Frontal EEG Changes with the Recovery of Carotid Blood Flow in a Cardiac Arrest Swine Model


Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Statement
2.2. Study Design and Setting
2.3. Experimental Animals and Housing
2.4. Surgical Preparation and Hemodynamic Measurements
2.5. EEG Measurement
2.6. Data Processing
2.7. Data Analysis
3. Results
3.1. Results of CPR Process
3.2. EEG Changes with the Recovery of CBF
3.3. Changes in EEG Parameters Depending on Four CBF Groups
3.4. EEG Parameters Depending on the Different CBF Recovery Groups
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Benjamin, E.J.; Blaha, M.J.; Chiuve, S.E.; Cushman, M.; Das, S.R.; Deo, R.; Floyd, J.; Fornage, M.; Gillespie, C.; Isasi, C. Heart disease and stroke statistics-2017 update: A report from the American Heart Association. Circulation 2017, 135, e146–e603. [Google Scholar] [CrossRef] [PubMed]
- Chan, P.S.; McNally, B.; Tang, F.; Kellermann, A. Recent trends in survival from out-of-hospital cardiac arrest in the United States. Circulation 2014, 130, 1876–1882. [Google Scholar] [CrossRef] [PubMed]
- Daya, M.R.; Schmicker, R.H.; Zive, D.M.; Rea, T.D.; Nichol, G.; Buick, J.E.; Brooks, S.; Christenson, J.; MacPhee, R.; Craig, A. Out-of-hospital cardiac arrest survival improving over time: Results from the Resuscitation Outcomes Consortium (ROC). Resuscitation 2015, 91, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Cummins, R.O.; Ornato, J.P.; Thies, W.H.; Pepe, P.E. Improving survival from sudden cardiac arrest: The “chain of survival” concept. A statement for health professionals from the Advanced Cardiac Life Support Subcommittee and the Emergency Cardiac Care Committee, American Heart Association. Circulation 1991, 83, 1832–1847. [Google Scholar] [CrossRef] [PubMed]
- Iwami, T.; Nichol, G.; Hiraide, A.; Hayashi, Y.; Nishiuchi, T.; Kajino, K.; Morita, H.; Yukioka, H.; Ikeuchi, H.; Sugimoto, H.; et al. Continuous Improvements in “Chain of Survival” Increased Survival After Out-of-Hospital Cardiac Arrests. Circulation 2009, 119, 728–734. [Google Scholar] [CrossRef]
- Hartmann, S.M.; Farris, R.W.; Di Gennaro, J.L.; Roberts, J.S. Systematic review and meta-analysis of end-tidal carbon dioxide values associated with return of spontaneous circulation during cardiopulmonary resuscitation. J. Intensive Care Med. 2015, 30, 426–435. [Google Scholar] [CrossRef]
- Moulaert, V.R.; Verbunt, J.A.; van Heugten, C.M.; Wade, D.T. Cognitive impairments in survivors of out-of-hospital cardiac arrest: A systematic review. Resuscitation 2009, 80, 297–305. [Google Scholar] [CrossRef]
- Torgersen, J.; Strand, K.; Bjelland, T.; Klepstad, P.; Kvåle, R.; Søreide, E.; Wentzel-Larsen, T.; Flaatten, H. Cognitive dysfunction and health-related quality of life after a cardiac arrest and therapeutic hypothermia. Acta Anaesthesiol. Scand. 2010, 54, 721–728. [Google Scholar] [CrossRef]
