Age-Related Changes in Mobility Evaluated by the Timed Up and Go Test Instrumented through a Single Sensor

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
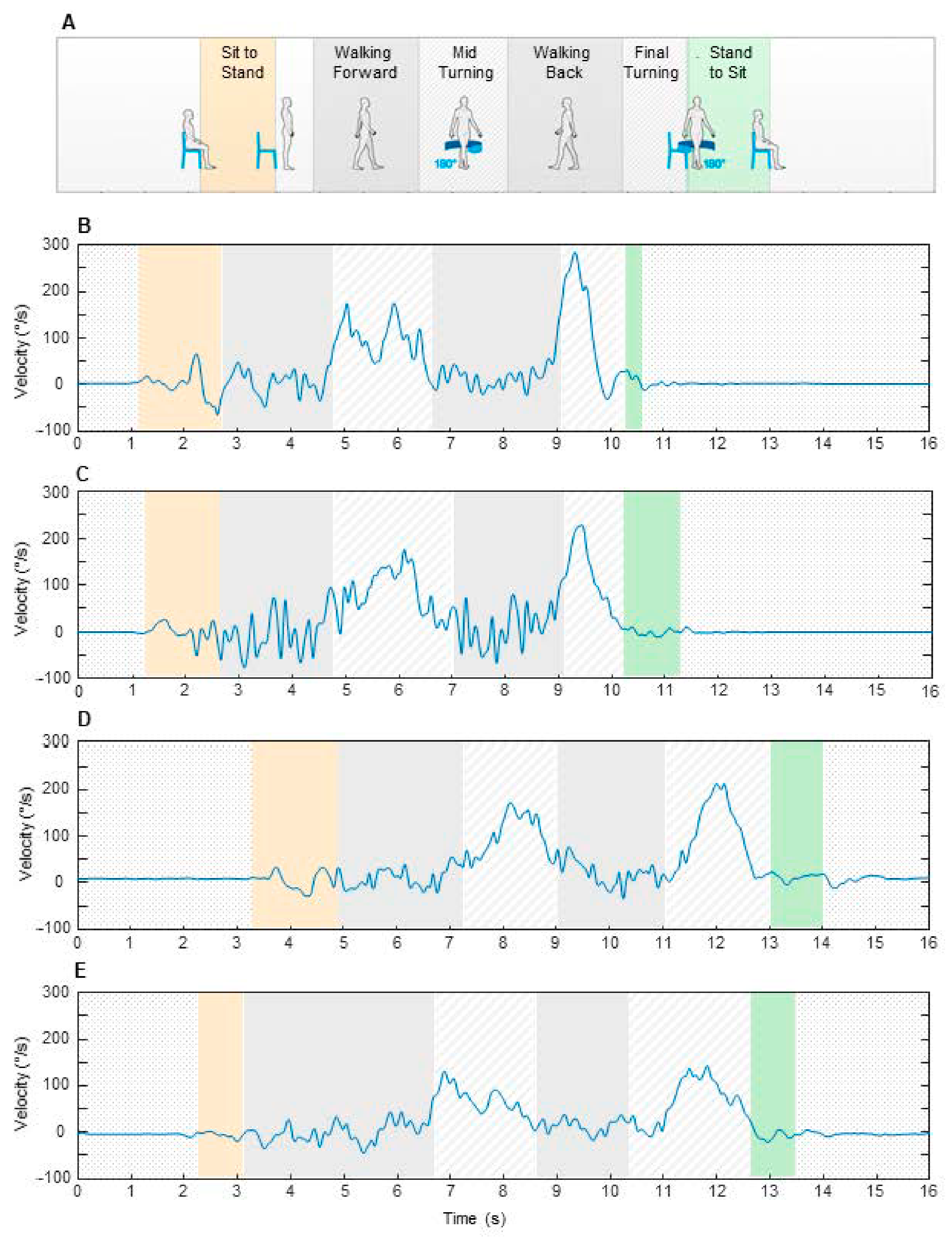
2.2. Experimental Procedure
2.3. Data Collection and Processing
2.4. Statistical Analysis
3. Results
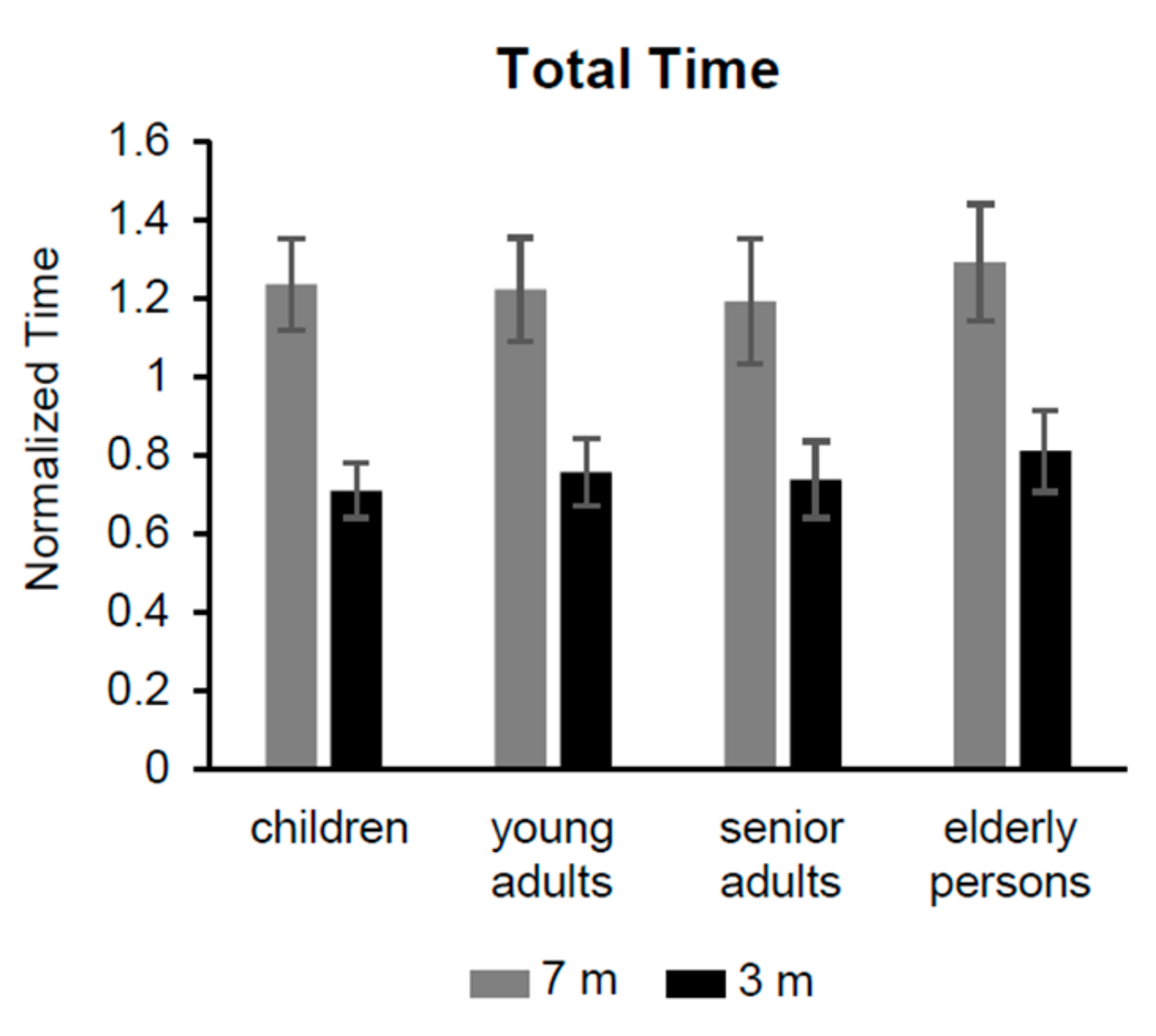
3.1. Changes in Total Time and Linear Subcomponents of iTUG
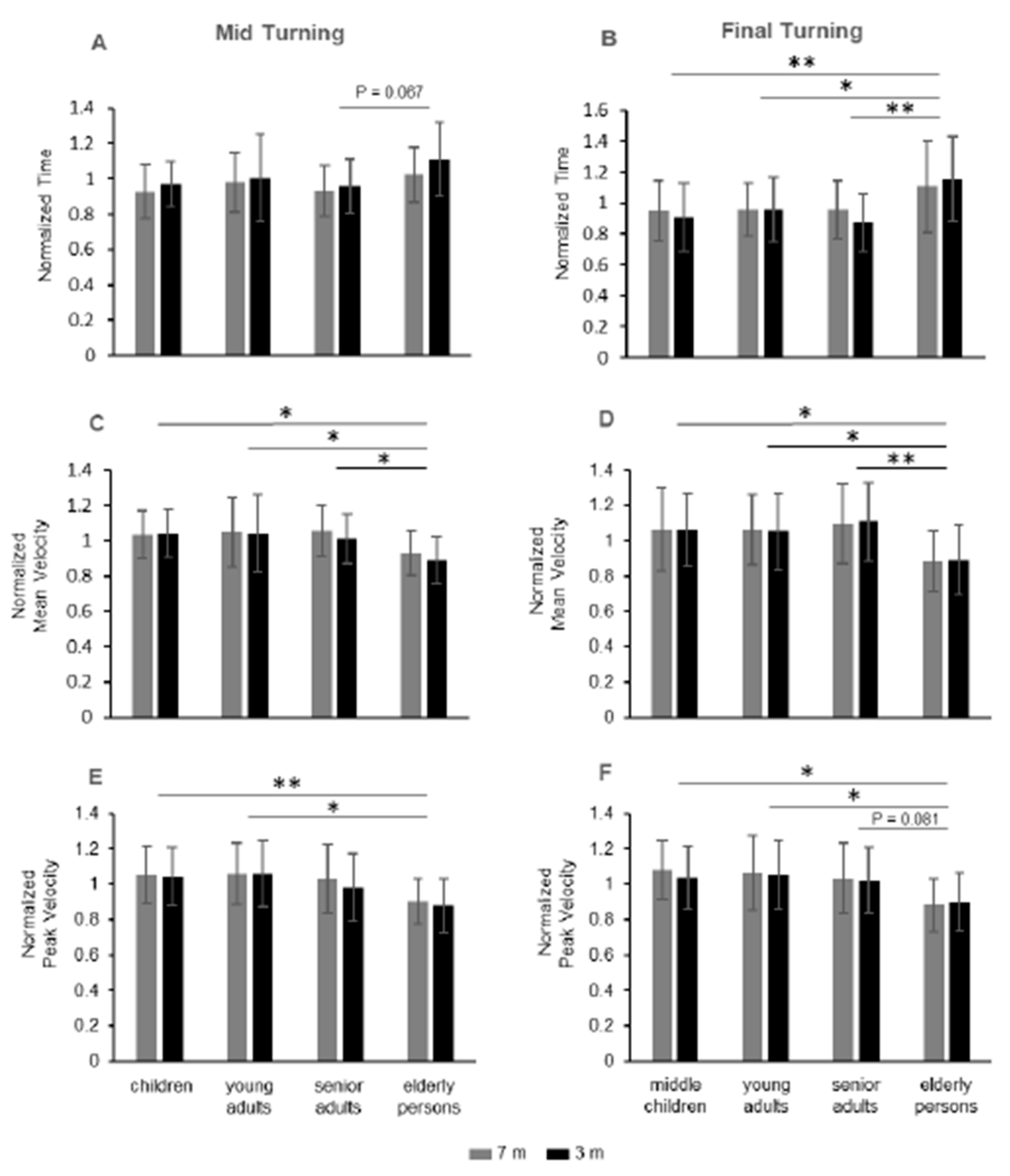
3.2. Changes in Duration and Velocity over the Turning Phases of iTUG
4. Discussion
4.1. The Effects of Age Observed by the iTUG Test
4.2. The Effects of Distance in Performing the iTUG Test
4.3. Benefits of Using Single Sensor to Perform the iTUG Test
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Tinetti, M.E. Performance-oriented assessment of mobility problems in elderly patients. J. Am. Geriatr. Soc. 1986, 34, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Lang, J.T.; Kassan, T.O.; Devaney, L.L.; Colon-Semenza, C.; Joseph, M.F. Test-Retest Reliability and Minimal Detectable Change for the 10-Meter Walk Test in Older Adults With Parkinson’s disease. J. Geriatr. Phys. Ther. 2016, 39, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Treacy, D.; Hassett, L. The Short Physical Performance Battery. J. Physiother. 2018, 64, 61. [Google Scholar] [CrossRef] [PubMed]
- Csuka, M.; McCarty, D.J. Simple method for measurement of lower extremity muscle strength. Am. J. Med. 1985, 78, 77–81. [Google Scholar] [CrossRef]
- Berg, K.; Wood-Dauphinee, S.; Williams, J.I.; Gayton, D. Measuring balance in the elderly: Preliminary development of an instrument. Physiother. Can. 1989, 41, 304–311. [Google Scholar] [CrossRef]
- Morris, M.E.; Huxham, F.; McGinley, J.; Dodd, K.; Iansek, R. The biomechanics and motor control of gait in Parkinson disease. Clin. Biomech. 2001, 16, 459–470. [Google Scholar] [CrossRef]
- Cioni, M.; Amata, O.; Seminara, M.R.; Marano, P.; Palermo, F.; Corallo, V. Responsiveness to sensory cues using the Timed Up and Go test in patients with Parkinson’s disease: A prospective cohort study. J. Rehabil. Med. 2015, 47, 824–829. [Google Scholar] [CrossRef]
