
Association Between Zinc Status and Insulin Resistance/Sensitivity Check Indexes in Gestational Diabetes Mellitus




Abstract
1. Introduction
2. Results
2.1. Characteristics and Comparison of Pregnant Women with and Without GDM
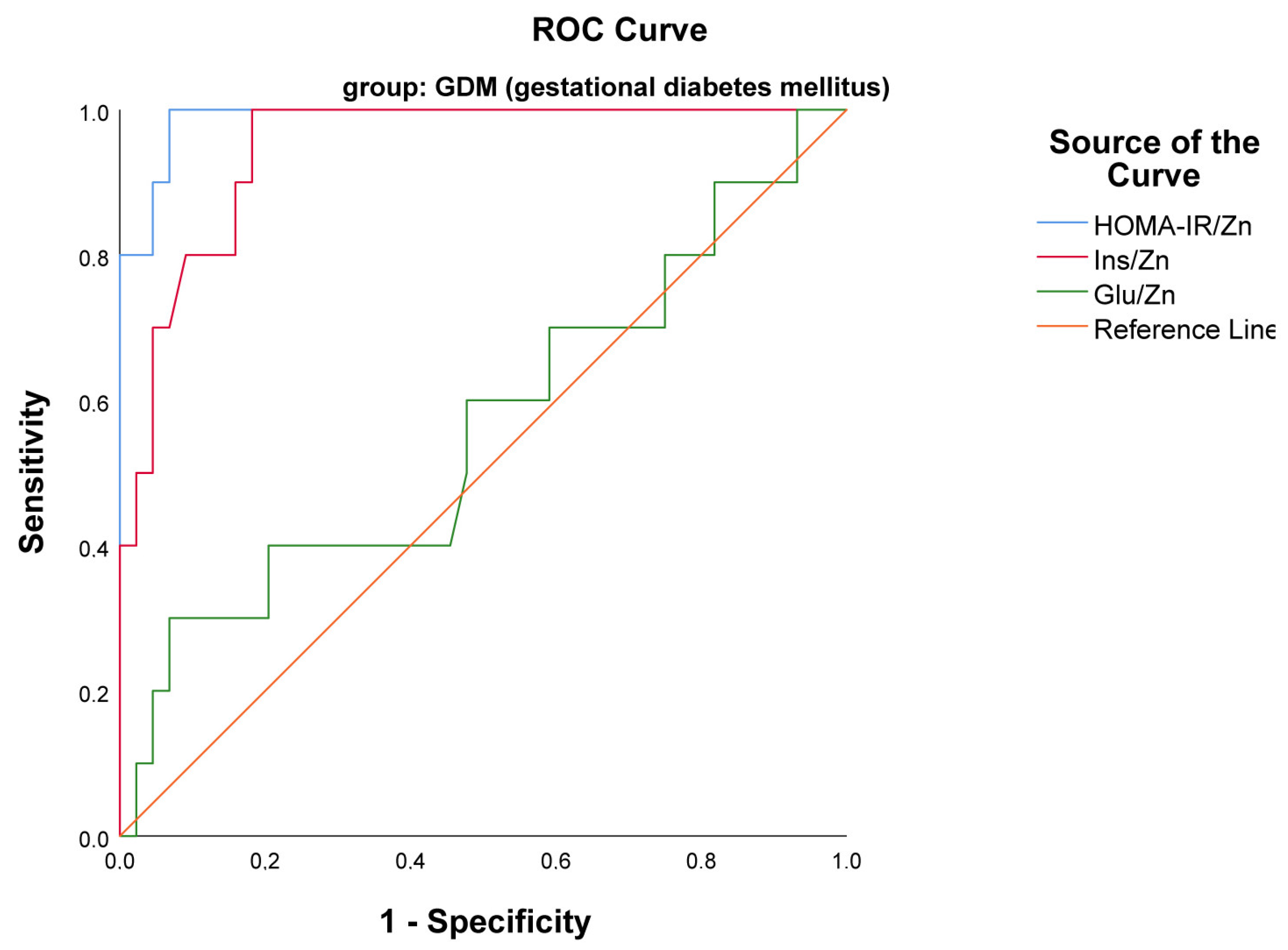
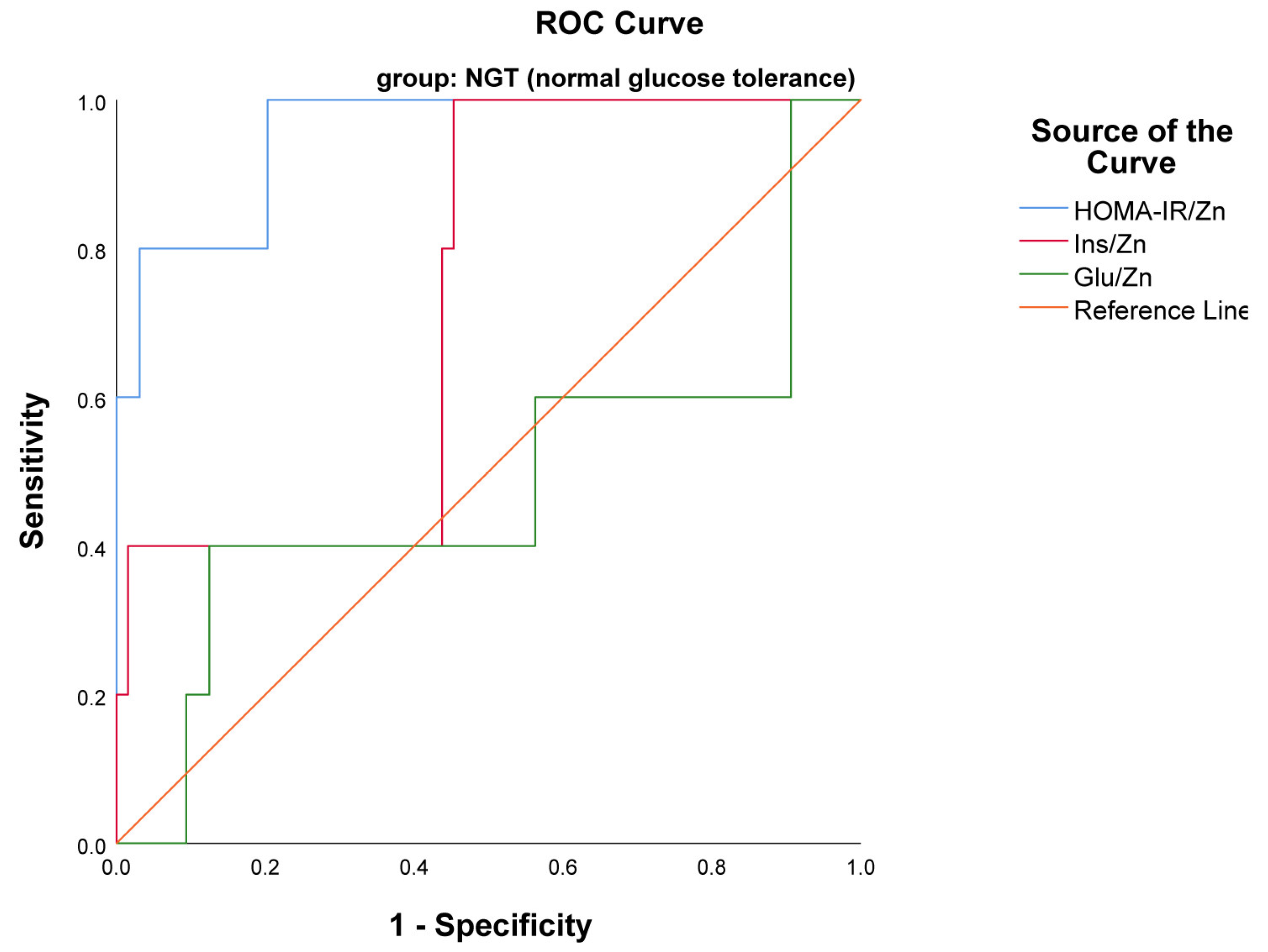
2.2. Assessment of the Usefulness of the Examined Indexes Glu/Zn, HOMA-IR/Zn, Ins/Zn as Markers of Insulin Resistance Using ROC Curves
3. Discussion
4. Materials and Methods
4.1. Diagnosis of GDM
4.2. Sample Collection and Measurement
4.3. Calculation of Indexes of Interest
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- International Diabetes Federation. IDF Diabetes ATLAS 9th Edition 2019. Available online: https://idf.org/about-diabetes/gestational-diabetes (accessed on 17 September 2024).