- Berka, C.; Levendowski, D.J.; Cvetinovic, M.M.; Petrovic, M.M.; Davis, G.; Lumicao, M.N.; Zivkovic, V.T.; Popovic, M.V.; Olmstead, R. Real-Time Analysis of EEG Indexes of Alertness, Cognition, and Memory Acquired With a Wireless EEG Headset. Int. J. Hum.–Comput. Interact. 2004, 17, 151–170. [Google Scholar] [CrossRef]
- Moss, J.; Rockoff, M. EEG monitoring during cardiac arrest and resuscitation. JAMA 1980, 244, 2750–2751. [Google Scholar] [CrossRef]
- England, M.R. The changes in bispectral index during a hypovolemic cardiac arrest. Anesthesiology 1999, 91, 1947. [Google Scholar] [CrossRef] [PubMed]
- Aminoff, M.J.; Scheinman, M.M.; Griffin, J.C.; Herre, J.M. Electrocerebral accompaniments of syncope associated with malignant ventricular arrhythmias. Ann. Intern. Med. 1988, 108, 791–796. [Google Scholar] [CrossRef]
- De Vries, J.W.; Bakker, P.F.; Visser, G.H.; Diephuis, J.C.; van Huffelen, A.C. Changes in cerebral oxygen uptake and cerebral electrical activity during defibrillation threshold testing. Anesth. Analg. 1998, 87, 16–20. [Google Scholar] [PubMed]
- Pana, R.; Hornby, L.; Shemie, S.; Dhanani, S.; Teitelbaum, J. Time to loss of brain function and activity during circulatory arrest. J. Crit. Care 2016, 34, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Losasso, T.J.; Muzzi, D.A.; Meyer, F.B.; Sharbrough, F.W. Electroencephalographic monitoring of cerebral function during asystole and successful cardiopulmonary resuscitation. Anesth. Analg. 1992, 75, 1021–1024. [Google Scholar] [CrossRef] [PubMed]
- Schäuble, B.; Klass, D.W.; Westmoreland, B.F. Resuscitation artifacts during electroencephalography. Am. J. Electroneurodiagn. Technol. 2002, 42, 16–21. [Google Scholar] [CrossRef]
- Azim, N.; Wang, C. The use of bispectral index during a cardiopulmonary arrest: A potential predictor of cerebral perfusion. Anaesthesia 2004, 59, 610–612. [Google Scholar] [CrossRef]
- Feng, G.; Jiang, G.; Li, Z.; Wang, X. Prognostic value of electroencephalography (EEG) for brain injury after cardiopulmonary resuscitation. Neurol. Sci. 2016, 37, 843–849. [Google Scholar] [CrossRef]
- Reagan, E.M.; Nguyen, R.T.; Ravishankar, S.T.; Chabra, V.; Fuentes, B.; Spiegel, R.; Parnia, S. Monitoring the Relationship Between Changes in Cerebral Oxygenation and Electroencephalography Patterns During Cardiopulmonary Resuscitation: A Feasibility Study. Crit. Care Med. 2018, 46, 757–763. [Google Scholar] [CrossRef]
- Mullie, A.; Lewi, P.; Van Hoeyweghen, R.; Group, C.R.S. Pre-CPR conditions and the final outcome of CPR. Resuscitation 1989, 17, S11–S21. [Google Scholar] [CrossRef]
- Wei, L.; Yu, T.; Gao, P.; Quan, W.; Li, Y. Detection of Spontaneous Pulse Using Acceleration Signals Acquired From CPR Feedback Sensor in Porcine Model of Cardiac Arrest. Circulation 2016, 134 (Suppl. 1), A12827. [Google Scholar] [CrossRef] [PubMed]
- Peberdy, M.A.; Callaway, C.W.; Neumar, R.W.; Geocadin, R.G.; Zimmerman, J.L.; Donnino, M.; Gabrielli, A.; Silvers, S.M.; Zaritsky, A.L.; Merchant, R. Part 9: Post–cardiac arrest care: 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 2010, 122 (Suppl. 3), S768. [Google Scholar] [CrossRef] [PubMed]