- Hafsteinsdottir, T.B.; Rensik, M.; Schuurmans, M. Clinimetric properties of the Timed Up and Go Test for Patients With Stroke: A Systematic Review. Top Stroke Reabil. 2014, 21, 197–210. [Google Scholar] [CrossRef]
- Nilsagard, Y.; Lundholm, C.; Gunnarsson, L.G.; Dcnison, E. Clinical relevance using timed walk tests and ‘timed up and go’ testing in persons with multiple sclerosis. Physiother. Res. Int. 2007, 12, 105–114. [Google Scholar] [CrossRef]
- Kaya, P.; Alemdaroğlu, İ.; Yılmaz, Ö.; Karaduman, A.; Topaloğlu, H. Effect of muscle weakness distribution on balance in neuromuscular disease. Pediatrics Int. 2014, 57, 92–97. [Google Scholar] [CrossRef]
- Gan, S.M.; Tung, L.C.; Tang, Y.H.; Wang, C.H. Psychometric properties of functional balance assessment in children with cerebral palsy. Neurorehabil. Neural. Repair. 2008, 22, 745–753. [Google Scholar] [CrossRef] [PubMed]
- Carey, H.; Martin, K.; Combs-Miller, S.; Heathcock, J.C. Reliability and Responsiveness of the Timed Up and Go Test in Children With Cerebral Palsy. Pediatr. Phys. Ther. 2016, 28, 401–408. [Google Scholar] [CrossRef] [PubMed]
- Imms, F.J.; Edholm, O.G. Studies of gait and mobility in the elderly. Age Ageing 1981, 10, 147–156. [Google Scholar] [CrossRef] [PubMed]
- Thigpen, M.T.; Light, K.E.; Creel, G.L.; Flynn, S.M. Turning difficulty characteristics of adults aged 65 years or older. Phys. Ther. 2000, 80, 1174–1187. [Google Scholar] [CrossRef] [PubMed]
- Pondal, M.; Del Ser, T. Normative data and determinants for the timed "up and go" test in a population-based sample of elderly individuals without gait disturbances. J. Geriatr. Phys. Ther. 2008, 31, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Greene, B.R.; O’Donovan, A.; Romero-Ortuno, R.; Cogan, L.; Scanaill, C.N.; Kenny, R.A. Quantitative falls risk assessment using the timed up and go test. IEEE Trans. Biomed. Eng. 2010, 57, 2918–2926. [Google Scholar] [CrossRef] [PubMed]
- Habib, Z.; Westcott, S. Assessment of Anthropometric Factors on Balance Tests in Children. Pediatr. Phys. Ther. 1998, 10, 101–109. [Google Scholar] [CrossRef]
- Habib, Z.; Westcott, S.; Valvano, J. Assessment of Balance Abilities in Pakistani Children: A Cultural Perspective. Pediatr. Phys. Ther. 1999, 11, 73–82. [Google Scholar] [CrossRef]
