
Prognostic Value of Liquid-Biopsy-Based Biomarkers in Upper Tract Urothelial Carcinoma

 ,
,  , , , ,
, , , ,
Abstract
1. Introduction
2. Results
2.1. Clinicopathological Features of the Cohort
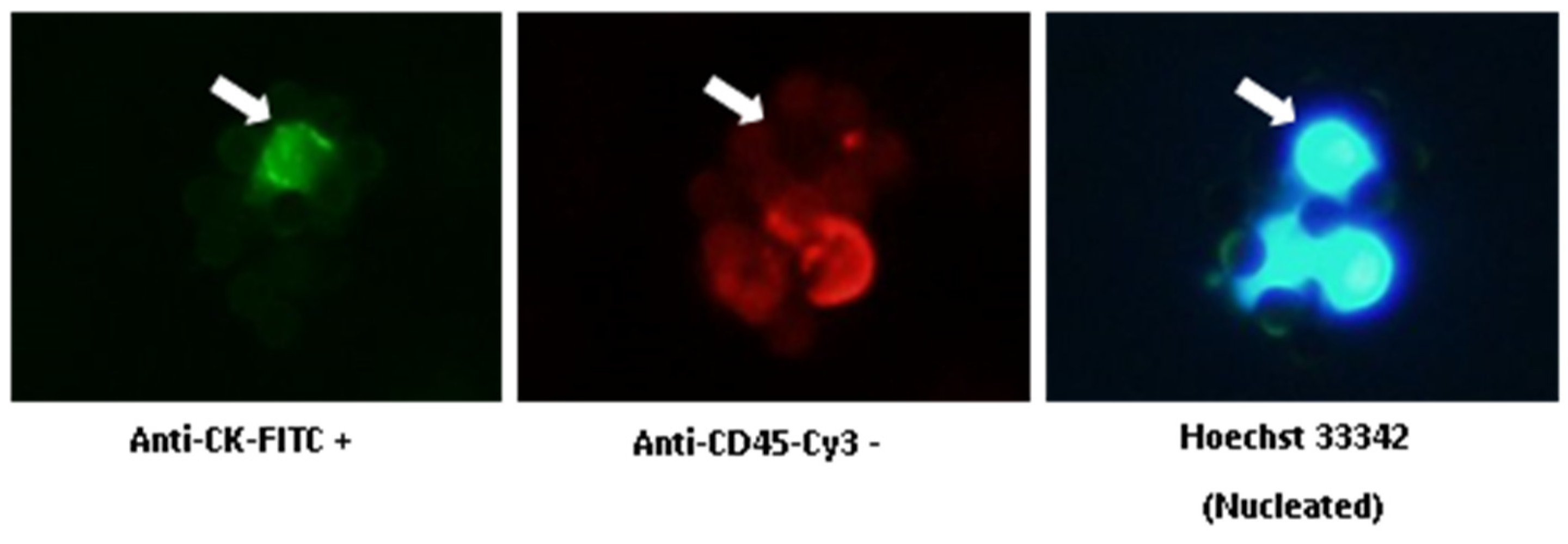
2.2. CTC Enumeration for Monitoring UTUC Patients
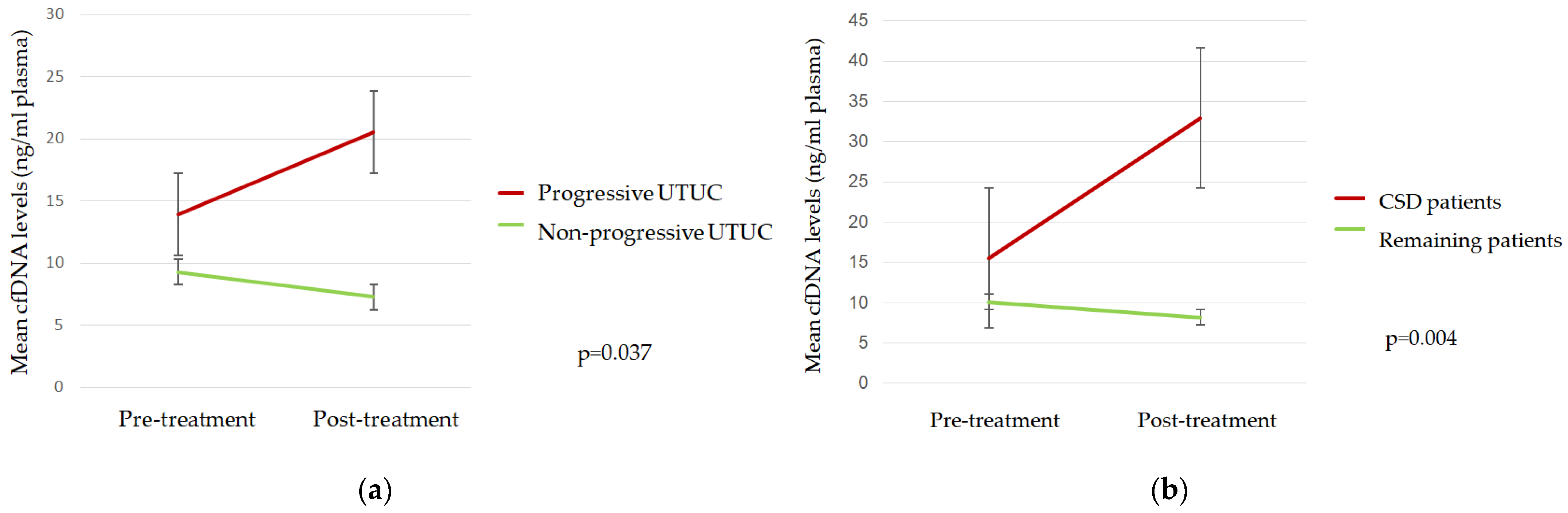
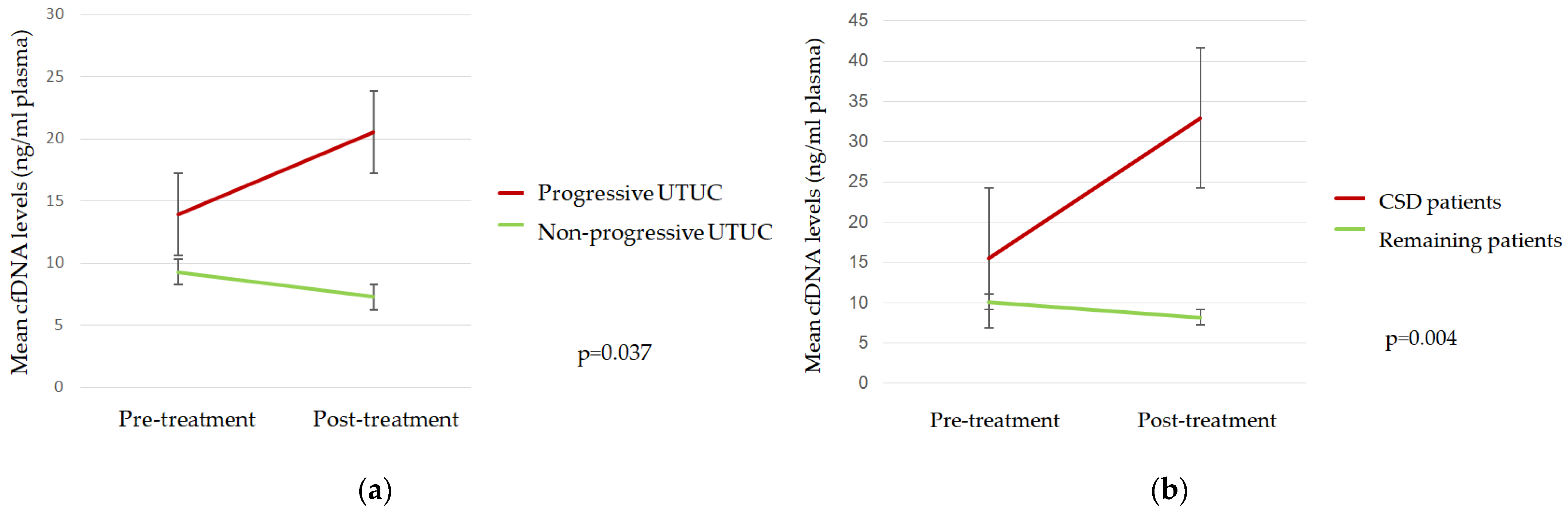
2.3. cfDNA Levels during Follow-Up
2.4. ctDNA Analysis
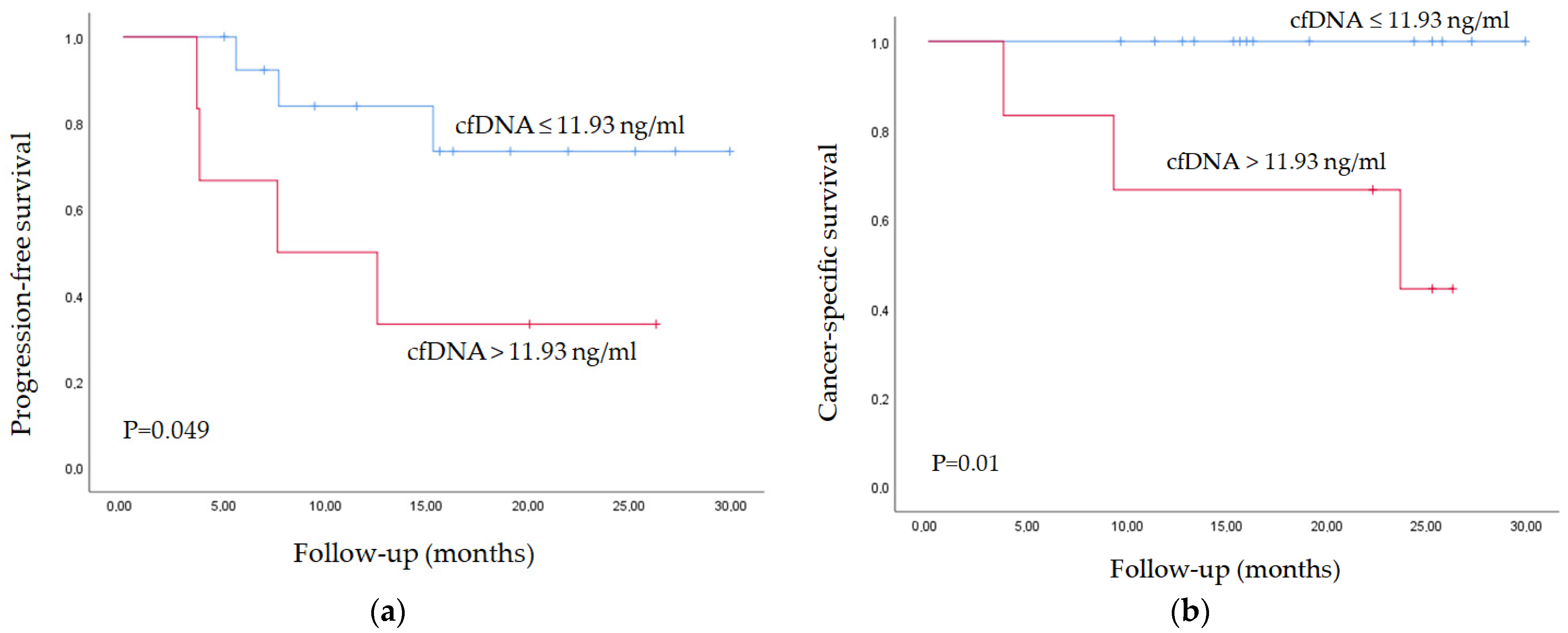
2.5. Survival Analysis
3. Discussion
4. Materials and Methods
4.1. Patients and Samples
4.2. CTC Isolation and Enumeration
4.3. cfDNA Isolation
4.4. Droplet Digital PCR
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Soria, F.; Shariat, S.F.; Lerner, S.P.; Fritsche, H.M.; Rink, M.; Kassouf, W.; Spiess, P.E.; Lotan, Y.; Ye, D.; Fernández, M.I.; et al. Epidemiology, Diagnosis, Preoperative Evaluation and Prognostic Assessment of Upper-Tract Urothelial Carcinoma (UTUC). World J. Urol. 2017, 35, 379–387. [Google Scholar] [CrossRef]
- Colin, P.; Ouzzane, A.; Pignot, G.; Ravier, E.; Crouzet, S.; Ariane, M.M.; Audouin, M.; Neuzillet, Y.; Albouy, B.; Hurel, S.; et al. Comparison of Oncological Outcomes after Segmental Ureterectomy or Radical Nephroureterectomy in Urothelial Carcinomas of the Upper Urinary Tract: Results from a Large French Multicentre Study. BJU Int. 2012, 110, 1134–1141. [Google Scholar] [CrossRef]
- Izquierdo, L.; Montalbo, R.; Ingelmo-Torres, M.; Mallofré, C.; Ramírez-Backhaus, M.; Rubio, J.; Van der Heijden, A.G.; Schaafsma, E.; Lopez-Beltran, A.; Blanca, A.; et al. Prognostic MicroRNAs in Upper Tract Urothelial Carcinoma: Multicenter and International Validation Study. Oncotarget 2017, 8, 51522–51529. [Google Scholar] [CrossRef]