- Council, N.R. Guide for the Care and Use of Laboratory Animals; National Academies Press: Washington, DC, USA, 2010. [Google Scholar]
- Rampil, I.J. A primer for EEG signal processing in Anesthesia. Anesthesiol. Phila. Hagerstown 1998, 89, 980–1002. [Google Scholar] [CrossRef] [PubMed]
- Raghu, S.; Sriraam, N.; Kumar, G.P. Classification of epileptic seizures using wavelet packet log energy and norm entropies with recurrent Elman neural network classifier. Cogn. Neurodyn. 2017, 11, 51–66. [Google Scholar] [CrossRef]
- Acharya, U.R.; Fujita, H.; Sudarshan, V.K.; Bhat, S.; Koh, J.E. Application of entropies for automated diagnosis of epilepsy using EEG signals: A review. Knowl.-Based Syst. 2015, 88, 85–96. [Google Scholar] [CrossRef]
- Foreman, B.; Claassen, J. Quantitative EEG for the detection of brain ischemia. Crit. Care 2012, 16, 216. [Google Scholar] [CrossRef]
- Bhalala, U.; Polglase, G.; Dempsey, E. Editorial: Neonatal and Pediatric Cerebro-Cardio-Pulmonary Resuscitation (CCPR): Where Do We Stand and Where Are We Heading? Front. Pediatr. 2018, 6, 165. [Google Scholar] [CrossRef]
- Zadini, F.; Newton, E.; Abdi, A.A.; Lenker, J.; Zadini, G.; Henderson, S.O. Use of the trendelenburg position in the porcine model improves carotid flow during cardiopulmonary resuscitation. West. J. Emerg. Med. 2008, 9, 206–211. [Google Scholar]
- Chollet-Xémard, C.; Combes, X.; Soupizet, F.; Jabre, P.; Penet, C.; Bertrand, C.; Margenet, A.; Marty, J. Bispectral index monitoring is useless during cardiac arrest patients’ resuscitation. Resuscitation 2009, 80, 213–216. [Google Scholar] [CrossRef]
- Fatovich, D.M.; Jacobs, I.G.; Celenza, A.; Paech, M.J. An observational study of bispectral index monitoring for out of hospital cardiac arrest. Resuscitation 2006, 69, 207–212. [Google Scholar] [CrossRef]
- Sekhon, M.S.; Ainslie, P.N.; Griesdale, D.E. Clinical pathophysiology of hypoxic ischemic brain injury after cardiac arrest: A “two-hit” model. Crit. Care 2017, 21, 90. [Google Scholar] [CrossRef] [PubMed]
- Rosso, O.A.; Blanco, S.; Yordanova, J.; Kolev, V.; Figliola, A.; Schürmann, M.; Başar, E. Wavelet entropy: A new tool for analysis of short duration brain electrical signals. J. Neurosci. Methods 2001, 105, 65–75. [Google Scholar] [CrossRef]
- Liang, Z.; Wang, Y.; Sun, X.; Li, D.; Voss, L.J.; Sleigh, J.W.; Hagihira, S.; Li, X. EEG entropy measures in anesthesia. Front. Comput. Neurosci. 2015, 9, 16. [Google Scholar] [CrossRef] [PubMed]
- Das, A.B.; Bhuiyan, M.I.H. Discrimination and classification of focal and non-focal EEG signals using entropy-based features in the EMD-DWT domain. Biomed. Signal Process. Control 2016, 29, 11–21. [Google Scholar] [CrossRef]
- Yin, Y.; Sun, K.; He, S. Multiscale permutation Rényi entropy and its application for EEG signals. PLoS ONE 2018, 13. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| EEG Parameters | Definition | Domain |
|---|---|---|
