
Can Ashwagandha Benefit the Endocrine System?—A Review

 , , and
, , and 
Abstract
:1. Introduction
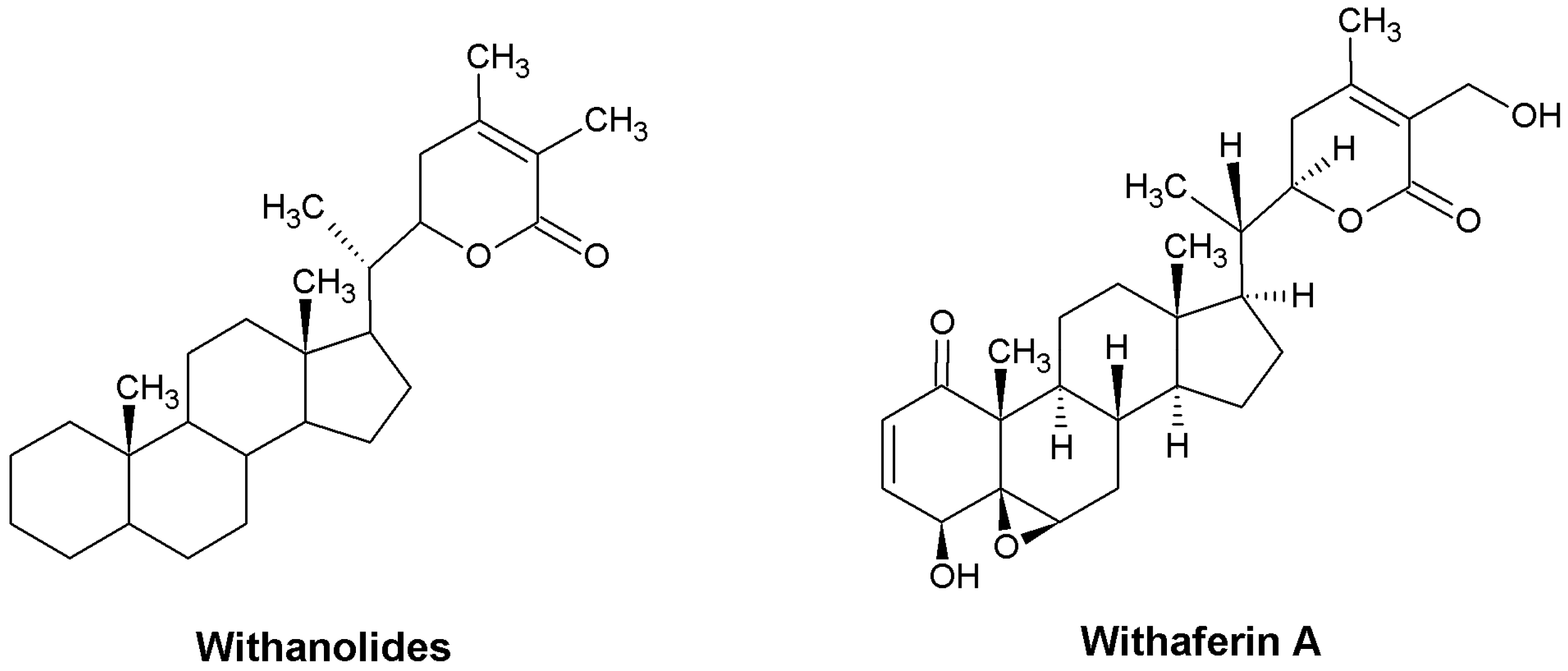
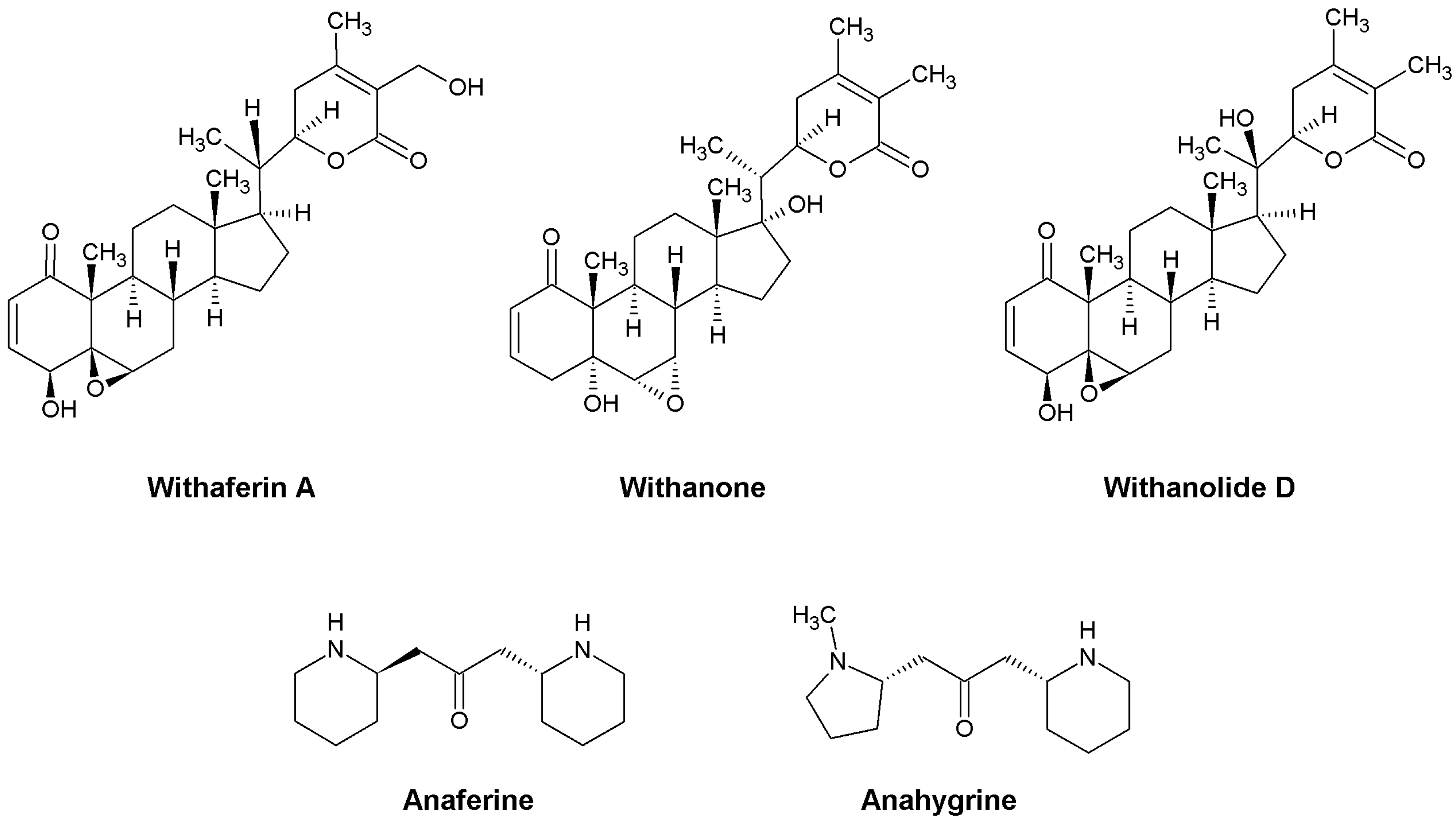
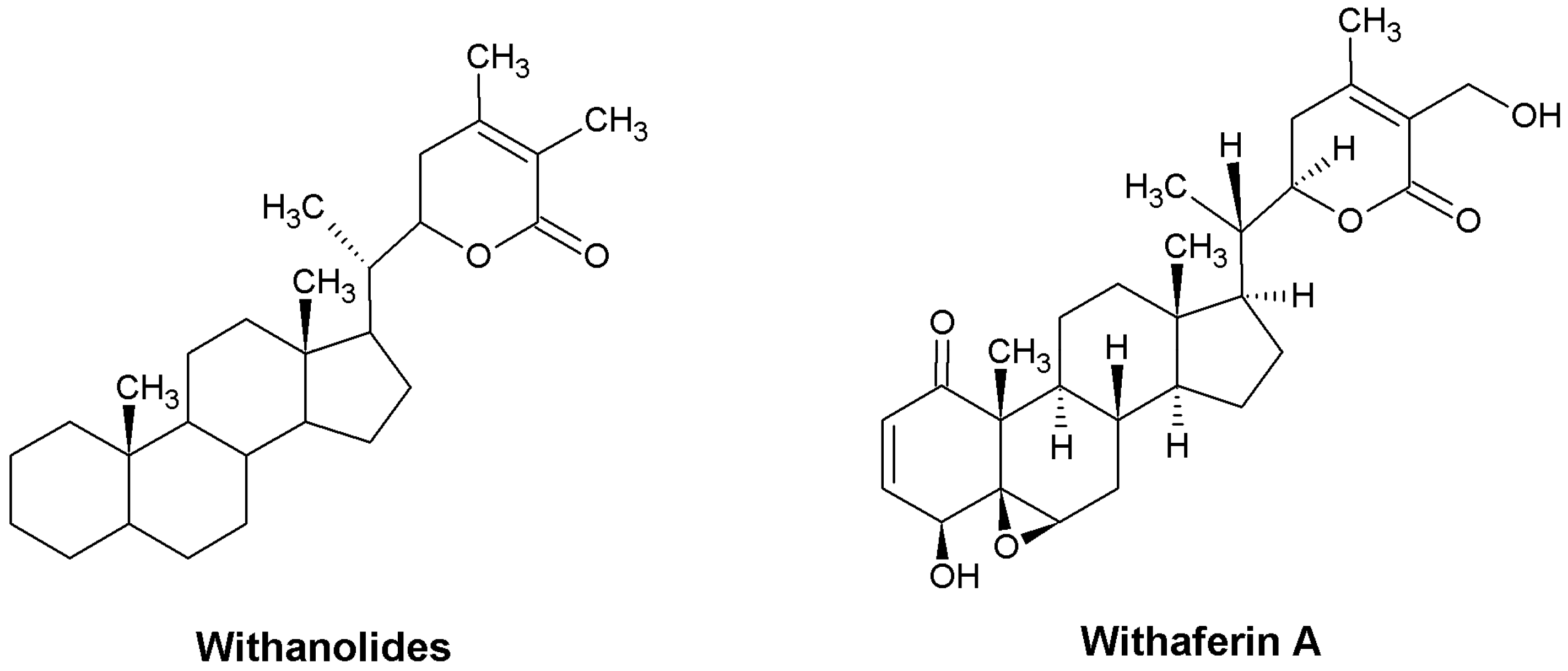
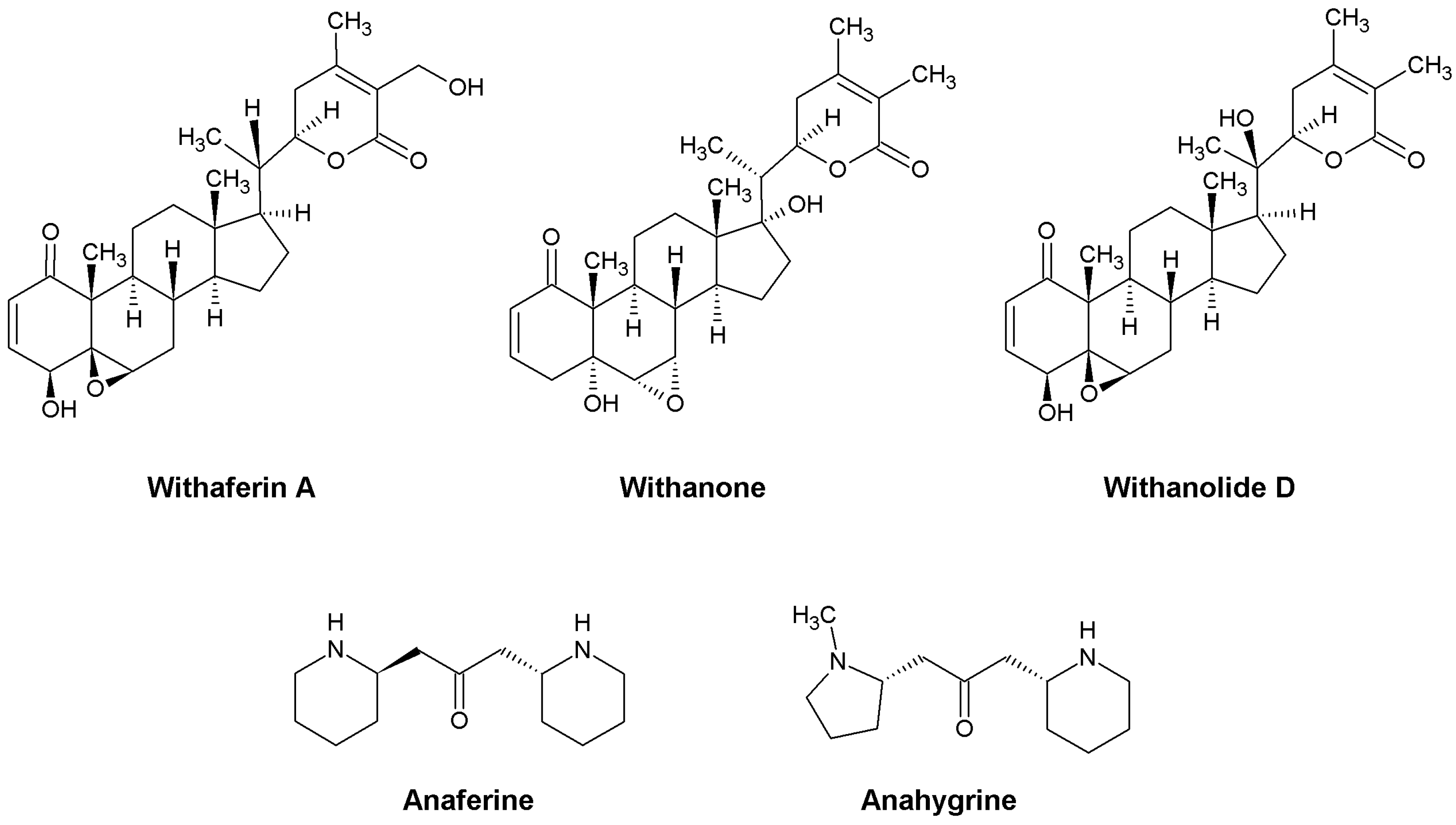
2. Ashwagandha’s Active Substances and Their Biological Effects
3. Methodology
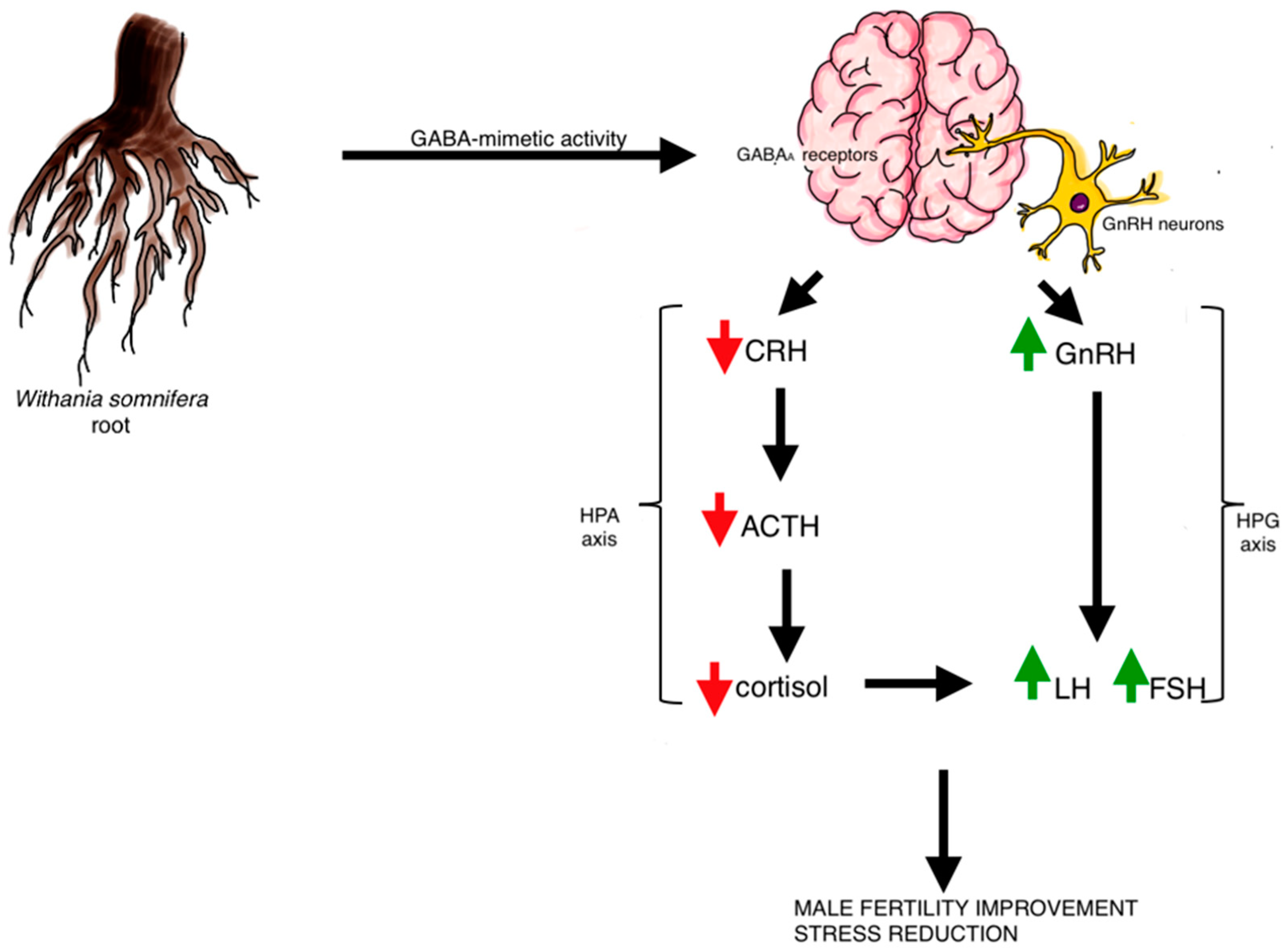
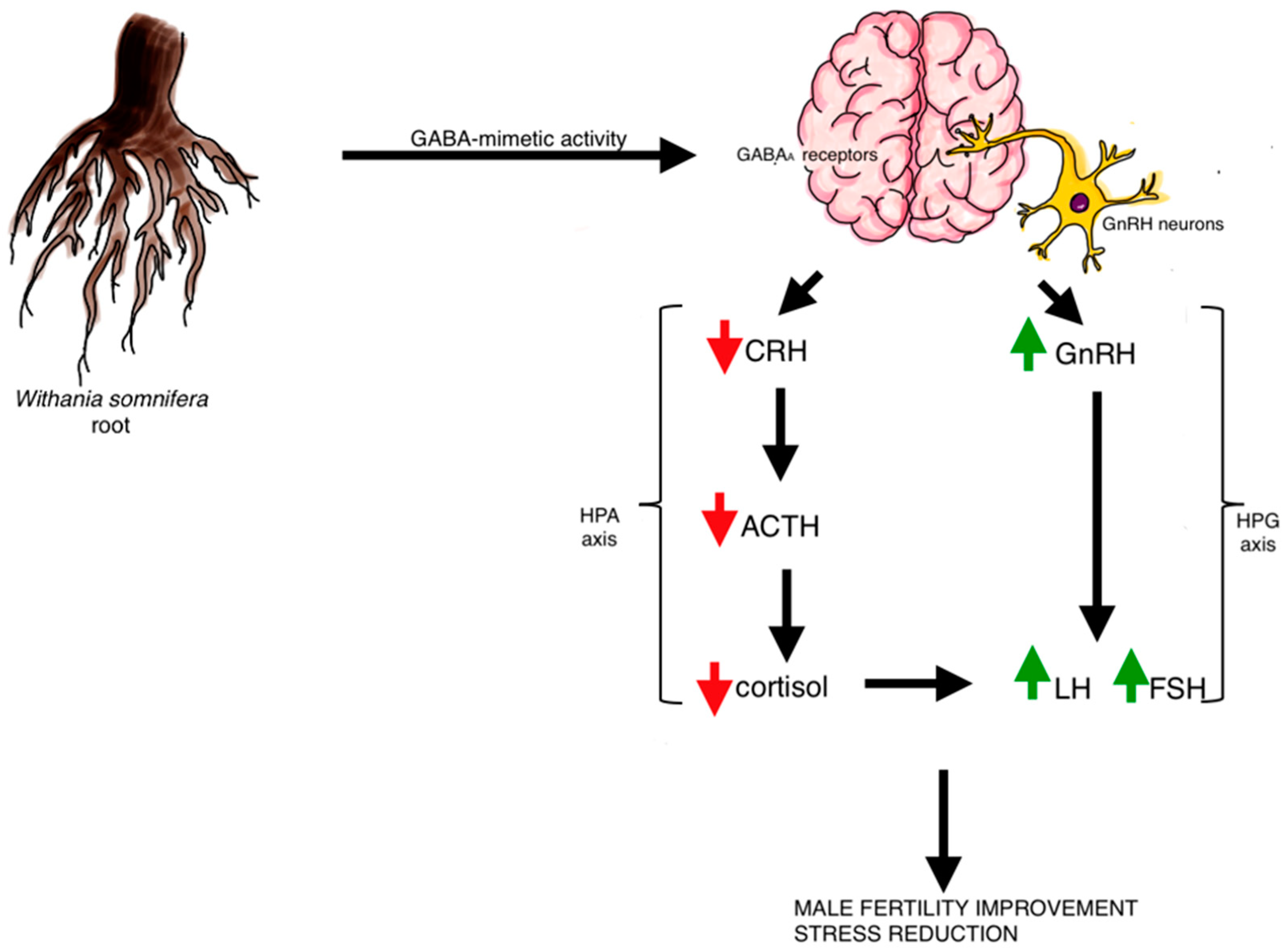
4. Regulating Hypothalamus, Pituitary Gland and Their Axis by Ashwagandha
5. Ashwagandha’s Impact on the Reproductive System
6. Ashwagandha and Thyroid Gland Dysfunctions
7. Limitations
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Paul, S.; Chakraborty, S.; Anand, U.; Dey, S.; Nandy, S.; Ghorai, M.; Saha, S.C.; Patil, M.T.; Kandimalla, R.; Proćków, J.; et al. Withania somnifera (L.) Dunal (Ashwagandha): A comprehensive review on ethnopharmacology, pharmacotherapeutics, biomedicinal and toxicological aspects. Biomed. Pharmacother. 2021, 143, 112175. [Google Scholar] [CrossRef] [PubMed]
- Mikulska, P.; Malinowska, M.; Ignacyk, M.; Szustowski, P.; Nowak, J.; Pesta, K.; Szeląg, M.; Szklanny, D.; Judasz, E.; Kaczmarek, G.; et al. Ashwagandha (Withania somnifera)—Current Research on the Health-Promoting Activities: A Narrative Review. Pharmaceutics 2023, 15, 1057. [Google Scholar] [CrossRef] [PubMed]
- Saleem, S.; Muhammad, G.; Hussain, M.A.; Altaf, M.; Abbas Bukhari, S.N. Withania somnifera L.: Insights into the phytochemical profile, therapeutic potential, clinical trials, and future prospective. Iran. J. Basic Med. Sci. 2020, 23, 1501. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, P.K.; Banerjee, S.; Biswas, S.; Das, B.; Kar, A.; Katiyar, C.K. Withania somnifera (L.) Dunal—Modern perspectives of an ancient Rasayana from Ayurveda. J. Ethnopharmacol. 2021, 264, 113157. [Google Scholar] [CrossRef]
- de la Peña, I.; Afable, T.; Dahilig-Talan, V.R.; Cruz, P. Review of Plant Extracts and Active Components: Mechanisms of Action for the Treatment of Obesity-Induced Cognitive Impairment. Brain Sci. 2023, 13, 929. [Google Scholar] [CrossRef]
- Siddharth, S.; Muniraj, N.; Saxena, N.K.; Sharma, D. Concomitant Inhibition of Cytoprotective Autophagy Augments the Efficacy of Withaferin A in Hepatocellular Carcinoma. Cancers 2019, 11, 453. [Google Scholar] [CrossRef]
- Gregory, J.; Vengalasetti, Y.V.; Bredesen, D.E.; Rao, R.V. Neuroprotective Herbs for the Management of Alzheimer’s Disease. Biomolecules 2021, 11, 543. [Google Scholar] [CrossRef]
- Dar, N.J.; Ahmad, M. Neurodegenerative diseases and Withania somnifera (L.): An update. J. Ethnopharmacol. 2020, 256, 112769. [Google Scholar] [CrossRef]
- Chengappa, K.N.R.; Brar, J.S.; Gannon, J.M.; Schlicht, P.J. Adjunctive use of a standardized extract of withania somnifera (ashwagandha) to treat symptom exacerbation in schizophrenia: A randomized, double-blind, placebo-controlled study. J. Clin. Psychiatry 2018, 79, 17m11826. [Google Scholar] [CrossRef]
- Ahmed, I.; Dubey, R.B.; Jain, D.; El-Sheikh, M.A.; Kaushik, P. Heterosis Studies for Root-Yield-Attributing Characters and Total Alkaloid Content over Different Environments in Withania somnifera L. Agriculture 2023, 13, 1025. [Google Scholar] [CrossRef]
