
Heterogeneity of Mismatch Repair Status and Microsatellite Instability between Primary Tumour and Metastasis and Its Implications for Immunotherapy in Colorectal Cancers

 ,
, 
 , , , , , add
Show full author list
, , , , , add
Show full author list
Abstract
:1. Introduction
2. Results
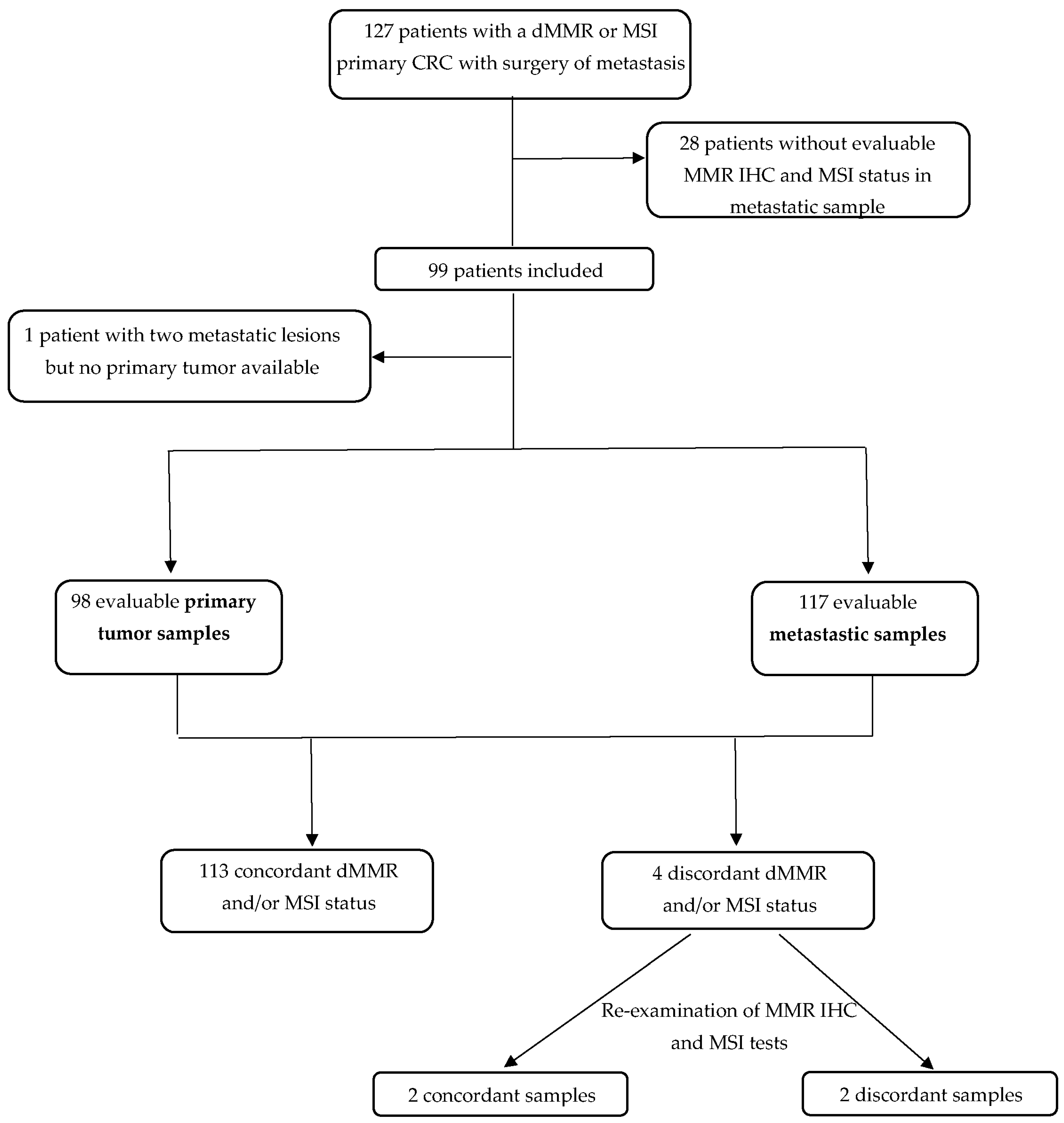
2.1. Study Population
2.2. Metastatic Samples
2.3. Concordance of MMR Immunohistochemistry and MSI Status between Primary Tumors and Paired Metastases
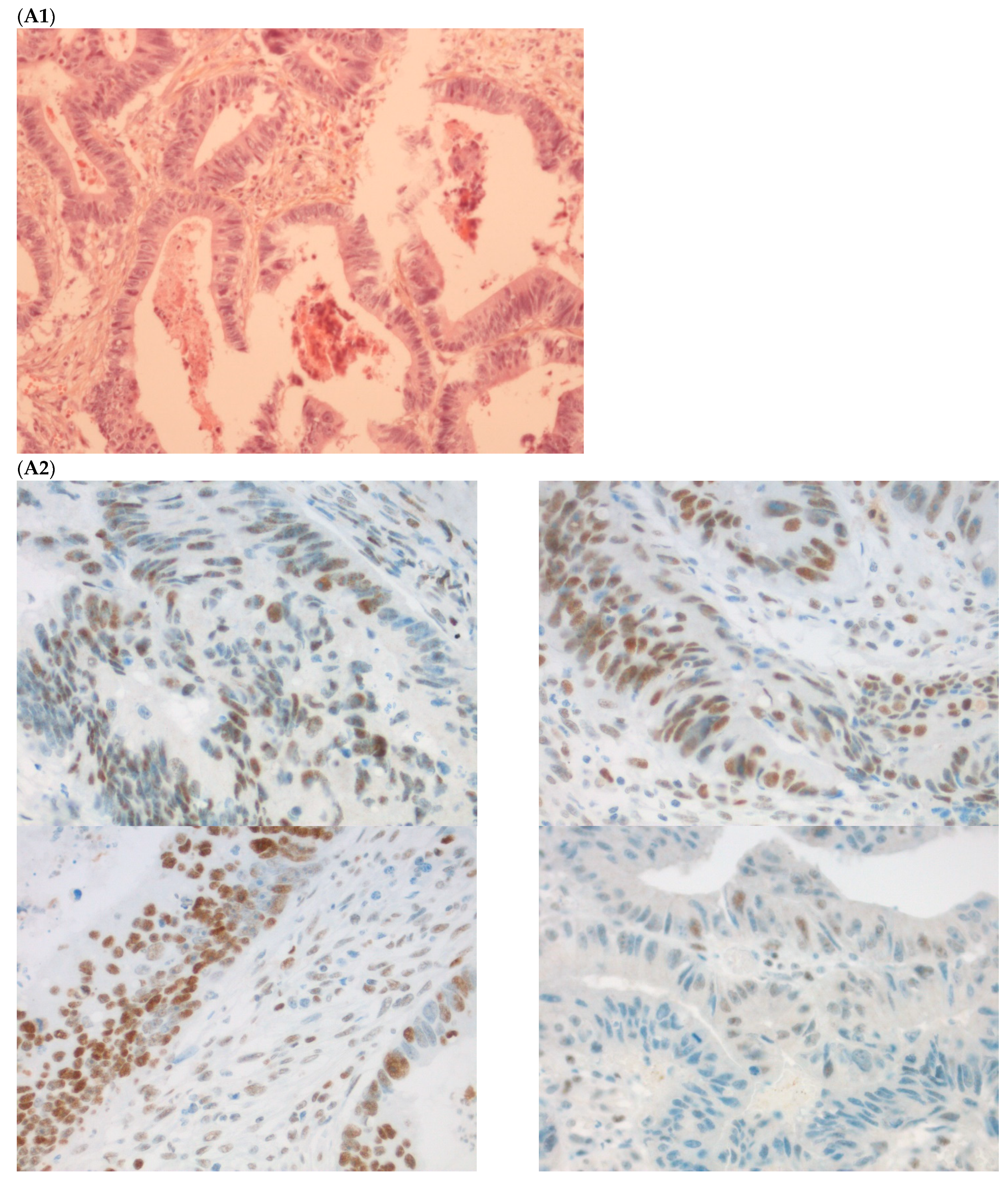
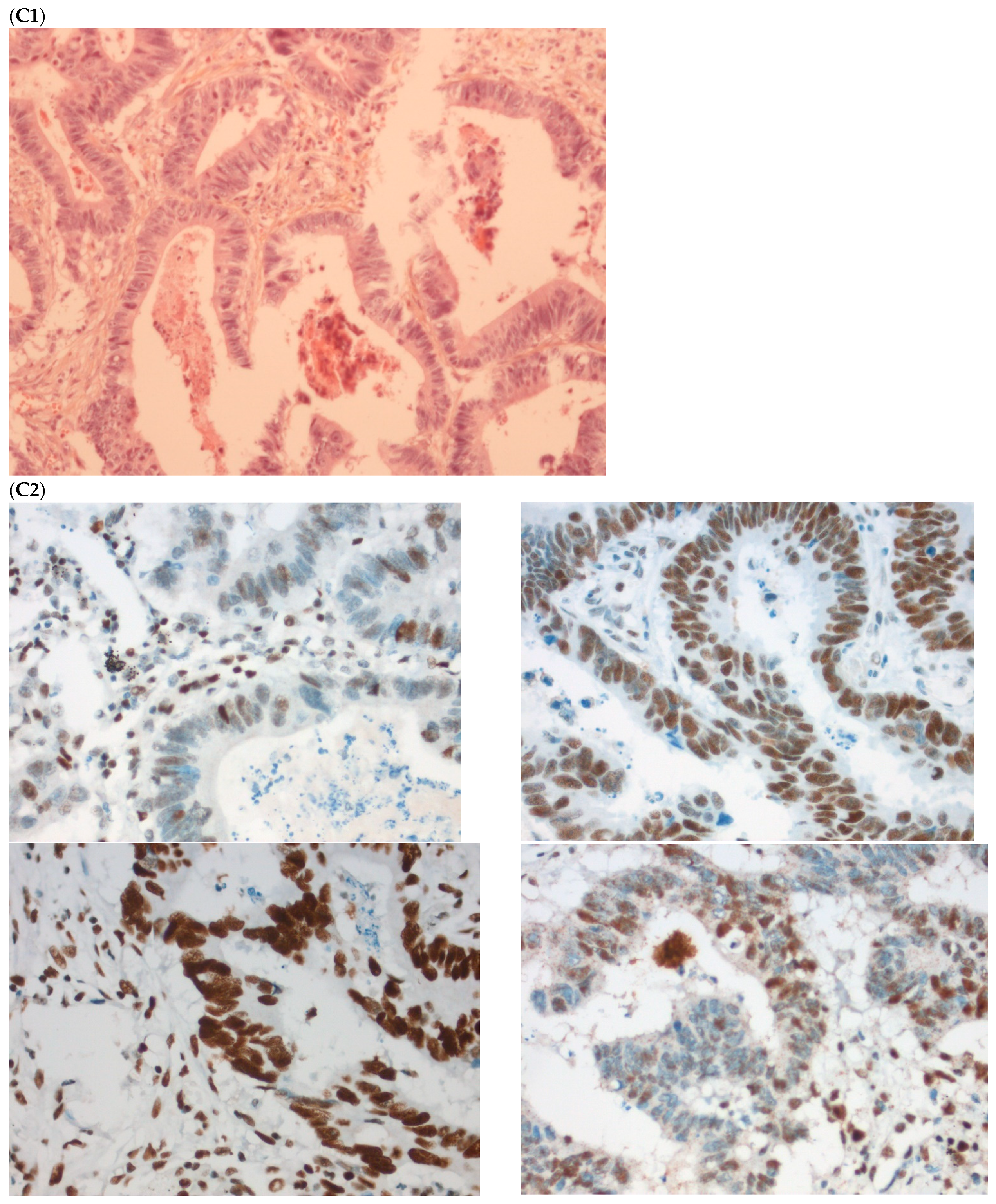
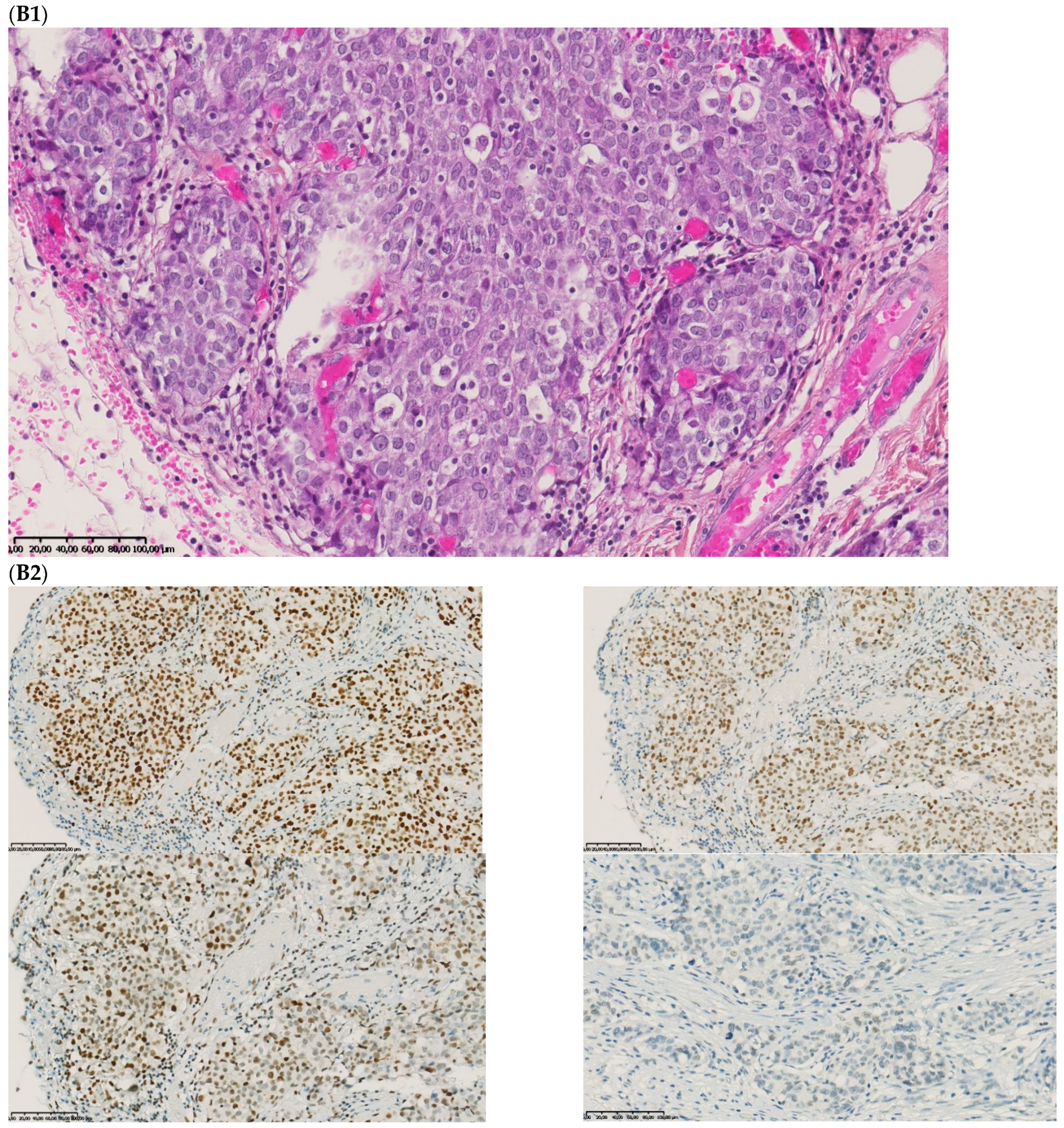
2.4. Description of the Four Cases with Discordant MMR IHC and MSI Status between Primary Tumors and Paired Metastases
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. MMR Immunohistochemistry and MSI Tests
4.3. Patient and Tumor Characteristics
4.4. Statistical Analyses
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Arnold, M.; Sierra, M.S.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Patterns and Trends in Colorectal Cancer Incidence and Mortality. Gut 2017, 66, 683–691. [Google Scholar] [CrossRef] [Green Version]
- Jass, J.R. Classification of Colorectal Cancer Based on Correlation of Clinical, Morphological and Molecular Features. Histopathology 2007, 50, 113–130. [Google Scholar] [CrossRef]
- Hampel, H.; Frankel, W.L.; Martin, E.; Arnold, M.; Khanduja, K.; Kuebler, P.; Clendenning, M.; Sotamaa, K.; Prior, T.; Westman, J.A.; et al. Feasibility of Screening for Lynch Syndrome among Patients with Colorectal Cancer. J. Clin. Oncol. 2008, 26, 5783–5788. [Google Scholar] [CrossRef]