- Mannelli, C. Tissue vs Liquid Biopsies for Cancer Detection: Ethical Issues. J. Bioeth. Inq. 2019, 16, 551–557. [Google Scholar] [CrossRef]
- Fujii, Y.; Sato, Y.; Suzuki, H.; Kakiuchi, N.; Yoshizato, T.; Lenis, A.; Maekawa, S.; Yokoyama, A.; Takeuchi, Y.; Inoue, Y.; et al. Molecular classification and diagnostics of upper urinary tract urothelial carcinoma. Cancer Cell 2021, 39, 793–809. [Google Scholar] [CrossRef]
- Stewart, C.M.; Tsui, D.W.Y. Circulating Cell-Free DNA for Non-Invasive Cancer Management. Cancer Genet. 2018, 228–229, 169–179. [Google Scholar] [CrossRef]
- Alix-Panabières, C.; Pantel, K. Clinical Applications of Circulating Tumor Cells and Circulating Tumor DNA as Liquid Biopsy. Cancer Discov. 2016, 6, 479–491. [Google Scholar] [CrossRef]
- Luo, W.; Rao, M.; Qu, J.; Luo, D. Applications of Liquid Biopsy in Lung Cancer-Diagnosis, Prognosis Prediction, and Disease Monitoring. Am. J. Transl. Res. 2018, 10, 3911. [Google Scholar]
- Nicolazzo, C.; Busetto, G.M.; Gradilone, A.; Sperduti, I.; del Giudice, F.; Loreni, F.; Cortesi, E.; de Berardinis, E.; Gazzaniga, P.; Raimondi, C. Circulating Tumor Cells Identify Patients with Super-High-Risk Non-Muscle-Invasive Bladder Cancer: Updated Outcome Analysis of a Prospective Single-Center Trial. Oncologist 2019, 24, 612–616. [Google Scholar] [CrossRef]
- Bidard, F.C.; Michiels, S.; Riethdorf, S.; Mueller, V.; Esserman, L.J.; Lucci, A.; Naume, B.; Horiguchi, J.; Gisbert-Criado, R.; Sleijfer, S.; et al. Circulating Tumor Cells in Breast Cancer Patients Treated by Neoadjuvant Chemotherapy: A Meta-Analysis. J. Natl. Cancer Inst. 2018, 110, 560–567. [Google Scholar] [CrossRef]
