
Platinum-Based Regimens Are Active in Advanced Pediatric-Type Rhabdomyosarcoma in Adults and Depending on HMGB1 Expression

 ,
,  ,
, 
Abstract
1. Introduction
2. Results
2.1. Clinical and Demographic Characteristics
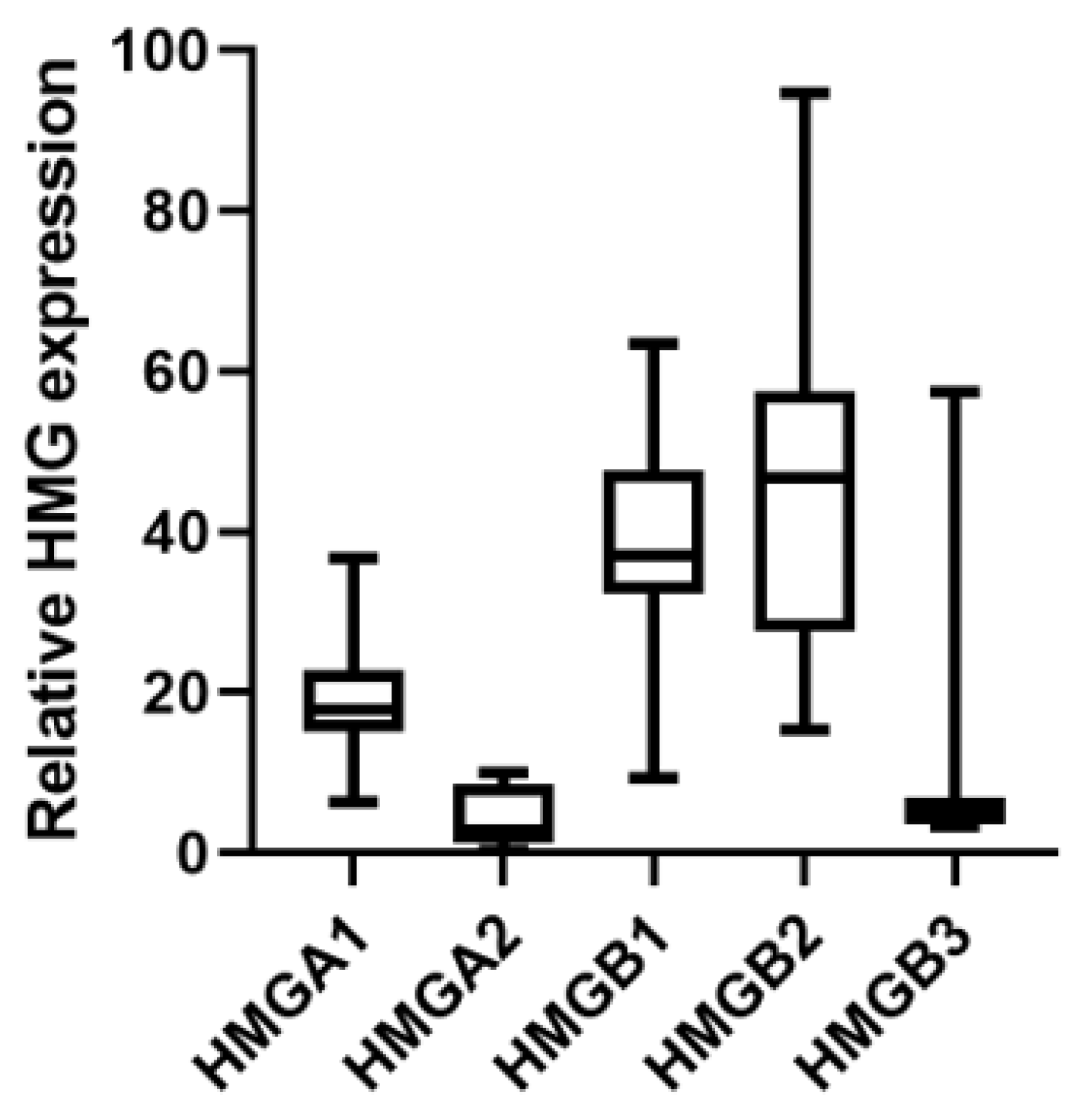
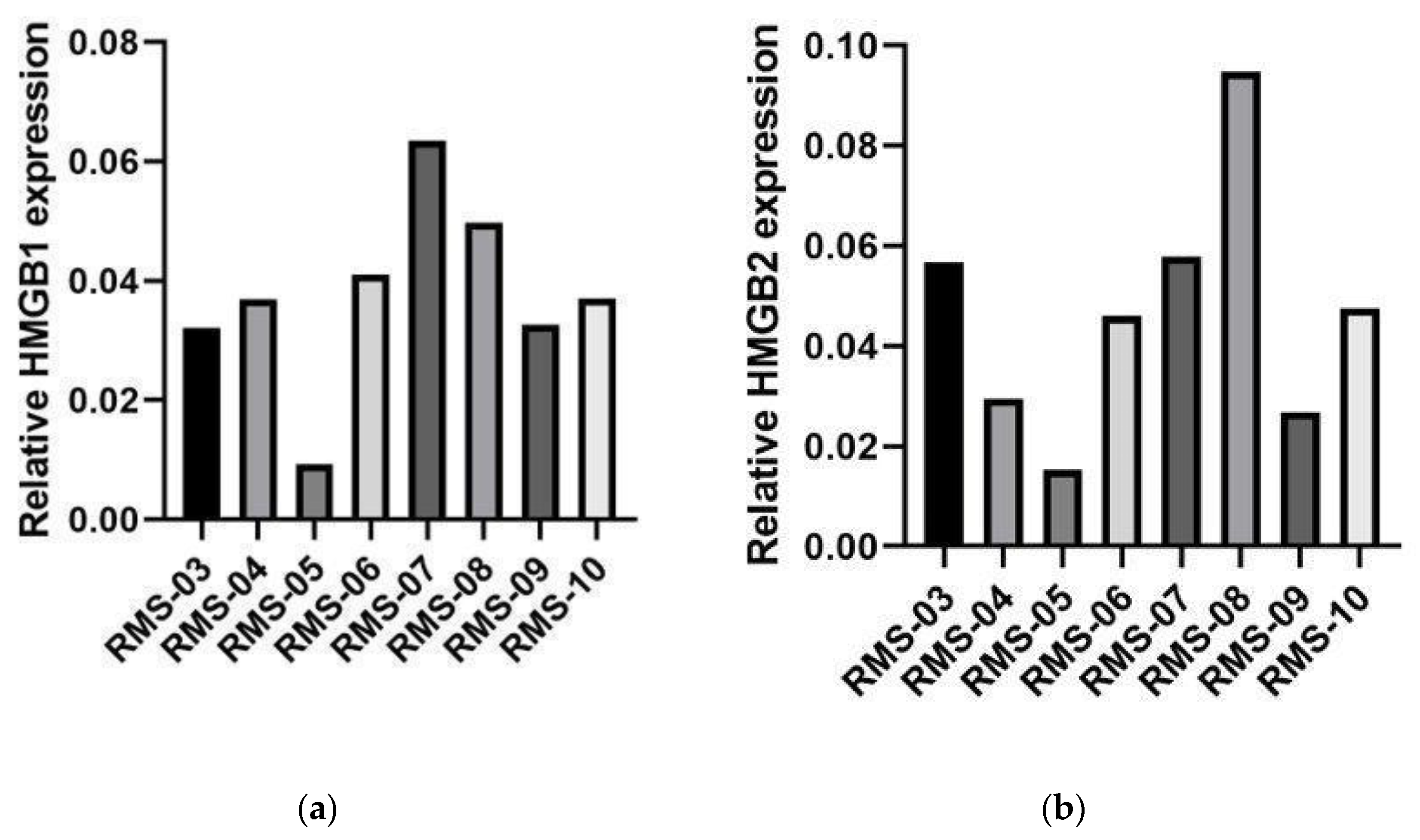
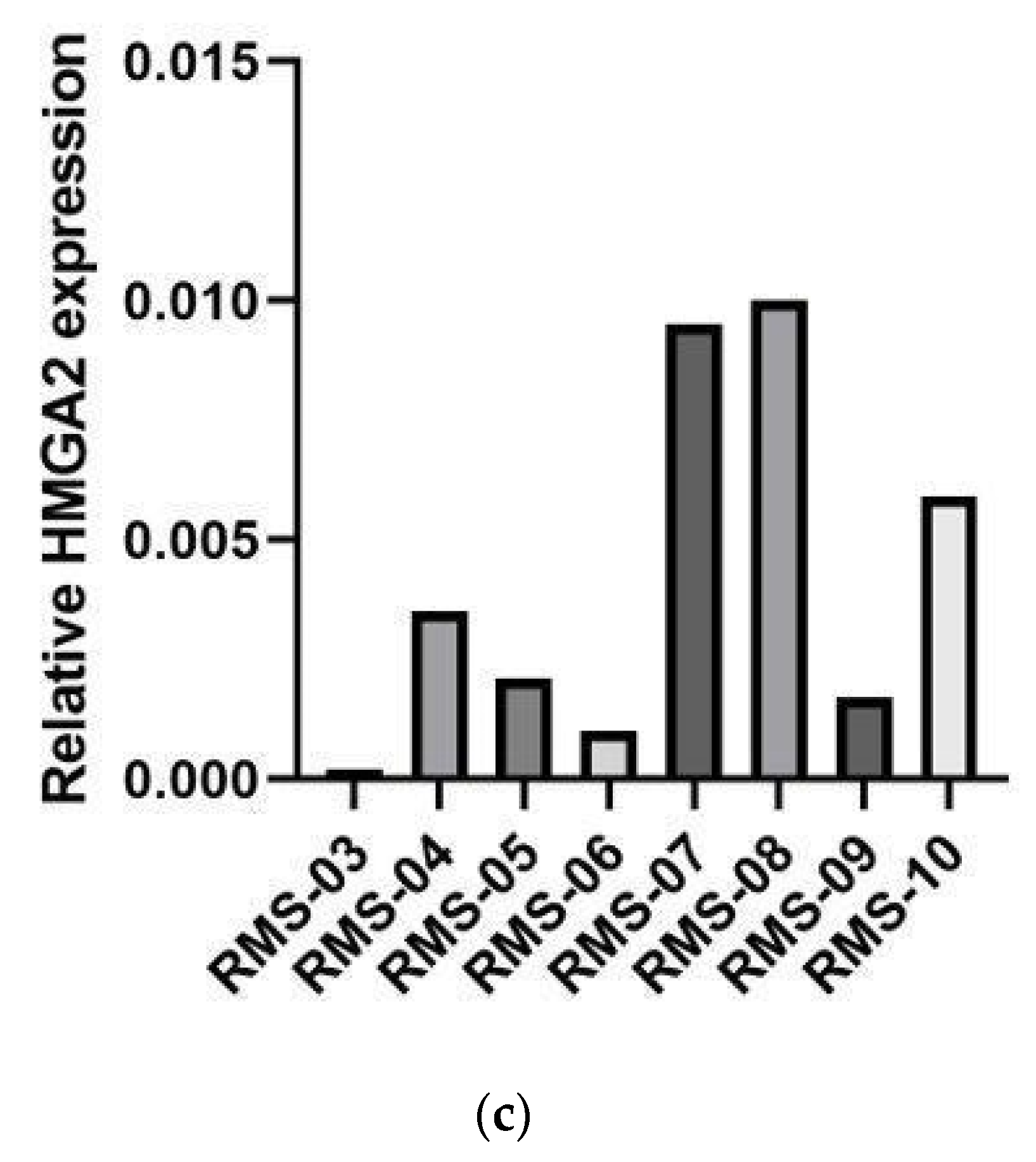
2.2. HMGB1 as a Predictive Biomarker for BOMP-EPI Treatment in RMS
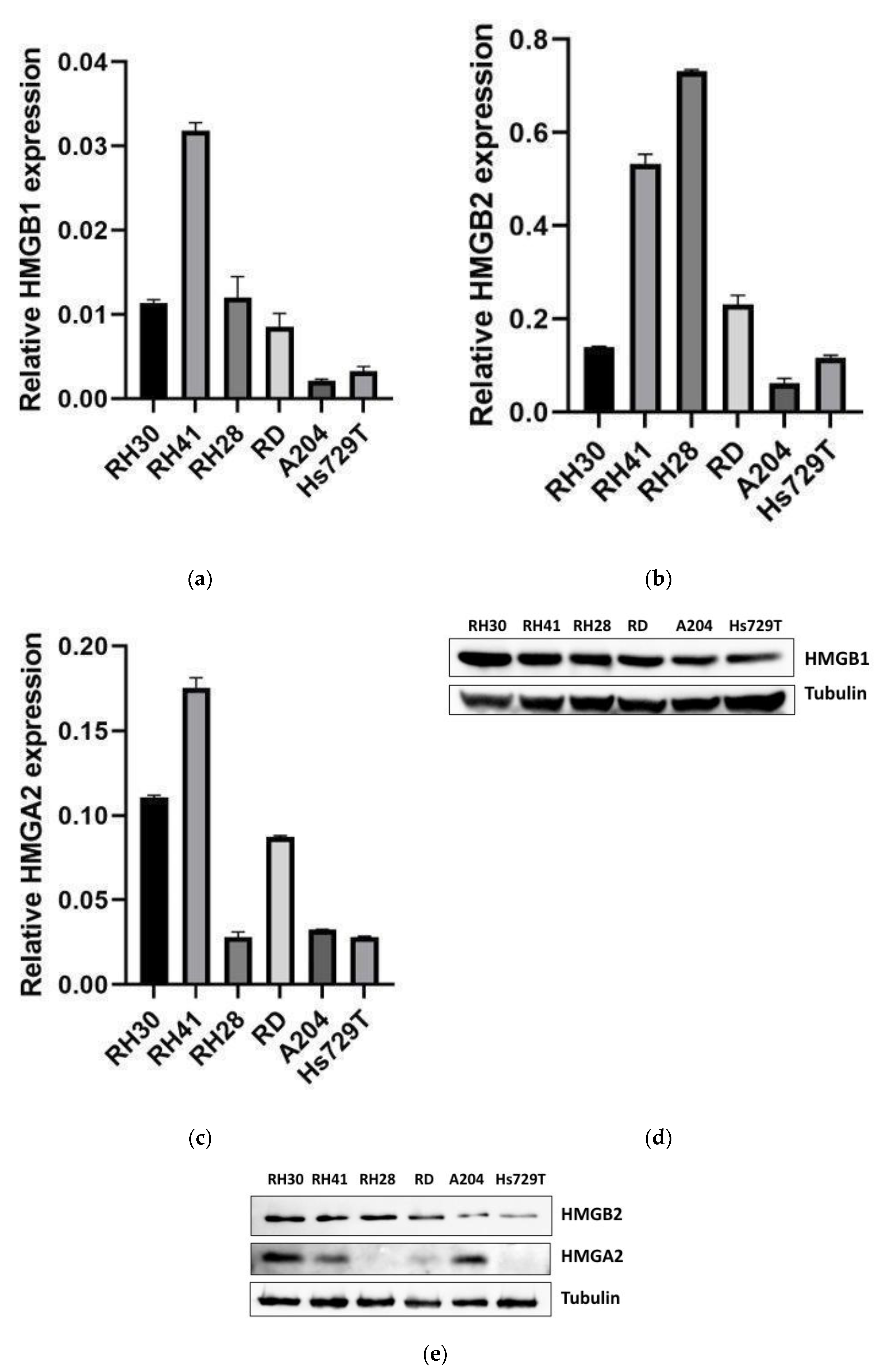
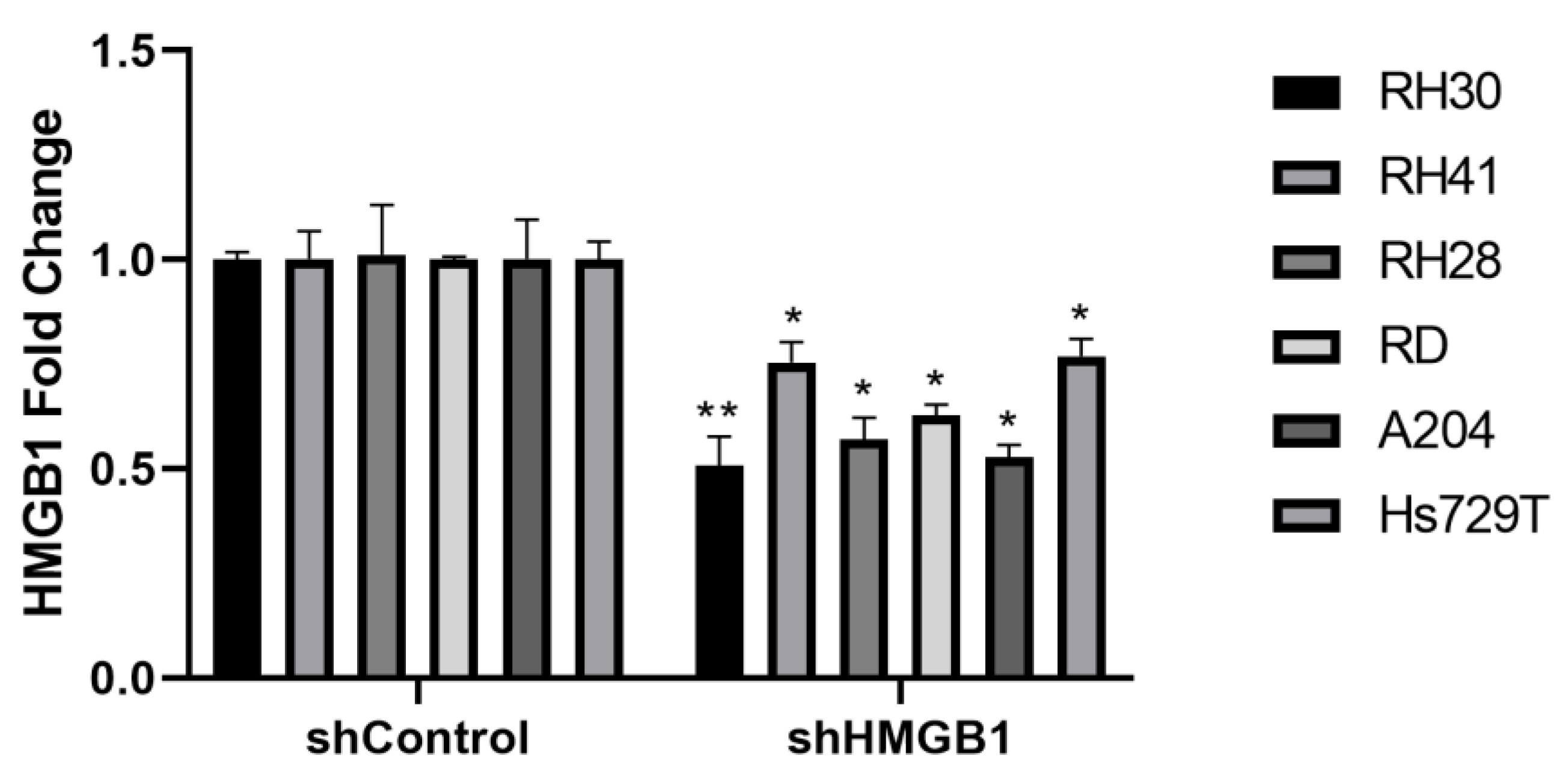
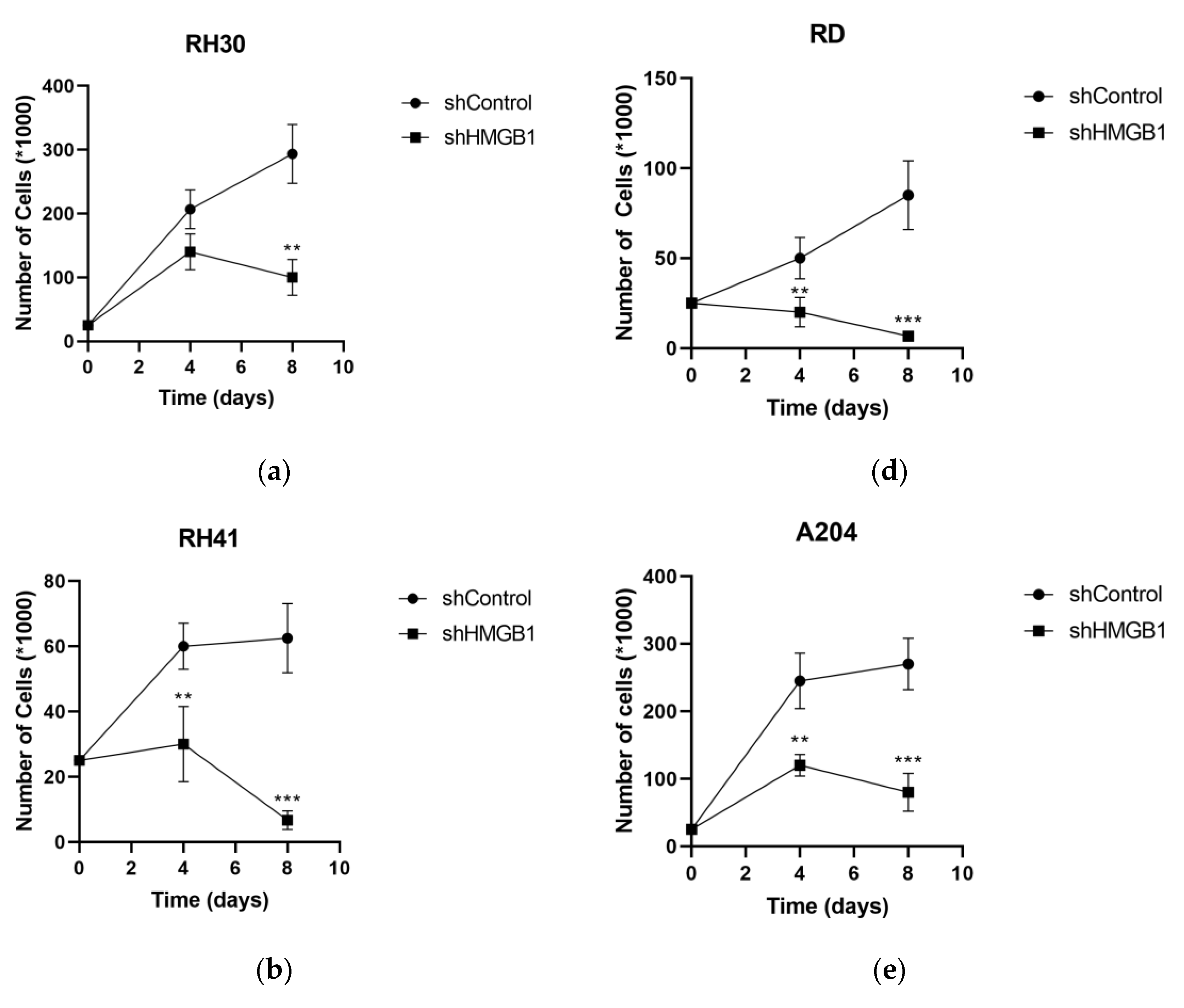
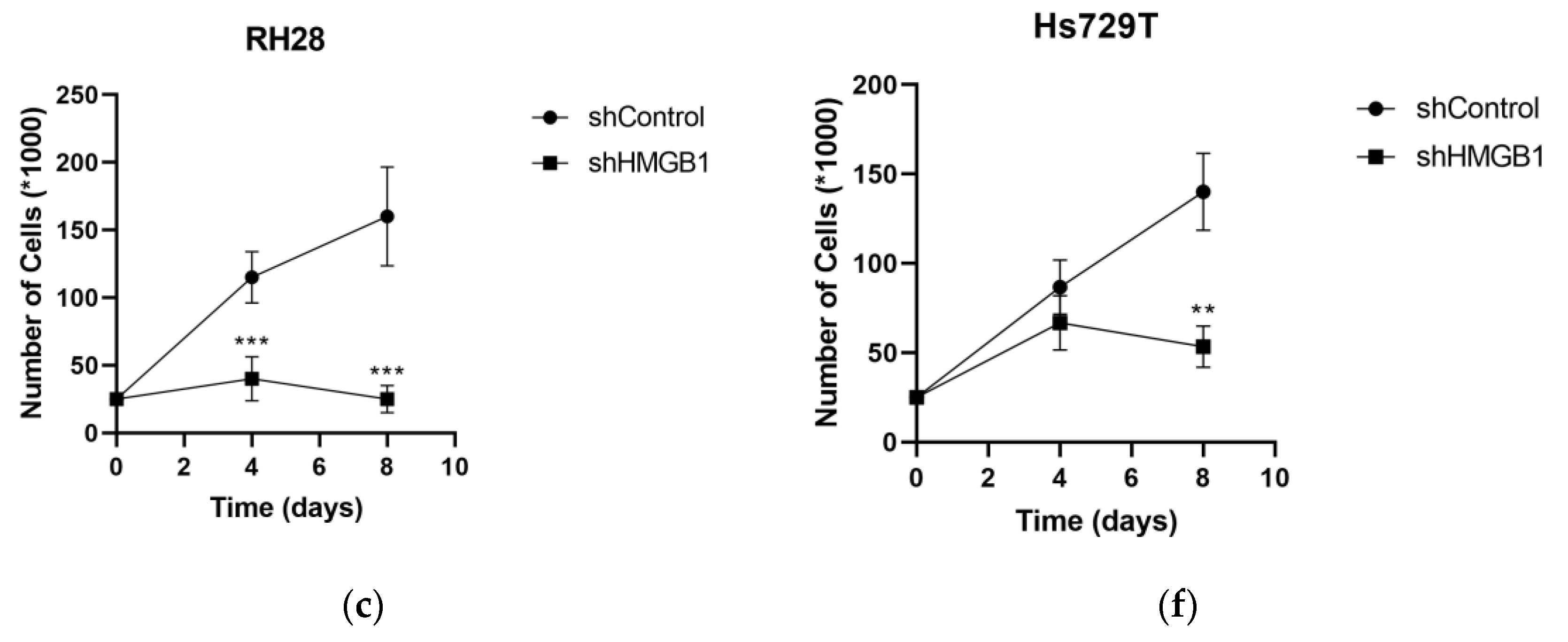
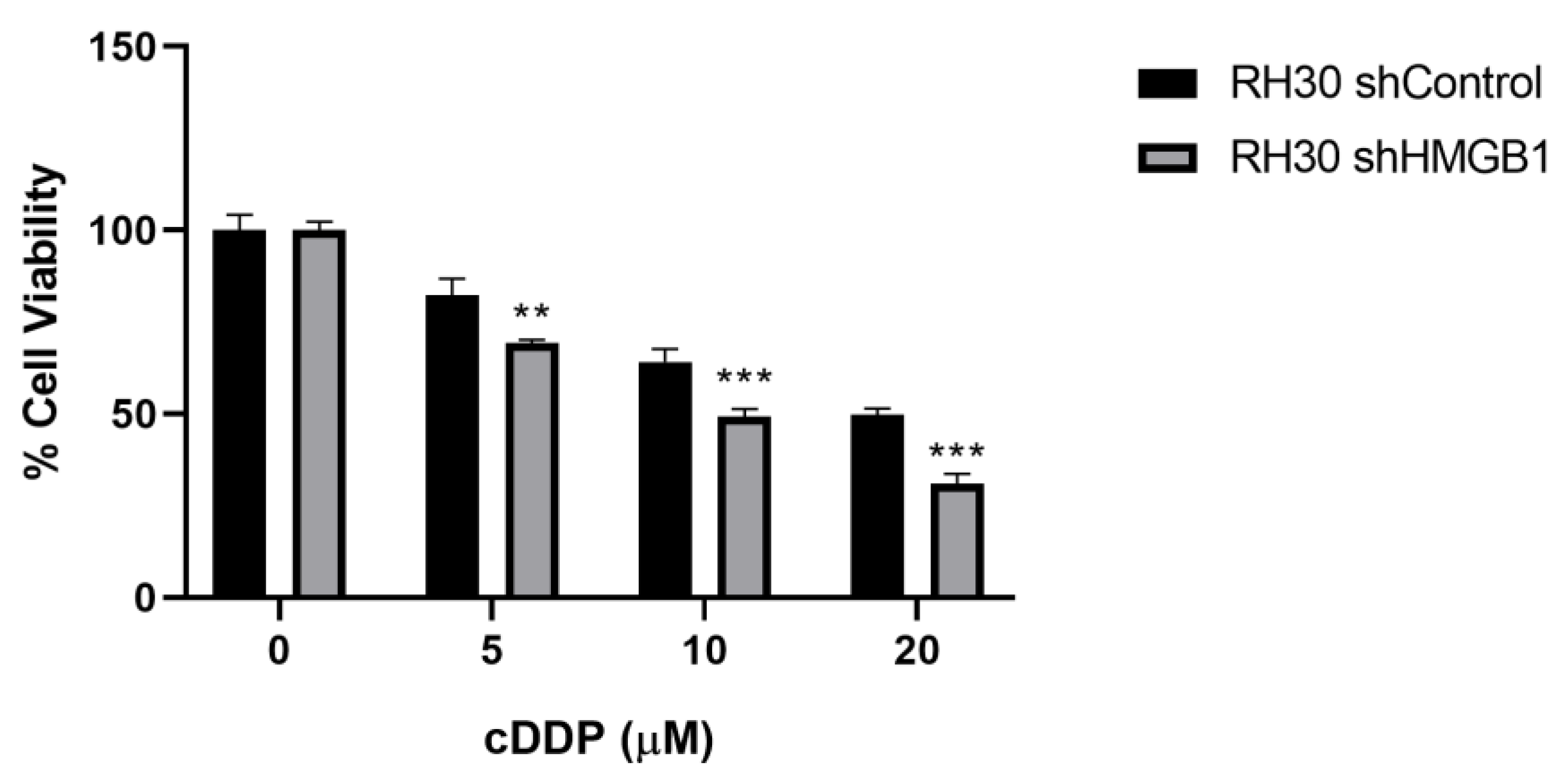
2.3. HMGB1 Knockdown Reduces Proliferation of RMS Cell Lines and Enhances Cisplatin Sensitivity
3. Discussion
4. Materials and Methods
4.1. Rhabdomyosarcoma Cell Lines
Rhabdomyosarcoma Cell Line Transduction
4.2. Patients
4.3. Gene Expression Assay in Tumor Samples
4.4. Cisplatin Treatment
4.5. RNA Extraction and RT-qPCR
4.6. Western Blotting
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kashi, V.P.; Hatley, M.E.; Galindo, R.L. Probing for a Deeper Understanding of Rhabdomyosarcoma: Insights from Complementary Model Systems. Nat. Rev. Cancer 2015, 15, 426–439. [Google Scholar] [CrossRef]
- Leiner, J.; Le Loarer, F. The Current Landscape of Rhabdomyosarcomas: An Update. Virchows Arch. Int. J. Pathol. 2020, 476, 97–108. [Google Scholar] [CrossRef]
- Skapek, S.X.; Ferrari, A.; Gupta, A.; Lupo, P.J.; Butler, E.; Shipley, J.; Barr, F.G.; Hawkins, D.S. Rhabdomyosarcoma. Nat. Rev. Dis. Primer 2019, 5, 1. [Google Scholar] [CrossRef]
- Dantonello, T.M.; Int-Veen, C.; Schuck, A.; Seitz, G.; Leuschner, I.; Nathrath, M.; Schlegel, P.-G.; Kontny, U.; Behnisch, W.; Veit-Friedrich, I.; et al. Survival Following Disease Recurrence of Primary Localized Alveolar Rhabdomyosarcoma. Pediatr. Blood Cancer 2013, 60, 1267–1273. [Google Scholar] [CrossRef]
- Malempati, S.; Hawkins, D.S. Rhabdomyosarcoma: Review of the Children’s Oncology Group (COG) Soft-Tissue Sarcoma Committee Experience and Rationale for Current COG Studies. Pediatr. Blood Cancer 2012, 59, 5–10. [Google Scholar] [CrossRef]
- Ferrari, A.; Dileo, P.; Casanova, M.; Bertulli, R.; Meazza, C.; Gandola, L.; Navarria, P.; Collini, P.; Gronchi, A.; Olmi, P.; et al. Rhabdomyosarcoma in Adults. A Retrospective Analysis of 171 Patients Treated at a Single Institution. Cancer 2003, 98, 571–580. [Google Scholar] [CrossRef]
- Weigel, B.J.; Lyden, E.; Anderson, J.R.; Meyer, W.H.; Parham, D.M.; Rodeberg, D.A.; Michalski, J.M.; Hawkins, D.S.; Arndt, C.A.S. Intensive Multiagent Therapy, Including Dose-Compressed Cycles of Ifosfamide/Etoposide and Vincristine/Doxorubicin/Cyclophosphamide, Irinotecan, and Radiation, in Patients With High-Risk Rhabdomyosarcoma: A Report From the Children’s Oncology Group. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2016, 34, 117–122. [Google Scholar] [CrossRef]
