
The Role of Physical Therapies in Wound Healing and Assisted Scarring


 ,
,  , and
, and
Abstract
1. Introduction
2. General Approach to Wounds
2.1. Epidemiology
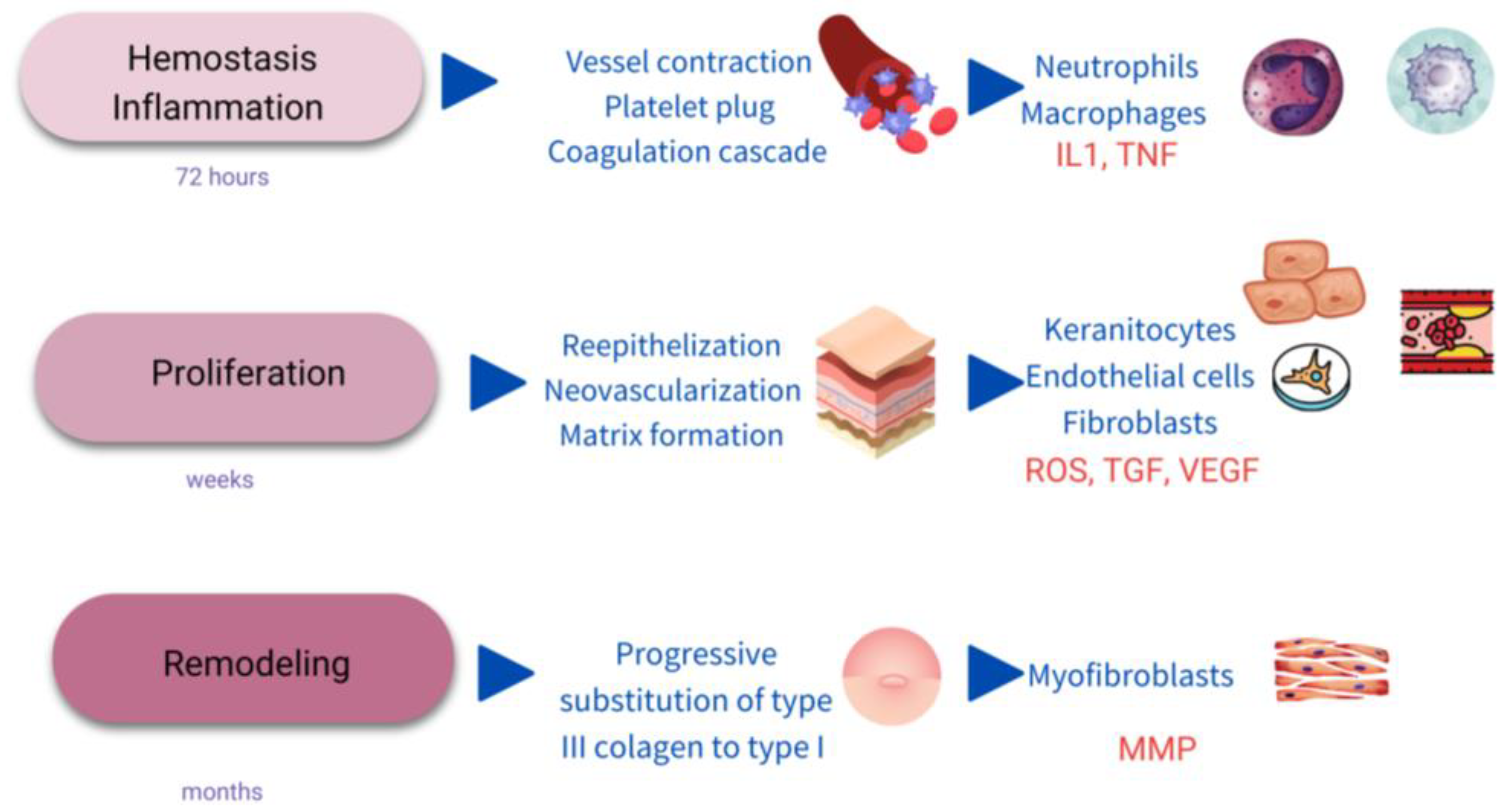
2.2. Process and Stages of Wound Healing
2.2.1. Hemostasis/Inflammatory Stage
2.2.2. Proliferation
2.2.3. Maturation/Remodeling
2.3. Chronic Wounds
2.3.1. Diabetic Ulcer
2.3.2. Pressure Ulcer
2.3.3. Venous Ulcer
2.4. General Management of Chronic Wounds
2.5. General Prevention of Scarring
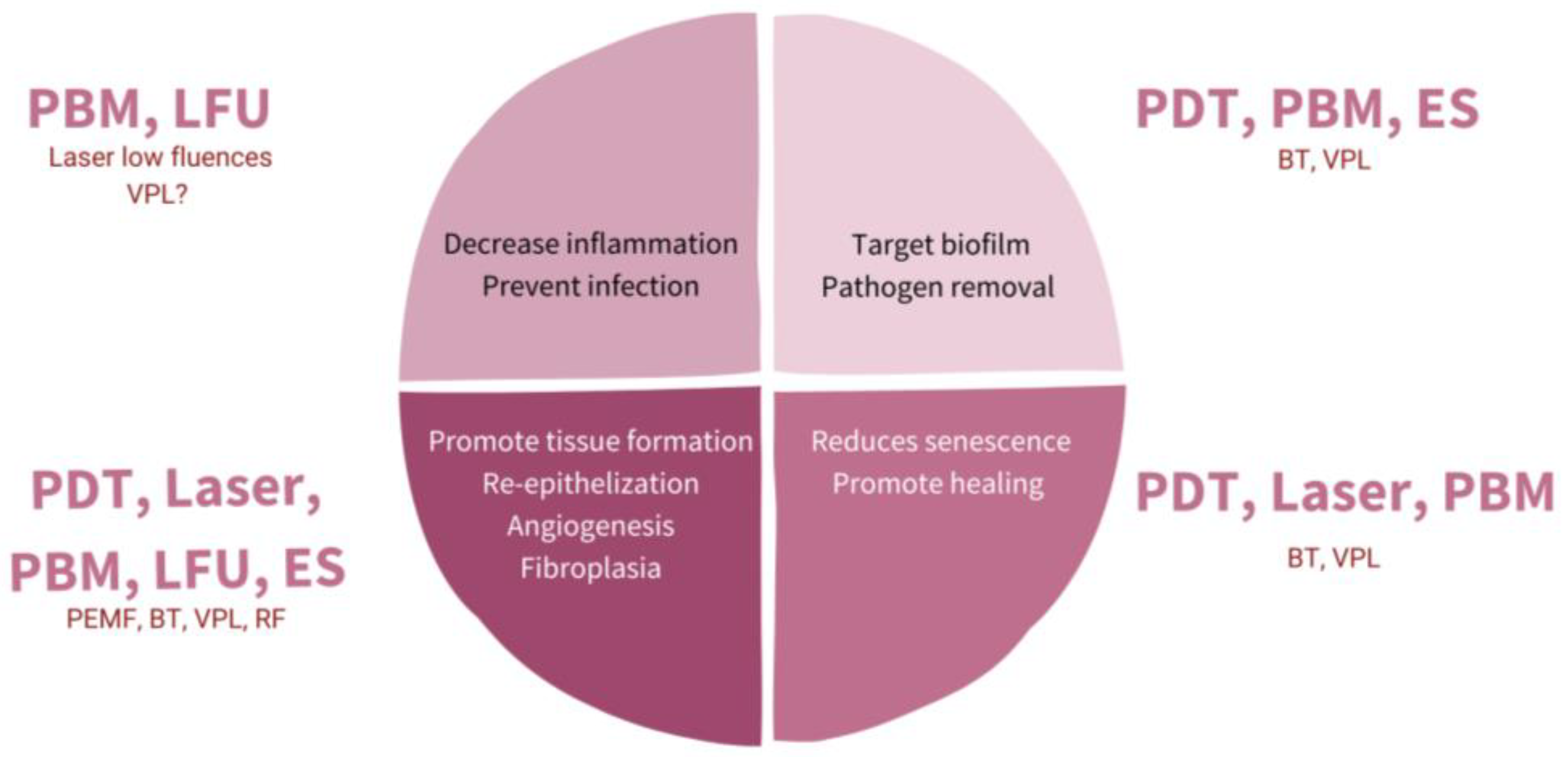
3. The Role of Physical Therapies in Hard-To-Heal Chronic Wounds
Principles and Basis
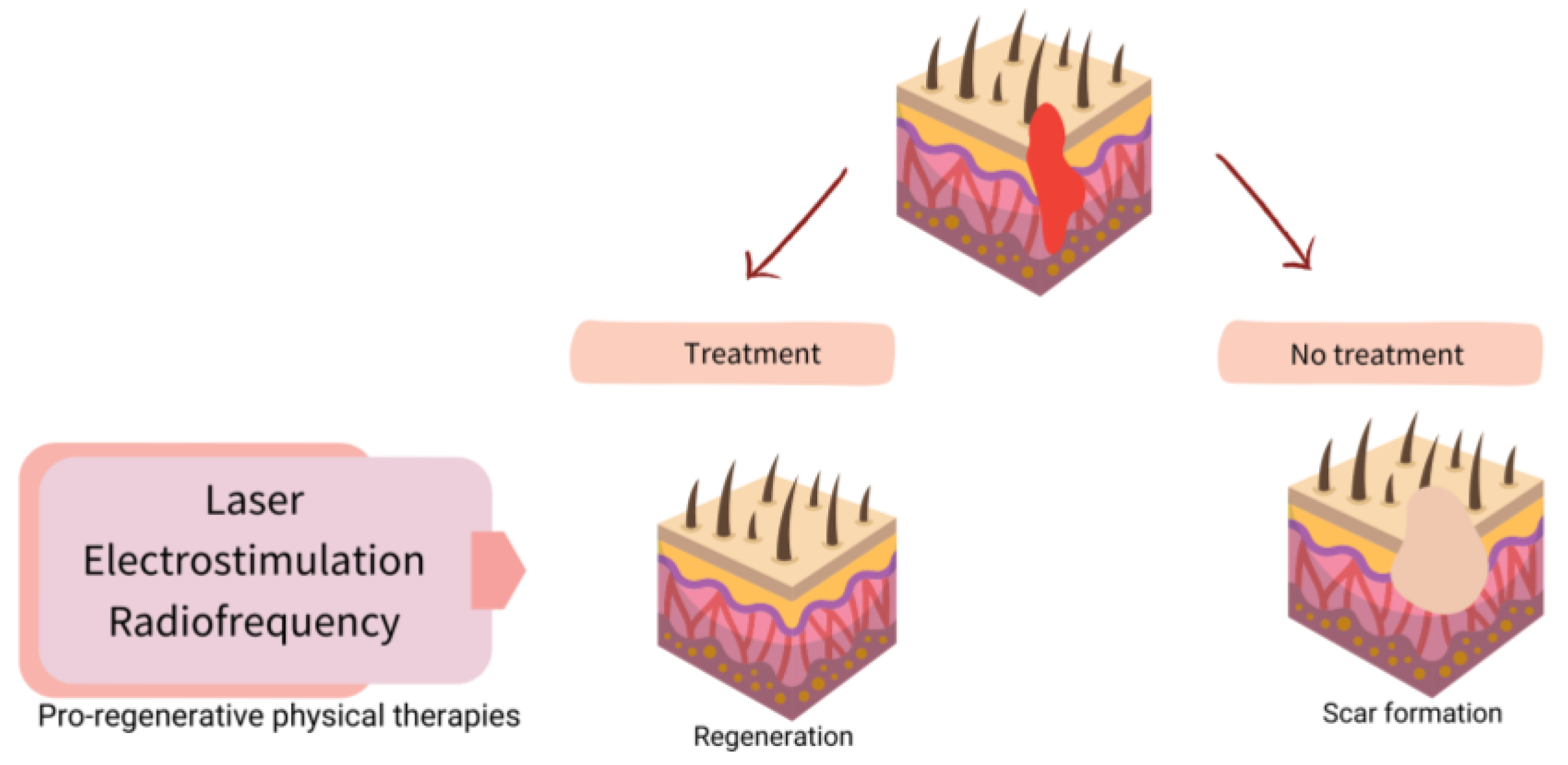
4. Physical Therapies in Assisted Healing and Scar Prevention
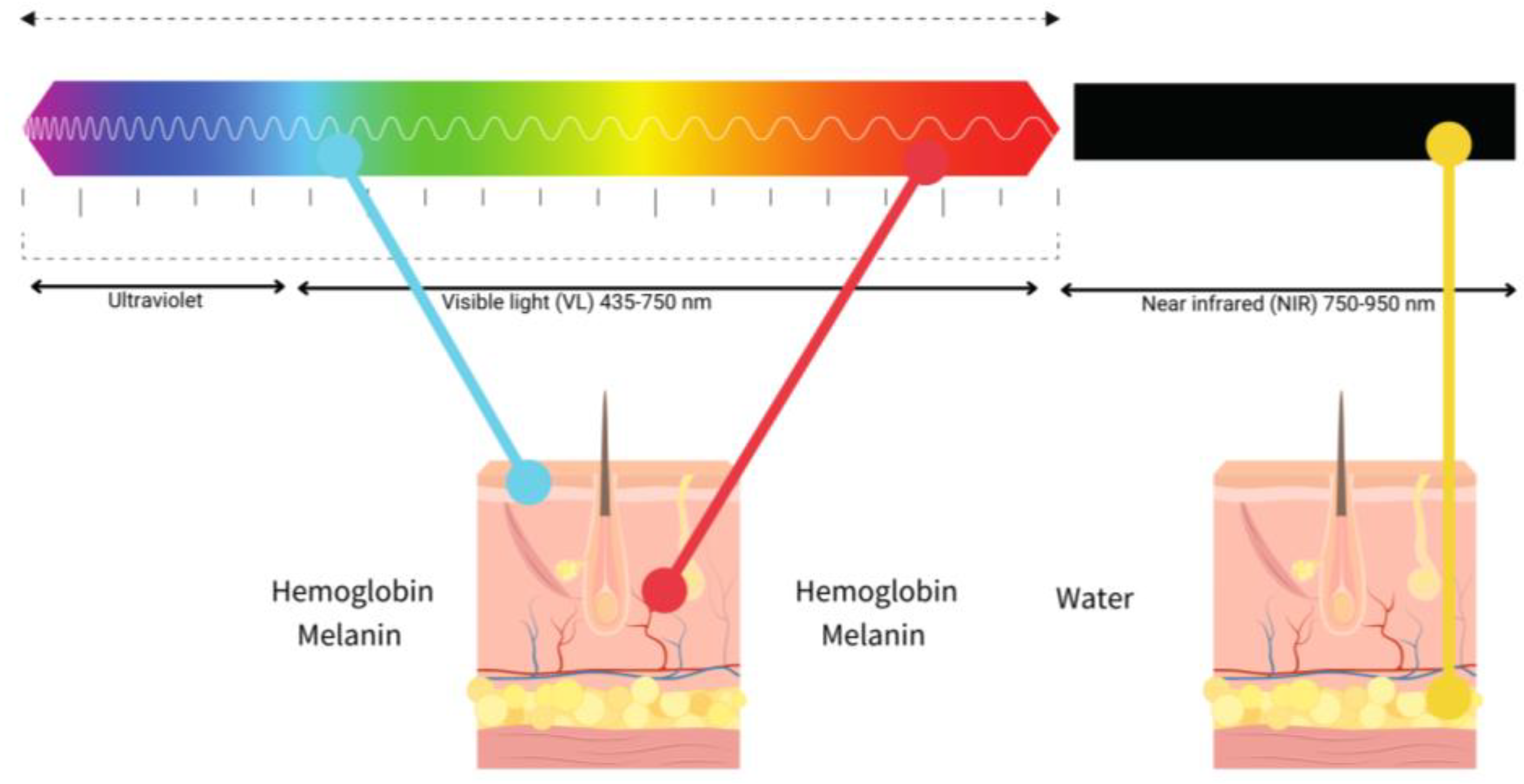
4.1. Laser
4.2. Photobiomodulation (Low-Level Light Therapy-LLLT)
Blue Light Emission Diode
4.3. Photodynamic Therapy
4.4. Electrical Stimulation
4.5. Others
4.5.1. Ultrasound Therapy
4.5.2. Electromagnetic Fields
4.5.3. Biophotonic Therapy
4.5.4. Visible Polarized Light
4.5.5. Radiofrequency
5. Summary of Clinical Trials of Physical Therapies in Wound Healing
6. Conclusions and Future Perspectives
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AU | Atypical ulcer |
| BT | Biophotonic therapy |
| CW | Chronic wound |
| DU | Diabetic ulcer |
| EBF | Endogenous bioelectric fields |
| ES | Electrical stimulation |
| FHW | Fail to heal wound |
| HS | Hypertrophic scar |
| LLLT | Low level laser light therapy |
| PDL | Pulsed dye laser |
| PEMF | Pulsed electromagnetic field |
| PT | Physical therapies |
| PU | Pressure ulcer |
| US | Ultrasound |
| UT | Ultrasound therapy |
| VU | Venous leg ulcer |
| WH | Wound healing |
References
- Gupta, S.; Andersen, C.; Black, J.; Fife, C.; Lantis, J.I.; Niezgoda, J.; Snyder, R.; Sumpio, B.; Tettelbach, W.; Treadwell, T.; et al. Management of Chronic Wounds: Diagnosis, Preparation, Treatment, and Follow-Up. Wounds Compend. Clin. Res. Pract. 2017, 29, S19–S36. [Google Scholar]
- Wang, P.H.; Huang, B.S.; Horng, H.C.; Yeh, C.C.; Chen, Y.J. Wound healing. J. Chin. Med. Assoc. 2018, 81, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, M.; Kosaric, N.; Bonham, C.A.; Gurtner, G.C. Wound Healing: A Cellular Perspective. Physiol. Rev. 2019, 99, 665–706. [Google Scholar] [CrossRef] [PubMed]
- Veith, A.P.; Henderson, K.; Spencer, A.; Sligar, A.D.; Baker, A.B. Therapeutic strategies for enhancing angiogenesis in wound healing. Adv. Drug Deliv. Rev. 2019, 146, 97–125. [Google Scholar] [CrossRef] [PubMed]
- Monavarian, M.; Kader, S.; Moeinzadeh, S.; Jabbari, E. Regenerative Scar-Free Skin Wound Healing. Tissue Eng. Part B Rev. 2019, 25, 294–311. [Google Scholar] [CrossRef]
- Bai, Q.; Han, K.; Dong, K.; Zheng, C.; Zhang, Y.; Long, Q.; Lu, T. Potential Applications of Nanomaterials and Technology for Diabetic Wound Healing. Int. J. Nanomed. 2020, 15, 9717–9743. [Google Scholar] [CrossRef]
- Palmieri, B.; Vadalà, M.; Laurino, C. Electromedical devices in wound healing management: A narrative review. J. Wound Care 2020, 29, 408–418. [Google Scholar] [CrossRef]
- Lu, W.-S.; Zheng, X.-D.; Yao, X.-H.; Zhang, L.-F. Clinical and epidemiological analysis of keloids in Chinese patients. Arch. Dermatol. Res. 2015, 307, 109–114. [Google Scholar] [CrossRef]
