
Anti-LAMP-2 Antibody Seropositivity in Children with Primary Systemic Vasculitis Affecting Medium- and Large-Sized Vessels

 ,
,  ,
on behalf of the PedVas Investigator’s Network
,
on behalf of the PedVas Investigator’s Network
Abstract
1. Introduction
2. Results
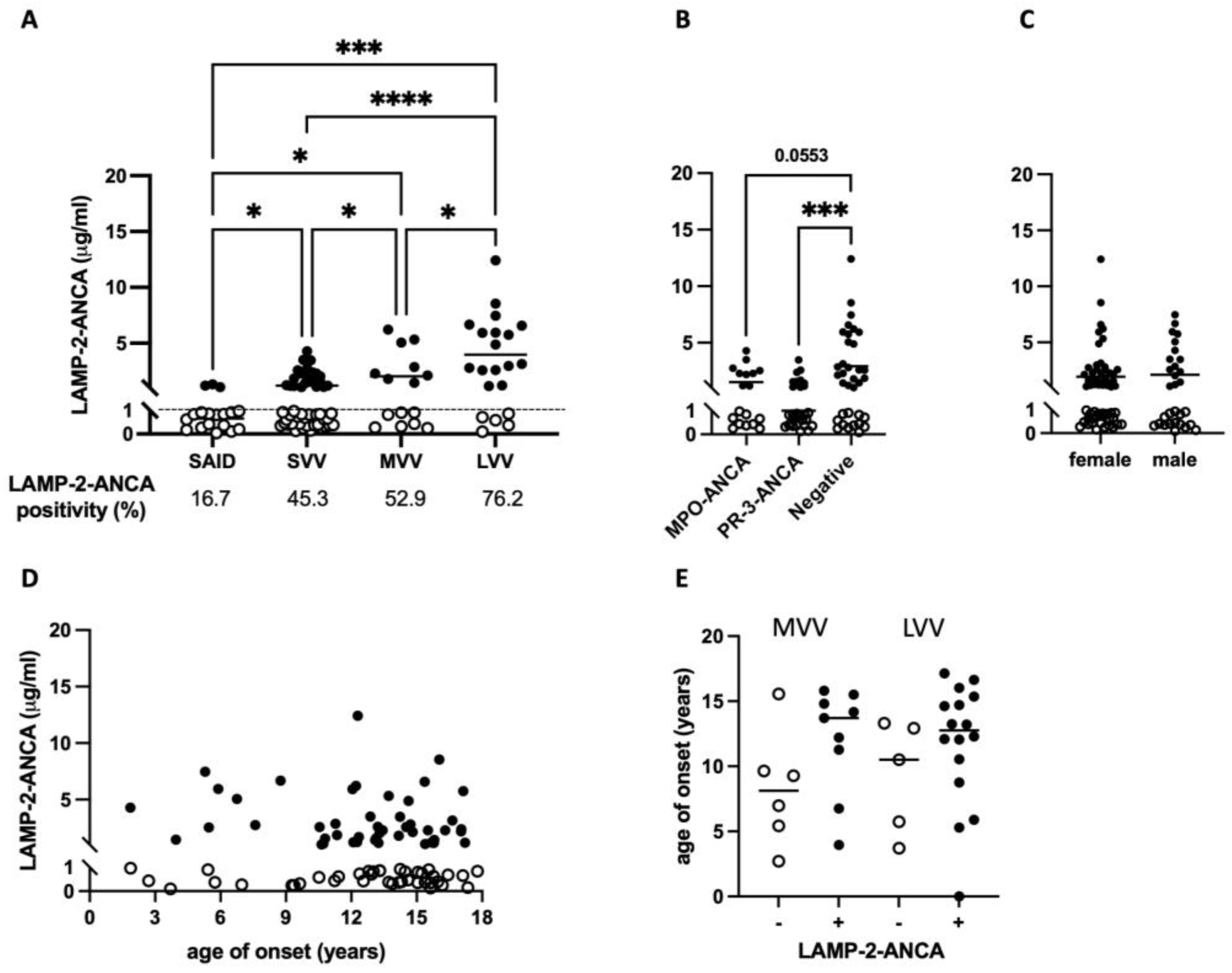
2.1. Greater Prevalence and Elevated Sera Concentration of LAMP-2-ANCA in PR3- and MPO- ANCA-Negative Vasculitis Subtypes Affecting Medium to Large Blood Vessels
2.2. LAMP-2-ANCA Seropositivity Is Associated with Lower Overall Disease Activity at Diagnosis
2.3. LAMP-2-ANCA Seropositivity and Concentration Are Not Significantly Associated with the Extent or Type of Organ Involvement
3. Discussion
4. Materials and Methods
4.1. Study Cohorts and Biosamples
4.2. Clinical Data for Chronic PSV Participants
4.3. Quantification of Active Disease in Chronic PSV Participants
4.4. Meso Scale Discovery (MSD) Electrochemiluminescence Assay to Detect Serum Anti-LAMP-2-Antibodies
4.5. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Okazaki, T.; Shinagawa, S.; Mikage, H. Vasculitis syndrome-diagnosis and therapy. J. Gen. Fam. Med. 2017, 18, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Weiss, P.F. Pediatric vasculitis. Pediatr. Clin. N. Am. 2012, 59, 407–423. [Google Scholar] [CrossRef] [PubMed]
- Gardner-Medwin, J.M.; Dolezalova, P.; Cummins, C.; Southwood, T.R. Incidence of Henoch-Schönlein purpura, Kawasaki disease, and rare vasculitides in children of different ethnic origins. Lancet 2002, 360, 1197–1202. [Google Scholar] [CrossRef] [PubMed]
- Lionaki, S.; Blyth, E.R.; Hogan, S.L.; Hu, Y.; Senior, B.A.; Jennette, C.E.; Nachman, P.H.; Jennette, J.C.; Falk, R.J. Classification of antineutrophil cytoplasmic autoantibody vasculitides: The role of antineutrophil cytoplasmic autoantibody specificity for myeloperoxidase or proteinase 3 in disease recognition and prognosis. Arthritis Rheum. 2012, 64, 3452–3462. [Google Scholar] [CrossRef] [PubMed]
- Silva de Souza, A.W. Autoantibodies in systemic vasculitis. Front. Immunol. 2015, 6, 184. [Google Scholar] [CrossRef] [PubMed]
- Kitching, A.R.; Anders, H.J.; Basu, N.; Brouwer, E.; Gordon, J.; Jayne, D.R.; Kullman, J.; Lyons, P.A.; Merkel, P.A.; Savage, C.O.S.; et al. ANCA-associated vasculitis. Nat. Rev. Dis. Primers 2020, 6, 71. [Google Scholar] [CrossRef] [PubMed]
- Quartuccio, L.; Treppo, E.; Urso, L.; Del Frate, G.; Mescia, F.; Alberici, F.; Vaglio, A.; Emmi, G. Unmet needs in ANCA-associated vasculitis: Physicians’ and patients’ perspectives. Front. Immunol. 2023, 14, 1112899. [Google Scholar] [CrossRef] [PubMed]