- Singh, M.; Jayant, K.; Singh, D.; Bhutani, S.; Poddar, N.K.; Chaudhary, A.A.; Khan, S.-U.; Adnan, M.; Siddiqui, A.J.; Hassan, I.; et al. Withania somnifera (L.) Dunal (Ashwagandha) for the possible therapeutics and clinical management of SARS-CoV-2 infection: Plant-based drug discovery and targeted therapy. Front. Cell. Infect. Microbiol. 2022, 12, 933824. [Google Scholar] [CrossRef] [PubMed]
- Sengupta, P.; Agarwal, A.; Pogrebetskaya, M.; Roychoudhury, S.; Durairajanayagam, D.; Henkel, R. Role of Withania somnifera (Ashwagandha) in the management of male infertility. Reprod. Biomed. Online 2018, 36, 311–326. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.K.; Basu, I.; Singh, S. Efficacy and Safety of Ashwagandha Root Extract in Subclinical Hypothyroid Patients: A Double-Blind, Randomized Placebo-Controlled Trial. J. Altern. Complement. Med. 2018, 24, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Ajgaonkar, A.; Jain, M.; Debnath, K. Efficacy and Safety of Ashwagandha (Withania somnifera) Root Extract for Improvement of Sexual Health in Healthy Women: A Prospective, Randomized, Placebo-Controlled Study. Cureus 2022, 14, e30787. [Google Scholar] [CrossRef] [PubMed]
- Ramli, S.; Wu, Y.S.; Batumalaie, K.; Mac Guad, R.; Choy, K.W.; Kumar, A.; Gopinath, S.C.B.; Sarker, M.R.; Subramaniyan, V.; Sekar, M.; et al. Phytochemicals of Withania somnifera as a Future Promising Drug against SARS-CoV-2: Pharmacological Role, Molecular Mechanism, Molecular Docking Evaluation, and Efficient Delivery. Microorganisms 2023, 11, 1000. [Google Scholar] [CrossRef] [PubMed]
- Lopresti, A.L.; Smith, S.J.; Malvi, H.; Kodgule, R. An investigation into the stress-relieving and pharmacological actions of an ashwagandha (Withania somnifera) extract: A randomized, double-blind, placebo-controlled study. Medicine 2019, 98, e17186. [Google Scholar] [CrossRef]
- Balkrishna, A.; Nain, P.; Chauhan, A.; Sharma, N.; Gupta, A.; Ranjan, R.; Varshney, A. Super Critical Fluid Extracted Fatty Acids from Withania somnifera Seeds Repair Psoriasis-Like Skin Lesions and Attenuate Pro-Inflammatory Cytokines (TNF-α and IL-6) Release. Biomolecules 2020, 10, 185. [Google Scholar] [CrossRef]
- Lee, D.; Yu, J.S.; Ha, J.W.; Lee, S.R.; Lee, B.S.; Kim, J.-C.; Kim, J.K.; Kang, K.S.; Kim, K.H. Antitumor Potential of Withanolide Glycosides from Ashwagandha (Withania somnifera) on Apoptosis of Human Hepatocellular Carcinoma Cells and Tube Formation in Human Umbilical Vein Endothelial Cells. Antioxidants 2022, 11, 1761. [Google Scholar] [CrossRef]
- Malik, V.; Kumar, V.; Kaul, S.C.; Wadhwa, R.; Sundar, D. Potential of Withaferin-A, Withanone and Caffeic Acid Phenethyl ester as ATP-competitive inhibitors of BRAF: A bioinformatics study. Curr. Res. Struct. Biol. 2021, 3, 301–311. [Google Scholar] [CrossRef]
- Singh, N.; Yadav, S.S.; Rao, A.S.; Nandal, A.; Kumar, S.; Ganaie, S.A.; Narasihman, B. Review on anticancerous therapeutic potential of Withania somnifera (L.) Dunal. J. Ethnopharmacol. 2021, 270, 113704. [Google Scholar] [CrossRef]
