
Influence of Klotho Protein Levels in Obesity and Sarcopenia: A Systematic Review


 , , , , and
, , , , and
Abstract
1. Introduction
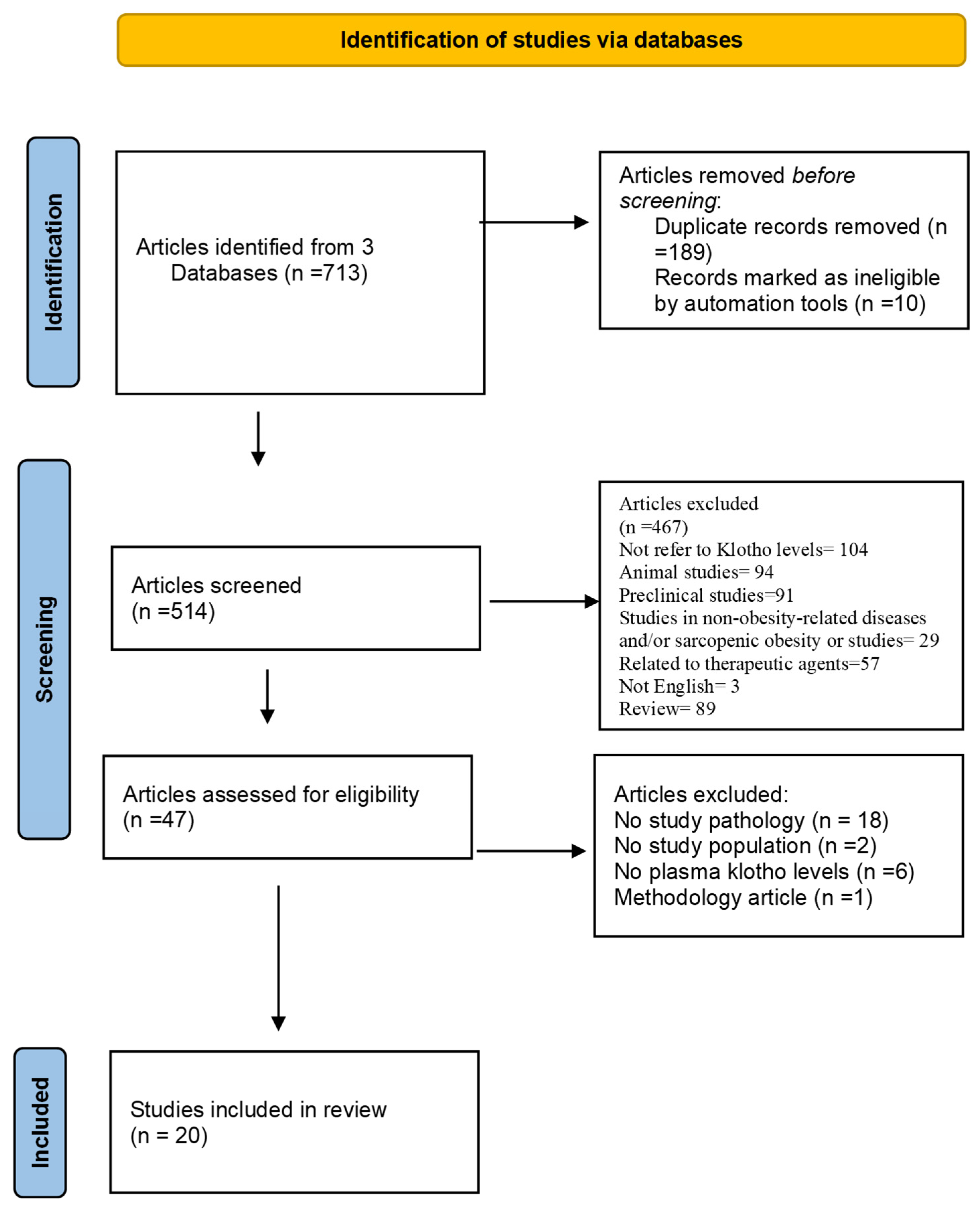
2. Materials and Methods
2.1. Systematic Review Question and PICOTS
2.2. Data Sources and Search Strategy
2.2.1. Study Design, Literature Search, and Data Collection
2.2.2. Data Extraction, Analysis, and Synthesis
- Klotho levels in a population with overweight, obesity, and/or sarcopenic obesity.
- The differences in klotho levels compared with a healthy population.
- The relationship between klotho levels and anthropometric parameters and between klotho levels and body composition.
- The relationship between klotho levels and muscle strength parameters.
- Populations related to obesity such as MS and polycystic ovary syndrome (PCOS) were included.