- Hunter, R.W.; Welsh, N.; Farrah, T.E.; Gallacher, P.J.; Dhaun, N. ANCA associated vasculitis. BMJ 2020, 369, m1070. [Google Scholar] [CrossRef] [PubMed]
- Eskelinen, E.L. Roles of LAMP-1 and LAMP-2 in lysosome biogenesis and autophagy. Mol. Asp. Med. 2006, 27, 495–502. [Google Scholar] [CrossRef]
- Kain, R.; Exner, M.; Brandes, R.; Ziebermayr, R.; Cunningham, D.; Alderson, C.A.; Davidovits, A.; Raab, I.; Jahn, R.; Ashour, O.; et al. Molecular mimicry in pauci-immune focal necrotizing glomerulonephritis. Nat. Med. 2008, 14, 1088–1096. [Google Scholar] [CrossRef]
- Li, N.; Zhu, B.; Zhu, Q.; Heizati, M.; Wu, T.; Wang, G.; Yao, X.; Luo, Q.; Liu, S.; Liu, S. Serum lysosomal-associated membrane protein-2 levels are increased in small and medium-vessel vasculitis, especially in polyarteritis nodosa. Clin. Exp. Rheumatol. 2019, 37 (Suppl. S117), 79–85. [Google Scholar] [PubMed]
- Peschel, A.; Basu, N.; Benharkou, A.; Brandes, R.; Brown, M.; Rees, A.J.; Kain, R. Autoantibodies to hLAMP-2 in ANCA-negative pauci-immune focal necrotizing GN. J. Am. Soc. Nephrol. 2014, 25, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Gibson, K.M.; Kain, R.; Luqmani, R.A.; Ross, C.J.; Cabral, D.A.; Brown, K.L. Autoantibodies Against Lysosome Associated Membrane Protein-2 (LAMP-2) in Pediatric Chronic Primary Systemic Vasculitis. Front. Immunol. 2021, 11, 624758. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Hu, C.; Sun, F.; Li, J.; Yang, Y.; Tian, X.; Zeng, X. Study on the association of serum pentraxin-3 and lysosomal-associated membrane protein-2 levels with disease activity in Chinese Takayasu’s arteritis patients. Clin. Exp. Rheumatol. 2019, 37 (Suppl. S117), 109–115. [Google Scholar]
- Kawakami, T.; Ishizu, A.; Arimura, Y.; Soma, Y. Serum anti-lysosomal-associated membrane protein-2 antibody levels in cutaneous polyarteritis nodosa. Acta Derm. Venereol. 2013, 93, 70–73. [Google Scholar] [CrossRef] [PubMed]
- Moiseev, S.; Zykova, A.; Bulanov, N.; Gitel, E.; Novikov, P.; Bulanova, M.; Kronbichler, A.; Jayne, D. Is There a Role for LAMP-2 Autoantibodies in Patients with Antineutrophil Cytoplasmic Antibody-associated Vasculitis? J. Rheumatol. 2020, 47, 636–638. [Google Scholar] [CrossRef]
- Kain, R.; Tadema, H.; McKinney, E.F.; Benharkou, A.; Brandes, R.; Peschel, A.; Hubert, V.; Feenstra, T.; Sengölge, G.; Stegeman, C.; et al. High prevalence of autoantibodies to hLAMP-2 in anti-neutrophil cytoplasmic antibody-associated vasculitis. J. Am. Soc. Nephrol. 2012, 23, 556–566. [Google Scholar] [CrossRef] [PubMed]