- Tougeron, D.; Fauquembergue, E.; Rouquette, A.; Le Pessot, F.; Sesboüé, R.; Laurent, M.; Berthet, P.; Mauillon, J.; Di Fiore, F.; Sabourin, J.-C.; et al. Tumor-Infiltrating Lymphocytes in Colorectal Cancers with Microsatellite Instability Are Correlated with the Number and Spectrum of Frameshift Mutations. Mod. Pathol. 2009, 22, 1186–1195. [Google Scholar] [CrossRef] [Green Version]
- Le, D.T.; Durham, J.N.; Smith, K.N.; Wang, H.; Bartlett, B.R.; Aulakh, L.K.; Lu, S.; Kemberling, H.; Wilt, C.; Luber, B.S.; et al. Mismatch-Repair Deficiency Predicts Response of Solid Tumors to PD-1 Blockade. Science 2017, 357, 409–413. [Google Scholar] [CrossRef] [Green Version]
- André, T.; Shiu, K.-K.; Kim, T.W.; Jensen, B.V.; Jensen, L.H.; Punt, C.; Smith, D.; Garcia-Carbonero, R.; Benavides, M.; Gibbs, P.; et al. Pembrolizumab in Microsatellite-Instability–High Advanced Colorectal Cancer. N. Engl. J. Med. 2020, 383, 2207–2218. [Google Scholar] [CrossRef]
- Jaffrelot, M.; Selves, J.; Fares, N.; Staub, A.; Laurenty, A.P.; Danjoux, M.; Meilleroux, J.; Chipoulet, E.; Toulas, C.; Guimbaud, R. Characterization of Atypical DMMR (Deficient MisMatch Repair) Tumors: A Study from a Large Cohort of 4948 Cases. Ann. Oncol. 2019, 30, v807. [Google Scholar] [CrossRef]
- Guyot D’Asnières De Salins, A.; Tachon, G.; Cohen, R.; Karayan-Tapon, L.; Junca, A.; Frouin, E.; Godet, J.; Evrard, C.; Randrian, V.; Duval, A.; et al. Discordance between Immunochemistry of Mismatch Repair Proteins and Molecular Testing of Microsatellite Instability in Colorectal Cancer. ESMO Open 2021, 6, 100120. [Google Scholar] [CrossRef]
