Temporal EHR Data in Predictive Models for Risk Stratification of Renal Function Deterioration. J. Biomed. Inform. 2015, 53, 220–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, K.; Vendt, B.; Smith, K.; Freymann, J.; Kirby, J.; Koppel, P.; Moore, S.; Phillips, S.; Maffitt, D.; Pringle, M.; et al. The Cancer Imaging Archive (TCIA): Maintaining and Operating a Public Information Repository. J. Digit. Imaging 2013, 26, 1045–1057. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.C.; Fitzgerald, J.M. Evaluation of Incidental Renal and Adrenal Masses. Am. Fam. Physician 2001, 63, 288–294, 299. [Google Scholar]
- Martin-Isla, C.; Campello, V.M.; Izquierdo, C.; Raisi-Estabragh, Z.; Baeßler, B.; Petersen, S.E.; Lekadir, K. Image-Based Cardiac Diagnosis With Machine Learning: A Review. Front. Cardiovasc. Med. 2020, 7, 1. [Google Scholar] [CrossRef] [Green Version]
- Ng, F.; Kozarski, R.; Ganeshan, B.; Goh, V. Assessment of Tumor Heterogeneity by CT Texture Analysis: Can the Largest Cross-Sectional Area Be Used as an Alternative to Whole Tumor Analysis? Eur. J. Radiol. 2013, 82, 342–348. [Google Scholar] [CrossRef]
- Starmans, M.P.A.; van der Voort, S.R.; Castillo Tovar, J.M.; Veenland, J.F.; Klein, S.; Niessen, W.J. Radiomics. In Handbook of Medical Image Computing and Computer Assisted Intervention; Zhou, S.K., Rueckert, D., Fichtinger, G., Eds.; Elsevier: Amsterdam, The Netherlands, 2020; pp. 429–456. ISBN 978-0-12-816176-0. [Google Scholar]
- Raschka, S. Model Evaluation, Model Selection, and Algorithm Selection in Machine Learning. arXiv 2018, arXiv:1811.12808. [Google Scholar] [CrossRef]
- Alnazer, I.; Bourdon, P.; Urruty, T.; Falou, O.; Khalil, M.; Shahin, A.; Fernandez-Maloigne, C. Recent Advances in Medical Image Processing for the Evaluation of Chronic Kidney Disease. Med. Image Anal. 2021, 69, 101960. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute. Computed Tomography (CT) Scans and Cancer Fact Sheet. Available online: https://www.cancer.gov/about-cancer/diagnosis-staging/ct-scans-fact-sheet (accessed on 7 April 2022).
- Khan, S.R.; Pearle, M.S.; Robertson, W.G.; Gambaro, G.; Canales, B.K.; Doizi, S.; Traxer, O.; Tiselius, H.-G. Kidney Stones. Nat. Rev. Dis. Prim. 2016, 2, 16008. [Google Scholar] [CrossRef] [PubMed]
- Burlacu, A.; Iftene, A.; Jugrin, D.; Popa, I.V.; Lupu, P.M.; Vlad, C.; Covic, A. Using Artificial Intelligence Resources in Dialysis and Kidney Transplant Patients: A Literature Review. Biomed Res. Int. 2020, 2020, 9867872. [Google Scholar] [CrossRef] [PubMed]
- Thishya, K.; Vattam, K.K.; Naushad, S.M.; Raju, S.B.; Kutala, V.K. Artificial Neural Network Model for Predicting the Bioavailability of Tacrolimus in Patients with Renal Transplantation. PLoS ONE 2018, 13, e0191921. [Google Scholar] [CrossRef] [Green Version]
- Stachowska, E.; Gutowska, I.; Strzelczak, A.; Wesołowska, T.; Safranow, K.; Chlubek, D. The Use of Neural Networks in Evaluation of the Direction and Dynamics of Changes in Lipid Parameters in Kidney Transplant Patients on the Mediterranean Diet. J. Ren. Nutr. 2006, 16, 150–159. [Google Scholar] [CrossRef] [PubMed]