- Speers, A.B.; Cabey, K.A.; Soumyanath, A.; Wright, K.M. Effects of Withania somnifera (Ashwagandha) on Stress and the Stress- Related Neuropsychiatric Disorders Anxiety, Depression, and Insomnia. Curr. Neuropharmacol. 2021, 19, 1468–1495. [Google Scholar] [CrossRef] [PubMed]
- Gaurav, H.; Yadav, D.; Maurya, A.; Yadav, H.; Yadav, R.; Shukla, A.C.; Sharma, M.; Gupta, V.K.; Palazon, J. Biodiversity, Biochemical Profiling, and Pharmaco-Commercial Applications of Withania somnifera: A Review. Molecules 2023, 28, 1208. [Google Scholar] [CrossRef] [PubMed]
- Polumackanycz, M.; Petropoulos, S.A.; Śledziński, T.; Goyke, E.; Konopacka, A.; Plenis, A.; Viapiana, A. Withania somnifera L.: Phenolic Compounds Composition and Biological Activity of Commercial Samples and Its Aqueous and Hydromethanolic Extracts. Antioxidants 2023, 12, 550. [Google Scholar] [CrossRef] [PubMed]
- Sultana, T.; Okla, M.K.; Ahmed, M.; Akhtar, N.; Al-Hashimi, A.; Abdelgawad, H.; Haq, I.-U. Withaferin A: From Ancient Remedy to Potential Drug Candidate. Molecules 2021, 26, 7696. [Google Scholar] [CrossRef]
- Behl, T.; Sharma, A.; Sharma, L.; Sehgal, A.; Zengin, G.; Brata, R.; Fratila, O.; Bungau, S. Exploring the Multifaceted Therapeutic Potential of Withaferin A and Its Derivatives. Biomedicines 2020, 8, 571. [Google Scholar] [CrossRef]
- Orrù, A.; Marchese, G.; Ruiu, S. Alkaloids in Withania somnifera (L.) Dunal Root Extract Contribute to Its Anti-Inflammatory Activity. Pharmacology 2023, 108, 301–307. [Google Scholar] [CrossRef]
- Gurushankar, K.; Rimac, H.; Nadezhda, P.; Grishina, M. Exploring the potential and identifying Withania somnifera alkaloids as novel dihydrofolate reductase (DHFR) inhibitors by the AlteQ method. J. Biomol. Struct. Dyn. 2023, 10, 1–14. [Google Scholar] [CrossRef]
- Kumar, G.; Patnaik, R. Exploring neuroprotective potential of Withania somnifera phytochemicals by inhibition of GluN2B-containing NMDA receptors: An in silico study. Med. Hypotheses 2016, 92, 35–43. [Google Scholar] [CrossRef]
- Pahal, S.; Gupta, A.; Choudhary, P.; Chaudhary, A.; Singh, S. Network pharmacological evaluation of Withania somnifera bioactive phytochemicals for identifying novel potential inhibitors against neurodegenerative disorder. J. Biomol. Struct. Dyn. 2022, 40, 10887–10898. [Google Scholar] [CrossRef]
- Shukla, R.; Pahal, S.; Gupta, A.; Choudhary, P.; Misra, K.; Singh, S. Modulation of GPCR receptors common to gut inflammatory diseases and neuronal disorders, Alzheimer’s and Parkinson’s diseases as druggable targets through Withania somnifera bioactives: An in silico study. J. Biomol. Struct. Dyn. 2023, 41, 4485–4503. [Google Scholar] [CrossRef]
- Grover, A.; Shandilya, A.; Punetha, A.; Bisaria, V.S.; Sundar, D. Inhibition of the NEMO/IKKβ association complex formation, a novel mechanism associated with the NF-κB activation suppression by Withania somnifera’s key metabolite withaferin A. BMC Genom. 2010, 11 (Suppl. S4), S25. [Google Scholar] [CrossRef] [PubMed]
- Saha, S.; Islam, M.K.; Shilpi, J.A.; Hasan, S. Inhibition of VEGF: A novel mechanism to control angiogenesis by Withania somnifera’s key metabolite Withaferin A. In Silico Pharmacol. 2013, 1, 11. [Google Scholar] [CrossRef] [PubMed]
