Breath Acetone Measurement-Based Prediction of Exercise-Induced Energy and Substrate Expenditure




Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Protocol
2.3. Measurements
2.3.1. Anthropometric Measurements
2.3.2. Cardiopulmonary Exercise Test
2.3.3. BrAce Analyzer
2.3.4. Blood Sampling
2.3.5. Statistical Analysis
3. Results
3.1. Characteristics of the Participants
3.2. Energy Expenditure and Substrate Oxidation at Rest, During and after Exercise
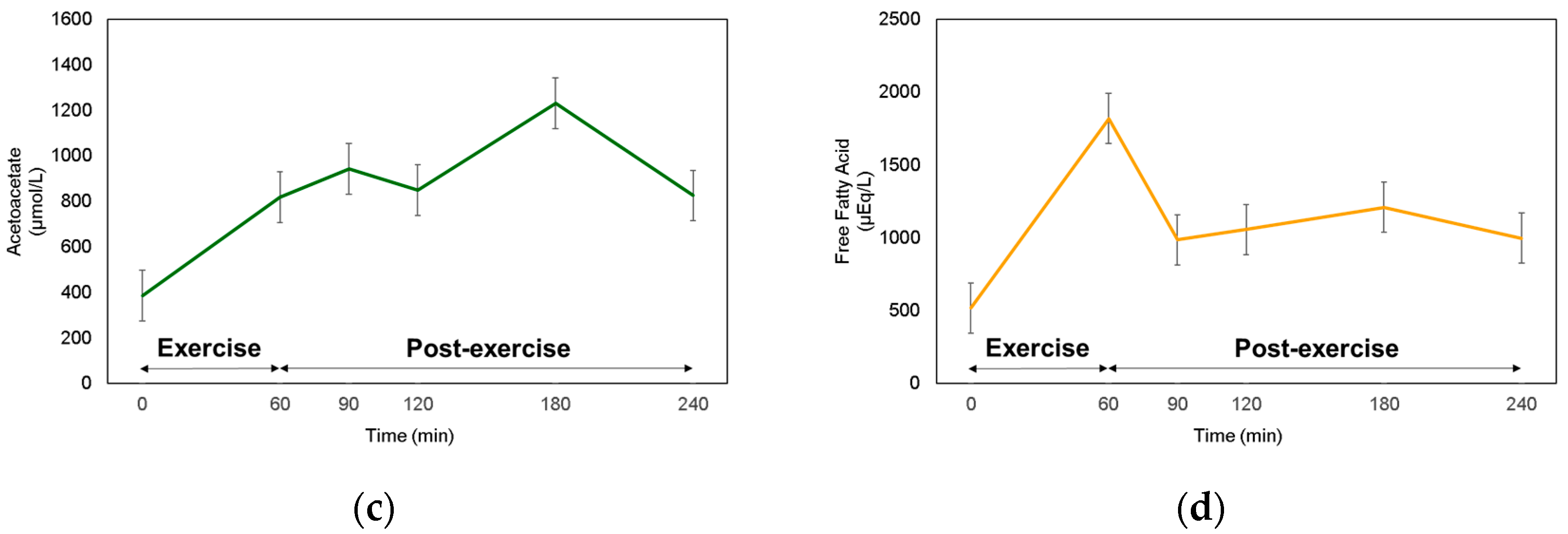
3.3. BrAce and Blood Ketone at Rest, during, and after Exercise
3.4. Correlation between BrAce, Blood Ketone, and RER
3.5. Predictability of Lipid Oxidation Using Breath Acetone
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Collaborators, G.B.D.O.; Afshin, A.; Forouzanfar, M.H.; Reitsma, M.B.; Sur, P.; Estep, K.; Lee, A.; Marczak, L.; Mokdad, A.H.; Moradi-Lakeh, M.; et al. Health effects of overweight and obesity in 195 countries over 25 years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar] [CrossRef]
- Gami, A.S.; Witt, B.J.; Howard, D.E.; Erwin, P.J.; Gami, L.A.; Somers, V.K.; Montori, V.M. Metabolic syndrome and risk of incident cardiovascular events and death: A systematic review and meta-analysis of longitudinal studies. J. Am. Coll. Cardiol. 2007, 49, 403–414. [Google Scholar] [CrossRef]
- Mokdad, A.H.; Ford, E.S.; Bowman, B.A.; Dietz, W.H.; Vinicor, F.; Bales, V.S.; Marks, J.S. Prevalence of obesity, diabetes, and obesity-related health risk factors, 2001. JAMA 2003, 289, 76–79. [Google Scholar] [CrossRef] [PubMed]
- Must, A.; Spadano, J.; Coakley, E.H.; Field, A.E.; Colditz, G.; Dietz, W.H. The disease burden associated with overweight and obesity. JAMA 1999, 282, 1523–1529. [Google Scholar] [CrossRef] [PubMed]
- Burton, W.N.; Chen, C.Y.; Schultz, A.B.; Edington, D.W. The economic costs associated with body mass index in a workplace. J. Occup. Environ. Med. 1998, 40, 786–792. [Google Scholar] [CrossRef] [PubMed]
- Thompson, D.; Wolf, A.M. The medical-care cost burden of obesity. Obes. Rev. 2001, 2, 189–197. [Google Scholar] [CrossRef]
- Horton, T.J.; Hill, J.O. Exercise and obesity. Proc. Nutr. Soc. 1998, 57, 85–91. [Google Scholar] [CrossRef]
- Poirier, P.; Despres, J.P. Exercise in weight management of obesity. Cardiol. Clin. 2001, 19, 459–470. [Google Scholar] [CrossRef]
- Danforth, E., Jr. Diet and obesity. Am. J. Clin. Nutr. 1985, 41, 1132–1145. [Google Scholar] [CrossRef]
- Venables, M.C.; Achten, J.; Jeukendrup, A.E. Determinants of fat oxidation during exercise in healthy men and women: A cross-sectional study. J. Appl Physiol. 2005, 98, 160–167. [Google Scholar] [CrossRef]
- Case, M.A.; Burwick, H.A.; Volpp, K.G.; Patel, M.S. Accuracy of smartphone applications and wearable devices for tracking physical activity data. JAMA 2015, 313, 625–626. [Google Scholar] [CrossRef] [PubMed]
