
Evaluation of Individualized Functional Electrical Stimulation-Induced Acute Changes during Walking: A Case Series in Children with Cerebral Palsy




Abstract
1. Introduction
2. Materials and Methods
2.1. Functional Electrical Stimulation
2.1.1. System
2.1.2. Stimulation Programming
2.1.3. Stimulation Thresholding
2.2. Experimental Protocol
2.2.1. Muscle Selection and Timing of Stimulation Delivery
2.2.2. Data Collection
2.2.3. Typically Developing (TD) Reference Dataset
2.3. Gait Analysis
2.4. Statistics Analysis
3. Results
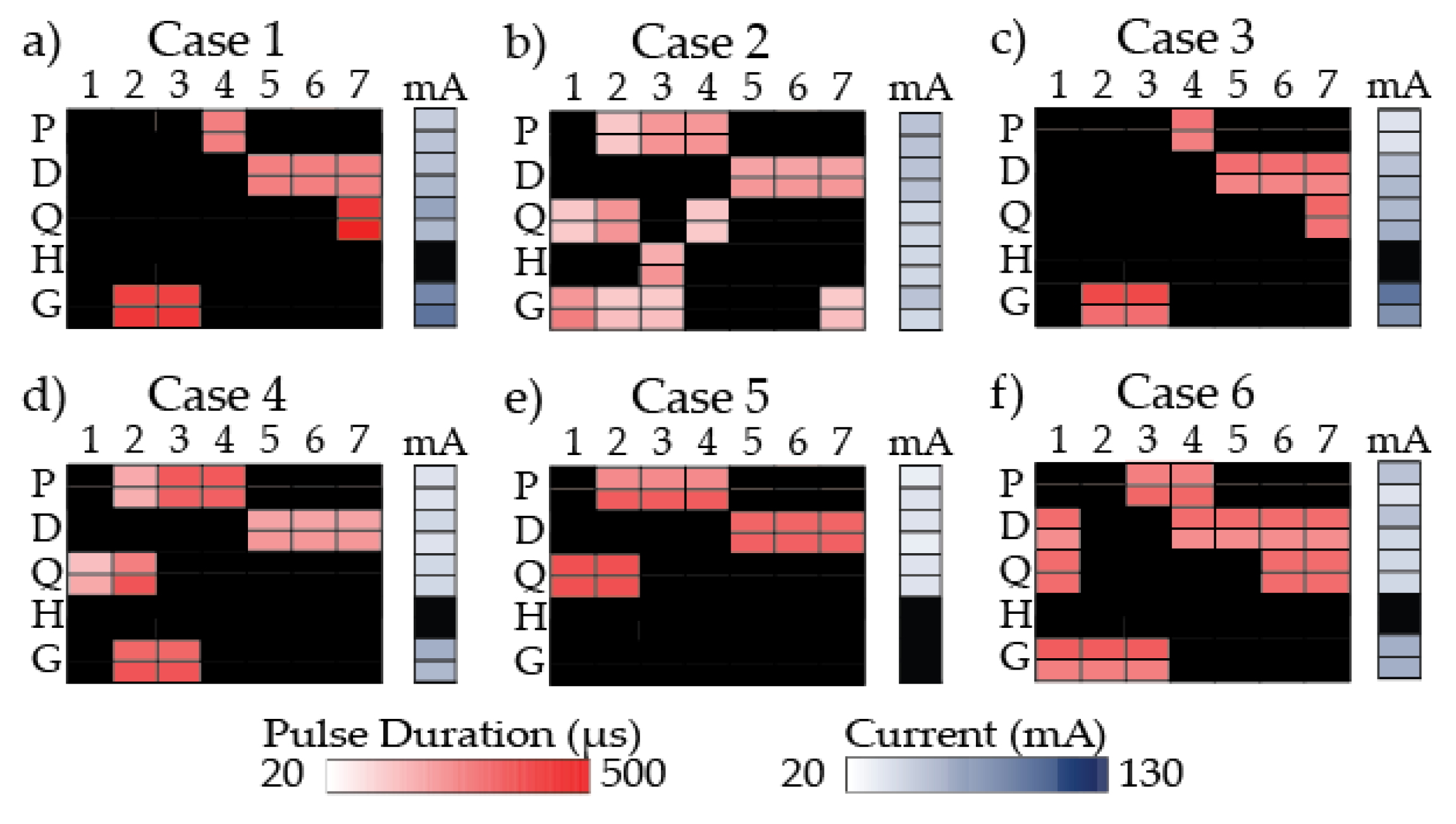
3.1. Individualized Stimulation Programs
3.2. Typically Developing (TD) Reference Dataset
