
PPAR-Gamma Activation May Inhibit the In Vivo Degeneration of Bioprosthetic Aortic and Aortic Valve Grafts under Diabetic Conditions


 ,
, 
Abstract
:1. Introduction
2. Results
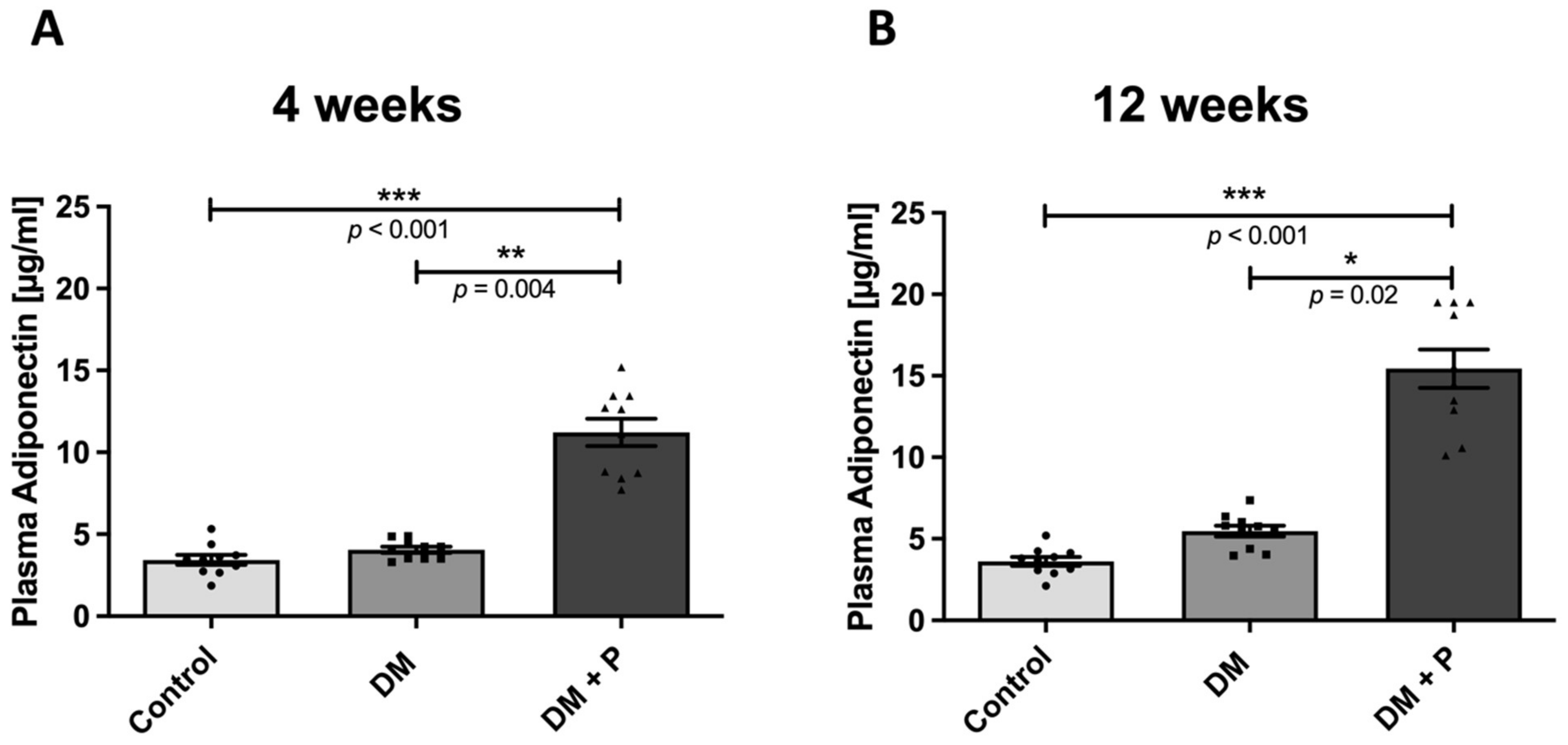
2.1. Body Weight, Blood Glucose Changes, and Plasma Analysis
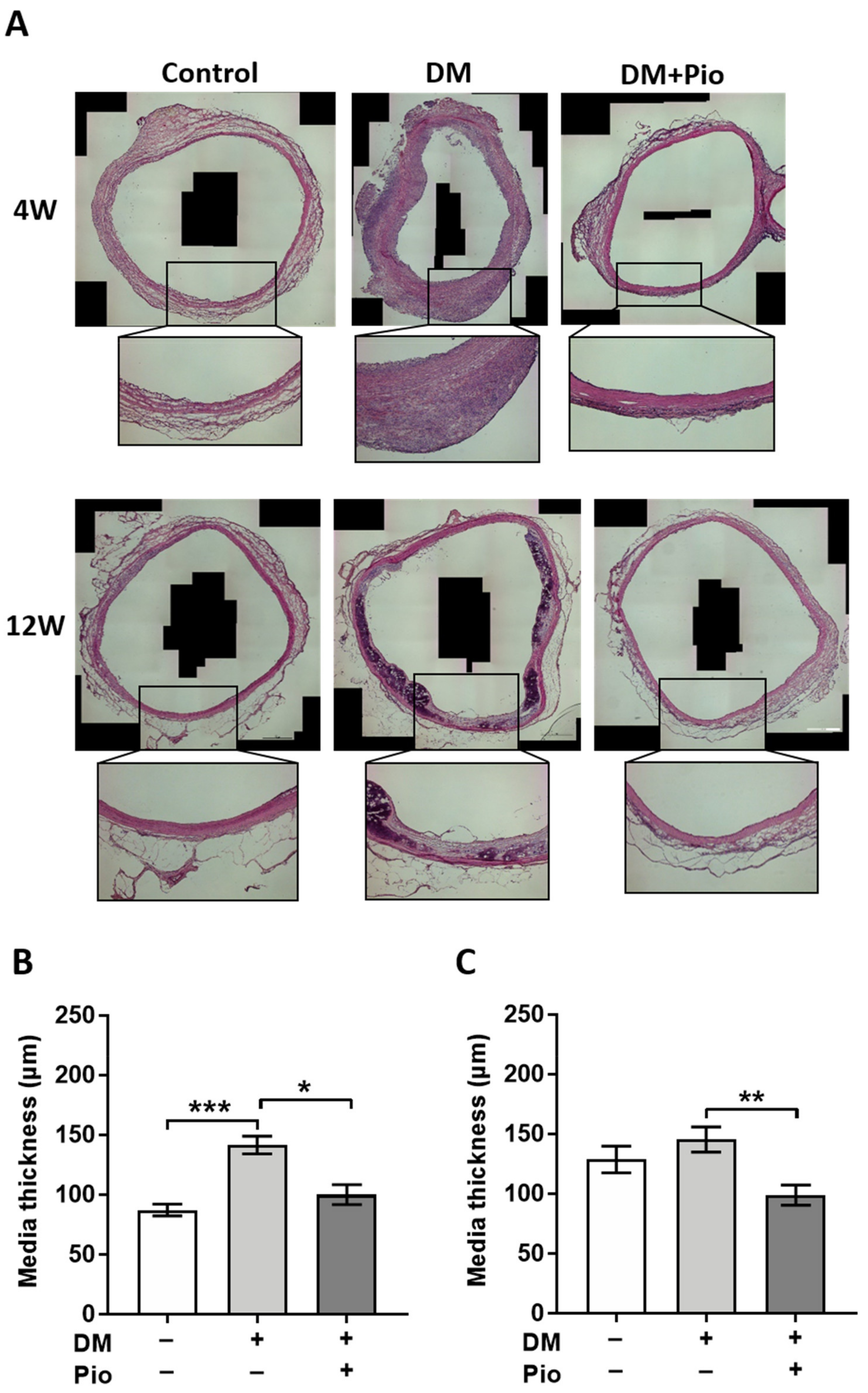
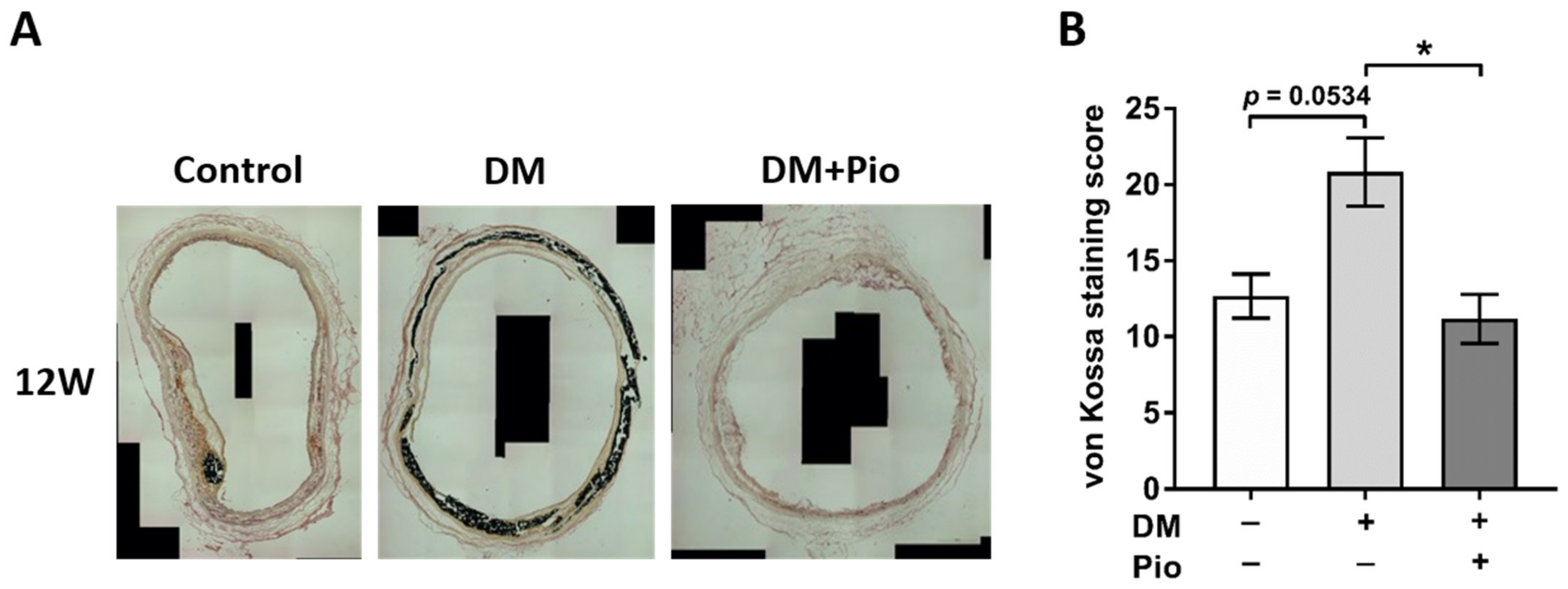
2.2. Histological Changes and Remodeling of the Aortic Wall
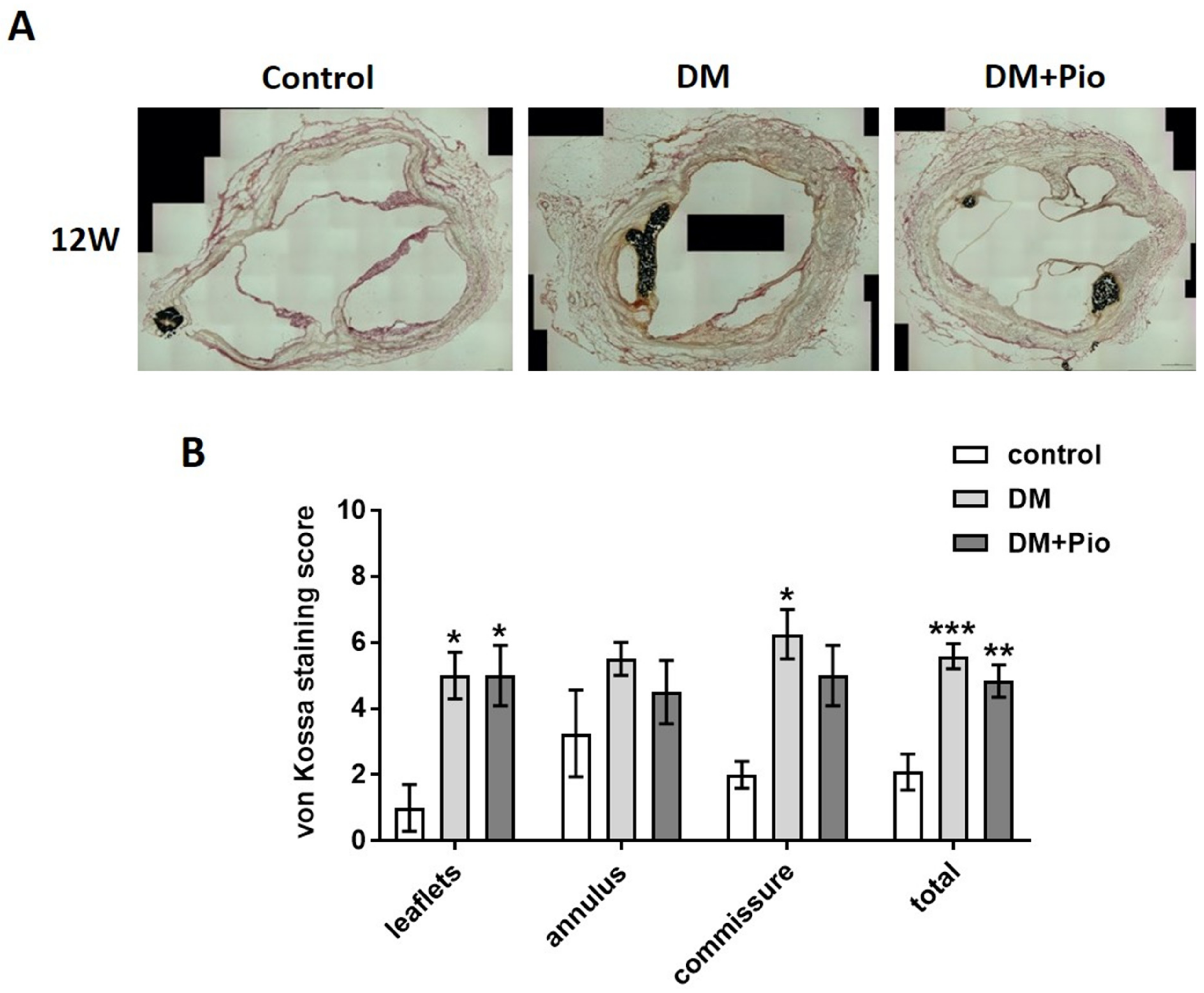
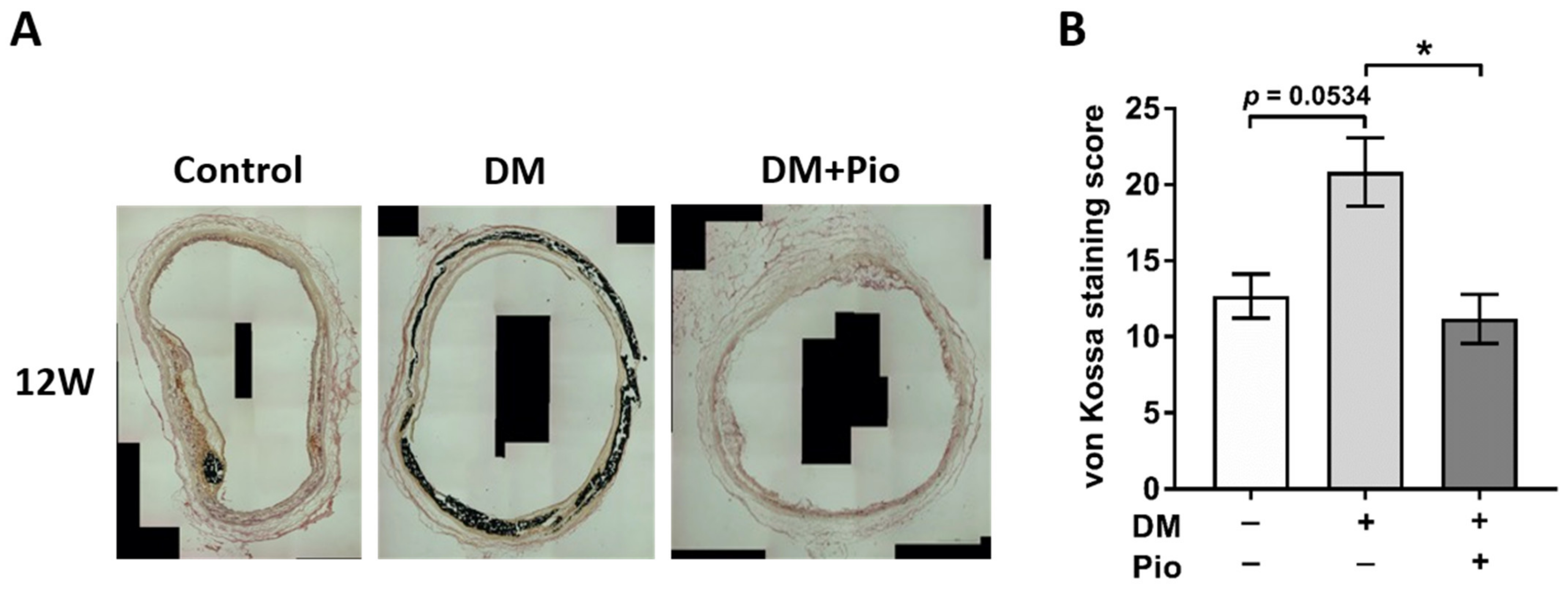
2.3. Degenerative Changes at the Level of the Bioprosthetic Aortic Valve
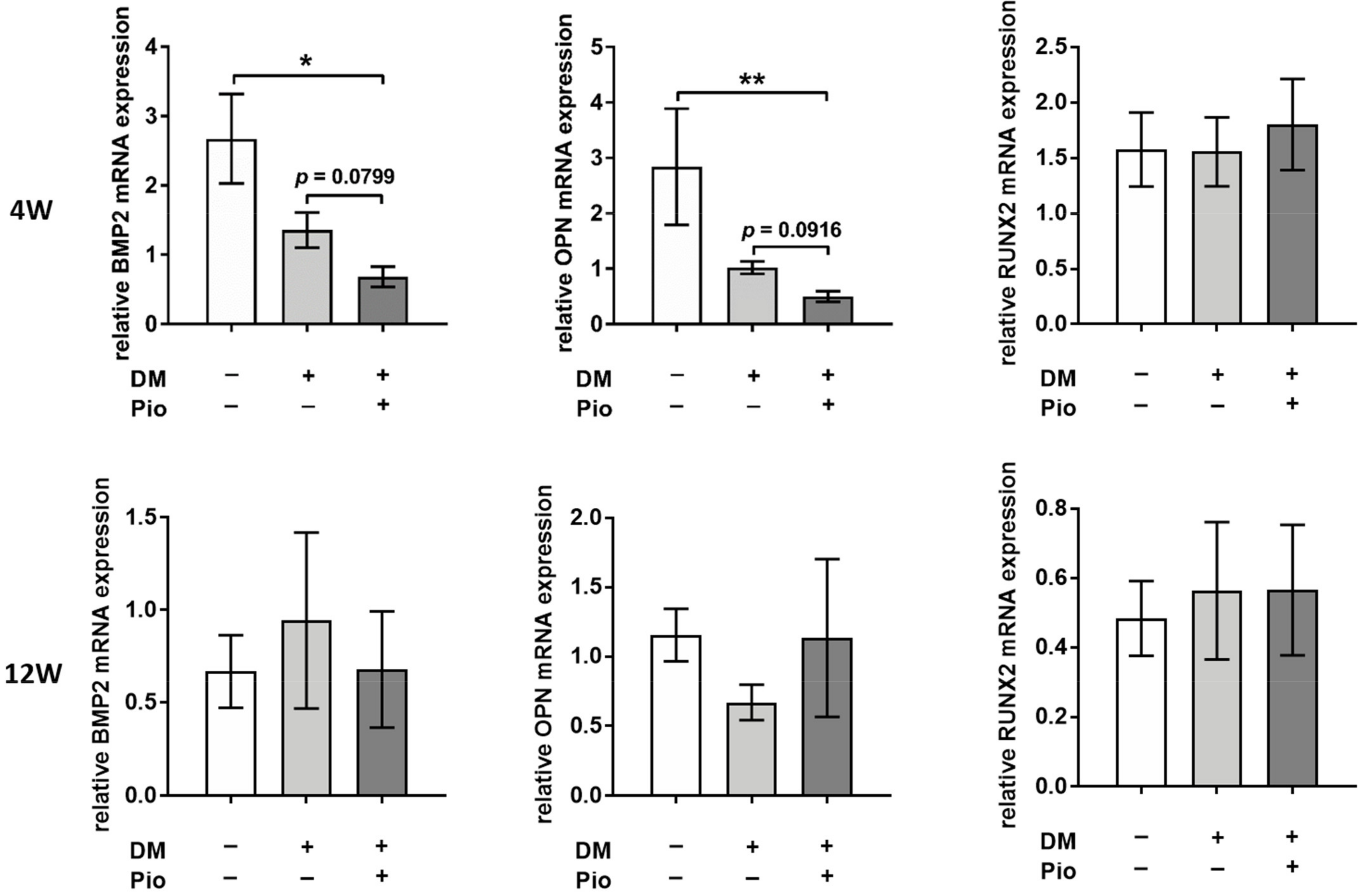
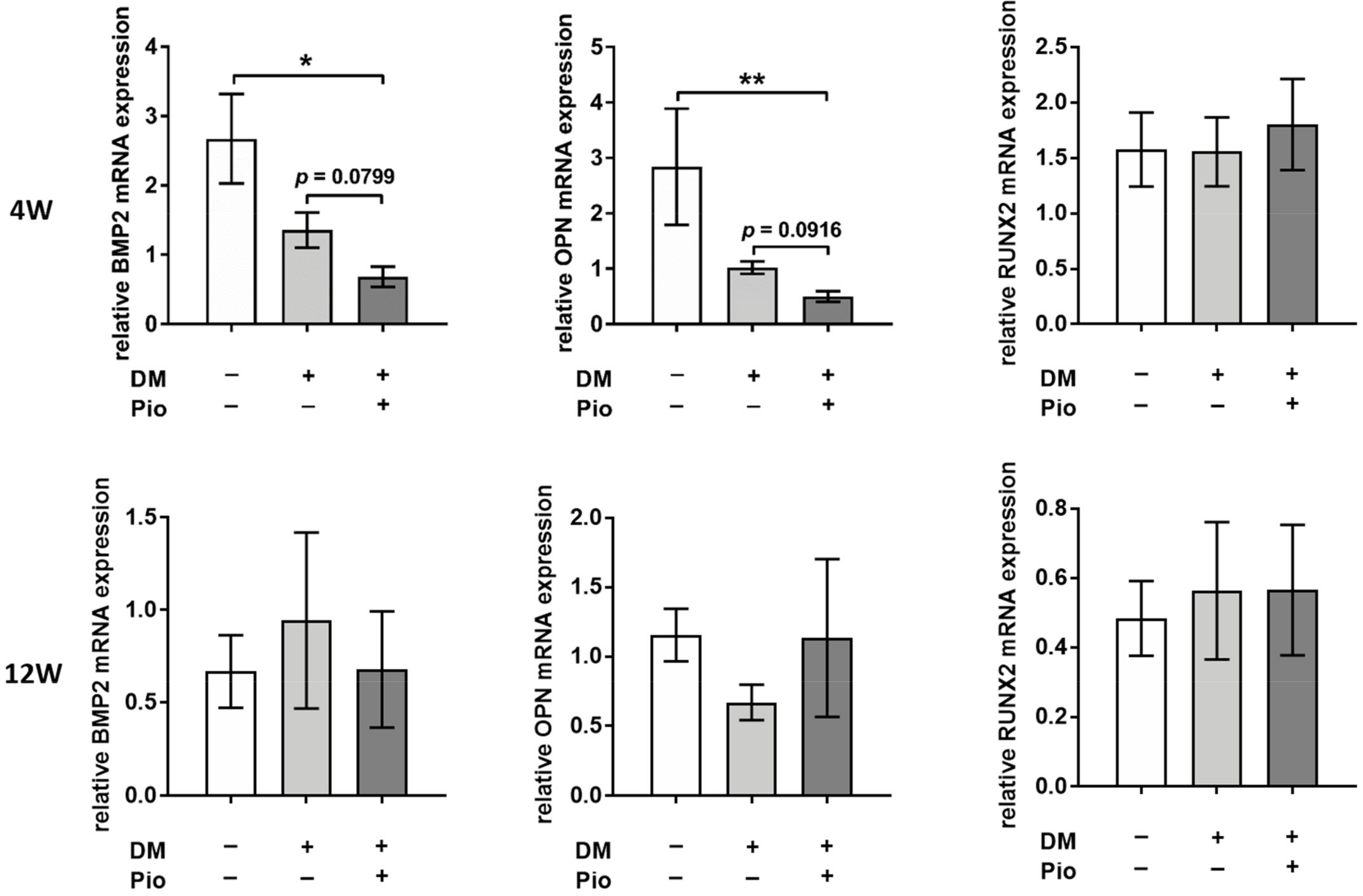
2.4. Gene-Expression Analysis of Explanted Bioprosthetic Grafts
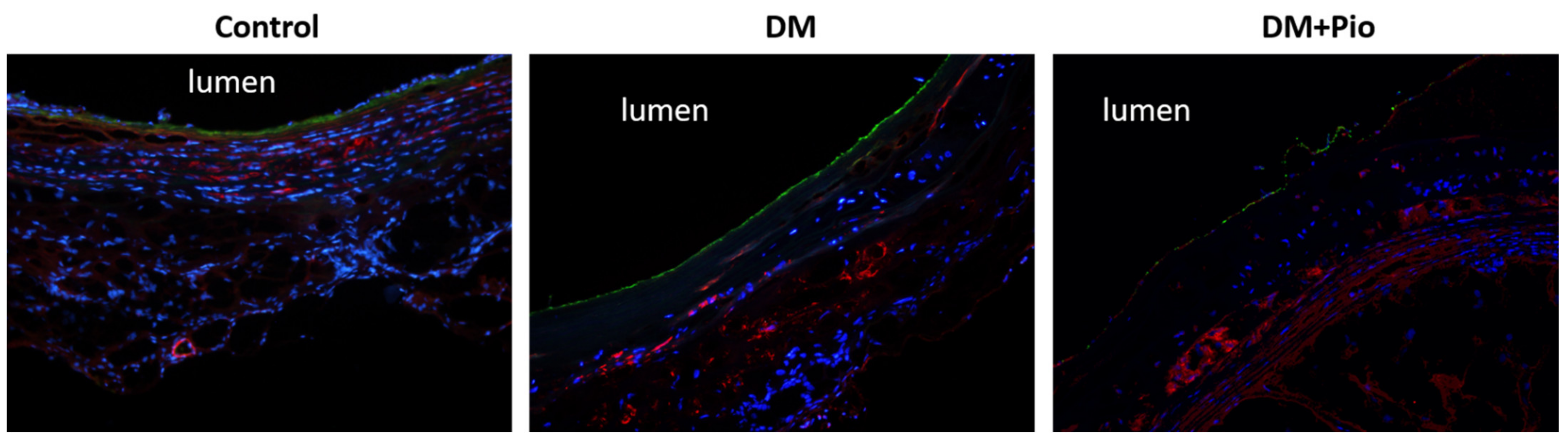
2.5. Identification of Cellular Remodeling
3. Discussion
4. Materials and Methods
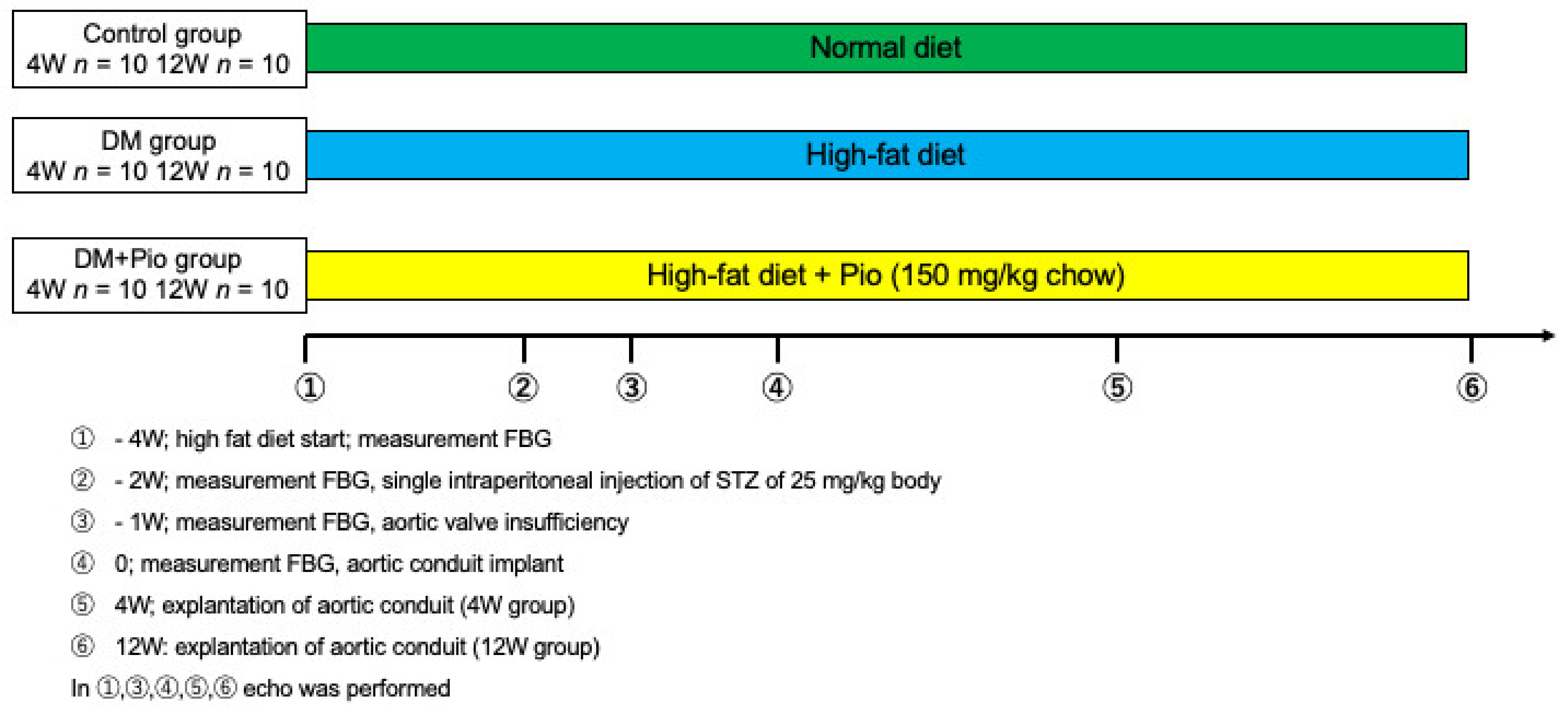
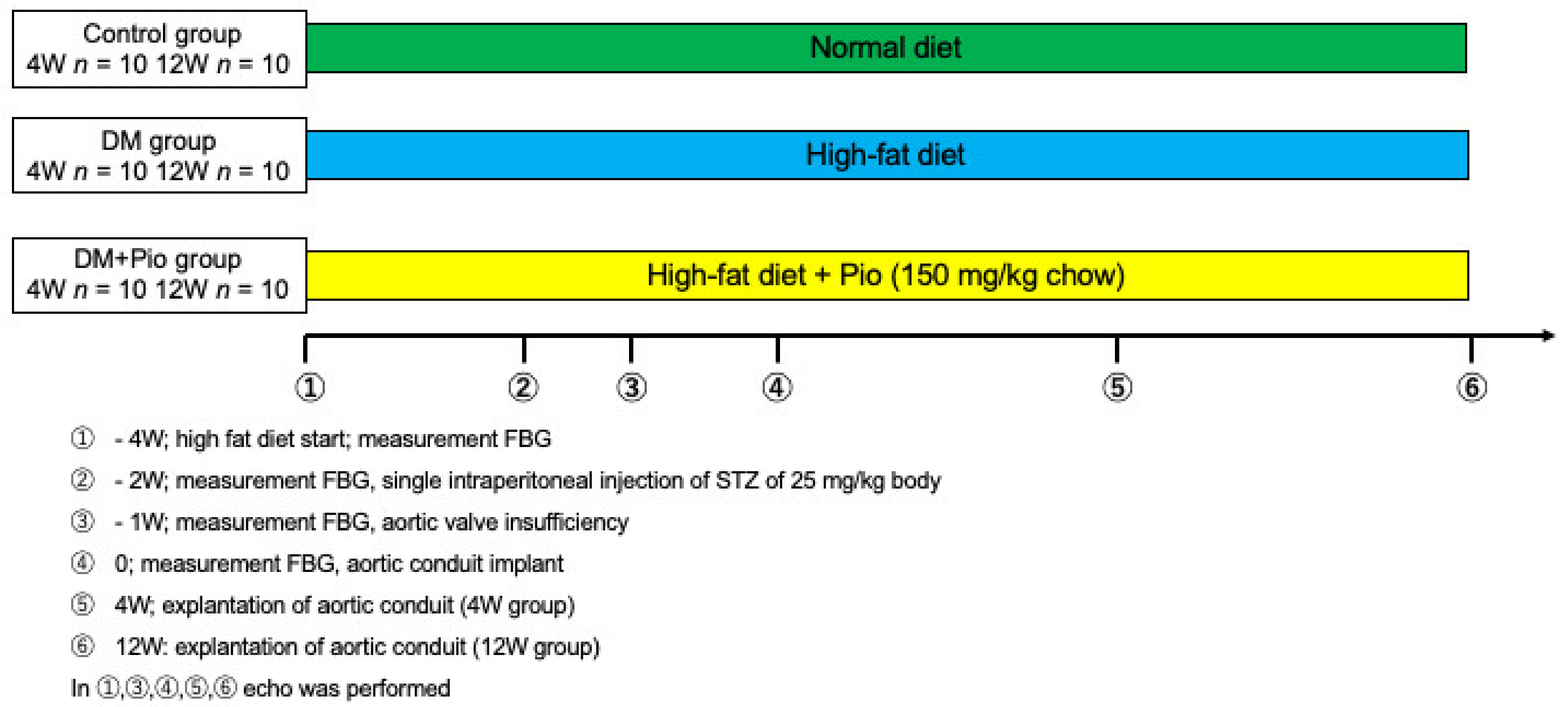
4.1. Animals and Experiment Protocol
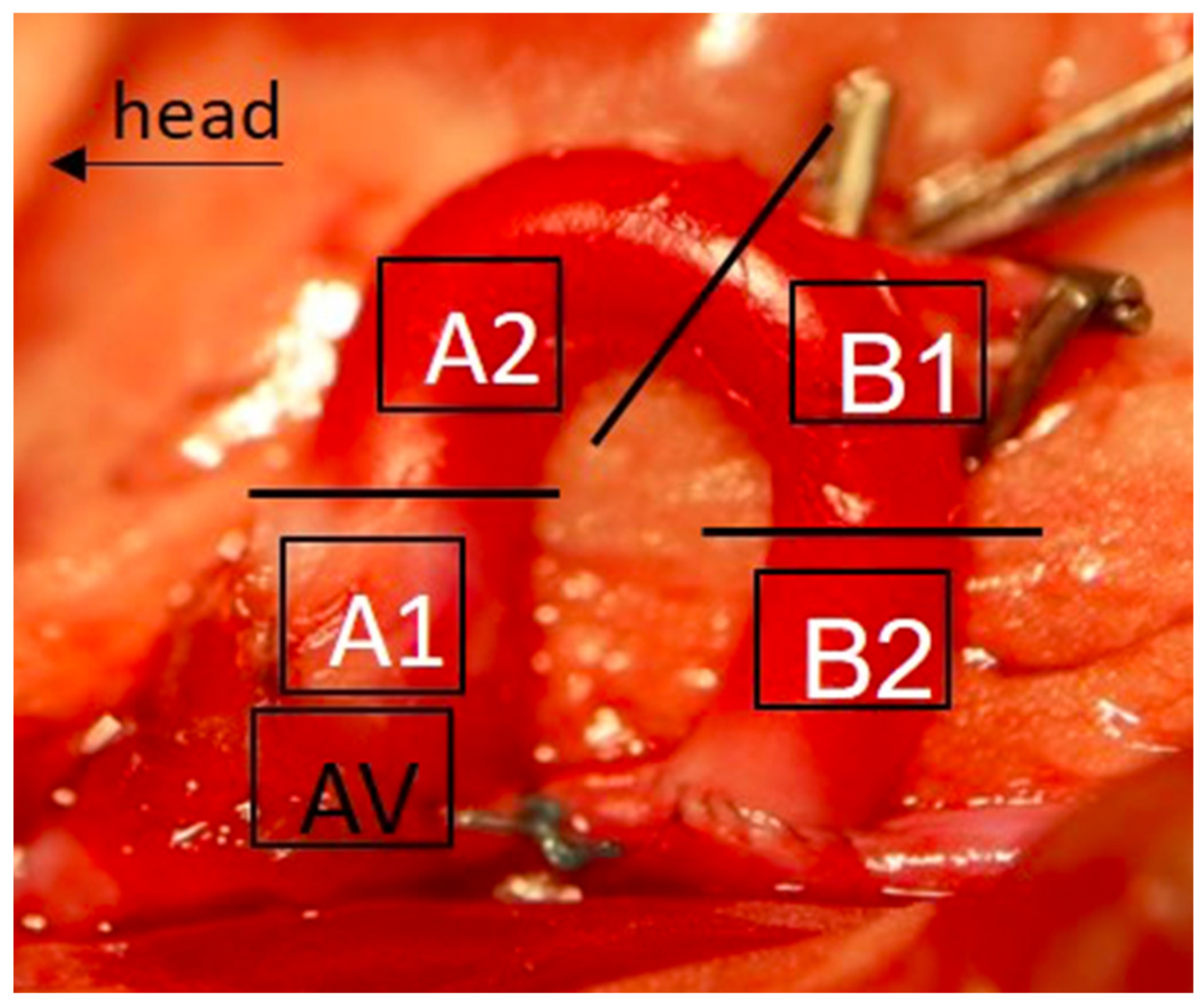
4.2. Donor Graft Harvesting and Cryopreserved Graft Preparation
4.3. Blood Serum Analyses
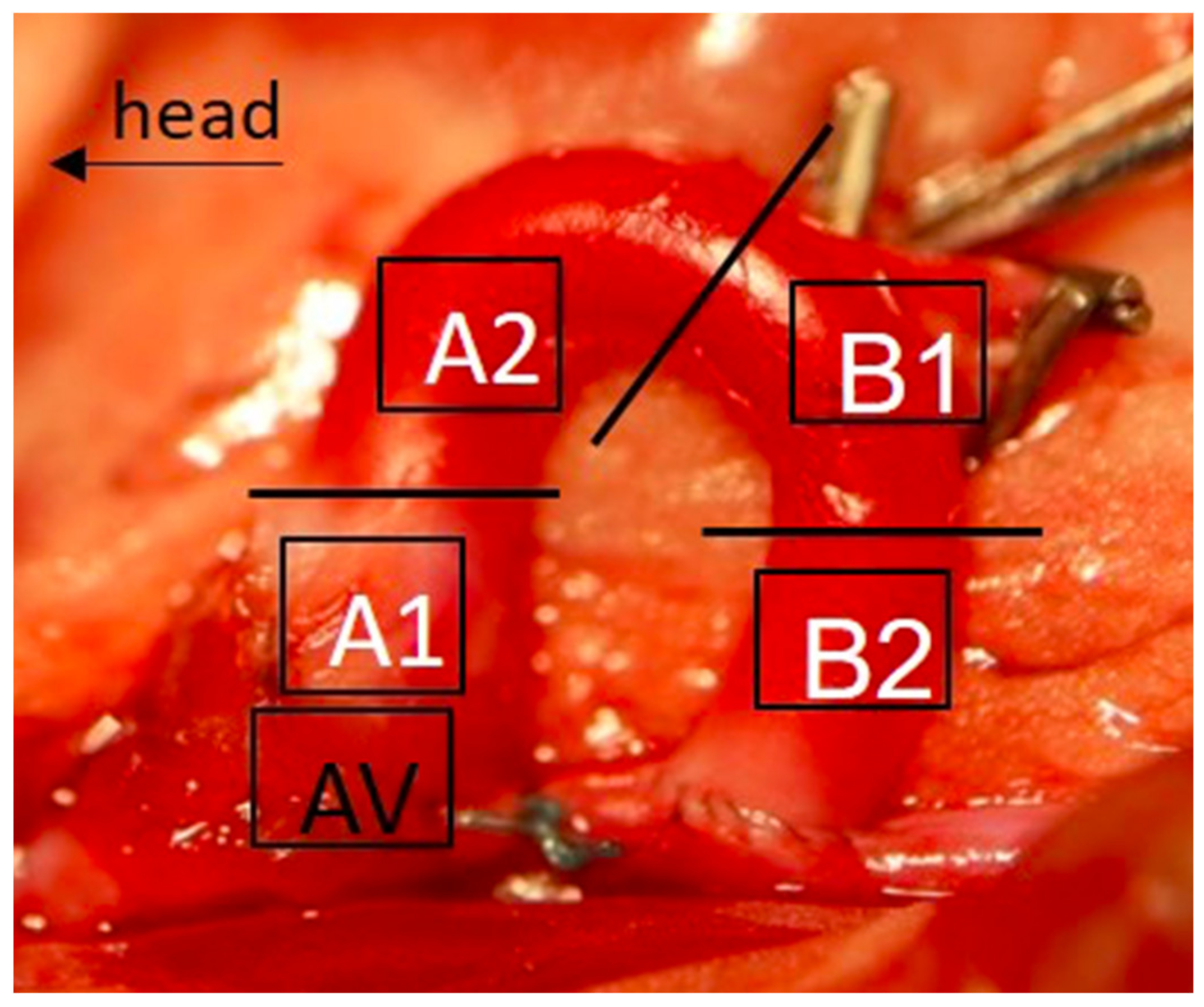
4.4. Histological Evaluation
4.5. Gene-Expression Analysis
