
Does Gait with an Ankle Foot Orthosis Improve or Compromise Minimum Foot Clearance?

 , , , ,
, , , ,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
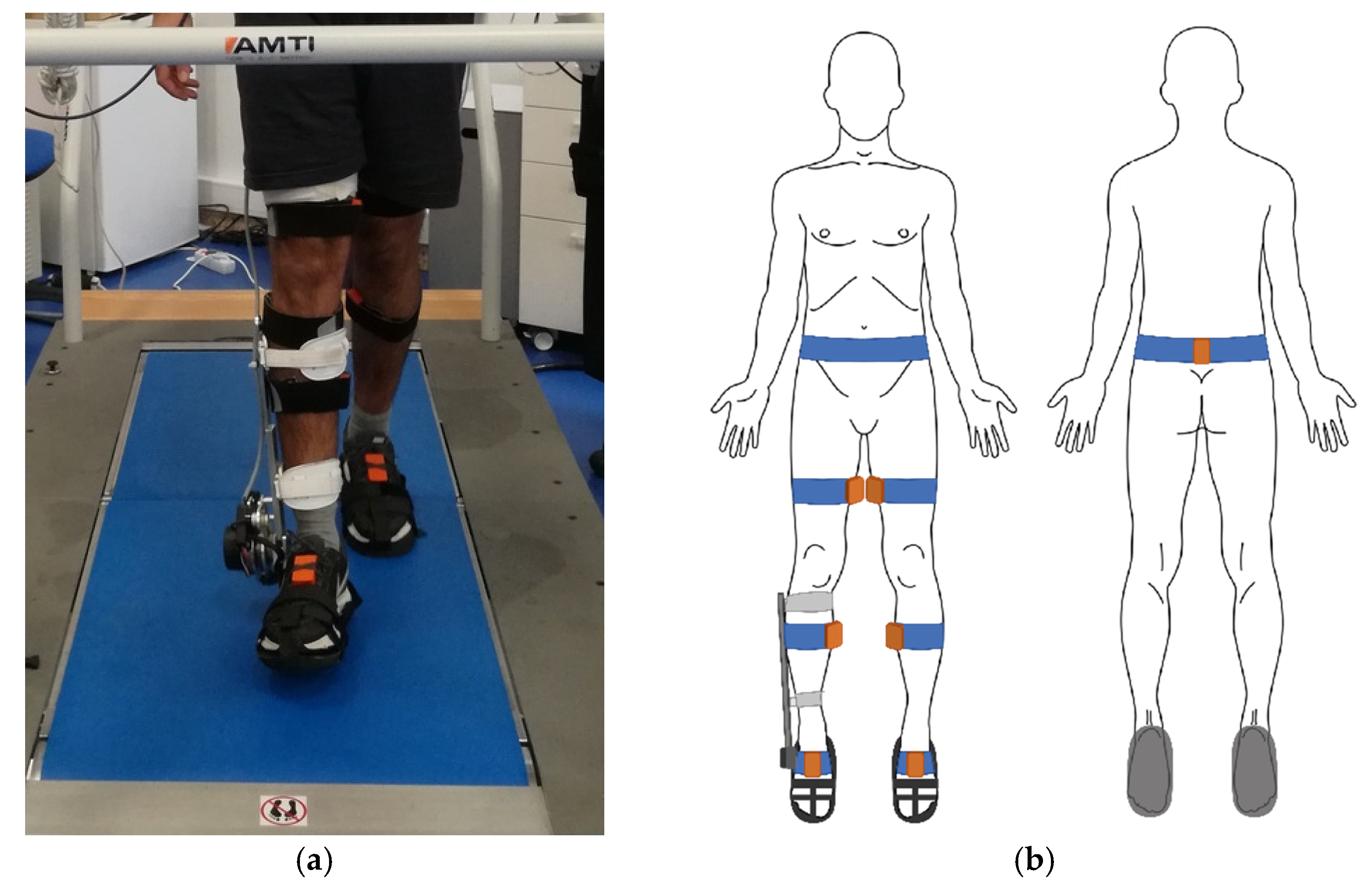
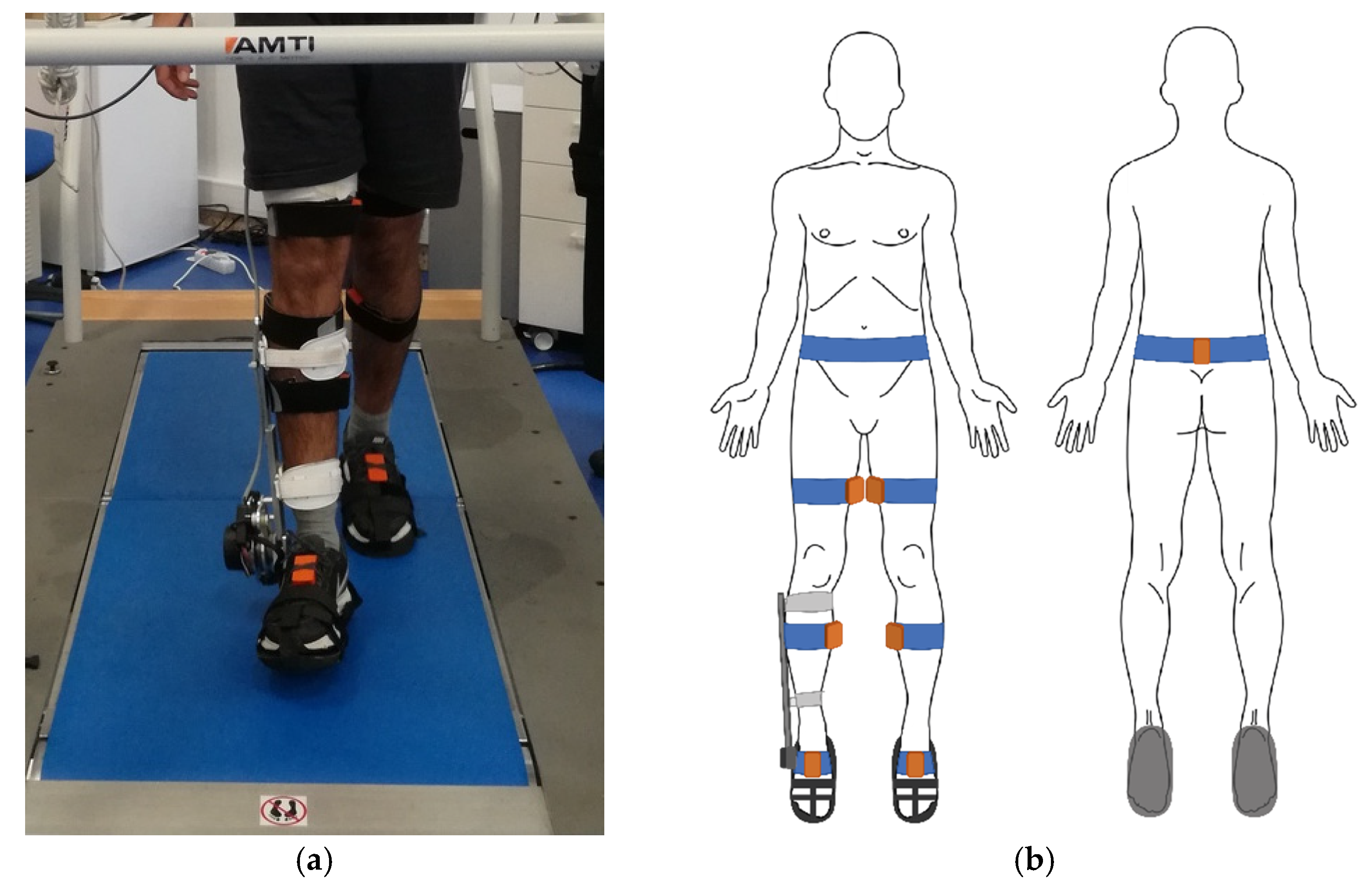
2.2. Experimental Setup
2.3. Data Analysis
2.4. Statistical Procedures
3. Results
3.1. Minimum Foot Clearance
3.2. Gait Linear Kinematic Parameters
3.3. Joint Kinematic Parameters
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alcock, L.; Vanicek, N.; O’Brien, T.D. Alterations in gait speed and age do not fully explain the changes in gait mechanics associated with healthy older women. Gait Posture 2013, 37, 586–592. [Google Scholar] [CrossRef]
- McGrath, D.; Greene, B.R.; Walsh, C.; Caulfield, B. Estimation of minimum ground clearance (MGC) using body-worn inertial sensors. J. Biomech. 2011, 44, 1083–1088. [Google Scholar] [CrossRef]
- Bonifácio, D.; Richards, J.; Selfe, J.; Curran, S.; Trede, R. Influence and benefits of foot orthoses on kinematics, kinetics and muscle activation during step descent task. Gait Posture 2018, 65, 106–111. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. World Health Organization Global Report on Falls Prevention in Older Age; WHO Press: Geneva, Switzerland, 2007. [Google Scholar]
- Berg, W.P.; Alessio, H.M.; Mills, E.M.; Tong, C. Circumstances and consequences of falls in independent community-dwelling older adults. Age Ageing 1997, 26, 261–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blake, A.J.; Morgan, K.; Bendall, M.J.; Dallosso, H.; Ebrahim, S.B.; Arie, T.H.; Fentem, P.H.; Bassey, E.J. Falls by elderly people at home: Prevalence and associated factors. Age Ageing 1988, 17, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Barrett, R.S.; Mills, P.M.; Begg, R.K. A systematic review of the effect of ageing and falls history on minimum foot clearance characteristics during level walking. Gait Posture 2010, 32, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Winter, D.A. Foot trajectory in human gait: A precise and multifactorial motor control task. Phys. Ther. 1992, 72, 45–53; discussion 54–56. [Google Scholar] [CrossRef]
