

Immunohistochemical Glucagon-like Peptide-1 Receptor Expression in Human Insulinomas

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
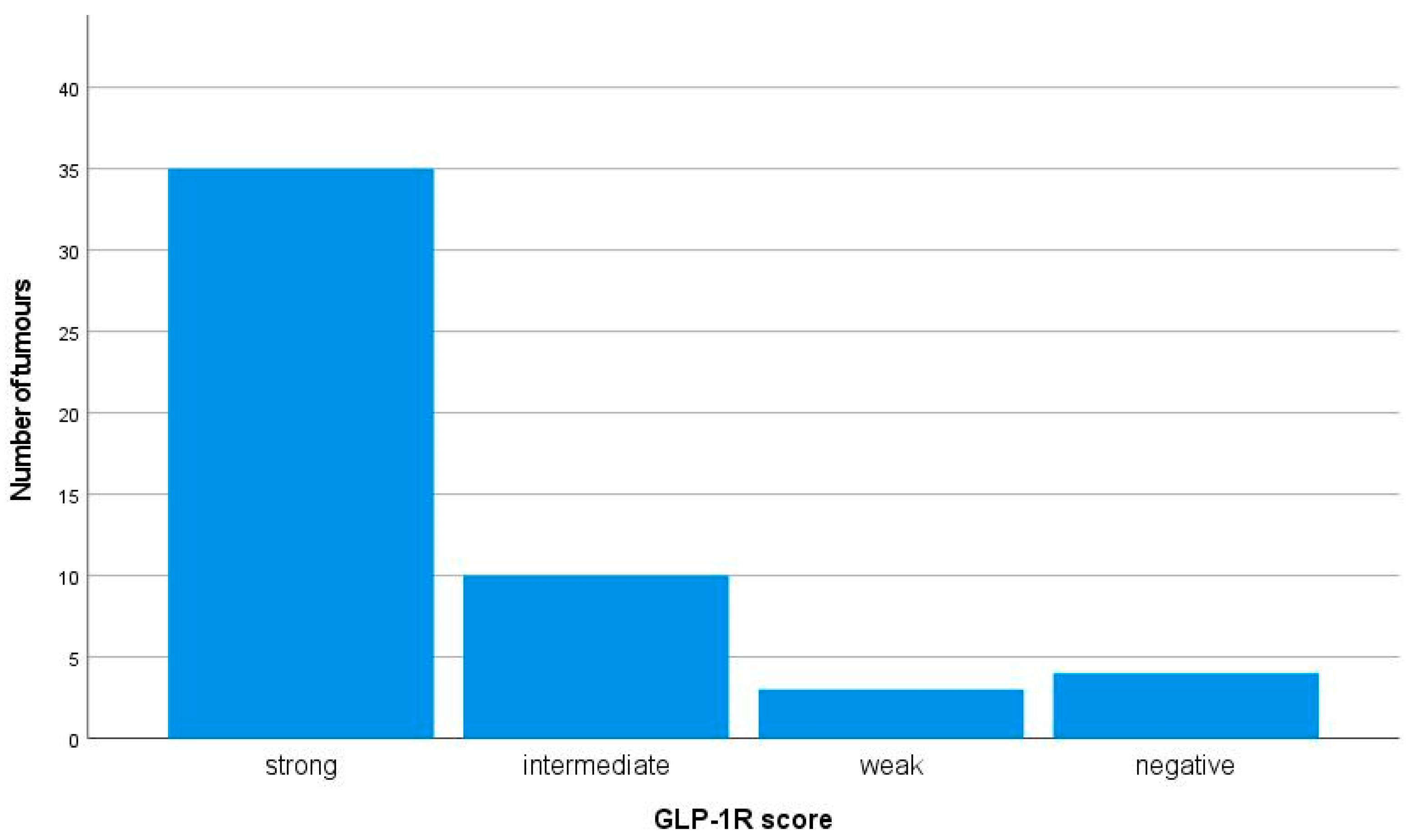
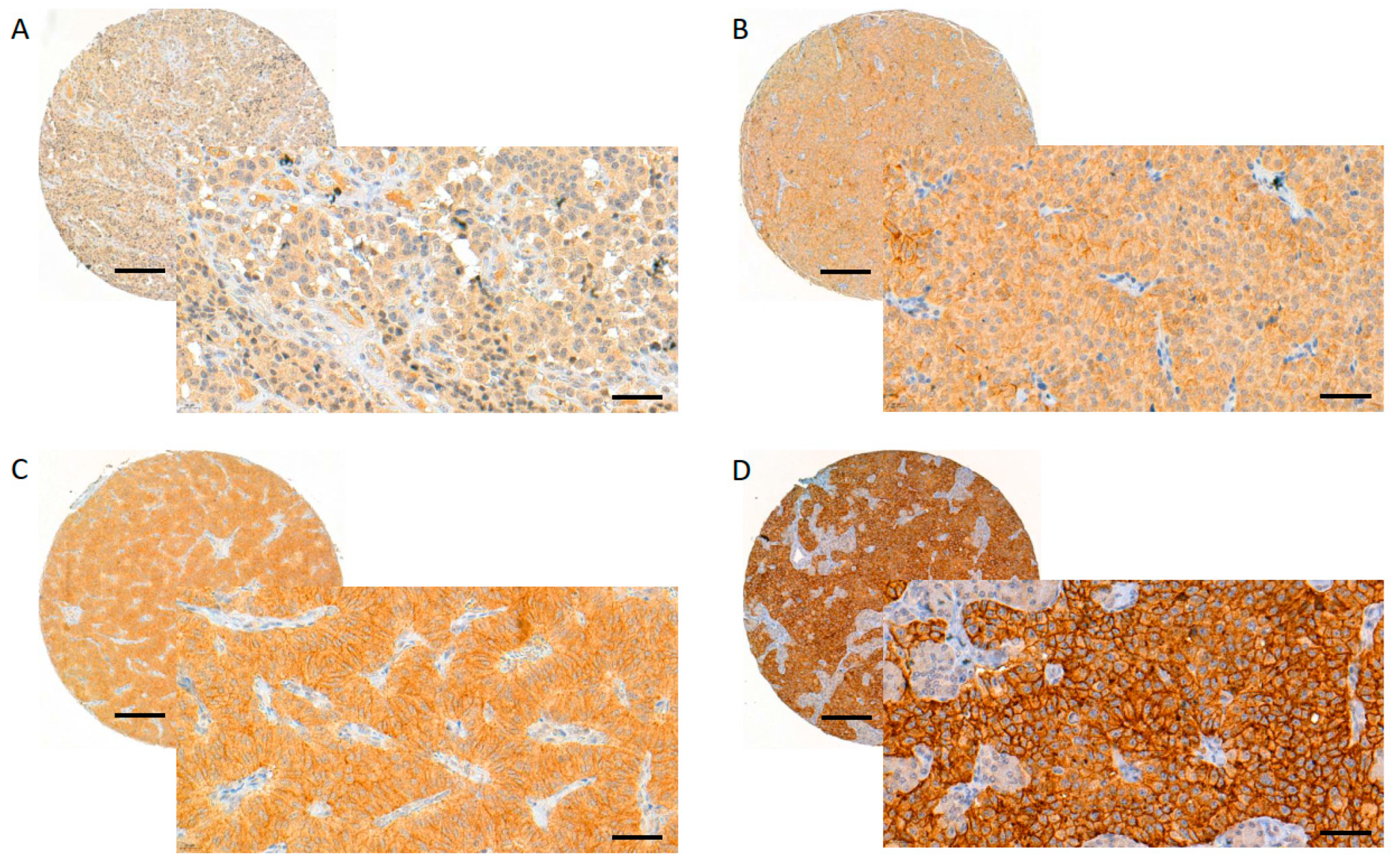
2.2. GLP-1 Receptor Expression
2.3. GLP-1 Receptors, Tumour Size and Ki-67 Proliferation Index (PI)
2.4. GLP-1 Receptors and Insulin Expression
2.5. GLP-1R versus SSTR Expression
2.6. GLP-1 Receptors and Metastatic or MEN1-Related Insulinoma
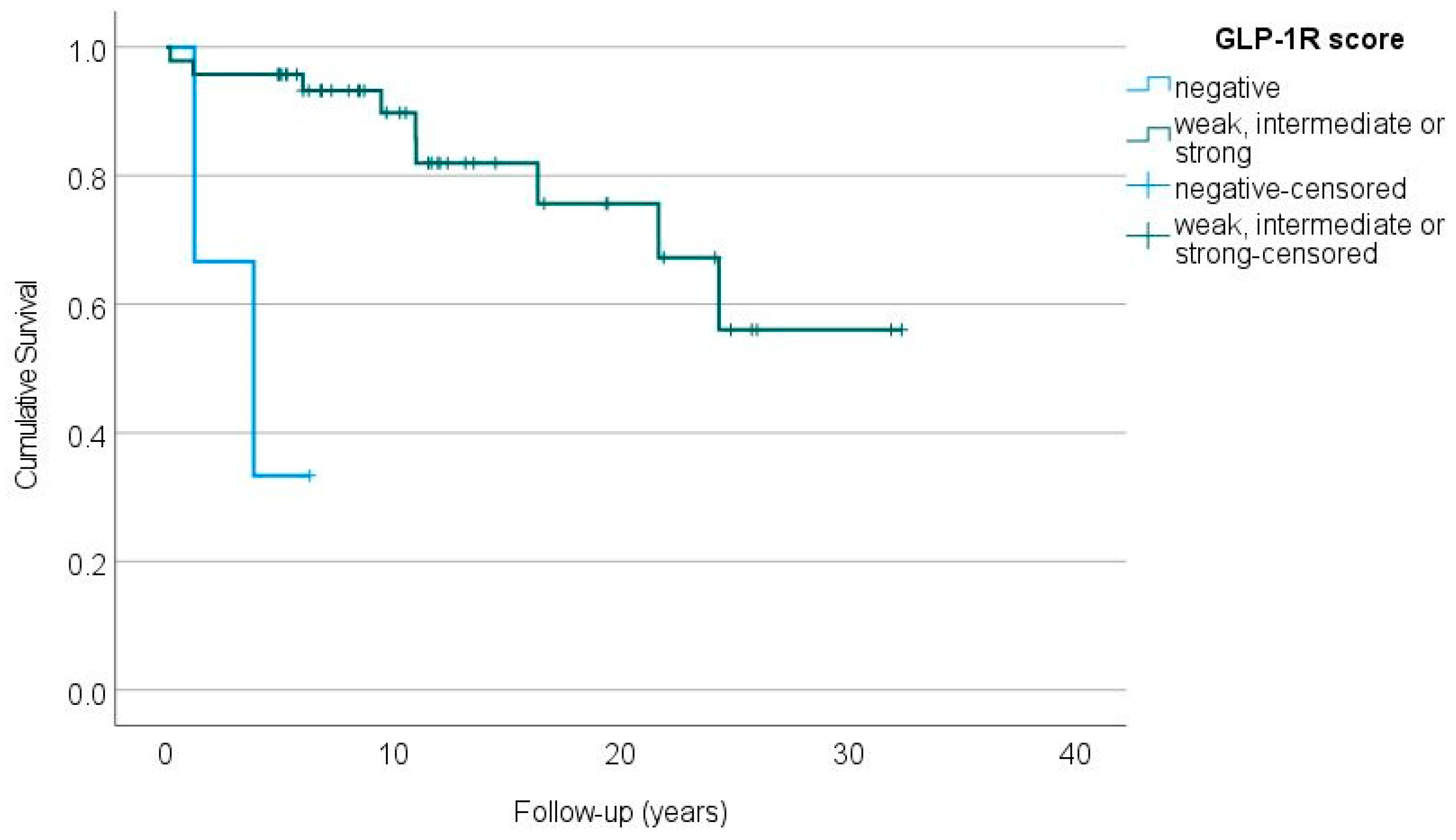
2.7. GLP-1 Receptors and Patient Outcome
3. Discussion
4. Materials and Methods
4.1. Tissue Microarray Construction
4.2. Immunohistochemistry
4.3. Scoring of the Staining Results
4.4. Statistical Analysis
4.5. Ethical Considerations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jensen, R.T.; Cadiot, G.; Brandi, M.L.; de Herder, W.W.; Kaltsas, G.; Komminoth, P.; Scoazec, J.-Y.; Salazar, R.; Sauvanet, A.; Kianmanesh, R.; et al. ENETS Consensus Guidelines for the Management of Patients with Digestive Neuroendocrine Neoplasms: Functional Pancreatic Endocrine Tumor Syndromes. Neuroendocrinology 2012, 95, 98–119. [Google Scholar] [CrossRef] [PubMed]
- Cryer, P.E.; Axelrod, L.; Grossman, A.B.; Heller, S.R.; Montori, V.M.; Seaquist, E.R.; Service, F.J. Evaluation and Management of Adult Hypoglycemic Disorders: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2009, 94, 709–728. [Google Scholar] [CrossRef] [PubMed]