3. Results
3.1. Studies Relating Klotho Levels with Obesity
3.2. Studies Relating Klotho Levels with Metabolic Syndrome
3.3. Studies Relating Klotho Levels with Cardiovascular Risk
3.4. Studies Relating Klotho Levels with Exercise and Diet
3.5. Studies Relating to Klotho Levels in Older Adults
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kurosu, H.; Ogawa, Y.; Miyoshi, M.; Yamamoto, M.; Nandi, A.; Rosenblatt, K.P.; Baum, M.G.; Schiavi, S.; Hu, M.C.; Moe, O.W.; et al. Regulation of fibroblast growth factor-23 signaling by klotho. J. Biol. Chem. 2006, 281, 6120–6123. [Google Scholar] [CrossRef] [PubMed]
- Kuro-o, M.; Matsumura, Y.; Aizawa, H.; Kawaguchi, H.; Suga, T.; Utsugi, T.; Ohyama, Y.; Kurabayashi, M.; Kaname, T.; Kume, E.; et al. Mutation of the mouse klotho gene leads to a syndrome resembling ageing. Nature 1997, 390, 45–51. [Google Scholar] [CrossRef]
- Matsumura, Y.; Aizawa, H.; Shiraki-Iida, T.; Nagai, R.; Kuro-o, M.; Nabeshima, Y. Identification of the human klotho gene and its two transcripts encoding membrane and secreted klotho protein. Biochem. Biophys. Res. Commun. 1998, 242, 626–630. [Google Scholar] [CrossRef]
- Ito, S.; Kinoshita, S.; Shiraishi, N.; Nakagawa, S.; Sekine, S.; Fujimori, T.; Nabeshima, Y.I. Molecular cloning and expression analyses of mouse betaklotho, which encodes a novel Klotho family protein. Mech. Dev. 2000, 98, 115–119. [Google Scholar] [CrossRef] [PubMed]
- Kurosu, H.; Choi, M.; Ogawa, Y.; Dickson, A.S.; Goetz, R.; Eliseenkova, A.V.; Mohammadi, M.; Rosenblatt, K.P.; Kliewer, S.A.; Kuro-O, M. Tissue-specific Expression of βKlotho and Fibroblast Growth Factor (FGF) Receptor Isoforms Determines Metabolic Activity of FGF19 and FGF21. J. Biol. Chem. 2007, 282, 26687–26695. [Google Scholar] [CrossRef] [PubMed]
- Ito, S.; Fujimori, T.; Hayashizaki, Y.; Nabeshima, Y. Identification of a novel mouse membrane-bound family 1 glycosidase-like protein, which carries an atypical active site structure. Biochim. Biophys. Acta. 2002, 1576, 341–345. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Sun, Z. Molecular basis of Klotho: From gene to function in aging. Endocr. Rev. 2015, 36, 174–193. [Google Scholar] [CrossRef] [PubMed]
- Kuro-o, M. Klotho as a regulator of oxidative stress and senescence. Biol. Chem. 2008, 389, 233–241. [Google Scholar] [CrossRef]
- Ben-Dov, I.Z.; Galitzer, H.; Lavi-Moshayoff, V.; Goetz, R.; Kuro-o, M.; Mohammadi, M.; Sirkis, R.; Naveh-Many, T.; Silver, J. The parathyroid is a target organ for FGF23 in rats. J. Clin. Investig. 2007, 117, 4003–4008. [Google Scholar] [CrossRef] [PubMed]
- Kurosu, H.; Yamamoto, M.; Clark, J.D.; Pastor, J.V.; Nandi, A.; Gurnani, P.; McGuinness, O.P.; Chikuda, H.; Yamaguchi, M.; Kawaguchi, H.; et al. Suppression of Aging in Mice by the Hormone Klotho. Science 2005, 309, 1829–1833. [Google Scholar] [CrossRef] [PubMed]
- Imura, A.; Iwano, A.; Tohyama, O.; Tsuji, Y.; Nozaki, K.; Hashimoto, N.; Fujimori, T.; Nabeshima, Y.I. Secreted Klotho protein in sera and CSF: Implication for post-translational cleavage in release of Klotho protein from cell membrane. FEBS Lett. 2004, 565, 143–147. [Google Scholar] [CrossRef]
- White, K.E.; Evans, W.E.; O’Riordan, J.L.H.; ADHR Consortium. Autosomal dominant hypophosphataemic rickets is associated with mutations in FGF23. Nat. Genet. 2000, 26, 345–348. [Google Scholar] [CrossRef] [PubMed]
- Urakawa, I.; Yamazaki, Y.; Shimada, T.; Iijima, K.; Hasegawa, H.; Okawa, K.; Fujita, T.; Fukumoto, S.; Yamashita, T. Klotho converts canonical FGF receptor into a specific receptor for FGF23. Nature 2006, 444, 770–774. [Google Scholar] [CrossRef]
- Yu, X.; Ibrahimi, O.A.; Goetz, R.; Zhang, F.; Davis, S.I.; Garringer, H.J.; Linhardt, R.J.; Ornitz, D.M.; Mohammadi, M.; White, K.E. Analysis of the Biochemical Mechanisms for the Endocrine Actions of Fibroblast Growth Factor-23. Endocrinology 2005, 146, 4647–4656. [Google Scholar] [CrossRef]
- Prud’homme, G.J.; Kurt, M.; Wang, Q. Pathobiology of the Klotho Antiaging Protein and Therapeutic Considerations. Front. Aging 2022, 12, 931331. [Google Scholar] [CrossRef]
