
Candidate Genes and Proteomic Biomarkers of Serum and Urine in Medication-Overuse Headache

 ,
,  , ,
, , 
Abstract
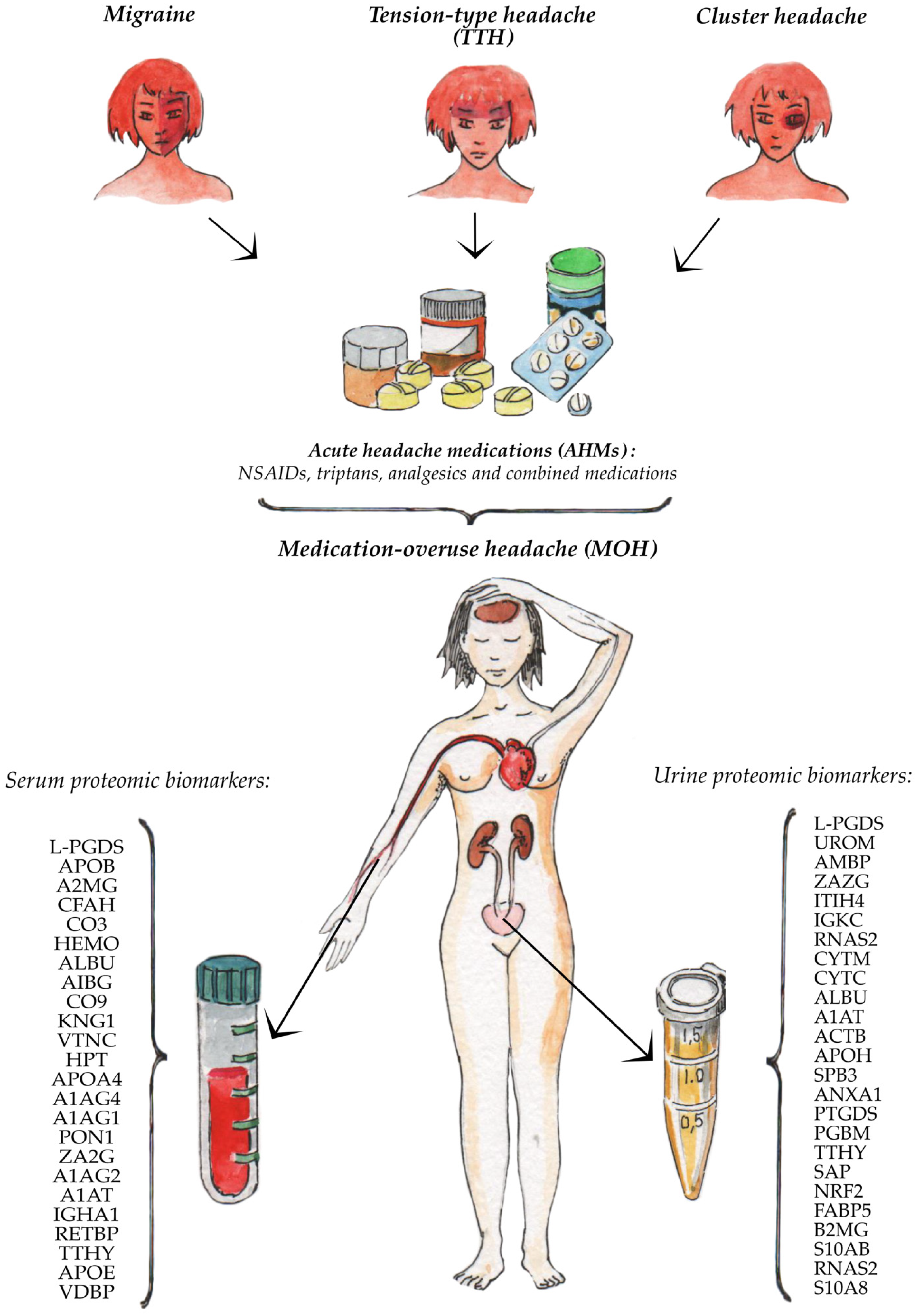
1. Introduction
2. Materials and Methods
3. Results
3.1. Candidate Serum Proteomic Biomarkers of Patients with Medication-Overuse Headache
3.2. Candidate Urine Proteomic Biomarkers of Patients with Medication-Overuse Headache
4. Discussion
4.1. The Promising Serum and Urinary Proteomic Biomarkers of Medication-Overuse Headache
4.2. Limitations
4.3. Summary
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Van Hecke, O.; Torrance, N.; Smith, B.H. Chronic pain epidemiology and its clinical relevance. Br. J. Anaesth. 2013, 111, 13–18. [Google Scholar] [CrossRef]
- Gaskin, D.J.; Richard, P. The Economic Costs of Pain in the United States. J. Pain 2012, 13, 715–724. [Google Scholar] [CrossRef]
- Stovner, L.J.; Zwart, J.-A.; Hagen, K.; Terwindt, G.M.; Pascual, J. Epidemiology of headache in Europe. Eur. J. Neurol. 2006, 13, 333–345. [Google Scholar] [CrossRef]
- Scher, A.I.; Lipton, R.B.; Stewart, W.F.; Bigal, M. Patterns of medication use by chronic and episodic headache sufferers in the general population: Results from the frequent headache epidemiology study. Cephalalgia 2009, 30, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Katsarava, Z. Medication-Overuse Headache (MOH). Comorbidities Headache Disord. 2016, 207–222. [Google Scholar] [CrossRef]
- Diener, H.-C.; Dodick, D.; Evers, S.; Holle, D.; Jensen, R.H.; Lipton, R.B.; Porreca, F.; Silberstein, S.; Schwedt, T. Pathophysiology, prevention, and treatment of medication overuse headache. Lancet Neurol. 2019, 18, 891–902. [Google Scholar] [CrossRef]
- Wakerley, B.R. Medication-overuse headache: Painkillers are not always the answer. Br. J. Gen. Pract. 2020, 70, 58–59. [Google Scholar] [CrossRef]
- Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia 2013, 33, 629–808. [CrossRef] [PubMed]
- Westergaard, M.L.; Hansen, E.H.; Glümer, C.; Olesen, J.; Jensen, R.H. Definitions of medication-overuse headache in population-based studies and their implications on prevalence estimates: A systematic review. Cephalalgia 2014, 34, 409–425. [Google Scholar] [CrossRef]
- Ayzenberg, I.; Katsarava, Z.; Sborowski, A.; Chernysh, M.; Osipova, V.; Tabeeva, G.; Yakhno, N.; Steiner, T.J.; Burden, O.B.O.L.T. The prevalence of primary headache disorders in Russia: A countrywide survey. Cephalalgia 2012, 32, 373–381. [Google Scholar] [CrossRef]
