
Oral Toxicokinetics, Tissue Distribution, and 28-Day Oral Toxicity of Two Differently Manufactured Food Additive Silicon Dioxides



Abstract
:1. Introduction
2. Results and Discussion
2.1. Physicochemical Properties
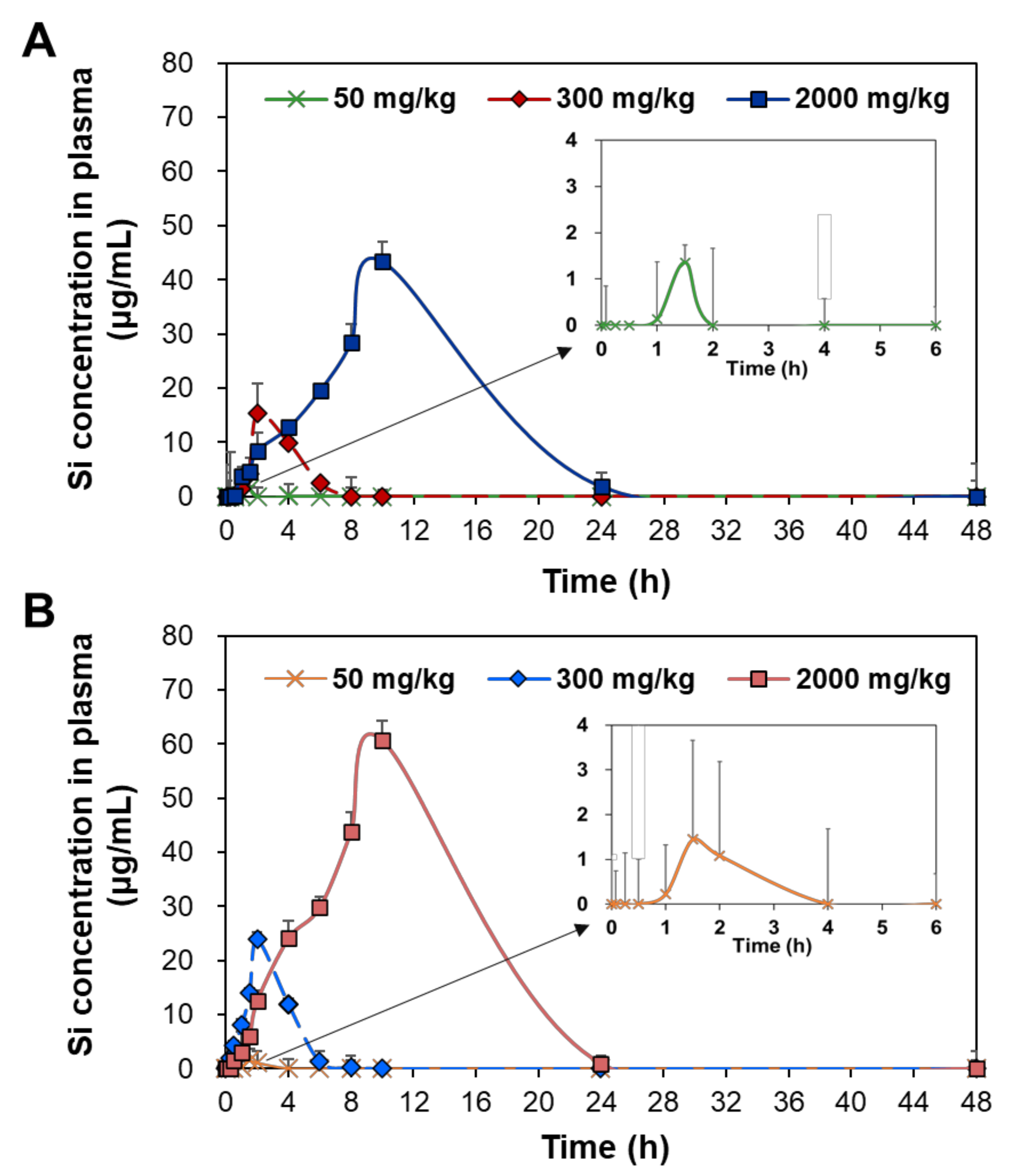
2.2. Plasma Concentration–Time Profiles
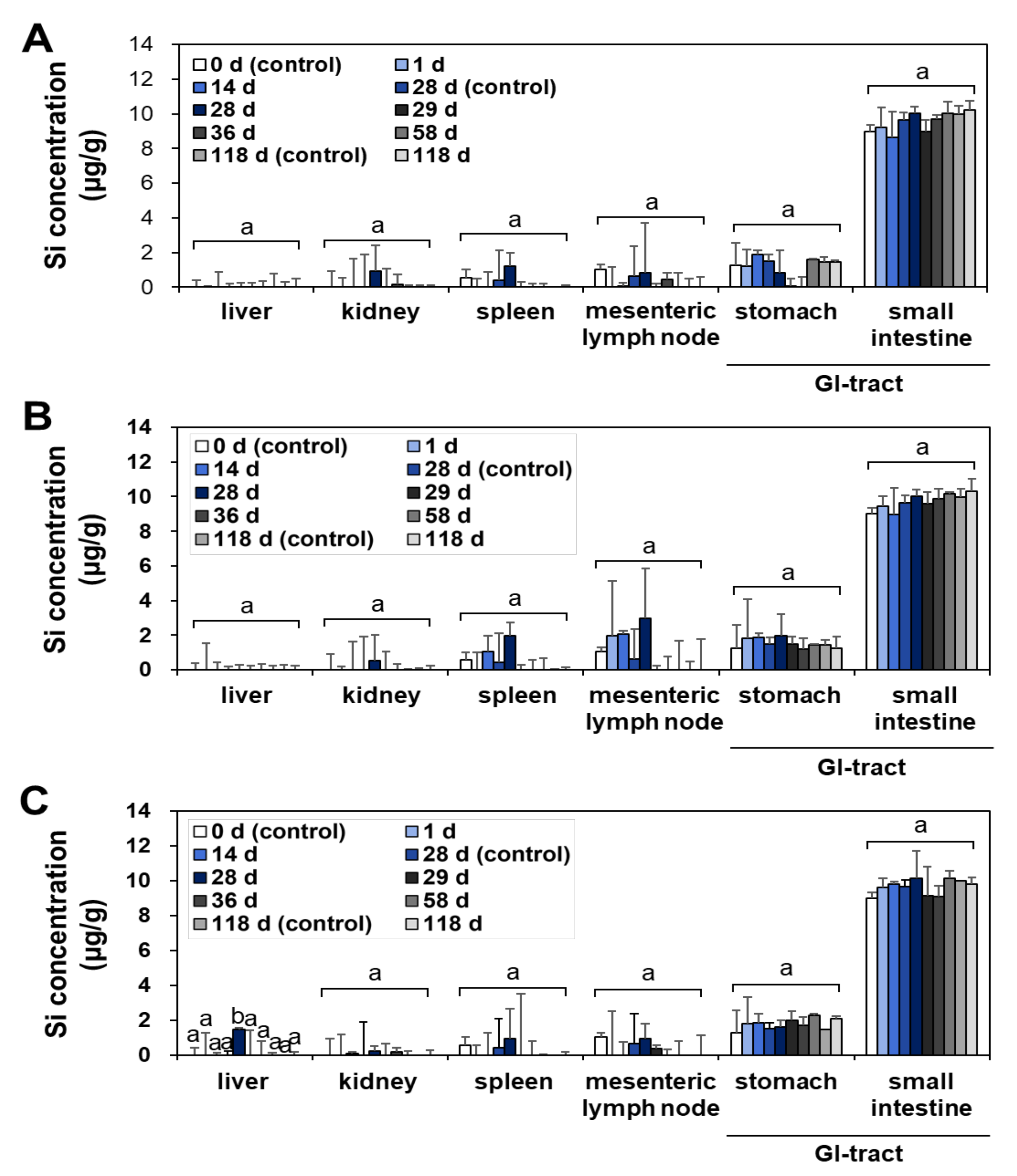
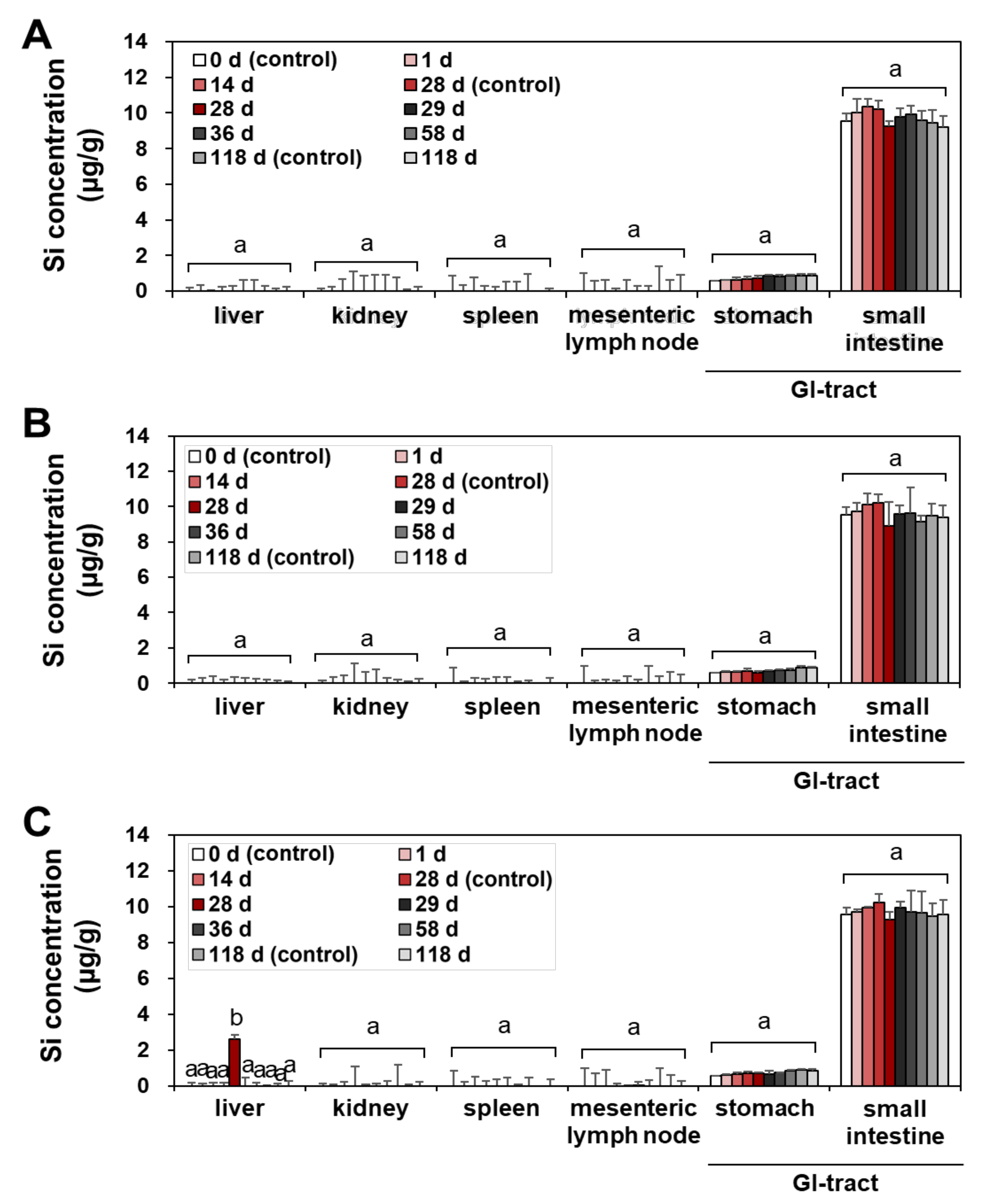
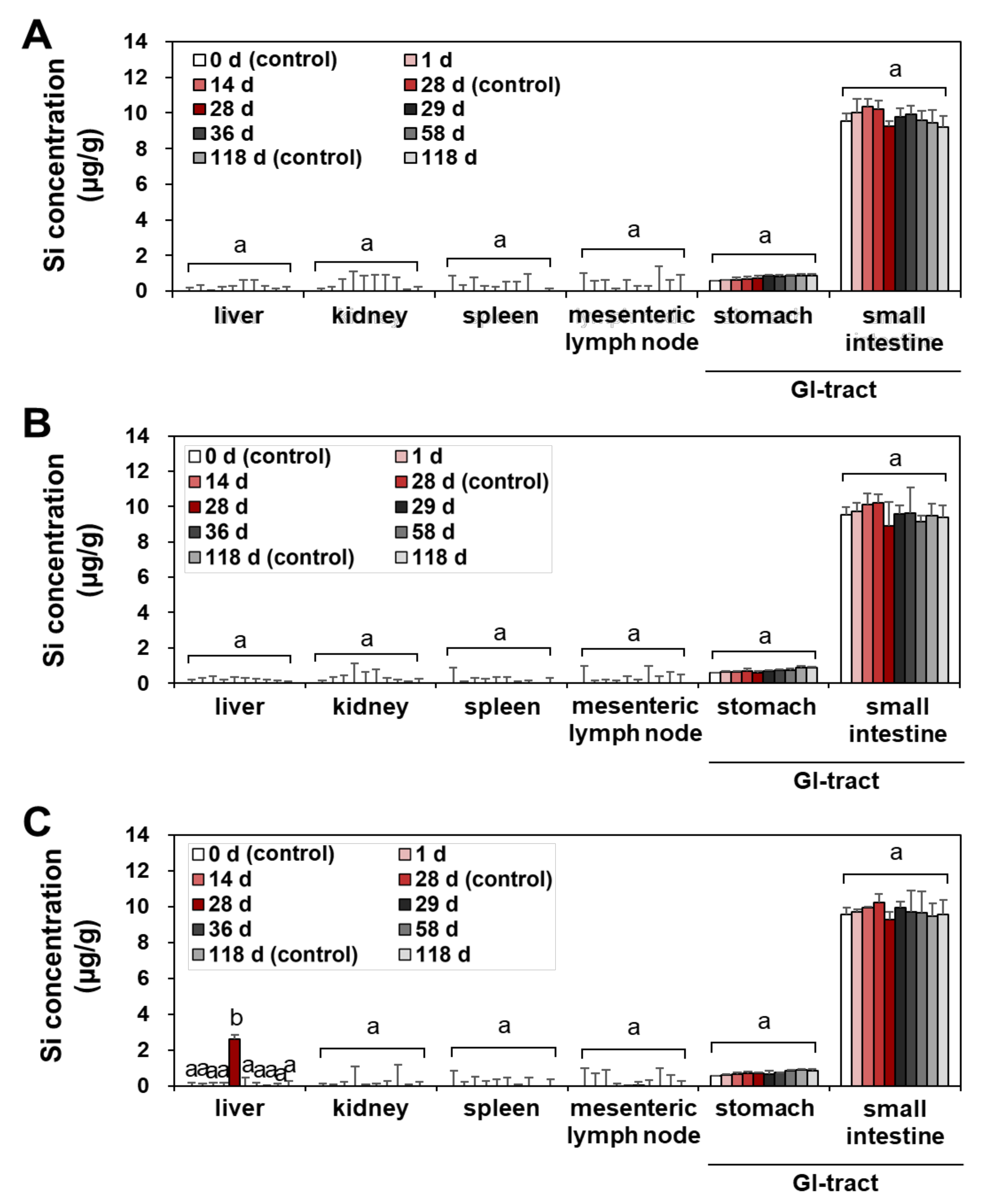
2.3. Tissue Distribution
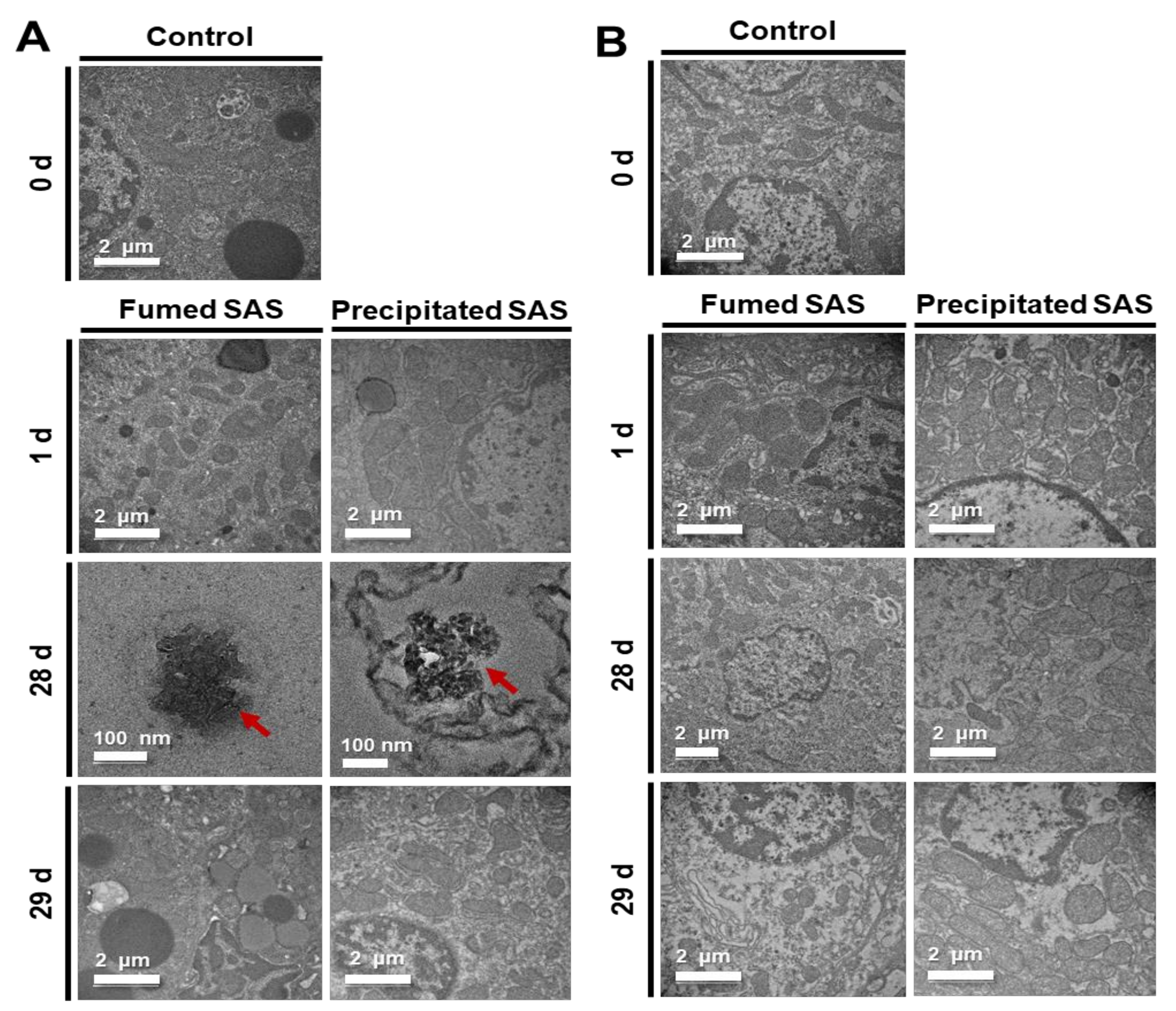
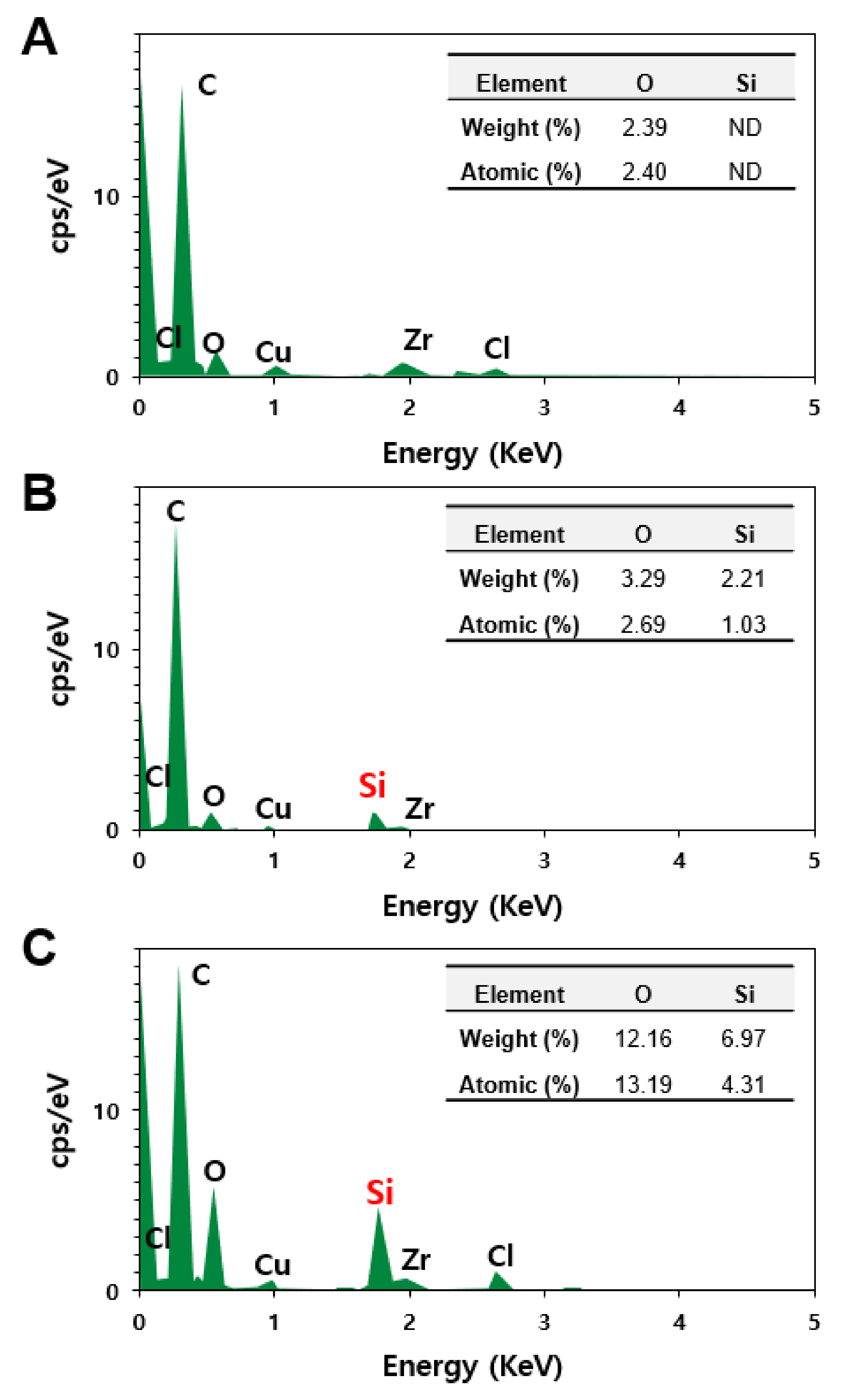