- Roth, A.J.; Brown, M.C.; Smith, R.N.; Badhwar, A.K.; Parente, O.; Chung, H.; Bunch, D.O.; McGregor, J.G.; Hogan, S.L.; Hu, Y.; et al. Anti-LAMP-2 antibodies are not prevalent in patients with antineutrophil cytoplasmic autoantibody glomerulonephritis. J. Am. Soc. Nephrol. 2012, 23, 545–555. [Google Scholar] [CrossRef] [PubMed]
- Zhu, B.; Cai, X.; Zhu, Q.; Wu, T.; Liu, S.; Liu, S.; Hong, J.; Li, N. The Association of Serum Anti-Lysosomal-Associated Membrane Protein-2 Antibody with Vasculitis Combined with Hypertension. Int. J. Hypertens. 2022, 2022, 9656560. [Google Scholar] [CrossRef] [PubMed]
- Ball, G.V. The history of ANCA-associated vasculitis. Rheum. Dis. Clin. N. Am. 2010, 36, 439–446. [Google Scholar] [CrossRef]
- Hilhorst, M.; van Paassen, P.; Tervaert, J.W. Proteinase 3-ANCA Vasculitis versus Myeloperoxidase-ANCA Vasculitis. J. Am. Soc. Nephrol. 2015, 26, 2314–2327. [Google Scholar] [CrossRef]
- Cohen Tervaert, J.W. Should proteinase-3 and myeloperoxidase anti-neutrophil cytoplasmic antibody vasculitis be treated differently: Part 2. Nephrol. Dial. Transpl. 2019, 34, 384–387. [Google Scholar] [CrossRef]
- Fussner, L.A.; Hummel, A.M.; Schroeder, D.R.; Silva, F.; Cartin-Ceba, R.; Snyder, M.R.; Hoffman, G.S.; Kallenberg, C.G.; Langford, C.A.; Merkel, P.A.; et al. Factors Determining the Clinical Utility of Serial Measurements of Antineutrophil Cytoplasmic Antibodies Targeting Proteinase 3. Arthritis Rheumatol. 2016, 68, 1700–1710. [Google Scholar] [CrossRef] [PubMed]
- Kemna, M.J.; Damoiseaux, J.; Austen, J.; Winkens, B.; Peters, J.; van Paassen, P.; Cohen Tervaert, J.W. ANCA as a predictor of relapse: Useful in patients with renal involvement but not in patients with nonrenal disease. J. Am. Soc. Nephrol. 2015, 26, 537–542. [Google Scholar] [CrossRef] [PubMed]
- Hilhorst, M.; Arndt, F.; Joseph Kemna, M.; Wieczorek, S.; Donner, Y.; Wilde, B.; Thomas Epplen, J.; van Paassen, P.; Cohen Tervaert, J.W. HLA-DPB1 as a Risk Factor for Relapse in Antineutrophil Cytoplasmic Antibody-Associated Vasculitis: A Cohort Study. Arthritis Rheumatol. 2016, 68, 1721–1730. [Google Scholar] [CrossRef] [PubMed]
- Kain, R.; Rees, A.J. What is the evidence for antibodies to LAMP-2 in the pathogenesis of ANCA associated small vessel vasculitis? Curr. Opin. Rheumatol. 2013, 25, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Tomasson, G.; Grayson, P.C.; Mahr, A.D.; Lavalley, M.; Merkel, P.A. Value of ANCA measurements during remission to predict a relapse of ANCA-associated vasculitis—A meta-analysis. Rheumatology 2012, 51, 100–109. [Google Scholar] [CrossRef]
