

The IGF–PAPP-A–Stanniocalcin Axis in Serum and Ascites Associates with Prognosis in Patients with Ovarian Cancer

 ,
,  and
and
Abstract
1. Introduction
2. Results
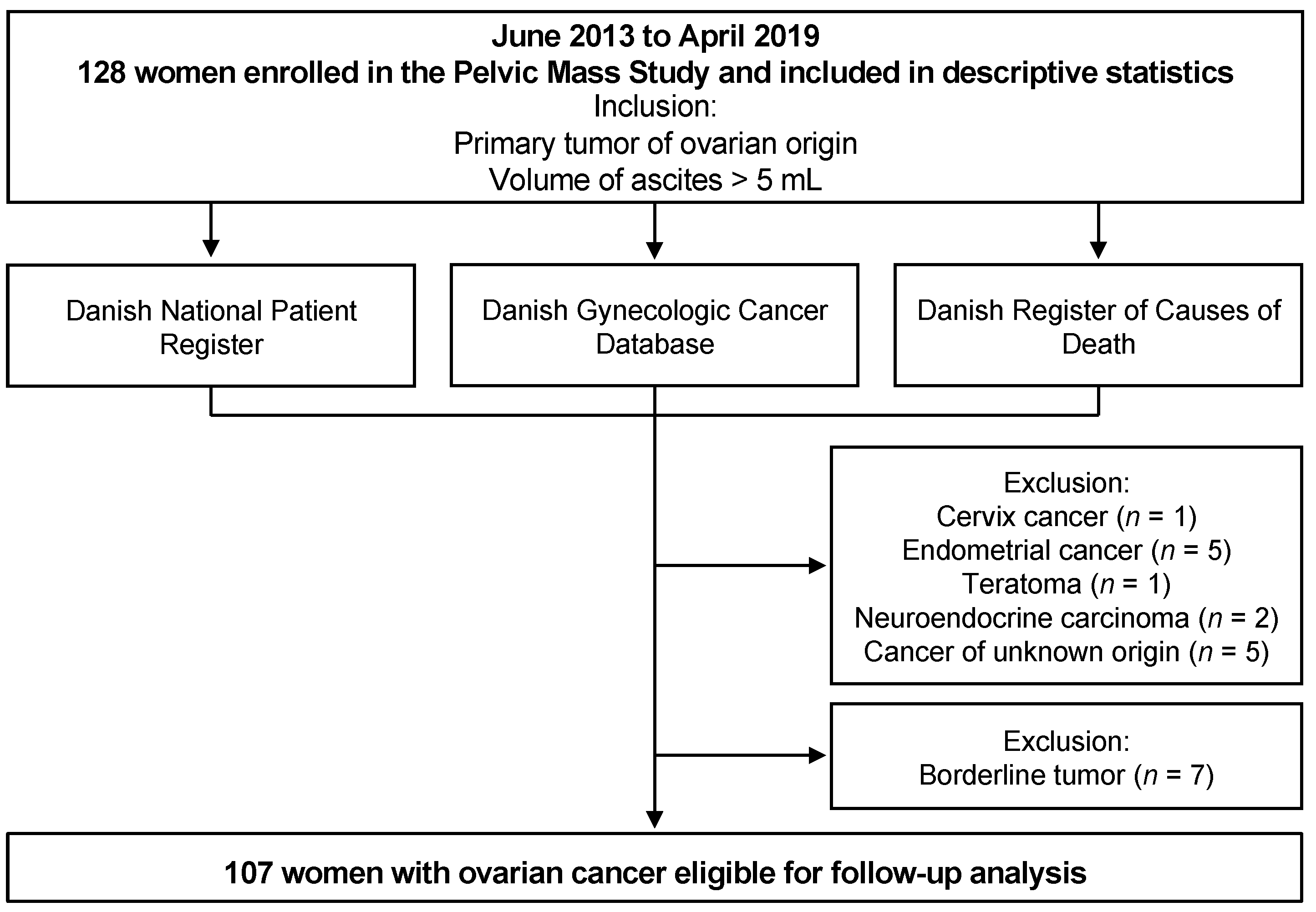
2.1. Study Cohort and Characteristics
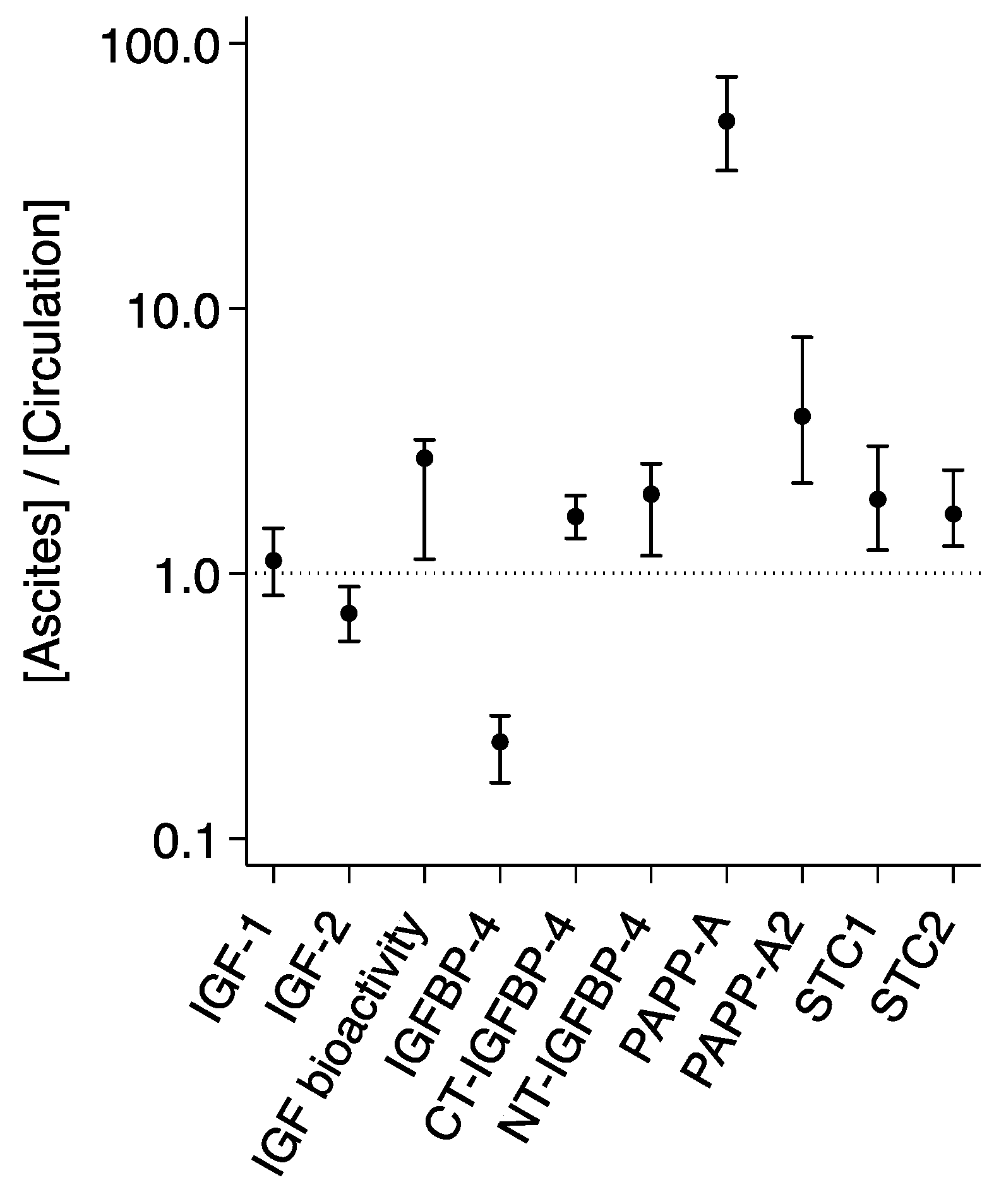
2.2. IGF Levels in the Circulation and Ascites from Patients with Ovarian Cancer
2.3. Relations between IGF Protein Levels
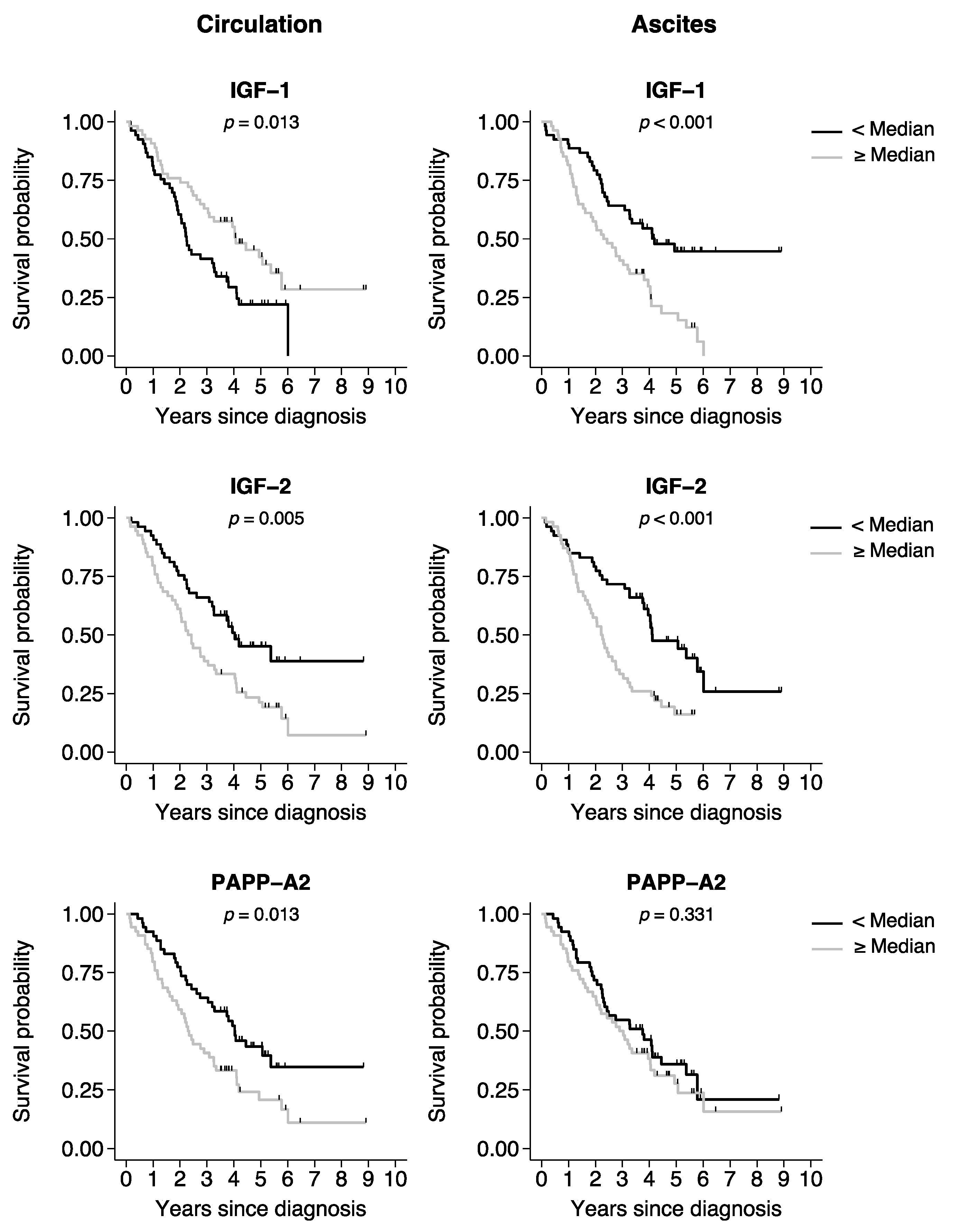
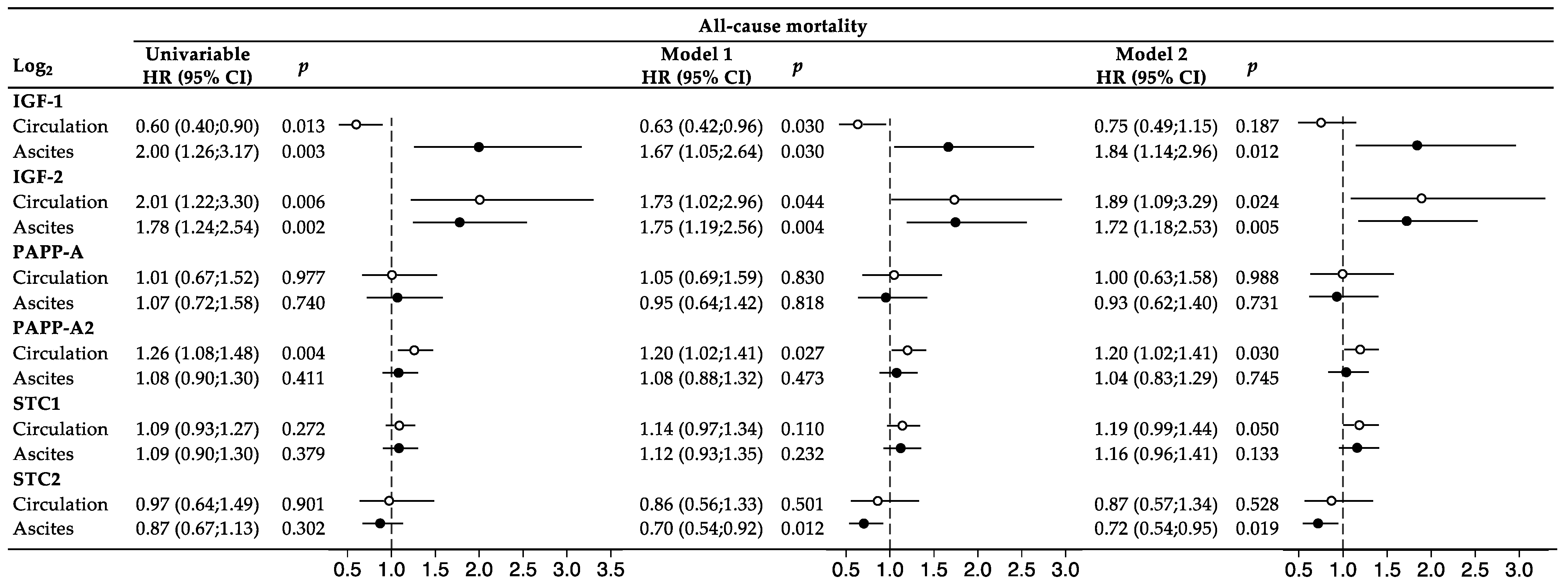
2.4. Survival Analyses of Ovarian Cancer Patients
3. Discussion
4. Materials and Methods
4.1. Study Cohort
4.2. Patient Follow-Up
4.3. Laboratory Measurements
4.4. Statistics
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Penet, M.-F.; Krishnamachary, B.; Wildes, F.B.; Mironchik, Y.; Hung, C.-F.; Wu, T.; Bhujwalla, Z.M. Ascites Volumes and the Ovarian Cancer Microenvironment. Front. Oncol. 2018, 8, 595. [Google Scholar] [CrossRef]
- Kipps, E.; Tan, D.S.; Kaye, S.B. Meeting the challenge of ascites in ovarian cancer: New avenues for therapy and research. Nat. Rev. Cancer 2013, 13, 273–282. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.-F.; Huang, H.-S.; Chen, P.-C.; Ding, D.-C.; Chu, T.-Y. IGF-axis confers transformation and regeneration of fallopian tube fimbria epithelium upon ovulation. EBioMedicine 2019, 41, 597–609. [Google Scholar] [CrossRef] [PubMed]
- Thomsen, J.; Hjortebjerg, R.; Espelund, U.; Ortoft, G.; Vestergaard, P.; Magnusson, N.E.; Conover, C.A.; Tramm, T.; Hager, H.; Hogdall, C.; et al. PAPP-A proteolytic activity enhances IGF bioactivity in ascites from women with ovarian carcinoma. Oncotarget 2015, 6, 32266–32278. [Google Scholar] [CrossRef] [PubMed]
- Baxter, R.C. IGF binding proteins in cancer: Mechanistic and clinical insights. Nat. Rev. Cancer 2014, 14, 329. [Google Scholar] [CrossRef] [PubMed]
- Livingstone, C. IGF2 and cancer. Endocr. Relat. Cancer 2013, 20, R321–R339. [Google Scholar] [CrossRef]
- Conover, C.A.; Hartmann, L.C.; Bradley, S.; Stalboerger, P.; Klee, G.G.; Kalli, K.R.; Jenkins, R.B. Biological Characterization of Human Epithelial Ovarian Carcinoma Cells in Primary Culture: The Insulin-like Growth Factor System. Exp. Cell Res. 1998, 238, 439–449. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Li, J.; Han, F.; Chen, H.; Zhao, X.; Qin, Q.; Shi, R.; Liu, J. High IGF2 expression is associated with poor clinical outcome in human ovarian cancer. Oncol. Rep. 2015, 34, 936–942. [Google Scholar] [CrossRef]
- Buck, E.; Gokhale, P.C.; Koujak, S.; Brown, E.; Eyzaguirre, A.; Tao, N.; Rosenfeld-Franklin, M.; Lerner, L.; Chiu, M.I.; Wild, R.; et al. Compensatory insulin receptor (IR) activation on inhibition of insulin-like growth factor-1 receptor (IGF-1R): Rationale for cotargeting IGF-1R and IR in cancer. Mol. Cancer Ther. 2010, 9, 2652–2664. [Google Scholar] [CrossRef]
