

The Role of Vitamin D and Its Molecular Bases in Insulin Resistance, Diabetes, Metabolic Syndrome, and Cardiovascular Disease: State of the Art



Abstract
1. Introduction
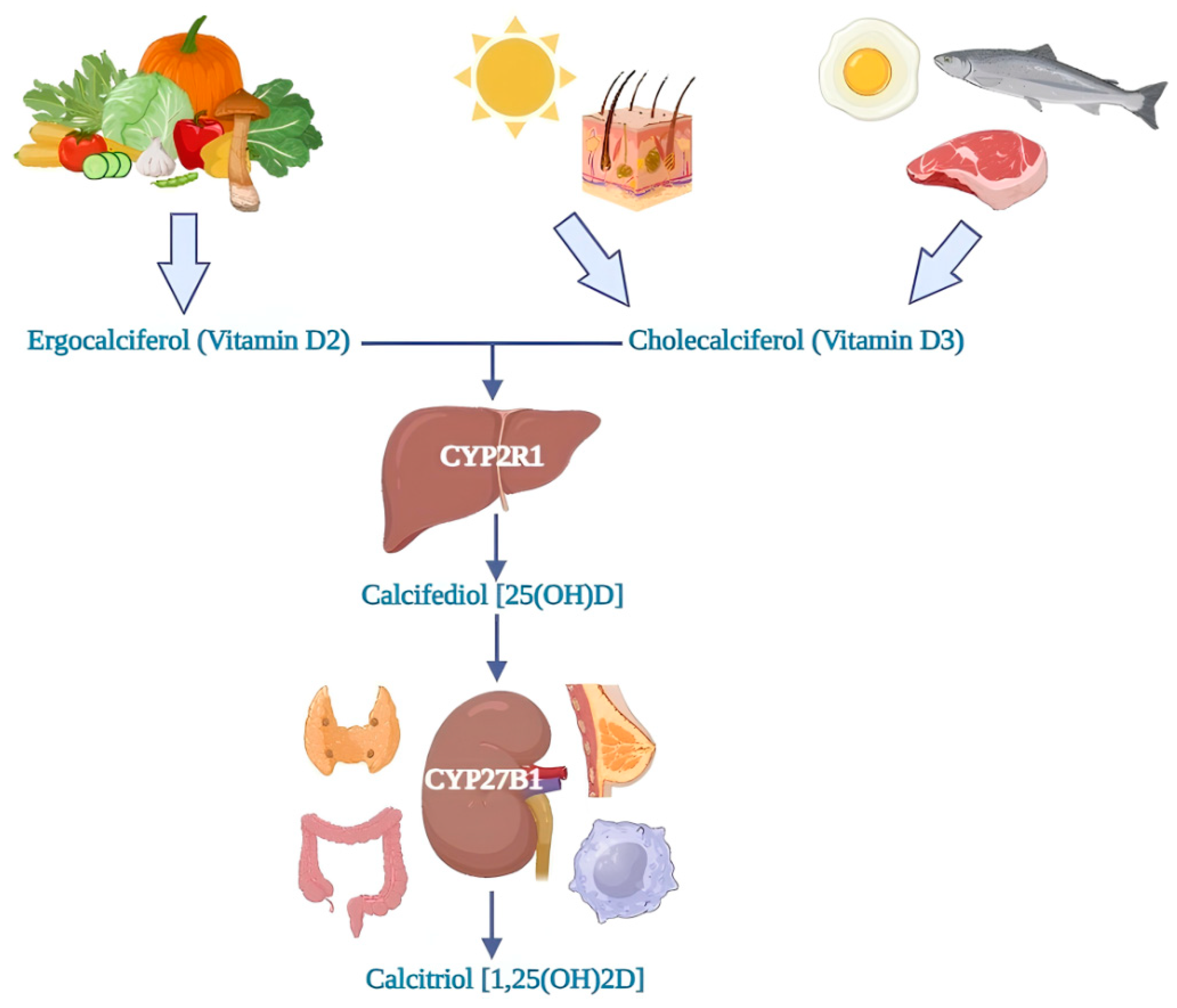
2. Vitamin D Metabolism
3. Vitamin D and Insulin Resistance
3.1. Vitamin D, Insulin Resistance, and Molecular Mechanisms
3.2. Studies and Research
4. Vitamin D and Type 2 Diabetes Mellitus (T2DM)
4.1. Vitamin D, T2DM and Molecular Mechanisms
4.2. Studies and Research
5. Vitamin D and Type 1 Diabetes Mellitus (T1DM)
5.1. Vitamin D, T1DM and Molecular Mechanisms
5.2. Studies and Research
6. Vitamin D and Gestational Diabetes Mellitus (GDM)
6.1. Pathophysiology of Vitamin D Levels in Pregnancy
6.2. Vitamin D, GDM, and Molecular Mechanisms
6.3. Studies and Research
7. Vitamin D, Metabolic Syndrome (MetS), and Cardiovascular Disease (CVD)
7.1. MetS and CVD: Burden of the Problem
7.2. Vitamin D, MetS, CVD, and Molecular Mechanisms
7.3. Studies and Research
8. Discussion and Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Dattola, A.; Silvestri, M.; Bennardo, L.; Passante, M.; Scali, E.; Patruno, C.; Nisticò, S.P. Role of Vitamins in Skin Health: A Systematic Review. Curr. Nutr. Rep. 2020, 9, 226–235. [Google Scholar] [CrossRef] [PubMed]
- Umar, M.; Sastry, K.S.; Chouchane, A.I. Role of Vitamin D Beyond the Skeletal Function: A Review of the Molecular and Clinical Studies. Int. J. Mol. Sci. 2018, 19, 1618. [Google Scholar] [CrossRef] [PubMed]
- Maddaloni, E.; Cavallari, I.; Napoli, N.; Conte, C. Vitamin D and Diabetes Mellitus. Front. Horm. Res. 2018, 50, 161–176. [Google Scholar] [CrossRef]
- Mitri, J.; Muraru, M.D.; Pittas, A.G. Vitamin D and Type 2 Diabetes: A Systematic Review. Eur. J. Clin. Nutr. 2011, 65, 1005–1015. [Google Scholar] [CrossRef] [PubMed]
- Targher, G.; Bertolini, L.; Scala, L.; Cigolini, M.; Zenari, L.; Falezza, G.; Arcaro, G. Associations between Serum 25-Hydroxyvitamin D3 Concentrations and Liver Histology in Patients with Non-Alcoholic Fatty Liver Disease. Nutr. Metab. Cardiovasc. Dis. 2007, 17, 517–524. [Google Scholar] [CrossRef]
- Chen, X.; Zhou, M.; Yan, H.; Chen, J.; Wang, Y.; Mo, X. Association of Serum Total 25-Hydroxy-Vitamin D Concentration and Risk of All-Cause, Cardiovascular and Malignancies-Specific Mortality in Patients with Hyperlipidemia in the United States. Front. Nutr. 2022, 9, 971720. [Google Scholar] [CrossRef]
- Wimalawansa, S.J. Non-Musculoskeletal Benefits of Vitamin D. J. Steroid Biochem. Mol. Biol. 2018, 175, 60–81. [Google Scholar] [CrossRef]
- Teleni, L.; Baker, J.; Koczwara, B.; Kimlin, M.G.; Walpole, E.; Tsai, K.; Isenring, E.A. Clinical Outcomes of Vitamin D Deficiency and Supplementation in Cancer Patients. Nutr. Rev. 2013, 71, 611–621. [Google Scholar] [CrossRef]
- Khademi, Z.; Hamedi-Shahraki, S.; Amirkhizi, F. Vitamin D Insufficiency Is Associated with Inflammation and Deregulation of Adipokines in Patients with Metabolic Syndrome. BMC Endocr. Disord. 2022, 22, 223. [Google Scholar] [CrossRef]
- Argano, C.; Mallaci Bocchio, R.; Natoli, G.; Scibetta, S.; Lo Monaco, M.; Corrao, S. Protective Effect of Vitamin D Supplementation on COVID-19-Related Intensive Care Hospitalization and Mortality: Definitive Evidence from Meta-Analysis and Trial Sequential Analysis. Pharmaceuticals 2023, 16, 130. [Google Scholar] [CrossRef]
- Corrao, S.; Mallaci Bocchio, R.; Lo Monaco, M.; Natoli, G.; Cavezzi, A.; Troiani, E.; Argano, C. Does Evidence Exist to Blunt Inflammatory Response by Nutraceutical Supplementation during COVID-19 Pandemic? An Overview of Systematic Reviews of Vitamin D, Vitamin C, Melatonin, and Zinc. Nutrients 2021, 13, 1261. [Google Scholar] [CrossRef] [PubMed]
- Argano, C.; Mallaci Bocchio, R.; Lo Monaco, M.; Scibetta, S.; Natoli, G.; Cavezzi, A.; Troiani, E.; Corrao, S. An Overview of Systematic Reviews of the Role of Vitamin D on Inflammation in Patients with Diabetes and the Potentiality of Its Application on Diabetic Patients with COVID-19. Int. J. Mol. Sci. 2022, 23, 2873. [Google Scholar] [CrossRef] [PubMed]
- Barragan, M.; Good, M.; Kolls, J.K. Regulation of Dendritic Cell Function by Vitamin D. Nutrients 2015, 7, 8127–8151. [Google Scholar] [CrossRef]
- Saklayen, M.G. The Global Epidemic of the Metabolic Syndrome. Curr. Hypertens. Rep. 2018, 20, 12. [Google Scholar] [CrossRef] [PubMed]
- Argano, C.; Natoli, G.; Mularo, S.; Nobili, A.; Monaco, M.L.; Mannucci, P.M.; Perticone, F.; Pietrangelo, A.; Corrao, S. Impact of Diabetes Mellitus and Its Comorbidities on Elderly Patients Hospitalized in Internal Medicine Wards: Data from the RePoSi Registry. Healthcare 2022, 10, 86. [Google Scholar] [CrossRef]
- International Diabetes Federation. Diabetes Is “A Pandemic of Unprecedented Magnitude” Now Affecting One in 10 Adults Worldwide. Diabetes Res. Clin. Pract. 2021, 181, 109133. [Google Scholar] [CrossRef]
- Dong, J.-Y.; Zhang, W.; Chen, J.J.; Zhang, Z.-L.; Han, S.-F.; Qin, L.-Q. Vitamin D Intake and Risk of Type 1 Diabetes: A Meta-Analysis of Observational Studies. Nutrients 2013, 5, 3551–3562. [Google Scholar] [CrossRef]
- Littorin, B.; Blom, P.; Schölin, A.; Arnqvist, H.J.; Blohmé, G.; Bolinder, J.; Ekbom-Schnell, A.; Eriksson, J.W.; Gudbjörnsdottir, S.; Nyström, L.; et al. Lower Levels of Plasma 25-Hydroxyvitamin D among Young Adults at Diagnosis of Autoimmune Type 1 Diabetes Compared with Control Subjects: Results from the Nationwide Diabetes Incidence Study in Sweden (DISS). Diabetologia 2006, 49, 2847–2852. [Google Scholar] [CrossRef]
- Song, Y.; Wang, L.; Pittas, A.G.; Del Gobbo, L.C.; Zhang, C.; Manson, J.E.; Hu, F.B. Blood 25-Hydroxy Vitamin D Levels and Incident Type 2 Diabetes: A Meta-Analysis of Prospective Studies. Diabetes Care 2013, 36, 1422–1428. [Google Scholar] [CrossRef]
- Afzal, S.; Bojesen, S.E.; Nordestgaard, B.G. Low 25-Hydroxyvitamin D and Risk of Type 2 Diabetes: A Prospective Cohort Study and Meta-analysis. Clin. Chem. 2013, 59, 381–391. [Google Scholar] [CrossRef]
- Lee, C.J.; Iyer, G.; Liu, Y.; Kalyani, R.R.; Bamba, N.; Ligon, C.B.; Varma, S.; Mathioudakis, N. The Effect of Vitamin D Supplementation on Glucose Metabolism in Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis of Intervention Studies. J. Diabetes Complicat. 2017, 31, 1115–1126. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Biswal, N.; Bethou, A.; Rajappa, M.; Kumar, S.; Vinayagam, V. Does Vitamin D Supplementation Improve Glycaemic Control In Children With Type 1 Diabetes Mellitus?—A Randomized Controlled Trial. J. Clin. Diagn. Res. 2017, 11, SC15–SC17. [Google Scholar] [CrossRef] [PubMed]
- Ataie-Jafari, A.; Loke, S.-C.; Rahmat, A.B.; Larijani, B.; Abbasi, F.; Leow, M.K.S.; Yassin, Z. A Randomized Placebo-Controlled Trial of Alphacalcidol on the Preservation of Beta Cell Function in Children with Recent Onset Type 1 Diabetes. Clin. Nutr. 2013, 32, 911–917. [Google Scholar] [CrossRef]
- Contreras-Bolívar, V.; García-Fontana, B.; García-Fontana, C.; Muñoz-Torres, M. Mechanisms Involved in the Relationship between Vitamin D and Insulin Resistance: Impact on Clinical Practice. Nutrients 2021, 13, 3491. [Google Scholar] [CrossRef]
- Gysemans, C.A.; Cardozo, A.K.; Callewaert, H.; Giulietti, A.; Hulshagen, L.; Bouillon, R.; Eizirik, D.L.; Mathieu, C. 1,25-Dihydroxyvitamin D3 Modulates Expression of Chemokines and Cytokines in Pancreatic Islets: Implications for Prevention of Diabetes in Nonobese Diabetic Mice. Endocrinology 2005, 146, 1956–1964. [Google Scholar] [CrossRef]