- Berman, B.; Maderal, A.; Raphael, B. Keloids and Hypertrophic Scars: Pathophysiology, Classification, and Treatment. Dermatol. Surg. 2017, 43, S3–S18. [Google Scholar] [CrossRef]
- He, Y.; Deng, Z.; Alghamdi, M.; Lu, L.; Fear, M.W.; He, L. From genetics to epigenetics: New insights into keloid scarring. Cell Prolif. 2017, 50, e12326. [Google Scholar] [CrossRef]
- Huang, C.; Ogawa, R. Systemic factors that shape cutaneous pathological scarring. FASEB J. 2020, 34, 13171–13184. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Ogawa, R. Keloidal pathophysiology: Current notions. Scars Burn. Health 2021, 7. [Google Scholar] [CrossRef]
- Bowers, S.; Franco, E. Chronic Wounds: Evaluation and Management. Am. Fam. Physician 2020, 101, 159–166. [Google Scholar]
- Gottrup, F. A specialized wound-healing center concept: Importance of a multidisciplinary department structure and surgical treatment facilities in the treatment of chronic wounds. Am. J. Surg. 2004, 187, S38–S43. [Google Scholar] [CrossRef] [PubMed]
- Fife, C.E.; Carter, M.J. Wound Care Outcomes and Associated Cost among Patients Treated in US Outpatient Wound Centers: Data from the US Wound Registry. Wounds A Compend. Clin. Res. Pract. 2012, 24, 10–17. [Google Scholar]
- Gurtner, G.C.; Werner, S.; Barrandon, Y.; Longaker, M.T. Wound repair and regeneration. Nature 2008, 453, 314–321. [Google Scholar] [CrossRef]
- Furie, B.; Furie, B.C. Mechanisms of thrombus formation. N. Engl. J. Med. 2008, 359, 938–949. [Google Scholar] [CrossRef]
- Bacci, S. Fine Regulation during Wound Healing by Mast Cells, a Physiological Role Not Yet Clarified. Int. J. Mol. Sci. 2022, 23, 1820. [Google Scholar] [CrossRef]
- Jorch, S.K.; Kubes, P. An emerging role for neutrophil extracellular traps in noninfectious disease. Nat Med. 2017, 23, 279–287. [Google Scholar] [CrossRef]
- Kolaczkowska, E.; Kubes, P. Neutrophil recruitment and function in health and inflammation. Nat. Rev. Immunol. 2013, 13, 159–175. [Google Scholar] [CrossRef]
- Akbik, D.; Ghadiri, M.; Chrzanowski, W.; Rohanizadeh, R. Curcumin as a wound healing agent. Life Sci. 2014, 116, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, H.N.; Hardman, M.J. Wound healing: Cellular mechanisms and pathological outcomes. Open Biol. 2020, 10, 200223. [Google Scholar] [CrossRef] [PubMed]
- Jupiter, D.C.; Thorud, J.C.; Buckley, C.J.; Shibuya, N. The impact of foot ulceration and amputation on mortality in diabetic patients. I: From ulceration to death, a systematic review. Int. Wound J. 2016, 13, 892–903. [Google Scholar] [CrossRef] [PubMed]
- Meulendijks, A.M.; de Vries, F.M.C.; van Dooren, A.A.; Schuurmans, M.J.; Neumann, H.A.M. A systematic review on risk factors in developing a first-time Venous Leg Ulcer. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 1241–1248. [Google Scholar] [CrossRef] [PubMed]
- Aleksandrowicz, H.; Owczarczyk-Saczonek, A.; Placek, W. Venous Leg Ulcers: Advanced Therapies and New Technologies. Biomedicines 2021, 9, 1569. [Google Scholar] [CrossRef]
- Wilcox, J.R.; Carter, M.J.; Covington, S. Frequency of debridements and time to heal: A retrospective cohort study of 312 744 wounds. JAMA Dermatol. 2013, 149, 1050–1058. [Google Scholar] [CrossRef]