- Chen, C.; Dorado Garcia, H.; Scheer, M.; Henssen, A.G. Current and Future Treatment Strategies for Rhabdomyosarcoma. Front. Oncol. 2019, 9, 1458. [Google Scholar] [CrossRef]
- Pappo, A.S.; Dirksen, U. Rhabdomyosarcoma, Ewing Sarcoma, and Other Round Cell Sarcomas. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2018, 36, 168–179. [Google Scholar] [CrossRef]
- Winter, S.; Fasola, S.; Brisse, H.; Mosseri, V.; Orbach, D. Relapse after Localized Rhabdomyosarcoma: Evaluation of the Efficacy of Second-Line Chemotherapy. Pediatr. Blood Cancer 2015, 62, 1935–1941. [Google Scholar] [CrossRef]
- Dharmarajan, K.V.; Wexler, L.H.; Wolden, S.L. Concurrent Radiation with Irinotecan and Carboplatin in Intermediate- and High-Risk Rhabdomyosarcoma: A Report on Toxicity and Efficacy from a Prospective Pilot Phase II Study. Pediatr. Blood Cancer 2013, 60, 242–247. [Google Scholar] [CrossRef]
- Carli, M.; Perilongo, G.; di Montezemolo, L.C.; De Bernardi, B.; Ceci, A.; Paolucci, G.; Pianca, C.; Calculli, G.; Di Tullio, M.T.; Grotto, P. Phase II Trial of Cisplatin and Etoposide in Children with Advanced Soft Tissue Sarcoma: A Report from the Italian Cooperative Rhabdomyosarcoma Group. Cancer Treat. Rep. 1987, 71, 525–527. [Google Scholar]
- Compostella, A.; Affinita, M.C.; Casanova, M.; Milano, G.M.; Scagnellato, A.; Dall’Igna, P.; Chiaravalli, S.; Pierobon, M.; Manzitti, C.; Zanetti, I.; et al. Topotecan/Carboplatin Regimen for Refractory/Recurrent Rhabdomyosarcoma in Children: Report from the AIEOP Soft Tissue Sarcoma Committee. Tumori 2019, 105, 138–143. [Google Scholar] [CrossRef]
- Tajbakhsh, M.; Houghton, P.J.; Morton, C.L.; Kolb, E.A.; Gorlick, R.; Maris, J.M.; Keir, S.T.; Wu, J.; Reynolds, C.P.; Smith, M.A.; et al. Initial Testing of Cisplatin by the Pediatric Preclinical Testing Program. Pediatr. Blood Cancer 2008, 50, 992–1000. [Google Scholar] [CrossRef]
- Dasari, S.; Tchounwou, P.B. Cisplatin in Cancer Therapy: Molecular Mechanisms of Action. Eur. J. Pharmacol. 2014, 740, 364–378. [Google Scholar] [CrossRef]
- Deans, A.J.; West, S.C. DNA Interstrand Crosslink Repair and Cancer. Nat. Rev. Cancer 2011, 11, 467–480. [Google Scholar] [CrossRef]
- Galluzzi, L.; Vitale, I.; Michels, J.; Brenner, C.; Szabadkai, G.; Harel-Bellan, A.; Castedo, M.; Kroemer, G. Systems Biology of Cisplatin Resistance: Past, Present and Future. Cell Death Dis. 2014, 5, e1257. [Google Scholar] [CrossRef]
- Reeves, R.; Adair, J.E. Role of High Mobility Group (HMG) Chromatin Proteins in DNA Repair. DNA Repair 2005, 4, 926–938. [Google Scholar] [CrossRef]
- Siddik, Z.H. Cisplatin: Mode of Cytotoxic Action and Molecular Basis of Resistance. Oncogene 2003, 22, 7265–7279. [Google Scholar] [CrossRef]
- Huang, J.C.; Zamble, D.B.; Reardon, J.T.; Lippard, S.J.; Sancar, A. HMG-Domain Proteins Specifically Inhibit the Repair of the Major DNA Adduct of the Anticancer Drug Cisplatin by Human Excision Nuclease. Proc. Natl. Acad. Sci. USA 1994, 91, 10394–10398. [Google Scholar] [CrossRef]