- Cha, S.K.; Ortega, B.; Kurosu, H.; Rosenblatt, K.P.; Kuro-o, M.; Huang, C.L. Removal of sialic acid involving Klotho causes cell-surface retention of TRPV5 channel via binding to galectin-1. Proc. Natl. Acad. Sci. USA 2008, 105, 9805–9810. [Google Scholar] [CrossRef] [PubMed]
- Goetz, R.; Beenken, A.; Ibrahimi, O.A.; Kalinina, J.; Olsen, S.K.; Eliseenkova, A.V.; Xu, C.F.; Neubert, T.A.; Zhang, F.; Linhardt, R.J.; et al. Molecular Insights into the Klotho-Dependent, Endocrine Mode of Action of Fibroblast Growth Factor 19 Subfamily Members. Mol. Cell Biol. 2007, 27, 3417–3428. [Google Scholar] [CrossRef]
- Inagaki, T.; Dutchak, P.; Zhao, G.; Ding, X.; Gautron, L.; Parameswara, V.; Li, Y.; Goetz, R.; Mohammadi, M.; Esser, V.; et al. Endocrine regulation of the fasting response by PPARalpha-mediated induction of fibroblast growth factor 21. Cell Metab. 2007, 5, 415–425. [Google Scholar] [CrossRef] [PubMed]
- Kuro-o, M. Klotho. Pflüg Arch. Eur. J. Physiol. 2010, 459, 333–343. [Google Scholar] [CrossRef] [PubMed]
- Hojman, P.; Pedersen, M.; Krogh-Madsen, R.; Yfanti, C.; Akerstrom, T.; Nielsen, S.; Pedersen, B.K. Fibroblast Growth Factor-21 Is Induced in Human Skeletal Muscles by Hyperinsulinemia. Diabetes 2009, 58, 2797–2801. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, B.K.; Febbraio, M.A. Muscles, exercise and obesity: Skeletal muscle as a secretory organ. Nat. Rev. Endocrinol. 2012, 8, 457–465. [Google Scholar] [CrossRef]
- Keipert, S.; Ost, M.; Johann, K.; Imber, F.; Jastroch, M.; van Schothorst, E.M.; Keijer, J.; Klaus, S. Skeletal muscle mitochondrial uncoupling drives endocrine cross-talk through the induction of FGF21 as a myokine. Am. J. Physiol. Endocrinol. Metab. 2014, 306, E469–E482. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Donini, L.M.; Busetto, L.; Bischoff, S.C.; Cederholm, T.; Ballesteros-Pomar, M.D.; Batsis, J.A.; Bauer, J.M.; Boirie, Y.; Cruz-Jentoft, A.J.; Dicker, D.; et al. Definition and diagnostic criteria for sarcopenic obesity: ESPEN and EASO consensus statement. Clin. Nutr. Edinb. Scotl. 2022, 41, 990–1000. [Google Scholar] [CrossRef]
- Amitani, M.; Asakawa, A.; Amitani, H.; Kaimoto, K.; Sameshima, N.; Koyama, K.I.; Haruta, I.; Tsai, M.; Nakahara, T.; Ushikai, M.; et al. Plasma klotho levels decrease in both anorexia nervosa and obesity. Nutrition 2013, 29, 1106–1109. [Google Scholar] [CrossRef] [PubMed]
- Amaro-Gahete, F.J.; De-la-O, A.; Jurado-Fasoli, L.; Espuch-Oliver, A.; de Haro, T.; Gutiérrez, A.; Ruiz, J.R.; Castillo, M.J. Body Composition and S-Klotho Plasma Levels in Middle-Aged Adults: A Cross-Sectional Study. Rejuvenation Res. 2019, 22, 478–483. [Google Scholar] [CrossRef] [PubMed]
- Bednarska, S.; Fryczak, J.; Siejka, A. Serum β-Klotho concentrations are increased in women with polycystic ovary syndrome. Cytokine 2020, 134, 155188. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.W.; Fang, W.H.; Chen, W.L. Clinical Relevance of Serum Klotho Concentration and Sagittal Abdominal Diameter. J. Clin. Med. 2022, 11, 7376. [Google Scholar] [CrossRef]
- Orces, C.H. The Association of Obesity and the Antiaging Humoral Factor Klotho in Middle-Aged and Older Adults. Sci. World J. 2022, 2022, 7274858. [Google Scholar] [CrossRef] [PubMed]
- Collins, K.A.; Ambrosio, F.; Rogers, R.J.; Lang, W.; Schelbert, E.B.; Davis, K.K.; Jakicic, J.M. Change in circulating klotho in response to weight loss, with and without exercise, in adults with overweight or obesity. Front. Aging 2023, 4, 1213228. [Google Scholar] [CrossRef]
- Cheng, Y.W.; Hung, C.C.; Fang, W.H.; Chen, W.L. Association between Soluble α-Klotho Protein and Metabolic Syndrome in the Adult Population. Biomolecules 2022, 12, 70. [Google Scholar] [CrossRef]
- Orces, C.H. The association between metabolic syndrome and the anti-aging humoral factor klotho in middle-aged and older adults. Diabetes Metab. Syndr. Clin. Res. Rev. 2022, 16, 102522. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez-Pérez, M.E.; Urraza-Robledo, A.I.; Miranda-Pérez, A.A.; Molina-Flores, C.A.; Ruíz-Flores, P.; Delgadillo-Guzmán, D.; López-Márquez, F.C. Role of β-Klotho and Malondialdehyde in Metabolic Disorders, HIV Infection, and Antiretroviral Therapy. DNA Cell Biol. 2022, 41, 691–698. [Google Scholar] [CrossRef] [PubMed]