- Vandenbussche, N.; Laterza, D.; Lisicki, M.; Lloyd, J.; Lupi, C.; Tischler, H.; Toom, K.; Vandervorst, F.; Quintana, S.; Paemeleire, K.; et al. Medication-overuse headache: A widely recognized entity amidst ongoing debate. J. Headache Pain 2018, 19, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Jonsson, P.; Hedenrud, T.; Linde, M.; Bjerkeli, P. Epidemiology of medication overuse headache in the general Swedish population. Cephalalgia 2011, 31, 1015–1022. [Google Scholar] [CrossRef]
- Wang, S.-J.; Fuh, J.-L.; Lu, S.-R.; Liu, C.-Y.; Hsu, L.-C.; Wang, P.-N.; Liu, H.-C. Chronic daily headache in Chinese elderly: Prevalence, risk factors, and biannual follow-up. Neurology 2000, 54, 314. [Google Scholar] [CrossRef] [PubMed]
- Straube, A.; Pfaffenrath, V.; Ladwig, K.-H.; Meisinger, C.; Hoffmann, W.; Fendrich, K.; Vennemann, M.; Berger, K. Prevalence of chronic migraine and medication overuse headache in Germany—The German DMKG headache study. Cephalalgia 2009, 30, 207–213. [Google Scholar] [CrossRef]
- Kristoffersen, E.S.; Lundqvist, C. Medication-overuse headache: Epidemiology, diagnosis and treatment. Ther. Adv. Drug Saf. 2014, 5, 87–99. [Google Scholar] [CrossRef] [PubMed]
- Bahra, A.; Walsh, M.; Menon, S.; Goadsby, P.J. Does Chronic Daily Headache Arise De Novo in Association With Regular Use of Analgesics? Headache J. Head Face Pain 2003, 43, 179–190. [Google Scholar] [CrossRef] [PubMed]
- Suchkov, S.; Kostyushev, D.; Krynskii, S.; Gnatenko, D.; Paltsev, M.A. Proteomics as a Fundamental Tool for Subclinical Screening, Tests Verification and Assessment of Applied Therapy. Ann. Russ. Acad. Med. Sci. 2013, 68, 65–71. [Google Scholar] [CrossRef][Green Version]
- Fredriksson, S.; Horecka, J.; Brustugun, O.T.; Schlingemann, J.; Koong, A.C.; Tibshirani, R.; Davis, R.W. Multiplexed Proximity Ligation Assays to Profile Putative Plasma Biomarkers Relevant to Pancreatic and Ovarian Cancer. Clin. Chem. 2008, 54, 582–589. [Google Scholar] [CrossRef]
- Fredriksson, S.; Dixon, W.; Ji, H.; Koong, A.C.; Mindrinos, M.; Davis, R.W. Multiplexed protein detection by proximity ligation for cancer biomarker validation. Nat. Chem. Biol. 2007, 4, 327–329. [Google Scholar] [CrossRef]
- Kwok, Y.H. Potential Peripheral Biomarkers for Chronic Pain. Ph.D. Thesis, The University of Adelaide, Adelaide, Australia, June 2014. Available online: https://digital.library.adelaide.edu.au/dspace/bitstream/2440/88013/9/01front.pdf (accessed on 15 June 2021).
