
MAFLD and CKD: An Updated Narrative Review

 , , , and
, , , and
Abstract
:1. Introduction
2. Association between NAFLD and Risk of Incident CKD
3. Association between MAFLD and Risk of CKD
4. Is MAFLD Concordant (or Superior) to NAFLD in Detecting Patients at Higher Risk of CKD?
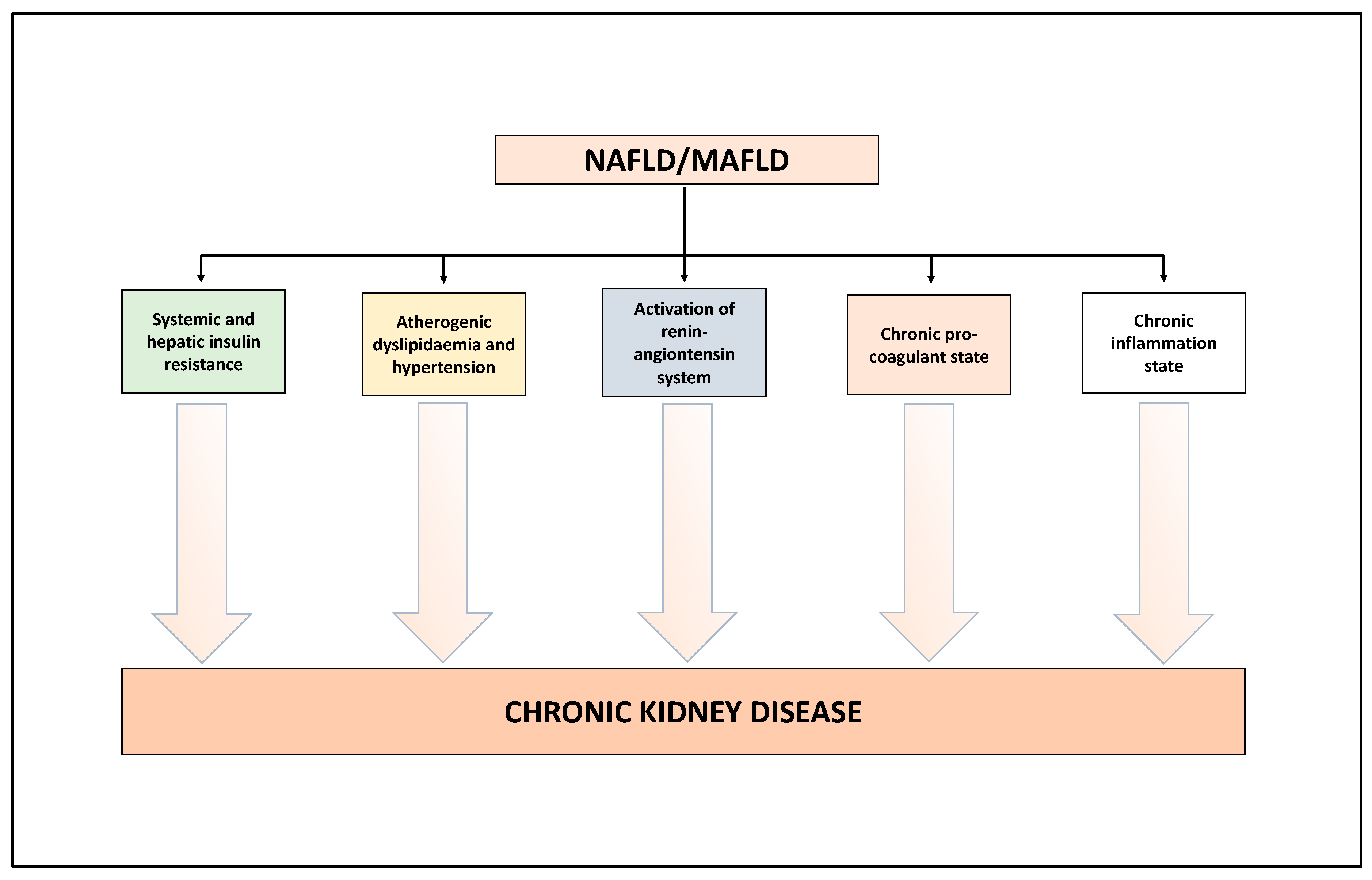
5. Putative Mechanisms Underpinning the Association between NAFLD/MAFLD and Risk of CKD
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mantovani, A.; Scorletti, E.; Mosca, A.; Alisi, A.; Byrne, C.D.; Targher, G. Complications, morbidity and mortality of nonalcoholic fatty liver disease. Metabolism 2020, 111, 154170. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Le, M.H.; Yeo, Y.H.; Li, X.; Li, J.; Zou, B.; Wu, Y.; Ye, Q.; Huang, D.Q.; Zhao, C.; Zhang, J.; et al. 2019 Global NAFLD Prevalence: A Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Golabi, P.; de Avila, L.; Paik, J.M.; Srishord, M.; Fukui, N.; Qiu, Y.; Burns, L.; Afendy, A.; Nader, F. The global epidemiology of NAFLD and NASH in patients with type 2 diabetes: A systematic review and meta-analysis. J. Hepatol. 2019, 71, 793–801. [Google Scholar] [CrossRef] [PubMed]
- Lonardo, A.; Mantovani, A.; Lugari, S.; Targher, G. Epidemiology and pathophysiology of the association between NAFLD and metabolically healthy or metabolically unhealthy obesity. Ann. Hepatol. 2020, 19, 359–366. [Google Scholar] [CrossRef]
- Byrne, C.D.; Targher, G. NAFLD: A multisystem disease. J. Hepatol. 2015, 62, S47–S64. [Google Scholar] [CrossRef] [Green Version]
- Mantovani, A.; Csermely, A.; Petracca, G.; Beatrice, G.; Corey, K.E.; Simon, T.G.; Byrne, C.D.; Targher, G. Non-alcoholic fatty liver disease and risk of fatal and non-fatal cardiovascular events: An updated systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2021, 6, 903–913. [Google Scholar] [CrossRef]
- Mantovani, A.; Petracca, G.; Beatrice, G.; Tilg, H.; Byrne, C.D.; Targher, G. Non-alcoholic fatty liver disease and risk of incident diabetes mellitus: An updated meta-analysis of 501 022 adult individuals. Gut 2021, 70, 962–969. [Google Scholar] [CrossRef]
- Mantovani, A.; Petracca, G.; Beatrice, G.; Csermely, A.; Lonardo, A.; Schattenberg, J.M.; Tilg, H.; Byrne, C.D.; Targher, G. Non-alcoholic fatty liver disease and risk of incident chronic kidney disease: An updated meta-analysis. Gut 2022, 71, 156–162. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Rinella, M.E.; Sanyal, A.J.; Harrison, S.A.; Brunt, E.M.; Goodman, Z.; Cohen, D.E.; Loomba, R. From NAFLD to MAFLD: Implications of a Premature Change in Terminology. Hepatology 2021, 73, 1194–1198. [Google Scholar] [CrossRef]
- Wong, V.W.; Lazarus, J.V. Prognosis of MAFLD vs. NAFLD and implications for a nomenclature change. J. Hepatol. 2021, 75, 1267–1270. [Google Scholar] [CrossRef] [PubMed]