- Azevedo, M.-M.; Lisboa, C.; Cobrado, L.; Pina-Vaz, C.; Rodrigues, A.G. Hard-to-heal wounds, biofilm and wound healing: An intricate interrelationship. Br. J. Nurs. 2020, 29, S6–S13. [Google Scholar] [CrossRef]
- Sun, F.; Qu, F.; Ling, Y.; Mao, P.; Xia, P.; Chen, H.; Zhou, D. Biofilm-associated infections: Antibiotic resistance and novel therapeutic strategies. Futur. Microbiol. 2013, 8, 877–886. [Google Scholar] [CrossRef]
- Pastar, I.; Stojadinovic, O.; Yin, N.C.; Ramirez, H.; Nusbaum, A.G.; Sawaya, A.; Patel, S.B.; Khalid, L.; Isseroff, R.R.; Tomic-Canic, M. Epithelialization in Wound Healing: A Comprehensive Review. Adv. Wound Care 2014, 3, 445–464. [Google Scholar] [CrossRef]
- Grandi, V.; Corsi, A.; Pimpinelli, N.; Bacci, S. Cellular Mechanisms in Acute and Chronic Wounds after PDT Therapy: An Update. Biomedicines 2022, 10, 1624. [Google Scholar] [CrossRef]
- Huang, C.; Akaishi, S.; Hyakusoku, H.; Ogawa, R. Are keloid and hypertrophic scar different forms of the same disorder? A fibroproliferative skin disorder hypothesis based on keloid findings. Int. Wound J. 2014, 11, 517–522. [Google Scholar] [CrossRef] [PubMed]
- Khetarpal, S.; Kaw, U.; Dover, J.S.; Arndt, K.A. Laser advances in the treatment of burn and traumatic scars. Semin. Cutan. Med. Surg. 2017, 36, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Jourdan, M.; Madfes, D.C.; Lima, E.; Tian, Y.; Seité, S. Skin Care Management for Medical and Aesthetic Procedures to Prevent Scarring. Clin. Cosmet. Investig. Dermatol. 2019, 12, 799–804. [Google Scholar] [CrossRef] [PubMed]
- Kauvar, A.N.B.; Kubicki, S.L.; Suggs, A.K.; Friedman, P.M. Laser Therapy of Traumatic and Surgical Scars and an Algorithm for Their Treatment. Lasers Surg. Med. 2020, 52, 125–136. [Google Scholar] [CrossRef]
- Altemir, A.; Boixeda, P. Laser Treatment of Burn Scars. Actas Dermosifiliogr. 2022, 113, T938–T944. [Google Scholar] [CrossRef] [PubMed]
- Clementoni, M.T.; Pedrelli, V.; Zaccaria, G.; Pontini, P.; Motta, L.R.; Azzopardi, E.A. New Developments for Fractional CO2 Resurfacing for Skin Rejuvenation and Scar Reduction. Facial Plast. Surg. Clin. N. Am. 2020, 28, 17–28. [Google Scholar] [CrossRef]
- Azzam, O.A.; Bassiouny, D.A.; El-Hawary, M.S.; El Maadawi, Z.M.; Sobhi, R.M.; El-Mesidy, M.S. Treatment of hypertrophic scars and keloids by fractional carbon dioxide laser: A clinical, histological, and immunohistochemical study. Lasers Med. Sci. 2016, 31, 9–18. [Google Scholar] [CrossRef]
- Yang, Q.; Ma, Y.; Zhu, R.; Huang, G.; Guan, M.; Avram, M.M.; Lu, Z. The effect of flashlamp pulsed dye laser on the expression of connective tissue growth factor in keloids. Lasers Surg. Med. 2012, 44, 377–383. [Google Scholar] [CrossRef]
- Zhibo, X.; Miaobo, Z. Molecular mechanism of pulsed-dye laser in treatment of keloids: An in vitro study. Adv. Skin Wound Care 2010, 23, 29–33. [Google Scholar] [CrossRef]
- Lv, K.; Xia, Z.; Chinese Consensus Panel on the Prevention and Treatment of Scars. Chinese expert consensus on clinical prevention and treatment of scar+. Burn. Trauma 2018, 6, 27. [Google Scholar] [CrossRef]
- Sobanko, J.F.; Vachiramon, V.; Rattanaumpawan, P.; Miller, C.J. Early postoperative single treatment ablative fractional lasing of Mohs micrographic surgery facial scars: A split-scar, evaluator-blinded study. Lasers Surg. Med. 2015, 47, 1–5. [Google Scholar] [CrossRef]