- Bellei, E.; Cuoghi, A.; Monari, E.; Bergamini, S.; Fantoni, L.I.; Zappaterra, M.; Guerzoni, S.; Bazzocchi, A.; Tomasi, A.; Pini, L.A. Proteomic analysis of urine in medication-overuse headache patients: Possible relation with renal damages. J. Headache Pain 2012, 13, 45–52. [Google Scholar] [CrossRef][Green Version]
- Liangos, O.; Perianayagam, M.C.; Vaidya, V.S.; Han, W.K.; Wald, R.; Tighiouart, H.; MacKinnon, R.W.; Li, L.; Balakrishnan, V.S.; Pereira, B.J.; et al. Urinary N-Acetyl-β-(D)-Glucosaminidase Activity and Kidney Injury Molecule-1 Level Are Associated with Adverse Outcomes in Acute Renal Failure. J. Am. Soc. Nephrol. 2007, 18, 904–912. [Google Scholar] [CrossRef]
- Bellei, E.; Monari, E.; Cuoghi, A.; Bergamini, S.; Guerzoni, S.; Ciccarese, M.; Ozben, T.; Tomasi, A.; Pini, L.A. Discovery by a proteomic approach of possible early biomarkers of drug-induced nephrotoxicity in medication-overuse headache. J. Headache Pain 2013, 14, 6. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Bellei, E.; Vilella, A.; Monari, E.; Bergamini, S.; Tomasi, A.; Cuoghi, A.; Guerzoni, S.; Manca, L.; Zoli, M.; Pini, L.A. Serum protein changes in a rat model of chronic pain show a correlation between animal and humans. Sci. Rep. 2017, 7, 41723. [Google Scholar] [CrossRef]
- Vacca, V.; Marinelli, S.; Pieroni, L.; Urbani, A.; Luvisetto, S.; Pavone, F. Higher pain perception and lack of recovery from neuropathic pain in females: A behavioural, immunohistochemical, and proteomic investigation on sex-related differences in mice. Pain 2014, 155, 388–402. [Google Scholar] [CrossRef]
- Vacca, V.; Marinelli, S.; Pieroni, L.; Urbani, A.; Luvisetto, S.; Pavone, F. 17beta-estradiol counteracts neuropathic pain: A behavioural, immunohistochemical and proteomic investigation on sex-related differences in mice. Sci. Rep. 2016, 6, srep18980. [Google Scholar] [CrossRef]
- Diener, H.-C.; Holle, D.; Solbach, K.; Gaul, C. Medication-overuse headache: Risk factors, pathophysiology and management. Nat. Rev. Neurol. 2016, 12, 575–583. [Google Scholar] [CrossRef] [PubMed]
- Pellesi, L.; Bellei, E.; Guerzoni, S.; Cainazzo, M.M.; Baraldi, C.; Monari, E.; Pini, L.A. Exploration of candidate serum biomarkers potentially related to the chronic pain condition in Medication–overuse headache. BMC Neurol. 2019, 19, 1–9. [Google Scholar] [CrossRef]
- Pellesi, L.; Guerzoni, S.; Baraldi, C.; Cainazzo, M.M.; Pini, L.A.; Bellei, E. Identification of candidate proteomic markers in the serum of medication overuse headache patients: An exploratory study. Cephalalgia 2020, 40, 1070–1078. [Google Scholar] [CrossRef] [PubMed]
- Bellei, E.; Monari, E.; Bergamini, S.; Cuoghi, A.; Tomasi, A.; Guerzoni, S.; Ciccarese, M.; Pini, L.A. Validation of potential candidate biomarkers of drug-induced nephrotoxicity and allodynia in medication-overuse headache. J. Headache Pain 2015, 16, 1–9. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kalantari, S.; Jafari, A.; Moradpoor, R.; Ghasemi, E.; Khalkhal, E. Human Urine Proteomics: Analytical Techniques and Clinical Applications in Renal Diseases. Int. J. Proteom. 2015, 2015, 1–17. [Google Scholar] [CrossRef]
- Good, D.M.; Thongboonkerd, V.; Novak, J.; Bascands, J.-L.; Schanstra, J.P.; Coon, J.J.; Dominiczak, A.; Mischak, H. Body Fluid Proteomics for Biomarker Discovery: Lessons from the Past Hold the Key to Success in the Future. J. Proteome Res. 2007, 6, 4549–4555. [Google Scholar] [CrossRef]
- Bellei, E.; Monari, E.; Bergamini, S.; Pini, L.A.; Tomasi, A.; Ozben, T. Urinary proteomics in biomarker discovery of kidney-related disorders: Diabetic nephropathy and drug-induced nephrotoxicity in chronic headache. Electron. J. Int. Fed. Clin. Chem. Lab. Med. 2018, 29, 290–297. [Google Scholar]
- Fischer, M.A.; Jan, A. Medication-Overuse Headache. Available online: https://www.ncbi.nlm.nih.gov/books/NBK538150/ (accessed on 30 June 2020).
