
Diagnostic Significance of Selected Serum Inflammatory Markers in Women with Advanced Endometriosis

 , ,
, ,  , and
, and 
Abstract
1. Introduction
2. Results
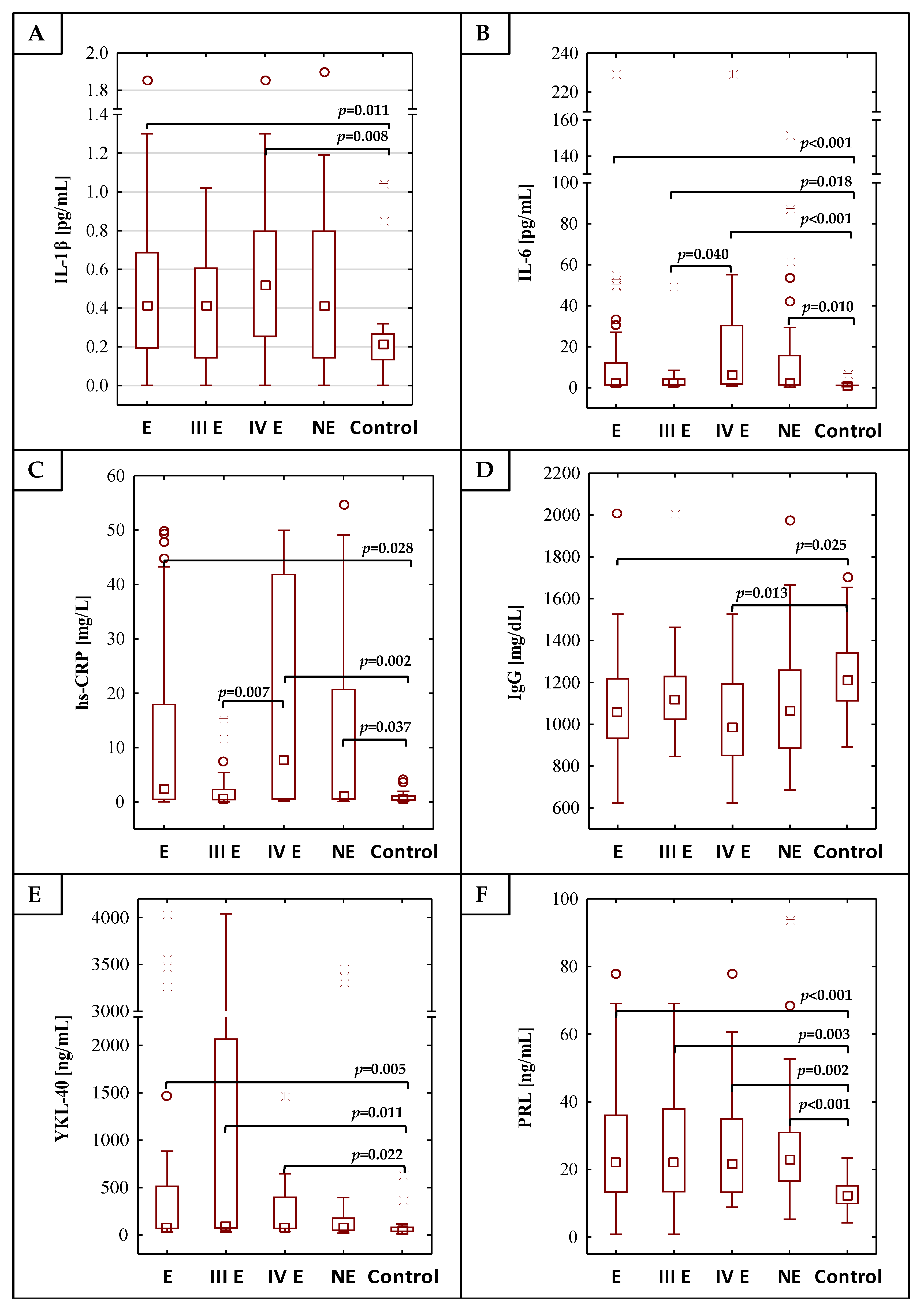
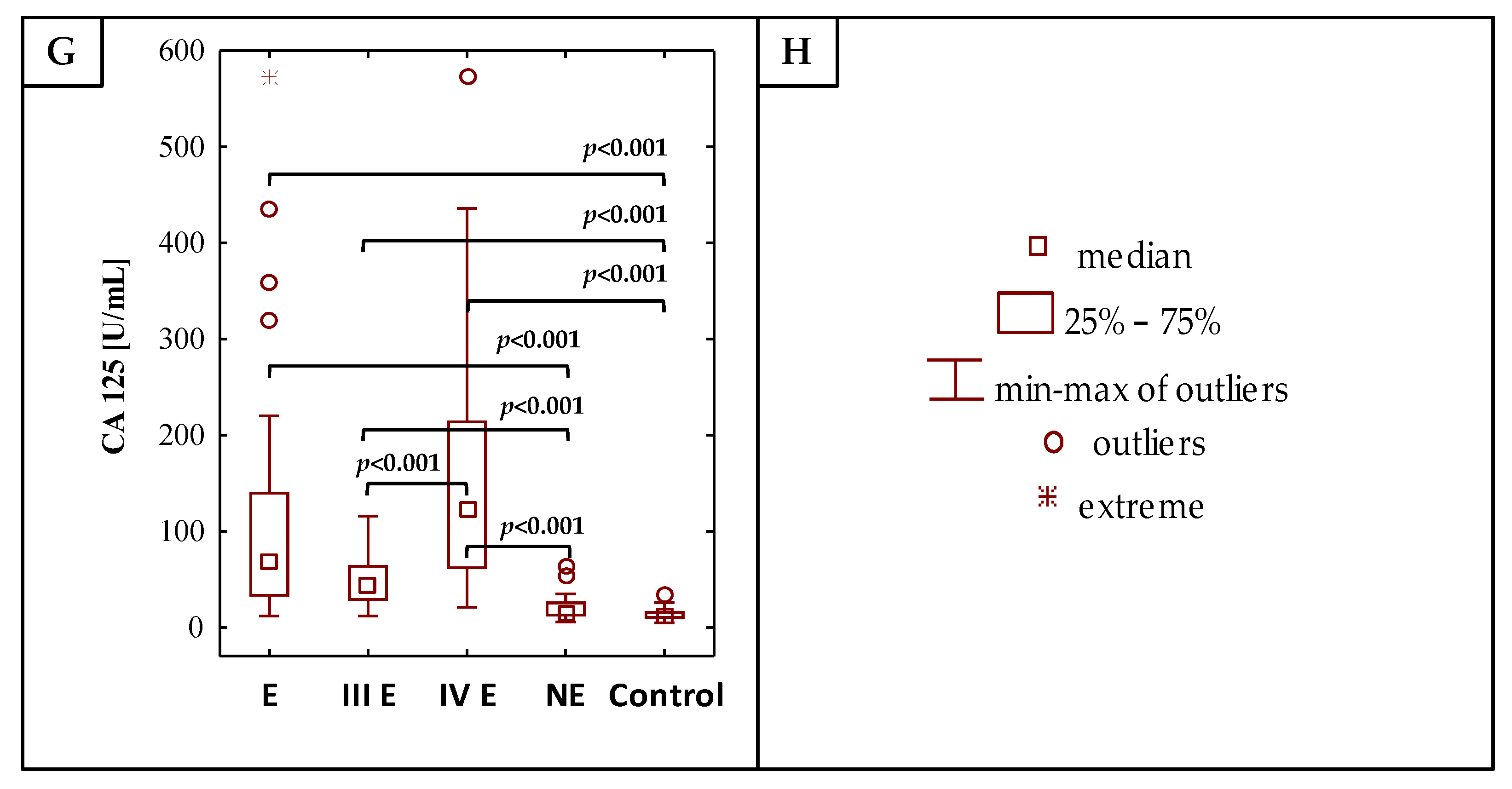
2.1. The Concentrations of Inflammatory Parameters
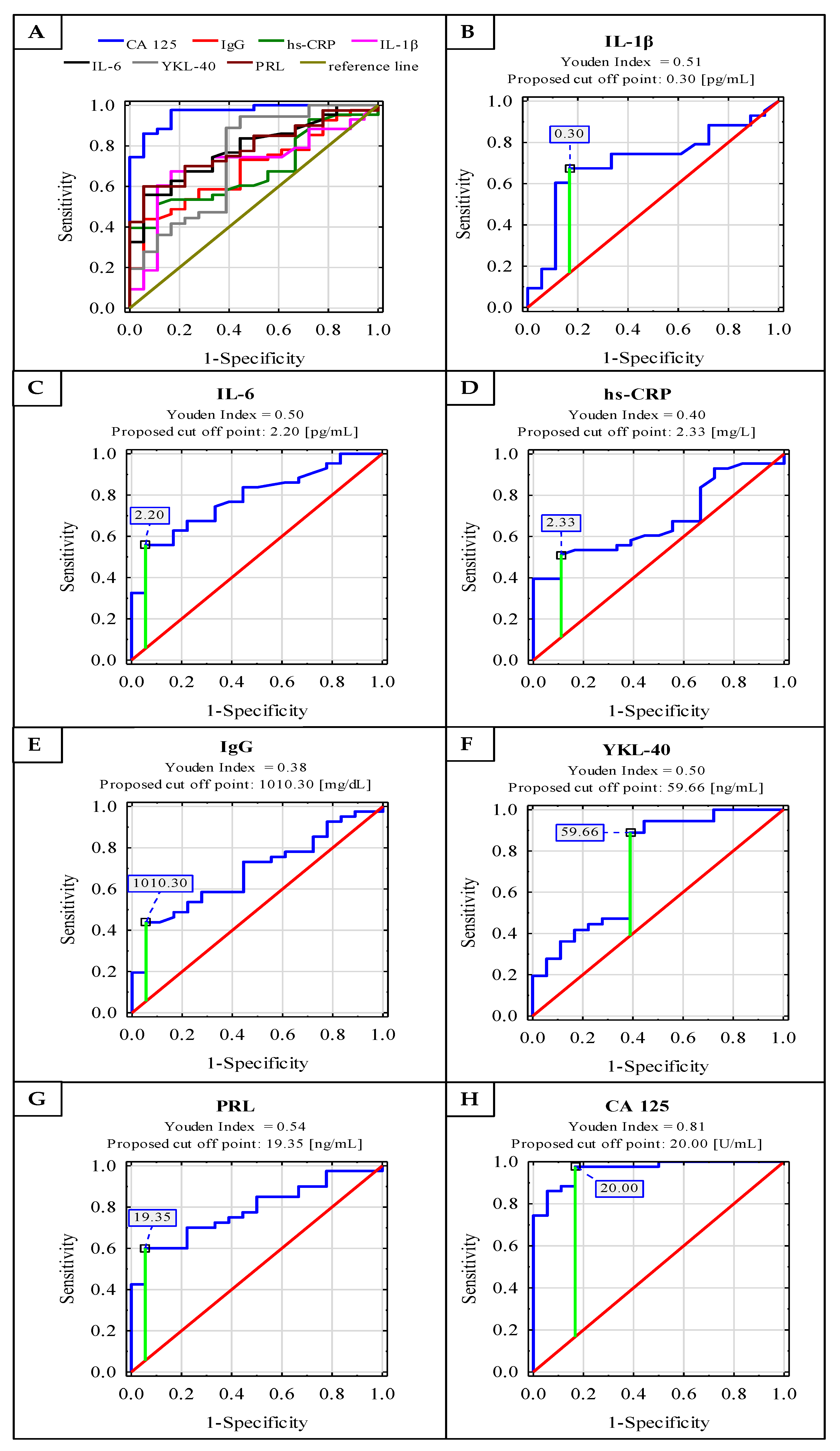
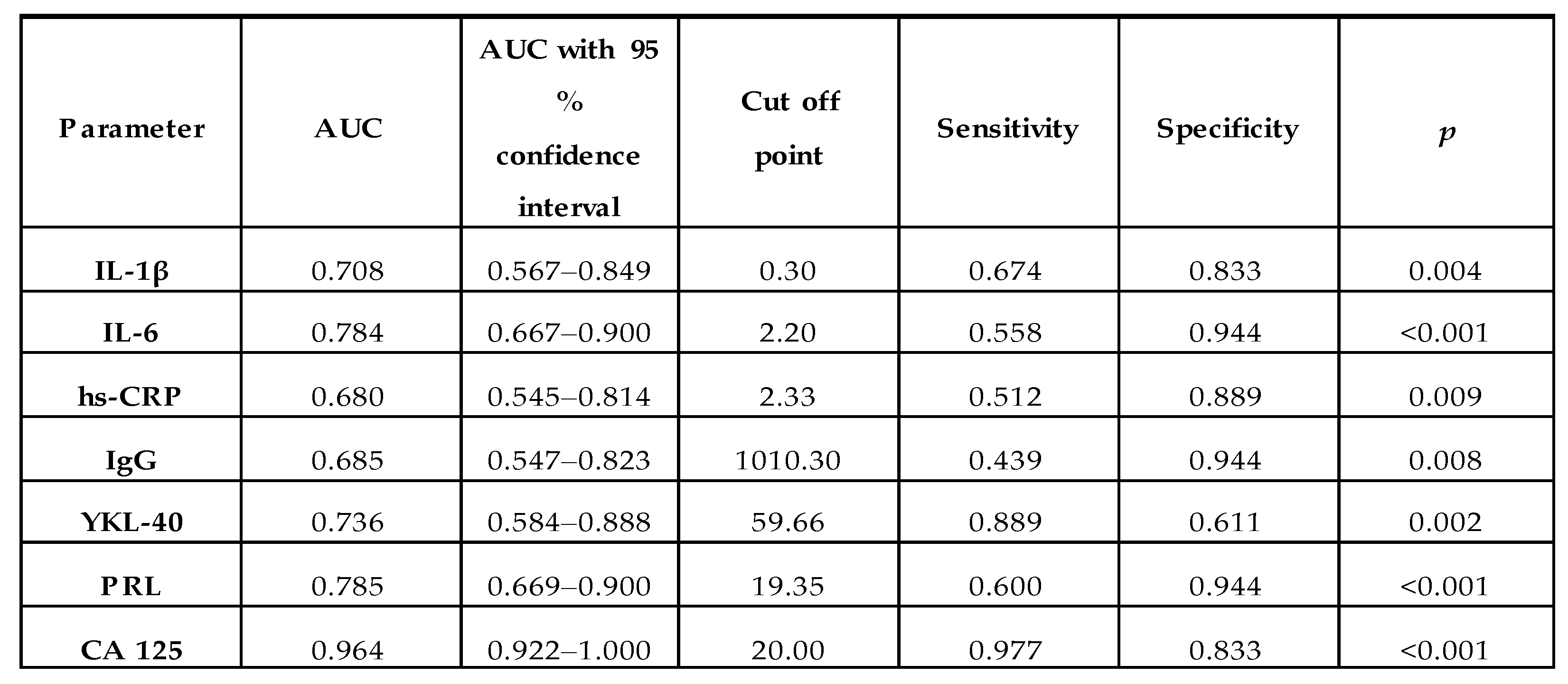
2.2. ROC Curve Analysis
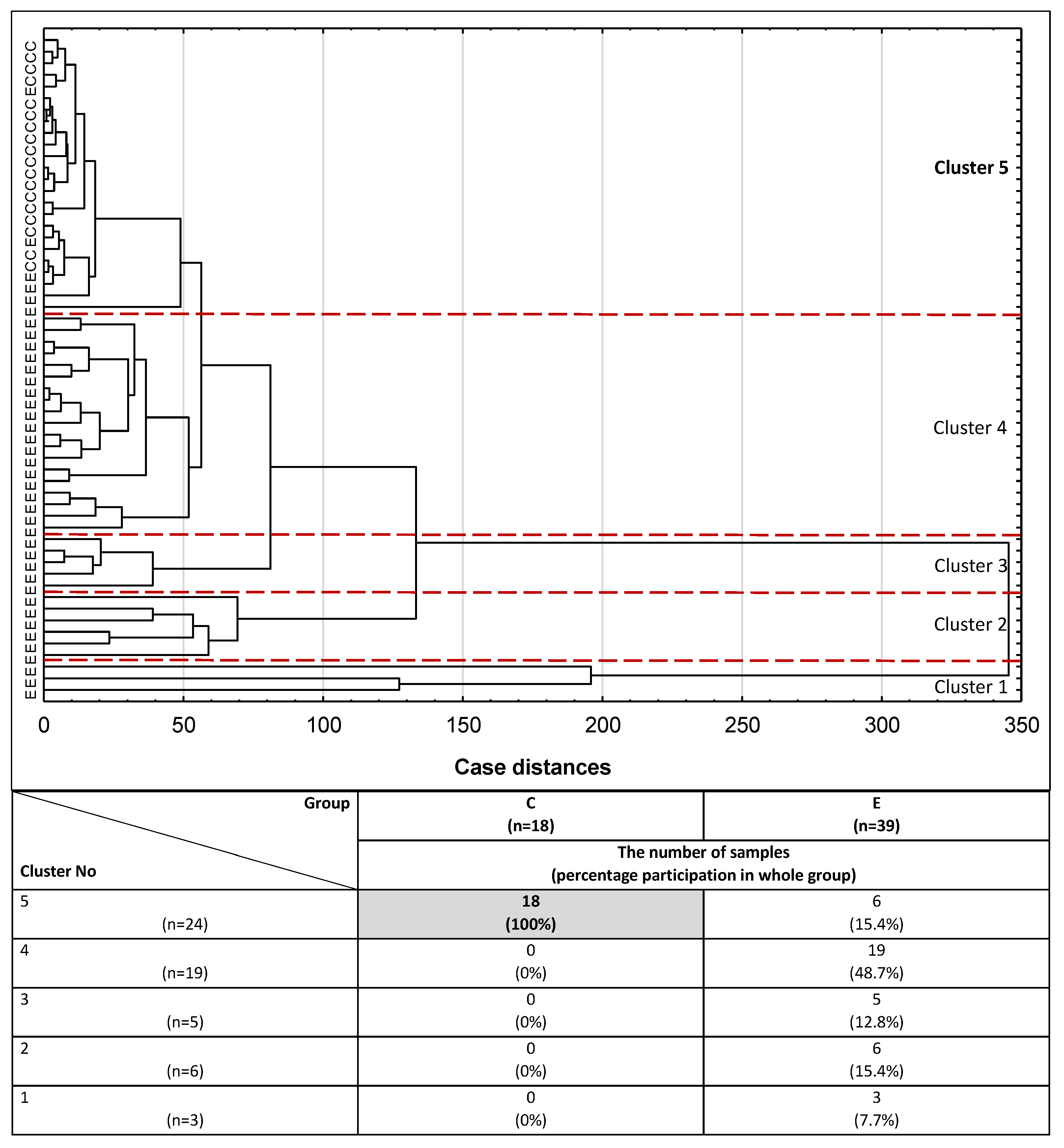
2.3. Cluster Analysis
3. Discussion
- Lack of a representative early-stage endometriosis group, which makes it impossible to verify the parameters analysed in this study and evaluate them as useful biomarkers for the early stages of endometriosis.
- The broad range of concentration values obtained for all the parameters subject to analysis has an influence on the results of statistical analysis and makes it difficult to draw unequivocal conclusions.
- Lack of the peritoneal fluid needed to compare the concentrations of inflammatory parameters with their expression in the serum.
- The proposed panel of easily measurable serum markers of inflammation (especially IL-6, PRL and CA 125) may be helpful in the differentiation of the advanced stage of endometriosis, and for its diagnostics.
- The set of parameters analysed in this study could be a useful clinical tool to identify women with a high risk of severe endometriosis development, who could qualify for a laparoscopy procedure.
- The results of this study encourage further research concerning a noninvasive, easily measurable diagnostic panel of inflammatory markers, with potential clinical utility in women with advanced endometriosis.
- The study showed that the non-endometriosis group, suffering from benign gynecological diseases, did not seem to be a proper comparative population representing disorders with similar inflammatory parameters compared to women with advanced endometriosis.