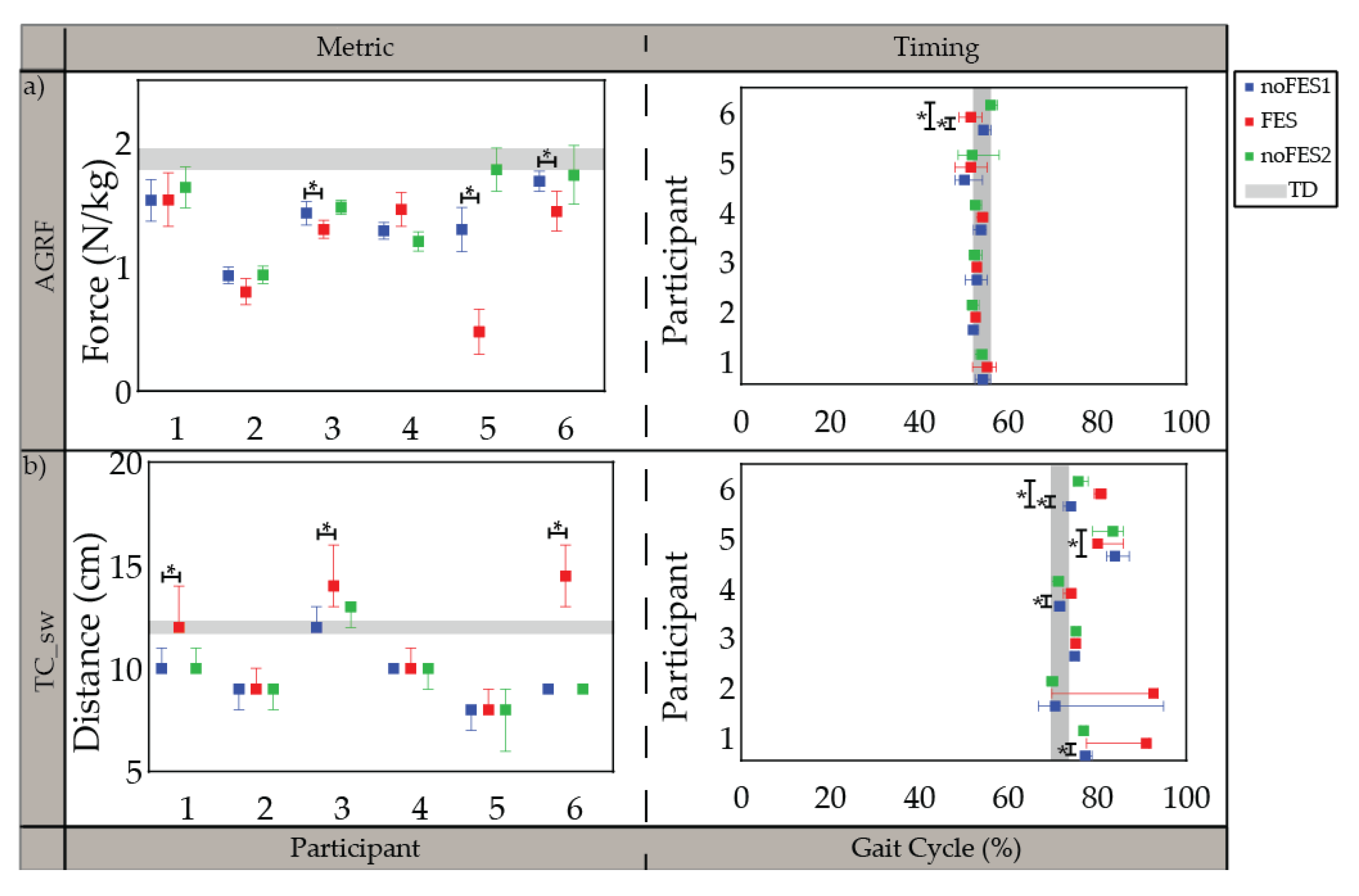
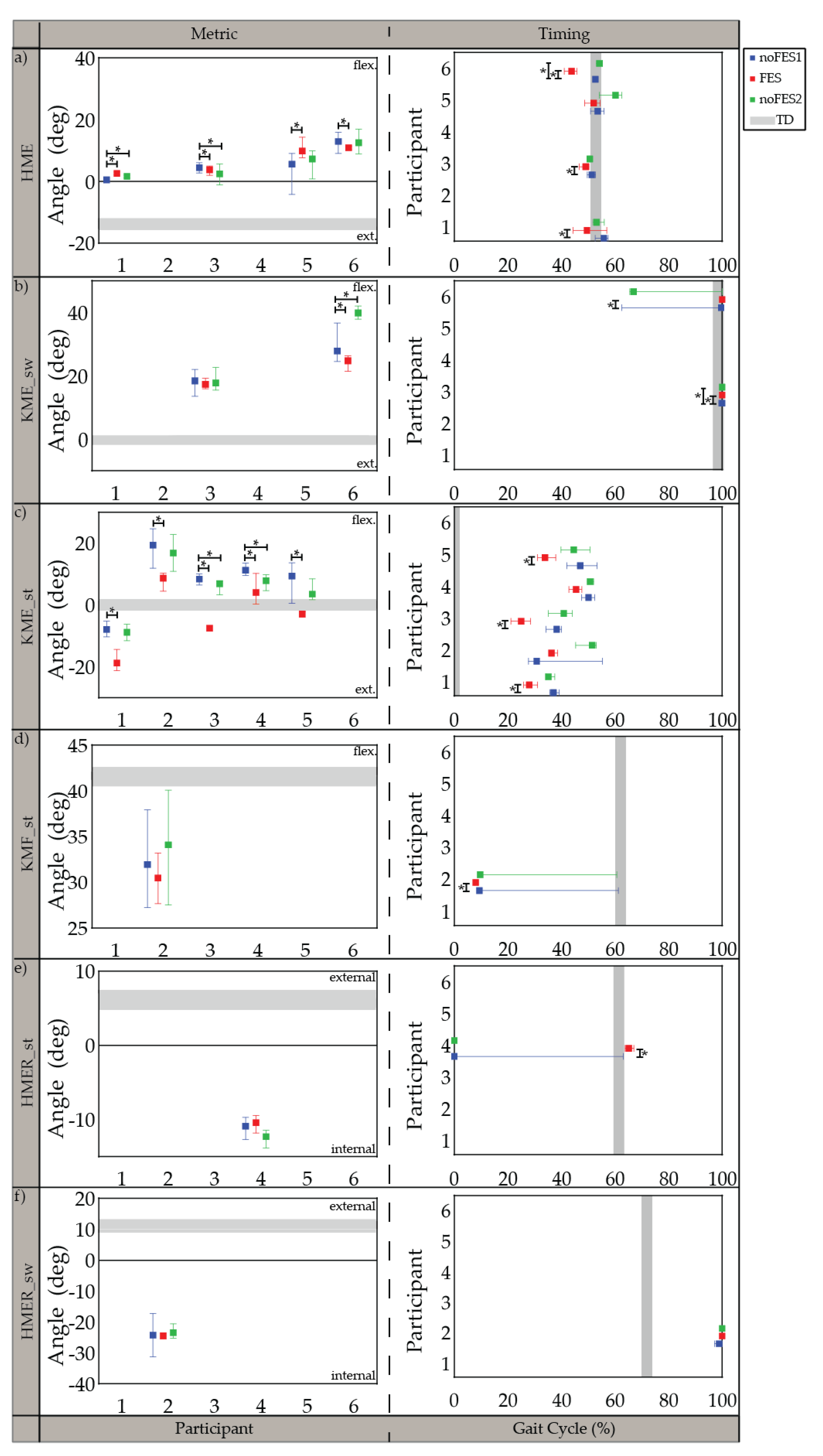
3.3. Gait Metrics and Timing in CP
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Poinsett, P.M. Cerebral Palsy Facts and Statistics. Available online: https://www.cerebralpalsyguidance.com/cerebral-palsy/research/facts-and-statistics/ (accessed on 27 June 2021).