- Vella, V.; Milluzzo, A.; Scalisi, N.M.; Vigneri, P.; Sciacca, L. Insulin Receptor Isoforms in Cancer. Int. J. Mol. Sci. 2018, 19, 3615. [Google Scholar] [CrossRef]
- Conover, C.A. Role of PAPP-A in aging and age-related disease. Exp. Gerontol. 2013, 48, 612–613. [Google Scholar] [CrossRef]
- Hoeflich, A.; David, R.; Hjortebjerg, R. Current IGFBP-related biomarker research in cardiovascular disease—We need more structural and functional information in clinical studies. Front. Endocrinol. 2018, 9, 388. [Google Scholar] [CrossRef]
- Hjortebjerg, R.; Espelund, U.; Rasmussen, T.R.; Folkersen, B.; Steiniche, T.; Georgsen, J.B.; Oxvig, C.; Frystyk, J. Pregnancy-Associated Plasma Protein-A2 Is Associated with Mortality in Patients with Lung Cancer. Front. Endocrinol. 2020, 11, 614. [Google Scholar] [CrossRef]
- Becker, M.A.; Haluska, P.; Bale, L.K.; Oxvig, C.; Conover, C.A. A Novel Neutralizing Antibody Targeting Pregnancy-Associated Plasma Protein-A Inhibits Ovarian Cancer Growth and Ascites Accumulation in Patient Mouse Tumorgrafts. Mol. Cancer Ther. 2015, 14, 973–981. [Google Scholar] [CrossRef]
- Takabatake, Y.; Oxvig, C.; Nagi, C.; Adelson, K.; Jaffer, S.; Schmidt, H.; Keely, P.J.; Eliceiri, K.W.; Mandeli, J.; Germain, D. Lactation opposes pappalysin-1-driven pregnancy-associated breast cancer. EMBO Mol. Med. 2016, 8, 388–406. [Google Scholar] [CrossRef] [PubMed]
- Conover, C.A.; Oxvig, C. PAPP-A and cancer. J. Mol. Endocrinol. 2018, 61, T1–T10. [Google Scholar] [CrossRef] [PubMed]
- Hjortebjerg, R. IGFBP-4 and PAPP-A in normal physiology and disease. Growth Horm. IGF Res. 2018, 41, 7–22. [Google Scholar] [CrossRef] [PubMed]
- Frystyk, J.; Teran, E.; Gude, M.F.; Bjerre, M.; Hjortebjerg, R. Pregnancy-associated plasma proteins and Stanniocalcin-2—Novel players controlling IGF-I physiology. Growth Horm. IGF Res. 2020, 53–54, 101330. [Google Scholar] [CrossRef] [PubMed]
- Clemmons, D.R. Insulin-like growth factor binding proteins and their role in controlling IGF actions. Cytokine Growth Factor Rev. 1997, 8, 45–62. [Google Scholar] [CrossRef] [PubMed]
- Espelund, U.; Renehan, A.G.; Cold, S.; Oxvig, C.; Lancashire, L.; Su, Z.; Flyvbjerg, A.; Frystyk, J. Prognostic relevance and performance characteristics of serum IGFBP-2 and PAPP-A in women with breast cancer: A long-term Danish cohort study. Cancer Med. 2018, 7, 2391–2404. [Google Scholar] [CrossRef] [PubMed]