- Nagano, H.; Sparrow, W.A.; Begg, R.K. Can toe-ground footwear margin alter swing-foot ground clearance? Gait Posture 2015, 42, 214–217. [Google Scholar] [CrossRef] [PubMed]
- Tyson, S.F.; Sadeghi-Demneh, E.; Nester, C.J. A systematic review and meta-analysis of the effect of an ankle-foot orthosis on gait biomechanics after stroke. Clin. Rehabil. 2013, 27, 879–891. [Google Scholar] [CrossRef]
- Burdett, R.G.; Borello-France, D.; Blatchly, C.; Potter, C. Gait comparison of subjects with hemiplegia walking unbraced, with ankle-foot orthosis, and with Air-Stirrup brace. Phys. Ther. 1988, 68, 1197–1203. [Google Scholar]
- Yamamoto, S.; Fuchi, M.; Yasui, T. Change of rocker function in the gait of stroke patients using an ankle foot orthosis with an oil damper: Immediate changes and the short-term effects. Prosthet. Orthot. Int. 2011, 35, 350–359. [Google Scholar] [CrossRef] [Green Version]
- Pongpipatpaiboon, K.; Mukaino, M.; Matsuda, F.; Ohtsuka, K.; Tanikawa, H.; Yamada, J.; Tsuchiyama, K.; Saitoh, E. The impact of ankle–foot orthoses on toe clearance strategy in hemiparetic gait: A cross-sectional study. J. NeuroEng. Rehabil. 2018, 15, 41. [Google Scholar] [CrossRef]
- Matsuda, F.; Mukaino, M.; Ohtsuka, K.; Tanikawa, H.; Tsuchiyama, K.; Teranishi, T.; Kanada, Y.; Kagaya, H.; Saitoh, E. Biomechanical factors behind toe clearance during the swing phase in hemiparetic patients. Top. Stroke Rehabil. 2017, 24, 177–182. [Google Scholar] [CrossRef]
- Greene, P.J.; Granat, M.H. The effects of knee and ankle flexion on ground clearance in paraplegic gait. Clin. Biomech. 2000, 15, 536–540. [Google Scholar] [CrossRef]
- Meyer, C.; Killeen, T.; Easthope, C.S.; Curt, A.; Bolliger, M.; Linnebank, M.; Zörner, B.; Filli, L. Familiarization with treadmill walking: How much is enough? Sci. Rep. 2019, 9, 5232. [Google Scholar] [CrossRef]
- Bortole, M.; Venkatakrishnan, A.; Zhu, F.; Moreno, J.C.; Francisco, G.E.; Pons, J.L.; Contreras-Vidal, J.L. The H2 robotic exoskeleton for gait rehabilitation after stroke: Early findings from a clinical study. J. NeuroEng. Rehabil. 2015, 12, 54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1988. [Google Scholar]