- Hagen, K.B.; Vatten, L.J.; Stovner, L.J.; Zwart, J.-A.; Krokstad, S.; Bovim, G. Low Socio-Economic Status is Associated with Increased Risk of Frequent Headache: A Prospective Study of 22718 Adults in Norway. Cephalalgia 2002, 22, 672–679. [Google Scholar] [CrossRef]
- PernillaJonsson, P.; Linde, M.; Hensing, G.; Hedenrud, T. Sociodemographic differences in medication use, health-care contacts and sickness absence among individuals with medication-overuse headache. J. Headache Pain 2012, 13, 281–290. [Google Scholar] [CrossRef][Green Version]
- Atasoy, H.T.; Unal, A.E.; Atasoy, N.; Emre, U.; Sumer, M. Low Income and Education Levels May Cause Medication Overuse and Chronicity in Migraine Patients. Headache J. Head Face Pain 2005, 45, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Wiendels, N.; Neven, A.K.; Rosendaal, F.; Spinhoven, P.; Zitman, F.; Assendelft, W.; Ferrari, M.D. Chronic Frequent Headache in the General Population: Prevalence and Associated Factors. Cephalalgia 2006, 26, 1434–1442. [Google Scholar] [CrossRef] [PubMed]
- Mose, L.S.; Pedersen, S.S.; Debrabant, B.; Jensen, R.H.; Gram, B. The role of personality, disability and physical activity in the development of medication-overuse headache: A prospective observational study. J. Headache Pain 2018, 19, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Bendtsen, L.; Munksgaard, S.B.; Tassorelli, C.; Nappi, G.; Katsarava, Z.; Lainez, M.; Leston, J.; Fadic, R.; Spadafora, S.; Stoppini, A.; et al. Disability, anxiety and depression associated with medication-overuse headache can be considerably reduced by detoxification and prophylactic treatment. Results from a multicentre, multinational study (COMOESTAS project). Cephalalgia 2014, 34, 426–433. [Google Scholar] [CrossRef] [PubMed]
- Kristoffersen, E.S.; Straand, J.; Russell, M.B.; Lundqvist, C. Disability, anxiety and depression in patients with medication-overuse headache in primary care—The BIMOH study. Eur. J. Neurol. 2016, 23, 28–35. [Google Scholar] [CrossRef]
- Radat, F.; Créac’H, C.; Swendsen, J.; Lafittau, M.; Irachabal, S.; Dousset, V.; Henry, P. Psychiatric Comorbidity in the Evolution From Migraine to Medication Overuse Headache. Cephalalgia 2005, 25, 519–522. [Google Scholar] [CrossRef]
- Zeeberg, P.; Olesen, J.; Jensen, R. Probable medication-overuse headache: The effect of a 2-month drug-free period. Neurology 2006, 66, 1894–1898. [Google Scholar] [CrossRef] [PubMed]
- Cevoli, S.; Sancisi, E.; Grimaldi, D.; Pierangeli, G.; Zanigni, S.; Nicodemo, M.; Cortelli, P.; Montagna, P. Family History for Chronic Headache and Drug Overuse as a Risk Factor for Headache Chronification. Headache J. Head Face Pain 2009, 49, 412–418. [Google Scholar] [CrossRef] [PubMed]
- De Felice, M.; Ossipov, M.H.; Wang, R.; Lai, J.; Chichorro, J.; Meng, I.; Dodick, D.W.; Vanderah, T.W.; Dussor, G.; Porreca, F. Triptan-induced latent sensitization: A possible basis for medication overuse headache. Ann. Neurol. 2009, 67, 325–337. [Google Scholar] [CrossRef] [PubMed]
- Kondratyev, A.V.; Shulmin, A.V.; Shnayder, N.A.; Lomakin, A.I. Headache as a sociomedical problem: A review of literature. Neurol. Neuropsychiatry Psychosom. 2017, 9, 83–88. [Google Scholar] [CrossRef]
- Wang, Y.-F.; Yu, C.-C.; Kuan, A.S.; Chen, S.-P.; Wang, S.-J. Association between suicidal risks and medication-overuse headache in chronic migraine: A cross-sectional study. J. Headache Pain 2021, 22, 1–8. [Google Scholar] [CrossRef]
- Radat, F.; Créac’H, C.; Guegan-Massardier, E.; Mick, G.; Guy, N.; Fabre, N.; Giraud, P.; Nachit-Ouinekh, F.; Lanteri-Minet, M. Behavioral Dependence in Patients With Medication Overuse Headache: A Cross-Sectional Study in Consulting Patients Using the DSM-IV Criteria. Headache J. Head Face Pain 2008, 48, 1026–1036. [Google Scholar] [CrossRef]
- Radat, F.; Lanteri-Minet, M. What is the Role of Dependence-Related Behavior in Medication-Overuse Headache? Headache J. Head Face Pain 2010, 50, 1597–1611. [Google Scholar] [CrossRef]