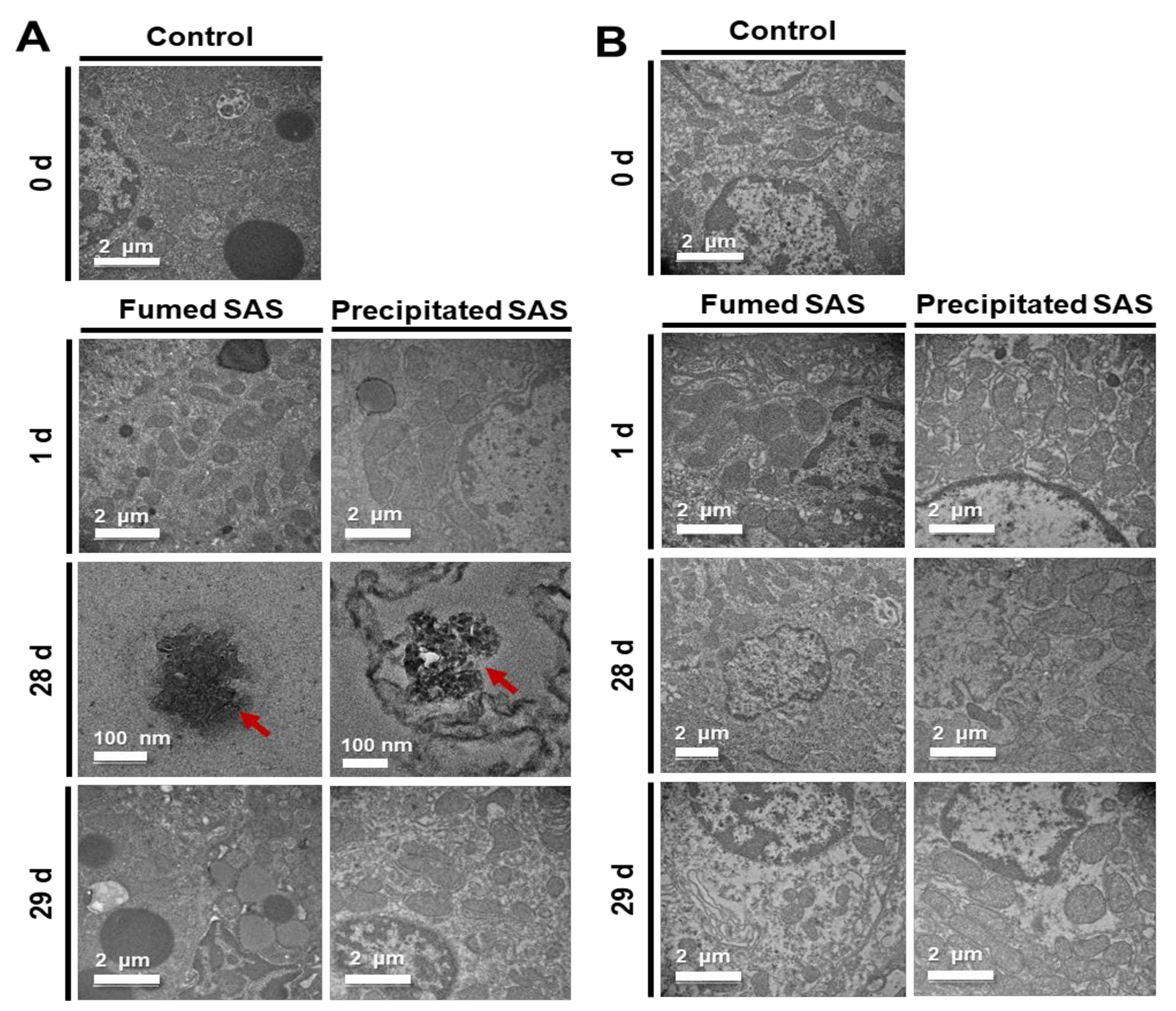
2.4. Tissue Distribution Fates
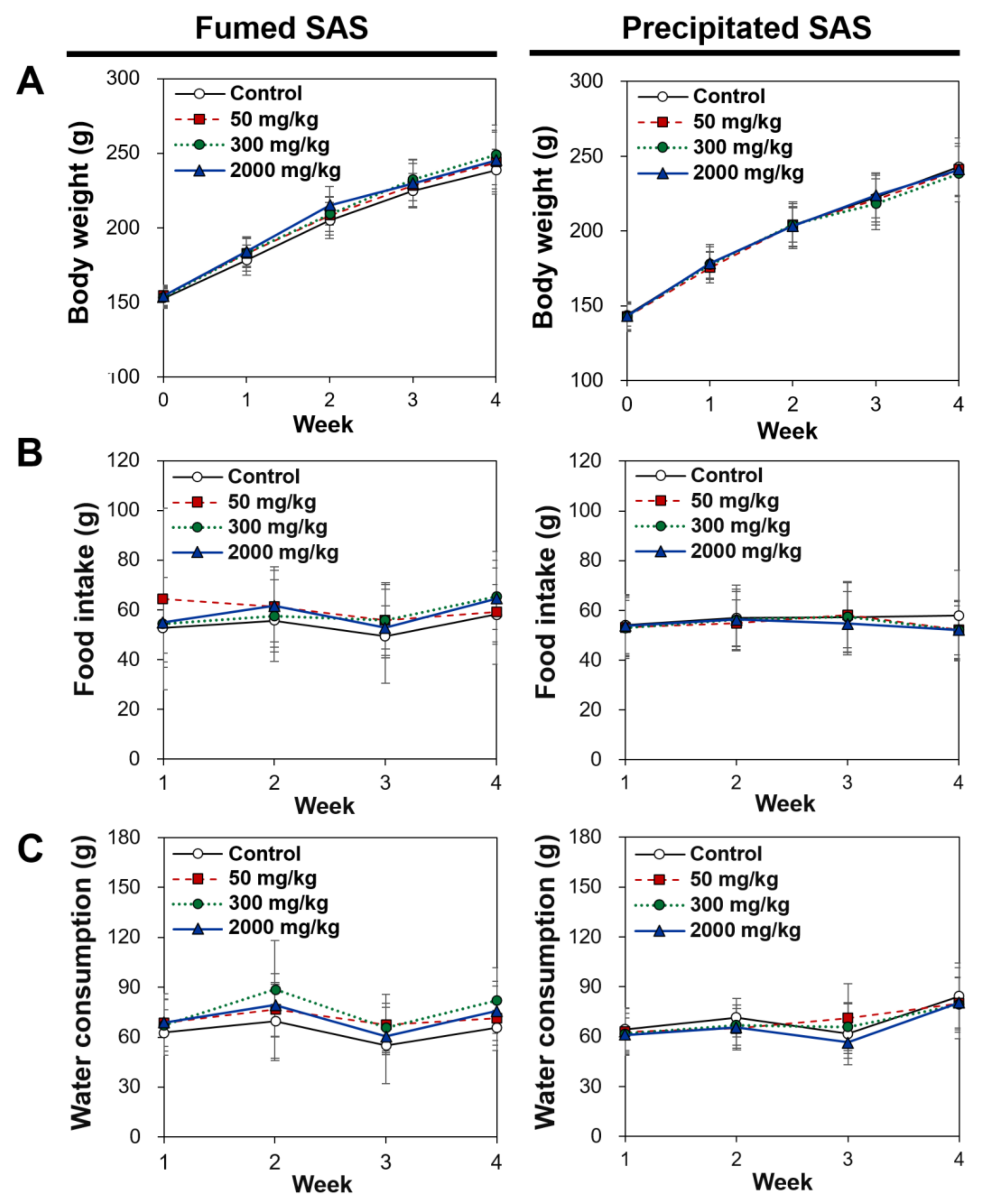
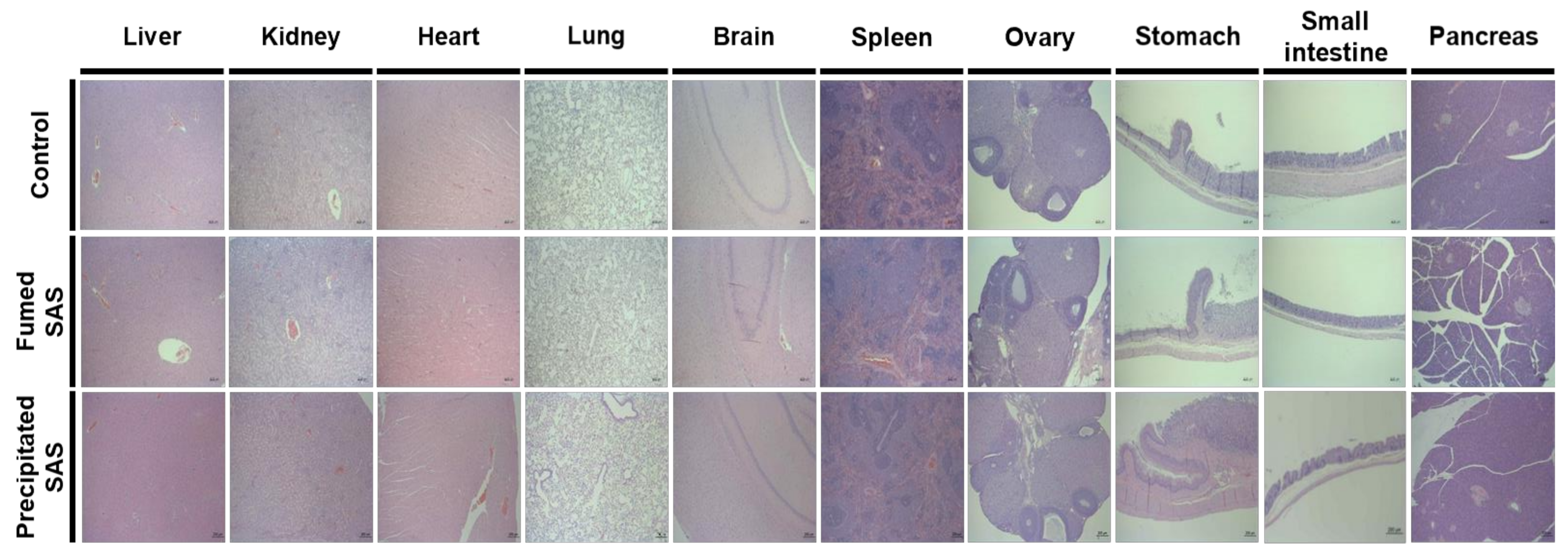
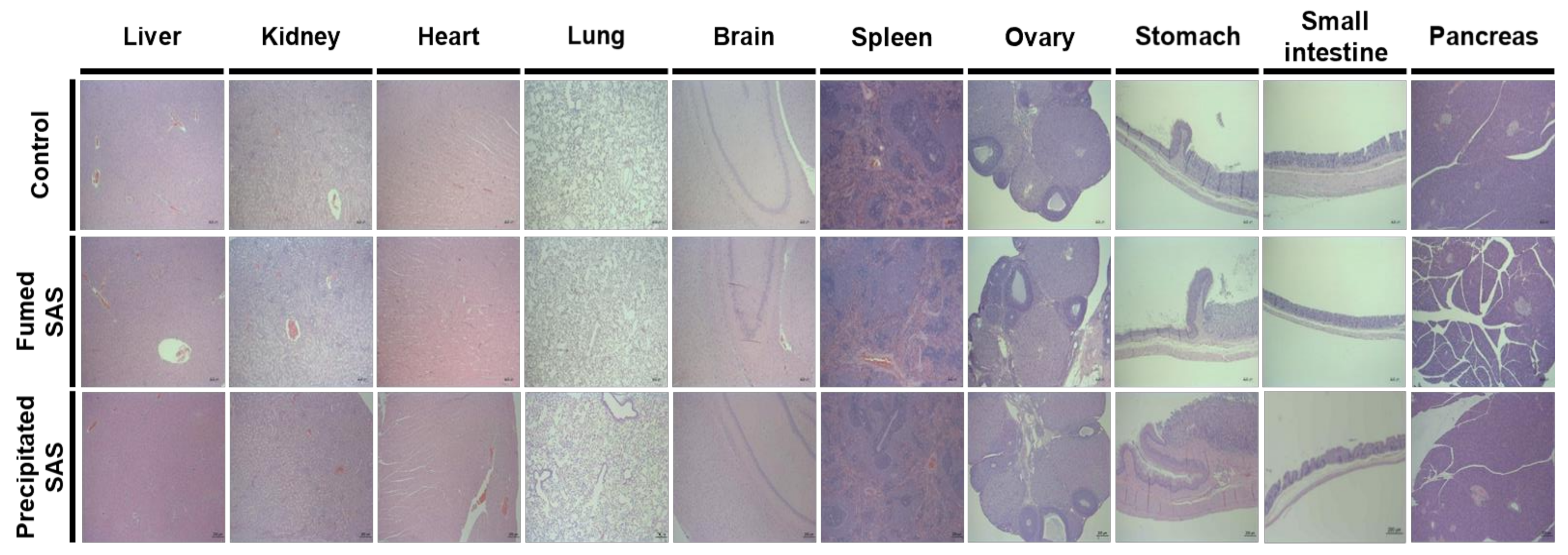
2.5. Twenty-Eight-Day Repeated Oral Toxicity
3. Materials and Methods
3.1. Materials
3.2. Animals
3.3. Microwave Digestion and ICP–AES Analysis
3.4. Plasma Concentration–Time Profiles
3.5. Tissue Distribution after 28-d Repeated Oral Administration
3.6. Twenty-Eight-Day Repeated Oral Toxicity
3.7. TEM–EDS Analysis
3.8. Statistical Analysis