- Fouad, Y.; Dufour, J.F.; Zheng, M.H.; Bollipo, S.; Desalegn, H.; Gronbaek, H.; Gish, R.G. The NAFLD-MAFLD debate: Is there a Consensus-on-Consensus methodology? Liver Int. 2022, 42, 742–748. [Google Scholar] [CrossRef] [PubMed]
- Eslam, M.; Newsome, P.N.; Sarin, S.K.; Anstee, Q.M.; Targher, G.; Romero-Gomez, M.; Zelber-Sagi, S.; Wai-Sun Wong, V.; Dufour, J.F.; Schattenberg, J.M.; et al. A new definition for metabolic dysfunction-associated fatty liver disease: An international expert consensus statement. J. Hepatol. 2020, 73, 202–209. [Google Scholar] [CrossRef]
- Eslam, M.; Sanyal, A.J.; George, J.; International Consensus, P. MAFLD: A Consensus-Driven Proposed Nomenclature for Metabolic Associated Fatty Liver Disease. Gastroenterology 2020, 158, 1999–2014.e1. [Google Scholar] [CrossRef]
- Mantovani, A. MAFLD vs NAFLD: Where are we? Dig. Liver Dis. 2021, 53, 1368–1372. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Dalbeni, A. NAFLD, MAFLD and DAFLD. Dig. Liver Dis. 2020, 52, 1519–1520. [Google Scholar] [CrossRef] [PubMed]
- Ayada, I.; van Kleef, L.A.; Alferink, L.J.M.; Li, P.; de Knegt, R.J.; Pan, Q. Systematically comparing epidemiological and clinical features of MAFLD and NAFLD by meta-analysis: Focusing on the non-overlap groups. Liver Int. 2022, 42, 277–287. [Google Scholar] [CrossRef]
- Kalantar-Zadeh, K.; Jafar, T.H.; Nitsch, D.; Neuen, B.L.; Perkovic, V. Chronic kidney disease. Lancet 2021, 398, 786–802. [Google Scholar] [CrossRef]
- Lv, J.C.; Zhang, L.X. Prevalence and Disease Burden of Chronic Kidney Disease. Adv. Exp. Med. Biol. 2019, 1165, 3–15. [Google Scholar] [CrossRef]
- Hounkpatin, H.O.; Harris, S.; Fraser, S.D.S.; Day, J.; Mindell, J.S.; Taal, M.W.; O’Donoghue, D.; Roderick, P.J. Prevalence of chronic kidney disease in adults in England: Comparison of nationally representative cross-sectional surveys from 2003 to 2016. BMJ Open 2020, 10, e038423. [Google Scholar] [CrossRef]
- Mantovani, A.; Zusi, C.; Dalbeni, A.; Grani, G.; Buzzetti, E. Risk of Kidney Dysfunction IN Nafld. Curr. Pharm. Des. 2020, 26, 1045–1061. [Google Scholar] [CrossRef] [PubMed]
- Byrne, C.D.; Targher, G. NAFLD as a driver of chronic kidney disease. J. Hepatol. 2020, 72, 785–801. [Google Scholar] [CrossRef] [Green Version]
- Wang, T.Y.; Wang, R.F.; Bu, Z.Y.; Targher, G.; Byrne, C.D.; Sun, D.Q.; Zheng, M.H. Association of metabolic dysfunction-associated fatty liver disease with kidney disease. Nat. Rev. Nephrol. 2022, 18, 259–268. [Google Scholar] [CrossRef] [PubMed]
- Cheung, A.; Ahmed, A. Nonalcoholic Fatty Liver Disease and Chronic Kidney Disease: A Review of Links and Risks. Clin. Exp. Gastroenterol. 2021, 14, 457–465. [Google Scholar] [CrossRef] [PubMed]
- Tao, Z.; Li, Y.; Cheng, B.; Zhou, T.; Gao, Y. Influence of Nonalcoholic Fatty Liver Disease on the Occurrence and Severity of Chronic Kidney Disease. J. Clin. Transl. Hepatol. 2022, 10, 164–173. [Google Scholar] [CrossRef]