- Semba, R.D.; Cappola, A.R.; Sun, K.; Bandinelli, S.; Dalal, M.; Crasto, C.; Guralnik, J.M.; Ferrucci, L. Plasma klotho and cardiovascular disease in adults. J. Am. Geriatr. Soc. 2011, 59, 1596–1601. [Google Scholar] [CrossRef] [PubMed]
- Amaro-Gahete, F.J.; Jurado-Fasoli, L.; Sanchez-Delgado, G.; García-Lario, J.V.; Castillo, M.J.; Ruiz, J.R. Relationship between plasma S-Klotho and cardiometabolic risk in sedentary adults. Aging 2020, 12, 2698–2710. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Kim, D.; Lee, H.J.; Choi, J.Y.; Min, J.Y.; Min, K.B. Association between serum klotho levels and cardiovascular disease risk factors in older adults. BMC Cardiovasc. Disord. 2022, 22, 442. [Google Scholar] [CrossRef] [PubMed]
- Amaro-Gahete, F.J.; De-la-O, A.; Jurado-Fasoli, L.; Ruiz, J.R.; Castillo, M.J. Association of basal metabolic rate and fuel oxidation in basal conditions and during exercise, with plasma S-klotho: The FIT-AGEING study. Aging 2019, 11, 5319–5333. [Google Scholar] [CrossRef] [PubMed]
- Amaro-Gahete, F.J.; De-la-O, A.; Jurado-Fasoli, L.; Espuch-Oliver, A.; de Haro, T.; Gutierrez, A.; Ruiz, J.R.; Castillo, M.J. Exercise training increases the S-Klotho plasma levels in sedentary middle-aged adults: A randomised controlled trial. The FIT-AGEING study. J. Sports Sci. 2019, 37, 2175–2183. [Google Scholar] [CrossRef] [PubMed]
- Ma, T.C.; Zhou, J.; Wang, C.X.; Lin, Z.Z.; Gao, F. Associations between the Healthy Eating Index-2015 and S-Klotho plasma levels: A cross-sectional analysis in middle-to-older aged adults. Front. Nutr. 2022, 9, 904745. [Google Scholar] [CrossRef] [PubMed]
- Silva-Reis, A.; Rodrigues Brandao-Rangel, M.A.; Moraes-Ferreira, R.; Gonçalves-Alves, T.G.; Souza-Palmeira, V.H.; Aquino-Santos, E.H.; Lacerda Bachi, A.L.; Franco de Oliveira, L.V.; Brandão Lopes-Martins, R.A.; Oliveira-Silva, I.; et al. Combined resistance and aerobic training improves lung function and mechanics and fibrotic biomarkers in overweight and obese women. Front. Physiol. 2022, 13, 946402. [Google Scholar] [CrossRef]
- Semba, R.D.; Cappola, A.R.; Sun, K.; Bandinelli, S.; Dalal, M.; Crasto, C.; Guralnik, J.M.; Ferrucci, L. Relationship of low plasma klotho with poor grip strength in older community-dwelling adults: The InCHIANTI study. Eur. J. Appl. Physiol. 2012, 112, 1215–1220. [Google Scholar] [CrossRef] [PubMed]
- Semba, R.D.; Ferrucci, L.; Sun, K.; Simonsick, E.; Turner, R.; Miljkovic, I.; Harris, T.; Schwartz, A.V.; Asao, K.; Kritchevsky, S.; et al. Low Plasma Klotho Concentrations and Decline of Knee Strength in Older Adults. J. Gerontol. A Biol. Sci. Med. Sci. 2016, 71, 103–108. [Google Scholar] [CrossRef]
- Chalhoub, D.; Marques, E.; Meirelles, O.; Semba, R.D.; Ferrucci, L.; Satterfield, S.; Nevitt, M.; Cauley, J.A.; Harris, T.; Health ABC Study. Association of serum klotho with loss of bone mineral density and fracture risk in older adults. J. Am. Geriatr. Soc. 2016, 64, e304–e308. [Google Scholar] [CrossRef]
- Polat, Y.; Yalcin, A.; Yazihan, N.; Bahsi, R.; Surmeli, D.M.; Akdas, S.; Aras, S.; Varli, M. The relationship between frailty and serum alpha klotho levels in geriatric patients. Arch. Gerontol. Geriatr. 2020, 91, 104225. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.D.; Chen, Q.F.; Yang, W.; Zuluaga, M.; Targher, G.; Byrne, C.D.; Valenti, L.; Luo, F.; Katsouras, C.S.; Thaher, O.; et al. Burden of disease attributable to high body mass index: An analysis of data from the Global Burden of Disease Study 2021. EClinicalMedicine 2024, 76, 102848. [Google Scholar] [CrossRef]
- Park, M.J.; Choi, K.M. Interplay of skeletal muscle and adipose tissue: Sarcopenic obesity. Metabolism 2023, 144, 155577. [Google Scholar] [CrossRef] [PubMed]
- Yuan, S.; Larsson, S.C. Epidemiology of sarcopenia: Prevalence, risk factors, and consequences. Metabolism 2023, 144, 155533. [Google Scholar] [CrossRef] [PubMed]