4.6. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Le Quang, K.; Bouchareb, R.; Lachance, D.; Laplante, M.-A.; El Husseini, D.; Boulanger, M.-C.; Fournier, D.; Fang, X.P.; Avramoglu, R.K.; Pibarot, P.; et al. Early Development of Calcific Aortic Valve Disease and Left Ventricular Hypertrophy in a Mouse Model of Combined Dyslipidemia and Type 2 Diabetes Mellitus. Arter. Thromb. Vasc. Biol. 2014, 34, 2283–2291. [Google Scholar] [CrossRef] [PubMed]
- Selig, J.I.; Ouwens, D.M.; Raschke, S.; Thoresen, G.H.; Fischer, J.W.; Lichtenberg, A.; Akhyari, P.; Barth, M. Impact of hyperinsulinemia and hyperglycemia on valvular interstitial cells—A link between aortic heart valve degeneration and type 2 diabetes. Biochim. Biophys. Acta (BBA)—Mol. Basis Dis. 2019, 1865, 2526–2537. [Google Scholar] [CrossRef] [PubMed]
- Tazaki, J.; Shiomi, H.; Morimoto, T.; Imai, M.; Yamaji, K.; Sakata, R.; Okabayashi, H.; Hanyu, M.; Shimamoto, M.; Nishiwaki, N.; et al. Three-year outcome after percutaneous coronary intervention and coronary artery bypass grafting in patients with triple-vessel coronary artery disease: Observations from the CREDO-Kyoto PCI/CABG registry cohort-2. EuroIntervention 2013, 9, 437–445. [Google Scholar] [CrossRef] [PubMed]
- Yki-Jarvinen, H. Thiazolidinediones. N. Engl. J. Med. 2004, 351, 1106–1118. [Google Scholar] [CrossRef]
