
Medical Ozone Increases Methotrexate Effects in Rheumatoid Arthritis Through a Shared New Mechanism Which Involves Adenosine

 , ,
, ,
Abstract
1. Introduction
2. Methods
Statistical Analysis
3. Results
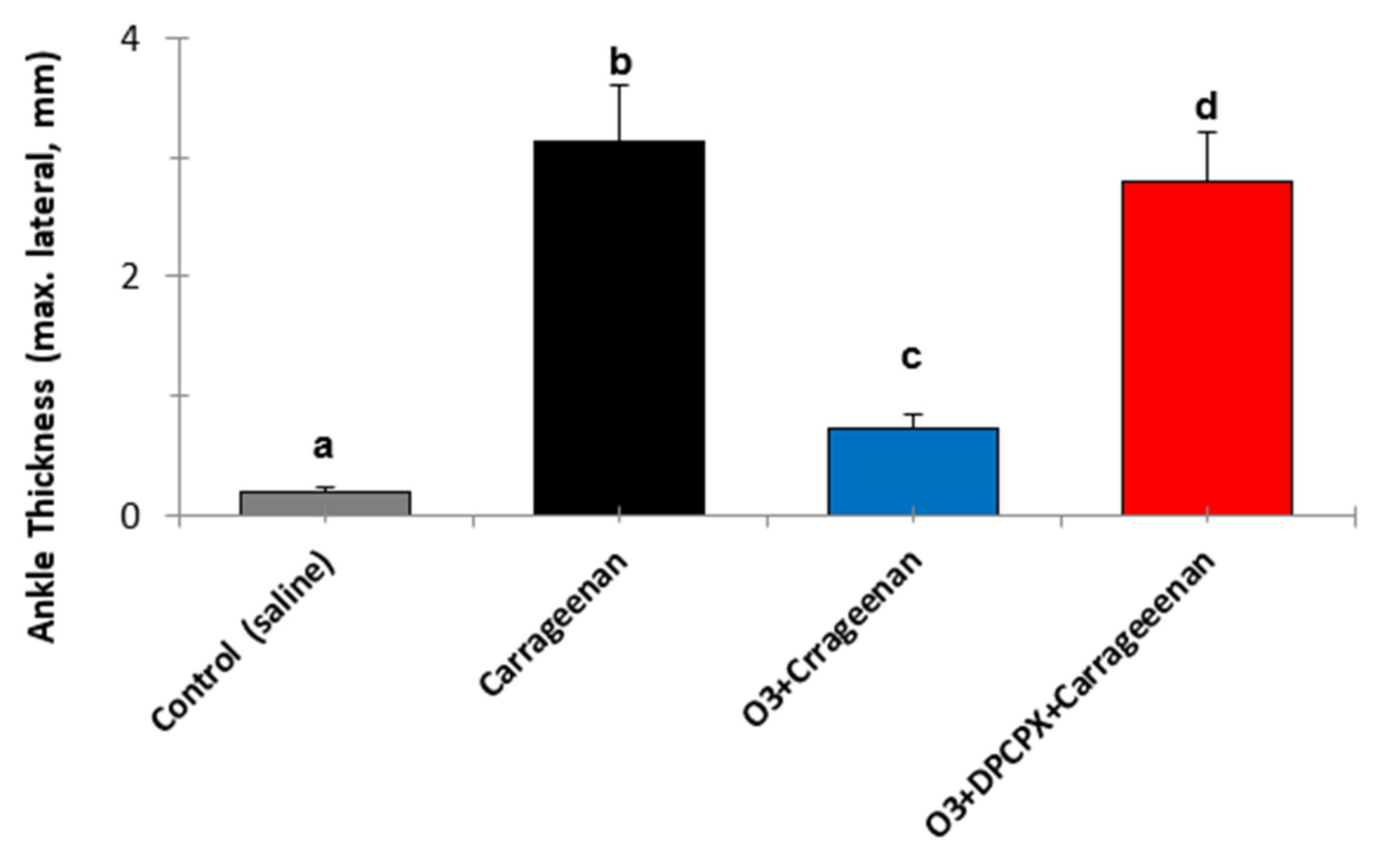
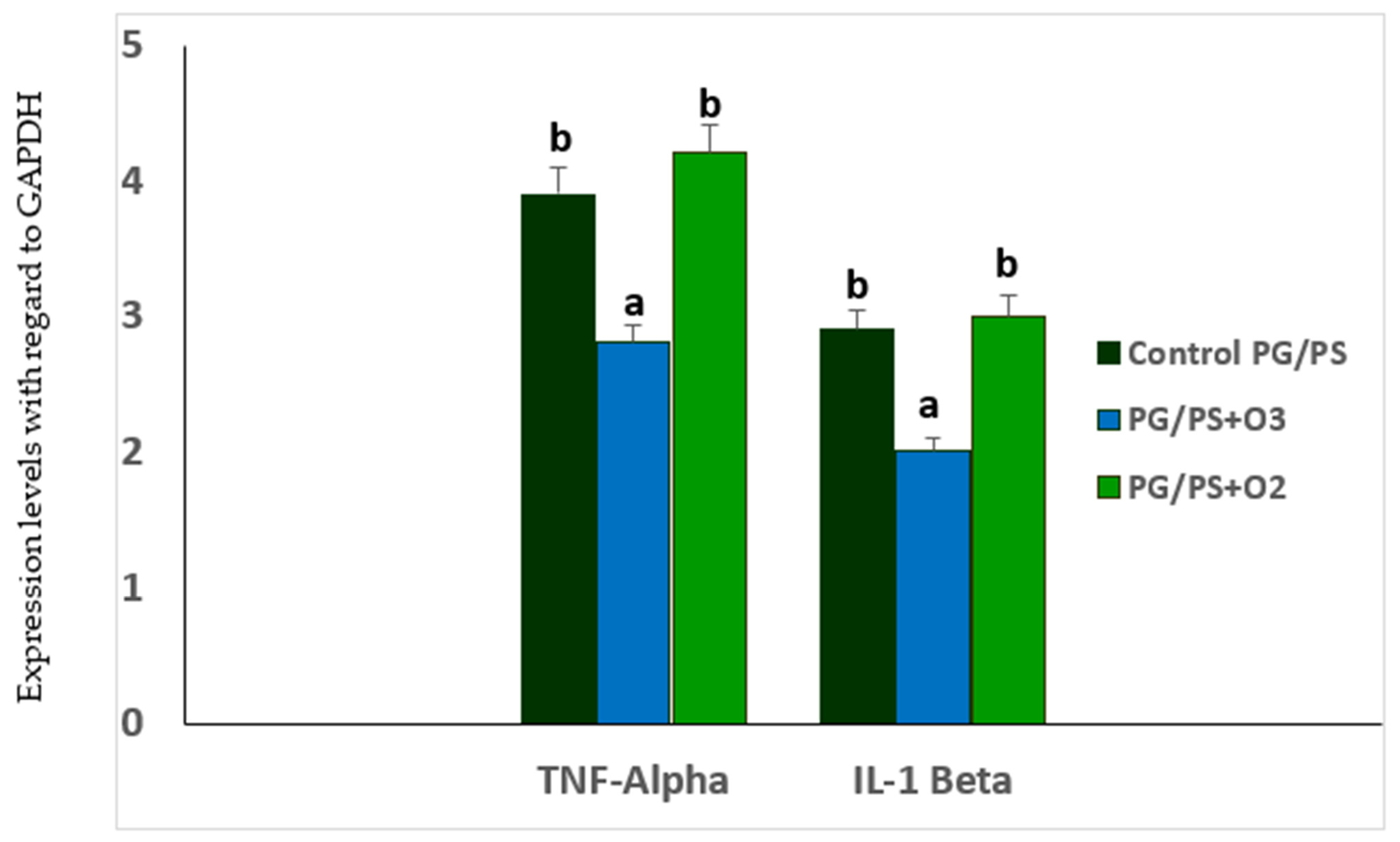
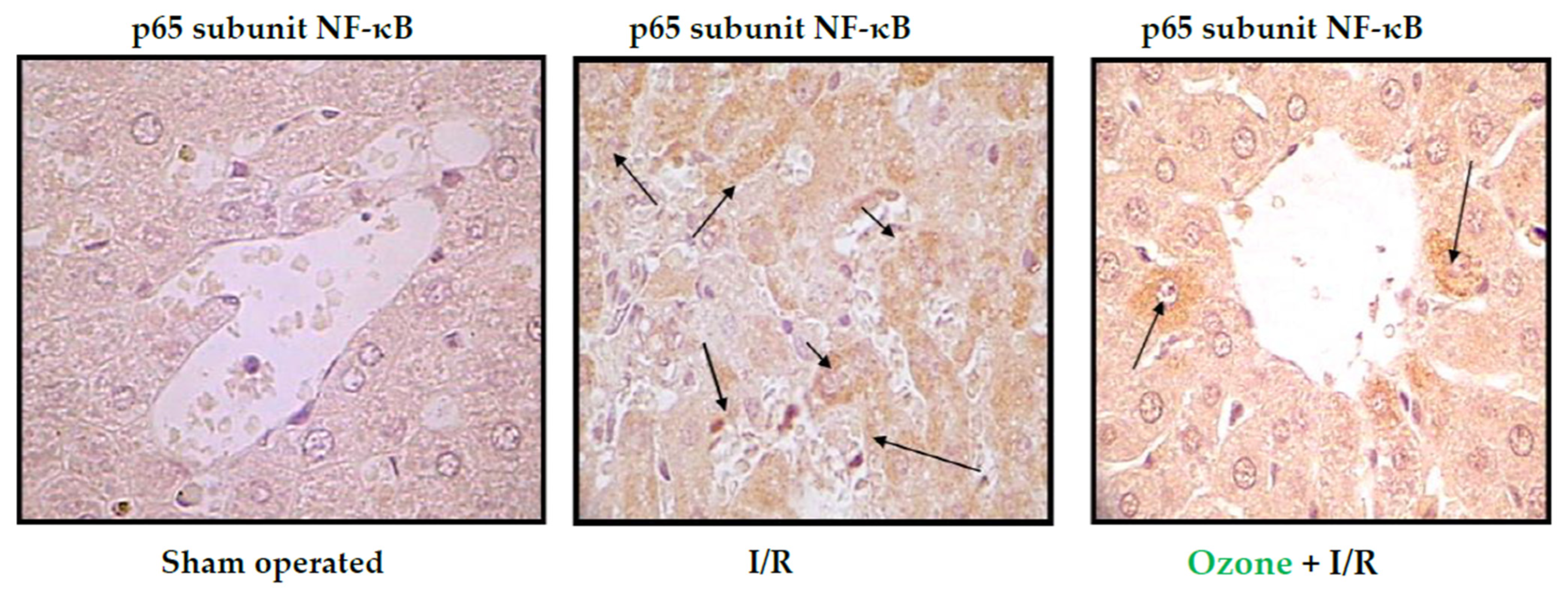
3.1. Studies in Animal Models
3.2. Studies in Patients with Rheumatoid Arthritis
4. Discussion
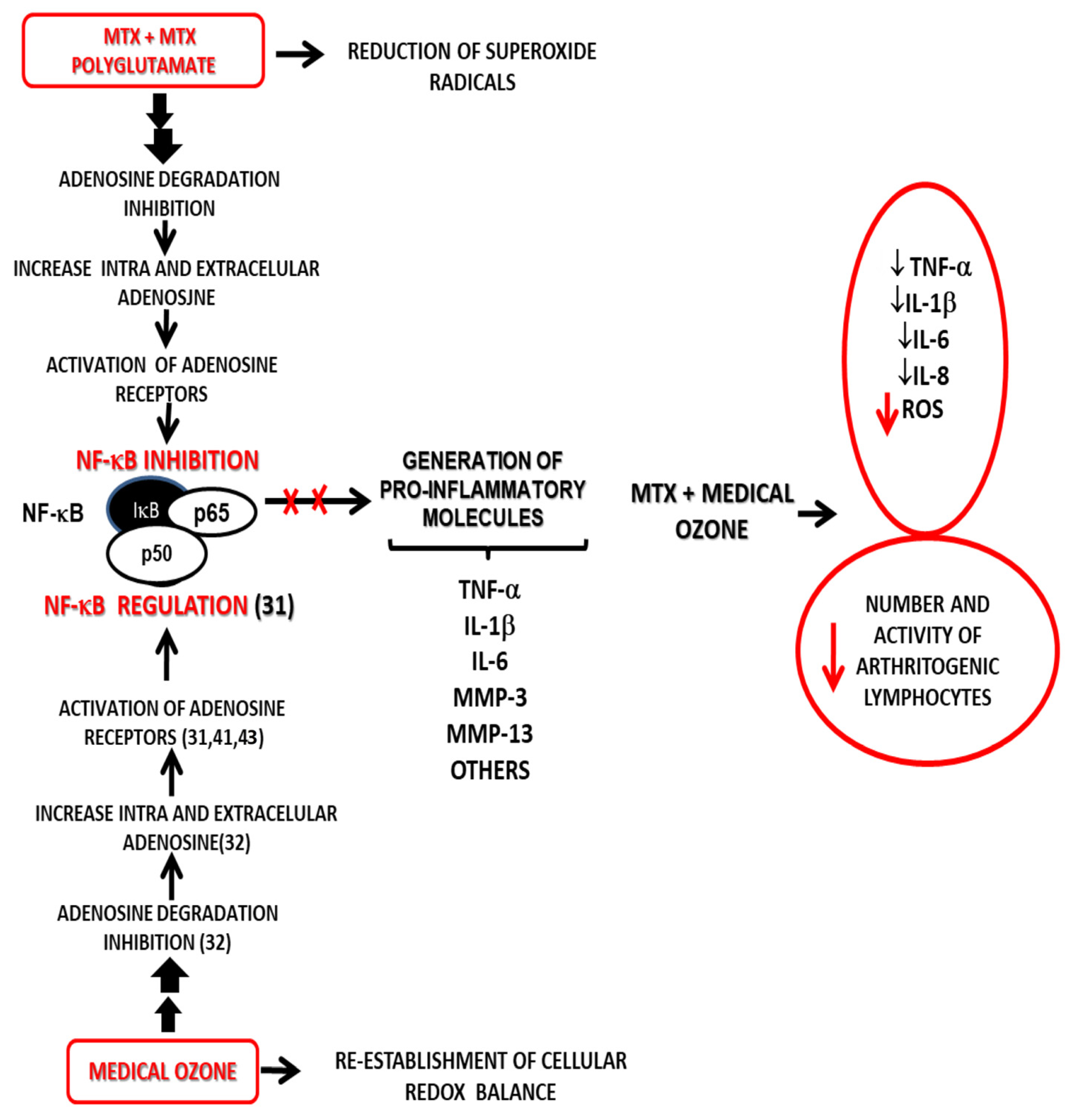
4.1. MTX and Adenosine Mechanisms in Rheumatoid Arthritis
4.2. Medical Ozone and Adenosine Mechanisms in Rheumatoid Arthritis
5. Conclusions
6. Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| A1AR | A1 adenosine receptors |
| ADA | Adenosine Deaminase |
| Anti-CCP | Antibodies against Cycllic Citrullinate Peptide |
| AOPP | Advanced Oxidation Protein Products |
| bDMARDs | Biological DMARDs |
| CAT | Catalase |
| CCPA | 2-chloro-N6-cyclopentyladenosine |
| CENIC | National Center for Scientific Research |
| CRP | C Reactive Protein |
| csDMARDs | Conventional synthetic DMARDs |
| DAS28 | Disease Activity Score 28 |
| DMARDs | Disease Modifying Antirheumatic Drugs |
| DPCPX | 8 cyclopentyl-1,3 dipeptilxanthine |
| ESR | Erythrocyte Sedimentation Rate |
| FLSS | Fibroblasts like synoviocytes |
| GSH | Reduced Glutathione |
| GSH-Px | Glutathione Peroxidase |
| H2O2 | Hydrogen Peroxide |
| HAQ-DI | Assessment Questionnarie-Disabiity |
| HCLO | Hypochlorous Acid |
| I/R | Ischemia/Reperfusion |
| IL-1β | Interleukin 1 Beta |
| IL-6 | Interleukin 6 |
| IL-8 | Interleukin 8 |
| LPO | Lipid Peroxidation |
| MDA | Malondialdehyde |
| MMP | Metalloproteinases |
| MPO | Mieloperoxidase |
| MTX | Methotrexate |
| NF-κB | Nuclear Factor kappa B |
| NO | Nitrric Oxide |
| Nrf2 | (Erythroid-derived 2)-like 2 |
| O2 | Oxygen |
| O2− | Superoxide Radical |
| O3 | Ozone |
| O3/O2 | Ozone/Oxygen mixture |
| OS | Oxidative Stress |
| p50 | P50 subunit of NF kappa B |
| P65 | P65 subunit of NF kappa B |
| PG/PS | Glycan/Polysaccaride Peptide |
| PGI2 | Prostacyclin 2 |
| RA | Rheumatoid Arthritis |
| ROS | Reactive Oxygen Species |
| SOD | Superoxide Dismutase |
| TB | Tuberculosis |
| TBX A2 | Thromboxane A2 |
| TH | Total Hydropeoxides |
| TNF-α | Tumor Necrosis Factor alpha |
| tsDMARDs | Targeted synthetic DMARDs |
| VEGF | Vascular Endothelial Growth Factor |
References
- López-Armada, M.J.; Fernández-Rodríguez, J.A.; Blanco, F.J. Mitochondrial Dysfunction and Oxidative Stress in Rheumatoid Arthritis. Antioxidants 2022, 11, 1151. [Google Scholar] [CrossRef] [PubMed]
- Souliotis, V.L.; Vlachogiannis, N.I.; Pappa, M.; Argyriou, A.; Ntouros, P.A.; Sfikakis, P.P. DNA Damage Response and Oxidative Stress in Systemic Autoimmunity. Int. J. Mol. Sci. 2020, 21, 55. [Google Scholar] [CrossRef] [PubMed]