- Zahiruddin, S.; Basist, P.; Parveen, A.; Parveen, R.; Khan, W.; Gaurav; Ahmad, S. Ashwagandha in brain disorders: A review of recent developments. J. Ethnopharmacol. 2020, 257, 112876. [Google Scholar] [CrossRef] [PubMed]
- Gaurav, I.; Singh, T.; Thakur, A.; Kumar, G.; Rathee, P.; Kumari, P.; Sweta, K. Synthesis, In-Vitro and In-Silico Evaluation of Silver Nanoparticles with Root Extract of Withania somnifera for Antibacterial Activity via Binding of Penicillin-Binding Protein-4. Curr. Pharm. Biotechnol. 2020, 21, 1674–1687. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, S.; Mallick, D.; Goswami, M.; Guengerich, F.P.; Chakrabarty, A.; Chowdhury, G. The Natural Products Withaferin A and Withanone from the Medicinal Herb Withania somnifera Are Covalent Inhibitors of the SARS-CoV-2 Main Protease. J. Nat. Prod. 2022, 85, 2340–2350. [Google Scholar] [CrossRef]
- Kumar, V.; Dhanjal, J.K.; Bhargava, P.; Kaul, A.; Wang, J.; Zhang, H.; Kaul, S.C.; Wadhwa, R.; Sundar, D. Withanone and Withaferin-A are predicted to interact with transmembrane protease serine 2 (TMPRSS2) and block entry of SARS-CoV-2 into cells. J. Biomol. Struct. Dyn. 2022, 40, 1–13. [Google Scholar] [CrossRef]
- Bungau, S.; Vesa, C.M.; Abid, A.; Behl, T.; Tit, D.M.; Purza, A.L.; Pasca, B.; Todan, L.M.; Endres, L. Withaferin A-A Promising Phytochemical Compound with Multiple Results in Dermatological Diseases. Molecules 2021, 26, 2407. [Google Scholar] [CrossRef]
- Björnsson, H.K.; Björnsson, E.S.; Avula, B.; Khan, I.A.; Jonasson, J.G.; Ghabril, M.; Hayashi, P.H.; Navarro, V. Ashwagandha-induced liver injury: A case series from Iceland and the US Drug-Induced Liver Injury Network. Liver Int. 2020, 40, 825–829. [Google Scholar] [CrossRef]
- Siddiqui, S.; Ahmed, N.; Goswami, M.; Chakrabarty, A.; Chowdhury, G. DNA damage by Withanone as a potential cause of liver toxicity observed for herbal products of Withania somnifera (Ashwagandha). Curr. Res. Toxicol. 2021, 2, 72–81. [Google Scholar] [CrossRef]
- Kataria, H.; Gupta, M.; Lakhman, S.; Kaur, G. Withania somnifera aqueous extract facilitates the expression and release of GnRH: In vitro and in vivo study. Neurochem. Int. 2015, 89, 111–119. [Google Scholar] [CrossRef]
- Bhattarai, J.P.; Park, S.A.; Han, S.K. The methanolic extract of Withania somnifera ACTS on GABAA receptors in gonadotropin releasing hormone (GnRH) neurons in mice. Phytother. Res. 2010, 24, 1147–1150. [Google Scholar] [CrossRef] [PubMed]
- Salve, J.; Pate, S.; Debnath, K.; Langade, D. Adaptogenic and Anxiolytic Effects of Ashwagandha Root Extract in Healthy Adults: A Double-blind, Randomized, Placebo-controlled Clinical Study. Cureus 2019, 11, e6466. [Google Scholar] [CrossRef] [PubMed]
- Mahdi, A.A.; Shukla, K.K.; Ahmad, M.K.; Rajender, S.; Shankhwar, S.N.; Singh, V.; Dalela, D. Withania somnifera Improves Semen Quality in Stress-Related Male Fertility. Evid. Based Complement. Altern. Med. 2011, 2011, 576962. [Google Scholar] [CrossRef] [PubMed]
- Priyanka, G.; Anil Kumar, B.; Lakshman, M.; Manvitha, V.; Kala Kumar, B. Adaptogenic and Immunomodulatory Activity of Ashwagandha Root Extract: An Experimental Study in an Equine Model. Front. Vet. Sci. 2020, 7, 541112. [Google Scholar] [CrossRef] [PubMed]