- Nakamura, T.; Yamamoto, E.; Kataoka, K.; Yamashita, T.; Tokutomi, Y.; Dong, Y.-F.; Matsuba, S.; Ogawa, H.; Kim-Mitsuyama, S. Beneficial Effects of Pioglitazone on Hypertensive Cardiovascular Injury Are Enhanced by Combination With Candesartan. Hypertension 2008, 51, 296–301. [Google Scholar] [CrossRef] [Green Version]
- Ricote, M.; Li, A.C.; Willson, T.M.; Kelly, C.J.; Glass, C.K. The peroxisome proliferator-activated receptor-gamma is a negative regulator of macrophage activation. Nature 1998, 391, 79–82. [Google Scholar] [CrossRef]
- Al-Awar, A.; Kupai, K.; Veszelka, M.; Szűcs, G.; Attieh, Z.; Murlasits, Z.; Török, S.; Pósa, A.; Varga, C. Experimental Diabetes Mellitus in Different Animal Models. J. Diabetes Res. 2016, 2016, 9051426. [Google Scholar] [CrossRef] [Green Version]
- Mansor, L.S.; Gonzalez, E.R.; Cole, M.A.; Tyler, D.J.; Beeson, J.H.; Clarke, K.; Carr, C.A.; Heather, L.C. Cardiac metabolism in a new rat model of type 2 diabetes using high-fat diet with low dose streptozotocin. Cardiovasc. Diabetol. 2013, 12, 136. [Google Scholar] [CrossRef] [Green Version]
- Islam, M.S.; Loots, D.T. Experimental rodent models of type 2 diabetes: A review. Methods Find. Exp. Clin. Pharmacol. 2009, 31, 249–261. [Google Scholar] [CrossRef]
- Zucker, L.M.; Antoniades, H.N. Insulin and Obesity in the Zucker Genetically Obese Rat “Fatty”. Endocrinology 1972, 90, 1320–1330. [Google Scholar] [CrossRef] [PubMed]