- Kristoffersen, E.S.; Grande, R.B.; Aaseth, K.; Russell, M.B.; Lundqvist, C. Medication-overuse headache detoxification reduces headache disability—The Akershus study of chronic headache. Eur. J. Neurol. 2018, 25, 1140–1147. [Google Scholar] [CrossRef]
- Ramusino, M.C.; De Cillis, I.; Costa, A.; Antonaci, F. Impact of Medical Care on Symptomatic Drug Consumption and Quality of Life in Headache: A One-Year Population Study. Front. Neurol. 2019, 10, 629. [Google Scholar] [CrossRef] [PubMed]
- Fischbach, W. Medikamenteninduzierte gastrointestinale Blutung. Der Internist 2019, 60, 597–607. [Google Scholar] [CrossRef]
- He, Z.; Dong, L.; Zhang, Y.; Kong, Q.; Tan, G.; Zhou, J. Metabolic syndrome in female migraine patients is associated with medication overuse headache: A clinic-based study in China. Eur. J. Neurol. 2015, 22, 1228–1234. [Google Scholar] [CrossRef] [PubMed]
- Bellei, E.; Rustichelli, C.; Bergamini, S.; Monari, E.; Baraldi, C.; Castro, F.L.; Tomasi, A.; Ferrari, A. Proteomic serum profile in menstrual-related and post menopause migraine. J. Pharm. Biomed. Anal. 2020, 184, 113165. [Google Scholar] [CrossRef] [PubMed]
- Ferroni, P.; Zanzotto, F.M.; Scarpato, N.; Spila, A.; Fofi, L.; Egeo, G.; Rullo, A.; Palmirotta, R.; Barbanti, P.; Guadagni, F. Machine learning approach to predict medication overuse in migraine patients. Comput. Struct. Biotechnol. J. 2020, 18, 1487–1496. [Google Scholar] [CrossRef]
- Guo, S.; Shalchian, S.; Gérard, P.; Küper, M.; Katsarava, Z.; Ashina, M.; Schoenen, J. Prevalence of right-to-left shunts on transcranial Doppler in chronic migraine and medication-overuse headache. Cephalalgia 2014, 34, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Jang, E.; Kim, J.-H.; Kim, J.-H.; Lee, W.-H.; Suk, K. Lipocalin-type Prostaglandin D2 Synthase Protein Regulates Glial Cell Migration and Morphology through Myristoylated Alanine-rich C-Kinase Substrate. J. Biol. Chem. 2012, 287, 9414–9428. [Google Scholar] [CrossRef] [PubMed]
- Minami, T.; Okuda-Ashitaka, E.; Nishizawa, M.; Mori, H.; Ito, S. Inhibition of nociceptin-induced allodynia in conscious mice by prostaglandin D2. Br. J. Pharmacol. 1997, 122, 605–610. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, T.; Urade, Y.; Kimura, H.; Eguchi, N.; Nishikawa, A.; Hayaishi, O. Lipocalin-type Prostaglandin D Synthase (β-Trace) Is a Newly Recognized Type of Retinoid Transporter. J. Biol. Chem. 1997, 272, 15789–15795. [Google Scholar] [CrossRef]
- Beuckmann, C.T.; Aoyagi, M.; Okazaki, I.; Hiroike, T.; Toh, H.; Hayaishi, O.; Urade, Y. Binding of Biliverdin, Bilirubin, and Thyroid Hormones to Lipocalin-Type Prostaglandin D Synthase†. Biochemistry 1999, 38, 8006–8013. [Google Scholar] [CrossRef]
- Mohri, I.; Taniike, M.; Okazaki, I.; Kagitani-Shimono, K.; Aritake, K.; Kanekiyo, T.; Yagi, T.; Takikita, S.; Kim, H.-S.; Urade, Y.; et al. Lipocalin-type prostaglandin D synthase is up-regulated in oligodendrocytes in lysosomal storage diseases and binds gangliosides. J. Neurochem. 2006, 97, 641–651. [Google Scholar] [CrossRef]
- Kanekiyo, T.; Ban, T.; Aritake, K.; Huang, Z.-L.; Qu, W.-M.; Okazaki, I.; Mohri, I.; Murayama, S.; Ozono, K.; Taniike, M.; et al. Lipocalin-type prostaglandin D synthase/beta-trace is a major amyloid beta-chaperone in human cerebrospinal fluid. Proc. Natl. Acad. Sci. USA 2007, 104, 6412–6417. [Google Scholar] [CrossRef]
- Bouillon, R.; Schuit, F.; Antonio, L.; Rastinejad, F. Vitamin D Binding Protein: A Historic Overview. Front. Endocrinol. 2020, 10, 910. [Google Scholar] [CrossRef] [PubMed]
- Gregory, K.J.; Zhao, B.; Bielenberg, D.R.; Dridi, S.; Wu, J.; Jiang, W.; Huang, B.; Pirie-Shepherd, S.; Fannon, M. Vitamin D Binding Protein-Macrophage Activating Factor Directly Inhibits Proliferation, Migration, and uPAR Expression of Prostate Cancer Cells. PLoS ONE 2010, 5, e13428. [Google Scholar] [CrossRef]
- The Functions of Vitamin D—Binding Protein (VDBP). Available online: https://www.researchgate.net/figure/The-functions-of-vitamin-D-binding-protein-VDBP_tbl2_43534863 (accessed on 7 June 2021).