- Shin, H.W.; Suk, S.; Chae, S.W.; Yoon, K.C.; Kim, J. Early postoperative treatment of mastectomy scars using a fractional carbon dioxide laser: A randomized, controlled, split-scar, blinded study. Arch. Plast. Surg. 2021, 48, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Zheng, Z.; Roh, M.R. Early Postoperative Treatment of Surgical Scars Using a Fractional Carbon Dioxide Laser: A Split-Scar, Evaluator-Blinded Study. Dermatol. Surg. 2013, 39, 1190–1196. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Ryu, H.J.; Choi, J.E.; Ahn, H.H.; Kye, Y.C.; Seo, S.H. A Comparison of the Scar Prevention Effect between Carbon Dioxide Fractional Laser and Pulsed Dye Laser in Surgical Scars. Dermatol. Surg. 2014, 40, 973–978. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.-J.; Liu, W.-H.; Fang, S.-W.; Zhou, X.-L.; Xu, J.-X.; Li, G.-S. Lasers and Intense Pulsed Light for the Treatment of Pathological Scars: A Network Meta-Analysis. Aesthetic Surg. J. 2022, 42, NP675–NP687. [Google Scholar] [CrossRef]
- Brewin, M.P.; Lister, T.S. Prevention or treatment of hypertrophic burn scarring: A review of when and how to treat with the Pulsed Dye Laser. Burns 2014, 40, 797–804. [Google Scholar] [CrossRef]
- Leszczynski, R.; da Silva, C.A.; Pinto, A.; Kuczynski, U.; da Silva, E.M. Laser therapy for treating hypertrophic and keloid scars. Cochrane Database Syst. Rev. 2022, 9, CD011642. [Google Scholar] [CrossRef]
- Seago, M.; Shumaker, P.R.; Spring, L.K.; Alam, M.; Al-Niaimi, F.; Anderson, R.R.; Artzi, O.; Bayat, A.; Cassuto, D.; Chan, H.H.; et al. Laser Treatment of Traumatic Scars and Contractures: 2020 International Consensus Recommendations. Lasers Surg. Med. 2020, 52, 96–116. [Google Scholar] [CrossRef]
- Mosca, R.C.; Ong, A.A.; Albasha, O.; Bass, K.; Arany, P. Photobiomodulation Therapy for Wound Care: A Potent, Noninvasive, Photoceutical Approach. Adv. Ski. Wound Care 2019, 32, 157–167. [Google Scholar] [CrossRef]
- Calabrese, E.J.; Dhawan, G.; Kapoor, R.; Agathokleous, E.; Calabrese, V. Hormesis: Wound healing and fibroblasts. Pharmacol. Res. 2022, 184, 106449. [Google Scholar] [CrossRef]
- Tatmatsu-Rocha, J.C.; Ferraresi, C.; Hamblin, M.R.; Maia, F.D.; do Nascimento, N.R.; Driusso, P.; Parizotto, N. Low-level laser therapy (904 nm) can increase collagen and reduce oxidative and nitrosative stress in diabetic wounded mouse skin. J. Photochem. Photobiol. B Biol. 2016, 164, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Sperandio, F.F.; Simões, A.; Corrêa, L.; Aranha, A.C.C.; Giudice, F.S.; Hamblin, M.R.; Sousa, S.C. Low-level laser irradiation promotes the proliferation and maturation of keratinocytes during epithelial wound repair. J. Biophotonics 2014, 8, 795–803. [Google Scholar] [CrossRef] [PubMed]
- Calabrese, E.J.; Dhawan, G.; Kapoor, R.; Agathokleous, E.; Calabrese, V. Hormesis: Wound healing and keratinocytes. Pharmacol. Res. 2022, 183, 106393. [Google Scholar] [CrossRef] [PubMed]
- Heiskanen, V.; Hamblin, M.R. Photobiomodulation: Lasers vs. light emitting diodes? Photochem. Photobiol. Sci. 2018, 17, 1003–1017. [Google Scholar] [CrossRef] [PubMed]
- Vitse, J.; Bekara, F.; Byun, S.; Herlin, C.; Teot, L. A Double-Blind, Placebo-Controlled Randomized Evaluation of the Effect of Low-Level Laser Therapy on Venous Leg Ulcers. Int. J. Low. Extremity Wounds 2017, 16, 29–35. [Google Scholar] [CrossRef]