- Kawano, K.; Hirashima, T.; Mori, S.; Saitoh, Y.; Kurosumi, M.; Natori, T. Spontaneous Long-Term Hyperglycemic Rat with Diabetic Complications: Otsuka Long-Evans Tokushima Fatty (OLETF) Strain. Diabetes 1992, 41, 1422–1428. [Google Scholar] [CrossRef]
- Kawamori, R.; Kadowaki, T.; Onji, M.; Seino, Y.; Akanuma, Y.; PRACTICAL Study Group. Hepatic safety profile and glycemic control of pioglitazone in more than 20,000 patients with type 2 diabetes mellitus: Postmarketing surveillance study in Japan. Diabetes Res. Clin. Pract. 2007, 76, 229–235. [Google Scholar] [CrossRef]
- Alam, F.; Islam, A.; Mohamed, M.; Ahmad, I.; Kamal, M.A.; Donnelly, R.; Idris, I.; Gan, S.H. Efficacy and Safety of Pioglitazone Monotherapy in Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Sci. Rep. 2019, 9, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Dormandy, J.A.; Charbonnel, B.; Eckland, D.J.; Erdmann, E.; Massi-Benedetti, M.; Moules, I.K.; Skene, A.M.; Tan, M.H.; Lefèbvre, P.J.; Murray, G.D.; et al. Secondary prevention of macrovascular events in patients with type 2 diabetes in the PROactive Study (PROspective pioglitAzone Clinical Trial In macroVascular Events): A randomised controlled trial. Lancet 2005, 366, 1279–1289. [Google Scholar] [CrossRef]