- Nicolini-Panisson, R.D.; Donadio, M.V. Timed "Up & Go" test in children and adolescents. Rev. Paul. Pediatr. 2013, 31, 377–383. [Google Scholar] [CrossRef]
- Vervoort, D.; Vuillerme, N.; Kosse, N.; Hortobágyi, T.; Lamoth, C.J. Multivariate Analyses and Classification of Inertial Sensor Data to Identify Aging Effects on the Timed-Up-and-Go Test. PLoS ONE 2016, 11, e0155984. [Google Scholar] [CrossRef]
- Lara, J.; Godfrey, A.; Evans, E.; Heaven, B.; Brown, L.J.; Barron, E.; Mathers, J.C. Towards measurement of the Healthy Ageing Phenotype in lifestyle-based intervention studies. Maturitas 2013, 76, 189–199. [Google Scholar] [CrossRef] [PubMed]
- Zampieri, C.; Salarian, A.; Carlson-Kuhta, P.; Aminian, K.; Nutt, J.G.; Horak, F.B. The instrumented timed up and go test: Potential outcome measure for disease modifying therapies in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2010, 81, 171–176. [Google Scholar] [CrossRef] [PubMed]
- Bonnyaud, C.; Pradon, D.; Vuillerme, N.; Bensmail, D.; Roche, N. Spatiotemporal and Kinematic Parameters Relating to Oriented Gait and Turn Performance in Patients with Chronic Stroke. PLoS ONE 2015, 10, e0129821. [Google Scholar] [CrossRef] [PubMed]
- Weiss, A.; Mirelman, A.; Giladi, N.; Barnes, L.L.; Bennett, D.A.; Buchman, A.S.; Hausdorff, J.M. Transition Between the Timed up and Go Turn to Sit Subtasks: Is Timing Everything? J. Am. Med. Dir. Assoc. 2016, 17, 864.e9–864.e15. [Google Scholar] [CrossRef]
- Greene, B.R.; Caulfield, B.; Lamichhane, D.; Bond, W.; Svendsen, J.; Zurski, C.; Pratt, D. Longitudinal assessment of falls in patients with Parkinson’s disease using inertial sensors and the Timed Up and Go test. J. Rehabil. Assist. Technol. Eng. 2018, 5, 2055668317750811. [Google Scholar] [CrossRef]
- O’Brien, M.K.; Hidalgo-Araya, M.D.; Mummidisetty, C.K.; Vallery, H.; Ghaffari, R.; Rogers, J.A.; Jayaraman, A. Augmenting Clinical Outcome Measures of Gait and Balance with a Single Inertial Sensor in Age-Ranged Healthy Adults. Sensors 2019, 19, 4537. [Google Scholar] [CrossRef]