- Suraweera, N.; Duval, A.; Reperant, M.; Vaury, C.; Furlan, D.; Leroy, K.; Seruca, R.; Iacopetta, B.; Hamelin, R. Evaluation of Tumor Microsatellite Instability Using Five Quasimonomorphic Mononucleotide Repeats and Pentaplex PCR. Gastroenterology 2002, 123, 1804–1811. [Google Scholar] [CrossRef]
- Luchini, C.; Bibeau, F.; Ligtenberg, M.J.L.; Singh, N.; Nottegar, A.; Bosse, T.; Miller, R.; Riaz, N.; Douillard, J.-Y.; Andre, F.; et al. ESMO Recommendations on Microsatellite Instability Testing for Immunotherapy in Cancer, and Its Relationship with PD-1/PD-L1 Expression and Tumour Mutational Burden: A Systematic Review-Based Approach. Ann. Oncol. 2019, 30, 1232–1243. [Google Scholar] [CrossRef] [Green Version]
- Cohen, R.; Hain, E.; Buhard, O.; Guilloux, A.; Bardier, A.; Kaci, R.; Bertheau, P.; Renaud, F.; Bibeau, F.; Fléjou, J.-F.; et al. Association of Primary Resistance to Immune Checkpoint Inhibitors in Metastatic Colorectal Cancer with Misdiagnosis of Microsatellite Instability or Mismatch Repair Deficiency Status. JAMA Oncol. 2019, 5, 551–555. [Google Scholar] [CrossRef]
- Jeantet, M.; Tougeron, D.; Tachon, G.; Cortes, U.; Archambaut, C.; Fromont, G.; Karayan-Tapon, L. High Intra- and Inter-Tumoral Heterogeneity of RAS Mutations in Colorectal Cancer. Int. J. Mol. Sci. 2016, 17, 2015. [Google Scholar] [CrossRef] [Green Version]
- Haraldsdottir, S.; Roth, R.; Pearlman, R.; Hampel, H.; Arnold, C.A.; Frankel, W.L. Mismatch Repair Deficiency Concordance between Primary Colorectal Cancer and Corresponding Metastasis. Fam. Cancer 2016, 15, 253–260. [Google Scholar] [CrossRef]