- Mazzone, T.; Meyer, P.M.; Feinstein, S.B.; Davidson, M.H.; Kondos, G.T.; D’Agostino, R.B.; Perez, A.; Provost, J.-C.; Haffner, S.M. Effect of Pioglitazone Compared With Glimepiride on Carotid Intima-Media Thickness in Type 2 Diabetes. JAMA 2006, 296, 2572–2581. [Google Scholar] [CrossRef]
- Towler, D.A. Molecular and Cellular Aspects of Calcific Aortic Valve Disease. Circ. Res. 2013, 113, 198–208. [Google Scholar] [CrossRef] [Green Version]
- Rajamannan, N.M.; Evans, F.J.; Aikawa, E.; Grande-Allen, K.J.; Demer, L.; Heistad, D.D.; Simmons, C.A.; Masters, K.S.; Mathieu, P.; O’Brien, K.D.; et al. Calcific Aortic Valve Disease: Not Simply a Degenerative Process. Circulation 2011, 124, 1783–1791. [Google Scholar] [CrossRef] [Green Version]
- Rattazzi, M.; Bertacco, E.; Del Vecchio, A.; Puato, M.; Faggin, E.; Pauletto, P. Aortic valve calcification in chronic kidney disease. Nephrol. Dial. Transplant. 2013, 28, 2968–2976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olsson, M.; Thyberg, J.; Nilsson, J. Presence of Oxidized Low Density Lipoprotein in Nonrheumatic Stenotic Aortic Valves. Arter. Thromb. Vasc. Biol. 1999, 19, 1218–1222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, F.; Cai, Z.; Chen, F.; Shi, X.; Zhang, Q.; Chen, S.; Shi, J.; Wang, D.W.; Dong, N. Pioglitazone attenuates progression of aortic valve calcification via down-regulating receptor for advanced glycation end products. Basic Res. Cardiol. 2012, 107, 306. [Google Scholar] [CrossRef] [PubMed]