- Wang, J.; Stephenson, M.L.; Hass, C.J.; Janelle, C.M.; Tillman, M.D. Carrying Asymmetric Loads While Walking on a Treadmill Interferes with Lower Limb Coordination. Int. J. Environ. Res. Public Health 2021, 18, 4549. [Google Scholar] [CrossRef] [PubMed]
- Mattes, S.J.; Martin, P.E.; Royer, T.D. Walking symmetry and energy cost in persons with unilateral transtibial amputations: Matching prosthetic and intact limb inertial properties. Arch. Phys. Med. Rehabil. 2000, 81, 561–568. [Google Scholar] [CrossRef]
- Lin-Chan, S.J.; Nielsen, D.H.; Yack, H.J.; Hsu, M.J.; Shurr, D.G. The effects of added prosthetic mass on physiologic responses and stride frequency during multiple speeds of walking in persons with transtibial amputation. Arch. Phys. Med. Rehabil. 2003, 84, 1865–1871. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, L.A.B.; Neto, H.P.; Grecco, L.A.C.; Christovão, T.C.L.; Duarte, N.A.; Lazzari, R.D.; Galli, M.; Oliveira, C.S. Effect of Ankle-foot Orthosis on Gait Velocity and Cadence of Stroke Patients: A Systematic Review. J. Phys. Sci. 2013, 25, 1503–1508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagano, H.; Begg, R.K.; Sparrow, W.A.; Taylor, S. Ageing and limb dominance effects on foot-ground clearance during treadmill and overground walking. Clin. Biomech. 2011, 26, 962–968. [Google Scholar] [CrossRef]
- Schulz, B.W. Minimum toe clearance adaptations to floor surface irregularity and gait speed. J. Biomech. 2011, 44, 1277–1284. [Google Scholar] [CrossRef] [Green Version]
- Khandoker, A.H.; Lynch, K.; Karmakar, C.K.; Begg, R.K.; Palaniswami, M. Toe clearance and velocity profiles of young and elderly during walking on sloped surfaces. J. NeuroEng. Rehabil. 2010, 7, 18. [Google Scholar] [CrossRef] [PubMed]
- Loverro, K.L.; Mueske, N.M.; Hamel, K.A. Location of minimum foot clearance on the shoe and with respect to the obstacle changes with locomotor task. J. Biomech. 2013, 46, 1842–1850. [Google Scholar] [CrossRef] [Green Version]