- Taradaj, J.; Halski, T.; Kucharzewski, M.; Urbanek, T.; Halska, U.; Kucio, C. Effect of Laser Irradiation at Different Wavelengths (940, 808, and 658 nm) on Pressure Ulcer Healing: Results from a Clinical Study. Evid. Based Complement. Altern. Med. 2013, 2013, 960240. [Google Scholar] [CrossRef]
- Barolet, D.; Boucher, A. Prophylactic low-level light therapy for the treatment of hypertrophic scars and keloids: A case series. Lasers Surg. Med. 2010, 42, 597–601. [Google Scholar] [CrossRef]
- Akasaki, I. Blue Light: A Fascinating Journey (Nobel Lecture). Angew. Chem. Int. Ed. Engl. 2015, 54, 7750–7763. [Google Scholar] [CrossRef]
- Dini, V.; Romanelli, M.; Oranges, T.; Davini, G.; Janowska, A. Blue light emission in the management of hard-to-heal wounds. G. Ital. Dermatol. E Venereol. 2021, 156, 703–713. [Google Scholar] [CrossRef]
- Ngoc, L.T.N.; Moon, J.Y.; Lee, Y.C. Utilization of light-emitting diodes for skin therapy: Systematic review and meta-analysis. Photodermatol. Photoimmunol. Photomed. 2022. [Google Scholar] [CrossRef]
- Morton, C.A.; Szeimies, R.M.; Basset-Seguin, N.; Calzavara-Pinton, P.; Gilaberte, Y.; Haedersdal, M.; Hofbauer, G.F.L.; Hunger, R.E.; Karrer, S.; Piaserico, S.; et al. European Dermatology Forum guidelines on topical photodynamic therapy 2019 Part 1: Treatment delivery and established indications—Actinic keratoses, Bowen’s disease and basal cell carcinomas. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 2225–2238. [Google Scholar] [CrossRef] [PubMed]
- Oyama, J.; Ramos-Milaré, Á.C.F.H.; Lera-Nonose, D.S.S.L.; Nesi-Reis, V.; Demarchi, I.G.; Aristides, S.M.A.; Teixeira, J.J.V.; Silveira, T.G.V.; Lonardoni, M.V.C. Photodynamic therapy in wound healing in vivo: A systematic review. Photodiagnosis Photodyn. Ther. 2020, 30, 101682. [Google Scholar] [CrossRef]
- Nesi-Reis, V.; Lera-Nonose, D.; Oyama, J.; Silva-Lalucci, M.P.P.; Demarchi, I.G.; Aristides, S.M.A.; Teixeira, J.J.V.; Silveira, T.G.V.; Lonardoni, M.V.C. Contribution of photodynamic therapy in wound healing: A systematic review. Photodiagnosis Photodyn. Ther. 2017, 21, 294–305. [Google Scholar] [CrossRef] [PubMed]
- Kang, K.; Bacci, S. Photodynamic Therapy. Biomedicines 2022, 10, 2701. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Guarino, M.; García-Morales, I.; Harto, A.; Montull, C.; Pérez-García, B.; Jaén, P. Photodynamic Therapy: New Indications. Actas Dermo-Sifiliográficas Engl. Ed. 2007, 98, 377–395. [Google Scholar] [CrossRef]
- Li, L.; Yang, Y.; Yang, Z.; Zheng, M.; Luo, G.; He, W.; Yin, R. Effects of ALA-PDT on the macrophages in wound healing and its related mechanisms in vivo and in vitro. Photodiagnosis Photodyn. Ther. 2022, 38, 102816. [Google Scholar] [CrossRef]
- Choi, J.Y.; Park, G.T.; Na, E.Y.; Wi, H.S.; Lee, S.-C.; Lee, J.-B. Molecular changes following topical photodynamic therapy using methyl aminolaevulinate in mouse skin. J. Dermatol. Sci. 2010, 58, 198–203. [Google Scholar] [CrossRef]
- Mroz, P.; Hamblin, M.R. The immunosuppressive side of PDT. Photochem. Photobiol. Sci. 2011, 10, 751–758. [Google Scholar] [CrossRef]
- Khorsandi, K.; Hosseinzadeh, R.; Esfahani, H.; Zandsalimi, K.; Shahidi, F.K.; Abrahamse, H. Accelerating skin regeneration and wound healing by controlled ROS from photodynamic treatment. Inflamm. Regen. 2022, 42, 40. [Google Scholar] [CrossRef]