- Wójcik, P.; Gegotek, A.; Žarković, N.; Skrzydlewska, E. Oxidative Stress and Lipid Mediators Modulate Immune Cell Functions in Autoimmune Diseases. Int. J. Mol. Sci. 2021, 22, 723. [Google Scholar] [CrossRef] [PubMed]
- Guo, Q.; Wang, Y.; Xu, D.; Nossent, J.; Pavlos, N.J.; Xu, J. Rheumatoid arthritis: Pathological mechanisms and modern pharmacologic therapies. Bone Res. 2018, 6, 15. [Google Scholar] [CrossRef]
- Saalfeld, W.; Mixon, A.M.; Zelie, J.; Lydon, E.J. Differentiating Psoriatic Arthritis from Osteoarthritis and Rheumatoid Arthritis: A Narrative Review and Guide for Advanced Practice Providers. Rheumatol. Ther. 2021, 8, 1493–1517. [Google Scholar] [CrossRef]
- Bullock, J.; Rizvi, S.A.; Saleh, A.M.; Ahmed, S.S.; Do, D.P.; Ansari, R.A.; Ahmed, J. Rheumatoid arthritis: A brief overview of the treatment. Med. Princ. Pract. 2018, 27, 501–507. [Google Scholar] [CrossRef]
- Buckley, C.D.; Ospelt, C.; Gay, S.; Midwood, K.S. How the tissue microenvironment affects inflammation in RA. Nat. Rev. Rheumatol. 2021, 17, 195–212. [Google Scholar] [CrossRef]
- Rilling, S.H. 30 years of ozone/oxygen therapy: A historical perspective. Proc. Elev. Ozone Congr. 1993, M-1-3–M-1-6. [Google Scholar]
- Malatesta, M.; Tabaracci, G.; Pellicciari, C. Low-Dose Ozone as a Eustress Inducer: Experimental Evidence of the Molecular Mechanisms Accounting for Its Therapeutic Action. Int. J. Mol. Sci. 2024, 25, 12657. [Google Scholar] [CrossRef]
- Al-Dalain, S.M.; Martíneza, G.; Candelario-Jalil, E.; Menéndez, S.; Re, L.; Giulianid, A.; León, O.S. Ozone treatment reduces markers of oxidative and endothelial damage in an experimental diabetes model in rats. Pharmacol. Res. 2001, 44, 191–196. [Google Scholar] [CrossRef]
- Díaz-Soto, M.T.; Pérez, A.F.; Vaillant, J.D.; Mallok, A.; Viebahn-Hänsler, R.; Cepero, S.M.; Fernández, O.S.L. Ozone Oxidative Postconditioning Protects Against the Injury Associated with Alcohol Withdrawal Syndrome in Rats. Ozone Sci. Eng. 2012, 34, 425–431. [Google Scholar] [CrossRef]
- Martínez-Sánchez, G.; Al-Dalain, S.M.; Menéndez, S.; Re, L.; Giu-liani, A.; Candelario-Jalil, E.; Álvarez, H.; Fernández-Montequín, J.I.; León, O.S. Therapeutic efficacy of ozone in patients with diabetic foot. Eur. J. Pharmacol. 2005, 523, 151–161. [Google Scholar] [CrossRef] [PubMed]
- Fernández, O.S.L.; Oru, G.T.; Viebahn-Hänsler, R.; Cabreja, G.L.; Espinosa, I.S.; Fernández, E.G. Medical ozone arrests oxidative damage progression and regulates vasoactive mediator levels in elderly patients (60–70 years) with oxidative etiology diseases. Front. Physiol. 2022, 13, 1029805. [Google Scholar] [CrossRef]
- León, O.S.; Menéndez, S.; Merino, N.; Castillo, R.; Sam, S.; Pérez, L.; Cruz, E.; Bocci, V. Ozone oxidative preconditioning: A protection against cellular damage by free radicals. Mediat. Inflamm. 1998, 7, 289–294. [Google Scholar] [CrossRef]