- Salem, H.M.; El-Saadony, M.T.; El-Mageed, T.A.A.; Soliman, S.M.; Khafaga, A.F.; Saad, A.M.; Swelum, A.A.; Korma, S.A.; Lima, C.M.G.; Selim, S.; et al. Promising prospective effects of Withania somnifera on broiler performance and carcass characteristics: A comprehensive review. Front. Vet. Sci. 2022, 9, 918961. [Google Scholar] [CrossRef]
- Shepherd, A.; Brunckhorst, O.; Ahmed, K.; Xu, Q. Botanicals in health and disease of the testis and male fertility: A scoping review. Phytomedicine 2022, 106, 154398. [Google Scholar] [CrossRef]
- Alfaro Gómez, M.; Fernández-Santos, M.D.R.; Jurado-Campos, A.; Soria-Meneses, P.J.; Montoro Angulo, V.; Soler, A.J.; Garde, J.J.; Rodríguez-Robledo, V. On Males, Antioxidants and Infertility (MOXI): Certitudes, Uncertainties and Trends. Antioxidants 2023, 12, 1626. [Google Scholar] [CrossRef]
- Leslie, S.W.; Soon-Sutton, T.L.; Khan, M.A.B. Male Infertility. 3 March 2023. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Chauhan, S.; Srivastava, M.K.; Pathak, A.K. Effect of standardized root extract of ashwagandha (Withania somnifera) on well-being and sexual performance in adult males: A randomized controlled trial. Health Sci. Rep. 2022, 5, e741. [Google Scholar] [CrossRef]
- Boroujeni, S.N.; Malamiri, F.A.; Bossaghzadeh, F.; Esmaeili, A.; Moudi, E. The most important medicinal plants affecting sperm and testosterone production: A systematic review. JBRA Assist. Reprod. 2022, 26, 522–530. [Google Scholar] [CrossRef]
- Baghel, K.; Srivastava, R. Photoperiod dependent expression of estrogen receptor alpha in testes of Japanese quail: Involvement of Withania somnifera in apoptosis amelioration. Biochem. Biophys. Res. Commun. 2021, 534, 957–965. [Google Scholar] [CrossRef]
- EMegahd, H.; MS Gabal, A. Evaluation of Matcha (Camellia sinensis) and Ashwagandha (Withania somnifera) Efficacy Against Utero-Ovarian Injury in Rats. Pak. J. Biol. Sci. 2021, 24, 1256–1268. [Google Scholar] [CrossRef] [PubMed]
- Gómez Afonso, A.; Fernandez-Lazaro, D.; Adams, D.P.; Monserdà-Vilaró, A.; Fernandez-Lazaro, C.I. Effects of Withania somnifera (Ashwagandha) on Hematological and Biochemical Markers, Hormonal Behavior, and Oxidant Response in Healthy Adults: A Systematic Review. Curr. Nutr. Rep. 2023, 12, 465–477. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.J.; Lopresti, A.L.; Teo, S.Y.M.; Fairchild, T.J. Examining the Effects of Herbs on Testosterone Concentrations in Men: A Systematic Review. Adv. Nutr. 2021, 12, 744–765. [Google Scholar] [CrossRef]
- Toufexis, D.; Rivarola, M.A.; Lara, H.; Viau, V. Stress and the reproductive axis. J. Neuroendocrinol. 2014, 26, 573–586. [Google Scholar] [CrossRef]