- Musso, G.; Gambino, R.; Tabibian, J.H.; Ekstedt, M.; Kechagias, S.; Hamaguchi, M.; Hultcrantz, R.; Hagstrom, H.; Yoon, S.K.; Charatcharoenwitthaya, P.; et al. Association of non-alcoholic fatty liver disease with chronic kidney disease: A systematic review and meta-analysis. PLoS Med. 2014, 11, e1001680. [Google Scholar] [CrossRef] [Green Version]
- Mantovani, A.; Zaza, G.; Byrne, C.D.; Lonardo, A.; Zoppini, G.; Bonora, E.; Targher, G. Nonalcoholic fatty liver disease increases risk of incident chronic kidney disease: A systematic review and meta-analysis. Metabolism 2018, 79, 64–76. [Google Scholar] [CrossRef]
- Sinn, D.H.; Kang, D.; Jang, H.R.; Gu, S.; Cho, S.J.; Paik, S.W.; Ryu, S.; Chang, Y.; Lazo, M.; Guallar, E.; et al. Development of chronic kidney disease in patients with non-alcoholic fatty liver disease: A cohort study. J. Hepatol. 2017, 67, 1274–1280. [Google Scholar] [CrossRef]
- Mahmoodi, B.K.; Matsushita, K.; Woodward, M.; Blankestijn, P.J.; Cirillo, M.; Ohkubo, T.; Rossing, P.; Sarnak, M.J.; Stengel, B.; Yamagishi, K.; et al. Associations of kidney disease measures with mortality and end-stage renal disease in individuals with and without hypertension: A meta-analysis. Lancet 2012, 380, 1649–1661. [Google Scholar] [CrossRef] [Green Version]
- Mantovani, A.; Turino, T.; Lando, M.G.; Gjini, K.; Byrne, C.D.; Zusi, C.; Ravaioli, F.; Colecchia, A.; Maffeis, C.; Salvagno, G.; et al. Screening for non-alcoholic fatty liver disease using liver stiffness measurement and its association with chronic kidney disease and cardiovascular complications in patients with type 2 diabetes. Diabetes Metab. 2020, 46, 296–303. [Google Scholar] [CrossRef]
- Cacoub, P.; Desbois, A.C.; Isnard-Bagnis, C.; Rocatello, D.; Ferri, C. Hepatitis C virus infection and chronic kidney disease: Time for reappraisal. J. Hepatol. 2016, 65, S82–S94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fabrizi, F.; Donato, F.M.; Messa, P. Association between hepatitis B virus and chronic kidney disease: A systematic review and meta-analysis. Ann. Hepatol. 2017, 16, 21–47. [Google Scholar] [CrossRef] [PubMed]
- Lai, Y.J.; Chen, Y.Y.; Lin, Y.K.; Chen, C.C.; Yen, Y.F.; Deng, C.Y. Alcohol Consumption and Risk of Chronic Kidney Disease: A Nationwide Observational Cohort Study. Nutrients 2019, 11, 2121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheungpasitporn, W.; Thongprayoon, C.; Kittanamongkolchai, W.; Brabec, B.A.; O’Corragain, O.A.; Edmonds, P.J.; Erickson, S.B. High alcohol consumption and the risk of renal damage: A systematic review and meta-analysis. QJM 2015, 108, 539–548. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Zhu, B.; Song, N.; Shi, Y.; Fang, Y.; Ding, X. Alcohol consumption and its association with chronic kidney disease: Evidence from a 12-year China health and Nutrition Survey. Nutr. Metab. Cardiovasc. Dis. 2022, 32, 1392–1401. [Google Scholar] [CrossRef]