- American Diabetes Association. 2. Classification and diagnosis of diabetes: Standards of medical care in diabetes—2018. Diabetes Care 2018, 41 (Suppl. S1), S13–S27. [Google Scholar] [CrossRef] [PubMed]
- Sweeting, A.; Wong, J.; Murphy, H.R.; Ross, G.P. A clinical update on gestational diabetes mellitus. Endocr. Rev. 2022, 43, 763–793. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Li, N.; Chivese, T.; Werfalli, M.; Sun, H.; Yuen, L.; Hoegfeldt, C.A.; Elise Powe, C.; Immanuel, J.; Karuranga, S.; et al. IDF Diabetes Atlas Committee Hyperglycaemia in Pregnancy Special Interest Group. IDF Diabetes Atlas: Estimation of Global and Regional Gestational Diabetes Mellitus Prevalence for 2021 by International Association of Diabetes in Pregnancy Study Group’s Criteria. Diabetes Res. Clin. Pract. 2022, 183, 109050. [Google Scholar] [CrossRef] [PubMed]
- Homko, C.; Sivan, E.; Chen, X.; Reece, E.A.; Boden, G. Insulin secretion during and after pregnancy in patients with gestational diabetes mellitus. J. Clin. Endocrinol. Metab. 2001, 86, 568–573. [Google Scholar] [CrossRef]
- Ekmekcioglu, C.; Prohaska, C.; Pomazal, K.; Steffan, I.; Schernthaner, G.; Marktl, W. Concentrations of seven trace elements in different hematological matrices in patients with type 2 diabetes as compared to healthy controls. Biol. Trace Elem. Res. 2001, 79, 205–219. [Google Scholar] [CrossRef]
- Genova, M.; Atanasova, B.; Ivanova, I.; Todorova, K.; Svinarov, D. Trace elements and vitamin D in gestational diabetes. Acta Med. Bulg. 2018, 45, 45–49. [Google Scholar] [CrossRef]
- Li, P.; Yin, J.; Zhu, Y.; Li, S.; Chen, S.; Sun, T.; Shan, Z.; Wang, J.; Shang, Q.; Li, X.; et al. Association between plasma concentration of copper and gestational diabetes mellitus. Clin. Nutr. 2019, 38, 2922–2927. [Google Scholar] [CrossRef]
- Maxfield, L.; Shukla, S.; Crane, J.S. Zinc Deficiency; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: http://www.ncbi.nlm.nih.gov/books/NBK493231 (accessed on 17 September 2024).
- Beyersmann, D.; Haase, H. Functions of zinc in signaling, proliferation and differentiation of mammalian cells. Biometals 2001, 14, 331–341. [Google Scholar] [CrossRef]
- Banaszak, M.; Górna, I.; Przysławski, J. Zinc and the Innovative Zinc-α2-Glycoprotein Adipokine Play an Important Role in Lipid Metabolism: A Critical Review. Nutrients 2021, 13, 2023. [Google Scholar] [CrossRef]
- Tuncay, E.; Bitirim, V.C.; Durak, A.; Carrat, G.R.J.; Taylor, K.M.; Rutter, G.A.; Turan, B. Hyperglycemia-Induced Changes in ZIP7 and ZnT7 Expression Cause Zn2+ Release from the Sarco(endo)plasmic Reticulum and Mediate ER Stress in the Heart. Diabetes 2017, 66, 1346–1358. [Google Scholar] [CrossRef]
- Ortega, R.M.; Rodríguez-Rodríguez, E.; Aparicio, A.; Jiménez, A.I.; López-Sobaler, A.M.; González-Rodríguez, L.G.; Andrés, P. Poor zinc status is associated with increased risk of insulin resistance in Spanish children. Br. J. Nutr. 2012, 107, 398–404. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Cao, J.C.; Warthon-Medina, M.; Moran, H.V.; Arija, V.; Doepking, C.; Serra-Majem, L.; Lowe, N.M. Zinc intake and status and risk of type 2 diabetes mellitus: A systematic review and meta-analysis. Nutrients 2019, 11, 1027. [Google Scholar] [CrossRef] [PubMed]