- Nishiguchi, S.; Yamada, M.; Nagai, K.; Mori, S.; Kajiwara, Y.; Sonoda, T.; Ito, T. Reliability and validity of gait analysis by android-based smartphone. Telemed. J. E Health. 2012, 18, 292–296. [Google Scholar] [CrossRef]
- Steins, D.; Sheret, I.; Dawes, H.; Esser, P.; Collett, J. A smart device inertial-sensing method for gait analysis. J. Biomech. 2014, 47, 3780–3785. [Google Scholar] [CrossRef]
- Medical Research Council. Aids to Examination of the Peripheral Nervous System; The White Rose Press: London, UK, 1976; Available online: https://mrc.ukri.org/documents/pdf/aids-to-the-examination-of-the-peripheral-nervous-system-mrc-memorandum-no-45-superseding-war-memorandum-no-7/ (accessed on 27 January 2020).
- Negrini, S.; Serpelloni, M.; Amici, C.; Gobbo, M.; Silvestro, C.; Buraschi, R.; Lopomo, N.F. Use of wearable inertial sensor in the assessment of Timed-Up-and-Go Test: Influence of device placement on temporal variable estimation. In Lecture Notes of the Institute for Computer Sciences, Social-Informatics and Telecommunications Engineering, Proceedings of the Wireless Mobile Communication and Healthcare, Mobihealth 2016, Milan, Italy, 14–16 November 2016; Springer International Publishing: Cham, Switzerland, 2017; Volume 192, pp. 310–317. [Google Scholar]
- Wahid, F.; Begg, R.; Lythgo, N.; Hass, C.J.; Halgamuge, S.; Ackland, D.C. A Multiple Regression Approach to Normalization of Spatiotemporal Gait Features. J. Appl. Biomech. 2016, 32, 128–139. [Google Scholar] [CrossRef]
- Pinzone, O.; Schwartz, M.H.; Baker, R. Comprehensive non-dimensional normalization of gait data. Gait Posture 2016, 44, 68–73. [Google Scholar] [CrossRef]
- Iosa, M.; Fusco, A.; Morone, G.; Paolucci, S. Development and decline of upright gait stability. Front. Aging Neurosci. 2014, 6, 14. [Google Scholar] [CrossRef]
- Berger, W.; Quintern, J.; Dietz, V. Development of bilateral coordination of stance and gait in children. Posture and Gait. In Proceedings of the 9th International Symposium on Postural and Gait Research, Marseille, France, 29 May–1 June; 1988; pp. 67–74. [Google Scholar]
- Pyykko, I.; Aalto, H.; Hytonen, M.; Starck, J.; Jantti, P.; Ramsay, H. Effect of age on postural control. Posture and Gait. In Proceedings of the 9th International Symposium on Postural and Gait Research, Marseille, France, 29 May–1 June; 1988; pp. 95–104. [Google Scholar]