- Fernandez-Garcia, D.; Hills, A.; Page, K.; Hastings, R.K.; Toghill, B.; Goddard, K.S.; Ion, C.; Ogle, O.; Boydell, A.R.; Gleason, K.; et al. Plasma Cell-Free DNA (CfDNA) as a Predictive and Prognostic Marker in Patients with Metastatic Breast Cancer. Breast Cancer Res. 2019, 21, 149. [Google Scholar] [CrossRef]
- Lin, L.H.; Chang, K.W.; Kao, S.Y.; Cheng, H.W.; Liu, C.J. Increased Plasma Circulating Cell-Free DNA Could Be a Potential Marker for Oral Cancer. Int. J. Mol. Sci. 2018, 19, 3303. [Google Scholar] [CrossRef]
- Kienel, A.; Porres, D.; Heidenreich, A.; Pfister, D. CfDNA as a Prognostic Marker of Response to Taxane Based Chemotherapy in Patients with Prostate Cancer. J. Urol. 2015, 194, 966–971. [Google Scholar] [CrossRef]
- Green, E.A.; Li, R.; Albiges, L.; Choueiri, T.K.; Freedman, M.; Pal, S.; Dyrskjøt, L.; Kamat, A.M. Clinical Utility of Cell-Free and Circulating Tumor DNA in Kidney and Bladder Cancer: A Critical Review of Current Literature. Eur. Urol. Oncol. 2021, 4, 893–903. [Google Scholar] [CrossRef]
- Carrasco, R.; Ingelmo-Torres, M.; Gómez, A.; Trullas, R.; Roldán, F.L.; Ajami, T.; Moreno, D.; Rodríguez-Carunchio, L.; Alcaraz, A.; Izquierdo, L.; et al. Cell-Free DNA as a Prognostic Biomarker for Monitoring Muscle-Invasive Bladder Cancer. Int. J. Mol. Sci. 2022, 23, 11732. [Google Scholar] [CrossRef]
- Carrasco, R.; Ingelmo-Torres, M.; Oriola, J.; Roldán, F.L.; Rodríguez-Carunchio, L.; Herranz, S.; Mellado, B.; Alcaraz, A.; Izquierdo, L.; Mengual, L. Assessment of Aggressive Bladder Cancer Mutations in Plasma Cell-Free DNA. Front. Oncol. 2023, 13, 1270962. [Google Scholar] [CrossRef]
- De Rubis, G.; Rajeev Krishnan, S.; Bebawy, M. Liquid Biopsies in Cancer Diagnosis, Monitoring, and Prognosis. Trends Pharmacol. Sci. 2019, 40, 172–186. [Google Scholar] [CrossRef]