- Kirby, R.S.; Wingate, M.S.; Van Naarden Braun, K.; Doernberg, N.S.; Arneson, C.L.; Benedict, R.E.; Mulvihill, B.; Durkin, M.S.; Fitzgerald, R.T.; Maenner, M.J.; et al. Prevalence and functioning of children with cerebral palsy in four areas of the United States in 2006: A report from the Autism and Developmental Disabilities Monitoring Network. Res. Dev. Disabil. 2011, 32, 462–469. [Google Scholar] [CrossRef] [PubMed]
- Taft, L.T. Cerebral Palsy. Pediatr. Rev. 1995, 16, 411–418. [Google Scholar] [CrossRef]
- Binder, H.; Eng, G.D. Rehabilitation management of children with spastic diplegic cerebral palsy. Arch. Phys. Med. Rehabil. 1989, 70, 482–489. [Google Scholar] [CrossRef]
- Wiley, M.E.; Damiano, D.L. Lower-extremity strength profiles in spastic cerebral palsy. Dev. Med. Child Neurol. 1998, 40, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Stackhouse, S.K.; Binder-Macleod, S.A.; Lee, S.C.K. Voluntary muscle activation, contractile properties, and fatigability in children with and without cerebral palsy. Muscle Nerve 2005, 31, 594–601. [Google Scholar] [CrossRef]
- Bell, K.; Ounpuu, S. Natural progression of gait in children with cerebral palsy. J. Pediatr. Orthop. 2002, 22, 677–682. [Google Scholar] [CrossRef]
- Hanna, S.E.S.; Rosenbaum, P.P.L.; Bartlett, D.J.; Palisano, R.J.; Walter, S.D.; Avery, L.; Russell, D.J. Stability and decline in gross motor function among children and youth with cerebral palsy aged 2 to 21 years. Dev. Med. Child Neurol. 2009, 51, 295–302. [Google Scholar] [CrossRef]
- Kerr, C.; Mcdowell, B.C.; Parkes, J.; Stevenson, M.; Cosgrove, A.P. Age-related changes in energy efficiency of gait, activity, and participation in children with cerebral palsy. Dev. Med. Child Neurol. 2011, 53, 61–67. [Google Scholar] [CrossRef]
- Rosenbaum, P.; Walter, S. Prognosis for gross motor function in cerebral palsy: Creation of motor development curves. JAMA 2002, 288, 1357–1363. [Google Scholar] [CrossRef]
- Sutherland, D.; Cooper, L. The pathomechanics of progressive crouch gait in spastic diplegia. Orthop. Clin. N. Am. 1978, 9, 143–154. [Google Scholar] [CrossRef]
- Johnson, D.C.; Damiano, D.L.; Abel, M.F. The Evolution of Gait in Childhood and Adolescent Cerebral Palsy. J. Pediatr. Orthop. 1997, 17, 392–396. [Google Scholar] [CrossRef] [PubMed]
- Arnold, A.S.; Anderson, F.C.; Pandy, M.G.; Delp, S.L. Muscular contributions to hip and knee extension during the single limb stance phase of normal gait: A framework for investigating the causes of crouch gait. J.Biomech. 2005, 38, 2181–2189. [Google Scholar] [CrossRef]
- Gage, J. The Treatment of Gait Problems in Cerebral Palsy, 2nd ed.; John & Sons, I., Ed.; Mac Keith Press: London, UK, 2004. [Google Scholar]
- Rodda, J.; Graham, H. Classification of gait patterns in spastic hemiplegia and spastic diplegia: A basis for a management algorithm. Eur. J. Neurol. 2001, 8, 98–108. [Google Scholar] [CrossRef] [PubMed]
- Rodda, J.; Graham, H. Sagittal gait patterns in spastic diplegia. J. Bone Jt. Surg.-Ser. B 2004, 86, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Sutherland, D.H.; Davids, J.R. Common gait abnormalities of the knee in cerebral palsy. Clin.Orthop. 1993, 288, 139–147. [Google Scholar]