- Park, S.; Kim, D.S.; Kang, S. Vitamin D Deficiency Impairs Glucose-Stimulated Insulin Secretion and Increases Insulin Resistance by Reducing PPAR-γ Expression in Nonobese Type 2 Diabetic Rats. J. Nutr. Biochem. 2016, 27, 257–265. [Google Scholar] [CrossRef]
- Melguizo-Rodríguez, L.; Costela-Ruiz, V.J.; García-Recio, E.; De Luna-Bertos, E.; Ruiz, C.; Illescas-Montes, R. Role of Vitamin D in the Metabolic Syndrome. Nutrients 2021, 13, 830. [Google Scholar] [CrossRef] [PubMed]
- Mancuso, P.; Rahman, A.; Hershey, S.D.; Dandu, L.; Nibbelink, K.A.; Simpson, R.U. 1,25-Dihydroxyvitamin-D3 Treatment Reduces Cardiac Hypertrophy and Left Ventricular Diameter in Spontaneously Hypertensive Heart Failure-Prone (Cp/+) Rats Independent of Changes in Serum Leptin. J. Cardiovasc. Pharmacol. 2008, 51, 559–564. [Google Scholar] [CrossRef] [PubMed]
- Pieńkowska, A.; Janicka, J.; Duda, M.; Dzwonnik, K.; Lip, K.; Mędza, A.; Szlagatys-Sidorkiewicz, A.; Brzeziński, M. Controversial Impact of Vitamin D Supplementation on Reducing Insulin Resistance and Prevention of Type 2 Diabetes in Patients with Prediabetes: A Systematic Review. Nutrients 2023, 15, 983. [Google Scholar] [CrossRef] [PubMed]
- Ross, A.C.; Taylor, C.L.; Yaktine, A.L.; Del Valle, H.B. (Eds.) Institute of Medicine (US) Committee to Review Dietary Reference Intakes for Vitamin D and Calcium. In Dietary Reference Intakes for Calcium and Vitamin D; The National Academies Collection: Reports Funded by National Institutes of Health; National Academies Press (US): Washington, DC, USA, 2011. [Google Scholar]
- Haussler, M.R.; Haussler, C.A.; Jurutka, P.W.; Thompson, P.D.; Hsieh, J.C.; Remus, L.S.; Selznick, S.H.; Whitfield, G.K. The Vitamin D Hormone and Its Nuclear Receptor: Molecular Actions and Disease States. J. Endocrinol. 1997, 154, S57–S73. [Google Scholar]
- Adams, J.S.; Rafison, B.; Witzel, S.; Reyes, R.E.; Shieh, A.; Chun, R.; Zavala, K.; Hewison, M.; Liu, P.T. Regulation of the Extrarenal CYP27B1-Hydroxylase. J. Steroid Biochem. Mol. Biol. 2014, 144 Pt A, 22–27. [Google Scholar] [CrossRef]
- Klopot, A.; Hance, K.W.; Peleg, S.; Barsony, J.; Fleet, J.C. Nucleo-Cytoplasmic Cycling of the Vitamin D Receptor in the Enterocyte-Like Cell Line, Caco-2. J. Cell. Biochem. 2007, 100, 617–628. [Google Scholar] [CrossRef] [PubMed]
- Charoenngam, N.; Shirvani, A.; Holick, M.F. Vitamin D for Skeletal and Non-Skeletal Health: What We Should Know. J. Clin. Orthop. Trauma 2019, 10, 1082–1093. [Google Scholar] [CrossRef] [PubMed]
- Battault, S.; Whiting, S.J.; Peltier, S.L.; Sadrin, S.; Gerber, G.; Maixent, J.M. Vitamin D Metabolism, Functions and Needs: From Science to Health Claims. Eur. J. Nutr. 2013, 52, 429–441. [Google Scholar] [CrossRef] [PubMed]
- Chagas, C.E.A.; Borges, M.C.; Martini, L.A.; Rogero, M.M. Focus on Vitamin D, Inflammation and Type 2 Diabetes. Nutrients 2012, 4, 52–67. [Google Scholar] [CrossRef] [PubMed]
- Hewison, M. An Update on Vitamin D and Human Immunity. Clin. Endocrinol. 2012, 76, 315–325. [Google Scholar] [CrossRef]
- Selvaraj, P.; Harishankar, M.; Afsal, K. Vitamin D: Immuno-Modulation and Tuberculosis Treatment. Can. J. Physiol. Pharmacol. 2015, 93, 377–384. [Google Scholar] [CrossRef]
- Wang, S.; Cai, B.; Han, X.; Gao, Y.; Zhang, X.; Wang, R.; Zhang, Y.; Chen, Q. Vitamin D Supplementation for Non-alcoholic Fatty Liver Disease in Type 2 Diabetes Mellitus: A Protocol for a Systematic Review and Meta-Analysis. Medicine 2020, 99, e20148. [Google Scholar] [CrossRef]
- Han, F.; Lv, Y.; Gong, L.; Liu, H.; Wan, Z.; Liu, L. VDR Gene Variation and Insulin Resistance Related Diseases. Lipids Health Dis. 2017, 16, 157. [Google Scholar] [CrossRef]
- Sindhughosa, D.A.; Wibawa, I.D.N.; Mariadi, I.K.; Somayana, G. Additional Treatment of Vitamin D for Improvement of Insulin Resistance in Non-Alcoholic Fatty Liver Disease Patients: A Systematic Review and Meta-Analysis. Sci. Rep. 2022, 12, 7716. [Google Scholar] [CrossRef]
- Rafiq, S.; Jeppesen, P.B. Vitamin D Deficiency Is Inversely Associated with Homeostatic Model Assessment of Insulin Resistance. Nutrients 2021, 13, 4358. [Google Scholar] [CrossRef] [PubMed]
- Mo, M.; Shao, B.; Xin, X.; Luo, W.; Si, S.; Jiang, W.; Wang, S.; Shen, Y.; Wu, J.; Yu, Y. The Association of Gene Variants in the Vitamin D Metabolic Pathway and Its Interaction with Vitamin D on Gestational Diabetes Mellitus: A Prospective Cohort Study. Nutrients 2021, 13, 4220. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Chen, Z.; Hu, Y.; Wang, Y.; Wu, Y.; Lian, F.; Li, H.; Yang, J.; Xu, X. The Effects of Vitamin D Supplementation on Glycemic Control and Maternal-Neonatal Outcomes in Women with Established Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis. Clin. Nutr. 2021, 40, 3148–3157. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.; Fu, J.; Zhao, R.; Wang, B.; Zhang, M.; Li, L.; Shi, C. The Effect of Combined Supplementation with Vitamin D and Omega-3 Fatty Acids on Blood Glucose and Blood Lipid Levels in Patients with Gestational Diabetes. Ann. Palliat. Med. 2021, 10, 5652–5658. [Google Scholar] [CrossRef]
- Asbaghi, O.; Khosroshahi, M.Z.; Kashkooli, S.; Abbasnezhad, A. Effect of Calcium-Vitamin D Co-Supplementation on Insulin, Insulin Sensitivity, and Glycemia: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Horm. Metab. Res. 2019, 51, 288–295. [Google Scholar] [CrossRef]
- Szymczak-Pajor, I.; Śliwińska, A. Analysis of Association between Vitamin D Deficiency and Insulin Resistance. Nutrients 2019, 11, 794. [Google Scholar] [CrossRef]
- Hii, C.S.; Ferrante, A. The Non-Genomic Actions of Vitamin D. Nutrients 2016, 8, 135. [Google Scholar] [CrossRef]
- Muoio, D.M.; Newgard, C.B. Mechanisms of Disease:Molecular and Metabolic Mechanisms of Insulin Resistance and Beta-Cell Failure in Type 2 Diabetes. Nat. Rev. Mol. Cell Biol. 2008, 9, 193–205. [Google Scholar] [CrossRef]
- Lotfy, M.; Adeghate, J.; Kalasz, H.; Singh, J.; Adeghate, E. Chronic Complications of Diabetes Mellitus: A Mini Review. Curr. Diabetes Rev. 2017, 13, 3–10. [Google Scholar] [CrossRef]
- Zheng, Y.; Ley, S.H.; Hu, F.B. Global Aetiology and Epidemiology of Type 2 Diabetes Mellitus and Its Complications. Nat. Rev. Endocrinol. 2018, 14, 88–98. [Google Scholar] [CrossRef]
- Rooney, M.R.; Fang, M.; Ogurtsova, K.; Ozkan, B.; Echouffo-Tcheugui, J.B.; Boyko, E.J.; Magliano, D.J.; Selvin, E. Global Prevalence of Prediabetes. Diabetes Care 2023, 46, 1388–1394. [Google Scholar] [CrossRef] [PubMed]
- Blaak, E.E.; Antoine, J.-M.; Benton, D.; Björck, I.; Bozzetto, L.; Brouns, F.; Diamant, M.; Dye, L.; Hulshof, T.; Holst, J.J.; et al. Impact of Postprandial Glycaemia on Health and Prevention of Disease. Obes. Rev. 2012, 13, 923–984. [Google Scholar] [CrossRef] [PubMed]
- Zakharova, I.; Klimov, L.; Kuryaninova, V.; Nikitina, I.; Malyavskaya, S.; Dolbnya, S.; Kasyanova, A.; Atanesyan, R.; Stoyan, M.; Todieva, A.; et al. Vitamin D Insufficiency in Overweight and Obese Children and Adolescents. Front. Endocrinol. 2019, 10, 103. [Google Scholar] [CrossRef]
- Kabadi, S.M.; Lee, B.K.; Liu, L. Joint Effects of Obesity and Vitamin D Insufficiency on Insulin Resistance and Type 2 Diabetes. Diabetes Care 2012, 35, 2048–2054. [Google Scholar] [CrossRef] [PubMed]
- Gagnon, C.; Lu, Z.X.; Magliano, D.J.; Dunstan, D.W.; Shaw, J.E.; Zimmet, P.Z.; Sikaris, K.; Grantham, N.; Ebeling, P.R.; Daly, R.M. Serum 25-Hydroxyvitamin D, Calcium Intake, and Risk of Type 2 Diabetes after 5 Years: Results from a National, Population-Based Prospective Study (the Australian Diabetes, Obesity and Lifestyle Study). Diabetes Care 2011, 34, 1133–1138. [Google Scholar] [CrossRef]