- Salvà, A.; Serra-Rexach, J.A.; Artaza, I.; Formiga, F.; Rojano, I.; Luque, X.; Cuesta, F.; López-Soto, A.; Masanés, F.; Ruiz, D.; et al. La prevalencia de sarcopenia en residencias de España: Comparación de los resultados del estudio multicéntrico ELLI con otras poblaciones [Prevalence of sarcopenia in Spanish nursing homes: Comparison of the results of the ELLI study with other populations]. Rev. Esp. Geriatr. Gerontol. 2016, 51, 260–264. (In Spanish) [Google Scholar] [CrossRef]
- González-Montalvo, J.I.; Alarcón, T.; Gotor, P.; Queipo, R.; Velasco, R.; Hoyos, R.; Pardo, A.; Otero, A. Prevalence of sarcopenia in acute hip fracture patients and its influence on short-term clinical outcome. Geriatr. Gerontol. Int. 2016, 16, 1021–1027. [Google Scholar] [CrossRef] [PubMed]
- Illamola-Martin, L.; Granados, A.; Sanllorente, A.; Rodríguez, J.J.; Broto, M. Prevalencia de inactividad física y riesgo de sarcopenia en atención primaria. Estudio transversal [Prevalence of physical inactivity and risk of sarcopenia in primary care. Cross-sectional study]. Aten. Primaria 2024, 56, 102993. (In Spanish) [Google Scholar] [CrossRef] [PubMed]
- Guillamón-Escudero, C.; Diago-Galmés, A.; Tenías-Burillo, J.M.; Soriano, J.M.; Fernández-Garrido, J.J. Prevalence of Sarcopenia in Community-Dwelling Older Adults in Valencia, Spain. Int. J. Environ. Res. Public Health 2020, 17, 9130. [Google Scholar] [CrossRef]
- Hernández-Martínez, P.; Olmos, J.M.; Llorca, J.; Hernández, J.L.; González-Macías, J. Sarcopenic osteoporosis, sarcopenic obesity, and sarcopenic osteoporotic obesity in the Camargo cohort (Cantabria, Spain). Arch. Osteoporos. 2022, 17, 105. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Cabello, A.; Pedrero-Chamizo, R.; Olivares, P.R.; Luzardo, L.; Juez-Bengoechea, A.; Mata, E.; Albers, U.; Aznar, S.; Villa, G.; Espino, L.; et al. Prevalence of overweight and obesity in non-institutionalized people aged 65 or over from Spain: The elderly EXERNET multi-centre study. Obes. Rev. 2011, 12, 583–592. [Google Scholar] [CrossRef]
- Koliaki, C.; Liatis, S.; Dalamaga, M.; Kokkinos, A. Sarcopenic Obesity: Epidemiologic Evidence, Pathophysiology, and Therapeutic Perspectives. Curr. Obes. Rep. 2019, 8, 458–471. [Google Scholar] [CrossRef] [PubMed]
- Lian, R.; Liu, Q.; Jiang, G.; Zhang, X.; Tang, H.; Lu, J.; Yang, M. Blood biomarkers for sarcopenia: A systematic review and meta-analysis of diagnostic test accuracy studies. Ageing Res. Rev. 2024, 93, 102148. [Google Scholar] [CrossRef] [PubMed]
- Fatima, R.; Kim, Y.; Baek, S.; Suram, R.P.; An, S.L.; Hong, Y. C-Terminal Agrin Fragment as a Biomarker for Sarcopenia: A Systematic Review and Meta-Analysis. J. Cachexia Sarcopenia Muscle 2025, 16, e13707. [Google Scholar] [CrossRef] [PubMed]
- Liang, J.; Zhang, H.; Zeng, Z.; Lv, J.; Huang, J.; Wu, X.; Wang, M.; Xu, J.; Fan, J.; Chen, N. MicroRNA profiling of different exercise interventions for alleviating skeletal muscle atrophy in naturally aging rats. J. Cachexia Sarcopenia Muscle 2023, 14, 356–368. [Google Scholar] [CrossRef]
- Ladang, A.; Beaudart, C.; Reginster, J.Y.; Al-Daghri, N.; Bruyère, O.; Burlet, N.; Cesari, M.; Cherubini, A.; da Silva, M.C.; Cooper, C.; et al. Biochemical Markers of Musculoskeletal Health and Aging to be Assessed in Clinical Trials of Drugs Aiming at the Treatment of Sarcopenia: Consensus Paper from an Expert Group Meeting Organized by the European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (ESCEO) and the Centre Académique de Recherche et d’Expérimentation en Santé (CARES SPRL), Under the Auspices of the World Health Organization Collaborating Center for the Epidemiology of Musculoskeletal Conditions and Aging. Calcif. Tissue Int. 2023, 112, 197–217. [Google Scholar] [CrossRef] [PubMed]
- Curcio, F.; Ferro, G.; Basile, C.; Liguori, I.; Parrella, P.; Pirozzi, F.; Della-Morte, D.; Gargiulo, G.; Testa, G.; Tocchetti, C.G.; et al. Biomarkers in sarcopenia: A multifactorial approach. Exp. Gerontol. 2016, 85, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kalinkovich, A.; Livshits, G. Sarcopenia--The search for emerging biomarkers. Ageing Res. Rev. 2015, 22, 58–71. [Google Scholar] [CrossRef]