- Winter, D. The Biomechanics and Motor Control of Human Gait: Normal, Elderly and Pathological; Wiley: Hoboken, NJ, USA, 1991; Volume 2, ISBN 0470398183. [Google Scholar]
- Perry, J.; Davids, J. Gait Analysis: Normal and Pathological Function, 1st ed.; Slack Incorporated: Thorofare, NJ, USA, 1992; Volume 12, ISBN 9781556421921. [Google Scholar]
- Bennett, B.C.; Abel, M.F.; Wolovick, A.; Franklin, T.; Allaire, P.E.; Kerrigan, D.C. Center of mass movement and energy transfer during walking in children with cerebral palsy. Arch. Phys. Med. Rehabil. 2005, 86, 2189–2194. [Google Scholar] [CrossRef]
- Campbell, J.; Ball, J. Energetics of walking in cerebral palsy. Orthop. Clin. N. Am. 1978, 9, 374–377. [Google Scholar]
- Johnston, T.E.; Moore, S.E.; Quinn, L.T.; Smith, B.T. Energy cost of walking in children with cerebral palsy: Relation to the Gross Motor Function Classification System. Dev. Med. Child Neurol. 2004, 46, 34–38. [Google Scholar] [CrossRef]
- Carmick, J. Clinical use of neuromuscular electrical stimulation for children with cerebral palsy, Part 1: Lower extremity. Phys. Ther. 1993, 73, 505–527. [Google Scholar] [CrossRef]
- Comeaux, P.; Patterson, N.; Rubin, M.; Meiner, R. Effect of neuromuscular electrical stimulation during gait in children with cerebral palsy. Pediatr. Phys. Ther. 1997, 9, 103–109. [Google Scholar] [CrossRef]
- Damiano, D.L.D.; Prosser, L.A.; Curatalo, L.A.; Alter, K.E. Muscle plasticity and ankle control after repetitive use of a functional electrical stimulation device for foot drop in cerebral palsy. Neurorehabil. Neural Repair 2013, 27, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Johnston, T.E.E.; Finson, R.L.L.; McCarthy, J.J.; Smith, B.T.; Betz, R.R.; Mulcahey, M.J. Use of functional electrical stimulation to augment traditional orthopaedic surgery in children with cerebral palsy. J. Pediatr. Orthop. 2004, 24, 283–291. [Google Scholar] [CrossRef]
- Durham, S.; Eve, L.; Stevens, C.; Ewins, D. Effect of Functional Electrical Stimulation on asymmetries in gait of children with hemiplegic cerebral palsy. Physiotherapy 2004, 90, 82–90. [Google Scholar] [CrossRef]
- van der Linden, M.L.; Hazlewood, M.E.; Hillman, S.J.; Robb, J.E. Functional Electrical Stimulation to the Dorsiflexors and Quadriceps in Children with Cerebral Palsy. Pediatr. Phys. Ther. 2008, 20, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Postans, N.J.; Granat, M.H. Effect of functional electrical stimulation, applied during walking, on gait in spastic cerebral palsy. Dev. Med. Child Neurol. 2005, 47, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Pierce, S.R.S.; Orlin, M.N.M.; Lauer, R.T.; Johnston, T.E.; Smith, B.T.; McCarthy, J.J. Comparison of percutaneous and surface functional electrical stimulation during gait in a child with hemiplegic cerebral palsy. Am. J. Phys. Med. Rehabil. 2004, 83, 798–805. [Google Scholar] [CrossRef] [PubMed]
- Pierce, S.R.; Laughton, C.A.; Smith, B.T.; Orlin, M.N.; Johnston, T.E.; McCarthy, J.J. Direct Effect of Percutaneous Electric Stimulation during Gait in Children with Hemiplegic Cerebral Palsy: A Report of 2 Cases. Arch. Phys. Med. Rehabil. 2004, 85, 339–343. [Google Scholar] [CrossRef]