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dera, M.W.W.; Teseme, W.B. Review on the application of food nanotechnology in food processing. Am. J. Eng. Technol. Manag. 2020, 5, 41–47. [Google Scholar] [CrossRef]
- Fruijtier-Polloth, C. The safety of nanostructured synthetic amorphous silica (SAS) as a food additive (E 551). Arch. Toxicol. 2016, 90, 2885–2916. [Google Scholar] [CrossRef] [Green Version]
- Younes, M.; Aggett, P.; Aguilar, F.; Crebelli, R.; Dusemund, B.; Filipič, M.; Frutos, M.J.; Galtier, P.; Gott, D.; Gundert-Remy, U.; et al. Re-evaluation of silicon dioxide (E 551) as a food additive. EFSA J. 2018, 16, e5088. [Google Scholar]
- Maharana, S.M.; Pandit, M.K.; Pradhan, A.K. Effect of chemical treatment and fumed silica coating on tensile and thermogravimetric properties of jute yarn. Mater. Today Proc. 2020, 27, 2693–2698. [Google Scholar] [CrossRef]
- Isfort, C.S.; Rochnia, M. Production and physico-chemical characterisation of nanoparticles. Toxicol. Lett. 2009, 186, 148–151. [Google Scholar] [CrossRef] [PubMed]
- Hewitt, N. Silica as a reinforcing filler. In Compounding Precipitated Silica in Elastomers, 1st ed.; Ebnesajjad, S., Ed.; William Andrew Publishing: Norwich, NY, USA, 2007; pp. 1–23. [Google Scholar]
- Musić, S.; Filipović-Vinceković, N.; Sekovanić, L. Precipitation of amorphous SiO2 particles and their properties. Braz. J. Chem. Eng. 2011, 28, 89–94. [Google Scholar] [CrossRef]
- Commision of the European Communities. Food-Science and Techniques: Reports of the Scientific Committee for Food (Twenty-Fifth Series). Available online: http://aei.pitt.edu/40834/1/25th_food.pdf (accessed on 14 December 2021).