- Mirhosseini, N.; Vatanparast, H.; Mazidi, M.; Kimball, S.M. Vitamin D Supplementation, Glycemic Control, and Insulin Resistance in Prediabetics: A Meta-Analysis. J. Endocr. Soc. 2018, 2, 687–709. [Google Scholar] [CrossRef]
- Borissova, A.M.; Tankova, T.; Kirilov, G.; Dakovska, L.; Kovacheva, R. The Effect of Vitamin D3 on Insulin Secretion and Peripheral Insulin Sensitivity in Type 2 Diabetic Patients. Int. J. Clin. Pract. 2003, 57, 258–261. [Google Scholar] [CrossRef]
- Fadda, G.Z.; Akmal, M.; Lipson, L.G.; Massry, S.G. Direct Effect of Parathyroid Hormone on Insulin Secretion from Pancreatic Islets. Am. J. Physiol. 1990, 258, E975–E984. [Google Scholar] [CrossRef]
- Sherman, M.H.; Yu, R.T.; Engle, D.D.; Ding, N.; Atkins, A.R.; Tiriac, H.; Collisson, E.A.; Connor, F.; Van Dyke, T.; Kozlov, S.; et al. Vitamin D Receptor-Mediated Stromal Reprogramming Suppresses Pancreatitis and Enhances Pancreatic Cancer Therapy. Cell 2014, 159, 80–93. [Google Scholar] [CrossRef]
- Pittas, A.G.; Lau, J.; Hu, F.B.; Dawson-Hughes, B. The Role of Vitamin D and Calcium in Type 2 Diabetes. A Systematic Review and Meta-Analysis. J. Clin. Endocrinol. Metab. 2007, 92, 2017–2029. [Google Scholar] [CrossRef]
- Cigolini, M.; Iagulli, M.P.; Miconi, V.; Galiotto, M.; Lombardi, S.; Targher, G. Serum 25-Hydroxyvitamin D3 Concentrations and Prevalence of Cardiovascular Disease among Type 2 Diabetic Patients. Diabetes Care 2006, 29, 722–724. [Google Scholar] [CrossRef] [PubMed]
- Scragg, R.; Sowers, M.; Bell, C. Serum 25-Hydroxyvitamin D, Diabetes, and Ethnicity in the Third National Health and Nutrition Examination Survey. Diabetes Care 2004, 27, 2813–2818. [Google Scholar] [CrossRef] [PubMed]
- Di Cesar, D.J.; Ploutz-Snyder, R.; Weinstock, R.S.; Moses, A.M. Vitamin D Deficiency Is More Common in Type 2 than in Type 1 Diabetes. Diabetes Care 2006, 29, 174. [Google Scholar] [CrossRef][Green Version]
- UK Prospective Diabetes Study (UKPDS) Group. Intensive Blood-Glucose Control with Sulphonylureas or Insulin Compared with Conventional Treatment and Risk of Complications in Patients with Type 2 Diabetes (UKPDS 33). Lancet 1998, 352, 837–853. [Google Scholar] [CrossRef]
- Hu, Z.; Chen, J.; Sun, X.; Wang, L.; Wang, A. Efficacy of Vitamin D Supplementation on Glycemic Control in Type 2 Diabetes Patients: A Meta-Analysis of Interventional Studies. Medicine 2019, 98, e14970. [Google Scholar] [CrossRef] [PubMed]
- Mitri, J.; Dawson-Hughes, B.; Hu, F.B.; Pittas, A.G. Effects of Vitamin D and Calcium Supplementation on Pancreatic β Cell Function, Insulin Sensitivity, and Glycemia in Adults at High Risk of Diabetes: The Calcium and Vitamin D for Diabetes Mellitus (CaDDM) Randomized Controlled Trial. Am. J. Clin. Nutr. 2011, 94, 486–494. [Google Scholar] [CrossRef] [PubMed]
- Nazarian, S.; St Peter, J.V.; Boston, R.C.; Jones, S.A.; Mariash, C.N. Vitamin D3 Supplementation Improves Insulin Sensitivity in Subjects with Impaired Fasting Glucose. Transl. Res. 2011, 158, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Pramono, A.; Jocken, J.W.E.; Blaak, E.E. Vitamin D Deficiency in the Aetiology of Obesity-Related Insulin Resistance. Diabetes Metab. Res. Rev. 2019, 35, e3146. [Google Scholar] [CrossRef]
- Alvarez, J.A.; Ashraf, A. Role of Vitamin D in Insulin Secretion and Insulin Sensitivity for Glucose Homeostasis. Int. J. Endocrinol. 2010, 2010, 351385. [Google Scholar] [CrossRef]
- Larrick, B.M.; Kim, K.-H.; Donkin, S.S.; Teegarden, D. 1,25-Dihydroxyvitamin D Regulates Lipid Metabolism and Glucose Utilization in Differentiated 3T3-L1 Adipocytes. Nutr. Res. 2018, 58, 72–83. [Google Scholar] [CrossRef]
- Karkeni, E.; Bonnet, L.; Marcotorchino, J.; Tourniaire, F.; Astier, J.; Ye, J.; Landrier, J.-F. Vitamin D Limits Inflammation-Linked MicroRNA Expression in Adipocytes In Vitro and In Vivo: A New Mechanism for the Regulation of Inflammation by Vitamin D. Epigenetics 2018, 13, 156–162. [Google Scholar] [CrossRef]
- Altieri, B.; Grant, W.B.; Della Casa, S.; Orio, F.; Pontecorvi, A.; Colao, A.; Sarno, G.; Muscogiuri, G. Vitamin D and Pancreas: The Role of Sunshine Vitamin in the Pathogenesis of Diabetes Mellitus and Pancreatic Cancer. Crit. Rev. Food Sci. Nutr. 2017, 57, 3472–3488. [Google Scholar] [CrossRef] [PubMed]
- Cade, C.; Norman, A.W. Vitamin D3 Improves Impaired Glucose Tolerance and Insulin Secretion in the Vitamin D-Deficient Rat In Vivo. Endocrinology 1986, 119, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Zeitz, U.; Weber, K.; Soegiarto, D.W.; Wolf, E.; Balling, R.; Erben, R.G. Impaired Insulin Secretory Capacity in Mice Lacking a Functional Vitamin D Receptor. FASEB J. 2003, 17, 509–511. [Google Scholar] [CrossRef] [PubMed]
- Bouillon, R.; Carmeliet, G.; Verlinden, L.; van Etten, E.; Verstuyf, A.; Luderer, H.F.; Lieben, L.; Mathieu, C.; Demay, M. Vitamin D and Human Health: Lessons from Vitamin D Receptor Null Mice. Endocr. Rev. 2008, 29, 726–776. [Google Scholar] [CrossRef] [PubMed]
- Maestro, B.; Campión, J.; Dávila, N.; Calle, C. Stimulation by 1,25-Dihydroxyvitamin D3 of Insulin Receptor Expression and Insulin Responsiveness for Glucose Transport in U-937 Human Promonocytic Cells. Endocr. J. 2000, 47, 383–391. [Google Scholar] [CrossRef] [PubMed]
- Maestro, B.; Molero, S.; Bajo, S.; Dávila, N.; Calle, C. Transcriptional Activation of the Human Insulin Receptor Gene by 1,25-Dihydroxyvitamin D3. Cell Biochem. Funct. 2002, 20, 227–232. [Google Scholar] [CrossRef]
- Pittas, A.G.; Harris, S.S.; Stark, P.C.; Dawson-Hughes, B. The Effects of Calcium and Vitamin D Supplementation on Blood Glucose and Markers of Inflammation in Nondiabetic Adults. Diabetes Care 2007, 30, 980–986. [Google Scholar] [CrossRef]
- Bland, R.; Markovic, D.; Hills, C.E.; Hughes, S.V.; Chan, S.L.F.; Squires, P.E.; Hewison, M. Expression of 25-Hydroxyvitamin D3-1alpha-Hydroxylase in Pancreatic Islets. J. Steroid Biochem. Mol. Biol. 2004, 89–90, 121–125. [Google Scholar] [CrossRef]
- Reusch, J.E.; Begum, N.; Sussman, K.E.; Draznin, B. Regulation of GLUT-4 Phosphorylation by Intracellular Calcium in Adipocytes. Endocrinology 1991, 129, 3269–3273. [Google Scholar] [CrossRef]
- Ryan, Z.C.; Craig, T.A.; Folmes, C.D.; Wang, X.; Lanza, I.R.; Schaible, N.S.; Salisbury, J.L.; Nair, K.S.; Terzic, A.; Sieck, G.C.; et al. 1α,25-Dihydroxyvitamin D3 Regulates Mitochondrial Oxygen Consumption and Dynamics in Human Skeletal Muscle Cells. J. Biol. Chem. 2016, 291, 1514–1528. [Google Scholar] [CrossRef] [PubMed]
- Baron, A.D.; Brechtel, G.; Wallace, P.; Edelman, S.V. Rates and Tissue Sites of Non-Insulin- and Insulin-Mediated Glucose Uptake in Humans. Am. J. Physiol. 1988, 255, E769–E774. [Google Scholar] [CrossRef] [PubMed]
- DeFronzo, R.A.; Jacot, E.; Jequier, E.; Maeder, E.; Wahren, J.; Felber, J.P. The Effect of Insulin on the Disposal of Intravenous Glucose. Results from Indirect Calorimetry and Hepatic and Femoral Venous Catheterization. Diabetes 1981, 30, 1000–1007. [Google Scholar] [CrossRef]
- Jefferson, G.E.; Schnell, D.M.; Thomas, D.T.; Bollinger, L.M. Calcitriol Concomitantly Enhances Insulin Sensitivity and Alters Myocellular Lipid Partitioning in High Fat-Treated Skeletal Muscle Cells. J. Physiol. Biochem. 2017, 73, 613–621. [Google Scholar] [CrossRef] [PubMed]
- Krul-Poel, Y.H.M.; Ter Wee, M.M.; Lips, P.; Simsek, S. Management of endocrine disease: The Effect of Vitamin D Supplementation on Glycaemic Control in Patients with Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis. Eur. J. Endocrinol. 2017, 176, R1–R14. [Google Scholar] [CrossRef] [PubMed]