- Bianco, C.; Romeo, S.; Petta, S.; Long, M.T.; Valenti, L. MAFLD vs NAFLD: Let the contest begin! Liver Int. 2020, 40, 2079–2081. [Google Scholar] [CrossRef]
- Jung, C.Y.; Koh, H.B.; Park, K.H.; Joo, Y.S.; Kim, H.W.; Ahn, S.H.; Park, J.T.; Kim, S.U. Metabolic Dysfunction-Associated Fatty Liver Disease and Risk of Incident Chronic Kidney Disease: A Nationwide Cohort Study. Diabetes Metab. 2022, 48, 101344. [Google Scholar] [CrossRef]
- Sun, D.Q.; Jin, Y.; Wang, T.Y.; Zheng, K.I.; Rios, R.S.; Zhang, H.Y.; Targher, G.; Byrne, C.D.; Yuan, W.J.; Zheng, M.H. MAFLD and risk of CKD. Metabolism 2021, 115, 154433. [Google Scholar] [CrossRef]
- Hashimoto, Y.; Hamaguchi, M.; Okamura, T.; Nakanishi, N.; Obora, A.; Kojima, T.; Fukui, M. Metabolic associated fatty liver disease is a risk factor for chronic kidney disease. J. Diabetes Investig. 2022, 13, 308–316. [Google Scholar] [CrossRef]
- Deng, Y.; Zhao, Q.; Gong, R. Association Between Metabolic Associated Fatty Liver Disease and Chronic Kidney Disease: A Cross-Sectional Study from NHANES 2017–2018. Diabetes Metab. Syndr. Obes. 2021, 14, 1751–1761. [Google Scholar] [CrossRef]
- Zhang, H.J.; Wang, Y.Y.; Chen, C.; Lu, Y.L.; Wang, N.J. Cardiovascular and renal burdens of metabolic associated fatty liver disease from serial US national surveys, 1999–2016. Chin. Med. J. 2021, 134, 1593–1601. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Chen, H.; Liu, Y.; Hou, X.; Wei, L.; Bao, Y.; Yang, C.; Zong, G.; Wu, J.; Jia, W. Association of MAFLD With Diabetes, Chronic Kidney Disease, and Cardiovascular Disease: A 4.6-Year Cohort Study in China. J. Clin. Endocrinol. Metab. 2022, 107, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Okamura, T.; Hashimoto, Y.; Hamaguchi, M.; Obora, A.; Kojima, T.; Fukui, M. Effect of alcohol consumption and the presence of fatty liver on the risk for incident type 2 diabetes: A population-based longitudinal study. BMJ Open Diabetes Res. Care 2020, 8, e001629. [Google Scholar] [CrossRef] [PubMed]
- Jang, H.R.; Kang, D.; Sinn, D.H.; Gu, S.; Cho, S.J.; Lee, J.E.; Huh, W.; Paik, S.W.; Ryu, S.; Chang, Y.; et al. Nonalcoholic fatty liver disease accelerates kidney function decline in patients with chronic kidney disease: A cohort study. Sci. Rep. 2018, 8, 4718. [Google Scholar] [CrossRef] [Green Version]
- Vilar-Gomez, E.; Calzadilla-Bertot, L.; Friedman, S.L.; Gra-Oramas, B.; Gonzalez-Fabian, L.; Villa-Jimenez, O.; Lazo-Del Vallin, S.; Diago, M.; Adams, L.A.; Romero-Gomez, M.; et al. Improvement in liver histology due to lifestyle modification is independently associated with improved kidney function in patients with non-alcoholic steatohepatitis. Aliment Pharmacol. Ther. 2017, 45, 332–344. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A. Time to revise the definition of NAFLD: A purist vision. Dig. Liver Dis. 2019, 51, 457–458. [Google Scholar] [CrossRef]