- Nowaczewska, M.; Wiciński, M.; Osiński, S.; Kaźmierczak, H. The Role of Vitamin D in Primary Headache–from Potential Mechanism to Treatment. Nutrients 2020, 12, 243. [Google Scholar] [CrossRef]
- Ghorbani, Z.; Togha, M.; Rafiee, P.; Ahmadi, Z.S.; Magham, R.R.; Haghighi, S.; Jahromi, S.R.; Mahmoudi, M. Vitamin D in migraine headache: A comprehensive review on literature. Neurol. Sci. 2019, 40, 2459–2477. [Google Scholar] [CrossRef] [PubMed]
- Levy, D.; Burstein, R.; Kainz, V.; Jakubowski, M.; Strassman, A.M. Mast cell degranulation activates a pain pathway underlying migraine headache. Pain 2007, 130, 166–176. [Google Scholar] [CrossRef]
- Burstein, R.; Noseda, R.; Borsook, D. Migraine: Multiple Processes, Complex Pathophysiology. J. Neurosci. 2015, 35, 6619–6629. [Google Scholar] [CrossRef]
- Moskaleva, P.; Shnayder, N.; Petrova, M.; Kaskaeva, D.; Gavrilyuk, O.; Radostev, S.; Garganeeva, N.; Sharavii, V.; Vaiman, E.; Nasyrova, R. The Role of Single Nucleotide Variants of NOS1, NOS2, and NOS3 Genes in the Development of the Phenotype of Migraine and Arterial Hypertension. Brain Sci. 2021, 11, 753. [Google Scholar] [CrossRef] [PubMed]
- Shnayder, N.; Petrova, M.; Moskaleva, P.; Shesternya, P.; Pozhilenkova, E.; Nasyrova, R. The Role of Single-Nucleotide Variants of NOS1, NOS2, and NOS3 Genes in the Comorbidity of Arterial Hypertension and Tension-Type Headache. Molecules 2021, 26, 1556. [Google Scholar] [CrossRef] [PubMed]
- Zhao, N.; Liu, C.-C.; Qiao, W.; Bu, G. Apolipoprotein E, Receptors, and Modulation of Alzheimer’s Disease. Biol. Psychiatry 2018, 83, 347–357. [Google Scholar] [CrossRef]
- Liu, S.; Liu, J.; Weng, R.; Gu, X.; Zhong, Z. Apolipoprotein E gene polymorphism and the risk of cardiovascular disease and type 2 diabetes. BMC Cardiovasc. Disord. 2019, 19, 1–6. [Google Scholar] [CrossRef]
- Gupta, R.; Kumar, V.; Luthra, K.; Banerjee, B.; Bhatia, M.S. Polymorphism in apolipoprotein E among migraineurs and tension-type headache subjects. J. Headache Pain 2009, 10, 115–120. [Google Scholar] [CrossRef] [PubMed]
- The Immune System and Headache. Available online: https://www.practicalpainmanagement.com/pain/headache/immune-system-headache (accessed on 7 June 2021).