- Awuah, S.G.; Riddell, I.A.; Lippard, S.J. Repair Shielding of Platinum-DNA Lesions in Testicular Germ Cell Tumors by High-Mobility Group Box Protein 4 Imparts Cisplatin Hypersensitivity. Proc. Natl. Acad. Sci. USA 2017, 114, 950–955. [Google Scholar] [CrossRef] [PubMed]
- Baldassarre, G.; Belletti, B.; Battista, S.; Nicoloso, M.S.; Pentimalli, F.; Fedele, M.; Croce, C.M.; Fusco, A. HMGA1 Protein Expression Sensitizes Cells to Cisplatin-Induced Cell Death. Oncogene 2005, 24, 6809–6819. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Huang, J.; Ni, J.; Liu, K.; Yu, Y.; Xie, M.; Kang, R.; Vernon, P.; Cao, L.; Tang, D. HMGB1 Promotes Drug Resistance in Osteosarcoma. Cancer Res. 2012, 72, 230–238. [Google Scholar] [CrossRef] [PubMed]
- Xia, Q.; Ni, J.; Huang, J.; Pan, B.; Yan, M.; Li, W. [Suppression of miR-30a/HMGA2-mediated autophagy in osteosarcoma cells impacts chemotherapeutics-induced apoptosis]. Zhong Nan Da Xue Xue Bao Yi Xue Ban 2019, 44, 757–766. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, A.; Huynh, V.; Gaines, K.; Reh, W.A.; Vasquez, K.M. Targeting the High-Mobility Group Box 3 Protein Sensitizes Chemoresistant Ovarian Cancer Cells to Cisplatin. Cancer Res. 2019, 79, 3185–3191. [Google Scholar] [CrossRef]
- Minard-Colin, V.; Ichante, J.-L.; Nguyen, L.; Paci, A.; Orbach, D.; Bergeron, C.; Defachelles, A.-S.; André, N.; Corradini, N.; Schmitt, C.; et al. Phase II Study of Vinorelbine and Continuous Low Doses Cyclophosphamide in Children and Young Adults with a Relapsed or Refractory Malignant Solid Tumour: Good Tolerance Profile and Efficacy in Rhabdomyosarcoma--a Report from the Société Française Des Cancers et Leucémies de l’Enfant et de l’adolescent (SFCE). Eur. J. Cancer Oxf. Engl. 1990 2012, 48, 2409–2416. [Google Scholar] [CrossRef]
- Bompas, E.; Campion, L.; Italiano, A.; Le Cesne, A.; Chevreau, C.; Isambert, N.; Toulmonde, M.; Mir, O.; Ray-Coquard, I.; Piperno-Neumann, S.; et al. Outcome of 449 Adult Patients with Rhabdomyosarcoma: An Observational Ambispective Nationwide Study. Cancer Med. 2018, 7, 4023–4035. [Google Scholar] [CrossRef]
- Wagemans, J.; Beuselinck, B.; Nuyts, S.; Sciot, R.; Delaere, P.; Vander Poorten, V.; Dumez, H.; Hermans, R.; Schöffski, P.; Van den Bogaert, W.; et al. A Case Series of Embryonal Rhabdomyosarcoma of the Head and Neck in Adults. Acta Clin. Belg. 2010, 65, 404–410. [Google Scholar] [CrossRef]
- Casanova, M.; Ferrari, A. Pharmacotherapy for Pediatric Soft-Tissue Sarcomas. Expert Opin. Pharmacother. 2011, 12, 517–531. [Google Scholar] [CrossRef]
- Blanchette, P.; Hogg, D.; Ferguson, P.; Wunder, J.S.; Swallow, C.; Gladdy, R.; Chung, P.; O’Sullivan, B.; Blackstein, M.E.; Catton, C.; et al. Topotecan and Cyclophosphamide in Adults with Relapsed Sarcoma. Sarcoma 2012, 2012, 749067. [Google Scholar] [CrossRef]