- U.S. Food and Drug Administration (FDA). CFR-Code of Federal Regulations Title 21. Available online: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?fr=172.480 (accessed on 1 April 2020).
- Bernardos Bau, A.; Kourlimska, L. Applications of mesoporous silica materials in food. Czech J. Food Sci. 2013, 31, 99–107. [Google Scholar] [CrossRef] [Green Version]
- Martin, K.R. The chemistry of silica and its potential health benefits. J. Nutr. Health Aging 2007, 11, 94. [Google Scholar]
- Dekkers, S.; Krystek, P.; Peters, R.J.; Lankveld, D.P.; Bokkers, B.G.; van Hoeven-Arentzen, P.H.; Bouwmeester, H.; Oomen, A.G. Presence and risks of nanosilica in food products. Nanotoxicology 2011, 5, 393–405. [Google Scholar] [CrossRef]
- Van Kesteren, P.C.; Cubadda, F.; Bouwmeester, H.; van Eilkeren, J.C.; Dekkers, S. Novel insights into the risk assessment of the nanomaterial synthetic amorphous silica, additive E551, in food. Nanotoxicology 2014, 9, 442–452. [Google Scholar] [CrossRef]
- Thakur, R.; Singh, S. Nanosilica particles in food: A case of synthetic amorphous silica. In Nanomaterials: Biomedical, Environmental, and Engineering Applications, 1st ed.; Kanchi, S., Ahmed, S., Eds.; Scrivener Publishing LLC: Beverly, MA, USA, 2018; pp. 153–163. [Google Scholar]
- Ogawa, T.; Okumura, R.; Nagano, K.; Minemura, T.; Izumi, M.; Motooka, D.; Nakamura, S.; Iida, T.; Maeda, Y.; Kumanogoh, A.; et al. Oral intake of silica nanoparticles exacerbates intestinal inflammation. Biochem. Biophys. Res. Commun. 2021, 534, 540–546. [Google Scholar] [CrossRef] [PubMed]
- Deng, Y.D.; Zhang, X.D.; Yang, X.S.; Huang, Z.L.; Wei, X.; Yang, X.F.; Liao, W.Z. Subacute toxicity of mesoporous silica nanoparticles to the intestinal tract and the underlying mechanism. J. Hazard. Mater. 2021, 409, 124502. [Google Scholar] [CrossRef]
- Du, Q.; Ge, D.; Mirshafiee, V.; Chen, C.; Li, M.; Xue, C.; Ma, X.; Sun, B. Assessment of neurotoxicity induced by differentsized Stöber silica nanoparticles: Induction of pyroptosis in microglia. Nanoscale 2019, 11, 12965–12972. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Wang, C.; Sun, J.; Xue, Y. Neurotoxicity of silica nanoparticles: Brain localization and dopaminergic neurons damage pathways. ACS Nano 2011, 5, 4476–4489. [Google Scholar] [CrossRef] [PubMed]
- Peters, R.J.; Oomen, A.G.; van Bemmel, G.; van Vliet, L.; Undas, A.K.; Munniks, S.; Bleys, R.L.A.W.; Tromp, P.C.; Brand, W.; van der Lee, M. Silicon dioxide and titanium dioxide particles found in human tissues. Nanotoxicology 2020, 14, 420–432. [Google Scholar] [CrossRef]
- Gmoshinski, I.V.; Shipelin, V.A.; Shumakova, A.A.; Trushina, E.N.; Mustafina, O.K.; Safenkova, I.V.; Khotimchenko, S.A.; Nikityuk, D.B.; Tutelyan, V.A. Toxicity evaluation of nanostructured silica orally administered to rats: Influence on immune system function. Nanomaterials 2020, 10, 2126. [Google Scholar] [CrossRef] [PubMed]
- Brand, W.; van Kesteren, P.C.E.; Peters, R.J.B.; Oomen, A.G. Issues currently complicating the risk assessment of synthetic amorphous silica (SAS) nanoparticles after oral exposure. Nanotoxicology 2021, 15, 905–933. [Google Scholar] [CrossRef]
- Yoo, N.K.; Jeon, Y.R.; Choi, S.J. Determination of two differently manufactured silicon dioxide nanoparticles by cloud point extraction approach in intestinal cells, intestinal barriers and tissues. Int. J. Mol. Sci. 2021, 22, 7035. [Google Scholar] [CrossRef]
- Tran, T.N.; Anh Pham, T.V.; Phung Le, M.L.; Thoa Nguyen, T.P.; Tran, V.M. Synthesis of amorphous silica and sulfonic acid functionalized silica used as reinforced phase for polymer electrolyte membrane. Adv. Nat. Sci. Nanosci. Nanotechnol. 2013, 4, 045007. [Google Scholar] [CrossRef] [Green Version]
- Paek, H.J.; Chung, H.E.; Lee, J.A.; Kim, M.K.; Lee, Y.J.; Kim, M.S.; Kim, S.H.; Maeng, E.H.; Lee, J.K.; Jeong, J.; et al. Quantitative determination of silica nanoparticles in biological matrices and their pharmacokinetics and toxicokinetics in rats. Sci. Adv. Mater. 2014, 6, 1605–1610. [Google Scholar] [CrossRef]
- Kim, Y.R.; Lee, S.Y.; Lee, E.J.; Park, S.H.; Seong, N.W.; Seo, H.S.; Shin, S.S.; Kim, S.J.; Meang, E.H.; Park, M.K.; et al. Toxicity of colloidal silica nanoparticles administered orally for 90 days in rats. Int. J. Nanomed. 2014, 9 (Suppl. 2), 67–78. [Google Scholar]
- Yu, J.; Choi, S.J. Particle size and biological fate of ZnO do not cause acute toxicity, but affect toxicokinetics and gene expression profiles in the rat livers after oral administration. Int. J. Mol. Sci. 2021, 22, 1698. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.K.; Lee, J.A.; Jo, M.R.; Choi, S.J. Bioavailability of silica, titanium dioxide, and zinc oxide nanoparticles in rats. J. Nanosci. Nanotechnol. 2016, 16, 6580–6586. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.A.; Kim, M.K.; Song, J.H.; Jo, M.R.; Yu, J.; Kim, K.M.; Kim, Y.R.; Oh, J.M.; Choi, S.J. Biokinetics of food additive silica nanoparticles and their interactions with food components. Colloids Surf. B Biointerfaces 2017, 150, 384–392. [Google Scholar] [CrossRef]
- Wu, T.; Tang, M. Review of the effects of manufactured nanoparticles on mammalian target organs. J. Appl. Toxicol. 2018, 38, 25–40. [Google Scholar] [CrossRef]
- Di Cristo, L.; Oomen, A.G.; Dekkers, S.; Moore, C.; Rocchia, W.; Murphy, F.; Johnston, H.J.; Janer, G.; Haase, A.; Stone, V.; et al. Grouping hypotheses and an integrated approach to testing and assessment of nanomaterials following oral ingestion. Nanomaterials 2021, 11, 2623. [Google Scholar] [CrossRef]
- Geraets, L.; Oomen, A.G.; Krystek, P.; Jacobsen, N.R.; Wallin, H.; Laurentie, M.; Verharen, H.W.; Brandon, E.F.; de Jong, W.H. Tissue distribution and elimination after oral and intravenous administration of different titanium dioxide nanoparticles in rats. Part. Fibre Toxicol. 2014, 11, 30. [Google Scholar] [CrossRef] [Green Version]
- Singh, R.; Lillard, J.W., Jr. Nanoparticle-based targeted drug delivery. Exp. Mol. Pathol. 2009, 86, 215–223. [Google Scholar] [CrossRef] [Green Version]
- Balaji, E.V.; Selvan, A. Nanopharmacology: A novel approach in therapeutics. Asian J. Pharm. Sci. 2019, 9, 9–16. [Google Scholar] [CrossRef]
- Lee, J.A.; Kim, M.K.; Paek, H.J.; Kim, Y.R.; Kim, M.K.; Lee, J.K.; Jeong, J.; Choi, S.J. Tissue distribution and excretion kinetics of orally administered silica nanoparticles in rats. Int. J. Nanomed. 2014, 9, 251–260. [Google Scholar]
- Scientific Committee on Consumer Safety (SCCS). Opinion on Silica, Hydrated Silica, and Silica Surface Modified with Alkyl Silylates (Nano Form). Available online: https://ec.europa.eu/health/scientific_committees/consumer_safety/docs/sccs_o_175.pdf (accessed on 14 December 2021).