- Hunt, J.M.; Tuder, R. Alpha 1 Anti-Trypsin: One Protein, Many Functions. Curr. Mol. Med. 2012, 12, 827–835. [Google Scholar] [CrossRef] [PubMed]
- Gallai, V.; Sarchielli, P. Nitric oxide in primary headaches. J. Headache Pain 2000, 1, 145–154. [Google Scholar] [CrossRef]
- Tolosano, E.; Altruda, F. Hemopexin: Structure, Function, and Regulation. DNA Cell Biol. 2002, 21, 297–306. [Google Scholar] [CrossRef]
- Galicia, N.; Díez, P.; Dégano, R.M.; Guest, P.C.; Ibarrola, N.; Fuentes, M. Proteomic Biomarker Identification in Cerebrospinal Fluid for Leptomeningeal Metastases with Neurological Complications. Adv. Exp. Med. Biol. 2017, 974, 85–96. [Google Scholar] [CrossRef]
- Castaño, E.M.; Roher, A.E.; Esh, C.L.; Kokjohn, T.A.; Beach, T. Comparative proteomics of cerebrospinal fluid in neuropathologically-confirmed Alzheimer’s disease and non-demented elderly subjects. Neurol. Res. 2006, 28, 155–163. [Google Scholar] [CrossRef]
- Retinol Binding Protein—An Overview. ScienceDirect Topics. Available online: https://www.sciencedirect.com/topics/neuroscience/retinol-binding-protein (accessed on 7 June 2021).
- Devuyst, O.; Olinger, E.; Rampoldi, L. Uromodulin: From physiology to rare and complex kidney disorders. Nat. Rev. Nephrol. 2017, 13, 525–544. [Google Scholar] [CrossRef]
- Ekström, B.; Peterson, P.; Berggárd, I. A urinary and plasma α1-glycoprotein of low molecular weight: Isolation and some properties. Biochem. Biophys. Res. Commun. 1975, 65, 1427–1433. [Google Scholar] [CrossRef]
- Åkerström, B.; Lögdberg, L. A1-Microglobulin. Available online: https://www.ncbi.nlm.nih.gov/books/NBK6003/ (accessed on 16 June 2021).
- Penders, J.; Delanghe, J.R. Alpha 1-microglobulin: Clinical laboratory aspects and applications. Clin. Chim. Acta 2004, 346, 107–118. [Google Scholar] [CrossRef] [PubMed]
- Hassan, I.; Waheed, A.; Yadav, S.; Singh, T.P.; Ahmad, F. Zinc α2-Glycoprotein: A Multidisciplinary Protein. Mol. Cancer Res. 2008, 6, 892–906. [Google Scholar] [CrossRef]
- Elsheikh, M.; Elhefnawy, K.A.; Emad, G.; Ismail, M.; Borai, M. Zinc alpha 2 glycoprotein as an early biomarker of diabetic nephropathy in patients with type 2 diabetes mellitus. Braz. J. Nephrol. 2019, 41, 509–517. [Google Scholar] [CrossRef]
- Tada, T.; Ohkubo, I.; Niwa, M.; Sasaki, M.; Tateyama, H.; Eimoto, T. Immunohistochemical localization of Zn-alpha 2-glycoprotein in normal human tissues. J. Histochem. Cytochem. 1991, 39, 1221–1226. [Google Scholar] [CrossRef]
- Pihl, R.; Jensen, R.K.; Poulsen, E.C.; Jensen, L.; Hansen, A.G.; Thøgersen, I.B.; Dobó, J.; Gál, P.; Andersen, G.R.; Enghild, J.J.; et al. ITIH4 acts as a protease inhibitor by a novel inhibitory mechanism. Sci. Adv. 2021, 7, eaba7381. [Google Scholar] [CrossRef]
- Mcheyzerwilliams, M.G.; Okitsu, S.L.; Wang, N.; Mcheyzerwilliams, L.J. Molecular programming of B cell memory. Nat. Rev. Immunol. 2011, 12, 24–34. [Google Scholar] [CrossRef] [PubMed]
- Fernando, S.; Polkinghorne, K.R. Cystatin C: Not just a marker of kidney function. Braz. J. Nephrol. 2020, 42, 6–7. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, T.W.; Komenda, P.; Tangri, N. Cystatin C as a biomarker for estimating glomerular filtration rate. Curr. Opin. Nephrol. Hypertens. 2015, 24, 295–300. [Google Scholar] [CrossRef]
- Kondratiev, A.V.; Shnayder, N.A.; Shulmin, A.; Dmitrenko, D.V.; Trefilova, V.V.; Zobova, S.N.; Kantimirova, E.A.; Petrova, M.M.; Kaskaeva, D.S.; Vaiman, E.E.; et al. Genetic aspects of primary headaches in Siberia (Russia). Pers. Psychiatry Neurol. 2021, 1, 54–63. [Google Scholar] [CrossRef]