- Walterhouse, D.O.; Lyden, E.R.; Breitfeld, P.P.; Qualman, S.J.; Wharam, M.D.; Meyer, W.H. Efficacy of Topotecan and Cyclophosphamide given in a Phase II Window Trial in Children with Newly Diagnosed Metastatic Rhabdomyosarcoma: A Children’s Oncology Group Study. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2004, 22, 1398–1403. [Google Scholar] [CrossRef] [PubMed]
- Saylors, R.L.; Stine, K.C.; Sullivan, J.; Kepner, J.L.; Wall, D.A.; Bernstein, M.L.; Harris, M.B.; Hayashi, R.; Vietti, T.J.; Pediatric Oncology Group. Cyclophosphamide plus Topotecan in Children with Recurrent or Refractory Solid Tumors: A Pediatric Oncology Group Phase II Study. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2001, 19, 3463–3469. [Google Scholar] [CrossRef] [PubMed]
- Mascarenhas, L.; Lyden, E.R.; Breitfeld, P.P.; Walterhouse, D.O.; Donaldson, S.S.; Paidas, C.N.; Parham, D.M.; Anderson, J.R.; Meyer, W.H.; Hawkins, D.S. Randomized Phase II Window Trial of Two Schedules of Irinotecan with Vincristine in Patients with First Relapse or Progression of Rhabdomyosarcoma: A Report from the Children’s Oncology Group. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2010, 28, 4658–4663. [Google Scholar] [CrossRef] [PubMed]
- Setty, B.A.; Stanek, J.R.; Mascarenhas, L.; Miller, A.; Bagatell, R.; Okcu, F.; Nicholls, L.; Lysecki, D.; Gupta, A.A. VIncristine, Irinotecan, and Temozolomide in Children and Adolescents with Relapsed Rhabdomyosarcoma. Pediatr. Blood Cancer 2018, 65, e26728. [Google Scholar] [CrossRef] [PubMed]
- Rapkin, L.; Qayed, M.; Brill, P.; Martin, M.; Clark, D.; George, B.A.; Olson, T.A.; Wasilewski-Masker, K.; Alazraki, A.; Katzenstein, H.M. Gemcitabine and Docetaxel (GEMDOX) for the Treatment of Relapsed and Refractory Pediatric Sarcomas. Pediatr. Blood Cancer 2012, 59, 854–858. [Google Scholar] [CrossRef]
- Van Winkle, P.; Angiolillo, A.; Krailo, M.; Cheung, Y.-K.; Anderson, B.; Davenport, V.; Reaman, G.; Cairo, M.S. Ifosfamide, Carboplatin, and Etoposide (ICE) Reinduction Chemotherapy in a Large Cohort of Children and Adolescents with Recurrent/Refractory Sarcoma: The Children’s Cancer Group (CCG) Experience. Pediatr. Blood Cancer 2005, 44, 338–347. [Google Scholar] [CrossRef] [PubMed]
- Han, T.; Chen, J.; Luan, Y.; Chen, X.; Yang, X.; Zhang, Y.; Li, G.; Wang, D.; Zheng, Z. Successful Treatment of Relapsed Testicular Embryonal Rhabdomyosarcoma with Endostar and Traditional Chemotherapy: A Case Report. OncoTargets Ther. 2018, 11, 5287. [Google Scholar] [CrossRef]
- Tang, D.; Kang, R.; Zeh, H.J.; Lotze, M.T. High-Mobility Group Box 1 and Cancer. Biochim. Biophys. Acta 2010, 1799, 131–140. [Google Scholar] [CrossRef]
- Sims, G.P.; Rowe, D.C.; Rietdijk, S.T.; Herbst, R.; Coyle, A.J. HMGB1 and RAGE in Inflammation and Cancer. Annu. Rev. Immunol. 2010, 28, 367–388. [Google Scholar] [CrossRef]