- Boorman, G.; Suttie, A.; Leininger, J.; Eustis, S.; Elwell, M.; Bradley, A.; Mackenzie, W. Boorman’s Pathology of the Rat: Reference and Atlas, 2nd ed.; Elsevier: Amsterdam, The Netherlands, 2017; pp. 39–162. [Google Scholar]
- Whalan, J.E. A Toxicologist’s Guide to Clinical Pathology in Animals: Hematology, Clinical Chemistry, Urinalysis, 2015th ed.; Springer: Berlin/Heidelberg, Germany, 2015; pp. 1–168. [Google Scholar]
- Yoo, N.K. Comparative Study on Physicochmical Properties, Dissolution and Toxicokinetics of Differently Manufactured Food Additive Silicon Dioxide Nanoparticles. Master’s Thesis, Seoul Women’s University, Seoul, Korea, 18 February 2021. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Toxicokinetic Parameters | Fumed SAS | Precipitated SAS | ||||
|---|---|---|---|---|---|---|
| 50 mg/kg | 300 mg/kg | 2000 mg/kg | 50 mg/kg | 300 mg/kg | 2000 mg/kg | |
| Cmax (μg/mL) | 1.4 ± 0.4 A,a | 15.3 ± 5.5 A,b | 43.4 ± 3.6 A,c | 1.5 ± 2.2 A,a | 23.9 ± 1.2 B,b | 60.7 ± 3.7 B,c |
| Tmax (h) | 1.5 ± 0.0 A,a | 2.0 ± 0.0 A,b | 10.0 ± 0.0 A,c | 1.5 ± 0.0 A,a | 2.0 ± 0.0 A,b | 10.0 ± 0.0 A,c |
| T1/2 (h) | 1.7 ± 0.2 A,a | 3.3 ± 0.2 A,b | 16.6 ± 0.2 A,c | 1.8 ± 0.1 A,a | 3.7 ± 0.1 B,b | 18.2 ± 0.5 B,c |
| MRT (h) | 1.8 ± 0.2 A,a | 3.8 ± 0.2 A,b | 18.6 ± 0.3 A,c | 2.0 ± 0.2 A,a | 4.2 ± 0.2 B,b | 20.7 ± 1.2 B,c |
| Cl/F (mL/h) | ND | 544.1 ± 9.5 A,a | 331.9 ± 11.1 A,b | ND | 352.2 ± 17.9 B,a | 20.7 ± 1.2 B,c |
| AUC (h × μg/mL) | 0.7 ± 0.1 A,a | 50.3 ± 8.8 A,b | 577.4 ± 55.1 A,c | 1.6 ± 0.1 B,a | 85.3 ± 4.5 B,b | 727.6 ± 19.2 B,c |
| Absorption (%) | 0.2 ± 0.0 A,a | 1.8 ± 0.3 A,b | 3.1 ± 0.3 A,c | 0.4 ± 0.0 B,a | 2.9 ± 0.2 B,b | 3.9 ± 0.1 B,c |
| Group | Liver (g) | Kidney (g) | Spleen (g) | Heart (g) | Brain (g) | Lung (g) | Thymus (g) | Submandibular Lymph Node (g) | Mesenteric Lymph Node (g) | Ovary (g) |
|---|---|---|---|---|---|---|---|---|---|---|
| Control | 7.2 ±0.3 | 2.3 ±0.2 | 0.5 ±0.1 | 1.0 ±0.1 | 2.1 ±0.1 | 1.3 ±0.4 | 0.7 ±0.1 | 0.9 ±0.4 | 0.3 ±0.1 | 0.1 ±0.0 |
| Fumed SAS | 7.4 ±0.8 | 2.4 ±0.5 | 0.6 ±0.1 | 1.0 ±0.1 | 2.1 ±0.1 | 1.2 ±0.4 | 0.7 ±0.4 | 0.6 ±0.2 | 0.3 ±0.1 | 0.1 ±0.0 |
| Precipitated SAS | 7.3 ±0.3 | 2.3 ±0.2 | 0.5 ±0.1 | 1.1 ±0.1 | 2.1 ±0.1 | 1.3 ±0.4 | 0.7 ±0.1 | 0.9 ±0.5 | 0.3 ±0.0 | 0.1 ±0.1 |
| Group | Body Weight (g) | Liver (%) | Kidney (%) | Spleen (%) | Heart (%) | Brain (%) | Lung (%) | Thymus (%) | Submandibular Lymph Node (%) | Mesenteric Lymph Node (%) | Ovary (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Control | 221.7 ±0.1 | 3.2 ±0.1 | 1.0 ±0.1 | 0.2 ±0.0 | 0.5 ±0.0 | 0.9 ±0.0 | 0.6 ±0.2 | 0.3 ±0.1 | 0.4 ±0.2 | 0.1 ±0.0 | 0.1 ±0.0 |
| Fumed SAS | 224.7 ±8.7 | 3.3 ±0.3 | 1.1 ±0.2 | 0.3 ±0.1 | 0.5 ±0.1 | 0.9 ±0.0 | 0.6 ±0.2 | 0.3 ±0.2 | 0.3 ±0.1 | 0.1 ±0.0 | 0.1 ±0.0 |
| Precipitated SAS | 225.5 ±6.0 | 3.2 ±0.1 | 1.0 ±0.1 | 0.2 ±0.0 | 0.5 ±0.0 | 0.9 ±0.0 | 0.6 ±0.2 | 0.3 ±0.1 | 0.4 ±0.2 | 0.1 ±0.1 | 0.1 ±0.0 |
| Group | WBC (103 cells/μL) | Differential Leucocyte Count (103 cells/μL) | Differential Leucocyte Count (%) | RBC (106 cells/µL) | HGB (g/dL) | HCT (%) | MCV (fL) | MCH (pg) | MCHC (g/dL) | Retic (109 cells/L) | Retic (%) | PLT (103 cells/μL) | PT (s) | APTT (s) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| NEs | LYs | MOs | EOs | BAs | NEs | LYs | MOs | EOs | BAs | |||||||||||||
| Control | 4.3 ±1.2 | 0.4 ±0.2 | 3.7 ±1.1 | 0.04 ±0.03 | 0.05 ±0.02 | 0.0 ±0.0 | 9.9 ±3.6 | 87.0 ±3.6 | 0.9 ±0.3 | 1.3 ±0.2 | 0.1 ±0.0 | 7.3 ±0.3 | 14.1 ±0.6 | 42.7 ±2.1 | 58.3 ±0.6 | 19.3 ±0.3 | 33.0 ±0.4 | 136.3 ±18.2 | 1.9 ±0.2 | 844.2 ±509.7 | 16.1 ±0.6 | 13.7 ±1.2 |
| Fumed SAS | 4.4 ±1.7 | 0.7 ±0.5 | 3.5 ±1.3 | 0.07 ±0.03 | 0.08 ±0.04 | 0.0 ±0.0 | 16.4 ±5.4 | 79.6 ±5.7 | 1.7 ±0.4 | 1.7 ±0.4 | 0.1 ±0.0 | 7.4 ±0.3 | 14.6 ±0.3 | 44.0 ±0.9 | 59.3 ±1.9 | 19.8 ±0.5 | 33.3 ±0.3 | 172.5 ±30.2 | 2.3 ±0.5 | 1159.0 ±65.0 | 16.1 ±0.7 | 13.4 ±1.7 |