- Scassellati, C.; Galoforo, A.C.; Bonvicini, C.; Esposito, C.; Ricevuti, G. Ozone: A natural bioactive molecule with antioxidant property as potential new strategy in aging and in neurodegenerative disorders. Ageing Res. Rev. 2020, 63, 101138. [Google Scholar] [CrossRef]
- Travagli, V.; Iorio, E.L. The Biological Molecular Action of Ozone Its Derivatives: State-of-the-Art Enhanced Scenarios Quality Insights. Int. J. Mol. Sci. 2023, 24, 8465. [Google Scholar] [CrossRef]
- Clavo, B.; Martínez-Sánchez, G.; Rodríguez-Esparragón, F.; Ro-dríguez-Abreu, D.; Galván, S.; Aguiar-Bujanda, D.; Díaz-Garrido, J.A.; Cañas, S.; Torres-Mata, L.B.; Fabelo, H.; et al. Modulation by Ozone Therapy of Oxidative Stress in Chemotherapy-Induced Peripheral Neuropathy: The Background for a Randomized Clinical Trial. Randomized Clin. Trial. Int. J. Mol. Sci. 2021, 22, 2802. [Google Scholar] [CrossRef]
- Cisterna, B.; Costanza, M.; Nodari, A.; Galiè, M.; Zanzoni, S.; Bernardi, P.; Covi, V.; Tabaracci, G.; Malatesta, M. Ozone Activates the Nrf2 Pathway and Improves Preservation of Explanted Adipose Tissue In Vitro. Antioxidants 2020, 9, 989. [Google Scholar] [CrossRef]
- Monti, S.; Klersy, C.; Gorla, R.; Sarzi-Puttini, P.; Atzeni, F.; Fu Pellerito, R.; Saro, E.; Paolazzi, G.; Roc-chetta, P.A.; Favalli, E.G. Factors influencing the choice of first- and second-line biologic therapy for the treatment of rheumatoid arthritis: Real-life data from the Italian LORHEN registry. Clin. Rheumatol. 2017, 36, 753–761. [Google Scholar] [CrossRef]
- Jing, W.; Liu, C.; Su, C.; Liu, L.; Chen, P.; Li, X.; Zhang, X.; Yuan, B.; Wang, H.; Du, X. Role of reactive oxygen species and mitochondrial damage in rheumatoid arthritis and targeted drugs. Front. Immunol. 2023, 14, 1107670. [Google Scholar] [CrossRef]
- Wang, D.F.; Cao, X.; Ye, Q.; Wang, Q.; Zhang, M.; Xiao, C. The Role of Reactive Oxygen Species in the Rheumatoid Arthritis-Associated Synovial Microenvironment. Antioxidants 2022, 11, 1153. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Zhou, H.; Liu, L. Side effects of methotrexate therapy for rheumatoid arthritis: A systematic review. Eur. J. Med. Chem. 2018, 158, 502–516. [Google Scholar] [CrossRef] [PubMed]
- Weinblatt, M.E.; Bathon, J.M.; Kremer, J.M.; Fleischmann, R.M.; Schiff, M.H.; Martin, R.W.; Baumgartner, S.W.; Park, G.S.; Mancini, E.L.; Genovese, M.C. Safety and efficacy of etanercept beyond 10 years of therapy in North American patients with early and longstanding rheumatoid arthritis. Arthritis Care Res. 2011, 63, 373–382. [Google Scholar] [CrossRef]
- Sartori, N.S.; Picon, P.; Papke, A.; Neyeloff, J.L.; da Silva Chakr, R.M. A population-based study of tuberculosis incidence among rheumatic disease patients under anti-TNF treatment. PLoS ONE 2019, 14, e02249. [Google Scholar] [CrossRef]