- Earthman, C.P.; Beckman, L.M.; Masodkar, K.; Sibley, S.D. The Link between Obesity and Low Circulating 25-Hydroxyvitamin D Concentrations: Considerations and Implications. Int. J. Obes. 2012, 36, 387–396. [Google Scholar] [CrossRef]
- Bajaj, S.; Singh, R.P.; Dwivedi, N.C.; Singh, K.; Gupta, A.; Mathur, M. Vitamin D Levels and Microvascular Complications in Type 2 Diabetes. Indian J. Endocrinol. Metab. 2014, 18, 537–541. [Google Scholar] [CrossRef]
- Zhao, J.; Dong, J.; Wang, H.; Shang, H.; Zhang, D.; Liao, L. Efficacy and Safety of Vitamin D3 in Patients with Diabetic Nephropathy: A Meta-Analysis of Randomized Controlled Trials. Chin. Med. J. 2014, 127, 2837–2843. [Google Scholar]
- Shehab, D.; Al-Jarallah, K.; Mojiminiyi, O.A.; Al Mohamedy, H.; Abdella, N.A. Does Vitamin D Deficiency Play a Role in Peripheral Neuropathy in Type 2 Diabetes? Diabet. Med. 2012, 29, 43–49. [Google Scholar] [CrossRef]
- Assy, M.H.; Draz, N.A.; Fathy, S.E.; Hamed, M.G. Impact of Vitamin D Level in Diabetic People with Peripheral Neuropathy. Egypt. J. Neurol. Psychiatry Neurosurg. 2021, 57, 117. [Google Scholar] [CrossRef]
- Al-Shoumer, K.A.; Al-Essa, T.M. Is There a Relationship between Vitamin D with Insulin Resistance and Diabetes Mellitus? World J. Diabetes 2015, 6, 1057–1064. [Google Scholar] [CrossRef]
- Mohd Saffian, S.; Jamil, N.A.; Mohd Tahir, N.A.; Hatah, E. Vitamin D Insufficiency Is High in Malaysia: A Systematic Review and Meta-Analysis of Studies on Vitamin D Status in Malaysia. Front. Nutr. 2022, 9, 1050745. [Google Scholar] [CrossRef]
- Ding, Y.-H.; Wei, T.-M.; Qian, L.-Y.; Ma, Y.; Lao, D.-B.; Yao, B.; Pang, J. Association between Serum 25-Hydroxyvitamin D and Carotid Atherosclerotic Plaque in Chinese Type 2 Diabetic Patients. Medicine 2017, 96, e6445. [Google Scholar] [CrossRef]
- De Boer, I.H.; Kestenbaum, B.; Shoben, A.B.; Michos, E.D.; Sarnak, M.J.; Siscovick, D.S. 25-hydroxyvitamin D levels inversely associate with risk for developing coronary artery calcification. J. Am. Soc. Nephrol. 2009, 20, 1805–1812. [Google Scholar] [CrossRef]
- Zehnder, D.; Bland, R.; Chana, R.S.; Wheeler, D.C.; Howie, A.J.; Williams, M.C.; Stewart, P.M.; Hewison, M. Synthesis of 1,25-dihydroxyvitamin D3 by human endothelial cells is regulated by inflammatory cytokines: A novel autocrine determinant of vascular cell adhesion. J. Am. Soc. Nephrol. 2002, 13, 621–629. [Google Scholar] [CrossRef]
- Wong, M.S.; Delansorne, R.; Man, R.Y.; Vanhoutte, P.M. Vitamin D derivatives acutely reduce endothelium-dependent contractions in the aorta of the spontaneously hypertensive rat. Am. J. Physiol. Heart Circ. Physiol. 2008, 295, H289–H296. [Google Scholar] [CrossRef]
- Richart, T.; Li, Y.; Staessen, J.A. Renal versus extrarenal activation of vitamin D in relation to atherosclerosis, arterial stiffening, and hypertension. Am. J. Hypertens. 2007, 20, 1007–1015. [Google Scholar] [CrossRef]
- Karadeniz, Y.; Özpamuk-Karadeniz, F.; Ahbab, S.; Ataoğlu, E.; Can, G. Vitamin D Deficiency Is a Potential Risk for Blood Pressure Elevation and the Development of Hypertension. Medicina 2021, 57, 1297. [Google Scholar] [CrossRef]
- McMullan, C.J.; Borgi, L.; Curhan, G.C.; Fisher, N.; Forman, J.P. The effect of vitamin D on renin-angiotensin system activation and blood pressure: A randomized control trial. J. Hypertens. 2017, 35, 822–829. [Google Scholar] [CrossRef]
- Tomaschitz, A.; Pilz, S.; Ritz, E.; Grammer, T.; Drechsler, C.; Boehm, B.O.; März, W. Independent association between 1,25-dihydroxyvitamin D, 25-hydroxyvitamin D and the renin-angiotensin system: The Ludwigshafen Risk and Cardiovascular Health (LURIC) study. Clin. Chim. Acta 2010, 411, 1354–1360. [Google Scholar] [CrossRef]
- Li, Y.C.; Kong, J.; Wei, M.; Chen, Z.F.; Liu, S.Q.; Cao, L.P. 1,25-Dihydroxyvitamin D3 is a negative endocrine regulator of the renin-angiotensin system. J. Clin. Investig. 2002, 110, 229–238. [Google Scholar] [CrossRef]
- Zhou, C.; Lu, F.; Cao, K.; Xu, D.; Goltzman, D.; Miao, D. Calcium-independent and 1,25(OH)2D3-dependent regulation of the renin-angiotensin system in 1alpha-hydroxylase knockout mice. Kidney Int. 2008, 74, 170–179. [Google Scholar] [CrossRef]
- Barbarawi, M.; Kheiri, B.; Zayed, Y.; Barbarawi, O.; Dhillon, H.; Swaid, B.; Yelangi, A.; Sundus, S.; Bachuwa, G.; Alkotob, M.L.; et al. Vitamin D Supplementation and Cardiovascular Disease Risks in More Than 83 000 Individuals in 21 Randomized Clinical Trials: A Meta-analysis. JAMA Cardiol. 2019, 4, 765–776. [Google Scholar] [CrossRef]
- Jorde, R.; Figenschau, Y.; Emaus, N.; Hutchinson, M.; Grimnes, G. Serum 25-hydroxyvitamin D levels are strongly related to systolic blood pressure but do not predict future hypertension. Hypertension 2010, 55, 792–798. [Google Scholar] [CrossRef]
- Paschou, S.A.; Papadopoulou-Marketou, N.; Chrousos, G.P.; Kanaka-Gantenbein, C. On Type 1 Diabetes Mellitus Pathogenesis. Endocr. Connect. 2018, 7, R38–R46. [Google Scholar] [CrossRef]
- Soltesz, G.; Patterson, C.C.; Dahlquist, G. EURODIAB Study Group Worldwide Childhood Type 1 Diabetes Incidence—What Can We Learn from Epidemiology? Pediatr. Diabetes 2007, 8 (Suppl. S6), 6–14. [Google Scholar] [CrossRef]
- Cernea, S.; Dobreanu, M.; Raz, I. Prevention of Type 1 Diabetes: Today and Tomorrow. Diabetes Metab. Res. Rev. 2010, 26, 602–605. [Google Scholar] [CrossRef]
- Huber, A.; Menconi, F.; Corathers, S.; Jacobson, E.M.; Tomer, Y. Joint Genetic Susceptibility to Type 1 Diabetes and Autoimmune Thyroiditis: From Epidemiology to Mechanisms. Endocr. Rev. 2008, 29, 697–725. [Google Scholar] [CrossRef]
- Mathieu, C.; Badenhoop, K. Vitamin D and Type 1 Diabetes Mellitus: State of the Art. Trends Endocrinol. Metab. 2005, 16, 261–266. [Google Scholar] [CrossRef]
- Takiishi, T.; Gysemans, C.; Bouillon, R.; Mathieu, C. Vitamin D and Diabetes. Endocrinol. Metab. Clin. N. Am. 2010, 39, 419–446. [Google Scholar] [CrossRef]
- Storm, T.L.; Sørensen, O.H.; Lund, B.; Lund, B.; Christiansen, J.S.; Andersen, A.R.; Lumholtz, I.B.; Parving, H.H. Vitamin D Metabolism in Insulin-Dependent Diabetes Mellitus. Metab. Bone Dis. Relat. Res. 1983, 5, 107–110. [Google Scholar] [CrossRef]
- Luong, K.V.Q.; Nguyen, L.T.H.; Nguyen, D.N.P. The Role of Vitamin D in Protecting Type 1 Diabetes Mellitus. Diabetes Metab. Res. Rev. 2005, 21, 338–346. [Google Scholar] [CrossRef]
- Danescu, L.G.; Levy, S.; Levy, J. Vitamin D and Diabetes Mellitus. Endocrine 2009, 35, 11–17. [Google Scholar] [CrossRef]
- Yang, C.-Y.; Leung, P.S.C.; Adamopoulos, I.E.; Gershwin, M.E. The Implication of Vitamin D and Autoimmunity: A Comprehensive Review. Clin. Rev. Allergy Immunol. 2013, 45, 217–226. [Google Scholar] [CrossRef]
- Norris, J.M.; Johnson, R.K.; Stene, L.C. Type 1 Diabetes-Early Life Origins and Changing Epidemiology. Lancet Diabetes Endocrinol. 2020, 8, 226–238. [Google Scholar] [CrossRef]
- Jiang, X.; Kiel, D.P.; Kraft, P. The Genetics of Vitamin D. Bone 2019, 126, 59–77. [Google Scholar] [CrossRef]
- Holick, M.F. Vitamin D Deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef]
- Bikle, D.D. Vitamin D Metabolism, Mechanism of Action, and Clinical Applications. Chem. Biol. 2014, 21, 319–329. [Google Scholar] [CrossRef]
- Dankers, W.; Colin, E.M.; van Hamburg, J.P.; Lubberts, E. Vitamin D in Autoimmunity: Molecular Mechanisms and Therapeutic Potential. Front. Immunol. 2016, 7, 697. [Google Scholar] [CrossRef]
- Penna, G.; Adorini, L. 1 Alpha,25-Dihydroxyvitamin D3 Inhibits Differentiation, Maturation, Activation, and Survival of Dendritic Cells Leading to Impaired Alloreactive T Cell Activation. J. Immunol. 2000, 164, 2405–2411. [Google Scholar] [CrossRef]