- Jung, J.; Kang, Y.; Lee, Y.J.; Kim, E.; Ahn, B.; Lee, E.; Kim, J.Y.; Lee, J.H.; Lee, Y.; Kim, C.H.; et al. Comparison of the Mismatch Repair System between Primary and Metastatic Colorectal Cancers Using Immunohistochemistry. J. Pathol. Transl. Med. 2017, 51, 129–136. [Google Scholar] [CrossRef] [Green Version]
- Fujiyoshi, K.; Yamamoto, G.; Takahashi, A.; Arai, Y.; Yamada, M.; Kakuta, M.; Yamaguchi, K.; Akagi, Y.; Nishimura, Y.; Sakamoto, H.; et al. High Concordance Rate of KRAS/BRAF Mutations and MSI-H between Primary Colorectal Cancer and Corresponding Metastases. Oncol. Rep. 2017, 37, 785–792. [Google Scholar] [CrossRef] [Green Version]
- He, W.-Z.; Hu, W.-M.; Wang, F.; Rong, Y.-M.; Yang, L.; Xie, Q.-K.; Yang, Y.-Z.; Jiang, C.; Qiu, H.-J.; Lu, J.-B.; et al. Comparison of Mismatch Repair Status between Primary and Matched Metastatic Sites in Patients with Colorectal Cancer. J. Natl. Compr. Cancer Netw. 2019, 17, 1174–1183. [Google Scholar] [CrossRef]
- Overbeek, L.I.H.; Ligtenberg, M.J.L.; Willems, R.W.; Hermens, R.P.M.G.; Blokx, W.A.M.; Dubois, S.V.; van der Linden, H.; Meijer, J.W.R.; Mlynek-Kersjes, M.L.; Hoogerbrugge, N.; et al. Interpretation of Immunohistochemistry for Mismatch Repair Proteins Is Only Reliable in a Specialized Setting. Am. J. Surg. Pathol. 2008, 32, 1246. [Google Scholar] [CrossRef]
- Wang, Y.; Shi, C.; Eisenberg, R.; Vnencak-Jones, C.L. Differences in Microsatellite Instability Profiles between Endometrioid and Colorectal Cancers. J. Mol. Diagn. 2017, 19, 57–64. [Google Scholar] [CrossRef] [Green Version]