4. Materials and Methods
4.1. Patients
4.2. Assays
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AUC | Area under the ROC curve |
| BMI | Body mass index |
| C | Control group |
| CRP | C-reactive protein |
| E | Endometriosis group |
| hs-CRP | high sensitive CRP |
| IgG | Immunoglobulin G |
| IL-1β | Interleukin 1β |
| IL-6 | Interleukin 6 |
| NE | Non-endometriosis group |
| PRL | Prolactin |
| rAFS | revised American Fertility Society classification |
| ROC | Receiver operating characteristic |
| SD | Standard deviation |
| YKL-40 | Chitinase-3-like protein 1 |
| III E | Moderate group of endometriosis (stage III according to rAFS classification) |
| IV E | Severe group of endometriosis (stage IV according to rAFS classification) |
References
- As-Sanie, S.; Black, R.; Giudice, L.C.; Gray Valbrun, T.; Gupta, J.; Jones, B.; Laufer, M.R.; Milspaw, A.T.; Missmer, S.A.; Norman, A.; et al. Assessing research gaps and unmet needs in endometriosis. Am. J. Obstet. Gynecol. 2019, 221, 86–94. [Google Scholar] [CrossRef]
- Patel, B.G.; Lenk, E.E.; Lebovic, D.I.; Shu, Y.; Yu, J.; Taylor, R.N. Pathogenesis of endometriosis: Interaction between Endocrine and inflammatory pathways. Best Pract. Res. Clin. Obstet. Gynaecol. 2018, 50, 50–60. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.; Jiang, Z.; Xue, M. Serum and peritoneal fluid levels of interleukin-6 and interleukin-37 as biomarkers for endometriosis. Gynecol. Endocrinol. 2019, 35, 571–575. [Google Scholar] [CrossRef] [PubMed]
- Thubert, T.; Santulli, P.; Marcellin, L.; Menard, S.; M’Baye, M.; Streuli, I.; Borghese, B.; De Ziegler, D.; Chapron, C. Measurement of hs-CRP is irrelevant to diagnose and stage endometriosis: Prospective study of 834 patients. Am. J. Obstet. Gynecol. 2014, 210, 533.e1–533.e10. [Google Scholar] [CrossRef]
- Wickiewicz, D.; Chrobak, A.; Gmyrek, G.B.; Halbersztadt, A.; Gabryś, M.S.; Goluda, M.; Chełmońska-Soyta, A. Diagnostic accuracy of interleukin-6 levels in peritoneal fluid for detection of endometriosis. Arch. Gynecol. Obstet. 2013, 288, 805–814. [Google Scholar] [CrossRef]
- Kyama, C.M.; Debrock, S.; Mwenda, J.M.; D’Hooghe, T.M. Potential involvement of the immune system in the development of endometriosis. Reprod. Biol. Endocrinol. 2003, 1, 123. [Google Scholar] [CrossRef] [PubMed]
- Andrews, W.C.; Buttram, V.C.; Behrman, S.J. Revised American fertility society classification of endometriosis: 1985. Fertil. Steril. 1985, 44, 7–8. [Google Scholar] [CrossRef]
- Canis, M.; Donnez, J.G.; Guzick, D.S.; Halme, J.K.; Rock, J.A.; Schenken, R.S.; Vernon, M.W. Revised American Society for Reproductive Medicine classification of endometriosis: 1996. Fertil. Steril. 1997, 67, 817–821. [Google Scholar] [CrossRef]
- Ahn, S.H.; Monsanto, S.P.; Miller, C.; Singh, S.S.; Thomas, R.; Tayade, C. Pathophysiology and immune dysfunction in endometriosis. BioMed Res. Int. 2015, 2015. [Google Scholar] [CrossRef]
- Sampson, J.A. Peritoneal endometriosis due to the menstrual dissemination of endometrial tissue into the peritoneal cavity. Am. J. Obstet. Gynecol. 1927, 14, 422–469. [Google Scholar] [CrossRef]
- Flores, I.; Waelkens, E.; D’Hooghe, T. Noninvasive diagnosis of endometriosis: Review of current peripheral blood and endometrial biomarkers. Best Pract. Res. Clin. Obstet. Gynaecol. 2018, 50, 72–83. [Google Scholar] [CrossRef]
- Dorien, F.O.; Roskams, T.; Van Den Eynde, K.; Vanhie, A.; Peterse, D.P.; Meuleman, C.; Tomassetti, C.; Peeraer, K.; D’Hooghe, T.M.; Fassbender, A. The Presence of Endometrial Cells in Peritoneal Fluid of Women with and Without Endometriosis. Reprod. Sci. 2017, 24, 242–251. [Google Scholar] [CrossRef]
- da Gama Coelho Riccio, L.; Santulli, P.; Marcellin, L.; Abrão, M.S.; Batteux, F.; Chapron, C. Immunology of endometriosis. Best Pract. Res. Clin. Obstet. Gynaecol. 2018, 50, 39–49. [Google Scholar] [CrossRef] [PubMed]
- Vodolazkaia, A.; Bossuyt, X.; Fassbender, A.; Kyama, C.M.; Meuleman, C.; Peeraer, K.; Tomassetti, C.; D’Hooghe, T.M. A high sensitivity assay is more accurate than a classical assay for the measurement of plasma CRP levels in endometriosis. Reprod. Biol. Endocrinol. 2011, 9, 113. [Google Scholar] [CrossRef] [PubMed]
- Le, N.P.L.; Bowden, T.A.; Struwe, W.B.; Crispin, M. Immune recruitment or suppression by glycan engineering of endogenous and therapeutic antibodies. Biochim. Biophys. Acta Gen. Subj. 2016, 1860, 1655–1668. [Google Scholar] [CrossRef]