- Yary, T.; Virtanen, J.K.; Ruusunen, A.; Tuomainen, T.P.; Voutilainen, S. Serum zinc and risk of type 2 diabetes incidence in men: The Kuopio Ischaemic Heart Disease Risk Factor Study. J. Trace Elem. Med. Biol. 2016, 33, 120–124. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.Y.; Hung, K.C.; Chuang, M.H.; Chang, R.; Chen, R.Y.; Wang, F.W.; Wu, J.Y.; Chen, J.Y. Effect of zinc supplementation on blood sugar control in the overweight and obese population: A systematic review and meta-analysis of randomized controlled trials. Obes. Res. Clin. Pract. 2023, 17, 308–317. [Google Scholar] [CrossRef] [PubMed]
- King, J.C. Determinants of maternal zinc status during pregnancy. Am. J. Clin. Nutr. 2000, 71 (Suppl. S5), 1334S–1343S. [Google Scholar] [CrossRef]
- Sandstead, H.H. Zinc is essential for brain development and function. J. Trace Elem. Exp. Med. 2003, 16, 165–173. [Google Scholar] [CrossRef]
- Karamali, M.; Bahramimoghadam, S.; Sharifzadeh, F.; Asemi, Z. Magnesium-zinc-calcium-vitamin D co-supplementation improves glycemic control and markers of cardiometabolic risk in gestational diabetes: A randomized, double-blind, placebo-controlled trial. Appl. Physiol. Nutr. Metab. 2018, 43, 565–570. [Google Scholar] [CrossRef]
- Li, D.; Cai, Z.; Pan, Z.; Yang, Y.; Zhang, J. The effects of vitamin and mineral supplementation on women with gestational diabetes mellitus. BMC Endocr. Disord. 2021, 21, 106. [Google Scholar] [CrossRef]
- Mishu, F.A.; Boral, N.; Ferdous, N.; Nahar, S.; Sultana, G.S.; Yesmin, M.S.; Khan, N.Z. Estimation of serum zinc, copper and magnesium levels in bangladeshi women with gestational diabetes mellitus attending in a tertiary care hospital. Mymensingh Med. J. 2019, 28, 157–162. [Google Scholar]
- Fan, J.; Zhang, T.; Yu, Y.; Zhang, B. Is serum zinc status related to gestational diabetes mellitus? A meta-analysis. Matern. Child. Nutr. 2021, 17, e13239. [Google Scholar] [CrossRef]
- Grădinaru, D.; Margină, D.; Ungurianu, A.; Nițulescu, G.; Pena, C.M.; Ionescu-Tîrgoviște, C.; Dănciulescu Miulescu, R. Zinc status, insulin resistance and glycoxidative stress in elderly subjects with type 2 diabetes mellitus. Exp. Ther. Med. 2021, 22, 1393. [Google Scholar] [CrossRef] [PubMed]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Dubey, P.; Thakur, V.; Chattopadhyay, M. Role of minerals and trace elements in diabetes and insulin resistance. Nutrients 2020, 12, 1864. [Google Scholar] [CrossRef]
- Khan, A.R.; Awan, F.R. Metals in the pathogenesis of type 2 diabetes. J. Diabetes Metab. Disord. 2014, 13, 16. [Google Scholar] [CrossRef]
- Hamdan, H.Z.; Elbashir, L.M.; Hamdan, S.Z.; Elhassan, E.M.; Adam, I. Zinc and selenium levels in women with gestational diabetes mellitus at Medani Hospital, Sudan. J. Obstet. Gynaecol. 2014, 34, 567–570. [Google Scholar] [CrossRef]
- Wilson, R.L.; Grieger, J.A.; Bianco-Miotto, T.; Roberts, C.T. Association between maternal zinc status, dietary zinc intake and pregnancy complications: A systematic review. Nutrients 2016, 8, 641. [Google Scholar] [CrossRef]
- Genova, M.P.; Atanasova, B.; Todorova-Ananieva, K.; Tzatchev, K. Plasma and Intracellular Erythocyte Zinc Levels during Pregnancy in Bulgarian Females with and without Gestational Diabetes. Int. J. Adv. Res. 2014, 2, 661–667. [Google Scholar]
- Deng, G.; Chen, H.; Liu, Y.; Zhou, Y.; Lin, X.; Wei, Y.; Sun, R.; Zhang, Z.; Huang, Z. Combined exposure to multiple essential elements and cadmium at early pregnancy on gestational diabetes mellitus: A prospective cohort study. Front. Nutr. 2023, 10, 1278617. [Google Scholar] [CrossRef]