- Begg, R.; Best, R.; Dell’Oro, L.; Taylor, S. Minimum foot clearance during walking: Strategies for the minimisation of trip-related falls. Gait Posture 2007, 25, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Choo, Y.J.; Chang, M.C. Effectiveness of an ankle–foot orthosis on walking in patients with stroke: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 15879. [Google Scholar] [CrossRef] [PubMed]
- Riveras, M.; Ravera, E.; Ewins, D.; Shaheen, A.F.; Catalfamo-Formento, P. Minimum toe clearance and tripping probability in people with unilateral transtibial amputation walking on ramps with different prosthetic designs. Gait Posture 2020, 81, 41–48. [Google Scholar] [CrossRef]
- Vistamehr, A.; Kautz, S.A.; Neptune, R.R. The influence of solid ankle-foot-orthoses on forward propulsion and dynamic balance in healthy adults during walking. Clin. Biomech. 2014, 29, 583–589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukuchi, C.A.; Fukuchi, R.K.; Duarte, M. Effects of walking speed on gait biomechanics in healthy participants: A systematic review and meta-analysis. Syst. Rev. 2019, 8, 153. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.-T.; Novak, A.C.; Brouwer, B.; Li, Q. Concurrent validation of Xsens MVN measurement of lower limb joint angular kinematics. Physiol. Meas. 2013, 34, N63–N69. [Google Scholar] [CrossRef]
- Kobsar, D.; Charlton, J.M.; Tse, C.T.F.; Esculier, J.-F.; Graffos, A.; Krowchuk, N.M.; Thatcher, D.; Hunt, M.A. Validity and reliability of wearable inertial sensors in healthy adult walking: A systematic review and meta-analysis. J. Neuroeng. Rehabil. 2020, 17, 62. [Google Scholar] [CrossRef] [PubMed]
- Mariani, B.; Rochat, S.; Büla, C.J.; Aminian, K. Heel and toe clearance estimation for gait analysis using wireless inertial sensors. IEEE Trans. Biomed. Eng. 2012, 59, 3162–3168. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Gait Condition | Gait Speed | Minimum Foot Clearance (cm) | |
|---|---|---|---|
| Right Lower Limb (RL) | Left Lower Limb (LL) | ||
| Without AFO | 0.8 km/h | 3.39 (2.14) | 3.49 (1.70) |
| 1.2 km/h | 2.92 (1.19) | 3.05 (1.04) | |