- Baigent, C.; Herrington, W.G.; Coresh, J.; Landray, M.J.; Levin, A.; Perkovic, V.; Pfeffer, M.A.; Rossing, P.; Walsh, M.; Wanner, C.; et al. Challenges in Conducting Clinical Trials in Nephrology: Conclusions from a Kidney Disease—Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int. 2017, 92, 297–305. [Google Scholar] [CrossRef] [Green Version]
- Ghassemi, M.; Naumann, T.; Schulam, P.; Beam, A.L.; Chen, I.Y.; Ranganath, R. A Review of Challenges and Opportunities in Machine Learning for Health. AMIA Jt. Summits Transl. Sci. Proc. 2020, 2020, 191–200. [Google Scholar]
- Yuan, Q.; Zhang, H.; Deng, T.; Tang, S.; Yuan, X.; Tang, W.; Xie, Y.; Ge, H.; Wang, X.; Zhou, Q.; et al. Role of Artificial Intelligence in Kidney Disease. Int. J. Med. Sci. 2020, 17, 970–984. [Google Scholar] [CrossRef] [Green Version]
- Gameiro, J.; Branco, T.; Lopes, J.A. Artificial Intelligence in Acute Kidney Injury Risk Prediction. J. Clin. Med. 2020, 9, 678. [Google Scholar] [CrossRef] [Green Version]
- Shortliffe, E.H.; Sepúlveda, M.J. Clinical Decision Support in the Era of Artificial Intelligence. JAMA 2018, 320, 2199. [Google Scholar] [CrossRef]
- Obermeyer, Z.; Lee, T.H. Lost in Thought—The Limits of the Human Mind and the Future of Medicine. N. Engl. J. Med. 2017, 377, 1209–1211. [Google Scholar] [CrossRef] [Green Version]
- Gampala, S.; Vankeshwaram, V.; Gadula, S.S.P. Is Artificial Intelligence the New Friend for Radiologists? A Review Article. Cureus 2020, 12, e11137. [Google Scholar] [CrossRef] [PubMed]
- Mistry, N.S.; Koyner, J.L. Artificial Intelligence in Acute Kidney Injury: From Static to Dynamic Models. Adv. Chronic Kidney Dis. 2021, 28, 74–82. [Google Scholar] [CrossRef] [PubMed]
- Chipidza, F.E.; Wallwork, R.S.; Stern, T.A. Impact of the Doctor-Patient Relationship. Prim. Care Companion CNS Disord. 2015, 17, 27354. [Google Scholar] [CrossRef] [Green Version]
- Neri, E.; Coppola, F.; Miele, V.; Bibbolino, C.; Grassi, R. Artificial Intelligence: Who Is Responsible for the Diagnosis? Radiol. Med. 2020, 125, 517–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
| Paper | Objective | Method | Database | Results | Year |
|---|---|---|---|---|---|
| [27] | Malignant renal cyst prediction | Bayesian classifier | [27] | AUC 0.96 | 2009 |
| [28] | Identify malignant renal masses | Statistical relational learning—RFGB: relational functional gradient boosting | [28] | Accuracy 82% | 2018 |
| [29] | Differentiate between malignant and benign masses | CT texture analysis with random forest | [29] | Accuracy 90.5% AUC 0.915 | 2020 |
| [30] | Diagnose ccRCC | WEKA with and without SMOTE | [41] | AUC contour-focused 0.865–0.984 AUC margin shrinkage 0.745–0.887 | 2019 |
| [31] | Diagnose ccRCC | Pyradiomics and random forest | [41] | Accuracy 84.6% Sensitivity 90.4% Specificity 78.8% Precision 81% | 2020 |
| [32] | Diagnose ccRCC | Radiomics and CatBoost | [32,41] | MR accuracy 73% internal 74% external CT accuracy 79% internal 69% external | 2020 |
| [33] | Diagnose ccRCC | MaZda and WEKA toolkit | [33] | Accuracy 85.1% | 2018 |
| [34] | Diagnose ccRCC | Proteomics-based random forest and imaging-based VGG16 | [41] | Proteomics accuracy 98% image accuracy 83% validation, 95% testing set | 2019 |
| [35] | Differentiate between kidney chromophobe renal cell carcinoma and oncocytoma | Linear SVM | [35] | Accuracy 80% | 2016 |