- Jepsen, M.R.; Kløverpris, S.; Mikkelsen, J.H.; Pedersen, J.H.; Füchtbauer, E.-M.; Laursen, L.S.; Oxvig, C. Stanniocalcin-2 Inhibits Mammalian Growth by Proteolytic Inhibition of the Insulin-like Growth Factor Axis. J. Biol. Chem. 2015, 290, 3430–3439. [Google Scholar] [CrossRef]
- Kløverpris, S.; Mikkelsen, J.H.; Pedersen, J.H.; Jepsen, M.R.; Laursen, L.S.; Petersen, S.V.; Oxvig, C. Stanniocalcin-1 Potently Inhibits the Proteolytic Activity of the Metalloproteinase Pregnancy-associated Plasma Protein-A. J. Biol. Chem. 2015, 290, 21915–21924. [Google Scholar] [CrossRef]
- Chang, A.C.; Jellinek, D.A.; Reddel, R.R. Mammalian stanniocalcins and cancer. Endocr. Relat. Cancer 2003, 10, 359–373. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Huang, Q.; Li, D.; Lv, L.; Li, Y.; Wu, Z. The significance of Stanniocalcin 2 in malignancies and mechanisms. Bioengineered 2021, 12, 7276–7285. [Google Scholar] [CrossRef] [PubMed]
- Liu, G.; Yang, G.; Chang, B.; Mercado-Uribe, I.; Huang, M.; Zheng, J.; Bast, R.C.; Lin, S.H.; Liu, J. Stanniocalcin 1 and ovarian tumorigenesis. J. Natl. Cancer Inst. 2010, 102, 812–827. [Google Scholar] [CrossRef] [PubMed]
- Hjortebjerg, R.; Lindberg, S.; Pedersen, S.; Mogelvang, R.; Jensen, J.S.; Oxvig, C.; Frystyk, J.; Bjerre, M. Insulin-Like Growth Factor Binding Protein 4 Fragments Provide Incremental Prognostic Information on Cardiovascular Events in Patients With ST-Segment Elevation Myocardial Infarction. J. Am. Heart Assoc. 2017, 6, e005358. [Google Scholar] [CrossRef] [PubMed]
- Hjortebjerg, R.; Rasmussen, L.M.; Gude, M.F.; Irmukhamedov, A.; Riber, L.P.; Frystyk, J.; De Mey, J.G.R. Local IGF Bioactivity Associates with High PAPP-A Activity in the Pericardial Cavity of Cardiovascular Disease Patients. J. Clin. Endocrinol. Metab. 2020, 105, e4083–e4093. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.W.; Ledet, T.; Ørskov, H.; Jessen, N.; Lund, S.; Whittaker, J.; De Meyts, P.; Larsen, M.B.; Christiansen, J.S.; Frystyk, J. A highly sensitive and specific assay for determination of IGF-I bioactivity in human serum. Am. J. Physiol. Endocrinol. Metab. 2003, 284, E1149–E1155. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, N.; Stenvers, K.L. Getting to know ovarian cancer ascites: Opportunities for targeted therapy-based translational research. Front. Oncol. 2013, 3, 256. [Google Scholar] [CrossRef]
- Rickard, B.P.; Conrad, C.; Sorrin, A.J.; Ruhi, M.K.; Reader, J.C.; Huang, S.A.; Franco, W.; Scarcelli, G.; Polacheck, W.J.; Roque, D.M.; et al. Malignant Ascites in Ovarian Cancer: Cellular, Acellular, and Biophysical Determinants of Molecular Characteristics and Therapy Response. Cancers 2021, 13, 4318. [Google Scholar] [CrossRef]