- Evenson, K.R.; Goto, M.M.; Furberg, R.D. Systematic review of the validity and reliability of consumer-wearable activity trackers. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 159. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.C. Measuring breath acetone for monitoring fat loss: Review. Obesity (Silver Spring) 2015, 23, 2327–2334. [Google Scholar] [CrossRef] [PubMed]
- Kundu, S.K.; Bruzek, J.A.; Nair, R.; Judilla, A.M. Breath acetone analyzer: Diagnostic tool to monitor dietary fat loss. Clin. Chem. 1993, 39, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Charles, R.A.; Bee, Y.M.; Eng, P.H.; Goh, S.Y. Point-of-care blood ketone testing: Screening for diabetic ketoacidosis at the emergency department. Singap. Med. J. 2007, 48, 986–989. [Google Scholar]
- Kalapos, M.P. On the mammalian acetone metabolism: From chemistry to clinical implications. Biochim. Biophys. Acta 2003, 1621, 122–139. [Google Scholar] [CrossRef]
- Laffel, L. Ketone bodies: A review of physiology, pathophysiology and application of monitoring to diabetes. Diabetes Metab. Res. Rev. 1999, 15, 412–426. [Google Scholar] [CrossRef]
- Toyooka, T.; Hiyama, S.; Yamada, Y. A prototype portable breath acetone analyzer for monitoring fat loss. J. Breath Res. 2013, 7, 036005. [Google Scholar] [CrossRef]
- Saasa, V.; Beukes, M.; Lemmer, Y.; Mwakikunga, B. Blood ketone bodies and breath acetone analysis and their correlations in type 2 diabetes mellitus. Diagnostics 2019, 9, 224. [Google Scholar] [CrossRef]
- Guntner, A.T.; Kompalla, J.F.; Landis, H.; Theodore, S.J.; Geidl, B.; Sievi, N.A.; Kohler, M.; Pratsinis, S.E.; Gerber, P.A. Guiding ketogenic diet with breath acetone sensors. Sensors 2018, 18, 3655. [Google Scholar] [CrossRef]
- Guntner, A.T.; Sievi, N.A.; Theodore, S.J.; Gulich, T.; Kohler, M.; Pratsinis, S.E. Noninvasive body fat burn monitoring from exhaled acetone with Si-doped WO3-sensing nanoparticles. Anal. Chem. 2017, 89, 10578–10584. [Google Scholar] [CrossRef] [PubMed]
- Jung, H.; Cho, W.; Yoo, R.; Lee, H.S.; Choe, Y.S.; Jeon, J.Y.; Lee, W. Highly selective real-time detection of breath acetone by using ZnO quantum dots with a miniaturized gas chromatographic column. Sens. Actuat. B Chem. 2018, 274, 527–532. [Google Scholar] [CrossRef]
- Thomas, S.; Reading, J.; Shephard, R.J. Revision of the physical activity readiness questionnaire (PAR-Q). Can. J. Sport Sci. 1992, 17, 338–345. [Google Scholar] [PubMed]
- Koeslag, J.H.; Noakes, T.D.; Sloan, A.W. Post-exercise ketosis. J. Physiol. 1980, 301, 79–90. [Google Scholar] [CrossRef]
- Peronnet, F.; Massicotte, D. Table of nonprotein respiratory quotient: An update. Can. J. Sport Sci. 1991, 16, 23–29. [Google Scholar]