- Mehrabi, A.; Fischer, L.; Hafezi, M.; Dirlewanger, A.; Grenacher, L.; Diener, M.K.; Fonouni, H.; Golriz, M.; Garoussi, C.; Fard, N.; et al. A Systematic Review of Localization, Surgical Treatment Options, and Outcome of Insulinoma. Pancreas 2014, 43, 675–686. [Google Scholar] [CrossRef] [PubMed]
- Falconi, M.; Eriksson, B.; Kaltsas, G.; Bartsch, D.K.; Capdevila, J.; Caplin, M.; Kos-Kudla, B.; Kwekkeboom, D.; Rindi, G.; Klöppel, G.; et al. ENETS Consensus Guidelines Update for the Management of Patients with Functional Pancreatic Neuroendocrine Tumors and Non-Functional Pancreatic Neuroendocrine Tumors. Neuroendocrinology 2016, 103, 153–171. [Google Scholar] [CrossRef] [PubMed]
- Veltroni, A.; Cosaro, E.; Spada, F.; Fazio, N.; Faggiano, A.; Colao, A.; Pusceddu, S.; Zatelli, M.C.; Campana, D.; Piovesan, A.; et al. Clinico–Pathological Features, Treatments and Survival of Malignant Insulinomas: A Multicenter Study. Eur. J. Endocrinol. 2020, 182, 439–446. [Google Scholar] [CrossRef] [PubMed]
- Hackeng, W.M.; Brosens, L.A.A.; Dreijerink, K.M.A. Aggressive versus Indolent Insulinomas—New Clinicopathological Insights. Endocr. Relat. Cancer 2023, 30, e220321. [Google Scholar] [CrossRef] [PubMed]
- Müller, T.D.; Finan, B.; Bloom, S.R.; D’Alessio, D.; Drucker, D.J.; Flatt, P.R.; Fritsche, A.; Gribble, F.; Grill, H.J.; Habener, J.F.; et al. Glucagon-like Peptide 1 (GLP-1). Mol. Metab. 2019, 30, 72–130. [Google Scholar] [CrossRef] [PubMed]
- Reubi, J.C.; Waser, B. Concomitant Expression of Several Peptide Receptors in Neuroendocrine Tumours: Molecular Basis for in Vivo Multireceptor Tumour Targeting. Eur. J. Nucl. Med. Mol. Imaging 2003, 30, 781–793. [Google Scholar] [CrossRef] [PubMed]