- Eslam, M.; Valenti, L.; Romeo, S. Genetics and epigenetics of NAFLD and NASH: Clinical impact. J. Hepatol. 2018, 68, 268–279. [Google Scholar] [CrossRef]
- Xia, M.; Zeng, H.; Wang, S.; Tang, H.; Gao, X. Insights into contribution of genetic variants towards the susceptibility of MAFLD revealed by the NMR-based lipoprotein profiling. J. Hepatol. 2021, 74, 974–977. [Google Scholar] [CrossRef]
- Mantovani, A.; Taliento, A.; Zusi, C.; Baselli, G.; Prati, D.; Granata, S.; Zaza, G.; Colecchia, A.; Maffeis, C.; Byrne, C.D.; et al. PNPLA3 I148M gene variant and chronic kidney disease in type 2 diabetic patients with NAFLD: Clinical and experimental findings. Liver Int. 2020, 40, 1130–1141. [Google Scholar] [CrossRef]
- Polyzos, S.A.; Kang, E.S.; Tsochatzis, E.A.; Kechagias, S.; Ekstedt, M.; Xanthakos, S.; Lonardo, A.; Mantovani, A.; Tilg, H.; Cote, I.; et al. Commentary: Nonalcoholic or metabolic dysfunction-associated fatty liver disease? The epidemic of the 21st century in search of the most appropriate name. Metabolism 2020, 113, 154413. [Google Scholar] [CrossRef]
- Lee, H.; Lee, Y.H.; Kim, S.U.; Kim, H.C. Metabolic Dysfunction-Associated Fatty Liver Disease and Incident Cardiovascular Disease Risk: A Nationwide Cohort Study. Clin. Gastroenterol. Hepatol. 2021, 19, 2138–2147.e10. [Google Scholar] [CrossRef] [PubMed]
- Byrne, C.D.; Targher, G. Non-alcoholic fatty liver disease is a risk factor for cardiovascular and cardiac diseases: Further evidence that a holistic approach to treatment is needed. Gut 2021. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Valenti, L. A call to action for fatty liver disease. Liver Int. 2021, 41, 1182–1185. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Dalbeni, A. Treatments for NAFLD: State of Art. Int. J. Mol. Sci. 2021, 22, 2350. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Byrne, C.D.; Targher, G. Efficacy of peroxisome proliferator-activated receptor agonists, glucagon-like peptide-1 receptor agonists, or sodium-glucose cotransporter-2 inhibitors for treatment of non-alcoholic fatty liver disease: A systematic review. Lancet Gastroenterol. Hepatol. 2022, 7, 367–378. [Google Scholar] [CrossRef]


{kind=link}
| Reference | Study Characteristics | Definition of NAFLD | Definition of CKD | Main Results |
|---|---|---|---|---|
| [26] | Systematic review and meta-analyses of 33 observational studies (20 cross-sectional ones and 13 longitudinal ones) for a total of 63,902 individuals | Liver enzymes, ultrasonography and liver biopsy | One or more of the following criteria:
|
|
| [27] | Systematic review and meta-analyses of nine longitudinal studies for a total of 96,595 individuals (34.1% with NAFLD). Median follow-up: 5.2 years | Liver enzymes, fatty liver index and ultrasonography | eGFR < 60 mL/min/1.73 m2 and/or overt proteinuria |
|