- Ignatiadis, M.; Sledge, G.W.; Jeffrey, S.S. Liquid Biopsy Enters the Clinic—Implementation Issues and Future Challenges. Nat. Rev. Clin. Oncol. 2021, 18, 297–312. [Google Scholar] [CrossRef]
- Carrasco, R.; Ingelmo-Torres, M.; Gómez, A.; Roldán, F.L.; Segura, N.; Ribal, M.J.; Alcaraz, A.; Izquierdo, L.; Mengual, L. Prognostic Implication of TERT Promoter Mutation and Circulating Tumor Cells in Muscle-Invasive Bladder Cancer. World J. Urol. 2022, 40, 2033–2039. [Google Scholar] [CrossRef]
- Zhang, Z.; Fan, W.; Deng, Q.; Tang, S.; Wang, P.; Xu, P.; Wang, J.; Yu, M. The Prognostic and Diagnostic Value of Circulating Tumor Cells in Bladder Cancer and Upper Tract Urothelial Carcinoma: A Meta-Analysis of 30 Published Studies. Oncotarget 2017, 8, 59527–59538. [Google Scholar] [CrossRef]
- Nakano, K.; Koh, Y.; Yamamichi, G.; Yumiba, S.; Tomiyama, E.; Matsushita, M.; Hayashi, Y.; Wang, C.; Ishizuya, Y.; Yamamoto, Y.; et al. Perioperative Circulating Tumor DNA Enables the Identification of Patients with Poor Prognosis in Upper Tract Urothelial Carcinoma. Cancer Sci. 2022, 113, 1830–1842. [Google Scholar] [CrossRef]
- Rink, M.; Chun, F.K.; Dahlem, R.; Soave, A.; Minner, S.; Hansen, J.; Stoupiec, M.; Coith, C.; Kluth, L.A.; Ahyai, S.A.; et al. Prognostic Role and HER2 Expression of Circulating Tumor Cells in Peripheral Blood of Patients Prior to Radical Cystectomy: A Prospective Study. Eur. Urol. 2012, 61, 810–817. [Google Scholar] [CrossRef]
- Toledano-Fonseca, M.; Cano, M.T.; Inga, E.; Rodríguez-Alonso, R.; Gómez-España, M.A.; Guil-Luna, S.; Mena-Osuna, R.; de la Haba-Rodríguez, J.R.; Rodríguez-Ariza, A.; Aranda, E. Circulating Cell-Free DNA-Based Liquid Biopsy Markers for the Non-Invasive Prognosis and Monitoring of Metastatic Pancreatic Cancer. Cancers 2020, 12, 1754. [Google Scholar] [CrossRef]