| [36] | Classify papillary renal cell carcinoma stages | Feature extraction and random forest | [42,43] | Accuracy 88.5% | 2018 |
| [38] | Kidney and tumor segmentation | 3D U-Net | [44] | Mean Kidney Tumor Dice 0.9168 | 2019 |
| [39] | Kidney and tumor segmentation | Cascade 3D U-Net | [44] | Mean Kidney Tumor Dice 0.9064 | 2019 |
| [40] | Kidney and tumor segmentation | Multi-resolution 3D V-Net | [44] | Mean Kidney Tumor Dice 0.8815 | 2019 |
| Paper | Objective | Method | Database | Results | Year |
|---|---|---|---|---|---|
| [45] | Predict AKI in adult and children | Boruta [56] (selection algorithm) + random forest | [57,58] | AUC 0.796 | 2018 |
| [46] | Predict AKI in adult and children | Gradient boosted machine | [59] | AUC 0.85 | 2021 |
| [47] | Predict AKI | Gradient boosted machine | [47] | AUC 0.76 | 2021 |
| [48] | Predict AKI in burn patients | K-NN | [48] | Accuracy 97% | 2019 |
| [50] | Predict AKI | Lasso + logistic regression | [60] | AUC 0.79 AUC 0.82 [p < 0.001] | 2019 |
| [51] | Predict AKI | RF + XGboost | [51] | AUC 0.843 | 2020 |
| [53] | Predict AKI | Streams | [53] | Accuracy 56% in 48 h Accuracy 84% in 30 d Accuracy 90% in 90 d | 2019 |
| [54] | Prediction of AKI from blood test | Feature selection + random forest | [54] | AUC 0.881 in 30 d | 2021 |
| [55] | Predict AKI | Gradient boosting tree-based machines | [61] | AUC 76% in 48 h AUC 81% stage 2 AUC 87% stage 3 | 2020 |
| Paper | Objective | Method | Database | Results | Year |
|---|---|---|---|---|---|
| [26] | Diagnose CKD based on patient stage | Support vector machine—SVM | [26] | Accuracy 82% on 2 stages Accuracy 67.21% on 3 stages Accuracy 51% on 5 stages | 2014 |
| [65] | CKD diagnosis | Random forest | [64] | Accuracy 99.3% | 2016 |
| [66] | CKD diagnosis | Decision tree C4.5 | [64] | Accuracy 63% | 2016 |
| [67] | CKD diagnosis | SVM | [64] | Accuracy 98.3% | 2016 |
| [68] | CKD diagnosis | k-NN with CFS and AdaBoost | [64] | Accuracy 98.1% | 2017 |
| [69] | CKD diagnosis | Random forest | [64] | Accuracy 100% | 2017 |
| [70] | CKD diagnosis | RPART | [64] | AUC 0.995 Sensitivity 0.9897 Specificity 1 | 2018 |
| [71] | CKD diagnosis | PSODP + DL-RNN | [64] | Accuracy 99.5% | 2018 |
| [72] | CKD diagnosis | PNN [77] | [64] | Accuracy 96.7% | 2019 |
| [73] | CKD diagnosis | RFE and Random Forest | [64] | F1 score 100% | 2021 |
| [74] | Predict diet plan for CKD patients | Multiclass Decision forest | [64] | Accuracy 99.17% | 2017 |
| [76] | Predict hemoglobin levels in CKD patients | Extraction rule—Re-RX + J48graft | [64] | Accuracy 95.18% | 2019 |
| Paper | Objective | Method | Database | Results | Year |
|---|---|---|---|---|---|
| [81] | Renal stone detection | Segmentation + ANN | [81] | Accuracy 86% | 2019 |
| [82] | Renal stones vs. phleboliths | Radiomics + AdaBoost classifier | [82] | Accuracy 85.1% | 2019 |
| [83] | Kidney stone removal, prediction of postoperative variables | ANN | [83] | Accuracy 81–98.2% | 2017 |
| [84] | Predict stone-free status after the first treatment | Feature extraction + sequential forward selection + multiple classifier scheme | [84] | Accuracy 60% | 2019 |
| [85] | Stone-free prediction | Light gradient boosting method | [85] | Accuracy 87.9% | 2020 |
| Paper | Objective | Method | Database | Results | Year |
|---|---|---|---|---|---|