- Mukherjee, M.; Thomas, S.R.; Radford, K.; Dvorkin-Gheva, A.; Davydchenko, S.; Kjarsgaard, M.; Svenningsen, S.; Almas, S.; Felix, L.C.; Stearns, J.; et al. Sputum Antineutrophil Cytoplasmic Antibodies in Serum Antineutrophil Cytoplasmic Antibody-Negative Eosinophilic Granulomatosis with Polyangiitis. Am. J. Respir. Crit. Care Med. 2019, 199, 158–170. [Google Scholar] [CrossRef] [PubMed]
- Seidowsky, A.; Hoffmann, M.; Ruben-Duval, S.; Mesbah, R.; Masy, E.; Kyndt, X.; Maouad, B.; Billion, S.; Noël, L.H.; Vanhille, P.; et al. Elastase-ANCA-associated idiopathic necrotizing crescentic glomerulonephritis—A report of three cases. Nephrol. Dial. Transplant. 2007, 22, 2068–2071. [Google Scholar] [CrossRef]
- Moodie, F.D.; Leaker, B.; Cambridge, G.; Totty, N.F.; Segal, A.W. Alpha-enolase: A novel cytosolic autoantigen in ANCA positive vasculitis. Kidney Int. 1993, 43, 675–681. [Google Scholar] [CrossRef][Green Version]
- Cabral, D.A.; Uribe, A.G.; Benseler, S.; O’Neil, K.M.; Hashkes, P.J.; Higgins, G.; Zeft, A.S.; Lovell, D.J.; Kingsbury, D.J.; Stevens, A.; et al. Classification, presentation, and initial treatment of Wegener’s granulomatosis in childhood. Arthritis Rheum. 2009, 60, 3413–3424. [Google Scholar] [CrossRef] [PubMed]
- Cabral, D.A.; Canter, D.L.; Muscal, E.; Nanda, K.; Wahezi, D.M.; Spalding, S.J.; Twilt, M.; Benseler, S.M.; Campillo, S.; Charuvanij, S.; et al. Comparing Presenting Clinical Features in 48 Children with Microscopic Polyangiitis to 183 Children Who Have Granulomatosis with Polyangiitis (Wegener’s): An ARChiVe Cohort Study. Arthritis Rheumatol. 2016, 68, 2514–2526. [Google Scholar] [CrossRef] [PubMed]
- Morishita, K.A.; Moorthy, L.N.; Lubieniecka, J.M.; Twilt, M.; Yeung, R.S.M.; Toth, M.B.; Shenoi, S.; Ristic, G.; Nielsen, S.M.; Luqmani, R.A.; et al. Early Outcomes in Children with Antineutrophil Cytoplasmic Antibody-Associated Vasculitis. Arthritis Rheumatol. 2017, 69, 1470–1479. [Google Scholar] [CrossRef] [PubMed]
- Gill, E.E.; Smith, M.L.; Gibson, K.M.; Morishita, K.A.; Lee, A.H.Y.; Falsafi, R.; Graham, J.; Foell, D.; Benseler, S.M.; Ross, C.J.; et al. Different Disease Endotypes in Phenotypically Similar Vasculitides Affecting Small-to-Medium Sized Blood Vessels. Front. Immunol. 2021, 12, 638571. [Google Scholar] [CrossRef] [PubMed]
- Marino, A.; Tirelli, F.; Giani, T.; Cimaz, R. Periodic fever syndromes and the autoinflammatory diseases (AIDs). J. Transl. Autoimmun. 2020, 3, 100031. [Google Scholar] [CrossRef] [PubMed]
- Tucker, L.B.; Niemietz, I.; Mangat, P.; Belen, M.; Tekano, J.; Cabral, D.A.; Guzman, J.; Houghton, K.M.; Morishita, K.A.; Chan, M.O.; et al. Children with systemic autoinflammatory diseases have multiple, mixed ethnicities that reflect regional ethnic diversity. Clin. Exp. Rheumatol. 2021, 39 (Suppl. S132), 124–128. [Google Scholar] [CrossRef] [PubMed]