- de Oliveira, A.B.; Ferrisse, T.M.; Fontana, C.R.; Basso, F.G.; Brighenti, F.L. Photodynamic therapy for treating infected skin wounds: A systematic review and meta-analysis from randomized clinical trials. Photodiagnosis Photodyn Ther. 2022, 40, 103118. [Google Scholar] [CrossRef]
- Rajendran, S.B.; Challen, K.; Wright, K.L.; Hardy, J.G. Electrical Stimulation to Enhance Wound Healing. J. Funct. Biomater. 2021, 12, 40. [Google Scholar] [CrossRef] [PubMed]
- Ud-Din, S.; Bayat, A. Electrical Stimulation and Cutaneous Wound Healing: A Review of Clinical Evidence. Healthcare 2014, 2, 445–467. [Google Scholar] [CrossRef] [PubMed]
- Koel, G.; Houghton, P.E. Electrostimulation: Current Status, Strength of Evidence Guidelines, and Meta-Analysis. Adv. Wound Care 2014, 3, 118–126. [Google Scholar] [CrossRef] [PubMed]
- Cullum, N.; Nelson, E.A.; Flemming, K.; Sheldon, T. Systematic reviews of wound care management: (5) beds; (6) compression; (7) laser therapy, therapeutic ultrasound, electrotherapy and electromagnetic therapy. Health Technol. Assess. 2001, 5, 9. [Google Scholar] [CrossRef] [PubMed]
- Beheshti, A.; Shafigh, Y.; Parsa, H.; Zangivand, A.A. Comparison of High-Frequency and MIST Ultrasound Therapy for the Healing of Venous Leg Ulcers. Adv. Clin. Exp. Med. 2014, 23, 969–975. [Google Scholar] [CrossRef] [PubMed]
- Cullum, N.; Liu, Z. Therapeutic ultrasound for venous leg ulcers. Cochrane Database Syst. Rev. 2017, 5, CD001180. [Google Scholar] [CrossRef]
- Guerriero, F.; Botarelli, E.; Mele, G.; Polo, L.; Zoncu, D.; Renati, P.; Sgarlata, C.; Rollone, M.; Ricevuti, G.; Maurizi, N.; et al. Effectiveness of an Innovative Pulsed Electromagnetic Fields Stimulation in Healing of Untreatable Skin Ulcers in the Frail Elderly: Two Case Reports. Case Rep. Dermatol. Med. 2015, 2015, 576580. [Google Scholar] [CrossRef]
- Kwan, R.L.; Wong, W.C.; Yip, S.L.; Chan, K.L.; Zheng, Y.P.; Cheing, G.L. Pulsed electromagnetic field therapy promotes healing and microcirculation of chronic diabetic foot ulcers: A pilot study. Adv. Skin Wound Care 2015, 28, 212–219. [Google Scholar] [CrossRef]
- Romanelli, M.; Piaggesi, A.; Scapagnini, G.; Dini, V.; Janowska, A.; Iacopi, E.; Scarpa, C.; Fauverghe, S.; Bassetto, F.; EUREKA Study Group. Evaluation of fluorescence biomodulation in the real-life management of chronic wounds: The EUREKA trial. J. Wound Care 2018, 27, 744–753. [Google Scholar] [CrossRef]
- Taha, M.M.; El-Nagar, M.M.; Elrefaey, B.H.; Elkholy, R.M.; Ali, O.I.; Alkhamees, N.; Felaya, E.-S.E.E.-S. Effect of Polarized Light Therapy (Bioptron) on Wound Healing and Microbiota in Diabetic Foot Ulcer: A Randomized Controlled Trial. Photobiomodulation Photomed. Laser Surg. 2022, 40, 792–799. [Google Scholar] [CrossRef]
- M. Allam, N.; Eladl, H.M.; Eid, M.M. Polarized Light Therapy in the Treatment of Wounds: A Review. Int. J. Low Extrem. Wounds 2022, 15347346221113991. [Google Scholar] [CrossRef] [PubMed]