| [87] | Predict diabetic kidney disease | SVM radial | [87] | Accuracy 94% | 2013 |
| [88] | Predict diabetic kidney disease | Unbalanced random forest | [88] | Accuracy 83.8% | 2018 |
| [89] | Predict diabetic kidney disease | Knime + WEKA | [89] | Accuracy 83.5% | 2019 |
| [92] | Resolution image-based renal pathology | Convolutional neural network | [92] | Accuracy > 80% | 2021 |
| [93] | Predict ESKD in patients with IgAN | ANN | [93] | AUC 0.82 with 5-year follow-up AUC 0.89 with 10-year follow-up | 2021 |
| [94] | Predict deterioration of kidney function in IgAN patients | SVM | [94] | Accuracy 79.8% | 2021 |
| [95] | Diagnose glomerular disease | Disjunctive least generalization—DLG algorithm | [95] | Accuracy 81.26–96.5% | 1992 |
| [96] | Detect pathogenic and non-pathogenic glomerulus and tubulus | RatSnake—ML automatic segmentation | [96] | Accuracy 94.7% | 2014 |
| [97] | Diagnose glomerular disease | Decision tree with J48 algorithm | [97] | Accuracy 89.47% | 2021 |
| [98] | Predict weight of children in renal dialysis | ANN | [98] | Mean difference 0.497 | 2018 |
| Paper | Objective | Method | Database | Results | Year |
|---|---|---|---|---|---|
| [102] | Predict transplant failure probability | Decision tree | [102] | Specificity 73.8% Sensitivity 88.2% | 2010 |
| [103] | Predict post- transplant survivability | Bayesian belief network | [103] | Accuracy 52% after 1 year Accuracy 56% after 3 years | 2012 |
| [104] | Classify risk levels for kidney graft survival after transplant | ElasticNet + Bayesian belief network | [107] | Accuracy 68.4% | 2018 |
| [105] | Predict early transplant rejection | Decision tree and random forest | [105] | Accuracy 85% | 2019 |
| [106] | Predict kidney transplantation compatibility Predict renal function worsening 1 year after transplant | Elderly KTbot | [106] | Precision 90% Sensitivity 71% F1 score 0.79 | 2020 |
| Paper | Objective | Method | Database | Results | Year |
|---|---|---|---|---|---|
| [108] | Predict hemoglobin in patients with kidney disfunction | Data merging + clustering + ensemble of classifiers | [108] | Mean absolute error 0.662—Italy, mean absolute error 0.673—Spain | 2014 |
| [110] | Recommend renal biopsy | Tokenization + NLP machine learning classifier | [110] | Accuracy 83.5% Precision 80.6% | 2019 |
| [111] | Prediction of 1-year survival in hemodialysis patients | Ensemble artificial intelligence model | [111] | Accuracy 94.8% | 2020 |
| [112] | Detect kidney and liver tissue for hydronephrosis patient | Homodyne-K feature extraction + random forest | [112] | Accuracy 94% | 2015 |
| [113] | Predict risk stratification of renal function deterioration based on eGFR threshold | Multitask temporal-based classifier | [113] | Specificity 0.828 with 10% threshold Specificity 0.786 with 20% threshold | 2015 |
| Database | Number of Patients | Description | Year (First Use/Published) | Open Access |
|---|---|---|---|---|
| [27] | 93 | Patients’ MDCT. Patients with complicated cysts: cyst with at least one focus of septa, a solid nodule, and any calcification or wall thickening on MDCT | 2009 | No |
| [28] | 150 | Patients’ CT. 100 malignant tumors: 70 clear cell renal cell carcinoma (ccRCC), 20 papillary renal cell carcinoma (pRCC), and 10 chromophobe renal cell carcinoma (chRCC); 50 benign tumors: 20 lipid-poor angiomyolipoma (lpAML), 30 renal oncocytoma | 2018 | No |