- Berger, Y.; Jacoby, H.; Kaufmann, M.I.; Ben-Yaacov, A.; Westreich, G.; Sharon, I.; Barda, L.; Sharif, N.; Nadler, R.; Horesh, N.; et al. Correlation Between Intraoperative and Pathological Findings for Patients Undergoing Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy. Ann. Surg. Oncol. 2019, 26, 1103–1109. [Google Scholar] [CrossRef]
- Larsen, N.B.; Engel, P.J.H.; Rasmussen, M.; Rasmussen, L.J. Differential Expression of HMLH1 in Sporadic Human Colorectal Cancer Tumors and Distant Metastases. Apmis 2009, 117, 839–848. [Google Scholar] [CrossRef]
- Tachon, G.; Frouin, E.; Karayan-Tapon, L.; Auriault, M.-L.; Godet, J.; Moulin, V.; Wang, Q.; Tougeron, D. Heterogeneity of Mismatch Repair Defect in Colorectal Cancer and Its Implications in Clinical Practice. Eur. J. Cancer 2018, 95, 112–116. [Google Scholar] [CrossRef] [PubMed]
- Le, D.T.; Uram, J.N.; Wang, H.; Bartlett, B.R.; Kemberling, H.; Eyring, A.D.; Skora, A.D.; Luber, B.S.; Azad, N.S.; Laheru, D.; et al. PD-1 Blockade in Tumors with Mismatch-Repair Deficiency. N. Engl. J. Med. 2015, 372, 2509–2520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, R.; Duval, A.; Svrcek, M. Primary Resistance to Immune Checkpoint Inhibitors in Metastatic Colorectal Cancer—Beyond the Misdiagnosis—In Reply. JAMA Oncol. 2019, 5, 741. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, J.B.; Wu, W.; Borras, E.; Masand, G.; Cuddy, A.; Mork, M.E.; Bannon, S.A.; Lynch, P.M.; Rodriguez-Bigas, M.; Taggart, M.W.; et al. Can Microsatellite Status of Colorectal Cancer Be Reliably Assessed after Neoadjuvant Therapy? Clin. Cancer Res. 2017, 23, 5246–5254. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Zhao, X.; Gao, C.; Gong, J.; Wang, X.; Gao, J.; Li, Z.; Wang, J.; Yang, B.; Wang, L.; et al. Plasma-Based Microsatellite Instability Detection Strategy to Guide Immune Checkpoint Blockade Treatment. J. Immunother. Cancer 2020, 8, e001297. [Google Scholar] [CrossRef]