- Zhang, X.; Zhou, M.; Guo, Y.; Song, Z.; Liu, B. 1,25-Dihydroxyvitamin D₃ Promotes High Glucose-Induced M1 Macrophage Switching to M2 via the VDR-PPARγ Signaling Pathway. Biomed. Res. Int. 2015, 2015, 157834. [Google Scholar] [CrossRef]
- Casteels, K.M.; Mathieu, C.; Waer, M.; Valckx, D.; Overbergh, L.; Laureys, J.M.; Bouillon, R. Prevention of Type I Diabetes in Nonobese Diabetic Mice by Late Intervention with Nonhypercalcemic Analogs of 1,25-Dihydroxyvitamin D3 in Combination with a Short Induction Course of Cyclosporin A. Endocrinology 1998, 139, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Mathieu, C.; Waer, M.; Laureys, J.; Rutgeerts, O.; Bouillon, R. Prevention of Autoimmune Diabetes in NOD Mice by 1,25 Dihydroxyvitamin D3. Diabetologia 1994, 37, 552–558. [Google Scholar] [CrossRef]
- Zella, J.B.; McCary, L.C.; DeLuca, H.F. Oral Administration of 1,25-Dihydroxyvitamin D3 Completely Protects NOD Mice from Insulin-Dependent Diabetes Mellitus. Arch. Biochem. Biophys. 2003, 417, 77–80. [Google Scholar] [CrossRef]
- Fronczak, C.M.; Barón, A.E.; Chase, H.P.; Ross, C.; Brady, H.L.; Hoffman, M.; Eisenbarth, G.S.; Rewers, M.; Norris, J.M. In Utero Dietary Exposures and Risk of Islet Autoimmunity in Children. Diabetes Care 2003, 26, 3237–3242. [Google Scholar] [CrossRef] [PubMed]
- Corrao, S.; Colomba, D.; Arnone, S.; Argano, C.; Di Chiara, T.; Scaglione, R.; Licata, G. Improving Efficacy of PubMed Clinical Queries for Retrieving Scientifically Strong Studies on Treatment. J. Am. Med. Inform. Assoc. 2006, 13, 485–487. [Google Scholar] [CrossRef]
- Corrao, S.; Colomba, D.; Argano, C.; Calvo, L.; Scaglione, R.; Licata, G. Optimized Search Strategy for Detecting Scientifically Strong Studies on Treatment through PubMed. Intern. Emerg. Med. 2012, 7, 283–287. [Google Scholar] [CrossRef]
- Hou, Y.; Song, A.; Jin, Y.; Xia, Q.; Song, G.; Xing, X. A Dose–Response Meta-Analysis between Serum Concentration of 25-Hydroxy Vitamin D and Risk of Type 1 Diabetes Mellitus. Eur. J. Clin. Nutr. 2021, 75, 1010–1023. [Google Scholar] [CrossRef]
- Bener, A.; Alsaied, A.; Al-Ali, M.; Al-Kubaisi, A.; Basha, B.; Abraham, A.; Guiter, G.; Mian, M. High Prevalence of Vitamin D Deficiency in Type 1 Diabetes Mellitus and Healthy Children. Acta Diabetol. 2009, 46, 183–189. [Google Scholar] [CrossRef]
- Omar, D.F.; Kamal, M.M.; El-Hefnawy, M.H.; El-Mesallamy, H.O. Serum Vitamin D and Its Upregulated Protein, Thioredoxin Interacting Protein, Are Associated With Beta-Cell Dysfunction in Adult Patients With Type 1 and Type 2 Diabetes. Can. J. Diabetes 2018, 42, 588–594. [Google Scholar] [CrossRef]
- ALkharashi, N.A. Estimation of Vitamin D Deficiency Prevalence among Saudi Children in Armed Forces Hospital and Riyadh Care Hospital in Riyadh, Kingdom of Saudi Arabia and Its Relation to Type 1 Diabetes Mellitus. Saudi Med. J. 2019, 40, 1290–1293. [Google Scholar] [CrossRef] [PubMed]
- Hyppönen, E.; Läärä, E.; Reunanen, A.; Järvelin, M.R.; Virtanen, S.M. Intake of Vitamin D and Risk of Type 1 Diabetes: A Birth-Cohort Study. Lancet 2001, 358, 1500–1503. [Google Scholar] [CrossRef] [PubMed]
- Norris, J.M.; Lee, H.-S.; Frederiksen, B.; Erlund, I.; Uusitalo, U.; Yang, J.; Lernmark, Å.; Simell, O.; Toppari, J.; Rewers, M.; et al. Plasma 25-Hydroxyvitamin D Concentration and Risk of Islet Autoimmunity. Diabetes 2018, 67, 146–154. [Google Scholar] [CrossRef] [PubMed]
- The EURODIAB Substudy 2 Study Group. Vitamin D Supplement in Early Childhood and Risk for Type I (Insulin-Dependent) Diabetes Mellitus. Diabetologia 1999, 42, 51–54. [Google Scholar] [CrossRef]
- Wei, Z.; Yoshihara, E.; He, N.; Hah, N.; Fan, W.; Pinto, A.F.M.; Huddy, T.; Wang, Y.; Ross, B.; Estepa, G.; et al. Vitamin D Switches BAF Complexes to Protect β Cells. Cell 2018, 173, 1135–1149.e15. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Sharma, P.; Girgis, C.M.; Gunton, J.E. Vitamin D and Beta Cells in Type 1 Diabetes: A Systematic Review. Int. J. Mol. Sci. 2022, 23, 14434. [Google Scholar] [CrossRef]
- Gregoriou, E.; Mamais, I.; Tzanetakou, I.; Lavranos, G.; Chrysostomou, S. The Effects of Vitamin D Supplementation in Newly Diagnosed Type 1 Diabetes Patients: Systematic Review of Randomized Controlled Trials. Rev. Diabet. Stud. 2017, 14, 260–268. [Google Scholar] [CrossRef]
- Nascimento, B.F.; Moreira, C.F.F.; da Fonseca, E.R.; Fedeszen, P.M.K.; de Paula, T.P.; de Sena, A.S.S.; de Almeida, N.F.A.; Bandeira Filho, O.C.S.; Curval, D.R.; Padilha, P.C. Effects of vitamin D supplementation on glycemic control of children and adolescents with type 1 diabetes mellitus: A systematic review. J. Pediatr. Endocrinol. Metab. 2022, 35, 973–988. [Google Scholar] [CrossRef]
- Najjar, L.; Sutherland, J.; Zhou, A.; Hyppönen, E. Vitamin D and Type 1 Diabetes Risk: A Systematic Review and Meta-Analysis of Genetic Evidence. Nutrients 2021, 13, 4260. [Google Scholar] [CrossRef]
- von Websky, K.; Hasan, A.A.; Reichetzeder, C.; Tsuprykov, O.; Hocher, B. Impact of Vitamin D on Pregnancy-Related Disorders and on Offspring Outcome. J. Steroid Biochem. Mol. Biol. 2018, 180, 51–64. [Google Scholar] [CrossRef]
- American Diabetes Association 2. Classification and Diagnosis of Diabetes. Diabetes Care 2017, 40, S11–S24. [Google Scholar] [CrossRef] [PubMed]
- Jenum, A.K.; Mørkrid, K.; Sletner, L.; Vangen, S.; Torper, J.L.; Nakstad, B.; Voldner, N.; Rognerud-Jensen, O.H.; Berntsen, S.; Mosdøl, A.; et al. Impact of Ethnicity on Gestational Diabetes Identified with the WHO and the Modified International Association of Diabetes and Pregnancy Study Groups Criteria: A Population-Based Cohort Study. Eur. J. Endocrinol. 2012, 166, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Noctor, E.; Crowe, C.; Carmody, L.A.; Kirwan, B.; O’Dea, A.; Glynn, L.G.; McGuire, B.E.; O’Shea, P.M.; Dunne, F.P. ATLANTIC-DIP: Prevalence of Metabolic Syndrome and Insulin Resistance in Women with Previous Gestational Diabetes Mellitus by International Association of Diabetes in Pregnancy Study Groups Criteria. Acta Diabetol. 2015, 52, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Milajerdi, A.; Tehrani, H.; Haghighatdoost, F.; Larijani, B.; Surkan, P.J.; Azadbakht, L. Associations between Higher Egg Consumption during Pregnancy with Lowered Risks of High Blood Pressure and Gestational Diabetes Mellitus. Int. J. Vitam. Nutr. Res. 2018, 88, 166–175. [Google Scholar] [CrossRef] [PubMed]
- Groof, Z.; Garashi, G.; Husain, H.; Owayed, S.; AlBader, S.; Mouhsen, H.; Mohammad, A.; Ziyab, A.H. Prevalence, Risk Factors, and Fetomaternal Outcomes of Gestational Diabetes Mellitus in Kuwait: A Cross-Sectional Study. J. Diabetes Res. 2019, 2019, e9136250. [Google Scholar] [CrossRef]
- Verma, A.; Boney, C.M.; Tucker, R.; Vohr, B.R. Insulin Resistance Syndrome in Women with Prior History of Gestational Diabetes Mellitus. J. Clin. Endocrinol. Metab. 2002, 87, 3227–3235. [Google Scholar] [CrossRef][Green Version]
- Andersson-Hall, U.; Gustavsson, C.; Pedersen, A.; Malmodin, D.; Joelsson, L.; Holmäng, A. Higher Concentrations of BCAAs and 3-HIB Are Associated with Insulin Resistance in the Transition from Gestational Diabetes to Type 2 Diabetes. J. Diabetes Res. 2018, 2018, 4207067. [Google Scholar] [CrossRef]
- Nutrition Therapy in Gestational Diabetes Mellitus: Time to Move Forward | Diabetes Care | American Diabetes Association. Available online: https://diabetesjournals.org/care/article/41/7/1343/36441/Nutrition-Therapy-in-Gestational-Diabetes-Mellitus (accessed on 23 August 2023).