- Barthel, F.P.; Wei, W.; Tang, M.; Martinez-Ledesma, E.; Hu, X.; Amin, S.B.; Akdemir, K.C.; Seth, S.; Song, X.; Wang, Q.; et al. Systematic Analysis of Telomere Length and Somatic Alterations in 31 Cancer Types. Nat. Genet. 2017, 49, 349–357. [Google Scholar] [CrossRef]
- Huang, D.-S.; Wang, Z.; He, X.-J.; Diplas, B.H.; Yang, R.; Killela, P.J.; Meng, Q.; Ye, Z.-Y.; Wang, W.; Jiang, X.-T.; et al. Recurrent TERT Promoter Mutations Identified in a Large-Scale Study of Multiple Tumour Types Are Associated with Increased TERT Expression and Telomerase Activation. Eur. J. Cancer 2015, 51, 969–976. [Google Scholar] [CrossRef]
- Kinde, I.; Munari, E.; Faraj, S.F.; Hruban, R.H.; Schoenberg, M.; Bivalacqua, T.; Allaf, M.; Springer, S.; Wang, Y.; Diaz, L.A.; et al. TERT Promoter Mutations Occur Early in Urothelial Neoplasia and Are Biomarkers of Early Disease and Disease Recurrence in Urine. Cancer Res. 2013, 73, 7162–7167. [Google Scholar] [CrossRef]
- Wu, S.; Huang, P.; Li, C.; Huang, Y.; Li, X.; Wang, Y.; Chen, C.; Lv, Z.; Tang, A.; Sun, X.; et al. Telomerase Reverse Transcriptase Gene Promoter Mutations Help Discern the Origin of Urogenital Tumors: A Genomic and Molecular Study. Eur. Urol. 2014, 65, 274–277. [Google Scholar] [CrossRef]
- Borah, S.; Xi, L.; Zaug, A.J.; Powell, N.M.; Dancik, G.M.; Cohen, S.B.; Costello, J.C.; Theodorescu, D.; Cech, T.R. Cancer. TERT Promoter Mutations and Telomerase Reactivation in Urothelial Cancer. Science 2015, 347, 1006–1010. [Google Scholar] [CrossRef]