- Cases, A.I.; Ohtsuka, T.; Fujino, M.; Ideno, N.; Kozono, S.; Zhao, M.; Ohuchida, K.; Aishima, S.; Nomura, M.; Oda, Y.; et al. Expression of Glucagon-Like Peptide 1 Receptor and Its Effects on Biologic Behavior in Pancreatic Neuroendocrine Tumors. Pancreas 2014, 43, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Waser, B.; Blank, A.; Karamitopoulou, E.; Perren, A.; Reubi, J.C. Glucagon-like-Peptide-1 Receptor Expression in Normal and Diseased Human Thyroid and Pancreas. Mod. Pathol. 2015, 28, 391–402. [Google Scholar] [CrossRef] [PubMed]
- Peltola, E.; Vesterinen, T.; Leijon, H.; Hannula, P.; Huhtala, H.; Mäkinen, M.; Nieminen, L.; Pirinen, E.; Rönty, M.; Söderström, M.; et al. Immunohistochemical Somatostatin Receptor Expression in Insulinomas. APMIS 2023, 131, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Peltola, E.; Hannula, P.; Huhtala, H.; Metso, S.; Kiviniemi, U.; Vornanen, M.; Sand, J.; Laukkarinen, J.; Tiikkainen, M.; Schalin-Jäntti, C.; et al. Characteristics and Outcomes of 79 Patients with an Insulinoma: A Nationwide Retrospective Study in Finland. Int. J. Endocrinol. 2018, 2018, 2059481. [Google Scholar] [CrossRef] [PubMed]
- Antwi, K.; Nicolas, G.; Fani, M.; Heye, T.; Pattou, F.; Grossman, A.; Chanson, P.; Reubi, J.C.; Perren, A.; Gloor, B.; et al. 68Ga-Exendin-4 PET/CT Detects Insulinomas in Patients with Endogenous Hyperinsulinemic Hypoglycemia in MEN-1. J. Clin. Endocrinol. Metab. 2019, 104, 5843–5852. [Google Scholar] [CrossRef] [PubMed]