- Magni, G.; Ceruti, S. Adenosine Signaling in Autoimmune Disorders. Pharmaceuticals 2020, 13, 260. [Google Scholar] [CrossRef]
- Wolff, A. Eine medizinische Verwendbarkeit von Ozon. Dtsche. Med. Wschr. 1915, 11, 311–314. [Google Scholar] [CrossRef]
- Viebahn-Hänsler, R.; Fernández, O.S.L. Ozone in Medicine: Clinical Evaluation and Evidence Classification of the Systemic Ozone Applications, Major Autohemotherapy and Rectal Insufflation, According to the Requirements for Evidence-Based Medicine. Ozone Sci. Eng. 2016, 38, 322–345. [Google Scholar] [CrossRef]
- Steppan, J.M.; Meaders, T.; Muto, B.S.M.; Murphy, K.J. A Metaanalysis of the Effectiveness and Safety of Ozone Treatments for Herniated Lumbar Discs. J. Vasc. Interv. Radiol. 2010, 21, 534–548. [Google Scholar] [CrossRef]
- Oru, G.T.; Viebhan-Haensler, R.; Matos, Y.H.; Rodríguez, D.D.; Orta, M.C.; Fernández, O.S.L. Medical ozone prevents inflammatory effects from carrageenan-induced knee joint synovitis in rats through A1 adenosine receptor, as well as lipid and protein oxidative damages. J. Sci. Res. Stud. 2018, 5, 65–72. [Google Scholar]
- Vaillant, J.D.; Fraga, A.; Díaz, M.T.; Mallok, A.; Vie-bahn-Hänsler, R.; Fahmy, Z.; Barberá, A.; Delgado, L.; Menéndez, S.; Fernández, O.S.L. Ozone oxidative postconditioning ameliorates joint damage and decreases pro-inflammatory cytokine levels and oxidative stress in PG/PS-induced arthritis in rats. Eur. J. Pharmacol. 2013, 714, 318–324. [Google Scholar] [CrossRef]
- León Fernández, O.S.; Ajamieh, H.H.; Berlanga, J.; Menéndez, S.; Viebahn-Hánsler, R.; Re, L. Ozone oxidative preconditioning is mediated by A1 adenosine receptors in a rat model of liver ischemia/reperfusion. Transplantation 2008, 21, 39–48. [Google Scholar]
- Peralta, C.; Vals, C.; Bartrons, R.; León, O.S.; Gelpí, E.; Roselló-Catafau, J. Effect of ozone treatment on Reactive Oxygen Species and Adenosine production during hepatic ischemia-reperfusion. Free Radic. Res. 2000, 33, 595–605. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, O.S.L.; Viebahn-Hansler, R.; Cabreja, G.L.; Espinosa, I.S.; Matos, Y.H.; Roche, L.D.; Santos, B.T.; Oru, G.T.; Vega, J.C.P. Medical ozone increases methotrexate clinical response and improves cellular redox balance in patients with rheumatoid arthritis. Eur. J. Pharmacol. 2016, 789, 313–318. [Google Scholar] [CrossRef]
- Ramkumar, V.; Hallam, D.M.; Nie, Z. Adenosine, oxidative stress and cytoprotection. Jpn. J. Pharmacol. 2001, 86, 265–274. [Google Scholar] [CrossRef]
- Asquith, D.L.; Miller, A.M.; McInnes, I.B.; Liew, F.Y. Animal models of rheumatoid arthritis. Eur. J. Immunol. 2009, 39, 2040–2044. [Google Scholar] [CrossRef]