| 1.6 km/h | 2.89 (1.49) | 3.03 (1.03) | |
| With AFO | 0.8 km/h | 3.27 (1.52) | 4.49 (1.29) |
| 1.2 km/h | 3.90 (1.85) | 4.77 (2.02) | |
| 1.6 km/h | 3.37 (1.48) | 4.53 (2.25) | |
| Gait Condition | Limb | Gait Speed | Duration (% Gait Cycle) | Length (% Stature) | |||
|---|---|---|---|---|---|---|---|
| Stance | Swing | Step | Step | Stride | |||
| Without AFO | Right (RL) | 0.8 km/h | 77.10 (3.59) | 23.15 (3.94) | 51.13 (2.57) | 21.01 (5.06) | 45.65 (8.72) |
| 1.2 km/h | 73.08 (3.14) | 26.91 (3.14) | 51.38 (1.76) | 23.64 (4.41) | 51.06 (5.99) | ||
| 1.6 km/h | 69.52 (1.86) | 30.47 (1.86) | 51.55 (1.80) | 24.72 (4.46) | 52.80 (7.54) | ||
| Left (LL) | 0.8 km/h | 77.46 (2.69) | 22.55 (2.70) | 49.17 (0.44) | 24.52 (4.32) | 45.66 (8.66) | |
| 1.2 km/h | 73.57 (2.16) | 26.46 (2.16) | 49.00 (1.72) | 27.13 (2.68) | 51.06 (5.98) | ||
| 1.6 km/h | 69.96 (0.76) | 30.03 (0.76) | 48.91 (1.57) | 27.73 (3.64) | 53.09 (7.86) | ||
| With AFO | Right (RL) | 0.8 km/h | 72.48 (2.65) * | 27.51 (2.65) * | 56.80 (4.48) * | 24.46 (2.50) | 47.65 (2.21) |
| 1.2 km/h | 67.76 (3.24) * | 32.23 (3.24) * | 58.92 (3.19) * | 31.12 (3.11) | 59.21 (2.63) | ||
| 1.6 km/h | 64.94 (3.96) * | 35.05 (3.96) * | 56.60 (1.71) * | 32.03 (2.73) | 62.25 (2.60) | ||
| Left (LL) | 0.8 km/h | 77.16 (2.31) | 22.83 (2.31) | 43.31 (4.47) | 22.87 (3.10) | 47.50 (1.98) | |
| 1.2 km/h | 73.06 (3.09) | 26.93 (3.09) | 41.12 (3.16) | 27.35 (3.61) | 59.29 (2.57) | ||
| 1.6 km/h | 69.95 (2.58) | 30.40 (2.58) | 43.44 (1.69) | 29.21 (2.87) | 62.26 (2.57) | ||
| Gait Condition | Limb | Gait Speed | Joint Angle (Degrees) | Joint Range of Motion (Degrees) | ||||
|---|---|---|---|---|---|---|---|---|
| Hip | Knee | Ankle | Hip | Knee | Ankle | |||
| Without AFO | Right (RL) | 0.8 km/h | 26.86 (5.23) | 55.51 (10.16) | −12.55 (4.65) | 27.69 (8.37) | 47.24 (12.18) | 22.54 (8.42) |
| 1.2 km/h | 25.61 (5.77) | 56.55 (7.40) | −13.23 (5.82) | 28.95 (7.72) | 50.41 (8.77) | 23.68 (7.90) c | ||
| 1.6 km/h | 25.46 (7.57) | 58.31 (8.95) | −10.11 (7.71) | 27.77 (8.08) | 53.37 (7.34) | 19.24 (7.13) b | ||