- Conover, C.A.; Bale, L.K.; Mader, J.R.; Mason, M.A.; Keenan, K.P.; Marler, R.J. Longevity and Age-Related Pathology of Mice Deficient in Pregnancy-Associated Plasma Protein-A. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2010, 65A, 590–599. [Google Scholar] [CrossRef]
- Conover, C.A.; Bale, L.K. Loss of pregnancy-associated plasma protein A extends lifespan in mice. Aging Cell 2007, 6, 727–729. [Google Scholar] [CrossRef]
- Bulut, I.; Gulcan, E.; Coskun, A.; Ciftci, A.; Cetinkaya, E.; Altiay, G.; Caglar, T. Relationship Between Pregnancy-Associated Plasma Protein-A and Lung Cancer. Am. J. Med. Sci. 2009, 337, 241–244. [Google Scholar] [CrossRef] [PubMed]
- Kalli, K.R.; Chen, B.K.; Bale, L.K.; Gernand, E.; Overgaard, M.T.; Oxvig, C.; Cliby, W.A.; Conover, C.A. Pregnancy-associated plasma protein-A (PAPP-A) expression and insulin-like growth factor binding protein-4 protease activity in normal and malignant ovarian surface epithelial cells. Int. J. Cancer 2004, 110, 633–640. [Google Scholar] [CrossRef] [PubMed]
- Barrios, V.; Chowen, J.A.; Martín-Rivada, Á.; Guerra-Cantera, S.; Pozo, J.; Yakar, S.; Rosenfeld, R.G.; Pérez-Jurado, L.A.; Suárez, J.; Argente, J. Pregnancy-Associated Plasma Protein (PAPP)-A2 in Physiology and Disease. Cells 2021, 10, 3576. [Google Scholar] [CrossRef] [PubMed]
- Tamsma, J.T.; Keizer, H.J.; Meinders, A.E. Pathogenesis of malignant ascites: Starling’s law of capillary hemodynamics revisited. Ann. Oncol. 2001, 12, 1353–1357. [Google Scholar] [CrossRef] [PubMed]
- Jüngst, D.; Xie, Y.; Gerbes, A.L. Pathophysiology of elevated ascites fluid cholesterol in malignant ascites: Increased ascites to serum relation of proteins and lipoproteins in patients with peritoneal carcinomatosis as compared to patients with cirrhosis of the liver. J. Hepatol. 1992, 14, 244–248. [Google Scholar] [CrossRef] [PubMed]
- Oxvig, C.; Sand, O.; Kristensen, T.; Gleich, G.J.; Sottrup-Jensen, L. Circulating human pregnancy-associated plasma protein-A is disulfide-bridged to the proform of eosinophil major basic protein. J. Biol. Chem. 1993, 268, 12243–12246. [Google Scholar] [CrossRef] [PubMed]
- Overgaard, M.T.; Boldt, H.B.; Laursen, L.S.; Sottrup-Jensen, L.; Conover, C.A.; Oxvig, C. Pregnancy-associated plasma protein-A2 (PAPP-A2), a novel insulin-like growth factor-binding protein-5 proteinase. J. Biol. Chem. 2001, 276, 21849–21853. [Google Scholar] [CrossRef] [PubMed]
- Liefers-Visser, J.A.L.; Meijering, R.A.M.; Reyners, A.K.L.; van der Zee, A.G.J.; de Jong, S. IGF system targeted therapy: Therapeutic opportunities for ovarian cancer. Cancer Treat. Rev. 2017, 60, 90–99. [Google Scholar] [CrossRef]