- Gibson, A.L.; Holmes, J.C.; Desautels, R.L.; Edmonds, L.B.; Nuudi, L. Ability of new octapolar bioimpedance spectroscopy analyzers to predict 4-component-model percentage body fat in Hispanic, black, and white adults. Am. J. Clin. Nutr. 2008, 87, 332–338. [Google Scholar] [CrossRef]
- Ling, C.H.; de Craen, A.J.; Slagboom, P.E.; Gunn, D.A.; Stokkel, M.P.; Westendorp, R.G.; Maier, A.B. Accuracy of direct segmental multi-frequency bioimpedance analysis in the assessment of total body and segmental body composition in middle-aged adult population. Clin. Nutr. 2011, 30, 610–615. [Google Scholar] [CrossRef]
- McLester, C.N.; Nickerson, B.S.; Kliszczewicz, B.M.; McLester, J.R. Reliability and agreement of various inbody body composition analyzers as compared to dual-energy X-ray absorptiometry in healthy men and women. J. Clin. Densitom. 2020, 23, 443–450. [Google Scholar] [CrossRef]
- Bruce, R.A.; Lovejoy, F.W.; Pearson, R.; Paul, N.G.; Brothers, G.B.; Velasquez, T. Normal respiratory and circulatory pathways of adaptation in exercise. J. Clin. Investig. 1949, 28, 1423–1430. [Google Scholar] [CrossRef]
- Bruce, R.A.; Pearson, R.; Lovejoy, F.W.; Paul, N.G.; Brothers, G.B. Variability of respiratory and circulatory performance during standardized exercise. J. Clin. Investig. 1949, 28, 1431–1438. [Google Scholar] [CrossRef]
- Choe, Y.S. Apparatus and Method of Analyzing Constituents of Gas in Oral Cavity and Alveolar Gas. U.S. Patent US9144396B2, 26 February 2009. [Google Scholar]
- Musa-Veloso, K.; Likhodii, S.S.; Cunnane, S.C. Breath acetone is a reliable indicator of ketosis in adults consuming ketogenic meals. Am. J. Clin. Nutr. 2002, 76, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Musa-Veloso, K.; Likhodii, S.S.; Rarama, E.; Benoit, S.; Liu, Y.M.C.; Chartrand, D.; Curtis, R.; Carmant, L.; Lortie, A.; Comeau, F.J.E. Breath acetone predicts plasma ketone bodies in children with epilepsy on a ketogenic diet. Nutrition 2006, 22, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Qiao, Y.; Gao, Z.; Liu, Y.; Cheng, Y.; Yu, M.; Zhao, L.; Duan, Y.; Liu, Y. Breath ketone testing: A new biomarker for diagnosis and therapeutic monitoring of diabetic ketosis. Biomed. Res. Int. 2014, 2014, 869186. [Google Scholar] [CrossRef]
- Rooth, G.; Carlstrom, S. Therapeutic fasting. Acta Med. Scand. 1970, 187, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Tassopoulos, C.N.; Barnett, D.; Fraser, T.R. Breath-acetone and blood-sugar measurements in diabetes. Lancet 1969, 1, 1282–1286. [Google Scholar] [CrossRef]
- Prabhakar, A.; Quach, A.; Wang, D.; Zhang, H.; Terrera, M.; Jackemeyer, D.; Xian, X.; Tsow, F.; Tao, N.; Forzani, E. Breath acetone as biomarker for lipid oxidation and early ketone detection. Glob. J. Obes. Diabetes Metab. Syndr. 2014, 1, 12. [Google Scholar]