- Ismail, N.A.; Mohamed Ismail, N.A.; Bador, K.M. Vitamin D in Gestational Diabetes Mellitus and Its Association with Hyperglycaemia, Insulin Sensitivity and Other Factors. J. Obstet. Gynaecol. 2021, 41, 899–903. [Google Scholar] [CrossRef]
- Magnusdottir, K.S.; Tryggvadottir, E.A.; Magnusdottir, O.K.; Hrolfsdottir, L.; Halldorsson, T.I.; Birgisdottir, B.E.; Hreidarsdottir, I.T.; Hardardottir, H.; Gunnarsdottir, I. Vitamin D Status and Association with Gestational Diabetes Mellitus in a Pregnant Cohort in Iceland. Food Nutr. Res. 2021, 65, 5574. [Google Scholar] [CrossRef]
- Agüero-Domenech, N.; Jover, S.; Sarrión, A.; Baranda, J.; Quesada-Rico, J.A.; Pereira-Expósito, A.; Gil-Guillén, V.; Cortés-Castell, E.; García-Teruel, M.J. Vitamin D Deficiency and Gestational Diabetes Mellitus in Relation to Body Mass Index. Nutrients 2021, 14, 102. [Google Scholar] [CrossRef]
- Khambule, L.; George, J.A. The Role of Inflammation in the Development of GDM and the Use of Markers of Inflammation in GDM Screening. Adv. Exp. Med. Biol. 2019, 1134, 217–242. [Google Scholar] [CrossRef] [PubMed]
- Wolf, M.; Sauk, J.; Shah, A.; Vossen Smirnakis, K.; Jimenez-Kimble, R.; Ecker, J.L.; Thadhani, R. Inflammation and Glucose Intolerance: A Prospective Study of Gestational Diabetes Mellitus. Diabetes Care 2004, 27, 21–27. [Google Scholar] [CrossRef] [PubMed]
- López-Tinoco, C.; Roca, M.; García-Valero, A.; Murri, M.; Tinahones, F.J.; Segundo, C.; Bartha, J.L.; Aguilar-Diosdado, M. Oxidative Stress and Antioxidant Status in Patients with Late-Onset Gestational Diabetes Mellitus. Acta Diabetol. 2013, 50, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Shang, M.; Zhao, J.; Yang, L.; Lin, L. Oxidative Stress and Antioxidant Status in Women with Gestational Diabetes Mellitus Diagnosed by IADPSG Criteria. Diabetes Res. Clin. Pract. 2015, 109, 404–410. [Google Scholar] [CrossRef]
- Peuchant, E.; Brun, J.-L.; Rigalleau, V.; Dubourg, L.; Thomas, M.-J.; Daniel, J.-Y.; Leng, J.-J.; Gin, H. Oxidative and Antioxidative Status in Pregnant Women with Either Gestational or Type 1 Diabetes. Clin. Biochem. 2004, 37, 293–298. [Google Scholar] [CrossRef]
- Grissa, O.; Atègbo, J.-M.; Yessoufou, A.; Tabka, Z.; Miled, A.; Jerbi, M.; Dramane, K.L.; Moutairou, K.; Prost, J.; Hichami, A.; et al. Antioxidant Status and Circulating Lipids Are Altered in Human Gestational Diabetes and Macrosomia. Transl. Res. 2007, 150, 164–171. [Google Scholar] [CrossRef]
- Maged, A.M.; Torky, H.; Fouad, M.A.; GadAllah, S.H.; Waked, N.M.; Gayed, A.S.; Salem, A.K. Role of Antioxidants in Gestational Diabetes Mellitus and Relation to Fetal Outcome: A Randomized Controlled Trial. J. Matern. Fetal Neonatal Med. 2016, 29, 4049–4054. [Google Scholar] [CrossRef]
- Haidari, F.; Zakerkish, M.; Karandish, M.; Saki, A.; Pooraziz, S. Association between Serum Vitamin D Level and Glycemic and Inflammatory Markers in Non-Obese Patients with Type 2 Diabetes. Iran. J. Med. Sci. 2016, 41, 367–373. [Google Scholar]
- Wang, W.; Zhang, J.; Wang, H.; Wang, X.; Liu, S. Vitamin D Deficiency Enhances Insulin Resistance by Promoting Inflammation in Type 2 Diabetes. Int. J. Clin. Exp. Pathol. 2019, 12, 1859–1867. [Google Scholar]
- Berridge, M.J. Vitamin D Deficiency and Diabetes. Biochem. J. 2017, 474, 1321–1332. [Google Scholar] [CrossRef]
- Johannesson, B.; Sui, L.; Freytes, D.O.; Creusot, R.J.; Egli, D. Toward Beta Cell Replacement for Diabetes. EMBO J. 2015, 34, 841–855. [Google Scholar] [CrossRef] [PubMed]
- Taheri, E.; Saedisomeolia, A.; Djalali, M.; Qorbani, M.; Madani Civi, M. The Relationship between Serum 25-Hydroxy Vitamin D Concentration and Obesity in Type 2 Diabetic Patients and Healthy Subjects. J. Diabetes Metab. Disord. 2012, 11, 16. [Google Scholar] [CrossRef] [PubMed]
- Milajerdi, A.; Abbasi, F.; Mousavi, S.M.; Esmaillzadeh, A. Maternal Vitamin D Status and Risk of Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis of Prospective Cohort Studies. Clin. Nutr. 2021, 40, 2576–2586. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Song, Y.; Wang, X. Vitamin D Supplementation for the Outcomes of Patients with Gestational Diabetes Mellitus and Neonates: A Meta-Analysis and Systematic Review. Int. J. Clin. Pract. 2023, 2023, 1907222. [Google Scholar] [CrossRef] [PubMed]
- Akbari, M.; Moosazaheh, M.; Lankarani, K.B.; Tabrizi, R.; Samimi, M.; Karamali, M.; Jamilian, M.; Kolahdooz, F.; Asemi, Z. The Effects of Vitamin D Supplementation on Glucose Metabolism and Lipid Profiles in Patients with Gestational Diabetes: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Horm. Metab. Res. 2017, 49, 647–653. [Google Scholar] [CrossRef]
- Wang, H.; Xia, N.; Yang, Y.; Peng, D.-Q. Influence of Vitamin D Supplementation on Plasma Lipid Profiles: A Meta-Analysis of Randomized Controlled Trials. Lipids Health Dis. 2012, 11, 42. [Google Scholar] [CrossRef]
- Jahanjoo, F.; Farshbaf-Khalili, A.; Shakouri, S.K.; Dolatkhah, N. Maternal and Neonatal Metabolic Outcomes of Vitamin D Supplementation in Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis. Ann. Nutr. Metab. 2018, 73, 145–159. [Google Scholar] [CrossRef]
- Kron-Rodrigues, M.R.; Rudge, M.V.C.; Lima, S.A.M. Supplementation of Vitamin D in the Postdelivery Period of Women with Previous Gestational Diabetes Mellitus: Systematic Review and Meta-Analysis of Randomized Trials. Rev. Bras. Ginecol. Obstet. 2021, 43, 699–709. [Google Scholar] [CrossRef]
- Saha, S.; Saha, S. Changes in Anthropometric and Blood 25-Hydroxyvitamin D Measurements in Antenatal Vitamin Supplemented Gestational Diabetes Mellitus Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Turk. Ger. Gynecol. Assoc. 2021, 22, 217–234. [Google Scholar] [CrossRef]
- Wang, M.M.; Chen, Z.J.; Wang, Y.; Xu, X.R.; Li, H.J.; Yang, J. Effects of Vitamin D Supplementation on Serum Lipid Profiles and Neonatal Outcomes in Gestational Diabetes Mellitus:a Meta-analysis. Zhongguo Yi Xue Ke Xue Yuan Xue Bao 2021, 43, 82–91. [Google Scholar] [CrossRef]
- Yang, C.; Jing, W.; Ge, S.; Sun, W. Vitamin D Status and Vitamin D Deficiency Risk Factors among Pregnancy of Shanghai in China. BMC Pregnancy Childbirth 2021, 21, 431. [Google Scholar] [CrossRef] [PubMed]
- Chatzakis, C.; Sotiriadis, A.; Tsakmaki, E.; Papagianni, M.; Paltoglou, G.; Dinas, K.; Mastorakos, G. The Effect of Dietary Supplements on Oxidative Stress in Pregnant Women with Gestational Diabetes Mellitus: A Network Meta-Analysis. Nutrients 2021, 13, 2284. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zhang, C.; Song, Y.; Zhang, Z. Serum Vitamin D Deficiency and Risk of Gestational Diabetes Mellitus: A Meta-Analysis. Arch. Med. Sci. 2020, 16, 742–751. [Google Scholar] [CrossRef] [PubMed]
- Jin, S.; Sha, L.; Dong, J.; Yi, J.; Liu, Y.; Guo, Z.; Hu, B. Effects of Nutritional Strategies on Glucose Homeostasis in Gestational Diabetes Mellitus: A Systematic Review and Network Meta-Analysis. J. Diabetes Res. 2020, 2020, 6062478. [Google Scholar] [CrossRef]
- Soheilykhah, S.; Mojibian, M.; Rashidi, M.; Rahimi-Saghand, S.; Jafari, F. Maternal Vitamin D Status in Gestational Diabetes Mellitus. Nutr. Clin. Pract. 2010, 25, 524–527. [Google Scholar] [CrossRef]
- Zhang, Y.; Gong, Y.; Xue, H.; Xiong, J.; Cheng, G. Vitamin D and Gestational Diabetes Mellitus: A Systematic Review Based on Data Free of Hawthorne Effect. BJOG Int. J. Obstet. Gynaecol. 2018, 125, 784–793. Available online: https://obgyn.onlinelibrary.wiley.com/doi/abs/10.1111/1471-0528.15060 (accessed on 23 August 2023). [CrossRef]
- Vaidya, A.; Williams, J.S. Vitamin D and Insulin Sensitivity: Can Gene Association and Pharmacogenetic Studies of the Vitamin D Receptor Provide Clarity? Metabolism 2012, 61, 759–761. [Google Scholar] [CrossRef]
- Lu, M.; Xu, Y.; Lv, L.; Zhang, M. Association between Vitamin D Status and the Risk of Gestational Diabetes Mellitus: A Meta-Analysis. Arch. Gynecol. Obstet. 2016, 293, 959–966. [Google Scholar] [CrossRef]
- Chen, Y.; Zhu, B.; Wu, X.; Li, S.; Tao, F. Association between Maternal Vitamin D Deficiency and Small for Gestational Age: Evidence from a Meta-Analysis of Prospective Cohort Studies. BMJ Open 2017, 7, e016404. [Google Scholar] [CrossRef]
- Licata, G.; Argano, C.; Di Chiara, T.; Parrinello, G.; Scaglione, R. Obesity: A main factor of metabolic syndrome? Panminerva Med. 2006, 48, 77–85. [Google Scholar]
- Fahed, G.; Aoun, L.; Bou Zerdan, M.; Allam, S.; Bou Zerdan, M.; Bouferraa, Y.; Assi, H.I. Metabolic Syndrome: Updates on Pathophysiology and Management in 2021. Int. J. Mol. Sci. 2022, 23, 786. [Google Scholar] [CrossRef]
- Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2022 | Diabetes Care | American Diabetes Association. Available online: https://diabetesjournals.org/care/article/45/Supplement_1/S17/138925/2-Classification-and-Diagnosis-of-Diabetes (accessed on 23 August 2023).