- Wang, Y.; Tan, M.; Huang, Z.; Sheng, L.; Ge, Y.; Zhang, H.; Jiang, M.; Zhang, G. Elemental contents in serum of pregnant women with gestational diabetes mellitus. Biol. Trace Elem. Res. 2002, 88, 113–118. [Google Scholar] [CrossRef]
- Lewandowska, M.; Więckowska, B.; Sajdak, S.; Lubiński, J. First trimester microelements and their relationships with pregnancy outcomes and complications. Nutrients 2020, 12, 1108. [Google Scholar] [CrossRef]
- Liu, J.; Yang, H.; Shi, H.; Shen, C.; Zhou, W.; Dai, Q.; Jiang, Y. Blood copper, zinc, calcium, and magnesium levels during different duration of pregnancy in Chinese. Biol. Trace Elem. Res. 2010, 135, 31–37. [Google Scholar] [CrossRef] [PubMed]
- King, J.C. Zinc: An essential but elusive nutrient. Am. J. Clin. Nutr. 2011, 94, 679S–684S. [Google Scholar] [CrossRef] [PubMed]
- Grieger, J.A.; Grzeskowiak, L.E.; Wilson, R.L.; Bianco-Miotto, T.; Leemaqz, S.Y.; Jankovic-Karasoulos, T.; Perkins, A.V.; Norman, R.J.; Dekker, G.A.; Roberts, C.T. Maternal Selenium, Copper and Zinc Concentrations in Early Pregnancy, and the Association with Fertility. Nutrients 2019, 11, 1609. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.B.; Lu, J.X.; Wang, L.J.; Hu, Y.C.; Wang, R.; Mao, D.Q.; Huang, J.; Zhao, L.Y.; Yang, X.G.; Yang, L.C. Evaluation of Serum Zinc Status of Pregnant Women in the China Adult Chronic Disease and Nutrition Surveillance (CACDNS) 2015. Nutrients 2021, 13, 1375. [Google Scholar] [CrossRef]
- Liu, X.; Zhang, Y.; Piao, J.; Mao, D.; Li, Y.; Li, W.; Yang, L.; Yang, X. Reference Values of 14 Serum Trace Elements for Pregnant Chinese Women: A Cross-Sectional Study in the China Nutrition and Health Survey 2010–2012. Nutrients 2017, 9, 309. [Google Scholar] [CrossRef]
- Watson, C.V.; Lewin, M.; Ragin-Wilson, A.; Jones, R.; Jarrett, J.M.; Wallon, K.; Ward, C.; Hilliard, N.; Irvin-Barnwell, E. Characterization of trace elements exposure in pregnant women in the United States, NHANES 1999–2016. Environ. Res. 2020, 183, 109208. [Google Scholar] [CrossRef]
- Izquierdo Alvarez, S.; Castañón, S.G.; Ruata, M.L.; Aragüés, E.F.; Terraz, P.B.; Irazabal, Y.G.; González, E.G.; Rodríguez, B.G. Updating of normal levels of copper, zinc and selenium in serum of pregnant women. J. Trace Elem. Med. Biol. 2007, 21 (Suppl. S1), 49–52. [Google Scholar] [CrossRef]
- Pop, V.; Krabbe, J.; Maret, W.; Rayman, M. Plasma mineral (selenium, zinc or copper) concentrations in the general pregnant population, adjusted for supplement intake, in relation to thyroid function. Br. J. Nutr. 2021, 125, 71–78. [Google Scholar] [CrossRef]
- Choi, R.; Sun, J.; Yoo, H.; Kim, S.; Cho, Y.Y.; Kim, H.J.; Kim, S.W.; Chung, J.H.; Oh, S.Y.; Lee, S.Y. A prospective study of serum trace elements in healthy Korean pregnant women. Nutrients 2016, 8, 749. [Google Scholar] [CrossRef]
- Moran, V.H.; Skinner, A.L.; Medina, M.W.; Patel, S.; Dykes, F.; Souverein, O.W.; Dullemeijer, C.; Lowe, N.M. The relationship between zinc intake and serum/plasma zinc concentration in pregnant and lactating women: A systematic review with dose-response meta-analyses. J. Trace Elem. Med. Biol. 2012, 26, 74–79. [Google Scholar] [CrossRef]