- Kalli, K.R.; Falowo, O.I.; Bale, L.K.; Zschunke, M.A.; Roche, P.C.; Conover, C.A. Functional Insulin Receptors on Human Epithelial Ovarian Carcinoma Cells: Implications for IGF-II Mitogenic Signaling. Endocrinology 2002, 143, 3259–3267. [Google Scholar] [CrossRef]
- Ouban, A.; Muraca, P.; Yeatman, T.; Coppola, D. Expression and distribution of insulin-like growth factor-1 receptor in human carcinomas. Hum. Pathol. 2003, 34, 803–808. [Google Scholar] [CrossRef]
- Frasca, F.; Pandini, G.; Scalia, P.; Sciacca, L.; Mineo, R.; Costantino, A.; Goldfine, I.D.; Belfiore, A.; Vigneri, R. Insulin Receptor Isoform A, a Newly Recognized, High-Affinity Insulin-Like Growth Factor II Receptor in Fetal and Cancer Cells. Mol. Cell. Biol. 1999, 19, 3278–3288. [Google Scholar] [CrossRef] [PubMed]
- Belfiore, A.; Malaguarnera, R.; Vella, V.; Lawrence, M.C.; Sciacca, L.; Frasca, F.; Morrione, A.; Vigneri, R. Insulin Receptor Isoforms in Physiology and Disease: An Updated View. Endocr. Rev. 2017, 38, 379–431. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.-F.; Cheng, W.-F.; Wu, Y.-P.; Cheng, Y.-M.; Hsu, K.-F.; Chou, C.-Y. Circulating IGF system and treatment outcome in epithelial ovarian cancer. Endocr. Relat. Cancer 2014, 21, 217–229. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Li, Y.; Zhang, J.; Zheng, C.; Zhu, H.; Yu, H.; Fan, L. Circulating Insulin-Like Growth Factor-1 Level and Ovarian Cancer Risk. Cell. Physiol. Biochem. 2016, 38, 589–597. [Google Scholar] [CrossRef] [PubMed]
- Flyvbjerg, A.; Mogensen, O.; Mogensen, B.; Nielsen, O.S. Elevated serum insulin-like growth factor-binding protein 2 (IGFBP-2) and decreased IGFBP-3 in epithelial ovarian cancer: Correlation with cancer antigen 125 and tumor-associated trypsin inhibitor. J. Clin. Endocrinol. Metab. 1997, 82, 2308–2313. [Google Scholar] [CrossRef] [PubMed]
- Lukanova, A.; Lundin, E.; Toniolo, P.; Micheli, A.; Akhmedkhanov, A.; Rinaldi, S.; Muti, P.; Lenner, P.; Biessy, C.; Krogh, V.; et al. Circulating levels of insulin-like growth factor-I and risk of ovarian cancer. Int. J. Cancer 2002, 101, 549–554. [Google Scholar] [CrossRef] [PubMed]
- Baron-Hay, S.; Boyle, F.; Ferrier, A.; Scott, C. Elevated serum insulin-like growth factor binding protein-2 as a prognostic marker in patients with ovarian cancer. Clin. Cancer Res. 2004, 10, 1796–1806. [Google Scholar] [CrossRef]
- Knuppel, A.; Fensom, G.K.; Watts, E.L.; Gunter, M.J.; Murphy, N.; Papier, K.; Perez-Cornago, A.; Schmidt, J.A.; Smith Byrne, K.; Travis, R.C.; et al. Circulating Insulin-like Growth Factor-I Concentrations and Risk of 30 Cancers: Prospective Analyses in UK Biobank. Cancer Res. 2020, 80, 4014–4021. [Google Scholar] [CrossRef]