- Descotes, F.; Kara, N.; Decaussin-Petrucci, M.; Piaton, E.; Geiguer, F.; Rodriguez-Lafrasse, C.; Terrier, J.E.; Lopez, J.; Ruffion, A. Non-Invasive Prediction of Recurrence in Bladder Cancer by Detecting Somatic TERT Promoter Mutations in Urine. Br. J. Cancer 2017, 117, 583–587. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Total UTUC (N = 20) | Progressive UTUC (N = 7) | Non-Progressive UTUC (N = 13) | |
|---|---|---|---|
| Gender, n (%) | |||
| Male | 12 (60) | 4 (57) | 8 (62) |
| Female | 8 (40) | 3 (43) | 5 (38) |
| Tumor location, n (%) | |||
| Pelvis | 9 (45) | 3 (43) | 6 (46) |
| Ureter | 7 (35) | 1 (14) | 6 (46) |
| Both | 4 (20) | 3 (43) | 1 (8) |
| Pathological Stage, n (%) | |||
| pTa | 3 (15) | - | 3 (23) |
| pT1 | 7 (35) | 3 (43) | 4 (31) |
| pT2 | 4 (20) | - | 4 (31) |
| pT3 | 6 (30) | 4 (57) | 2 (15) |
| pT4 | - | - | - |
| Histological Grade, n (%) | |||
| Low | 6 (30) | 0 (0) | 6 (46) |
| High | 14 (70) | 7 (100) | 7 (54) |
| Metastasis, n (%) | |||
| Local | 2 (10) | 2 (29) | - |
| Distant | 1 (5) | 1 (14) | - |
| Local + distant | 4 (20) | 4 (57) | - |
| Nodes, n (%) | 4 (57) | 4 (57) | - |
| Chemotherapy, n (%) | |||
| Adjuvant | 2 (10) | 2 (29) | - |
| Neoadjuvant | 1 (5) | 1 (14) | - |
| Pre-Treatment VAF | Post-Treatment VAF | p-Value | |
|---|---|---|---|
| Progressive UTUC | |||
| TERT c.-124C>T | 81% | 18% | 0.19 |
| TERT c.-146C>T | 8% | 3% | 0.24 |
| ATM c.1236-2A>T | 1% | 0% | 0.31 |
| TP53 c.853G>A | 6% | 40% | 0.11 |
| Nonprogressive UTUC | |||
| TERT c.-124C>T | 1% | 7% | 0.21 |
| TERT c.-146C>T | 19% | 10% | 0.79 |
| ATM c.1236-2A>T | 6% | 7% | 0.60 |
| TP53 c.853G>A | 82% | 86% | 0.12 |
| Pre-Treatment VAF | Post-Treatment VAF | p-Value | |
|---|---|---|---|
| Cancer-specific death | |||
| TERT c.-124C>T | 159% | 34% | 0.09 |
| TERT c.-146C>T | 8% | 0% | 0.23 |