- Ekundi-Valentim, E.; Santos, K.T.; Camargo, E.A.; Denadai-Souza, A.; Teixeira, S.A.; Zanoni, C.I.; Grant, A.D.; Wallace, J.; Muscará, M.N.; Costa, S.K. Differing effects of exogenous and endogenous hydrogen sulphide in carrageenan-induced knee joint synovitis in the rat. Br. J. Pharmacol. 2010, 15, 1463–1474. [Google Scholar] [CrossRef]
- Kimpel, D.; Dayton, T.; Fuseler, J.; Gray, L.; Kauman, K.; Wolf, R.; Grisham, M. Splenectomy attenuates streptococcal cell wall-induced arthritis and alters leucocyte activation. Arthritis Rheum. 2003, 48, 3557–3567. [Google Scholar] [CrossRef]
- Murry, C.E.; Jennings, R.B.; Reimer, K.A. Preconditioning with Ischemia: A Delay of Lethal Injury in Ischemic Myocardium. Circulation 1986, 74, 1124–1136. [Google Scholar] [CrossRef]
- Viebahn-Hänsler, R.; Fernández, O.S.L.; Fahmy, Z. Ozone in Medicine: The Low-Dose Ozone Concept—Guidelines and Treatment Strategies. Ozone Sci. Eng. 2012, 34, 408–424. [Google Scholar] [CrossRef]
- Friedman, B.; Cronstein, B. Methotrexate mechanism in treatment of rheumatoid arthritis. Jt. Bone Spine 2018, 86, 301–307. [Google Scholar] [CrossRef]
- Mallok, A.; Vaillant, J.D.; Soto, M.T.D.; Viebahn-Hänsler, R.; Viart, M.d.L.A.B.; Pérez, A.F.; Cedeño, R.I.D.; Fernández, O.S.L. Ozone protective effects against PTZ-induced generalized seizures are mediated by re-establishment of cellular redox balance and A1 adenosine receptors. Neurol. Res. 2015, 37, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Nie, Z.; Mei, Y.; Ford, M.; Rybak, L.; Marcuzzi, A.; Ren, H.; Stiles, G.L.; Ramkumar, V. Oxidative stress increases A1 adenosine receptor expression by activating nuclear factor kB. Mol. Pharmacol. 1998, 53, 663. [Google Scholar] [CrossRef] [PubMed]
- Thiele, G.M.; Duryee, M.J.; Hunter, C.D.; England, B.R.; Fletcher, B.S.; Daubach, E.C.; Pospisil, T.P.; Klassen, L.W.; Mikuls, T.R. Immunogenicand Inflammatory Responses to Citrullinated Proteins Are Enhanced Following Modification with Malondialdehyde-Acetaldehyde Adducts. Int. Immunopharmacol. 2020, 83, 106433. [Google Scholar] [CrossRef]
- Willis, M.S.; Thiele, G.M.; Tuma, D.J.; Klassen, L.W. T cell proliferative responses to malondialdehyde/acetaldehyde haptenated protein are scavenger receptor mediated. Int. Immunopharmacol. 2003, 3, 1381–1399. [Google Scholar] [CrossRef]
- Oru, G.T.; Viebhan-Haensler, R.; Cabreja, G.L.; Espinosa, I.S.; Santos, B.T.; Vega, J.C.P.; Cintas, S.S.; Sonia, O. Medical Ozone Reduces the Risk of γ-Glutamyl Transferase and Alkaline Phosphatase Abnormalities and Oxidative Stress in Rheumatoid Arthritis Patients Treated with Methotrexate. SMJ Arthritis Res. 2017, 1, 1004. [Google Scholar]
- Schmidt, S.; Messner, C.J.; Gaiser, C.; Hämmerli, C.; Suter-Dick, L. Methotrexate-Induced Liver Injury Is Associated with Oxidative Stress, Impaired Mitochondrial Respiration, and Endoplasmic Reticulum Stress In Vitro. Int. J. Mol. Sci. 2022, 23, 15116. [Google Scholar] [CrossRef]