- Yasunari, E.; Takeno, K.; Funayama, H.; Tomioka, S.; Tamaki, M.; Fujitani, Y.; Kawamori, R.; Watada, H.; Hirose, T. Efficacy of pioglitazone on glycemic control and carotid intima-media thickness in type 2 diabetes patients with inadequate insulin therapy. J. Diabetes Investig. 2010, 2, 56–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Assmann, A.; Zwirnmann, K.; Heidelberg, F.; Schiffer, F.; Horstkötter, K.; Munakata, H.; Gremse, F.; Barth, M.; Lichtenberg, A.; Akhyari, P. The degeneration of biological cardiovascular prostheses under pro-calcific metabolic conditions in a small animal model. Biomaterials 2014, 35, 7416–7428. [Google Scholar] [CrossRef] [PubMed]
- Munakata, H.; Assmann, A.; Poudel-Bochmann, B.; Horstkötter, K.; Kamiya, H.; Okita, Y.; Lichtenberg, A.; Akhyari, P. Aortic Conduit Valve Model With Controlled Moderate Aortic Regurgitation in Rats. Circ. J. 2013, 77, 2295–2302. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 4 Week | 12 Week | |||||
|---|---|---|---|---|---|---|
| Control | DM | DM + p | Control | DM | DM + p | |
| (n = 10) | (n = 10) | (n = 10) | (n = 10) | (n = 10) | (n = 10) | |
| Body Weight(g) | ||||||
| Start | 274.8 ± 13.8 | 270.7 ± 19.8 | 273.5 ± 22.6 | 271.2 ± 11.3 | 263.2 ± 17.4 | 260.3 ± 10.8 |