- Danino, B.; Khamis, S.; Hemo, Y.; Batt, R.; Snir, E.; Wientroub, S.; Hayek, S. The efficacy of neuroprosthesis in young hemiplegic patients, measured by three different gait indices: Early results. J. Child. Orthop. 2013, 7, 537–542. [Google Scholar] [CrossRef]
- Pool, D.; Valentine, J.; Bear, N.; Donnelly, C.J.; Elliott, C.; Stannage, K. The orthotic and therapeutic effects following daily community applied functional electrical stimulation in children with unilateral spastic cerebral palsy: A randomised controlled trial. BMC Pediatr. 2015, 15, 154. [Google Scholar] [CrossRef]
- Khamis, S.; Martikaro, R.; Wientroub, S.; Hemo, Y.; Hayek, S. A functional electrical stimulation system improves knee control in crouch gait. J. Child. Orthop. 2015, 9, 137–143. [Google Scholar] [CrossRef]
- Al-Abdulwahab, S.S.; Al-Khatrawi, W.M. Neuromuscular electrical stimulation of the gluteus medius improves the gait of children with cerebral palsy. NeuroRehabilitation 2009, 24, 209–217. [Google Scholar] [CrossRef]
- Svoboda, Z.; Janura, M.; Kutilek, P.; Janurova, E. Relationships between movements of the lower limb joints and the pelvis in open and closed kinematic chains during a gait cycle. J. Hum. Kinet. 2016, 50, 37–43. [Google Scholar] [CrossRef]
- Seifart, A.; Unger, M.; Burger, M. The effect of lower limb functional electrical stimulation on gait of children with cerebral palsy. Pediatr. Phys. Ther. 2009, 21, 23–30. [Google Scholar] [CrossRef]
- Cauraugh, J.; Naik, S. Children with cerebral palsy: A systematic review and meta-analysis on gait and electrical stimulation. Clin. Rehabil. 2010, 24, 963. [Google Scholar] [CrossRef]
- Dobson, F.; Morris, M.; Baker, R.; Graham, H. Gait classification in children with cerebral palsy: A systematic review. Gait Posture 2007, 25, 140–152. [Google Scholar] [CrossRef]
- Mooney, J.A.; Rose, J. A Scoping Review of Neuromuscular Electrical Stimulation to Improve Gait in Cerebral Palsy: The Arc of Progress and Future Strategies. Front. Neurol. 2019, 10, 887. [Google Scholar] [CrossRef]
- Seifart, A.; Unger, M.; Burger, M. Functional electrical stimulation to lower limb muscles after botox in children with cerebral palsy. Pediatr. Phys. Ther. 2010, 22, 199–206. [Google Scholar] [CrossRef]
- Orlin, M.N.; Pierce, S.R.; Stackhouse, C.L.; Smith, B.T.; Johnston, T.; Shewokis, P.A.; McCarthy, J.J. Immediate effect of percutaneous intramuscular stimulation during gait in children with cerebral palsy: A feasibility study. Dev. Med. Child Neurol. 2005, 47, 684–690. [Google Scholar] [CrossRef]
- Shideler, B.L.; Bulea, T.C.; Chen, J.; Stanley, C.J.; Gravunder, A.J.; Damiano, D.L. Toward a hybrid exoskeleton for crouch gait in children with cerebral palsy: Neuromuscular electrical stimulation for improved knee extension. J. Neuroeng. Rehabil. 2020, 17, 1–14. [Google Scholar] [CrossRef]
- Behboodi, A.; Zahradka, N.; Alesi, J.; Wright, H.; Lee, S.C.K. Use of a Novel Functional Electrical Stimulation Gait Training System in 2 Adolescents with Cerebral Palsy: A Case Series Exploring Neurotherapeutic Changes. Phys. Ther. 2019, 99, 739–747. [Google Scholar] [CrossRef]
- Rose, J.; Cahill-Rowley, K.; Butler, E.E. Artificial Walking Technologies to Improve Gait in Cerebral Palsy: Multichannel Neuromuscular Stimulation. Artif. Organs 2017, 41, E233–E239. [Google Scholar] [CrossRef] [PubMed]