- Aslaner, A.; Çakır, T.; Çelik, B.; Doğan, U.; Akyüz, C.; Baştürk, A.; Polat, C.; Gündüz, U.; Mayir, B.; Şehirli, A.Ö. The protective effect of intraperitoneal medical ozone preconditioning and treatment on hepatotoxicity induced by methotrexate. Int. J. Clin. Exp. Med. 2015, 8, 13303–13309. [Google Scholar]
- Vincenzi, F.; Pasquini, S.; Borea, P.A.; Varani, K. Targeting Adenosine Receptors: A Potential Pharmacological Avenue for Acute and Chronic Pain. Int. J. Mol. Sci. 2020, 21, 8710. [Google Scholar] [CrossRef]
- Bhagavatham, S.K.S.; Khanchandani, P.; Kannan, V.; Potikuri, D.; Sridharan, D.; Pulukool, S.K.; Naik, A.A.; Dandamudi, R.B.; Divi, S.M.; Pargaonkar, A.; et al. Adenosine deaminase modulates metabolic remodeling and orchestrates joint destruction in rheumatoid arthritis. Sci. Rep. 2021, 11, 15129. [Google Scholar] [CrossRef]
- Montesinos, M.C.; Desai, A.; Cronstein, B.N. Suppression of inflammation by low-dose methotrexate is mediated by adenosine A2A receptor but not A3 receptor activation in thioglycollate-induced peritonitis. Arthritis Res. Ther. 2006, 8, R53. [Google Scholar] [CrossRef]
- Pasquini, S.; Contri, C.; Borea, P.A.; Vincenzi, F.; Varani, K. Adenosine Inflammation: Here There Everywhere. Int. J. Mol. Sci. 2021, 22, 7685. [Google Scholar] [CrossRef] [PubMed]
- Konishi, H.; Kanou, E.; Yukimatsu, R.; Inui, M.; Sato, M.; Yamamoto, N.; Nakano, M.; Koshiba, M. Adenosine inhibits TNFα-induced MMP-3 production in MH7A rheumatoid arthritis synoviocytes via A2A receptor signaling. Sci. Rep. 2022, 12, 6033. [Google Scholar] [CrossRef] [PubMed]
- Pasquini, S.; Contri, C.; Cappello, M.; Borea, P.A.; Varani, K.; Vincenzi, F. Update on the recent development of allosteric modulators for adenosine receptors and their therapeutic applications. Front. Pharmacol. 2022, 13, 1030895. [Google Scholar] [CrossRef] [PubMed]
- Surapneni, K.M.; Gopan, V.S.C. Lipid peroxidation and antioxidant status in patients with rheumatoid arthritis. Indian J. Clin. Biochem. 2008, 23, 41–44. [Google Scholar] [CrossRef]
- Pacher, P.; Beckman, J.S.; Tobin, Y.M.; Liandet, L. Nitric oxide and peroxinitrite in health and disease. Physiol. Rev. 2007, 87, 315–424. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Medical Ozone Effects | Brief Study Description | Reference |
|---|---|---|
| Model 1 of Synovitis (acute) | BALB/c mice. Synovitis inducer: Carrageenan. Specific A1 receptor antagonist (DPCPX), redox status. Optical microscopy. Ozone 15 intra-articular treatments (50 µg/mL). | Oru, GT et al. (2018) [29] |
| Model 2 of Arthritis(chronic) | Lewis rats. Inducer PG/PS. TNF-α, IL-1β mRNA, redox status. Optical microscopy. Ozone for 3.5 weeks (3 times/week), intra-articular ozone (20 µg/mL). | J Dranguet et al. (2013) [30] |