- Aschermann, S.; Lux, A.; Baerenwaldt, A.; Biburger, M.; Nimmerjahn, F. The other side of immunoglobulin G: Suppressor of inflammation. Clin. Exp. Immunol. 2010, 160, 161–167. [Google Scholar] [CrossRef]
- Gonzalez-Quintela, A.; Alende, R.; Gude, F.; Campos, J.; Rey, J.; Meijide, L.M.; Fernandez-Merino, C.; Vidal, C. Serum levels of immunoglobulins (IgG, IgA, IgM) in a general adult population and their relationship with alcohol consumption, smoking and common metabolic abnormalities. Clin. Exp. Immunol. 2008, 151, 42–50. [Google Scholar] [CrossRef]
- Rusak, A.; Jabłońska, K.; Dzięgiel, P. The role of YKL-40 in a cancerous process. Postepy Hig. Med. Dosw. (Online) 2016, 70, 1286–1299. [Google Scholar] [CrossRef]
- Lee, C.G.; Da Silva, C.A.; Dela Cruz, C.S.; Ahangari, F.; Ma, B.; Kang, M.-J.; He, C.-H.; Takyar, S.; Elias, J.A. Role of Chitin and Chitinase/Chitinase-Like Proteins in Inflammation, Tissue Remodeling, and Injury. Annu. Rev. Physiol. 2011, 73, 479–501. [Google Scholar] [CrossRef]
- Kokot, I.; Pawlik-Sobecka, L.; Płaczkowska, S.; Piwowar, A. Prolactin as an immunomodulatory factor in psoriatic arthritis. Postepy Hig. Med. Dosw. 2013, 67, 1265–1272. [Google Scholar] [CrossRef]
- Borba, V.V.; Zandman-Goddard, G.; Shoenfeld, Y. Prolactin and autoimmunity: The hormone as an inflammatory cytokine. Best Pract. Res. Clin. Endocrinol. Metab. 2019, 33, 101324. [Google Scholar] [CrossRef]
- Borba, V.V.; Zandman-Goddard, G.; Shoenfeld, Y. Prolactin and autoimmunity. Front. Immunol. 2018, 9, 73. [Google Scholar] [CrossRef]
- Gao, Y.; Shen, M.; Ma, X.; Li, J.; Wang, B.; Wang, J.; Tian, J. Seven hormonal biomarkers for diagnosing endometriosis: Meta-analysis and adjusted indirect comparison of diagnostic test accuracy. J. Minim. Invasive Gynecol. 2019, 26, 1026–1035.e4. [Google Scholar] [CrossRef]
- Esmaeilzadeh, S.; Mirabi, P.; Basirat, Z.; Zeinalzadeh, M.; Khafri, S. Association between endometriosis and hyperprolactinemia in infertile women. Iran. J. Reprod. Med. 2015, 13, 155–160. [Google Scholar]
- Mirabi, P.; Alamolhoda, S.H.; Golsorkhtabaramiri, M.; Namdari, M.; Esmaeilzadeh, S. Prolactin concentration in various stages of endometriosis in infertile women. J. Bras. Reprod. Assist. 2019, 23, 225–229. [Google Scholar] [CrossRef]
- Hirsch, M.; Duffy, J.M.N.; Davis, C.J.; Nieves Plana, M.; Khan, K.S. Diagnostic accuracy of cancer antigen 125 for endometriosis: A systematic review and meta-analysis. BJOG Int. J. Obstet. Gynaecol. 2016, 123, 1761–1768. [Google Scholar] [CrossRef] [PubMed]
- Bossuyt, X. Clinical performance characteristics of a laboratory test. A practical approach in the autoimmune laboratory. Autoimmun. Rev. 2009, 8, 543–548. [Google Scholar] [CrossRef]
- Othman, E.E.D.R.; Hornung, D.; Salem, H.T.; Khalifa, E.A.; El-Metwally, T.H.; Al-Hendy, A. Serum cytokines as biomarkers for nonsurgical prediction of endometriosis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2008, 137, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Oku, H.; Tsuji, Y.; Kashiwamura, S.I.; Adachi, S.; Kubota, A.; Okamura, H.; Koyama, K. Role of IL-18 in pathogenesis of endometriosis. Hum. Reprod. 2004, 19, 709–714. [Google Scholar] [CrossRef] [PubMed]
- Bedaiwy, M.A.; Falcone, T.; Sharma, R.K.; Goldberg, J.M.; Attaran, M.; Nelson, D.R.; Agarwal, A. Prediction of endometriosis with serum and peritoneal fluid markers: A prospective controlled trial. Hum. Reprod. 2002, 17, 426–431. [Google Scholar] [CrossRef]
- Malutan, A.M.; Drugan, T.; Costin, N.; Ciortea, R.; Bucuri, C.; Rada, M.P.; Mihu, D. Pro-inflammatory cytokines for evaluation of inflammatory status in endometriosis. Cent. Eur. J. Immunol. 2015, 40, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Paul Dmowski, W.; Braun, D.P. Immunology of endometriosis. Best Pract. Res. Clin. Obstet. Gynaecol. 2004, 18, 245–263. [Google Scholar] [CrossRef] [PubMed]
- Kashanian, M.; Sariri, E.; Vahdat, M.; Ahmari, M.; Moradi, Y.; Sheikhansari, N. A comparison between serum levels of interleukin-6 and CA125 in patients with endometriosis and normal women. Med. J. Islam. Repub. Iran 2015, 29, 1062–1067. [Google Scholar]
- Younis, A.; Hawkins, K.; Mahini, H.; Butler, W.; Garelnabi, M. Serum tumor necrosis factor-α, interleukin-6, monocyte chemotactic protein-1 and paraoxonase-1 profiles in women with endometriosis, pcos, or unexplained infertility. J. Assist. Reprod. Genet. 2014, 31, 1445–1451. [Google Scholar] [CrossRef] [PubMed]