- Chabosseau, P.; Rutter, G.A. Zinc and diabetes. Arch. Biochem. Biophys. 2016, 611, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Ruz, M.; Carrasco, F.; Rojas, P.; Basfi-Fer, K.; Hernández, M.C.; Pérez, A. Nutritional effects of zinc on metabolic syndrome and type 2 diabetes: Mechanisms and main findings in human studies. Biol. Trace Elem. Res. 2019, 188, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Norouzi, S.; Adulcikas, J.; Sohal, S.S.; Myers, S. Zinc stimulates glucose oxidation and glycemic control by modulating the insulin signaling pathway in human and mouse skeletal muscle cell lines. PLoS ONE 2018, 13, e0191727. [Google Scholar] [CrossRef] [PubMed]
- Kelishadi, R.; Hashemipour, M.; Adeli, K.; Tavakoli, N.; Movahedian-Attar, A.; Shapouri, J.; Poursafa, P.; Rouzbahani, A. Effect of zinc supplementation on markers of insulin resistance, oxidative stress, and inflammation among prepubescent children with metabolic syndrome. Metab. Syndr. Relat. Disord. 2010, 8, 505–510. [Google Scholar] [CrossRef]
- Ranasinghe, P.; Pigera, S.; Galappatthy, P.; Katulanda, P.; Constantine, G.R. Zinc and diabetes mellitus: Understanding molecular mechanisms and clinical implications. DARU J. Pharm. Sci. 2015, 23, 44. [Google Scholar] [CrossRef]
- Vardatsikos, G.; Pandey, N.R.; Srivastava, A.K. Insulino-mimetic and anti-diabetic effects of zinc. J. Inorg. Biochem. 2013, 120, 8–17. [Google Scholar] [CrossRef]
- Buchner, D.A.; Charrier, A.; Srinivasan, E.; Wang, L.; Paulsen, M.T.; Ljungman, M.; Bridges, D.; Saltiel, A.R. Zinc finger protein 407 (ZFP407) regulates insulin-stimulated glucose uptake and glucose transporter 4 (Glut4) mRNA. J. Biol. Chem. 2015, 290, 6376–6386. [Google Scholar] [CrossRef]
- Vashum, K.P.; McEvoy, M.; Milton, A.H.; Islam, M.R.; Hancock, S.; Attia, J. Is Serum Zinc Associated with Pancreatic Beta Cell Function and Insulin Sensitivity in Pre-Diabetic and Normal Individuals? Findings from the Hunter Community Study. PLoS ONE 2014, 9, e83944. [Google Scholar] [CrossRef]
- Daneshvar, M.; Ghaheri, M.; Safarzadeh, D.; Karimi, F.; Adib-Hajbagheri, P.; Ahmadzade, M.; Haedi, A. Diabetology Metabolic Syndrome. Diabetol. Metab. Syndr. 2024, 16, 124. [Google Scholar] [CrossRef]
- Li, X.; Zhao, J. The influence of zinc supplementation on metabolic status in gestational diabetes: A meta-analysis of randomized controlled studies. J. Matern. -Fetal Neonatal Med. 2021, 34, 2140–2145. [Google Scholar] [CrossRef]
- Pompano, L.M.; Boy, E. Effects of dose and duration of zinc interventions on risk factors for type 2 diabetes and cardiovascular disease: A systematic review and meta-analysis. Adv. Nutr. 2021, 12, 141–160. [Google Scholar] [CrossRef] [PubMed]
- Khazdouz, M.; Djalalinia, S.; Sarrafi Zadeh, S.; Hasani, M.; Shidfar, F.; Ataie-Jafari, A.; Asayesh, H.; Zarei, M.; Gorabi, A.M.; Noroozi, M.; et al. Effects of zinc supplementation on cardiometabolic risk factors: A systematic review and meta-analysis of randomized controlled trials. Biol. Trace Elem. Res. 2020, 195, 373–398. [Google Scholar] [CrossRef] [PubMed]
- Nazari, M.; Nikbaf-Shandiz, M.; Pashayee-Khamene, F.; Bagheri, R.; Goudarzi, K.; Hosseinnia, N.V.; Dolatshahi, S.; Omran, H.S.; Amirani, N.; Ashtary-Larky, D.; et al. Zinc supplementation in individuals with pre–diabetes and type 2 diabetes: A GRADE-assessed systematic review and dose-response meta-analysis. Biol. Trace Elem. Res. 2023, 202, 2966–2990. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Ronsmans, C.; Woolf, B. Triangulating evidence for the causal impact of single-intervention zinc supplement on glycaemic control for type 2 diabetes: Systematic review and meta-analysis of randomised controlled trial and two-sample Mendelian randomisation. Br. J. Nutr. 2023, 129, 1929–1944. [Google Scholar] [CrossRef]