| Model 3 of Liver ischemia/Reperfusion | Wistar rats. 90 min ischemia/90 min reperfusion. Transaminases, specific A1 adenosine receptor agonists (CCPX) and antagonists (DPCPX). Redox status. Optical microscopy. Ozone 15 treatments (50 µg/mL). | León et al. (2008) [31] |
| Model 4 of Liver Ischemia/Reperfusion | Wistar rats. 90 min ischemia/90 min reperfusion. Transaminases, ATP degradation, adenosine production. Redox status. Ozone 10 treatments (50 µg/mL). | C Peralta et al. (2000) [32] |
| Model 5 of Hepatotoxicity by CCl4 | Wistar rats. Hepatotoxicity (hepatic damage markers). Optical microscopy. Redox status. Ozone 15 treatments (50 µg/ml). | OS León et al. (1998) [14] |
| Model 6 of Alcohol Withdrawal | Wistar rats. Ethanol withdrawal. Redox status. Behavioral tests. Ozone 10 treatments (20 µg/mL). | MT Díaz Soto et al. (2012) [11] |
| Clinical Study: Diabetes and Diabetic Foot | 100 patients (52 received ozone). Healing, diabetic control, redox status. Ozone 20 treatments (50 µg/mL). | G Martínez-Sánchez et al. (2005) [12] |
| Clinical Study: Elderly Patients | 60 patients (45 received ozone) with rheumatoid arthritis and bronchial dysfunctions. Disease activity, prostaglandins (TBX A2, PGI2), redox status. Ozone 20 treatments (20-30 µg/mL). | OS, León et al. (2022) [13] |
| Clinical Study: Meta-analysis on Ozone Safety via Systemic Routes | 657 patients. Rectal insufflation and major autohemotherapy. According to Evidence-Based Medicine standards. | R Viebahnn, et al. (2016) [27] |
| Clinical Study: MTX + Ozone in Rheumatoid Arthritis | 60 patients (30 received ozone). Disease activity, redox status, antibodies vs. cyclic citrullinated peptides. | OS, León et al. (2016) [33] |
| Clinical Study: Hepatotoxicity Risk in MTX + Medical Ozone | 100 patients (50 received ozone). Disease activity, redox status, antibodies vs. cyclic citrullinated peptides. Hepatic damage markers. Hepatotoxicity risk evaluation. Ozone 20 treatments (20–40 µg/mL). | Oru, GT et al. (2017) [34] |
| 95% Confidence Interval | |||
|---|---|---|---|
| MARKERS | MEAN ± SD | LOWER LIMIT | UPPER LIMIT |
| IL-1β | |||
| PG/PS (inductor del daño) | 2.81 ± 0.04 | 2.76 | 2.86 |
| PG/PS + Ozone | 1.96 ± 0.08 | 1.85 | 2.07 |
| PG/PS + Oxygen | 2.87 ± 0.04 | 2.82 | 2.92 |
| TNF-α | |||
| PG/PS (inductor del daño) | 3.9 ± 0.22 | 3.6 | 3.9 |
| PG/PS ± Ozone | 2.75 ± 0.22 | 2.45 | 3.05 |
| PG/PS + Oxygen | 4.22 ± 0.43 | 3.63 | 4.81 |
| 95% Confidence Interval | |||
|---|---|---|---|
| MARKERS | MEAN ± SD | LOWER LIMIT | UPPER LIMIT |
| (A). Acute Model | |||
| MDA(μM) | |||
| Control (saline) | 1.6 ± 0.001(a) | 1.6 | 1.61 |
| Carrageenan | 1.99 ± 0.01(b) | 2.1 | 2.2 |
| Carrageenan + Ozone | 1.4 ± 0 (c) | 1.4 | 1.4 |