- Shia, J. Evolving approach and clinical significance of detecting DNA mismatch repair deficiency in colorectal carcinoma. Semin. Diagn. Pathol. 2015, 32, 352–361. [Google Scholar] [CrossRef] [Green Version]
- Tougeron, D.; Sueur, B.; Zaanan, A.; de la Fouchardiére, C.; Sefrioui, D.; Lecomte, T.; Aparicio, T.; Guetz, G.D.; Artru, P.; Hautefeuille, V.; et al. Prognosis and Chemosensitivity of Deficient MMR Phenotype in Patients with Metastatic Colorectal Cancer: An AGEO Retrospective Multicenter Study. Int. J. Cancer 2020, 147, 285–296. [Google Scholar] [CrossRef]
- Carethers, J.M.; Stoffel, E.M. Lynch Syndrome and Lynch Syndrome Mimics: The Growing Complex Landscape of Hereditary Colon Cancer. World J. Gastroenterol. WJG 2015, 21, 9253–9261. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics (n = 99) | n (%) |
|---|---|
| Median age (years, range) | 59.0 [17, 98] |
| Gender (n = 99) | |
| Female | 47 (47.5%) |
| Male | 52 (52.5%) |
| TNM stage at diagnosis (n = 99) | |
| I–II | 14 (14.2%) |
| III | 31 (31.3%) |
| IV | 54 (54.5%) |
| Primary tumour site (n = 98 *) | |
| Right colon | 65 (66.3%) |
| Left colon | 28 (28.6%) |
| Rectum | 5 (5.1%) |
| Grade (n = 98 *) | |
| Poorly differentiated | 38 (39.6%) |
| Moderately differentiated | 43 (44.8%) |
| Well differentiated | 15 (15.6%) |
| Missing | 2 |
| RAS status on primary tumors (n = 98 *) | |
| Mutated | 20 (23.3%) |
| Wild-type | 66 (76.7%) |
| Missing | 12 |
| BRAFV600E status on primary tumors (n = 98 *) | |