- Munir, N.; Mahmood, Z.; Shahid, M.; Afzal, M.N.; Jahangir, M.; Ali Shah, S.M.; Tahir, I.M.; Riaz, M.; Hussain, S.; Akram, M.; et al. Withania somnifera Chemical Constituents’ in vitro Antioxidant Potential and Their Response on Spermatozoa Parameters. Dose Response 2022, 20, 15593258221074936. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Wahhab, K.G.; Mourad, H.H.; Mannaa, F.A.; Morsy, F.A.; Hassan, L.K.; Taher, R.F. Role of ashwagandha methanolic extract in the regulation of thyroid profile in hypothyroidism modeled rats. Mol. Biol. Rep. 2019, 46, 3637–3649. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, N.; Diab, M.; Hassan, A.; Anwar, H.; Ragab, W.; Morsi, E.; Diab, M.; Boushra, A.; Sadek, N. The Ameliorating Effect of Ashwagandha (Withania somnifera) Extract on Hippocampus and Growth Plate Changes Associated with Propylthiouracil Induced Hypothyroidism in Juvenile Rats: Ashwagandha on Hippocampus and Growth Plate Changes Associated with hypothyroid rats. AL-Kindy Coll. Med. J. 2023, 19, 30–41. [Google Scholar] [CrossRef]
- Curry, K.M.; McNeil, L.E.; Flores, A.; Fuks, J. Thyrotoxicosis with Ashwagandha: A Case Report. SSRN, 23 December 2019. [Google Scholar] [CrossRef]
- Kamal, H.I.; Patel, K.; Brdak, A.; Heffernan, J.; Ahmad, N. Ashwagandha as a Unique Cause of Thyrotoxicosis Presenting with Supraventricular Tachycardia. Cureus 2022, 14, e23494. [Google Scholar] [CrossRef]
- Verma, N.; Gupta, S.K.; Tiwari, S.; Mishra, A.K. Safety of Ashwagandha Root Extract: A Randomized, Placebo-Controlled, study in Healthy Volunteers. Complement. Ther. Med. 2021, 57, 102642. [Google Scholar] [CrossRef]
- Philips, C.A.; Valsan, A.; Theruvath, A.H.; Ravindran, R.; Oommen, T.T.; Rajesh, S.; Bishnu, S.; Augustine, P.; on behalf of The Liver Research Club India. Ashwagandha-induced liver injury-A case series from India and literature review. Hepatol. Commun. 2023, 7, e0270. [Google Scholar] [CrossRef]
- Pires, N.; Gota, V.; Gulia, A.; Hingorani, L.; Agarwal, M.; Puri, A. Safety and pharmacokinetics of Withaferin-A in advanced stage high grade osteosarcoma: A phase I trial. J. Ayurveda Integr. Med. 2020, 11, 68–72. [Google Scholar] [CrossRef] [PubMed]
- Gopukumar, K.; Thanawala, S.; Somepalli, V.; Rao, T.S.S.; Thamatam, V.B.; Chauhan, S. Efficacy and Safety of Ashwagandha Root Extract on Cognitive Functions in Healthy, Stressed Adults: A Randomized, Double-Blind, Placebo-Controlled Study. Evid. Based Complement. Altern. Med. 2021, 2021, 8254344. [Google Scholar] [CrossRef] [PubMed]
- Joshi, V.K.; Joshi, A. Rational use of Ashwagandha in Ayurveda (Traditional Indian Medicine) for health and healing. J. Ethnopharmacol. 2021, 276, 114101. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Compounds | Part of W. Somnifera | Active Substances |
|---|---|---|
| Alkaloids | Leaves, roots, stems | Ashwagandhine, anahygrine, anaferine, pseudotropine, tropine, isopelletierine, [3]-tigloyloxtropine, tropeltigloate, dlisopelletierine, hygrine, mesoanaferine, choline, somniferine, withanine, withananine, hentriacontane, visamine, withasomnine, somniferinine, somninine, nicotine, cuscohygrine |
| Flavonoids | Roots, stems | Quercetin, 7-hydroxyflavone kaempferol |
| Glycosides | Roots, stems | Withanosides I–VII, withanamides |
| Phenolic | Roots, stems | Coumaric acid, caffeic acid, chlorogenic acid, gallic acid, ferulic acid, catechin |
| Saponins | Roots, berries | Sitoindoside VII, sitoindoside VIII |
| Steroids | Roots | β-sitosterol, cholesterol, diosgenin, ergostane, sitoindosides IX, X, stigmastadien, stigmasterol |