- Axelrod, C.; Dantas, W.S.; Kirwan, J.P. Sarcopenic obesity: Emerging mechanisms and therapeutic potential. Metabolism 2023, 146, 155639. [Google Scholar] [CrossRef]
- Brzeszczyński, F.; Hamilton, D.; Bończak, O.; Brzeszczyńska, J. Systematic Review of Sarcopenia Biomarkers in Hip Fracture Patients as a Potential Tool in Clinical Evaluation. Int. J. Mol. Sci. 2024, 25, 13433. [Google Scholar] [CrossRef]
- Wang, Y.; Sun, Z. Current understanding of klotho. Ageing Res. Rev. 2009, 8, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Abraham, C.R.; Li, A. Aging-suppressor Klotho: Prospects in diagnostics and therapeutics. Ageing Res. Rev. 2022, 82, 101766. [Google Scholar] [CrossRef]
- Liu, Y.; Chen, M. Emerging role of α-Klotho in energy metabolism and cardiometabolic diseases. Diabetes Metab. Syndr. 2023, 17, 102854. [Google Scholar] [CrossRef] [PubMed]
- Carreras-Badosa, G.; Puerto-Carranza, E.; Mas-Parés, B.; Gómez-Vilarrubla, A.; Gómez-Herrera, B.; Díaz-Roldán, F.; Riera-Pérez, E.; de Zegher, F.; Ibañez, L.; Bassols, J.; et al. Higher levels of serum α-Klotho are longitudinally associated with less central obesity in girls experiencing weight gain. Front. Endocrinol. 2023, 14, 1218949. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Yu, L.; Yun, G. Reduced Serum Levels of Klotho are Associated with Mild Cognitive Impairment in Patients with Type 2 Diabetes Mellitus. Diabetes Metab. Syndr. Obes. 2023, 16, 129–137. [Google Scholar] [CrossRef] [PubMed]
- de Luca Corrêa, H.; Oppelt Raab, A.T.; Marra Araújo, T.; Alves Deus, L.; Lucena Reis, A.; Sousa Honorato, F.; Rodrigues-Silva, P.L.; Passos Neves, R.V.; Simionato Brunetta, H.; Alves da Silva Mori, M.; et al. A systematic review and meta-analysis demonstrating Klotho as an emerging exerkine. Sci. Rep. 2022, 12, 17587. [Google Scholar] [CrossRef]
- Donate-Correa, J.; Martín-Núñez, E.; Martin-Olivera, A.; Mora-Fernández, C.; Tagua, V.G.; Ferri, C.M.; López-Castillo, A.; Delgado-Molinos, A.; Castro López-Tarruella, V.; Arévalo-Gómez, M.A.; et al. Klotho inversely relates with carotid intima- media thickness in atherosclerotic patients with normal renal function (eGFR ≥60 mL/min/1.73 m2): A proof-of-concept study. Front. Endocrinol. 2023, 14, 1146012. [Google Scholar] [CrossRef] [PubMed]
- Rostamzadeh, F.; Joukar, S.; Yeganeh-Hajahmadi, M. The role of Klotho and sirtuins in sleep-related cardiovascular diseases: A review study. NPJ Aging 2024, 10, 43. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Study | Patient Type n | Groups (n) | Age (years) | Sex | BMI (Kg/m2) | Body Composition | Strength Parameter | Parameter and Measuring Method, (Unit.). Level |
|---|---|---|---|---|---|---|---|---|
| Amitani et al., 2013 [25] Cross-sectional study | r-AN—Obesity 2013 Women n = 34 | r-AN 12 O 11 CG 11 | r-AN 21.0 ± 1.65 O 21.3 ± 0.95 CG 21.0 ± 1.29 | N/A | r-AN 13.12 ± 0.26 O 35.72 ± 3.17 CG 21.84 ± 0.36 p = <0.001 | N/A | N/A | S-Klotho, ELISA, (pg/mL) r-AN 764.64 ± 65.43 O 847.09 ± 111.31 CG 1391.62 ± 144.96 p = <0.01 |
| Amaro-Gahete et al., 2018 [26] Cross-sectional study | FIT-AGING study. 40–65 years n = 74 | BMI (Kg/m2) NW ≥ 18.5–<25 OW ≥ 25–<30 O ≥ 30 | 53.7 ± 5.1 | M (n) 35 | 27.7 | DEXA LM (Kg) 43.5 ± 11.7 LMI (LM/m2) 43.5 ± 11.7 FMI (FM/m2) 10.7 ± 3.1 FM (Kg.%) 30 ± 8.4, 3.9 ± 9.1 | N/A | S-Klotho, ELISA, (pg/mL). NW = 988.08 O = 668.43 p = 0.033 |
| Bednarska et al., 2020 [27] Cross-sectional study | PCOS 2020 18–40 years n = 67 | PCOS 49 CG 18 | PCOS 25.85 ± 5.22 CG 27.78 ± 5.6 | N/A | PCOS 26.55 ± 6.92 CG 21.35 ± 2.08 | N/A | N/A | β-Klotho, ELISA, (pg/mL) NW 8695.1 ± 3484.5 OW 9287.5 ± 3337 O 7734.7 ± 4183.5 p = 0.427 |
| Huang et al., 2022 [28] Cross-sectional study | NHANES 2011–2012 40–79 years n = 9756 | QSAD (cm) Q1 < 20.4 Q2 20.4 to <23.2 Q3 23.2 to <26.1 Q4 > 26.1 | Q1 52.66 ± 9.54 Q2 56.36 ± 10.31 Q3 57.34 ± 10.65 Q4 58.20 ± 10.49 p < 0.001 | M (%, n) Q1 27.3, 35 Q2 39.2, 187 Q3 54.0, 415 Q4 53.3, 494 | Q1 21.15 ± 2.03 Q2 24.15 ± 2.39 Q3 27.52 ± 2.87 Q4 34.78 ± 6.05 p < 0.001 | N/A | N/A | S-Klotho, ELISA, (pg/mL) Q1 956.38 ± 303.37 Q2 911.56 ± 316.43 Q3 888.53 ± 324.32 Q4 877.95 ± 310.98 p = 0.029 |