| EXP | 433.2 ± 12.4 | 492 ± 42.6 # | 519.6 ± 73.9 # | 535.9 ± 45.3 | 668.8 ± 73.4 # | 701.5 ± 61.7 # |
| Glucose(mg/dL) | ||||||
| Start | 113.2 ± 8.8 | 113.8 ± 7.9 | 122.5 ± 9.3 | 114.4 ± 7.6 | 108.1 ± 12.6 | 105.7 ± 11 |
| EXP | 124.7 ± 15.7 | 197.7 ± 30.1 # | 185.6 ± 21.5 # | 118.6 ± 21.5 | 203.5 ± 21.5 # | 174 ± 21.4 # |
| K (mmol/L) | 3.3 ± 0.3 | 3.9 ± 0.5 # | 3.51 ± 0.5 | 3.3 ± 0.2 | 3.6 ± 0.2 | 3.5 ± 0.3 |
| Ca (mg/dL) | 2.1 ± 0.2 | 2.2 ± 0.2 | 2.1 ± 0.2 | 2.3 ± 0.1 | 2.3 ± 0.2 | 2.2 ± 0.1 |
| Cre (mg/dL) | 0.28 ± 0.1 | 0.32 ± 0.1 | 0.3 ± 0.1 | 0.35 ± 0.1 | 0.38 ± 0.07 | 0.35 ± 0.1 |
| T-Cho (mg/dL) | 48.6 ± 7.3 | 67.1 ± 11.8 # | 53.7 ± 9.2 * | 59.4 ± 9.9 | 71.1 ± 12.2 | 68.2 ± 13 |
| TG (mg/dL) | 46 ± 10.3 | 152.9 ± 65.3 # | 93.4 ± 29.9 # | 79.5 ± 32 | 132 ± 46 | 101 ± 35 |
| HDL (mg/dL) | 29.5 ± 5.8 | 43.8 ± 10.7 # | 33.8 ± 8.5 | 38.8 ± 9.1 | 47.7 ± 10.3 # | 46.2 ± 9.7 |
| LDL (mg/dL) | 10.5 ± 1.7 | 11.5 ± 3.2 | 13.2 ± 2.8 | 12.2 ± 2.8 | 12.9 ± 4 | 12.9 ± 4 |
| AST (IU/L) | 95 ± 43.8 | 77.4 ± 22.4 | 69.6 ± 15.7 | 64.3 ± 11.9 | 87.9 ± 32.5 | 75.1 ± 13.5 |
| ALT (IU/L) | 36 ± 7.6 | 53.5 ± 17.5 # | 63.8 ± 13.2 # | 48.3 ± 13.9 | 54.3 ± 15.7 | 67.9 ± 20.