- Xia, J.; Yu, X.; Song, X.; Li, G.; Mao, X.; Zhang, Y. Inhibiting the Cytoplasmic Location of HMGB1 Reverses Cisplatin Resistance in Human Cervical Cancer Cells. Mol. Med. Rep. 2017, 15, 488–494. [Google Scholar] [CrossRef]
- Zhang, R.; Li, Y.; Wang, Z.; Chen, L.; Dong, X.; Nie, X. Interference with HMGB1 Increases the Sensitivity to Chemotherapy Drugs by Inhibiting HMGB1-Mediated Cell Autophagy and Inducing Cell Apoptosis. Tumor Biol. 2015, 36, 8585–8592. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zhang, H.; Sun, M.; Yin, Z.; Qian, J. High Mobility Group Box 1-Mediated Autophagy Promotes Neuroblastoma Cell Chemoresistance. Oncol. Rep. 2015, 34, 2969–2976. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Liu, K.; Yu, Y.; Xie, M.; Kang, R.; Vernon, P.; Cao, L.; Tang, D.; Ni, J. Targeting HMGB1-Mediated Autophagy as a Novel Therapeutic Strategy for Osteosarcoma. Autophagy 2012, 8, 275–277. [Google Scholar] [CrossRef] [PubMed]
- Syed, N.; Chavan, S.; Sahasrabuddhe, N.A.; Renuse, S.; Sathe, G.; Nanjappa, V.; Radhakrishnan, A.; Raja, R.; Pinto, S.M.; Srinivasan, A.; et al. Silencing of High-Mobility Group Box 2 (HMGB2) Modulates Cisplatin and 5-Fluorouracil Sensitivity in Head and Neck Squamous Cell Carcinoma. Proteomics 2015, 15, 383–393. [Google Scholar] [CrossRef]
- Kwon, J.-H.; Kim, J.; Park, J.Y.; Hong, S.M.; Park, C.W.; Hong, S.J.; Park, S.Y.; Choi, Y.J.; Do, I.-G.; Joh, J.-W.; et al. Overexpression of High-Mobility Group Box 2 Is Associated with Tumor Aggressiveness and Prognosis of Hepatocellular Carcinoma. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2010, 16, 5511–5521. [Google Scholar] [CrossRef] [PubMed]
- Mansoori, B.; Mohammadi, A.; Ditzel, H.J.; Duijf, P.H.G.; Khaze, V.; Gjerstorff, M.F.; Baradaran, B. HMGA2 as a Critical Regulator in Cancer Development. Genes 2021, 12, 269. [Google Scholar] [CrossRef]
- Pfannkuche, K.; Summer, H.; Li, O.; Hescheler, J.; Dröge, P. The High Mobility Group Protein HMGA2: A Co-Regulator of Chromatin Structure and Pluripotency in Stem Cells? Stem Cell Rev. Rep. 2009, 5, 224–230. [Google Scholar] [CrossRef]
- Li, Z.; Zhang, Y.; Ramanujan, K.; Ma, Y.; Kirsch, D.G.; Glass, D.J. Oncogenic NRAS, Required for Pathogenesis of Embryonic Rhabdomyosarcoma, Relies upon the HMGA2-IGF2BP2 Pathway. Cancer Res. 2013, 73, 3041–3050. [Google Scholar] [CrossRef]
- De Vita, A.; Vanni, S.; Fausti, V.; Cocchi, C.; Recine, F.; Miserocchi, G.; Liverani, C.; Spadazzi, C.; Bassi, M.; Gessaroli, M.; et al. Deciphering the Genomic Landscape and Pharmacological Profile of Uncommon Entities of Adult Rhabdomyosarcomas. Int. J. Mol. Sci. 2021, 22, 11564. [Google Scholar] [CrossRef]
- De Vita, A.; Ferrari, A.; Miserocchi, G.; Vanni, S.; Domizio, C.; Fonzi, E.; Fausti, V.; Recine, F.; Bassi, M.; Campobassi, A.; et al. Identification of a Novel RAB3IP-HMGA2 Fusion Transcript in an Adult Head and Neck Rhabdomyosarcoma. Oral Dis. 2022, 28, 2052–2054. [Google Scholar] [CrossRef]