- Assaiante, C. Action and representation of action during childhood and adolescence: A functional approach. Neurophysiol. Clin. 2012, 42, 43–51. [Google Scholar] [CrossRef]
- Orendurff, M.S.; Segal, A.D.; Berge, J.S.; Flick, K.C.; Spanier, D.; Klute, G.K. The kinematics and kinetics of turning: Limb asymmetries associated with walking a circular path. Gait Posture 2006, 23, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Conradsson, D.; Paquette, C.; Franzén, E. Medio-lateral stability during walking turns in older adults. PLoS ONE 2018, 13, e0198455. [Google Scholar] [CrossRef] [PubMed]
- Nolasco, L.A.; Silverman, A.K.; Gates, D.H. Whole-body and segment angular momentum during 90-degree turns. Gait Posture 2019, 70, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Paquette, M.R.; Fuller, J.R.; Adkin, A.L.; Vallis, L.A. Age-related modifications in steering behaviour: Effects of base-of-support constraints at the turn point. Exp. Brain Res. 2008, 190, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Godi, M.; Giardini, M.; Schieppati, M. Walking Along Curved Trajectories. Changes With Age and Parkinson’s Disease. Hints to Rehabilitation. Front Neurol. 2019, 10, 532. [Google Scholar] [CrossRef]
- Caronni, A.; Sterpi, I.; Antoniotti, P.; Aristidou, E.; Nicolaci, F.; Picardi, M.; Corbo, M. Criterion validity of the instrumented timed up and go test: A partial least square regression study. Gait Posture 2018, 61, 287–293. [Google Scholar] [CrossRef]
- Kanekar, N.; Aruin, A.S. Improvement of anticipatory postural adjustments for balance control: Effect of a single training session. J. Electromyogr. Kinesiol. 2015, 25, 400–405. [Google Scholar] [CrossRef]
- Smith, J.A.; Fisher, B.E. Anticipatory postural adjustments and spatial organization of motorcortex: Evidence of adaptive compensations in healthy older adults. J. Neurophysiol. 2018, 120, 2796–2805. [Google Scholar] [CrossRef]
- Xu, D.; Carlton, L.G.; Rosengren, K.S. Anticipatory postural adjustments for altering direction during walking. J. Mot. Behav. 2004, 36, 316–326. [Google Scholar] [CrossRef] [PubMed]