- Wang, H.; Naghavi, M.; Allen, C.; Barber, R.M.; Bhutta, Z.A.; Carter, A.; Casey, D.C.; Charlson, F.J.; Chen, A.Z.; Coates, M.M.; et al. Global, Regional, and National Life Expectancy, All-Cause Mortality, and Cause-Specific Mortality for 249 Causes of Death, 1980–2015: A Systematic Analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1459–1544. [Google Scholar] [CrossRef]
- Zhu, Y.; Xian, X.; Wang, Z.; Bi, Y.; Chen, Q.; Han, X.; Tang, D.; Chen, R. Research Progress on the Relationship between Atherosclerosis and Inflammation. Biomolecules 2018, 8, 80. [Google Scholar] [CrossRef] [PubMed]
- Hojs, R.; Ekart, R.; Bevc, S.; Hojs, N. Markers of Inflammation and Oxidative Stress in the Development and Progression of Renal Disease in Diabetic Patients. Nephron 2016, 133, 159–162. [Google Scholar] [CrossRef]
- Flaim, C.; Kob, M.; Di Pierro, A.M.; Herrmann, M.; Lucchin, L. Effects of a Whey Protein Supplementation on Oxidative Stress, Body Composition and Glucose Metabolism among Overweight People Affected by Diabetes Mellitus or Impaired Fasting Glucose: A Pilot Study. J. Nutr. Biochem. 2017, 50, 95–102. [Google Scholar] [CrossRef]
- Mannarino, E.; Pirro, M. Molecular Biology of Atherosclerosis. Clin. Cases Miner. Bone Metab. 2008, 5, 57–62. [Google Scholar]
- Hussin, A.M.; Ashor, A.W.; Schoenmakers, I.; Hill, T.; Mathers, J.C.; Siervo, M. Effects of Vitamin D Supplementation on Endothelial Function: A Systematic Review and Meta-Analysis of Randomised Clinical Trials. Eur. J. Nutr. 2017, 56, 1095–1104. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, T.A.; Maki, K.C.; Orringer, C.E.; Jones, P.H.; Kris-Etherton, P.; Sikand, G.; La Forge, R.; Daniels, S.R.; Wilson, D.P.; Morris, P.B.; et al. National Lipid Association Recommendations for Patient-Centered Management of Dyslipidemia: Part 2. J. Clin. Lipidol. 2015, 9, S1–S122.e1. [Google Scholar] [CrossRef]
- Cholesterol Treatment Trialists’ (CTT) Collaboration; Fulcher, J.; O’Connell, R.; Voysey, M.; Emberson, J.; Blackwell, L.; Mihaylova, B.; Simes, J.; Collins, R.; Kirby, A.; et al. Efficacy and Safety of LDL-Lowering Therapy among Men and Women: Meta-Analysis of Individual Data from 174,000 Participants in 27 Randomised Trials. Lancet 2015, 385, 1397–1405. [Google Scholar] [CrossRef]
- Bovolini, A.; Garcia, J.; Andrade, M.A.; Duarte, J.A. Metabolic Syndrome Pathophysiology and Predisposing Factors. Int. J. Sports Med. 2021, 42, 199–214. [Google Scholar] [CrossRef]
- Castro-Barquero, S.; Ruiz-León, A.M.; Sierra-Pérez, M.; Estruch, R.; Casas, R. Dietary Strategies for Metabolic Syndrome: A Comprehensive Review. Nutrients 2020, 12, 2983. [Google Scholar] [CrossRef] [PubMed]
- Pan, G.-T.; Guo, J.-F.; Mei, S.-L.; Zhang, M.-X.; Hu, Z.-Y.; Zhong, C.-K.; Zeng, C.-Y.; Liu, X.-H.; Ma, Q.-H.; Li, B.-Y.; et al. Vitamin D Deficiency in Relation to the Risk of Metabolic Syndrome in Middle-Aged and Elderly Patients with Type 2 Diabetes Mellitus. J. Nutr. Sci. Vitaminol. 2016, 62, 213–219. [Google Scholar] [CrossRef]
- Faraji, S.; Alizadeh, M. Mechanistic Effects of Vitamin D Supplementation on Metabolic Syndrome Components in Patients with or without Vitamin D Deficiency. J. Obes. Metab. Syndr. 2020, 29, 270–280. [Google Scholar] [CrossRef] [PubMed]
- Sepidarkish, M.; Farsi, F.; Akbari-Fakhrabadi, M.; Namazi, N.; Almasi-Hashiani, A.; Maleki Hagiagha, A.; Heshmati, J. The Effect of Vitamin D Supplementation on Oxidative Stress Parameters: A Systematic Review and Meta-Analysis of Clinical Trials. Pharmacol. Res. 2019, 139, 141–152. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.K.; Micinski, D. Vitamin D Upregulates Glutamate Cysteine Ligase and Glutathione Reductase, and GSH Formation, and Decreases ROS and MCP-1 and IL-8 Secretion in High-Glucose Exposed U937 Monocytes. Biochem. Biophys. Res. Commun. 2013, 437, 7–11. [Google Scholar] [CrossRef]
- Brandenburg, V.M.; Vervloet, M.G.; Marx, N. The Role of Vitamin D in Cardiovascular Disease: From Present Evidence to Future Perspectives. Atherosclerosis 2012, 225, 253–263. [Google Scholar] [CrossRef]
- Siti, H.N.; Kamisah, Y.; Kamsiah, J. The Role of Oxidative Stress, Antioxidants and Vascular Inflammation in Cardiovascular Disease (a Review). Vascul. Pharmacol. 2015, 71, 40–56. [Google Scholar] [CrossRef]
- Sies, H. Total Antioxidant Capacity: Appraisal of a Concept. J. Nutr. 2007, 137, 1493–1495. [Google Scholar] [CrossRef]
- Namazi, N.; Larijani, B.; Azadbakht, L. Alpha-Lipoic Acid Supplement in Obesity Treatment: A Systematic Review and Meta-Analysis of Clinical Trials. Clin. Nutr. 2018, 37, 419–428. [Google Scholar] [CrossRef]
- Heshmati, J.; Farsi, F.; Shokri, F.; Rezaeinejad, M.; Almasi-Hashiani, A.; Vesali, S.; Sepidarkish, M. A Systematic Review and Meta-Analysis of the Probiotics and Synbiotics Effects on Oxidative Stress. J. Funct. Foods 2018, 46, 66–84. [Google Scholar] [CrossRef]
- Slominski, A.T.; Kim, T.-K.; Hobrath, J.V.; Janjetovic, Z.; Oak, A.S.W.; Postlethwaite, A.; Lin, Z.; Li, W.; Takeda, Y.; Jetten, A.M.; et al. Characterization of a New Pathway That Activates Lumisterol in Vivo to Biologically Active Hydroxylumisterols. Sci. Rep. 2017, 7, 11434. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, S.F.; Idiculla, J.; Joshi, R.; Joshi, S.; Kulkarni, S. Vitamin D Supplementation in Adults with Vitamin D Deficiency and Its Effect on Metabolic Syndrome—A Randomized Controlled Study. Int. J. Vitam. Nutr. Res. 2016, 86, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, J.S.; Bull Ferreira Campos, A.; Cordeiro, A.; Pereira, S.E.; Saboya, C.J.; Ramalho, A. Vitamin D Nutritional Status and Its Relationship with Metabolic Changes in Adolescents and Adults with Severe Obesity. Nutr. Hosp. 2018, 35, 847–853. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, P.P.; Cangussu, L.; Bueloni-Dias, F.N.; Orsatti, C.L.; Schmitt, E.B.; Nahas-Neto, J.; Nahas, E.A.P. Vitamin D Supplementation Improves the Metabolic Syndrome Risk Profile in Postmenopausal Women. Climacteric 2020, 23, 24–31. [Google Scholar] [CrossRef]
- Xu, Y.; Zhou, Y.; Liu, J.; Wang, C.; Qu, Z.; Wei, Z.; Zhou, D. Genetically Increased Circulating 25(OH)D Level Reduces the Risk of Type 2 Diabetes in Subjects with Deficiency of Vitamin D. Medicine 2020, 99, e23672. [Google Scholar] [CrossRef]
- Pilz, S.; Tomaschitz, A.; Ritz, E.; Pieber, T.R. Vitamin D status and arterial hypertension: A systematic review. Nat. Rev. Cardiol. 2009, 6, 621–630. [Google Scholar] [CrossRef]
- Shi, H.; Norman, A.W.; Okamura, W.H.; Sen, A.; Zemel, M.B. 1a,25-Dihydroxyvitamin D3 modulates human adipocyte metabolism via nongenomic action. FASEB J. 2001, 15, 2751–2753. [Google Scholar] [CrossRef]
- Clarke, N.M.P.; Page, J.E. Vitamin D deficiency. Curr. Opin. Pediatr. 2012, 24, 46–49. [Google Scholar] [CrossRef]
- Vimaleswaran, K.S.; Cavadino, A.; Berry, D.J.; Jorde, R.; Dieffenbach, A.K.; Lu, C.; Alves, A.C.; Heerspink, H.J.L.; Tikkanen, E.; Eriksson, J.; et al. Association of vitamin D status with arterial blood pressure and hypertension risk: A mendelian randomisation study. Lancet Diabetes Endocrinol. 2014, 2, 719–729. [Google Scholar] [CrossRef]
- Rosen, C.J.; Adams, J.S.; Bikle, D.D.; Black, D.M.; Demay, M.B.; Manson, J.E.; Murad, M.H.; Kovacs, C.S. The nonskeletal effects of vitamin D: An endocrine society scientific statement. Endocr. Rev. 2012, 33, 456–492. [Google Scholar] [CrossRef]
- Zhu, W.; Heil, D.P. Associations of Vitamin D Status with Markers of Metabolic Health: A Community-Based Study in Shanghai, China. Diabetes Metab. Syndr. 2018, 12, 727–732. [Google Scholar] [CrossRef] [PubMed]
- Jafari, T.; Fallah, A.A.; Barani, A. Effects of Vitamin D on Serum Lipid Profile in Patients with Type 2 Diabetes: A Meta-Analysis of Randomized Controlled Trials. Clin. Nutr. 2016, 35, 1259–1268. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Liu, Y.; Zheng, Y.; Wang, P.; Zhang, Y. The Effect of Vitamin D Supplementation on Glycemic Control in Type 2 Diabetes Patients: A Systematic Review and Meta-Analysis. Nutrients 2018, 10, 375. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Wang, T.; Zhu, S.; Li, L. Effects of Vitamin D Supplementation as an Adjuvant Therapy in Coronary Artery Disease Patients. Scand. Cardiovasc. J. 2016, 50, 9–16. [Google Scholar] [CrossRef]
- Ganji, V.; Sukik, A.; Alaayesh, H.; Rasoulinejad, H.; Shraim, M. Serum Vitamin D Concentrations Are Inversely Related to Prevalence of Metabolic Syndrome in Qatari Women. Biofactors 2020, 46, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Wang, N.; Wang, C.; Chen, X.; Wan, H.; Chen, Y.; Chen, C.; Han, B.; Lu, Y. Vitamin D, Prediabetes and Type 2 Diabetes: Bidirectional Mendelian Randomization Analysis. Eur. J. Nutr. 2020, 59, 1379–1388. [Google Scholar] [CrossRef]
- Zheng, J.-S.; Luan, J.; Sofianopoulou, E.; Sharp, S.J.; Day, F.R.; Imamura, F.; Gundersen, T.E.; Lotta, L.A.; Sluijs, I.; Stewart, I.D.; et al. The Association between Circulating 25-Hydroxyvitamin D Metabolites and Type 2 Diabetes in European Populations: A Meta-Analysis and Mendelian Randomisation Analysis. PLoS Med. 2020, 17, e1003394. [Google Scholar] [CrossRef]
- Ostadmohammadi, V.; Milajerdi, A.; Ghayour-Mobarhan, M.; Ferns, G.; Taghizadeh, M.; Badehnoosh, B.; Mirzaei, H.; Asemi, Z. The Effects of Vitamin D Supplementation on Glycemic Control, Lipid Profiles and C-Reactive Protein Among Patients with Cardiovascular Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Curr. Pharm. Des. 2019, 25, 201–210. [Google Scholar] [CrossRef]
- Qi, K.-J.; Zhao, Z.-T.; Zhang, W.; Yang, F. The Impacts of Vitamin D Supplementation in Adults with Metabolic Syndrome: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Front. Pharmacol. 2022, 13, 1033026. [Google Scholar] [CrossRef]
- De Paula, T.P.; Kramer, C.K.; Viana, L.V.; Azevedo, M.J. Effects of Individual Micronutrients on Blood Pressure in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Sci. Rep. 2017, 7, 40751. [Google Scholar] [CrossRef]
- McGreevy, C.; Williams, D. New Insights about Vitamin D and Cardiovascular Disease: A Narrative Review. Ann. Intern. Med. 2011, 155, 820–826. [Google Scholar] [CrossRef] [PubMed]
- Grossman, E. Ambulatory Blood Pressure Monitoring in the Diagnosis and Management of Hypertension. Diabetes Care 2013, 36 (Suppl. S2), S307–S311. [Google Scholar] [CrossRef] [PubMed]
- Hajhashemy, Z.; Shahdadian, F.; Moslemi, E.; Mirenayat, F.S.; Saneei, P. Serum Vitamin D Levels in Relation to Metabolic Syndrome: A Systematic Review and Dose-Response Meta-Analysis of Epidemiologic Studies. Obes. Rev. 2021, 22, e13223. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Author/Year | Design | Duration | Participants (I/C) | Dose of Vitamin D | Results |