| Mutated | 36 (38.3%) |
| Wild-type | 58 (61.7%) |
| Missing | 4 |
| MLH1 promoter hypermethylation (n = 75 **) | |
| Yes | 46 (70.8%) |
| No | 19 (29.2%) |
| Missing | 10 |
| Lynch syndrome or sporadic cases (n = 99) | |
| Proven Lynch syndrome (MMR gene mutation) | 20 (20.8%) |
| Suspected Lynch syndrome | 21 (21.9%) |
| Sporadic case | 55 (57.3%) |
| Missing | 3 |
| Characteristics (n, %) | Primary Tumors (n = 98) | Metastases (n = 117) |
|---|---|---|
| Chemotherapy or radiochemotherapy before testing | ||
| Yes | 7 (7.1%) | 39 (34.2%) |
| No | 91 (92.9%) | 75 (65.8%) |
| Missing | 0 | 3 |
| Synchronous/metachronous | - | 55 (47.0%)/62 (53.0%) |
| Site of metastases | - | |
| Peritoneum | - | 54 (46.2%) |
| Liver | - | 28 (23.9%) |
| Lymph nodes | - | 14 (12.0%) |
| Lung | - | 6 (5.1%) |
| Others | - | 15 (12.8%) |
| MMR IHC status | ||
| Loss of MLH1 and PMS2 expression | 69 (70.4%) | 72 (61.5%) |
| Loss of MSH2 and MSH6 expression | 17 (17.3%) | 21 (18.7%) |
| Isolated loss of PMS2 expression | 6 (6.1%) | 10 (8.9%) |
| Isolated loss of MSH6 expression | 2 (2.1%) | 1 (0.9%) |
| Others | 4 (4.1%) | 4 (3.6%) |
| pMMR | 0 | 4 (3.6%) |
| Missing | 0 | 5 |
| MSI test | ||
| MSI | 98 (100%) | 99 (96.1%) |
| MSS | 0 | 4 (3.9%) |
| Missing | 0 | 14 |
| MMR IHC and MSI tests | 98/98 (100%) | 98/117 (83.8%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Evrard, C.; Messina, S.; Sefrioui, D.; Frouin, É.; Auriault, M.-L.; Chautard, R.; Zaanan, A.; Jaffrelot, M.; De La Fouchardière, C.; Aparicio, T.; et al. Heterogeneity of Mismatch Repair Status and Microsatellite Instability between Primary Tumour and Metastasis and Its Implications for Immunotherapy in Colorectal Cancers. Int. J. Mol. Sci. 2022, 23, 4427. https://doi.org/10.3390/ijms23084427