- Agaram, N.P.; Huang, S.-C.; Tap, W.D.; Wexler, L.H.; Antonescu, C.R. Clinicopathologic and Survival Correlates of Embryonal Rhabdomyosarcoma Driven by RAS/RAF Mutations. Genes Chromosomes Cancer 2022, 61, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Esmailzadeh, S.; Mansoori, B.; Mohammadi, A.; Shanehbandi, D.; Baradaran, B. SiRNA-Mediated Silencing of HMGA2 Induces Apoptosis and Cell Cycle Arrest in Human Colorectal Carcinoma. J. Gastrointest. Cancer 2017, 48, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Krafft, U.; Tschirdewahn, S.; Hess, J.; Harke, N.N.; Hadaschik, B.; Olah, C.; Krege, S.; Nyirády, P.; Szendröi, A.; Szücs, M.; et al. Validation of Survivin and HMGA2 as Biomarkers for Cisplatin Resistance in Bladder Cancer. Urol. Oncol. Semin. Orig. Investig. 2019, 37, 810.e7–810.e15. [Google Scholar] [CrossRef] [PubMed]
- Liang, L.; Kang, H.; Jia, J. HCP5 Contributes to Cisplatin Resistance in Gastric Cancer through MiR-128/HMGA2 Axis. Cell Cycle Georget. Tex 2021, 20, 1080–1090. [Google Scholar] [CrossRef]
- Miao, J.-T.; Gao, J.-H.; Chen, Y.-Q.; Chen, H.; Meng, H.-Y.; Lou, G. LncRNA ANRIL Affects the Sensitivity of Ovarian Cancer to Cisplatin via Regulation of Let-7a/HMGA2 Axis. Biosci. Rep. 2019, 39, BSR20182101. [Google Scholar] [CrossRef]
- Xiang, Q.; Tang, H.; Yu, J.; Yin, J.; Yang, X.; Lei, X. MicroRNA-98 Sensitizes Cisplatin-Resistant Human Lung Adenocarcinoma Cells by up-Regulation of HMGA2. Int. J. Pharm. Sci. 2013, 68, 274–281. [Google Scholar]
- Germà-Lluch, J.R.; Garcia del Muro, X.; Tabernero, J.M.; Sánchez, M.; Aparicio, J.; Alba, E.; Barnadas, A. BOMP/EPI Intensive Alternating Chemotherapy for IGCCC Poor-Prognosis Germ-Cell Tumors: The Spanish Germ-Cell Cancer Group Experience (GG). Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 1999, 10, 289–293. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New Response Evaluation Criteria in Solid Tumours: Revised RECIST Guideline (Version 1.1). Eur. J. Cancer Oxf. Engl. 1990 2009, 45, 228–247. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient ID | Gender | 1 Age (Years) | Histologic Subtype | Pathology Details | Location | 2 IRS Group | Risk Group | 3 Upfront Syst. Therapy | Surgery |
|---|---|---|---|---|---|---|---|---|---|
| RMS-01 | F | 19.9 | Alveolar | Myo, Des FOXO+ | Limb | IV | Very high risk | IVADo/IVA | Y (R1) |
| RMS-02 | F | 17.2 | Alveolar | Myo, Act, V | Limb | I | High risk | IVA | Y (R0) |
| RMS-03 | M | 21.6 | Alveolar | Myo, Des | Head & Neck | IIb | Very high risk | IVA/V | Y (R0) |
| RMS-04 | M | 16.7 | Embryonal | Myo, Des | Heart | IV | High risk | EPI-IFOS | Y (R0) |
| RMS-05 | M | 27.4 | Embryonal | Des, Act | Pelvis | IV | High risk | BOMP/EPI | Y (R0) |
| RMS-06 | F | 20.8 | Embryonal | Des, Act | Head & Neck | IV | High risk | BOMP/EPI | Y (R0) |