| Steroidal lactones | Leaves, roots | Withaferin–A, withanone, withasomidienone, withanolides A-Y, withasomniferine, withasomniferols A-C |
| Tannins | Roots, leaves, fruits, flowers | Not available |
| Active Substance | Potential Effects | References |
|---|---|---|
| Anaferine | anti-tuberculous, | [27] |
| neuroprotective | [28,33] | |
| Anahygrine | anti-tuberculous, | [27] |
| neuroprotective | [29,30] | |
| Withaferin A | anti-inflammatory, | [24] |
| anti-cancer, | [19,24,31,32] | |
| anti-diabetic, | [25] | |
| cardioprotective, | [25] | |
| neuroprotective, | [25,28,33] | |
| antibacterial, | [34] | |
| anti-SARS-CoV-2, | [35,36] | |
| in dermatological diseases | [37] | |
| Withanolide D | neuroprotective, | [28,33] |
| anti-cancer | [20] | |
| Withanone | antibacterial, | [34] |
| anti-SARS-CoV-2, | [35,36] | |
| anti-cancer | [19] |
| Authors | Characteristic of the Group | Ashwagandha Formulation Characteristics | Duration of the Observation | Results | References |
|---|---|---|---|---|---|
| Lopresti et al. | stressed healthy males and females 18–64 years old, with a HAM-A between 6 and 17 | 240 mg of Ashwagandha extract per day for 15–days, standarized contain 35% withanolide glycosides—approximately 84 mg withanolide; oral administraion | 60 days after commencement of 15-day capsule intake | ↓cortisol ↓DHEA-S ↑testosterone level in males - emotional improvement ↓anxiety measured in HAM-A score and DASS-21 | [16] |
| Salve J et al. | 60 participants (males and females), divided into three groups | one study group receiving 250 mg of Ashwagandha root extract per day; another study group receiving 600 mg of Ashwaganda extract per day; oral administraion | 8 weeks | ↓anxiety ↓cortisol - sleep improvement | [42] |
| Mahdi et al. | 121 men, 25–38 years. 60 men with unexplained infertility under environmental or constant mental stress in the study group, divided into three subgroups | 5 mg of Ashwagandha root powder for three months; oral administration | The patients were followed for partner’s pregnancy outcome for a period of 3 months after the treatment | ↑LH ↑testosterone ↑antioxidants ↓stress ↓cortisol | [43] |
| Priyanka G et al. | 24 healthy Kathiawari horses of either sex, 5–10 years old, divided into four groups: one control group and three experimental groups given varying dose of Ashwagandha | high-concentration full-spectrum Ashwagandha root powder, containing ≥5% of withanolides; experimental groups were given a varying dose of Ashwagandha (2.5 mg/animal, 5 mg/animal, and 10 mg/animal) with jiggery, respectively; oral administration | 21 days of intake, after 14 days of intake horses were subjected to different kind of stress | ↓cortisol ↓epinephrine ↑serotonine | [44] |
| Authors | Characteristic of the Group | Ashwagandha Formulation Characteristics | Duration of the Observation | Results | References |
|---|---|---|---|---|---|
| Baghel et al. | 18 sexually mature six weeks old male Japanese quail as a animal model of infertility, provoked by using photoperiodic chambers | 100 mg/day/kg of W. Somnifera root extract; oral administraion | few months of inducing infertility using photoperiodic chambers and 45 days of Ashwagandha administration | ↑expression of estrogen receptor alpha ↑estrogen ↓corticosterone | [51] |