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Katahira, S.; Sugimura, Y.; Grupp, S.; Doepp, R.; Selig, J.I.; Barth, M.; Lichtenberg, A.; Akhyari, P. PPAR-Gamma Activation May Inhibit the In Vivo Degeneration of Bioprosthetic Aortic and Aortic Valve Grafts under Diabetic Conditions. Int. J. Mol. Sci. 2021, 22, 11081. https://doi.org/10.3390/ijms222011081
Katahira S, Sugimura Y, Grupp S, Doepp R, Selig JI, Barth M, Lichtenberg A, Akhyari P. PPAR-Gamma Activation May Inhibit the In Vivo Degeneration of Bioprosthetic Aortic and Aortic Valve Grafts under Diabetic Conditions. International Journal of Molecular Sciences. 2021; 22(20):11081. https://doi.org/10.3390/ijms222011081
Chicago/Turabian StyleKatahira, Shintaro, Yukiharu Sugimura, Sophia Grupp, Robin Doepp, Jessica Isabel Selig, Mareike Barth, Artur Lichtenberg, and Payam Akhyari. 2021. "PPAR-Gamma Activation May Inhibit the In Vivo Degeneration of Bioprosthetic Aortic and Aortic Valve Grafts under Diabetic Conditions" International Journal of Molecular Sciences 22, no. 20: 11081. https://doi.org/10.3390/ijms222011081
APA StyleKatahira, S., Sugimura, Y., Grupp, S., Doepp, R., Selig, J. I., Barth, M., Lichtenberg, A., & Akhyari, P. (2021). PPAR-Gamma Activation May Inhibit the In Vivo Degeneration of Bioprosthetic Aortic and Aortic Valve Grafts under Diabetic Conditions. International Journal of Molecular Sciences, 22(20), 11081. https://doi.org/10.3390/ijms222011081