- Somigliana, E.; Viganò, P.; Tirelli, A.S.; Felicetta, I.; Torresani, E.; Vignali, M.; Di Blasio, A.M. Use of the concomitant serum dosage of CA 125, CA 19-9 and interleukin-6 to detect the presence of endometriosis. Results from a series of reproductive age women undergoing laparoscopic surgery for benign gynaecological conditions. Hum. Reprod. 2004, 19, 1871–1876. [Google Scholar] [CrossRef] [PubMed]
- Lermann, J.; Mueller, A.; Körber, F.; Oppelt, P.; Beckmann, M.W.; Dittrich, R.; Renner, S.P. Evaluation of high-sensitivity C-reactive protein in comparison with C-reactive protein as biochemical serum markers in women with endometriosis. Fertil. Steril. 2010, 93, 2125–2129. [Google Scholar] [CrossRef] [PubMed]
- Xavier, P.; Belo, L.; Beires, J.; Rebelo, I.; Martinez-de-Oliveira, J.; Lunet, N.; Barros, H. Serum levels of VEGF and TNF-a and their association with C-reactive protein in patients with endometriosis. Arch. Gynecol. Obstet. 2006, 273, 227–231. [Google Scholar] [CrossRef] [PubMed]
- Gebel, H.M.; Braun, D.P.; Rotman, C.; Rana, N.; Dmowski, W.P. Mitogen induced production of polyclonal IgG is decreased in women with severe endometriosis. Am. J. Reprod. Immunol. 1993, 29, 124–130. [Google Scholar] [CrossRef]
- Meek, S.C.; Hodge, D.D.; Musich, J.R. Autoimmunity in infertile patients with endometriosis. Am. J. Obstet. Gynecol. 1988, 158, 1365–1373. [Google Scholar] [CrossRef]
- Van Schoor, J.; Toogood, J.H.; Pauwels, R.A. Differential effects of inhaled budesonide and oral prednisolone on serum immunoglobulin G and its subclasses in healthy adult volunteers. Clin. Exp. Allergy 1997, 27, 192–195. [Google Scholar] [CrossRef]
- Confino, E.; Harlow, L.; Gleicher, N. Peritoneal fluid and serum autoantibody levels in patients with endometriosis. Fertil. Steril. 1990, 53, 242–245. [Google Scholar] [CrossRef]
- Odukoya, O.; Bansal, A.; Cooke, I. Serum endometrial IgG antibodies and soluble CD23 concentrations in patients with endometriosis. Acta Obstet. Gynecol. Scand. 1996, 75, 927–931. [Google Scholar] [CrossRef] [PubMed]
- Kim, P.J.; Hong, D.G.; Park, J.Y.; Cho, Y.L.; Park, I.S.; Lee, Y.S. Immunohistochemical expression of YKL-40 in peritoneal endometriosis YKL-40 in peritoneal endometriosis. Gynecol. Endocrinol. 2010, 26, 58–62. [Google Scholar] [CrossRef]
- Tuten, A.; Kucur, M.; Imamoglu, M.; Oncul, M.; Acikgoz, A.S.; Sofiyeva, N.; Ozturk, Z.; Kaya, B.; Oral, E. Serum YKL-40 levels are altered in endometriosis. Gynecol. Endocrinol. 2014, 30, 381–384. [Google Scholar] [CrossRef] [PubMed]
- Ural, U.M.; Tekin, Y.B.; Cüre, M.; Şahin, F.K. Serum YKL-40 levels as a novel marker of inflammation in patients with endometriosis. Clin. Exp. Obstet. Gynecol. 2015, 42, 495–497. [Google Scholar] [CrossRef]
- Johansen, J.S.; Lottenburger, T.; Nielsen, H.J.; Jensen, J.E.B.; Svendsen, M.N.; Kollerup, G.; Christensen, I.J. Diurnal, weekly, and long-time variation in serum concentrations of YKL-40 in healthy subjects. Cancer Epidemiol. Biomark. Prev. 2008, 17, 2603–2608. [Google Scholar] [CrossRef] [PubMed]
- Lima, A.P.; Moura, M.D.; Rosa e Silva, A.A.M. Prolactin and cortisol levels in women with endometriosis. Braz. J. Med. Biol. Res. 2006, 39, 1121–1127. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.K.; Park, J.Y.; Jee, B.C.; Suh, C.S.; Kim, S.H. Association of the neutrophil-to-lymphocyte ratio and CA 125 with the endometriosis score. Clin. Exp. Reprod. Med. 2014, 41, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Karimi-Zarchi, M.; Dehshiri-Zadeh, N.; Sekhavat, L.; Nosouhi, F. Correlation of CA-125 serum level and clinico-pathological characteristic of patients with endometriosis. Int. J. Reprod. Biomed. 2016, 14, 713–718. [Google Scholar] [CrossRef]
- Oliveira, M.A.P.; Raymundo, T.S.; Soares, L.C.; Pereira, T.R.D.; Demôro, A.V.E. How to Use CA-125 more effectively in the diagnosis of deep endometriosis. BioMed Res. Int. 2017, 2017, 9857196. [Google Scholar] [CrossRef] [PubMed]
- Yucel, N.; Baskent, E.; Karamustafaoglu Balci, B.; Goynumer, G. The levonorgestrel-releasing intrauterine system is associated with a reduction in dysmenorrhoea and dyspareunia, a decrease in CA 125 levels, and an increase in quality of life in women with suspected endometriosis. Aust. N. Z. J. Obstet. Gynaecol. 2018, 58, 560–563. [Google Scholar] [CrossRef]