| Megahd et al. | 50 adult female rats; model of H2O2-induced utero-ovarian oxidative injury and cell death, what caused reduction in serum level of FSH, LH, progesterone, and estrogen compared to a healthy control group | 200 mg/kg Ashwagandha tea extract; oral administraion | 1 month | ↑FSH ↑LH ↑progesterone ↑estrogen -significantly restored estrous cycle length | [52] |
| Ajgaonkar et al. | prospective, randomized, placebo-controlled study; 80 women, 18–50 years old, without any hormonal disturbances and having hypoactive sexual desire disorder (HSDD) with a Female Sexual Function Index (FSFI) score < 26, or Female Sexual Distress Scale (FSDS) score > 11 | 300 mg of standardized Ashwagandha root extract twice daily; oral administraion | 8 weeks | -improvement in sexual functions | [14] |
| Chauhan et al. | randomized, controlled trial; 50 healthy male subjects with low sexual desire | 300 mg of Ashwagandha root extract twice daily; oral administraion | 8 weeks | ↑testosterone -improvement of sexual functions measured by DISF-M | [49] |
| Authors | Characteristic of the Group | Ashwagandha Formulation Characteristics | Duration of the Observation | Results | References |
|---|---|---|---|---|---|
| Sharma et al. | males and females, 18–50 years old, with subclinical hypothyroidism | 300 mg of Ashwagandha root extract twice a day; oral administration | 8 weeks of treatment | ↑ T3 ↑ T4 ↓ TSH | [13] |
| Abdel-Wahhab et al. | male albino rats with induced hypothyroidism | 500 mg/kg/day of Ashwagandha methanolic extract; oral administraion | 30 days | ↑ T3 ↑ fT3 ↑ T4 ↑ fT4 ↓ TSH | [57] |
| Ibrahim et al. | male Wistar albino rats with induced hypothyroidism | 50 mg/kg/day of Ashwagandha extract; oral administraion | 30 days | ↑ T3 ↑ T4 ↓ TSH | [58] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wiciński, M.; Fajkiel-Madajczyk, A.; Kurant, Z.; Kurant, D.; Gryczka, K.; Falkowski, M.; Wiśniewska, M.; Słupski, M.; Ohla, J.; Zabrzyński, J. Can Ashwagandha Benefit the Endocrine System?—A Review. Int. J. Mol. Sci. 2023, 24, 16513. https://doi.org/10.3390/ijms242216513
Wiciński M, Fajkiel-Madajczyk A, Kurant Z, Kurant D, Gryczka K, Falkowski M, Wiśniewska M, Słupski M, Ohla J, Zabrzyński J. Can Ashwagandha Benefit the Endocrine System?—A Review. International Journal of Molecular Sciences. 2023; 24(22):16513. https://doi.org/10.3390/ijms242216513
Chicago/Turabian StyleWiciński, Michał, Anna Fajkiel-Madajczyk, Zuzanna Kurant, Dominik Kurant, Karol Gryczka, Michal Falkowski, Magdalena Wiśniewska, Maciej Słupski, Jakub Ohla, and Jan Zabrzyński. 2023. "Can Ashwagandha Benefit the Endocrine System?—A Review" International Journal of Molecular Sciences 24, no. 22: 16513. https://doi.org/10.3390/ijms242216513
APA StyleWiciński, M., Fajkiel-Madajczyk, A., Kurant, Z., Kurant, D., Gryczka, K., Falkowski, M., Wiśniewska, M., Słupski, M., Ohla, J., & Zabrzyński, J. (2023). Can Ashwagandha Benefit the Endocrine System?—A Review. International Journal of Molecular Sciences, 24(22), 16513. https://doi.org/10.3390/ijms242216513