- Christ, E.; Antwi, K.; Fani, M.; Wild, D. Innovative Imaging of Insulinoma: The End of Sampling? A Review. Endocr. Relat. Cancer 2020, 27, R79–R92. [Google Scholar] [CrossRef] [PubMed]
- Iikuni, S.; Kamei, I.; Ohara, T.; Watanabe, H.; Ono, M. Development of an 111 In-Labeled Glucagon-Like Peptide-1 Receptor-Targeting Exendin-4 Derivative That Exhibits Reduced Renal Uptake. Mol. Pharm. 2022, 19, 1019–1027. [Google Scholar] [CrossRef] [PubMed]
- Buitinga, M.; Jansen, T.; Van Der Kroon, I.; Woliner-van Der Weg, W.; Boss, M.; Janssen, M.; Aarntzen, E.; Béhé, M.; Wild, D.; Visser, E.; et al. Succinylated Gelatin Improves the Theranostic Potential of Radiolabeled Exendin-4 in Insulinoma Patients. J. Nucl. Med. 2019, 60, 812–816. [Google Scholar] [CrossRef] [PubMed]
- Körner, M.; Waser, B.; Schonbrunn, A.; Perren, A.; Reubi, J.C. Somatostatin Receptor Subtype 2A Immunohistochemistry Using a New Monoclonal Antibody Selects Tumors Suitable for In Vivo Somatostatin Receptor Targeting. Am. J. Surg. Pathol. 2012, 36, 242–252. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| n (%) | Median (Range) | |
|---|---|---|
| Age at surgery, years | 52.7 (23.1–84.2) | |
| Duration of follow-up after primary surgery, years | 10.4 (0.2–32.4) | |
| Sex | ||
| Female | 39 (75) | |
| Male | 13 (25) | |
| Disease | ||
| Sporadic, non-metastatic | 47 (90) | |
| Sporadic, metastatic | 3 (6) | |
| MEN1 1-related, non-metastatic | 2 (4) | |