| RMS-07 | F | 42.2 | Alveolar | Des, Act | Head & Neck | IV | Very high risk | BOMP/EPI | N |
| RMS-08 | M | 20.9 | Alveolar | Myo, Act, V. FOXO+ | Head & Neck | III | Very high risk | VAC/IE | Y (R2) |
| RMS-09 | F | 20.8 | Alveolar | Myo, FOXO− | Head & Neck | IIIa | High Risk | VAC/IE | Y (R0) |
| RMS-10 | F | 44.1 | Spindle cell | Myo, Des. FOXO− | Head & Neck | IIIa | High Risk | IVADo | Y (R1) |
| Characteristics | N (%) |
|---|---|
| Previous lines of systemic therapy: | |
| 0 | 3 (30) |
| 1 | 5 (70) |
| 2 | 2 (20) |
| Previous chemotherapy: | |
| IVADo/IVA | 4 (60) |
| VAC/IE | 2 (20) |
| EPI/IFOS | 1 (20) |
| Median of number of cycles (range) of BOMP-EPI | 2.5 (1–8) |
| Toxicity: | |
| • Hematologic: | |
| Grade 3-4 neutropenia | 7 (70) |
| Neutropenic fever | 2 (20) |
| G3-4 Anemia | 2 (20) |
| G3-4 thrombocytopenia | 1 (10) |
| • Non-hematologic: | |
| Grade 2 neuropathy | 1 (10) |
| Grade 2 hearing impairment | 1 (10) |
| Grade 3 mucositis | 1 (10) |
| • Toxic deaths | 0 |
| Patient | Line | Best RECIST Response | PFS (Months) | OS (Months) |
|---|---|---|---|---|
| RMS-01 | 2 | SD | 4.9 | 10.8 |
| RMS-02 | 2 | PR | 8.5 | 24.7 |
| RMS-03 | 2 | SD | 24.3 | 30.5+ |
| RMS-04 | 2 | SD | 8.9 | 18.3 |
| RMS-05 | 1 | PR | 28.9 | 258+ |
| RMS-06 | 1 | PR | 6.2 | 26.2 |
| RMS-07 | 1 | PR | 11.3 | 35.4 |
| RMS-08 | 2 | PD | 1 | 1 |
| RMS-09 | 3 | PR | 3.5 | 3.8 |
| RMS-10 | 3 | PR | 8.3 | 15.7+ |
| RMS-02 * | 3 | PR | 15.8 | 16.2 |
| RMS-04 * | 3 | SD | 9.4 | 9.4 |
| RMS-05 * | 2 | CR | 229+ | 258+ |
| Subtype | Cell Line | cDDP IC50 (µM) |
|---|---|---|
| ERMS | A204 | 7.6 |
| ARMS | RH28 | 7.8 |
| ERMS | Hs729T | 8.7 |
| ARMS | RH41 | 10.3 |
| ARMS | RH30 | 9.7 |
| ERMS | RD | 11.8 |
| Regimen | Type of Study | N | Setting | RR | PFS (Months) | Toxicity | Ref |
|---|---|---|---|---|---|---|---|
| Vinorelbine | Phase II | 33 (13 RMS) | Pediatric sarcoma patients | 50% | 3.5 (all the series) | 63% G3-4 neutropenia | [29] |
| Vinorelbine-Cyclophosphamide | Phase II | 117 (50 RMS) | Pediatric and <25 and adults relapsed tumors | 36% | NR | 38% G3-4 neutropenia | [26] |
| Cyclophosphamide-Topotecan | Retrospective | 15 (6 RMS) | Adult relapsed sarcoma patients | 33% (2/6) | 2.5 (all the series) | 47% hematologic toxicity | [30] |
| Cyclophosphamide-Topotecan | Phase II window trial | 61 | Pediatric metastatic RMS (1st line) | 47% | NR (3-y DFS: 10%) | G3-4: leucopenia 52%, anemia 37% | [31] |
| Cyclophosphamide-Topotecan | Phase II | 91 (15 RMS) | Pediatric relapsed tumors | 66% (10/15 RMS) | NR | G3-4: leucopenia 53%, anemia 27% | [32] |
| Vincristine-Irinotecan | Phase II window trial (2 regimens) | 92 | Pediatric relapsed RMS | 26–37% | NR (1y-FFS 37 and 38%) | ≥G3: 50–66% | [33] |
| Vincristine-temozolomide-irinotecan | Retrospective | 19 | Pediatric relapsed RMS | 0 | PFS-3 months: 23% | NR | [34] |