- Akram, S.B.; Frank, J.S.; Fraser, J. Effect of walking velocity on segment coordination during pre-planned turns in healthy older adults. Gait Posture 2010, 32, 211–214. [Google Scholar] [CrossRef] [PubMed]
- Fino, P.C.; Lockhart, T.E.; Fino, N.F. Corner height influences center of mass kinematics and path trajectory during turning. J. Biomech. 2015, 48, 104–112. [Google Scholar] [CrossRef]
- Bayot, M.; Dujardin, K.; Tard, C.; Defebvre, L.; Bonnet, C.T.; Allart, E.; Delval, A. The interaction between cognition and motor control: A theoretical framework for dual-task interference effects on posture, gait initiation, gait and turning. Neurophysiol. Clin. 2018, 48, 361–375. [Google Scholar] [CrossRef] [PubMed]
- Grasso, R.; Prévost, P.; Ivanenko, Y.P.; Berthoz, A. Eye-head coordination for the steering of locomotion in humans: An anticipatory synergy. Neurosci. Lett. 1998, 253, 115–118. [Google Scholar] [CrossRef]
- Hollands, M.A.; Patla, A.E.; Vickers, J.N. “Look where you’re going!”: Gaze behaviour associated with maintaining and changing the direction of locomotion. Exp. Brain Res. 2002, 143, 221–230. [Google Scholar] [CrossRef]
- Weerdesteyn, V.; Hollands, K.L.; Hollands, M.A. Gait adaptability. Handb. Clin. Neurol. 2018, 159, 135–146. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Groups | Age Range (years) | Age (years) | Weight (kg) | Height (cm) |
|---|---|---|---|---|
| Children | 7–12 | 9.27 ± 1.80 | 36.24 ± 10.08 | 139.68 ± 12.21 |
| Young adults | 31–40 | 34.15 ± 3.15 | 70.75 ± 11.66 | 167.63 ± 8.64 |
| Senior adults | 60–69 | 64.20 ± 2.98 | 74.09 ± 13.02 | 164.83 ± 7.39 |
| Elderly persons | 70–85 | 76.28 ± 4.06 | 71.56 ± 10.72 | 160.48 ± 10 |
| Temporal Parameters | Total Time (s) | Sit to Stand (s) | Walking Forward (s) | Mid Turning (s) | Walking Back (s) | Final Turning (s) | Stand to Sit (s) |
|---|---|---|---|---|---|---|---|
| 3-m iTUG | |||||||
| Children | 9.2 ± 0.8 | 1.2 ± 0.1 | 2.3 ± 0.4 | 1.6 ± 0.2 | 1.9 ± 0.3 | 1.2 ± 0.3 | 1.4 ± 0.3 |
| Young adults | 10.5 ± 1.1 | 1.4 ± 0.2 | 2.2 ± 0.4 | 2.1 ± 0.5 | 2.0 ± 0.6 | 1.6 ± 0.3 | 1.9 ± 0.4 |
| Senior adults | 10.5 ± 1.5 | 1.4 ± 0.2 | 2.3 ± 0.5 | 2.1 ± 0.3 | 2.1 ± 0.5 | 1.5 ± 0.3 | 1.8 ± 0.3 |