- Brooks, G.A.; Mercier, J. Balance of carbohydrate and lipid utilization during exercise: The “crossover” concept. J. Appl. Physiol. 1994, 76, 2253–2261. [Google Scholar] [CrossRef]
- Achten, J.; Jeukendrup, A.E. Optimizing fat oxidation through exercise and diet. Nutrition 2004, 20, 716–727. [Google Scholar] [CrossRef]
- Brooks, G.A.; Trimmer, J.K. Glucose kinetics during high-intensity exercise and the crossover concept. J. Appl. Physiol. 1996, 80, 1073–1075. [Google Scholar] [CrossRef]
- Bahr, R.; Ingnes, I.; Vaage, O.; Sejersted, O.M.; Newsholme, E.A. Effect of duration of exercise on excess postexercise O-2 consumption. J. Appl. Physiol. 1987, 62, 485–490. [Google Scholar] [CrossRef]
- Warren, A.; Howden, E.J.; Williams, A.D.; Fell, J.W.; Johnson, N.A. Postexercise fat oxidation: Effect of exercise duration, intensity, and modality. Int. J. Sport Nutr. Exe. 2009, 19, 607–623. [Google Scholar] [CrossRef] [PubMed]
- Bovey, F.; Cros, J.; Tuzson, B.; Seyssel, K.; Schneiter, P.; Emmenegger, L.; Tappy, L. Breath acetone as a marker of energy balance: An exploratory study in healthy humans. Nutr. Diabetes 2018, 8, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.W.; Manini, A.F.; Szekely, T.; Hoffman, R.S. Bedside detection of urine beta-hydroxybutyrate in diagnosing metabolic acidosis. Acad. Emerg. Med. 2008, 15, 751–756. [Google Scholar] [CrossRef] [PubMed]
- The UK Biobank Submaximal Cycle Ergometer Test for Assessment of Cardiorespiratory Fitness: Validity, Reliability, and Association with Disease Outcomes. Available online: https://www.medrxiv.org/content/10.1101/2020.09.29.20203828v1.full.pdf+html (accessed on 25 November 2020).
- Hong, S.H.; Yang, H.I.; Kim, D.I.; Gonzales, T.I.; Brage, S.; Jeon, J.Y. Validation of submaximal step tests and the 6-min walk test for predicting maximal oxygen consumption in young and healthy participants. Int. J. Environ. Res. Public Health 2019, 16, 4858. [Google Scholar] [CrossRef]
- Resting Heart Rate as a Biomarker for Tracking Change in Cardiorespiratory Fitness of UK Adults: The Fenland Study. Available online: https://www.medrxiv.org/content/10.1101/2020.07.01.20144154v1.full.pdf+html (accessed on 25 November 2020).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total (n = 6) |
|---|---|
| Age (years) | 27.0 ± 1.8 |
| Height (cm) | 178.9 ± 5.3 |
| Weight (kg) | 79.6 ± 8.8 |
| Body Mass Index (kg/m2) | 24.4 ± 1.3 |
| Skeletal Muscle Mass (kg) | 39.2 ± 4.5 |
| Body Fat Mass (kg) | 11.6 ± 1.5 |
| Body Fat Percent (%) | 14.5 ± 0.9 |
| VO2max (mL/kg/min) | 51.7 ± 3.7 |
| Period | Total | Carbohydrate | Lipid | ||
|---|---|---|---|---|---|
| kcal/h | kcal/h | % | kcal/h | % | |