- Ozen, S.; Pistorio, A.; Iusan, S.M.; Bakkaloglu, A.; Herlin, T.; Brik, R.; Buoncompagni, A.; Lazar, C.; Bilge, I.; Uziel, Y.; et al. EULAR/PRINTO/PRES criteria for Henoch-Schönlein purpura, childhood polyarteritis nodosa, childhood Wegener granulomatosis and childhood Takayasu arteritis: Ankara 2008. Part II: Final classification criteria. Ann. Rheum. Dis. 2010, 69, 798–806. [Google Scholar] [CrossRef] [PubMed]
- Fries, J.F.; Hunder, G.G.; Bloch, D.A.; Michel, B.A.; Arend, W.P.; Calabrese, L.H.; Fauci, A.S.; Leavitt, R.Y.; Lie, J.T.; Lightfoot, R.W., Jr.; et al. The American College of Rheumatology 1990 criteria for the classification of vasculitis. Summary. Arthritis Rheum 1990, 33, 1135–1136. [Google Scholar] [CrossRef] [PubMed]
- Watts, R.; Lane, S.; Hanslik, T.; Hauser, T.; Hellmich, B.; Koldingsnes, W.; Mahr, A.; Segelmark, M.; Cohen-Tervaert, J.W.; Scott, D. Development and validation of a consensus methodology for the classification of the ANCA-associated vasculitides and polyarteritis nodosa for epidemiological studies. Ann. Rheum. Dis. 2007, 66, 222–227. [Google Scholar] [CrossRef]
- Lanham, J.G.; Elkon, K.B.; Pusey, C.D.; Hughes, G.R. Systemic vasculitis with asthma and eosinophilia: A clinical approach to the Churg-Strauss syndrome. Medicine 1984, 63, 65–81. [Google Scholar] [CrossRef]
- Dolezalova, P.; Price-Kuehne, F.E.; Özen, S.; Benseler, S.M.; Cabral, D.A.; Anton, J.; Brunner, J.; Cimaz, R.; O’Neil, K.M.; Wallace, C.A.; et al. Disease activity assessment in childhood vasculitis: Development and preliminary validation of the Paediatric Vasculitis Activity Score (PVAS). Ann. Rheum. Dis. 2013, 72, 1628–1633. [Google Scholar] [CrossRef] [PubMed]
- Kain, R.; Matsui, K.; Exner, M.; Binder, S.; Schaffner, G.; Sommer, E.M.; Kerjaschki, D. A novel class of autoantigens of anti-neutrophil cytoplasmic antibodies in necrotizing and crescentic glomerulonephritis: The lysosomal membrane glycoprotein h-lamp-2 in neutrophil granulocytes and a related membrane protein in glomerular endothelial cells. J. Exp. Med. 1995, 181, 585–597. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Small Vessel (n = 53) | Medium Vessel (n = 16) | Large Vessel (n = 21) | |
|---|---|---|---|
| PSV subtype, n (%) | |||
| GPA/limGPA | 43 (81.1) | - | - |
| MPA | 5 (9.4) | - | - |
| EGPA | 2 (3.8) | - | - |
| ANCA + GN | 1 (1.9) | - | - |
| PAN/cPAN | - | 14 (87.5) | - |
| TA | - | - | 19 (90.5) |
| UPV | 2 (3.8) | 2 (12.5) | 2 (9.5) |
| Sex, n (%) | |||
| Female | 35 (66.0) | 10 (62.5) | 15 (71.4) |
| Male | 18 (34.0) | 6 (37.5) | 6 (28.6) |