| Topotecan-carboplatin | Phase II | 38 | Pediatric relapsed RMS | 28% | 5-y PFS 14% | 63% G4 hematologic | [13] |
| Cisplatin-etoposide | Phase II | 27 (21 RMS) | Pediatric relapsed tumors | 33% (7/21) | NR | NR | [12] |
| Ifosfamide-carboplatin-etoposide (ICE) | Phase I and II trials analysis | 97 (27 RMS) | Pediatric and adolescent relapse sarcoma | 66% (RMS) | NR | G3-4 hematologic: 100% | [36] |
| Vincristine, ifosfamide and doxorubicin (VIA)/etoposide, ifosfamide and cisplatin (VIP) | Retrospective | 6 | Adult patients (advance disease) | 100% | NR | NR | [28] |
| Several regimenes | Retrospective | 49 | Pediatric relapsed RMS | NR | NR | [10] | |
| Carboplatin-epirubicin- vincristine ad ifosfamide-vincristine- etoposide (CEV/IVE) | 15 | 73.3% | |||||
| Vincristine/irinotecan ± temozolomide (VI[T]) | 7 | 42.9% | |||||
| Gemcitabine-docetaxel | Retrospective | 19 (5 RMS) | Pediatric relapsed sarcoma | 40% (2/5) | 2 (all series) | G3-4 toxicity 74% | [35] |
| BOMP | EPI |
|---|---|
| Day 1: Vincristine 2 mg bolus iv Methotrexate 100 mg/m2 iv in 20′ Methotrexate 200 mg/m2 in 12 h infusion | Days 1–4: Cisplatin 25 mg/m2 in 30′ Etoposide 120 mg/m2 in 90′ Ifosfamide 1300 mg/m2 in 60′ MESNA rescues as per protocol |
| Day 2: Bleomycin 30 mg in 12 h infusion | |
| Day 3: Cisplatin 100 mg/m2 in 30′ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hindi, N.; Carrillo-García, J.; Blanco-Alcaina, E.; Renshaw, M.; Luna, P.; Durán, J.; Jiménez, N.; Sancho, P.; Ramos, R.; Moura, D.S.; et al. Platinum-Based Regimens Are Active in Advanced Pediatric-Type Rhabdomyosarcoma in Adults and Depending on HMGB1 Expression. Int. J. Mol. Sci. 2023, 24, 856. https://doi.org/10.3390/ijms24010856
Hindi N, Carrillo-García J, Blanco-Alcaina E, Renshaw M, Luna P, Durán J, Jiménez N, Sancho P, Ramos R, Moura DS, et al. Platinum-Based Regimens Are Active in Advanced Pediatric-Type Rhabdomyosarcoma in Adults and Depending on HMGB1 Expression. International Journal of Molecular Sciences. 2023; 24(1):856. https://doi.org/10.3390/ijms24010856
Chicago/Turabian StyleHindi, Nadia, Jaime Carrillo-García, Elena Blanco-Alcaina, Marta Renshaw, Pablo Luna, José Durán, Natalia Jiménez, Pilar Sancho, Rafael Ramos, David S. Moura, and et al. 2023. "Platinum-Based Regimens Are Active in Advanced Pediatric-Type Rhabdomyosarcoma in Adults and Depending on HMGB1 Expression" International Journal of Molecular Sciences 24, no. 1: 856. https://doi.org/10.3390/ijms24010856
APA StyleHindi, N., Carrillo-García, J., Blanco-Alcaina, E., Renshaw, M., Luna, P., Durán, J., Jiménez, N., Sancho, P., Ramos, R., Moura, D. S., & Martín-Broto, J. (2023). Platinum-Based Regimens Are Active in Advanced Pediatric-Type Rhabdomyosarcoma in Adults and Depending on HMGB1 Expression. International Journal of Molecular Sciences, 24(1), 856. https://doi.org/10.3390/ijms24010856