| Orces et al., 2022 [29] Cross-sectional study | NHANES 2013–2014, 2015–2016 40–79 years n = 4971 | 10 years and 25 years to baseline NO, ONO, NOO, AO | 57.4 ± 10.6 | (%, n) M 47.9, 2380 | NW 23.8 OW 34.4 O 41.8 | N/A | N/A | S-Klotho, ELISA, (pg/mL) NW 820.6, OW 765.1, O 772.8 p = <0.001 |
| Collins et al., 2023 [30] Clinical trial | Heart Health Study 2011–2015 n = 152 | DIET DIET + MVIPA150 DIET + MVIPA250 | 45.4 ± 8.0 | N/A | 32.1 ± 3.7 | LM (Kg): R. 48.4, NoR. 47.2 FM (Kg): R. 39.3, NoR. 38.4 PBF (%): R. 44.8, NoR. 45 WC (cm): R. 107.3, NoR. 104.5 | N/A | S-Klotho, ELISA, (pg/mL) Before the intervention R = 936.2 (870.6–1006.5) NoR = 926.1 (800.4–1077) |
| Study | Patient Type n | Groups (n) | Age (years) | Sex | BMI (Kg/m2) | Body Composition | Strength Parameter | Parameter and Measuring Method, (Unit.). Level |
|---|---|---|---|---|---|---|---|---|
| Semba et al., 2011 [34] Cross-sectional study | InCHIANTI study 2001–2003 24–102 years n = 1023 | TK (pg/mL) T1 < 586 T2 587–769 T3 > 770 | T1 75 (69–80) T2 72 (66–78) T3 72 (64–77) | M (%) Q1 47.9 Q2 46.5 Q3 40.2 | Q1 26.3 (23.6–28.8) Q2 26 (23–28.6) Q3 26 (23.1–28.4) | N/A | LG (Kg): Q1 90.1, Q2 92.0, Q3 93.8 LG N-m/Kg: Q1 1.19, Q2 1.23, Q3 1.26 DN (Kg): Q1 0.9, Q2 0.40, Q3 0.41 | S-Klotho, ELISA, (pg/mL) N/A |
| Amaro-Gahete et al., 2020 [35] Cross-sectional study | FIT-AGING and ACTIBATE study 40–65 and 18–25 years. n = 214 | YA 145 OA 74 | N/A | M (n) YA 42 OA 35 | YA 25 OA 26.7 | N/A | N/A | S-Klotho, ELISA, (pg/mL) YA 823.1 OA 775.3 |
| Lee et al., 2022 [36] Observational study | NHANES 2007–2016 40–79 years n = 13,154 | QK (pg/mL) Q1 < 654.6 Q2 654.6 to 802.4 Q3 802.4 to 993.3 Q4 ≥ 992.4 | Q1 59.10 ± 11.11 Q2 57.94 ± 10.84 Q3 57.35 ± 10.73 Q4 56.35 ± 10.62 p = < 0.0001 | M (%, n) Q1 26.32, 1669 Q2 26.87, 1704 Q3 24.50, 1554 Q4 22.29, 1414 | N/A | N/A | N/A | S-Klotho, ELISA, (pg/mL) N/A |
| Cheng et al., 2022 [31] Cross-sectional study | NHANES 2007–2012 ≥18 years. n = 9976 | MS 3906 CG 6070 | MS 58.93 ± 10.4 CG 56.4 ± 10.83 | M (%, n) MS 48.1. 1880 CG 50.3, 3053 | MS 32.40 ± 6.29 CG 27.65 ± 5.85 | N/A | N/A | S-Klotho, ELISA, (pg/mL) MS 848.35 ± 292.92 CG 871.54 ± 311.68 p = <0.001 |
| Orces et al., 2022 [32] Cross-sectional study | NHANES: 2013–2014, 2015–2016 40–79 years n = 5069 | MS 2279 CG 2290 | 57.4 ± 10.6 | M (%, n) MS 44.8. 1080 CG 55.2, 1330 | NW 23.8 O 34.4 MO 41.8 | N/A | NA | S-Klotho, ELISA, (pg/mL) N/A |
| Gutiérrez-Pérez et al. [33] Observational study | CAPASITS SAIH Mexico HIV infection 18–50 years n = 261 | WHIV: 179 NHIV: 82 | WHIV: 39.21 ± 10.66 NHIV: 32.39 ± 10.56 | M (%, n) WHIV 75.4, 135 NHIV 69.5, 57 | WHIV: NW 21.9, O 29.7 NHIV: NW 22.3, O 30.8 | N/A | N/A | β-Klotho, ELISA, (pg/mL) WHIV 4.05 ± 0.04 NHIV 4.19 ± 0.03 p = 0.011 |
| Study | Patient Type n | Groups (n) | Age (years) | Sex | BMI (Kg/m2) | Body Composition | Strength Parameter | Parameter and Measuring Method, (Unit.). Level |
|---|---|---|---|---|---|---|---|---|
| Amaro-Gahete et al., 2019 [37] Cross-sectional study | FIT-AGING study 40–65 years n = 74 | N/A | 53.7 ± 5.1 | M (%, n) 47.35 | 26.7 ± 3.8 | DEXA LM (Kg) 43.5 ± 11.7 LMI (LM/m2) 43.5 ± 11.7 FMI (FM/m2) 10.7 ± 3.1 FM (Kg, %) 30 ± 8.4, 39.9 ± 9.1 | VO2max (mL/Kg/min) 30.5 ± 5.6 | S-Klotho, ELISA, (pg/mL) 775.3 ± 363.7 |
| Amaro-Gahete et al., 2019 [38] Clinical trial | FIT-AGING study 40–65 years n = 68 | CG 15 PAR 17 HIIT 17 HIIT-EMS 19 | CG 51.7 ± 4.1 PAR 54.9 ± 4.5 HIIT 53.5 ± 5.6 HIIT-EMS 53.5 ± 5.2 | M (%, n) CG 40.6 PAR 47.1, 8 HIIT 47.1, 8 HIIT-EMS 52.6, 10. | CG 26.7 ± 3.9 PAR 25.4 ± 2.9 HIIT 26.4 ± 3.2 HIIT-EMS 28.6 ± 4.6 | All LMI (LM/m2) 15.4 ± 2.8 FMI (FM/m2) 10.7 ± 3.1 FM (%) 39.6 ± 8.5 | N/A | S-Klotho, ELISA, (pg/mL) B/PIT CG 922.5 ± 290.3/862.9 ± 364.4 PAR 714.3 ± 294.5/1055.4 ± 435.9 HIIT 788.5 ± 276.8/1057.1 ± 273.3 HIIT-EMS 808.5 ± 499.0/1259.7 ± 613.1 p = <0.001 |
| Ma et al., 2022 [39] Cross-sectional study | NHANES 2007–2016 40–79 years n = 8456 | QHEI-2015 Q1 ≤ 60 Q2 > 60, ≤70 Q3 > 70, ≤80 Q4 > 80 | Q1 56.76 ± 10.98 Q2 58.49 ± 10.77 Q3 59.19 ± 10.93 Q3 59.98 ± 10.32 | M (%, n) Q1 52.94, 3102 Q2 52.94, 3102 Q3 44.18, 338 Q4 44.62, 112 | Q1 28.33 ± 6.31 Q2 27.80 ± 5.84 Q3 26.91 ± 5.19 Q4 26.06 ± 5.02 | N/A | N/A | S-Klotho, ELISA, (pg/mL) Q1 851.64 ± 312.30 Q2 878.35 ± 329.71 Q3 879.80 ± 312.65 Q4 903.58 ± 332.19 p = <0.001 |