- Kant, R.; Verma, V.; Patel, S.; Chandra, R.; Chaudhary, R.; Shuldiner, A.R.; Munir, K.M. Effect of serum zinc and copper levels on insulin secretion, insulin resistance and pancreatic β cell dysfunction in US adults: Findings from the National Health and Nutrition Examination Survey (NHANES) 2011–2012. Diabetes Res. Clin. Pract. 2021, 172, 108627. [Google Scholar] [CrossRef]
- Wang, X.; Wu, W.; Zheng, W.; Fang, X.; Chen, L.; Rink, L.; Min, J.; Wang, F. Zinc supplementation improves glycemic control for diabetes prevention and management: A systematic review and meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2019, 110, 76–90. [Google Scholar] [CrossRef]
- Zhang, H.; Yan, C.; Yang, Z.; Zhang, W.; Niu, Y.; Li, X.; Qin, L.; Su, Q. Alterations of serum trace elements in patients with type 2 diabetes. J. Trace Elem. Med. Biol. 2017, 40, 91–96. [Google Scholar] [CrossRef]
- Eva, H.; Akter, Q.S.; Alam, M.K. Relationship of Serum Glycemic Status with Serum Zinc Level in Type 2 Diabetes Mellitus. Mymensingh Med. J. 2020, 29, 357–360. [Google Scholar]
- Zhu, G.; Zheng, T.; Xia, C.; Qi, L.; Papandonatos, G.D.; Ming, Y.; Zeng, Z.; Zhang, X.; Zhang, H.; Li, Y. Plasma levels of trace element status in early pregnancy and the risk of gestational diabetes mellitus: A nested case-control study. J. Trace Elem. Med. Biol. 2021, 68, 126829. [Google Scholar] [CrossRef]
- Carducci, B.; Keats, E.C.; Bhutta, Z.A. Zinc supplementation for improving pregnancy and infant outcome. Cochrane Database Syst. Rev. 2021, 3, CD000230. [Google Scholar] [CrossRef]
- Genova, M.P.; Atanasova, B.; Todorova-Ananieva, K.; Velisarova, M.; Hristova, J.; Tzatchev, K. Zinc and insulin resistance in pregnancy complicated with gestational diabetes. Int. J. Health Sci. Res. 2016, 6, 191–197. [Google Scholar]
- Moghaddam, F.F.; Mehrzad, J.; Saeidi, J.; Ghasemi, A. A Study on the Association of Copper and Zinc Serum Levels with Insulin Resistance Indices in Gestational Diabetes. Int. J. Pharm. Phytopharm. Res. 2020, 10, 231–236. [Google Scholar]
- Lobene, A.J.; Kindler, J.M.; Jenkins, N.T.; Pollock, N.K.; Laing, E.M.; Grider, A.; Lewis, R.D. Zinc Supplementation Does Not Alter Indicators of Insulin Secretion and Sensitivity in Black and White Female Adolescents. J. Nutr. 2017, 147, 1296–1300. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. J. Am. Med. Assoc. 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Song, Y.S.; Hwang, Y.C.; Ahn, H.Y.; Park, C.Y. Comparison of the Usefulness of the Updated Homeostasis Model Assessment (HOMA2) with the Original HOMA1 in the Prediction of Type 2 Diabetes Mellitus in Koreans. Diabetes Metab. J. 2016, 40, 318–325. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | GDM Pregnant Woman (n = 54) | NGT Pregnant Woman; (n = 54) | p-Value |
|---|---|---|---|
| Maternal age (years); mean ± SD | 32 ± 5.8 | 30.4 ± 5.1 | 0.078 ** |
| Pre-gestational BMI (kg/m2); mean ± SD | 27.6 ± 7.2 | 23.3 ± 4.1 | 0.001 ** |
| BMI at GDM diagnosis (kg/m2); mean ± SD | 30.4 ± 7.0 | 26.1 ± 4.2 | <0.001 ** |
| Gestational age at blood drawing (weeks); mean ± SD | 26.5 ± 3.2 | 25.9 ± 2.8 | 0.522 ** |