- Ohlsson, C.; Mohan, S.; Sjögren, K.; Tivesten, A.; Isgaard, J.; Isaksson, O.; Jansson, J.O.; Svensson, J. The role of liver-derived insulin-like growth factor-I. Endocr. Rev. 2009, 30, 494–535. [Google Scholar] [CrossRef]
- Rahmani, J.; Montesanto, A.; Giovannucci, E.; Zand, H.; Barati, M.; Kopchick, J.J.; Mirisola, M.G.; Lagani, V.; Bawadi, H.; Vardavas, R.; et al. Association between IGF-1 levels ranges and all-cause mortality: A meta-analysis. Aging Cell 2022, 21, e13540. [Google Scholar] [CrossRef] [PubMed]
- Werner, H.; Laron, Z. Insulin-like growth factors and aging: Lessons from Laron syndrome. Front. Endocrinol. 2023, 14, 1291812. [Google Scholar] [CrossRef]
- Charkhchi, P.; Cybulski, C.; Gronwald, J.; Wong, F.O.; Narod, S.A.; Akbari, M.R. CA125 and Ovarian Cancer: A Comprehensive Review. Cancers 2020, 12, 3730. [Google Scholar] [CrossRef] [PubMed]
- Hennessy, B.T.; Coleman, R.L.; Markman, M. Ovarian cancer. Lancet 2009, 374, 1371–1382. [Google Scholar] [CrossRef]
- Hjortebjerg, R.; Thomsen, K.L.; Agnholt, J.; Frystyk, J. The IGF system in patients with inflammatory bowel disease treated with prednisolone or infliximab: Potential role of the stanniocalcin-2/PAPP-A/IGFBP-4 axis. BMC Gastroenterol. 2019, 19, 83. [Google Scholar] [CrossRef] [PubMed]
- Ekmann-Gade, A.W.; Høgdall, C.K.; Seibæk, L.; Noer, M.C.; Fagö-Olsen, C.L.; Schnack, T.H. Incidence, treatment, and survival trends in older versus younger women with epithelial ovarian cancer from 2005 to 2018: A nationwide Danish study. Gynecol. Oncol. 2022, 164, 120–128. [Google Scholar] [CrossRef] [PubMed]
- West, H.; Jin, J.O. Performance Status in Patients with Cancer. JAMA Oncol. 2015, 1, 998. [Google Scholar] [CrossRef]
- Therneau, T.M.; Grambsch, P.M.; Fleming, T.R. Martingale-based residuals for survival models. Biometrika 1990, 77, 216–218. [Google Scholar] [CrossRef]
- Schoenfeld, D. Partial Residuals for The Proportional Hazards Regression Model. Biometrika 1982, 69, 239–241. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Ovarian Cancer | Other Cancer | Borderline Ovarian Tumor | p |
|---|---|---|---|---|
| Number, n | 107 | 14 | 7 | |
| Age, years | 67.2 (56.8–74.0) | 62.6(55.0–70.1) | 55.2 (43.4–58.1) * | 0.019 |
| BMI, kg/m2 | 23.8 (21.1–27.5) | 25.5 (22.4–29.8) | 35.9 (26.6–43.9) * | 0.017 |
| Treatment, n (%) | ||||
| Primary surgery | 49 (58.8) | |||
| Interval surgery | 41 (38.3) | |||
| Chemotherapy | 17 (15.9) | |||
| Postmenopausal, n (%) | ||||
| Yes | 92 (86.0) | 10 (71.4) | 4 (57.1) | 0.050 |
| No | 15 (14.0) | 4 (28.6) | 3 (42.9) | |
| Smoker, n (%) | ||||
| Never | 49 (45.8) | 6 (50.0) | 4 (57.1) | 0.408 |
| Former | 41 (38.3) | 5 (41.7) | 2 (28.6) | |
| Current | 16 (15.0) | 1 (8.3) | 0 (0.0) | |