Evrard C, Messina S, Sefrioui D, Frouin É, Auriault M-L, Chautard R, Zaanan A, Jaffrelot M, De La Fouchardière C, Aparicio T, et al. Heterogeneity of Mismatch Repair Status and Microsatellite Instability between Primary Tumour and Metastasis and Its Implications for Immunotherapy in Colorectal Cancers. International Journal of Molecular Sciences. 2022; 23(8):4427. https://doi.org/10.3390/ijms23084427
Chicago/Turabian StyleEvrard, Camille, Stéphane Messina, David Sefrioui, Éric Frouin, Marie-Luce Auriault, Romain Chautard, Aziz Zaanan, Marion Jaffrelot, Christelle De La Fouchardière, Thomas Aparicio, and et al. 2022. "Heterogeneity of Mismatch Repair Status and Microsatellite Instability between Primary Tumour and Metastasis and Its Implications for Immunotherapy in Colorectal Cancers" International Journal of Molecular Sciences 23, no. 8: 4427. https://doi.org/10.3390/ijms23084427
APA StyleEvrard, C., Messina, S., Sefrioui, D., Frouin, É., Auriault, M.-L., Chautard, R., Zaanan, A., Jaffrelot, M., De La Fouchardière, C., Aparicio, T., Coriat, R., Godet, J., Silvain, C., Randrian, V., Sabourin, J.-C., Guimbaud, R., Miquelestorena-Standley, E., Lecomte, T., Moulin, V., ... Tougeron, D. (2022). Heterogeneity of Mismatch Repair Status and Microsatellite Instability between Primary Tumour and Metastasis and Its Implications for Immunotherapy in Colorectal Cancers. International Journal of Molecular Sciences, 23(8), 4427. https://doi.org/10.3390/ijms23084427