- Feehan, J.; Burrows, S.P.; Cornelius, L.; Cook, A.M.; Mikkelsen, K.; Apostolopoulos, V.; Husaric, M.; Kiatos, D. Therapeutic applications of polarized light: Tissue healing and immunomodulatory effects. Maturitas 2018, 116, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Ekelem, C.; Thomas, L.; Van Hal, M.; Valdebran, M.; Lotfizadeh, A.; Mlynek, K.; Mesinkovska, N.A. Radiofrequency Therapy and Noncosmetic Cutaneous Conditions. Dermatol. Surg. 2019, 45, 908–930. [Google Scholar] [CrossRef]
- Cucu, C.; Butacu, A.; Niculae, B.D.; Tiplica, G.S. Benefits of fractional radiofrequency treatment in patients with atrophic acne scars—Literature review. J. Cosmet. Dermatol. 2021, 20, 381–385. [Google Scholar] [CrossRef] [PubMed]
- Zhou, K.; Krug, K.; Stachura, J.; Niewczyk, P.; Ross, M.; Tutuska, J.; Ford, G. Silver-Collagen Dressing and High-voltage, Pulsed-current Therapy for the Treatment of Chronic Full-thickness Wounds: A Case Series. J. Wound Ostomy Cont. Nurs. 2016, 62, 36–44. [Google Scholar]
- Fraccalvieri, M.; Salomone, M.; Zingarelli, E.M.; Rivarossa, F.; Bruschi, S. Electrical stimulation for difficult wounds: Only an alternative procedure? Int. Wound J. 2015, 12, 669–673. [Google Scholar] [CrossRef]
- Mohajeri-Tehrani, M.R.; Nasiripoor, F.; Torkaman, G.; Hedayati, M.; Annabestani, Z.; Asadi, M.R. Effect of low-intensity direct current on expression of vascular endothelial growth factor and nitric oxide in diabetic foot ulcers. J. Rehabil. Res. Dev. 2014, 51, 815–824. [Google Scholar] [CrossRef]
- Bora Karsli, P.; Gurcay, E.; Karaahmet, O.Z.; Cakci, A. High-Voltage Electrical Stimulation Versus Ultrasound in the Treatment of Pressure Ulcers. Adv. Skin Wound Care 2017, 30, 565–570. [Google Scholar] [CrossRef]
- Polak, A.; Taradaj, J.; Nawrat-Szoltysik, A.; Stania, M.; Dolibog, P.; Blaszczak, E.; Zarzeczny, R.; Juras, G.; Franek, A.; Kucio, C. Reduction of pressure ulcer size with high-voltage pulsed current and high-frequency ultrasound: A randomised trial. J. Wound Care 2016, 25, 742–754. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Keloids | Hypertrophic Scars |
|---|---|---|
| Trauma | Non-severe (acne, folliculitis) | Burns, incision |
| Body sites | Chest, upper back, earlobe | Any |
| Symptoms | Erythema, itch, pain | Erythema, itch |
| Exploration | Beyond the limit of the trauma | Limited to the initial wound |
| Treatment | Combined therapies with frequent recurrence | Good response |
| Surgical excision | Contraindicated due to recurrence | Without recurrences, could be considered a treatment |
| Wound | Cellular Mechanisms | Mediators |
|---|---|---|
| Inflammation Exudates Infection | Neutrophils’ excessive number and function Defective macrophages High number of mast cells Loss of microbiome diversity | Oxidative stress Wound proteases (MMPs, elastase, cathepsin G, and urokinase-type plasminogen activator (uPA)) Increase in inflammatory cytokines |
| Hyperkeratotic edge of the wound | Keratinocyte hyperproliferation and malfunction | Elevated b-catenin and c-myc |
| Failure to heal and close | Senescent fibroblasts | Degradation of VEGF, TGF-beta, and TNF-alfa |
| Prevention | Treatment | Alternative Therapies |
|---|---|---|
| Early diagnosis | Silicone gel or dressing Topical retinoids | Peelings |
| Careful wound care | Topical Imiquimod Topical 5-Fluorouracil Intralesional Bleomicin | Microneedling Dermabrasion Radiotherapy |
| Prevent infection | ||
| Sun protection Avoid risk areas if possible Avoid risk patients if possible |