| No significant difference in representation of males/females between groups (p = 0.8400) based on chi-squared test | |||
| Age (years) of symptom onset—median (range) | * 14.2 (1.9–17.3) | 11.2 (2.7–15.8) | 12.6 (3.7–17.1) |
| 1 ANCA Antigen Positivity, n (%) | |||
| Proteinase 3 (PR3) | 29 (55.8) | 1 (6.7) | - |
| Myeloperoxidase (MPO) | 18 (34.6) | - | - |
| PR3 and MPO | 2 (3.8) | - | - |
| Neither | 3 (5.8) | 14 (93.3) | 18 (100) |
| Disease activity (pVAS) at diagnosis | |||
| Total pVAS, median (range) | 19 (6–50) | 8 (1–18) | 16 (6–26) |
| Subcomponent pVAS, median (range) | |||
| Renal | 10 (0–12) | 0 (0–6) | 4 (0–12) |
| Cardiovascular | 0 (0–4) | 0 | 4 (0–6) |
| Pulmonary | 0 (0–6) | 0 (0–4) | 0 (0–6) |
| Upper respiratory tract | 4 (0–6) | 0 (0–6) | 0 (0–4) |
| 2 Induction Treatment, n (%) | |||
| 3 Immune-suppressing agents | 38 (73.0) | 4 (25.0) | 2 (9.5) |
| 4 Disease-modifying agents | 6 (11.5) | 6 (37.5) | 11 (52.4) |
| 5 Biologic agents | - | 1 (6.3) | 6 (28.6) |
| Corticosteroids | 48 (92.3) | 12 (75.0) | 20 (95.2) |
| 2 Maintenance Treatment, n (%) | |||
| 3 Immune-suppressing agents | 16 (37.2) | 4 (28.6) | 4 (20.0) |
| 4 Disease-modifying agents | 14 (32.5) | 9 (64.3) | 10 (50.0) |
| 5 Biologic agents | - | 2 (14.3) | 8 (40.0) |
| Corticosteroids | 41 (95.3) | 10 (71.4) | 19 (95.0) |
| PSV Total (n = 90) | Small Vessel (n = 53) | Medium Vessel (n = 16) | Large Vessel (n = 21) | |||||
|---|---|---|---|---|---|---|---|---|
| a LAMP-2-ANCA | − | + | − | + | − | + | − | + |
| n | n = 41 | n = 49 | n = 29 | n = 24 | n = 7 | n = 9 | n = 5 | n = 16 |
| % | 45.6% | 54.4% | 54.7% | 45.3% | 41.2% | 52.9% | 23.8% | * 76.2% |
| b Sex, n (%) | ||||||||
| Female | 26 (63.4) | 34 (69.4) | 18 (62.1) | 17 (70.8) | 4 (57.1) | 6 (66.7) | 4 (80.0) | 11 (68.8) |
| Male | 15 (36.6) | 15 (30.6) | 11 (37.9) | 7 (29.2) | 3 (42.9) | 3 (33.3) | 1 (20.0) | 5 (31.2) |
| c Age of onset, years | ||||||||
| Median | 13.8 | 13.2 | 14.5 | 13.1 | 8.1 | 13.7 | 10.5 | 13.2 |
| Range | 1.9–17.3 | 1.9–17.2 | 1.9–17.8 | 1.9–17.2 | 2.7–15.5 | 4.0–15.8 | 3.7–13.3 | 5.3–17.1 |
| d ANCA antigen positivity, n (%) | ||||||||
| PR3 | 19 (22.4) | 11 (12.9) | 18 (34.6) | 11 (21.2) | 1 (5.9) | − | − | − |
| MPO | 9 (10.6) | 9 (10.6) | 9 (17.3) | 9 (17.3) | − | − | − | − |
| PR3 and MPO | 1 (1.2) | 1 (1.2) | 1 (1.9) | 1 (1.9) | − | − | − | − |
| Neither | 12 (14.1) | 23 (27.1) | 1 (1.9) | 2 (3.8) | 6 (35.3) | 8 (47.1) | 5 (27.8) | 13 (72.2) |
| PSV Total | Small Vessel | Medium Vessel | Large Vessel | |||||
|---|---|---|---|---|---|---|---|---|
| a LAMP-2-ANCA | − | + | − | + | − | + | − | + |