| Resting | 76.3 ± 5.4 | 26.3 ± 6.3 | 35.8 ± 5.2 | 50.0 ± 5.2 | 64.2 ± 5.2 |
| Exercise (1 h) | 751.6 ± 45.8 | 419.8 ± 53.2 | 52.8 ± 4.7 | 331.8 ± 30.5 | 47.2 ± 4.7 |
| Post-Ex 1 h | 106.3 ± 7.6 | 23.6 ± 6.6 | 20.4 ± 5.2 | 82.7 ± 7.0 | 79.6 ± 5.2 |
| Post-Ex 2 h | 103.8 ± 7.9 | 23.8 ± 6.4 | 20.8 ± 4.6 | 80.0 ± 5.4 | 79.2 ± 4.6 |
| Post-Ex 3 h | 99.1 ± 9.9 | 28.2 ± 9.6 | 25.8 ± 6.8 | 70.9 ± 6.7 | 74.2 ± 6.8 |
| Adjusted R2 | SEE | ΔF | Intercept | BrAce | BMI | VO2max | ||
|---|---|---|---|---|---|---|---|---|
| At rest | Model 1 | 0.667 | 7.376 | 11.015 * | 38.498 * | 2.576 * | ||
| Model 2 | 0.584 | 8.251 | 4.503 | 25.667 | 2.640 | 0.514 | ||
| Model 3 | 0.972 | 2.143 | 58.677 * | −331.492 * | 3.800 * | 8.689 * | 2.951 * | |
| Post-Ex 1 h | Model 1 | 0.486 | 10.619 | 5.736 | 60.247 * | 2.598 | ||
| Model 2 | 0.546 | 9.986 | 4.005 | 104.339 | 2.317 | −1.743 | ||
| Model 3 | 0.917 | 4.260 | 19.502 * | −241.492 | 2.945 * | 6.183 | 2.883 | |
| Post-Ex 2 h | Model 1 | 0.276 | 12.770 | 2.904 | 58.323 * | 2.163 | ||
| Model 2 | 0.054 | 14.598 | 1.141 | 43.198 | 2.363 | 0.569 | ||
| Model 3 | 0.284 | 12.697 | 1.661 | −449.706 | 4.064 | 12.129 | 3.876 | |
| Post-Ex 3 h | Model 1 | 0.275 | 19.113 | 2.899 | 39.971 | 2.686 | ||
| Model 2 | 0.340 | 18.243 | 2.287 | −55.024 | 3.804 | 3.509 | ||
| Model 3 | 0.070 | 21.655 | 1.125 | −223.727 | 4.066 | 7.428 | 1.372 | |
| Equations | ||||||||
| Fat oxidation at rest | y = −331.492 + 3.800X1 + 8.689X2 + 2.951X3 | |||||||
| Fat oxidation during 3 h of recovery | y = −241.492 + 2.945X1 + 6.183X2 + 2.883X3 | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, M.J.; Hong, S.H.; Cho, W.; Park, D.-H.; Lee, E.-B.; Song, Y.; Choe, Y.-S.; Lee, J.H.; Jang, Y.; Lee, W.; et al. Breath Acetone Measurement-Based Prediction of Exercise-Induced Energy and Substrate Expenditure. Sensors 2020, 20, 6878. https://doi.org/10.3390/s20236878
Kim MJ, Hong SH, Cho W, Park D-H, Lee E-B, Song Y, Choe Y-S, Lee JH, Jang Y, Lee W, et al. Breath Acetone Measurement-Based Prediction of Exercise-Induced Energy and Substrate Expenditure. Sensors. 2020; 20(23):6878. https://doi.org/10.3390/s20236878
Chicago/Turabian StyleKim, Min Jae, Sung Hyun Hong, Wonhee Cho, Dong-Hyuk Park, Eun-Byeol Lee, Yoonkyung Song, Yong-Sahm Choe, Jun Ho Lee, Yeonji Jang, Wooyoung Lee, and et al. 2020. "Breath Acetone Measurement-Based Prediction of Exercise-Induced Energy and Substrate Expenditure" Sensors 20, no. 23: 6878. https://doi.org/10.3390/s20236878
APA StyleKim, M. J., Hong, S. H., Cho, W., Park, D.-H., Lee, E.-B., Song, Y., Choe, Y.-S., Lee, J. H., Jang, Y., Lee, W., & Jeon, J. Y. (2020). Breath Acetone Measurement-Based Prediction of Exercise-Induced Energy and Substrate Expenditure. Sensors, 20(23), 6878. https://doi.org/10.3390/s20236878