| Elderly persons | 11.4 ± 1.3 | 1.4 ± 0.2 | 2.5 ± 0.4 | 2.4 ± 0.4 | 2.2 ± 0.7 | 2.0 ± 0.5 | 1.9 ± 0.4 |
| Correlation with weight and height (r/p) | |||||||
| Un-normalized | 0.43/<0.001 | 0.44/<0.001 | 0.28/0.047 | 0.43/<0.001 | 0.20/0.199 | 0.43/<0.001 | 0.50/<0.001 |
| Normalized | 0.007/0.997 | 0.011/0.995 | 0.032/0.962 | 0.028/0.970 | 0.036/0.951 | 0.039/0.943 | 0.011/0.995 |
| 7-m iTUG | |||||||
| Children | 15.9 ± 1.4 | 1.2 ± 0.1 | 5.5 ± 0.8 | 1.6 ± 0.3 | 5.4 ± 0.4 | 1.3 ± 0.3 | 1.3 ± 0.3 |
| Young adults | 17.0 ± 1.7 | 1.4 ± 0.2 | 5.4 ± 0.7 | 2.1 ± 0.4 | 5.3 ± 0.6 | 1.6 ± 0.3 | 1.8 ± 0.4 |
| Senior adults | 17.0 ± 2.3 | 1.4 ± 0.2 | 5.5 ± 1.1 | 2.0 ± 0.3 | 5.3 ± 0.9 | 1.6 ± 0.3 | 1.7 ± 0.2 |
| Elderly persons | 18.1 ± 2.0 | 1.4 ± 0.2 | 5.9 ± 0.9 | 2.2 ± 0.3 | 5.7 ± 0.9 | 1.9 ± 0.4 | 2.0 ± 0.5 |
| Correlation with weight and height (r/p) | |||||||
| Un-normalized | 0.32/0.019 | 0.46/<0.001 | 0.23/0.122 | 0.53/<0.001 | 0.30/0.031 | 0.40/0.001 | 0.50/<0.001 |
| Normalized | 0.022/0.981 | 0.003/1 | 0.029/0.967 | 0.044/0.930 | 0.037/0.949 | 0.027/0.973 | 0.037/0.950 |
| Velocity Parameters | Average Mid Turning (°/s) | Peak Mid Turning (°/s) | Average Final Turning (°/s) | Peak Final Turning (°/s) |
|---|---|---|---|---|
| 3-m iTUG | ||||
| Children | 102.8 ± 14.2 | 205.6 ± 32.7 | 132.6 ± 26.2 | 255.7 ± 39.9 |
| Young adults | 84.3 ± 15.8 | 164.8 ± 23.6 | 104.7 ± 18.5 | 199.6 ± 30.98 |
| Senior adults | 84.7 ± 9.9 | 146.0 ± 25.1 | 105.0 ± 21.1 | 189.3 ± 36.2 |
| Elderly persons | 72.5 ± 10.3 | 134.4 ± 20.3 | 84.5 ± 19.9 | 168.4 ± 31.9 |
| Multiple regression with weight and height (r/p) | ||||
| Un-normalized | 0.52/<0.001 | 0.59/<0.001 | 0.54/<0.001 | 0.60/<0.001 |
| Normalized | 0.038/0.945 | 0.062/0.863 | 0.050/0.908 | 0.029/0.969 |
| 7-m iTUG | ||||
| Children | 102.2 ± 15.83 | 207.8 ± 37.83 | 134.5 ± 26.8 | 268.29 ± 40.5 |
| Young adults | 84.9 ± 14.4 | 164.6 ± 19.5 | 105.6 ± 16.5 | 202.5 ± 36.81 |
| Senior adults | 84.2 ± 9.9 | 152.9 ± 23.7 | 103.6 ± 18.6 | 191.07 ± 35.0 |
| Elderly persons | 76.9 ± 10.0 | 138.5 ± 18.9 | 85.8 ± 14.5 | 167.6 ± 24.1 |
| Multiple regression with weight and height (r/p) | ||||