- Armand, S.; Decoulon, G.; Bonnefoy-Mazure, A. Gait analysis in children with cerebral palsy. EFORT Open Rev. 2016, 1, 448–460. [Google Scholar] [CrossRef] [PubMed]
- Behboodi, A.; Wright, H.; Zahradka, N.; Lee, S.C.K. Seven phases of gait detected in real-time using shank attached gyroscopes. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBS, Milan, Italy, 25–29 August 2015; pp. 5529–5532. [Google Scholar]
- Behboodi, A.; Zahradka, N.; Wright, H.; Alesi, J.; Lee, S.C.K. Real-time detection of seven phases of gait in children with cerebral palsy using two gyroscopes. Sensors 2019, 19, 2517. [Google Scholar] [CrossRef]
- Zahradka, N.; Behboodi, A.; Wright, H.; Bodt, B.; Lee, S. Evaluation of gait phase detection delay compensation strategies to control a gyroscope-controlled functional electrical stimulation system during walking. Sensors 2019, 19, 2471. [Google Scholar] [CrossRef]
- Shirley Ryan Ability Lab Timed 10-Meter Walk Test. Available online: https://www.sralab.org/rehabilitation-measures/10-meter-walk-test (accessed on 27 June 2021).
- Robinson, A.J.; Synder-Mackler, L. (Eds.) Clinical Electrophysiology: Electrotherapy and Electrophysiologic Testing, 3rd ed.; Lippincott Williams & Wilkins, a Wolters Kluwer business: Baltimore, MD, USA, 2007. [Google Scholar]
- Zeni, J.A.; Higginson, J.S. Gait parameters and stride-to-stride variability during familiarization to walking on a split-belt treadmill. Clin. Biomech. 2010, 25, 383–386. [Google Scholar] [CrossRef]
- Zeni, J.A.; Richards, J.G.; Higginson, J.S. Two simple methods for determining gait events during treadmill and overground walking using kinematic data. Gait Posture 2008, 27, 710–714. [Google Scholar] [CrossRef] [PubMed]
- Bowden, M.G.; Balasubramanian, C.K.; Neptune, R.R.; Kautz, S.A. Anterior-posterior ground reaction forces as a measure of paretic leg contribution in hemiparetic walking. Stroke 2006, 37, 872–876. [Google Scholar] [CrossRef]
- Dadashi, F.; Mariani, B.; Rochat, S.; Büla, C.J.; Santos-Eggimann, B.; Aminian, K. Gait and foot clearance parameters obtained using shoe-worn inertial sensors in a large-population sample of older adults. Sensors 2013, 14, 443–457. [Google Scholar] [CrossRef] [PubMed]
- Palisano, R.; Rosenbaum, P.; Bartlett, D.; Livingston, M. Content validity of the exapnded and revised Gross Motor Function Classification System. Dev. Med. Child Neurol. 2008, 50, 744–750. [Google Scholar] [CrossRef]
- Ho, C.-L.; Holt, K.G.; Saltzman, E.; Wagenaar, R.C. Functional electrical stimulation changes dynamic resources in children with spastic cerebral palsy. Phys. Ther. 2006, 86, 987–1000. [Google Scholar] [CrossRef][Green Version]
- Klejman, S.; Andrysek, J.; Dupuis, A.; Wright, V. Test-Retest Reliability of Discrete Gait Parameters in Children with Cerebral Palsy. Arch. Phys. Med. Rehabil. 2010, 91, 781–787. [Google Scholar] [CrossRef]
- Gage, J. Gait Anlaysis in Cerebral Palsy; Mac Keith Press: London, UK, 1991. [Google Scholar]
- Prosser, L.A.; Curatalo, L.A.; Alter, K.E.; Damiano, D.L. Acceptability and potential effectiveness of a foot drop stimulator in children and adolescents with cerebral palsy. Dev. Med. Child Neurol. 2012, 54, 1044–1049. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Gait Metric | Definition |
|---|---|