| MEN1-related, metastatic | 0 | |
| Tumour diameter, mm (n = 46) | 15 (5–60) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vesterinen, T.; Peltola, E.; Leijon, H.; Hannula, P.; Huhtala, H.; Mäkinen, M.J.; Nieminen, L.; Pirinen, E.; Rönty, M.; Söderström, M.; et al. Immunohistochemical Glucagon-like Peptide-1 Receptor Expression in Human Insulinomas. Int. J. Mol. Sci. 2023, 24, 15164. https://doi.org/10.3390/ijms242015164
Vesterinen T, Peltola E, Leijon H, Hannula P, Huhtala H, Mäkinen MJ, Nieminen L, Pirinen E, Rönty M, Söderström M, et al. Immunohistochemical Glucagon-like Peptide-1 Receptor Expression in Human Insulinomas. International Journal of Molecular Sciences. 2023; 24(20):15164. https://doi.org/10.3390/ijms242015164
Chicago/Turabian StyleVesterinen, Tiina, Elina Peltola, Helena Leijon, Päivi Hannula, Heini Huhtala, Markus J. Mäkinen, Lasse Nieminen, Elina Pirinen, Mikko Rönty, Mirva Söderström, and et al. 2023. "Immunohistochemical Glucagon-like Peptide-1 Receptor Expression in Human Insulinomas" International Journal of Molecular Sciences 24, no. 20: 15164. https://doi.org/10.3390/ijms242015164
APA StyleVesterinen, T., Peltola, E., Leijon, H., Hannula, P., Huhtala, H., Mäkinen, M. J., Nieminen, L., Pirinen, E., Rönty, M., Söderström, M., Jaatinen, P., & Arola, J. (2023). Immunohistochemical Glucagon-like Peptide-1 Receptor Expression in Human Insulinomas. International Journal of Molecular Sciences, 24(20), 15164. https://doi.org/10.3390/ijms242015164