| Left (LL) | 0.8 km/h | 28.71 (2.85) | 57.05 (8.35) | −12.67 (3.83) | 29.30 (8.39) | 46.06 (11.87) | 20.28 (9.27) | |
| 1.2 km/h | 27.15 (3.08) | 56.95 (6.77) | −13.29 (4.85) | 30.38 (6.84) | 49.61 (8.50) | 20.65 (7.74) | ||
| 1.6 km/h | 27.09 (5.88) | 59.14 (7.29) | −11.78 (4.89) | 29.06 (7.82) | 51.66 (8.08) | 18.40 (8.17) | ||
| With AFO | Right (RL) | 0.8 km/h | 31.79 (6.79) * | 62.42 (4.96) | −14.00 (4.02) | 29.85 (3.61) | 51.02 (8.43) | 16.33 (2.73) |
| 1.2 km/h | 34.55 (7.83) * | 61.92 (7.16) | −16.72 (2.85) | 36.97 (6.97) | 52.42(10.36) | 19.95 (3.73) | ||
| 1.6 km/h | 33.79 (8.26) * | 62.87 (6.90) | −15.52 (3.53) | 38.37 (8.17) | 54.48 (8.99) | 18.43 (3.25) | ||
| Left (LL) | 0.8 km/h | 29.57 (4.94) | 61.19 (6.16) | −6.70 (5.38) | 33.81 (4.69) | 54.13 (9.23) | 16.63 (3.64) b,c | |
| 1.2 km/h | 30.73 (5.19) | 60.31 (7.85) | −12.14 (7.02) | 38.88 (6.75) | 54.52 (11.62) | 22.55 (4.40) a | ||
| 1.6 km/h | 31.27 (5.84) | 61.69 (8.13) | −11.81 (6.01) | 40.00 (7.63) | 56.55 (9.12) | 22.08 (4.24) a | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fonseca, P.; Machado, L.; Sousa, M.V.; Sebastião, R.; Sousa, F.; Figueiredo, J.; Santos, C.P.; Vilas-Boas, J.P. Does Gait with an Ankle Foot Orthosis Improve or Compromise Minimum Foot Clearance? Sensors 2021, 21, 8089. https://doi.org/10.3390/s21238089
Fonseca P, Machado L, Sousa MV, Sebastião R, Sousa F, Figueiredo J, Santos CP, Vilas-Boas JP. Does Gait with an Ankle Foot Orthosis Improve or Compromise Minimum Foot Clearance? Sensors. 2021; 21(23):8089. https://doi.org/10.3390/s21238089
Chicago/Turabian StyleFonseca, Pedro, Leandro Machado, Manoela Vieira Sousa, Ricardo Sebastião, Filipa Sousa, Joana Figueiredo, Cristina P. Santos, and João Paulo Vilas-Boas. 2021. "Does Gait with an Ankle Foot Orthosis Improve or Compromise Minimum Foot Clearance?" Sensors 21, no. 23: 8089. https://doi.org/10.3390/s21238089
APA StyleFonseca, P., Machado, L., Sousa, M. V., Sebastião, R., Sousa, F., Figueiredo, J., Santos, C. P., & Vilas-Boas, J. P. (2021). Does Gait with an Ankle Foot Orthosis Improve or Compromise Minimum Foot Clearance? Sensors, 21(23), 8089. https://doi.org/10.3390/s21238089