| Carrageenan + Oxygen | 1.8 ± 0.06 (d) | 1.73 | 1.89 |
| TH (μM) | |||
| Control (saline) | 49.3 ± 4.4 (a) | 37 | 49.4 |
| Carrageeenan | 57 ± 2.8 (b) | 48 | 56 |
| Carregenaan + Ozone | 39.6 ± 0.07 (c) | 39 | 39.5 |
| Carrageenan + Oxygen | 45.4 ± 0.3 (a) | 45 | 46 |
| (B). Chronic Model | |||
| SOD (U/mg protein) | |||
| Control (saline) | 25.8 ± 1.32 (a) | 24.5 | 27 |
| PG/PS | 3.7 ± 1.45 (b) | 2.7 | 5.2 |
| PG/PS + Ozone | 33.6 ± 1.39 (a) | 33.6 | 36.4 |
| PG/PS + Oxygen | 11.3 ± 1.75 (c) | 9.5 | 13 |
| CAT (U/mg protein) | |||
| Control (saline) | 212.2 ± 13.8 (a) | 193 | 231 |
| PG/PS | 182 ± 0.001 (a) | 181 | 182 |
| PG/PS + Ozone | 391 ±2.6 (b) | 387 | 394 |
| PG/PS + Oxygen | 208 ± 19.6 (a) | 178 | 236 |
| MTX (n = 30) | MTX + Ozone (n = 30) | |||
|---|---|---|---|---|
| Clinical Variables | Start | End | Start | End |
| Pain | 8.2 ± 0.47 (a) | 7 ± 0.65 (a) | 9.2 ± 0.37 (a) | 4.7 ± 0.33 (b,c) |
| DAS28 | 5.64 ± 0.36 (a) | 5.21 ± 0.37 (a) | 6.4 ± 0.22 (a) | 3.2 ± 0.37 (b,c) |
| HAQ-DI | 1.53 ± 0.16 (a) | 1.14 ± 0.17 (a) | 1.80 ± 0.10 (a) | 0.75 ± 0.07 (b,c) |
| CRP (mg/L) | 21.08 ± 7.12 (a) | 13.14 ± 4.26 (a) | 16.2 ± 4.75 (a) | 5.53 ± 1.48 (b,c) |
| ESR | 40.9 ± 6.62 (a) | 40.3 ± 6.08 (a) | 36.7 ± 6.38 (a) | 20 ± 4.64 (b,c) |
| Anti-CCP (U/mL) | 102.8 ± 34 (a) | 119.2 ± 39 (a) | 107 ± 62 (a) | 89.7 ± 33 (b,c) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
León Fernández, O.S.; Oru, G.T.; Viebahn-Haensler, R.; López Cabreja, G.; Serrano Espinosa, I.; Corrales Vázquez, M.E. Medical Ozone Increases Methotrexate Effects in Rheumatoid Arthritis Through a Shared New Mechanism Which Involves Adenosine. Int. J. Mol. Sci. 2025, 26, 5256. https://doi.org/10.3390/ijms26115256
León Fernández OS, Oru GT, Viebahn-Haensler R, López Cabreja G, Serrano Espinosa I, Corrales Vázquez ME. Medical Ozone Increases Methotrexate Effects in Rheumatoid Arthritis Through a Shared New Mechanism Which Involves Adenosine. International Journal of Molecular Sciences. 2025; 26(11):5256. https://doi.org/10.3390/ijms26115256
Chicago/Turabian StyleLeón Fernández, Olga Sonia, Gabriel Takon Oru, Renate Viebahn-Haensler, Gilberto López Cabreja, Irainis Serrano Espinosa, and María Elena Corrales Vázquez. 2025. "Medical Ozone Increases Methotrexate Effects in Rheumatoid Arthritis Through a Shared New Mechanism Which Involves Adenosine" International Journal of Molecular Sciences 26, no. 11: 5256. https://doi.org/10.3390/ijms26115256
APA StyleLeón Fernández, O. S., Oru, G. T., Viebahn-Haensler, R., López Cabreja, G., Serrano Espinosa, I., & Corrales Vázquez, M. E. (2025). Medical Ozone Increases Methotrexate Effects in Rheumatoid Arthritis Through a Shared New Mechanism Which Involves Adenosine. International Journal of Molecular Sciences, 26(11), 5256. https://doi.org/10.3390/ijms26115256