|---|---|---|---|---|---|
| VITAMIN D AND INSULIN RESISTANCE (IR) | |||||
| Asbaghi et al., 2019 [46] | MT (12 RCTs) | From 6 to 312 weeks | 8946 healthy subjects or patients with overweight/obesity, IFG, pre-diabetes, GDM, T2DM, PCOS, HIV infection (4395/4551) | From 200 IU/day Vitamin D3 to 50,000 IU/week Vitamin D3 (with supplementation dose of calcium that ranged from 500 mg/day to 1000 mg/day) | Reduce effects on FBG, circulating levels of insulin, and HOMA-IR |
| Sindhughosa et al., 2022 [41] | MT (7 RCTs) | From 10 to 52 weeks | 735 patients with NAFLD (423/312) | From 1000 IU/day Vitamin D3 to 50,000 IU/week Vitamin D3 | Improvement in IR (marked by a decrease in HOMA-IR), decrease in ALT levels |
| Pienkowska et al., 2023 [29] | SR (8 RCTs) | From 12 to 260 weeks | From 66 to 2423 patients with prediabetes | From 1000 IU/day Vitamin D3 to 88,000 IU/week Vitamin D3 | Only one trial showed improvements in FBG and HOMA-IR |
| VITAMIN D AND TYPE 2 DIABETES MELLITUS (T2DM) | |||||
| Pittas et al., 2007 [61] | MT (13 case–control studies; 15 cross-sectional studies; 12 RCTs) | N/A | Patients with T2DM or prediabetes | 2000 IU/day Vitamin D3 or Vitamin D3 700 IU/day with supplementation dose of 500 mg/day calcium citrate | Vitamin D and calcium insufficiency may negatively influence glycemia, whereas combined supplementation with both nutrients may be beneficial in optimizing glucose metabolism |
| Krul-Poel et al., 2017 [86] | MT (23 RCTs) | From 4 to 52 weeks | 1797 patients with T2DM: for the effect on HbA1c 1475 patients (755/720), for the effect on FBG 1180 patients (608/572) | From 1000 IU/day Vitamin D3 to 45,000 IU/week Vitamina D3 or 11,200 IU/day Vitamin D3 for 2 weeks followed by 5600 IU/day for 10 weeks or from 100,000 to 300,000 IU Vitamin D3 single dose | Significant effect on FBG in a subgroup of studies (n = 4); no significant effect in change in HbA1c |
| Mirhosseini et al., 2018 [57] | MT (28 RCTs) | From 8 to 260 weeks | 3848 healthy subjects or patients with prediabetes and/or overweight or obesity, NAFLD, arterial hypertension, cervical intraepithelial neoplasia, premenopausal and postmenopausal women | From 420 IU/day to 88,880 IU/week Vitamin D3 | Significant reduction in HbA1c, FBG, and HOMA-IR |
| Hu et al., 2019 [66] | MT (19 RCTs) | From 4 to 24 weeks | 1374 patients with T2DM (747/627) | Up to 50,000 UI/weekly Vitamin D3 or 300,000 UI single injection Vitamin D3 | Significant reduction in HbA1c, IR (marked by a decrease in HOMA-IR) and insulin levels in the short-term vitamin D supplementation group |
| VITAMIN D AND TYPE 1 DIABETES MELLITUS (T1DM) | |||||
| Gregoriou et al., 2017 [138] | MT (7 RCTs) | From 4 to 52 weeks | 287 patients with T1DM | Calcitriol 0.25 μg per day or on alternate days plus insulin Alphacalcidole 0.5 μg daily plus insulin Cholecalciferol 2000 IU per day plus insulin for 18 mo Cholecalciferol 70 IU/kg body weight/day plus insulin | Vitamin D supplementation in the form of alphacalcidole and chole- calciferol appears to be beneficial in daily insulin dose (DID), fasting C- peptide (FCP), stimulated C-peptide (SCP), and HbA1c. |
| Najjar et al., 2021 [140] | MT (10 studies: 3 cohort; 5 case–control; 2 matched case–control) | N/A | 39,884 patients with T1DM (16,370/23,514) | N/A | No large effect of a genetically determined reduction in 25(OH)D concentrations by selected polymorphisms on T1D risk |
| Hou et al., 2021 [129] | MT (16 studies: 12 case–control studies; 1 cross-sectional case–control study; 2 nested case–control study; 1 case–cohort study) | N/A | 10,605 patients with T1DM (3913/6692) | N/A | Results demonstrated a significant inverse association between the 25(OH)D concentration in circulation and the risk of T1DM |
| Nascimento et al., 2022 [139] | SR (10 studies) | From 6 to 52 weeks | Children and adolescents (0–19 years) with T1DM | Cholecalciferol, with dosages ranging from 1000 to 160,000 IU. Just one study used vitamin D in the form of alfacalcidol at a dosage of 0.25 to 0.5 μg/day | This study did not provide evidence to support the effect of vitamin D supplementation on glycemic control to aid in the treatment of T1DM |
| Yu et al., 2022 [137] | SR (13 studies: 9 RCTs; 2 open-label case–control; 1 open label; 1 cohort) | From 4 to 12 weeks | 527 patients with T1DM | The following therapeutic regimens were used: 1.25 D 0.25 μg 2nd daily; 25 D 2000 IU daily; 25 D to achieve serum 25 D > 125 nmol/L; Alfacalcidol 0.25 μg bd 25 D; 60,000 IU monthly; Ergocalciferol (D2) 2 m of 50,000 IU/w; 25 D 2000 IU/d; 25D. 3000 IU/d; Calciferol 2000 IU/d + etanercept + GAD-alum | The maintenance of optimal circulating 25 D levels may reduce the risk of T1D and that may have potential for benefits in delaying the development of absolute or near-absolute C-peptide deficiency |
| VITAMIN D AND GESTATIONAL DIABETES MELLITUS (GDM) | |||||
| Akbari et al., 2017 [167] | MT (6 RCTs) | From 6 to 12 weeks | 371 pregnant women with GDM (187/184) | 50,000 IU vitamin D3 2 times during the study or 50,000 IU vitamin D3 once every 2 weeks for 2 months, for a total of 200,000 IU vitamin D3 or 50,000 U vitamin D3 pearl twice during the study + 1000 mg calcium per day or 1000 IU vitamin D3 and 1000 mg evening primrose oil (EPO) or one intramuscular injection of 300,000 IU of vitamin D3 or a total of 700,000 IU vitamin D3 during pregnancy | This meta-analysis has demonstrated that vitamin D supplementation may lead to an improvement in HOMA-IR, QUICKI, and LDL-cholesterol levels but did not affect FPG, insulin, HbA1c, triglycerides, total-, and HDL-cholesterol levels; however, vitamin D supplementation increased HOMA-B. |
| Jahanjoo et al., 2018 [169] | MT (5 RCTs) | From 6 to 16 weeks | 310 women with GDM | 50,000 IU vitamin D3 2 times during the study or 200,000 IU vitamin D3 for each of the first 2 days, and then 50,000 IU per week thereafter, up to 700,000 IU in total. Those at week 28 of gestation or later were asked to take 100,000 IU weekly or 50,000 IU of vitamin D3 once every 2 weeks | This study showed that supplementation of GDM women with vitamin D may lead to an improvement in FPG, TC, LDL, HDL, and hs-CRP serum levels, as well as in newborns’ hyperbilirubinemia |
| Rodrigues et al., 2019 [170] | MT (6 RCT studies) | From 6 to 24 weeks and a study until delivery | 456 pregnant women with GDM diagnosed in the second or third trimester of pregnancy | 50,000 IU of vitamin D3 every 2 weeks or 1000 UI daily | Improves adverse maternal and neonatal outcomes related to GDM |
| Milajerdi et al., 2021 [145] | MT (29 studies: 18 cohort; 9 nested case–control; 1 prospective cross-sectional; 1 retrospective cohort) | N/A | 42,668 patients with GDM or not | Blood vitamin D levels | The lowest risk of GDM was found among those with serum vitamin D levels of 40 and 90 nmol/L |
| Wang et al., 2021 [44] | MT (19 RCTs; of these, 13 concerned GDM) | From 6 to 12 weeks | 1198 patients with GDM | From 50,000 IU of vitamin D3 2 times/day to 1200 IU daily | The results showed that vitamin D supplementation during pregnancy could significantly reduce maternal cesarean section rate, maternal hospitalization rate, and postpartum hemorrhage in women with GDM |
| Chatzakis et al., 2021 [174] | MT (15 studies: 9 cohort; 6 nestedcase–control) | N/A | 42,636 pregnant women (1848/40,788) | Blood vitamin D levels | The result showed that lower levels of serum 25(OH)D were associated with a higher chance of GDM |
| Wu et al., 2023 [166] | MT (20 RCT studies) | From 2 to 16 weeks | 1682 pregnant women with GDM diagnosed (837/845) | From 50,000 IU of vitamin D3 2 times/day to 1200 IU daily | Reduce serum LDL-C, TG, and TC levels and increase the serum HDL-C level. Reduce maternal and neonatal hyperbilirubinemia and hospitalization risk. |
| VITAMIN D, METABOLIC SYNDROME (MetS), AND CARDIOVASCULAR DISEASE (CVD) | |||||
| De Paula TP et al., 2017 [223] | MT (7 RCTs) | From 3 to 52 weeks | 542 patients with T2DM (472/70) | A single dose of vitamin D2 (100,000 IU) or vitamin D3 (100,000 IU or 200,000 IU) | Reduction in BP, especially in systolic BP |
| Ostadmohammadi et al., 2019 [221] | MT (8 RCTs) | From 8 to 24 weeks | 630 adults with CVD (305/325) | 50,000 IU/week Vitamin D3 or 50,000 IU every two weeks or 300,000 IU single dose | Improving glycemic control, HDL-C, and CRP levels; it did not affect TG, TC, and LDL-C levels |
| Hajhashemy Z. et al., 2021 [226] | Dose–response MT (43 epidemiological studies: 38 cross-sectional; 1 nested case control; 4 cohort studies) | N/A | 309.206 adults with or without MetS | Blood Vitamin D levels in adults | Inverse association between serum vitamin D concentrations and risk of MetS |
| Qi K.J. et al., 2022 [222] | MT (13 RCTs) | From 8 to 24 weeks | 1.076 adults with MetS (530/546) | From 1000 IU/day Vitamin D3 to 50,000 IU/week | Decreased BP, FPG, HOMA-IR, and CRP levels; it did not affect HDL-C, LDL-C, TC, and TG levels |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Argano, C.; Mirarchi, L.; Amodeo, S.; Orlando, V.; Torres, A.; Corrao, S. The Role of Vitamin D and Its Molecular Bases in Insulin Resistance, Diabetes, Metabolic Syndrome, and Cardiovascular Disease: State of the Art. Int. J. Mol. Sci. 2023, 24, 15485. https://doi.org/10.3390/ijms242015485
Argano C, Mirarchi L, Amodeo S, Orlando V, Torres A, Corrao S. The Role of Vitamin D and Its Molecular Bases in Insulin Resistance, Diabetes, Metabolic Syndrome, and Cardiovascular Disease: State of the Art. International Journal of Molecular Sciences. 2023; 24(20):15485. https://doi.org/10.3390/ijms242015485
Chicago/Turabian StyleArgano, Christiano, Luigi Mirarchi, Simona Amodeo, Valentina Orlando, Alessandra Torres, and Salvatore Corrao. 2023. "The Role of Vitamin D and Its Molecular Bases in Insulin Resistance, Diabetes, Metabolic Syndrome, and Cardiovascular Disease: State of the Art" International Journal of Molecular Sciences 24, no. 20: 15485. https://doi.org/10.3390/ijms242015485
APA StyleArgano, C., Mirarchi, L., Amodeo, S., Orlando, V., Torres, A., & Corrao, S. (2023). The Role of Vitamin D and Its Molecular Bases in Insulin Resistance, Diabetes, Metabolic Syndrome, and Cardiovascular Disease: State of the Art. International Journal of Molecular Sciences, 24(20), 15485. https://doi.org/10.3390/ijms242015485