- Kim, B.; Park, Y.; Kim, B.; Ahn, H.J.; Lee, K.A.; Chung, J.E.; Han, S.W. Diagnostic performance of CA 125, HE4, and risk of Ovarian Malignancy Algorithm for ovarian cancer. J. Clin. Lab. Anal. 2019, 33, e22624. [Google Scholar] [CrossRef] [PubMed]
- Ding, S.; Lin, Q.; Zhu, T.; Li, T.; Zhu, L.; Wang, J.; Zhang, X. Is there a correlation between inflammatory markers and coagulation parameters in women with advanced ovarian endometriosis? BMC Womens Health 2019, 19, 169. [Google Scholar] [CrossRef] [PubMed]
- Maiorana, A.; Cicerone, C.; Niceta, M.; Alio, L. Evaluation of Serum CA 125 Levels in Patients with Pelvic Pain Related to Endometriosis. Int. J. Biol. Markers 2007, 22, 200–202. [Google Scholar] [CrossRef] [PubMed]
- Nisenblat, V.; Bossuyt, P.M.M.; Shaikh, R.; Farquhar, C.; Jordan, V.; Scheffers, C.S.; Mol, B.W.J.; Johnson, N.; Hull, M.L. Blood biomarkers for the non-invasive diagnosis of endometriosis. Cochrane Database Syst. Rev. 2016, 5, CD012179. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| E N = 43 | III E N = 20 | IV E N = 23 | NE N = 35 | CONTROL N = 18 | |
|---|---|---|---|---|---|
| MEAN ± SD | MEAN ± SD | MEAN ± SD | MEAN ± SD | MEAN ± SD | |
| IL-1β(pg/mL) | 0.50 ± 0.39 p = 0.011 * | 0.43 ± 0.30 | 0.57 ± 0.44 p = 0.008 * | 0.50 ± 0.41 | 0.27 ± 0.26 |
| IL-6 (pg/mL) | 15.55 ± 36.93 p < 0.001 * | 5.07 ± 10.69 p = 0.018 * | 24.67 ± 48.16 p < 0.001 * p = 0.040 ** | 16.23 ± 31.53 p = 0.010 * | 1.47 ± 1.48 |
| hs-CRP (mg/L) | 12.18 ± 17.73 p = 0.028 * | 2.57 ± 4.24 | 20.53 ± 20.68 p = 0.002 * p = 0.007 ** | 11.80 ± 18.59 p = 0.037 * | 0.96 ± 1.19 |
| IgG (mg/dL) | 1086.04 ± 267.85 p = 0.025 * | 1161.54 ± 250.87 | 1014.14 ± 269.39 p = 0.013 * | 1111.94 ± 293.32 | 1237.28 ± 215.91 |
| YKL-40 (ng/mL) | 590.43 ± 1118.07 p = 0.005 * | 1007.16 ± 1557.98 p = 0.011 * | 257.05 ± 351.05 p = 0.022 * | 449.73 ± 1019.59 | 104.12 ± 154.07 |
| PRL (ng/mL) | 26.80 ± 17.33 p < 0.001 * | 27.58 ± 17.34 p = 0.003 * | 26.10 ± 17.72 p = 0.002 * | 27.55 ± 18.30 p < 0.001 * | 12.84 ± 4.86 |
| CA 125 (U/mL) | 109.56 ± 118.22 p < 0.001 * p < 0.001 *** | 47.55 ± 26.51 p < 0.001 * p < 0.001 *** | 163.48 ± 139.78 p < 0.001 * p < 0.001 ** p < 0.001 *** | 21.84 ± 16.20 | 14.28 ± 7.40 |
| Parameter | IL-1β [pg/mL] | IL-6 [pg/mL] | hs-CRP [mg/L] | IgG [mg/dL] | YKL-40 [ng/mL] | PRL [ng/mL] |
|---|---|---|---|---|---|---|
| IL-1β (pg/mL) | ||||||
| IL-6 (pg/mL) | R = 0.383 p < 0.001 | |||||
| hs-CRP (mg/L) | R = 0.337 p < 0.001 | R = 0.610 p < 0.001 | ||||
| IgG (mg/dL) | NS | R = −0.475 p < 0.001 | R = −0.448 p < 0.001 | |||
| YKL-40 (ng/mL) | R = 0.243 p = 0.008 | NS | NS | R = 0.186 p = 0.043 | ||
| PRL (ng/mL) | R = 0.371 p < 0.001 | R = 0.230 p = 0.008 | R = 0.286 p < 0.001 | NS | NS | |
| CA 125 (U/mL) | R = 0.181 p = 0.043 | R = 0.265 p = 0.003 | R = 0.316 p < 0.001 | R = −0.235 p = 0.009 | NS | R = 0.325 p < 0.001 |
| E | III E | IV E | NE | CONTROL | |
|---|---|---|---|---|---|
| MEAN ± SD | MEAN ± SD | MEAN ± SD | MEAN ± SD | MEAN ± SD | |
| N | 43 | 20 | 23 | 35 | 18 |
| Age [years] | 35 ± 8 | 33 ± 7 | 38 ± 8 | 38 ± 8 | 40 ± 8 |
| BMI [kg/m2] | 24.73 ± 3.43 | 23.80 ± 2.78 | 25.54 ± 3.79 | 25.91 ± 3.00 | 24.51 ± 3.99 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kokot, I.; Piwowar, A.; Jędryka, M.; Sołkiewicz, K.; Kratz, E.M. Diagnostic Significance of Selected Serum Inflammatory Markers in Women with Advanced Endometriosis. Int. J. Mol. Sci. 2021, 22, 2295. https://doi.org/10.3390/ijms22052295
Kokot I, Piwowar A, Jędryka M, Sołkiewicz K, Kratz EM. Diagnostic Significance of Selected Serum Inflammatory Markers in Women with Advanced Endometriosis. International Journal of Molecular Sciences. 2021; 22(5):2295. https://doi.org/10.3390/ijms22052295
Chicago/Turabian StyleKokot, Izabela, Agnieszka Piwowar, Marcin Jędryka, Katarzyna Sołkiewicz, and Ewa Maria Kratz. 2021. "Diagnostic Significance of Selected Serum Inflammatory Markers in Women with Advanced Endometriosis" International Journal of Molecular Sciences 22, no. 5: 2295. https://doi.org/10.3390/ijms22052295
APA StyleKokot, I., Piwowar, A., Jędryka, M., Sołkiewicz, K., & Kratz, E. M. (2021). Diagnostic Significance of Selected Serum Inflammatory Markers in Women with Advanced Endometriosis. International Journal of Molecular Sciences, 22(5), 2295. https://doi.org/10.3390/ijms22052295