| Un-normalized | 0.53/<0.001 | 0.63/<0.001 | 0.53/<0.001 | 0.65/<0.001 |
| Normalized | 0.04/0.941 | 0.075/0.804 | 0.041/0.938 | 0.053/0.896 |
| Parameters | Groups df: 3.76 | Distances df: 1.76 | Groups X Distances df: 3.76 | |||
|---|---|---|---|---|---|---|
| F | p | F | p | F | p | |
| 1. Total time | 2.461 | 0.069 | 3617.228 | <0.001 | 3.648 | 0.016 |
| 2. Sit to stand duration | 0.155 | 0.926 | 0.423 | 0.518 | 0.115 | 0.951 |
| 3. Walking forward duration | 1.821 | 0.150 | 1982.924 | <0.001 | 0.178 | 0.911 |
| 4. Walking back duration | 0.477 | 0.699 | 2778.295 | <0.001 | 1.768 | 0.161 |
| 5. Stand to sit duration | 0.811 | 0.492 | 2.700 | 0.104 | 0.428 | 0.734 |
| 6. Mid turning duration | 2.409 | 0.040 | 5.322 | 0.024 | 0.630 | 0.598 |
| 7. Final turning duration | 5.690 | 0.001 | 0.653 | 0.422 | 1.109 | 0.351 |
| 8. Average mid turning velocity | 4.081 | 0.010 | 2.719 | 0.103 | 1.117 | 0.347 |
| 9. Average final turning velocity | 5.288 | 0.002 | 0.057 | 0.940 | 0.053 | 0.984 |
| 10. Peak mid turning velocity | 4.741 | 0.004 | 1.910 | 0.171 | 0.535 | 0.659 |
| 11. Peak final turning velocity | 4.503 | 0.006 | 0.265 | 0.264 | 1.069 | 0.367 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mangano, G.R.A.; Valle, M.S.; Casabona, A.; Vagnini, A.; Cioni, M. Age-Related Changes in Mobility Evaluated by the Timed Up and Go Test Instrumented through a Single Sensor. Sensors 2020, 20, 719. https://doi.org/10.3390/s20030719
Mangano GRA, Valle MS, Casabona A, Vagnini A, Cioni M. Age-Related Changes in Mobility Evaluated by the Timed Up and Go Test Instrumented through a Single Sensor. Sensors. 2020; 20(3):719. https://doi.org/10.3390/s20030719
Chicago/Turabian StyleMangano, Giulia R.A., Maria S. Valle, Antonino Casabona, Alessandro Vagnini, and Matteo Cioni. 2020. "Age-Related Changes in Mobility Evaluated by the Timed Up and Go Test Instrumented through a Single Sensor" Sensors 20, no. 3: 719. https://doi.org/10.3390/s20030719
APA StyleMangano, G. R. A., Valle, M. S., Casabona, A., Vagnini, A., & Cioni, M. (2020). Age-Related Changes in Mobility Evaluated by the Timed Up and Go Test Instrumented through a Single Sensor. Sensors, 20(3), 719. https://doi.org/10.3390/s20030719