| Unknown/missing | 1 (0.9) | 0 (0.0) | 1 (14.3) | |
| Clinical stage, n (%) | ||||
| I | 7 (6.5) | 1 (9.1) * | 5 (71.4) * | 0.000 |
| II | 4 (3.7) | 1 (9.1) | 0 (0.0) | |
| III | 64 (59.8) | 4 (36.4) | 1 (14.3) | |
| IV | 32 (29.9) | 2 (18.2) | 0 (0.0) | |
| Unknown/missing | 0 (0.0) | 3 (27.3) | 1 (14.3) | |
| CCI, n (%) | ||||
| 0 | 89 (83.2) | 13 (92.9) | 5 (71.4) | 0.327 |
| 1 | 12 (11.2) | 0 (0.0) | 1 (14.3) | |
| 2 | 3 (2.8) | 1 (7.1) | 1 (14.3) | |
| 3 | 3 (2.8) | 0 (0.0) | 0 (0.0) | |
| Performance score, n (%) | ||||
| 0 | 50 (46.7) | 9 (75) | 3 (42.9) | 0.483 |
| 1 | 34 (31.8) | 2 (16.7) | 4 (57.1) | |
| 2 | 19 (17.8) | 1 (8.3) | 0 (0.0) | |
| 3 | 4 (3.7) | 0 (0.0) | 0 (0.0) | |
| CA125, U/mL | 850 (352–1870) | 425 (112–820) * | 259 (122–560) * | 0.007 |
| RMI score | 5463 (2196–12,150) | 2460 (441–3860) * | 840 (366–5040) * | 0.004 |
| Follow-up, months | 38.4 (18.6–51.3) | 39.7 (14.3–57.2) | 67.6 (59.5–70.5) * | 0.001 |
| Mortality at endpoint, n (%) | 73 (68.2) | 7 (50.0) * | 0 (0.0) * | 0.000 |
| Protein (ng/mL) | Circulation | Ascites | Ratio (Ascites/Circulation) | p |
|---|---|---|---|---|
| IGF-1 | 81 (62–101) | 92 (71–120) | 1.12 (0.83–1.48) | <0.01 |
| IGF-2 | 422 (335–566) | 313 (220–468) | 0.71 (0.56–0.89) | <0.001 |
| IGF bioactivity | 1.12 (0.89–1.33) | 2.62 (1.31–3.32) | 2.72 (1.13–3.20) | <0.001 |
| IGFBP-4 | 206 (187–237) | 48 (27–58) | 0.23 (0.16–0.29) | <0.001 |
| CT-IGFBP-4 | 69 (61–87) | 131 (77–157) | 1.64 (1.36–1.97) | <0.001 |
| NT-IGFBP-4 | 148 (103–180) | 298 (209–346) | 1.99 (1.17–2.60) | <0.001 |
| PAPP-A | 0.89 (0.75–1.12) | 45 (34–62) | 51 (33–75) | <0.001 |
| PAPP-A2 | 0.44 (0.22–1.05) | 1.77 (1.24–2.62) | 3.93 (2.19–7.78) | <0.001 |
| STC1 | 1.08 (0.63–1.94) | 2.12 (1.23–3.92) | 1.90 (1.23–3.02) | <0.001 |
| STC2 | 37 (28–48) | 68 (40–89) | 1.68 (1.27–2.45) | <0.001 |
| IGF-1 | IGF-2 | IGF Bioactivity | IGFBP-4 | CT-IGFBP-4 | NT-IGFBP-4 | PAPP-A | PAPP-A2 | STC1 | STC2 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| IGF-1 | r | 0.297 | 0.558 | −0.493 | −0.544 | −0.376 | 0.210 | ||||
| p | 0.002 | 0.000 | 0.027 | 0.001 | 0.000 | 0.021 | |||||
| IGF-2 | r | 0.627 | 0.248 | ||||||||
| p | 0.000 | 0.006 | |||||||||
| IGF bioactivity | r | 0.437 | 0.554 | ||||||||
| p | 0.008 | 0.001 | |||||||||
| IGFBP-4 | r | ||||||||||
| p | |||||||||||
| CT-IGFBP-4 | r | 0.319 | 0.500 | 0.485 | 0.686 | 0.745 | |||||
| p | 0.048 | 0.041 | 0.048 | 0.001 | 0.001 | ||||||
| NT-IGFBP-4 | r | 0.330 | 0.506 | 0.606 | 0.668 | ||||||
| p | 0.045 | 0.040 | 0.010 | 0.001 | |||||||
| PAPP-A | r | 0.180 | 0.223 | 0.289 | 0.310 | ||||||
| p | 0.048 | 0.013 | 0.003 | 0.001 | |||||||
| PAPP-A2 | r | 0.526 | |||||||||