| [9] | Systematic review and meta-analyses of 13 longitudinal studies (with a follow-up duration of ≥1 year) for a total of 1,222,032 individuals (28.1% with NAFLD). Median follow-up: 9.7 years | Liver enzymes, fatty liver index, imaging techniques, ICD-9 codes, and liver biopsy |
|
|
| Reference | Study Characteristics | Definition of NAFLD/MAFLD | Prevalence of NAFLD and MAFLD | Definition of CKD | Main Results |
|---|---|---|---|---|---|
| [37] | Cross-sectional and prospective (mean follow-up 5.1 years) study: 268,946 US participants attending the National Health Insurance Service health (2009–2015) in the USA | Fatty liver index |
| eGFR < 60 mL/min/1.73 m2 and/or proteinuria (i.e., ≥trace on dipstick test) |
|
| [38] | Cross-sectional study: 12,571 US individuals included in the Third National Health and Nutrition Examination Survey (1988–1994) in the USA | Ultrasonography |
| eGFR < 90 mL/min/1.73 m2 and or urinary albumin-to-creatinine ratio (ACR) ≥3 mg/mmol |
|
| [39] | Cross-sectional, prospective (median follow-up 4.6 years) study: 27,371 Japanese participants in medical health checkup program in Kyoto (2004–2014) | Ultrasonography |
| eGFR < 60 mL/min/1.73 m2 and/or proteinuria |
|
| [40] | Cross-sectional and prospective (median follow-up 4.6 years) study: 4869 US subjects from the National Health and Nutrition Examination Surveys (NHANES 2017–2018) in the USA | CAP >240 dB/min |
| eGFR < 60 mL/min/1.73 m2 and/or proteinuria |
|
| [41] | Cross-sectional study: 19,617 US subjects from the National Health and Nutrition Examination Surveys in the USA over four periods: 1999–2002; 2003–2006; 2007–2010; 2011–2016 | Fatty liver index >30 |
2003–2006: 29% 2007–2010: 32% 2011–2016: 33%
2003–2006: 31% 2007–2010: 34% 2011–2016: 36% | eGFR < 60 mL/min/1.73 m2 and/or albumin-to-creatinine ratio (ACR) ≥30 mg/g |
|
| [42] | Cohort study (median follow-up 4.6 years): 6873 Chinese subjects from The Shanghai Nicheng Cohort Study | Ultrasonography |
| eGFR < 60 mL/min/1.73 m2 and/or albumin-to-creatinine ratio (ACR) ≥30 mg/g |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mantovani, A.; Lombardi, R.; Cattazzo, F.; Zusi, C.; Cappelli, D.; Dalbeni, A. MAFLD and CKD: An Updated Narrative Review. Int. J. Mol. Sci. 2022, 23, 7007. https://doi.org/10.3390/ijms23137007
Mantovani A, Lombardi R, Cattazzo F, Zusi C, Cappelli D, Dalbeni A. MAFLD and CKD: An Updated Narrative Review. International Journal of Molecular Sciences. 2022; 23(13):7007. https://doi.org/10.3390/ijms23137007
Chicago/Turabian StyleMantovani, Alessandro, Rosa Lombardi, Filippo Cattazzo, Chiara Zusi, Davide Cappelli, and Andrea Dalbeni. 2022. "MAFLD and CKD: An Updated Narrative Review" International Journal of Molecular Sciences 23, no. 13: 7007. https://doi.org/10.3390/ijms23137007
APA StyleMantovani, A., Lombardi, R., Cattazzo, F., Zusi, C., Cappelli, D., & Dalbeni, A. (2022). MAFLD and CKD: An Updated Narrative Review. International Journal of Molecular Sciences, 23(13), 7007. https://doi.org/10.3390/ijms23137007