| ATM c.1236-2A>T | 1% | 1% | 0.55 |
| TP53 c.853G>A | 83% | 8% | 0.11 |
| Remaining patients | |||
| TERT c.-124C>T | 12% | 7% | 0.15 |
| TERT c.-146C>T | 16% | 9% | 0.33 |
| ATM c.1236-2A>T | 5% | 5% | 0.41 |
| TP53 c.853G>A | 73% | 81% | 0.20 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Padullés, B.; Carrasco, R.; Ingelmo-Torres, M.; Roldán, F.L.; Gómez, A.; Vélez, E.; Alfambra, H.; Figueras, M.; Carrion, A.; Gil-Vernet, J.; et al. Prognostic Value of Liquid-Biopsy-Based Biomarkers in Upper Tract Urothelial Carcinoma. Int. J. Mol. Sci. 2024, 25, 3695. https://doi.org/10.3390/ijms25073695
Padullés B, Carrasco R, Ingelmo-Torres M, Roldán FL, Gómez A, Vélez E, Alfambra H, Figueras M, Carrion A, Gil-Vernet J, et al. Prognostic Value of Liquid-Biopsy-Based Biomarkers in Upper Tract Urothelial Carcinoma. International Journal of Molecular Sciences. 2024; 25(7):3695. https://doi.org/10.3390/ijms25073695
Chicago/Turabian StylePadullés, Bernat, Raquel Carrasco, Mercedes Ingelmo-Torres, Fiorella L. Roldán, Ascensión Gómez, Elena Vélez, Héctor Alfambra, Marcel Figueras, Albert Carrion, Jordi Gil-Vernet, and et al. 2024. "Prognostic Value of Liquid-Biopsy-Based Biomarkers in Upper Tract Urothelial Carcinoma" International Journal of Molecular Sciences 25, no. 7: 3695. https://doi.org/10.3390/ijms25073695
APA StylePadullés, B., Carrasco, R., Ingelmo-Torres, M., Roldán, F. L., Gómez, A., Vélez, E., Alfambra, H., Figueras, M., Carrion, A., Gil-Vernet, J., Mengual, L., Izquierdo, L., & Alcaraz, A. (2024). Prognostic Value of Liquid-Biopsy-Based Biomarkers in Upper Tract Urothelial Carcinoma. International Journal of Molecular Sciences, 25(7), 3695. https://doi.org/10.3390/ijms25073695