| Silva-Reis et al., 2022 [34,40] Clinical trial | Combined physical exercise. Women 30–59 years n = 41 | NW 12 OW 17 O 11 | NW 43.5 ± 11.3 OW 47.35 ± 11.75 O 47.36 ± 10.64 | N/A | NW 22 ± 1.9 OW 27.93 ± 1.67 O 31.98 ± 1.45 | N/A | N/A | S-Klotho. ELISA, (pg/mL) Does not add value PRH vs. PoRH: NW < 0.0489, OW < 0.0333, O > 0.05 |
| Study | Patient Type n | Groups (n) | Age (years) | Sex | BMI (Kg/m2) | Body Composition | Strength Parameter | Parameter and Measuring Method, (Unit.). Level |
|---|---|---|---|---|---|---|---|---|
| Semba et al., 2012 [41] Longitudinal cohort study | InCHIANTI study 2001–2009 >65 years n = 804 | K (pg/mL), % >681, 46.8% <681, 53.2% | 75 (71–80) | M (%, n) 44.2, 355 | 26.4 (23.7–28.7) | N/A | Grip strength (Kg) 26.5 (20.3–36.5) | S-Klotho, ELISA, (pg/mL) 664 (521–811) |
| Semba et al., 2016 [42] Cross-sectional study | Health ABC Study 70–79 years n = 1983 | TK (pg/mL) T1 < 536 T2 536–747 T3 > 747 | T1 74.5 T2 74.5 T3 74.5 | M (%, n) T1 M 51.0 T2 M 52.0 T3 M 48.1 | T1 27.4 T2 27.1 T3 27.0 | N/A | Knee extensor strength (Kg): T1 90.1, T2 92.0, T3 93.8 Grip strength (Kg): T1 39, T2 40, T3 41 Knee extensor strength, mean/weight (N-m/Kg): T1 1.19, T2 1.23, T3 1.26 p = 0.002 | S-Klotho, ELISA, (pg/mL) N/A |
| Chalhoub D et al., 2016 [43] Longitudinal cohort study | Health ABC Study 70–79 years n = 2776 | QK (pg/mL) Every group, n = 694 Q1 320.6 to 437.3 Q2 521.6 to 592.1 Q3 670.1 to 756.2 Q4 887.7 to 1186.4 | Q1 74.7 ± 2.9 Q2 74.8 ± 2.9 Q3 74.5 ± 2.8 Q4 74.6 ± 2.9 | M (%, n) Q1 48.1, 334 Q2 52.9, 367 Q3 50.0, 347 Q4 44.5, 309 | Q1 27.3 ± 4.8 Q2 27.3 ± 4.4 Q3 27.1 ± 1 Q4 27.1 ± 5.1 | ALM (Kg) Q1 20.0 ± 5.0 Q2 20.0 ± 4.9 Q3 20.2 ± 4.9 Q4 20.2 ± 4.8 | Grip strength (Kg): Q1 31.4 ± 10.5, Q2 31.7 ± 10.5, Q3 32.1 ± 10.6, Q4 32.2 ± 10.9 Gait Speed (m/seg): Q1 0.93 ± 0.47, Q2 0.96 ± 0.46, Q3 0.97 ± 0.46, Q4 0.95 ± 0.44 | S-Klotho, ELISA, (pg/mL) N/A |
| Polat et al., 2020 [44] Cross-sectional study | Ankara University Faculty 2018 >65 years n = 89 | CG 44 FG 45 | FG 72.7 ± 4.45 CG 79.36 ± 6.91 p = <0.001 | M (n) FG 14 CG 17 | CG 30.53 ± 4.24 FG 27.76 ± 7.89 p = 0.003 | N/A | Grip strength (Kg): CG 25.6 ± 6.71, FG 16.65 ± 6.83 p = < 0.001 Walking speed, m/s: CG 7.19 ± 0.98, FG 9.51 ± 2.95 p = < 0.001 | S-Klotho, ELISA, (pg/mL) CG 0.76 ± 1.01 FG 0.54 ± 0.61 p = 0.286 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ariadel-Cobo, D.G.; Estébanez, B.; González-Arnáiz, E.; García-Pérez, M.P.; Rivera-Viloria, M.; Pintor de la Maza, B.; Barajas-Galindo, D.E.; García-Sastre, D.; Ballesteros-Pomar, M.D.; Cuevas, M.J. Influence of Klotho Protein Levels in Obesity and Sarcopenia: A Systematic Review. Int. J. Mol. Sci. 2025, 26, 1915. https://doi.org/10.3390/ijms26051915
Ariadel-Cobo DG, Estébanez B, González-Arnáiz E, García-Pérez MP, Rivera-Viloria M, Pintor de la Maza B, Barajas-Galindo DE, García-Sastre D, Ballesteros-Pomar MD, Cuevas MJ. Influence of Klotho Protein Levels in Obesity and Sarcopenia: A Systematic Review. International Journal of Molecular Sciences. 2025; 26(5):1915. https://doi.org/10.3390/ijms26051915
Chicago/Turabian StyleAriadel-Cobo, Diana G., Brisamar Estébanez, Elena González-Arnáiz, María Pilar García-Pérez, Marta Rivera-Viloria, Begoña Pintor de la Maza, David Emilio Barajas-Galindo, Diana García-Sastre, María D. Ballesteros-Pomar, and María J. Cuevas. 2025. "Influence of Klotho Protein Levels in Obesity and Sarcopenia: A Systematic Review" International Journal of Molecular Sciences 26, no. 5: 1915. https://doi.org/10.3390/ijms26051915
APA StyleAriadel-Cobo, D. G., Estébanez, B., González-Arnáiz, E., García-Pérez, M. P., Rivera-Viloria, M., Pintor de la Maza, B., Barajas-Galindo, D. E., García-Sastre, D., Ballesteros-Pomar, M. D., & Cuevas, M. J. (2025). Influence of Klotho Protein Levels in Obesity and Sarcopenia: A Systematic Review. International Journal of Molecular Sciences, 26(5), 1915. https://doi.org/10.3390/ijms26051915