| p | 0.000 | ||||||||||
| STC1 | r | 0.317 | 0.259 | −0.471 | 0.485 | 0.588 | |||||
| p | 0.001 | 0.005 | 0.045 | 0.048 | 0.000 | ||||||
| STC2 | r | −0.528 | 0.535 | 0.291 | 0.490 | ||||||
| p | 0.029 | 0.001 | 0.002 | 0.000 |
| Log-Rank Test | Low Protein Level (n = 53) | High Protein Level (n = 54) | p | ||
|---|---|---|---|---|---|
| Range (ng/mL) | Mortality, n (%) | Range (ng/mL) | Mortality, n (%) | ||
| IGF-1 | |||||
| Circulation | 62 [34–80] | 41 (77.4) | 101 [81–202] | 32 (59.3) | 0.013 |
| Ascites | 71 [31–90] | 28 (52.8) | 120 [92–211] | 45 (83.3) | <0.001 |
| IGF-2 | |||||
| Circulation | 335 [150–421] | 28 (52.8) | 565 [422–999] | 45 (83.3) | 0.005 |
| Ascites | 220 [111–312] | 29 (54.7) | 467 [313–890] | 44 (81.5) | <0.001 |
| PAPP-A | |||||
| Circulation | 0.75 [0.16–0.89] | 37 (69.8) | 1.12 [0.89–2.1] | 36 (66.7) | 0.986 |
| Ascites | 34 [12–44] | 40 (75.5) | 60 [45–101] | 33 (61.1) | 0.989 |
| PAPP-A2 | |||||
| Circulation | 0.22 [0.04–0.43] | 31 (58.5) | 1.04 [0.44–4.91] | 42 (77.8) | 0.013 |
| Ascites | 1.24 [0.18–1.70] | 34 (64.2) | 2.61 [1.77–84.4] | 39 (72.2) | 0.331 |
| STC1 | |||||
| Circulation | 0.63 [0.04–1.01] | 36 (67.9) | 1.91 [1.08–17.2] | 37 (68.5) | 0.215 |
| Ascites | 1.23 [0.08–2.09] | 34 (64.2) | 3.69 [2.12–17.3] | 39 (72.2) | 0.138 |
| STC2 | |||||
| Circulation | 28 [16–37] | 37 (69.8) | 48 [37–81] | 36 (66.7) | 0.826 |
| Ascites | 40 [16–68] | 41 (77.4) | 89 [68–235] | 32 (59.3) | 0.055 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hjortebjerg, R.; Høgdall, C.; Hansen, K.H.; Høgdall, E.; Frystyk, J. The IGF–PAPP-A–Stanniocalcin Axis in Serum and Ascites Associates with Prognosis in Patients with Ovarian Cancer. Int. J. Mol. Sci. 2024, 25, 2014. https://doi.org/10.3390/ijms25042014
Hjortebjerg R, Høgdall C, Hansen KH, Høgdall E, Frystyk J. The IGF–PAPP-A–Stanniocalcin Axis in Serum and Ascites Associates with Prognosis in Patients with Ovarian Cancer. International Journal of Molecular Sciences. 2024; 25(4):2014. https://doi.org/10.3390/ijms25042014
Chicago/Turabian StyleHjortebjerg, Rikke, Claus Høgdall, Kristian Horsman Hansen, Estrid Høgdall, and Jan Frystyk. 2024. "The IGF–PAPP-A–Stanniocalcin Axis in Serum and Ascites Associates with Prognosis in Patients with Ovarian Cancer" International Journal of Molecular Sciences 25, no. 4: 2014. https://doi.org/10.3390/ijms25042014
APA StyleHjortebjerg, R., Høgdall, C., Hansen, K. H., Høgdall, E., & Frystyk, J. (2024). The IGF–PAPP-A–Stanniocalcin Axis in Serum and Ascites Associates with Prognosis in Patients with Ovarian Cancer. International Journal of Molecular Sciences, 25(4), 2014. https://doi.org/10.3390/ijms25042014