| Smoking habit; n, % | 0 | 0 | - |
| Drinking habit; n, % | 0 | 0 | - |
| Family history of diabetes; n, % | 15(27.7) | 6(11.1) | 0.016 *** |
| FPG, mmol/L; median (interquartile range) | 5.3(5.1–5.4) | 4.4(4.1–4.7) | <0.001 * |
| OGTT-1h, mmol/L; median (interquartile range) | 8.3 ± 2.3 | 6.7 ± 1.5 | <0.001 ** |
| OGTT-2h; mmol/L; median (interquartile range) | 6.0(4.7–7.6) | 5.0(4.4–6.1) | <0.002 * |
| FSI µU/mL; median (interquartile range) | 10.3(5.4–16.1) | 7.3(5.0–10.4) | <0.002 * |
| HOMA-IR; median (interquartile range) | 2.0(1.3–3.4) | 0.9(0.6–1.3) | <0.001 * |
| HOMA-B; median (interquartile range) | 94.7(69.4–135) | 113.3(84.2–149.5) | 0.041 * |
| HOMA-S; median (interquartile range) | 76.8(51.4–138) | 126.1(81.7–180.3) | <0.001 * |
| QUICKI index; median (interquartile range) | 0.3(0.3–0.4) | 0.4(0.3–0.4) | <0.001 * |
| Zn, µmol/L; median (interquartile range) | 13.7(13–16.8) | 15.1(12.4–18.2) | 0.872 * |
| Parameters | GDM Pregnant Women (n = 54) Median (Interquartile Range) | NGT Pregnant Women; (n = 54) Median (Interquartile Range) | p-Value |
|---|---|---|---|
| Glu/Zn; mmol/L/ µmol/L | 0.39(0.30–0.41) | 0.29(0.24–0.35) | <0.001 * |
| Ins/Zn; µU/mL/ µmol/L | 0.73(0.33–1.16) | 0.48(0.25–0.70) | 0.017 * |
| HOMA-IR/Zn | 0.14(0.08–0.23) | 0.06(0.03–0.09) | <0.001 * |
| Indexes | HOMA-IR | HOMA-B | HOMA-S | QUICKI | ||||
|---|---|---|---|---|---|---|---|---|
| Spearman’s rho | p-Value | Spearman’s rho | p-Value | Spearman’s rho | p-Value | Spearman’s rho | p-Value | |
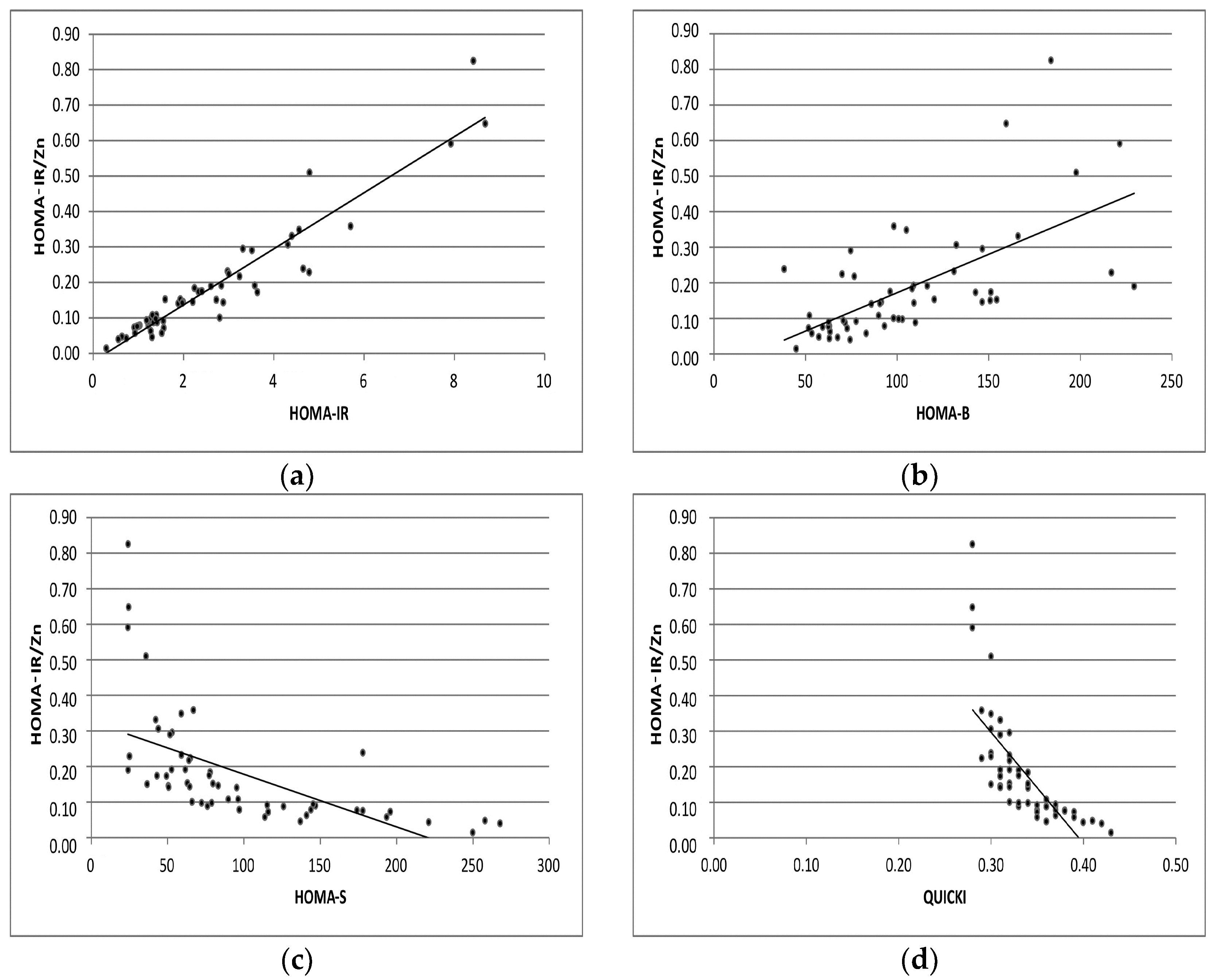
| Glu/Zn | 0.212 | 0.123 | 0.196 | 0.156 | −0.327 | 0.016 | −0.252 | 0.066 |
| HOMA-IR/Zn | 0.937 | 0.001 | 0.691 | 0.001 | −0.824 | 0.001 | −0.895 | 0.001 |
| Ins/Zn | 0.799 | 0.001 | 0.698 | 0.001 | −0.809 | 0.001 | −0.879 | 0.001 |
| Indexes | HOMA-IR | HOMA-B | HOMA-S | QUICKI | ||||
|---|---|---|---|---|---|---|---|---|
| Spearman’s rho | p-Value | Spearman’s rho | p-Value | Spearman’s rho | p-Value | Spearman’s rho | p-Value | |
| Glu/Zn | 0.285 | 0.018 | 0.004 | 0.972 | −0.196 | 0.107 | −0.270 | 0.025 |
| HOMA-IR/Zn | 0.918 | 0.001 | 0.665 | 0.001 | −0.846 | 0.001 | −0.795 | 0.001 |
| Ins/Zn | 0.777 | 0.001 | 0.554 | 0.001 | −0.724 | 0.001 | −0.871 | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Genova, M.P.; Ivanova, I.; Naseva, E.; Atanasova, B. Association Between Zinc Status and Insulin Resistance/Sensitivity Check Indexes in Gestational Diabetes Mellitus. Int. J. Mol. Sci. 2024, 25, 12193. https://doi.org/10.3390/ijms252212193
Genova MP, Ivanova I, Naseva E, Atanasova B. Association Between Zinc Status and Insulin Resistance/Sensitivity Check Indexes in Gestational Diabetes Mellitus. International Journal of Molecular Sciences. 2024; 25(22):12193. https://doi.org/10.3390/ijms252212193
Chicago/Turabian StyleGenova, Mariana P., Irena Ivanova, Emilia Naseva, and Bisera Atanasova. 2024. "Association Between Zinc Status and Insulin Resistance/Sensitivity Check Indexes in Gestational Diabetes Mellitus" International Journal of Molecular Sciences 25, no. 22: 12193. https://doi.org/10.3390/ijms252212193
APA StyleGenova, M. P., Ivanova, I., Naseva, E., & Atanasova, B. (2024). Association Between Zinc Status and Insulin Resistance/Sensitivity Check Indexes in Gestational Diabetes Mellitus. International Journal of Molecular Sciences, 25(22), 12193. https://doi.org/10.3390/ijms252212193