| [29] | 79 | 84 renal masses: 63 malignant (25 clear cell RCC, 23 papillary cell RCC, 15 chromophobe RCC), 21 benign (10 oncocytomas, 11 fat-poor angiomyolipomas) | 2020 | No |
| [32] | 440 | 440 MRI and CT of patients with ccRCC | 2020 | No |
| [33] | 54 | Patients’ CT. All patients have ccRCC. | 2019 | No |
| [41] | 216 | 216 proteomics data and 783 slide images (524 tumoral) | 2018 | Yes |
| [44] | 300 | CT of patients with one or more kidney tumors. Segmentation of kidneys and tumors. | 2019 | Yes |
| [26] | 188 | The database is composed of 40, 16, 38, 60, 28, and 6 entries for healthy, stage 1, 2, 3, 4, 5, respectively. These images are obtained from 35 observers taken at different times. The kidney ultrasonic images are segmented and annotated into three regions of interest (ROIs) | 2014 | No |
| [81] | 200 | 200 kidney stones harvested from nondestructive stone extraction at three different sites. Stone size was measured using a digital caliper | 2020 | No |
| [82] | 412 | LDCT of 235 kidney stones and 224 phleboliths | 2019 | No |
| [83] | 254 | Preoperative abdominopelvic ultrasound and intravenous urography or CT scan of PCNL patients. | 2017 | No |
| [112] | 9 | This dataset contains the 3D US abdominal images from 9 pediatric patients with hydronephrosis | 2015 | No |
| [96] | 1321 | Biopsy images of pathogenic (338) and nonpathogenic (396) glomerulus and some of pathogenic (338) and nonpathogenic (248) tubulus | 2014 | No |
| [97] | 584 | Renal biopsy reports, each of 4 or 5 slides with different stains, for each case: clinical and laboratory data, diagnostic hypothesis, histological biopsy study, histological report of glomerular disease | 2021 | No |
| [92] | 422 | Renal immunofluorescent images obtained by fluorescence microscopes relative to a renal biopsy of 162 patients with IgAN and 260 without | 2021 | No |
| [35] | 24 | 24 unstained deparaffinized formalin-fixed kidney tissue sections of chRCC and oncocytoma, 12 of each type | 2016 | No |
| Database | Number of Patients | Description | Year (First Use/Published) | Open Access |
|---|---|---|---|---|
| [42] | 260 | Tumor RNASeq and pathological stage (I, II, III, and IV): Stage I—172, Stage II—22, Stage III—51, and Stage IV—15. | 2010 | Yes |
| [43] | 34 | This dataset was obtained using Affymetrix HGU133 Plus 2.0 array platform and includes 19 and 15 samples in early (excellent survival) and late (poor survival) stages of PRCC. | 2005 | Yes |
| [57] | 269,999 | 6.1% of patients in the dataset had a clinical deterioration event: 424 cardiac arrests, 13,188 intensive care unit (ICU) transfers, and 2840 deaths on the wards. For each patient, there are a total of 29 features. | 2014 | No |
| [59] | 108,441 | Australian and New Zealand Society of Cardiac and Thoracic Surgeons Database registry recorded 110,342 cardiac surgery events in 108,441 unique patients. | 2018 | No |
| [47] | 780 | Medical data collected by natural language process module from EMRs including demographic data, daily documentation, laboratory and imaging results, anesthesia records, medications, interventions, and diagnosis. TRIPOD guidelines were followed. | 2021 | No |