| Magnitude | Maximal Amplitude during the Epoch (unit: µV) | Time |
| SynchFastSlow | log(B0.5–47 Hz/B40–47 Hz) | Frequency |
| BetaR | log(P30–47 Hz/P11–20 Hz) | Frequency |
| DeltaR | log(P8–20 Hz/P1–4 Hz) | Frequency |
| AlphaPR | P8–13 Hz/P0.5–47 Hz | Frequency |
| BetaPR | P13–30 Hz/P0.5–47 Hz | Frequency |
| DeltaPR | P0.5–4 Hz/P0.5–47 Hz | Frequency |
| ThetaPR | P4–8 Hz/P0.5–47 Hz | Frequency |
| BG_Alpha+ | P8–47 Hz/P0.5–47 Hz | Frequency |
| Log energy entropy | Entropy | |
| Rényi entropy | Entropy |
| EEG Parameters | Correlation Coefficient | p-Value |
|---|---|---|
| Magnitude | 0.778 | <0.001 |
| SynchFastSlow | 0.210 | 0.228 |
| BetaR | −0.329 | 0.016 |
| DeltaR | 0.196 | 0.032 |
| AlphaPR | 0.189 | 0.048 |
| BetaPR | 0.323 | 0.001 |
| DeltaPR | 0.032 | 0.797 |
| ThetaPR | −0.354 | 0.004 |
| BG_Alpha+ | 0.262 | 0.006 |
| Log energy entropy | 0.781 | <0.001 |
| Rényi entropy | 0.784 | <0.001 |
| Magnitude | Log Energy Entropy | Rényi Entropy | ||
|---|---|---|---|---|
| Group I/ Group II | Mean Difference/ Standard Deviation (p-value) | Mean Difference/ Standard Deviation (p-value) | Mean Difference/ Standard Deviation (p-value) | |
| 1 | 2 | −10.39/1.24 (<0.001) | −1375.15/164.65 (<0.001) | −2.69/0.319 (<0.001) |
| 1 | 3 | −13.34/1.37 (<0.001) | −1590.42/164.87 (<0.001) | −3.13/0.321 (<0.001) |
| 1 | 4 | −15.15/2.39 (0.012) | −1720.80/190.02 (<0.001) | −3.38/0.434 (<0.001) |
| 2 | 3 | −2.95/1.30 (0.169) | −215.27/87.24 (0.108) | −0.442/0.171 (0.084) |
| 2 | 4 | −4.75/2.35 (0.395) | −345.65/128.60 (0.180) | −0.695/0.338 (0.384) |
| 3 | 4 | −1.80/2.41 (0.958) | −130.39/128.87 (0.871) | −0.253/0.340 (0.957) |
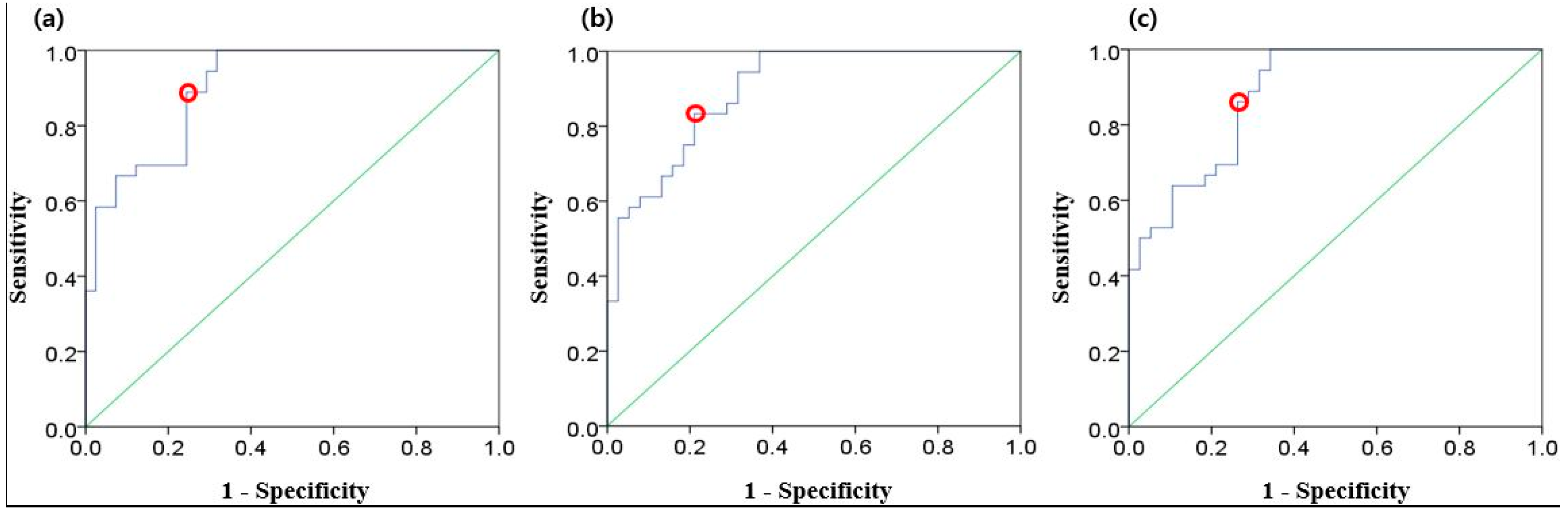
| EEG Parameter | AUC | Standard Error | True Positive Rate (Sensitivity) | False Positive Rate (1-Specificity) | Cut-off Value |
|---|---|---|---|---|---|
| Magnitude | 0.904 | 0.033 | 0.889 | 0.244 | 12.802 |
| Log energy entropy | 0.896 | 0.035 | 0.833 | 0.211 | 739.543 |
| Rényi entropy | 0.885 | 0.037 | 0.861 | 0.263 | 8.919 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.; Kim, K.H.; Hong, K.J.; Ku, Y.; Shin, S.D.; Kim, H.C. Frontal EEG Changes with the Recovery of Carotid Blood Flow in a Cardiac Arrest Swine Model. Sensors 2020, 20, 3052. https://doi.org/10.3390/s20113052
Kim H, Kim KH, Hong KJ, Ku Y, Shin SD, Kim HC. Frontal EEG Changes with the Recovery of Carotid Blood Flow in a Cardiac Arrest Swine Model. Sensors. 2020; 20(11):3052. https://doi.org/10.3390/s20113052
Chicago/Turabian StyleKim, Heejin, Ki Hong Kim, Ki Jeong Hong, Yunseo Ku, Sang Do Shin, and Hee Chan Kim. 2020. "Frontal EEG Changes with the Recovery of Carotid Blood Flow in a Cardiac Arrest Swine Model" Sensors 20, no. 11: 3052. https://doi.org/10.3390/s20113052
APA StyleKim, H., Kim, K. H., Hong, K. J., Ku, Y., Shin, S. D., & Kim, H. C. (2020). Frontal EEG Changes with the Recovery of Carotid Blood Flow in a Cardiac Arrest Swine Model. Sensors, 20(11), 3052. https://doi.org/10.3390/s20113052