| Skin Alteration | Type of Laser |
|---|---|
| Erythema | Pulsed dye laser Intense pulsed light Neodimio-Yag laser |
| Skin thickness/Hypertrophic | Erbio laser CO2 laser Non-ablative laser |
| Hyperpigmentation | Alejandrita laser Intense pulsed light KTP 532 nm Q-switched laser |
| Effect | Mediator | Phase of WH/CW |
|---|---|---|
| Anti-inflammatory | ROS, NO, IL | Inflammation |
| Vasodilatation | NO | Proliferation |
| Matrix formation | TGF-beta and MMPs | Proliferation and remodeling |
| Promote epithelial cell function | Cyclin D1 | Proliferation and remodeling |
| Group of Photosensitizers | Molecule | Light Sources (570–800 nm) | Protocol |
|---|---|---|---|
| Hematoporphyrin derivates | Photofrin® | LED (red and NIR) | 37–100 J/cm2/session |
| PpIX precursors | ALA, MAL | Laser (Vascular and Diode) | |
| Clorins | Foscan® (mTHPC) | 1–2 sessions/week/1 month |
| Effect | Mediator | Phase of Wound Healing |
|---|---|---|
| Activation/suppression of the immune system | TNF-alfa IL1, IL6, IL10 | Inflammation |
| Antibacterial activity | ROS | Chronic inflammation |
| Reepithelization, matrix formation | MMPs | Regeneration and remodeling |
| Neovascularization | VEGF | Regeneration and remodeling |
| Effect | Mediator | Phase of WH/CW |
|---|---|---|
| Angiogenesis | VEGF | Proliferation |
| Fibroblast proliferation | FGF | Proliferation and remodeling |
| Reduces bacterial colonization | PH alteration | Persistent inflammation and risk of infection |
| Modality | Type of Wound | Not yet Studied/Not Beneficial |
|---|---|---|
| Pulsed current Electrodes around the wound From 30 min to hours | Acute current in CW | |
| From 5 to 7 days a week | DU | Scarring prevention or treatment |
| After 2–5 days of the injury | LU |
| Modality | Type of Wound | Not yet Studied/Not Beneficial |
|---|---|---|
| LFU Around the wound | LU | HFU Contraindicated metal prosthesis, infection, or neuropathy |
| From 5 to 10 min Repeated sessions in a week | Prevent or treat keloids or HS | |
| After 2–5 days of the injury |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-Guarino, M.; Bacci, S.; Pérez González, L.A.; Bermejo-Martínez, M.; Cecilia-Matilla, A.; Hernández-Bule, M.L. The Role of Physical Therapies in Wound Healing and Assisted Scarring. Int. J. Mol. Sci. 2023, 24, 7487. https://doi.org/10.3390/ijms24087487
Fernández-Guarino M, Bacci S, Pérez González LA, Bermejo-Martínez M, Cecilia-Matilla A, Hernández-Bule ML. The Role of Physical Therapies in Wound Healing and Assisted Scarring. International Journal of Molecular Sciences. 2023; 24(8):7487. https://doi.org/10.3390/ijms24087487
Chicago/Turabian StyleFernández-Guarino, Montserrat, Stefano Bacci, Luis Alfonso Pérez González, Mariano Bermejo-Martínez, Almudena Cecilia-Matilla, and Maria Luisa Hernández-Bule. 2023. "The Role of Physical Therapies in Wound Healing and Assisted Scarring" International Journal of Molecular Sciences 24, no. 8: 7487. https://doi.org/10.3390/ijms24087487
APA StyleFernández-Guarino, M., Bacci, S., Pérez González, L. A., Bermejo-Martínez, M., Cecilia-Matilla, A., & Hernández-Bule, M. L. (2023). The Role of Physical Therapies in Wound Healing and Assisted Scarring. International Journal of Molecular Sciences, 24(8), 7487. https://doi.org/10.3390/ijms24087487