| Precipitated SAS | 6.6 ±1.4 * | 0.7 ±0.7 | 5.7 ±0.8 * | 0.07 ±0.03 * | 0.07 ±0.01 * | 0.0 ±0.0 | 9.8 ±7.1 | 87.8 ±6.1 | 1.0 ±0.2 | 1.3 ±0.1 | 0.1 ±0.0 | 7.3 ±0.3 | 14.4 ±0.6 | 43.4 ±2.1 | 59.1 ±0.3 | 19.7 ±0.2 | 33.2 ±0.7 | 129.2 ±18.2 | 1.8 ±0.3 | 843.8 ±971.8 | 17.4 ±0.8 | 14.7 ±1.5 |
| Group | TP (g/dL) | ALB (g/dL) | A/G ratio | T-BIL (mg/dL) | ALP (U/L) | AST (U/L) | ALT (U/L) | CREA (mg/dL) | BUN (mg/dL) | T-CHO (mg/dL) | TG (mg/dL) | GLU (mg/dL) | CA (mg/dL) | IP (mg/dL) | GGT (IU/L) | CK (IU/L) | TBA (µmol/L) | Na+ (mmol/L) | K+ (mmol/L) | Cl− (mmol/L) | CHE (U/L) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Control | 5.8 ±0.3 | 3.8 ±0.2 | 1.9 ±0.2 | 0.0 ±0.0 | 398.0 ±65.7 | 89.4 ±5.8 | 29.2 ±5.8 | 0.5 ±0.0 | 18.6 ±2.6 | 51.2 ±13.6 | 8.4 ±2.6 | 113.8 ±8.9 | 9.8 ±0.2 | 7.6 ±0.5 | 0.3 ±0.5 | 258.0 ±74.2 | 9.6 ±5.0 | 145.4 ±1.0 | 4.5 ±0.3 | 106.4 ±1.2 | 678.9 ±155.3 |
| Fumed SAS | 5.8 ±0.3 | 3.8 ±0.2 | 1.9 ±0.1 | 0.0 ±0.0 | 380.0 ±81.9 | 97.0 ±19.0 | 27.8 ±3.4 | 0.5 ±0.1 | 15.9 ±1.7 | 55.2 ±8.4 | 8.0 ±1.7 | 112.4 ±11.2 | 9.8 ±0.1 | 7.6 ±0.6 | 0.1 ±0.3 | 378.0 ±140.2 | 8.8 ±4.0 | 144.2 ±0.7 | 4.5 ±0.2 | 105.8 ±1.2 | 762.9 ±178.1 |
| Precipitated SAS | 5.8 ±0.2 | 3.8 ±0.1 | 1.9 ±0.1 | 0.0 ±0.0 | 460.1 ±108.1 | 83.3 ±2.6 | 25.0 ±2.2 | 0.5 ±0.0 | 20.7 ±2.2 | 51.4 ±11.1 | 8.3 ±3.8 | 111.7 ±6.4 | 9.6 ±0.2 | 8.1 ±0.3 | 0.4 ±0.5 | 198.0 ±25.1 | 7.7 ±3.6 | 146.0 ±1.5 | 4.6 ±0.4 | 106.9 ±0.7 | 683.8 ±213.2 |
| Organs | Number of Animals | Histopathological Findings | Group | ||
|---|---|---|---|---|---|
| Control | Fumed SAS | Precipitated SAS | |||
| Liver | 5 | No abnormality detected | 4 | 4 | 5 |
| Inflammatory cell foci | |||||
| -minimal, multifocal | 0 | 1 | 0 | ||
| Vacuolation, periportal | 1 | 0 | 0 | ||
| Kidney | 5 | No abnormality detected | 4 | 2 | 3 |
| Basophilia, tubular | |||||
| -minimal | 1 | 0 | 0 | ||
| -slight | 0 | 0 | 1 | ||
| -slight, focal | 0 | 1 | 0 | ||
| Cyst | |||||
| -medullary, present | 0 | 2 | 1 | ||
| Scar | |||||
| -cortical, present | 0 | 1 | 0 | ||
| Heart | 5 | No abnormality detected | 5 | 5 | 5 |
| Lung | 5 | No abnormality detected | 5 | 5 | 5 |
| Brain | 5 | No abnormality detected | 5 | 5 | 5 |
| Spleen | 5 | No abnormality detected | 5 | 5 | 5 |
| Ovary | 5 | No abnormality detected | 5 | 5 | 5 |
| Stomach | 5 | No abnormality detected | 5 | 5 | 4 |
| Cyst | |||||
| -squamous, present | 0 | 0 | 1 | ||
| Small/large intestine | 5 | No abnormality detected | 5 | 5 | 5 |
| Pancreas | 5 | No abnormality detected | 5 | 5 | 5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoo, N.-K.; Youn, S.-M.; Choi, S.-J. Oral Toxicokinetics, Tissue Distribution, and 28-Day Oral Toxicity of Two Differently Manufactured Food Additive Silicon Dioxides. Int. J. Mol. Sci. 2022, 23, 4023. https://doi.org/10.3390/ijms23074023
Yoo N-K, Youn S-M, Choi S-J. Oral Toxicokinetics, Tissue Distribution, and 28-Day Oral Toxicity of Two Differently Manufactured Food Additive Silicon Dioxides. International Journal of Molecular Sciences. 2022; 23(7):4023. https://doi.org/10.3390/ijms23074023
Chicago/Turabian StyleYoo, Na-Kyung, Su-Min Youn, and Soo-Jin Choi. 2022. "Oral Toxicokinetics, Tissue Distribution, and 28-Day Oral Toxicity of Two Differently Manufactured Food Additive Silicon Dioxides" International Journal of Molecular Sciences 23, no. 7: 4023. https://doi.org/10.3390/ijms23074023
APA StyleYoo, N.-K., Youn, S.-M., & Choi, S.-J. (2022). Oral Toxicokinetics, Tissue Distribution, and 28-Day Oral Toxicity of Two Differently Manufactured Food Additive Silicon Dioxides. International Journal of Molecular Sciences, 23(7), 4023. https://doi.org/10.3390/ijms23074023