| [48] | 50 | Serial creatinine testing of patients with ≥20% total body surface area (TBSA) burns at risk for AKI. AKI was defined using the Kidney Disease: Improving Global Outcomes (KDIGO) criteria. | 2019 | No |
| [61] | 153,821 | 153,821 patients from 6 different sites. Each patient had a mean of 67 (SD = 46) clinical facts per day. | 2020 | No (only in USA) |
| [51] | 671 | Information related to demographic characteristics, clinical condition, preoperative biochemistry data, preoperative medication, and intraoperative time-series hemodynamic features (systolic blood pressure (SBP), diastolic blood pressure (DBP), mean arterial blood pressure (MAP), and heart rate (HR)) from electronic medical records and records on intraoperative variables. | 2020 | No |
| [54] | 51,869 | 618,719 blood test occurrences for 51,869 distinct patients. | 2021 | No |
| [64] | 400 | The CKD dataset was collected from 400 patients from the University of California, Irvine Machine Learning Repository. | 2015 | Yes |
| [84] | 254 | This dataset includes information on preoperative, intraoperative, and postoperative parameters from 254 patients who underwent kidney surgery. | 2019 | No |
| [93] | 1015 | The variables contained per IgAN patient are age, sex, hypertension, serum creatinine, daily proteinuria, kidney biopsy, therapy—RASBs or corticosteroids. The primary outcome is ESRD, dialysis, or transplantation. | 2020 | No |
| [94] | 80 | Features of 80 IgAN patients: secondary IgA deposition, eGFR, MEST-C scores. | 2021 | No |
| [95] | 284 | 38 features for each patient and biopsy diagnosis. | 1992 | No |
| [102] | 194 | Features for each patient: age, sex, time in dialysis, donor type, donor age, HLA mismatches, delayed graft function, acute rejection episode, and chronic allograft nephropathy. | 2010 | No |
| [103] | 7348 | A total of 793 pre- and post-transplant variables per patient. | 2004 | No (only in USA) |
| [58] | 6564 | First 12 h of 6564 HER from critically ill children admitted to a pediatric ICU without evidence of AKI; 4% of the patients developed AKI by 72 h. | 2016 | No |
| [53] | 2642 | The dataset contains the data relative to 1781 patients pre-implementation and 861 patients post-implementation of a digital intervention system, with the relative alert severity. | 2019 | No |
| [85] | 358 | This dataset includes 42 features including the two target variables, stone-free and one-session success, for all 358 cases. The number of cases with stone-free and one-session success was 253 (70.7%) and 154 (43.0%). | 2020 | No |
| [60] | 1250 | Several serum markers per patient undergoing angiography as clinical standard care. | 2015 | No (only in USA) |
| [105] | 80 | 80 patients who received HLA-incompatible renal allografts; 14 features measured before transplantation. | 2019 | No |
| [106] | 118 | Medical records of 18 elderly and 100 younger patients. | 2020 | No |
| [87] | 1386 | Anthropometric measurements and blood pressure (BP), drug use and past medical history, physical assessment for retinopathy, sensory neuropathy, and peripheral arterial disease. eGFR calculated using the Chinese-modified Modification of Diet in Renal Disease equation. | 2013 | No |