| AGRF | Global maxima of the GRF in the anterior direction between contralateral IC and ipsilateral TC [54] |
| TC_sw | Global minima of the target path of the distal toe marker in the vertical direction between TC and IC [55] |
| HME | Global minima of hip angle during the gait cycle |
| KME_sw | Global maxima of knee angle between TC and IC |
| KME_st | Global maxima of knee angle between IC and TC |
| KMF_st | Global minima of knee angle between IC and TC |
| HMER_st | Global minima (right side) and maxima (left side) of hip rotation between IC and TC |
| HMER_sw | Global minima (right side) and maxima (left side) of hip rotation between TC and IC |
| Case | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|
| Sex | M | M | M | M | F | F |
| GMFCS 1 | III | III | II | II | III | II |
| Height (m) | 1.67 | 1.70 | 1.70 | 1.52 | 1.31 | 1.44 |
| Weight (kg) | 32.13 | 60.06 | 61.97 | 42.60 | 31.60 | 42.53 |
| Self-selected speed (m/s) | 0.77 | 0.83 | 0.98 | 1.07 | 0.60 | 0.90 |
| Treadmill speed (m/s) | 0.60 | 0.80 | 0.90 | 0.75 | 0.45 | 0.80 |
| Assistive Device | (B) lofstrand crutches | (B) lofstrand crutches | - | - | Posterior and Anterior Walkers | - |
| Braces | - | (B) AFO 2 | - | - | - | - |
| Gait Metric. | Metric Median (IQR) | Timing (% Gait Cycle) Median (IQR) |
|---|---|---|
| AGRF (N/kg) | 1.88 (0.66) | 54.11 (2.83) |
| TC_sw (cm) | 12.00 (1.0) | 71.63 (2.49) |
| HME (deg) | −14.03 (7.32) | 52.92 (1.89) |
| KME_sw (deg) | −0.10 (6.25) | 98.60 (2.11) |
| KME_st (deg) | 0.09 (5.93) | 0.00 (2.093) |
| KMF_st (deg) | 41.63 (6.10) | 62.15 (2.46) |
| HMER_st (deg) | 5.92 (7.41) | 61.43 (62.58) |
| HMER_sw (deg) | 11.37 (7.83) | 71.96 (3.32) |
| Case | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|
| AGRF (N/kg) | ** | ** | ** | ** | ** | 0.031 |
| TC_sw (cm) | ** | ** | ** | ** | ** | ** |
| HME (deg) | ** | N/A | ** | N/A | ** | ** |
| KME_sw (deg) | N/A | N/A | ** | N/A | N/A | ** |
| KME_st (deg) | ** | ** | ** | ** | ** | N/A |
| KMF_st (deg) | N/A | ** | N/A | N/A | N/A | N/A |
| HMER_st (deg) | N/A | N/A | N/A | ** | N/A | N/A |
| HMER_sw (deg) | N/A | ** | N/A | N/A | N/A | N/A |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zahradka, N.; Behboodi, A.; Sansare, A.; Lee, S.C.K. Evaluation of Individualized Functional Electrical Stimulation-Induced Acute Changes during Walking: A Case Series in Children with Cerebral Palsy. Sensors 2021, 21, 4452. https://doi.org/10.3390/s21134452
Zahradka N, Behboodi A, Sansare A, Lee SCK. Evaluation of Individualized Functional Electrical Stimulation-Induced Acute Changes during Walking: A Case Series in Children with Cerebral Palsy. Sensors. 2021; 21(13):4452. https://doi.org/10.3390/s21134452
Chicago/Turabian StyleZahradka, Nicole, Ahad Behboodi, Ashwini Sansare, and Samuel C. K. Lee. 2021. "Evaluation of Individualized Functional Electrical Stimulation-Induced Acute Changes during Walking: A Case Series in Children with Cerebral Palsy" Sensors 21, no. 13: 4452. https://doi.org/10.3390/s21134452
APA StyleZahradka, N., Behboodi, A., Sansare, A., & Lee, S. C. K. (2021). Evaluation of Individualized Functional Electrical Stimulation-Induced Acute Changes during Walking: A Case Series in Children with Cerebral Palsy. Sensors, 21(13), 4452. https://doi.org/10.3390/s21134452