| Disease activity (total pVAS), median (range) | ||||||||
| b at diagnosis | 19 (5–50) | * 15 (1–36) | 20 (7–50) | 18 (6–36) | 8 (5–31) | 7 (1–18) | 19 (6–20) | 15 (6–26) |
| c at 1-year | 0 (0–4) | 0 (0–12) | 0 (0–6) | 0 (0–12) | 0 (0) | 1 (0–4) | 2 (3–4) | 0 (0–12) |
| d Inactive disease (total pVAS ≤ 1), n (%) | ||||||||
| at 1-year | 26 (37.1) | 25 (35.7) | 19 (48.7) | 12 (30.8) | 5 (38.5) | 4 (30.8) | 2 (11.1) | 9 (50.0) |
| Organ System | LAMP-2-ANCA | b Adjusted OR (95% CI) | Standard Error | p-Value | |
|---|---|---|---|---|---|
| Seronegative (n = 36) a | Seropositive (n = 41) a | ||||
| Cardiovascular | 7 (19.4%) | 14 (34.1%) | 0.82 (0.15, 3.73) | 0.79 | 0.800 |
| Renal | 29 (81.0%) | 35 (85.4%) | 1.70 (0.46, 6.91) | 0.68 | 0.429 |
| Pulmonary | 16 (44.4%) | 9 (22.0%) | 0.49 (0.16, 1.46) | 0.56 | 0.198 |
| URT | 19 (52.8%) | 13 (31.7%) | 0.58 (0.19, 1.79) | 0.57 | 0.339 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Akbaba, T.H.; Toor, K.K.; Mann, S.K.; Gibson, K.M.; Alfaro, G.A.; Balci-Peynircioglu, B.; Cabral, D.A.; Morishita, K.A.; Brown, K.L., on behalf of the PedVas Investigator’s Network. Anti-LAMP-2 Antibody Seropositivity in Children with Primary Systemic Vasculitis Affecting Medium- and Large-Sized Vessels. Int. J. Mol. Sci. 2024, 25, 3771. https://doi.org/10.3390/ijms25073771
Akbaba TH, Toor KK, Mann SK, Gibson KM, Alfaro GA, Balci-Peynircioglu B, Cabral DA, Morishita KA, Brown KL on behalf of the PedVas Investigator’s Network. Anti-LAMP-2 Antibody Seropositivity in Children with Primary Systemic Vasculitis Affecting Medium- and Large-Sized Vessels. International Journal of Molecular Sciences. 2024; 25(7):3771. https://doi.org/10.3390/ijms25073771
Chicago/Turabian StyleAkbaba, Tayfun Hilmi, Kirandeep K. Toor, Simranpreet K. Mann, Kristen M. Gibson, Gabriel Alejandro Alfaro, Banu Balci-Peynircioglu, David A. Cabral, Kimberly A. Morishita, and Kelly L. Brown on behalf of the PedVas Investigator’s Network. 2024. "Anti-LAMP-2 Antibody Seropositivity in Children with Primary Systemic Vasculitis Affecting Medium- and Large-Sized Vessels" International Journal of Molecular Sciences 25, no. 7: 3771. https://doi.org/10.3390/ijms25073771
APA StyleAkbaba, T. H., Toor, K. K., Mann, S. K., Gibson, K. M., Alfaro, G. A., Balci-Peynircioglu, B., Cabral, D. A., Morishita, K. A., & Brown, K. L., on behalf of the PedVas Investigator’s Network. (2024). Anti-LAMP-2 Antibody Seropositivity in Children with Primary Systemic Vasculitis Affecting Medium- and Large-Sized Vessels. International Journal of Molecular Sciences, 25(7), 3771. https://doi.org/10.3390/ijms25073771