| [88] | 1000 | 1000 T2DM patients’ data collected by the IRCCS (Istituto di Ricovero e Cura a Carattere Scientifico) of the Hospital of Pavia. | 2018 | No |
| [89] | ~32,000 | Diabetes of type 2 patients with a 24-month analysis window. | 2019 | No |
| [110] | 3149 | This dataset contains a total of 3149 admission notes from the nephrology department. For the ground truth, there are recommendations given by physicians in first-day progress notes. | 2019 | No |
| [113] | 6435 | Electronic health records of patients with hypertension, diabetes, or both. | 2015 | No |
| [107] | ~31,000 | United Network for Organ Sharing, a private, non-profit (UNOS) dataset including information on all kidney waiting-list registrations and transplants that had been recorded in the U.S. | 2014 | No (only in USA) |
| [108] | 13,011 | 125 features from dialysis clinical practice of 13,011 patients. | 2014 | No |
| [98] | 14 | ESRD patients on chronic hemodialysis or hemodiafiltration weighing 20 kg or more. | 2018 | No |
| [111] | 79,860 | Various features for each patient are presented with the relative risk score based on mass, serum albumin level, cholesterol level, and creatinine. | 2020 | No |
| Method—ML Algorithm (Based) | Authors | Year |
|---|---|---|
| Bayesian classifier | [27] | 2009 |
| [103] | 2012 | |
| [104] | 2018 | |
| Logistic regression | [50] | 2019 |
| [106] | 2020 | |
| Decision tree | [66] | 2016 |
| [97] | 2021 | |
| [102] | 2010 | |
| Random forest | [112] | 2015 |
| [65] | 2016 | |
| [69] | 2017 | |
| [45] | 2018 | |
| [36] | 2018 | |
| [34] | 2019 | |
| [105] | 2019 | |
| [29] | 2020 | |
| [31] | 2020 | |
| [73] | 2021 | |
| [54] | 2021 | |
| [88] | 2018 | |
| SVM | [87] | 2013 |
| [26] | 2014 | |
| [35] | 2016 | |
| [67] | 2016 | |
| [94] | 2021 | |
| ANN | [81] | 2019 |
| [83] | 2017 | |
| [98] | 2018 | |
| [93] | 2021 | |
| Ensemble of classifiers | [84] | 2019 |
| [111] | 2020 | |
| [108] | 2014 | |
| [68] | 2017 | |
| [48] | 2019 | |
| [82] | 2019 | |
| [76] | 2019 | |
| [33] | 2018 | |
| [89] | 2019 | |
| [30] | 2019 | |
| [28] | 2018 | |
| [46] | 2021 | |
| [47] | 2021 | |
| [55] | 2020 | |
| [85] | 2020 | |
| [51] | 2020 | |
| [32] | 2020 | |
| DNN | [96] | 2014 |
| [113] | 2015 | |
| [110] | 2019 | |
| [53] | 2020 | |
| [95] | 1992 | |
| [70] | 2018 | |
| [71] | 2018 | |
| [72] | 2019 | |
| [34] | 2019 | |
| [92] | 2021 | |
| [38] | 2019 | |
| [39] | 2019 | |
| [40] | 2019 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Magherini, R.; Mussi, E.; Volpe, Y.; Furferi, R.; Buonamici, F.; Servi, M. Machine Learning for Renal Pathologies: An Updated Survey. Sensors 2022, 22, 4989. https://doi.org/10.3390/s22134989
Magherini R, Mussi E, Volpe Y, Furferi R, Buonamici F, Servi M. Machine Learning for Renal Pathologies: An Updated Survey. Sensors. 2022; 22(13):4989. https://doi.org/10.3390/s22134989
Chicago/Turabian StyleMagherini, Roberto, Elisa Mussi, Yary Volpe, Rocco Furferi, Francesco Buonamici, and Michaela Servi. 2022. "Machine Learning for Renal Pathologies: An Updated Survey" Sensors 22, no. 13: 4989. https://doi.org/10.3390/s22134989
APA StyleMagherini, R., Mussi, E., Volpe, Y., Furferi, R., Buonamici, F., & Servi, M. (2022). Machine Learning for Renal Pathologies: An Updated Survey. Sensors, 22(13), 4989. https://doi.org/10.3390/s22134989