- Linde, M.; Gustavsson, A.; Stovner, L.J.; Steiner, T.J.; Barré, J.; Katsarava, Z.; Lainez, J.M.; Lampl, C.; Lanteri-Minet, M.; Rastenyte, D.; et al. The cost of headache disorders in Europe: The Eurolight project. Eur. J. Neurol. 2011, 19, 703–711. [Google Scholar] [CrossRef] [PubMed]
- Raggi, A.; Leonardi, M.; Sansone, E.; Curone, M.; Grazzi, L.; D’Amico, D. The cost and the value of treatment of medication overuse headache in Italy: A longitudinal study based on patient-derived data. Eur. J. Neurol. 2020, 27, 62-e1. [Google Scholar] [CrossRef] [PubMed]
- Togha, M.; Nadjafi-Semnani, F.; Martami, F.; Mohammadshirazi, Z.; Vahidpour, N.; Akbari-Sari, A.; Daroudi, R. Economic burden of medication-overuse headache in Iran: Direct and indirect costs. Neurol. Sci. 2021, 42, 1869–1877. [Google Scholar] [CrossRef]
- Shah, A.M.; Bendtsen, L.; Zeeberg, P.; Jensen, R.H. Reduction of Medication Costs after Detoxification for Medication-Overuse Headache. Headache J. Head Face Pain 2012, 53, 665–672. [Google Scholar] [CrossRef] [PubMed]
- Schwedt, T.J.; Buse, D.C.; Argoff, C.E.; Reed, M.L.; Fanning, K.M.; Hussar, C.R.; Adams, A.M.; Lipton, R.B. Medication Overuse and Headache Burden: Results From the CaMEO Study. Neurol. Clin. Pract. 2021, 11, 216–226. [Google Scholar] [CrossRef]
- Kanki, R.; Nagaseki, Y.; Sakai, F. Medication-Overuse Headache in Japan. Cephalalgia 2008, 28, 1227–1228. [Google Scholar] [CrossRef]
- Neznanov, N.G. A paradigm shift to treat psychoneurological disorders. Pers. Psychiatry Neurol. 2021, 1, 1–2. [Google Scholar]


{kind=link}
| Protein Full Name | Entry Name | Gene Name | Locus | Protein Main Function | Theor. Mass. | References |
|---|---|---|---|---|---|---|
| Lipocalin-type prostaglandin D2 synthase | L-PGDS | PTGDS | 9q34.3 | Prostaglandin biosynthesis process | 21,029 | [23,30] |
| Apolipoprotein B100 | APOB | APOB | 2p24.1 | Cholesterol metabolism | 516,651 | [23,30] |
| Alpha-2-macroglobulin | A2MG | A2M | 12p13.31 | Enzyme binding | 164,613 | [23,30] |
| Complement factor H | CFAH | CFH | 1q31.3 | Complement activation | 143,480 | [23,30] |
| Complement C3 (fragm) | CO3 | C3 | 19p13.3 | Complement activation | 188,569 | [23,30] |
| Hemopexin | HEMO | HPX | 11p15.4 | Metal ion binding | 52,385 | [23,30] |
| Serum albumin | ALBU | ALB | 4q13.3 | Metal binding | 71,317 | [23,30] |
| Alpha-1B-glycoprotein | AIBG | A1BG | 19q13.43 | Neutrophil, platelet degranulation | 54,790 | [23,30] |
| Complement component C9 | CO9 | C9 | 5p13.1 | Complement activation | 64,615 | [23,30] |
| Kininogen-1 | KNG1 | KNG1 | 3q27.3 | Cysteine-type endopeptidase inhibitor activity | 72,996 | [23,30] |
| Vitronectin | VTNC | VTN | 17q11.2 | Heparin binding | 55,069 | [23,30] |
| Haptoglobin | HPT | HP | 16q22.2 | Acute phase response | 45,861 | [23,30] |
| Apolipoprotein A-4 | APOA4 | APOA4 | 11q23.3 | Lipid binding | 45,371 | [23,30] |
| Alpha-1-acid glycoprotein 1 | A1AG1 | ORM1 | 9q32 | Inflammatory response | 23,725 | [23,30] |
| Serum paraoxonase/arylesterase 1 | PON1 | PON1 | 7q21.3 | Hydrolase | 39,877 | [23,30] |
| Zinc-alpha-2-glycoprotein | ZA2G | AZGP1 | 7q22.1 | Protein transmembrane transporter activity | 34,465 | [23,30] |
| Alpha-1-acid glycoprotein 2 | A1AG2 | ORM2 | 9q32 | Acute phase response | 23,873 | [23,30] |
| Alpha-1-antitrypsin | A1AT | SERPINA1 | 14q32.13 | Protease inhibitor | 46,737 | [23,30] |
| Immunoglobulin heavy constant alpha 1 | IGHA1 | IGHA1 | 14q32.33 | Antigen binding | 37,655 | [23,30] |
| Retinol-binding protein | RETBP | RBP4 | 10q23.33 | Retinol binding | 23,010 | [23,30] |
| Transthyretin | TTHY | TTR | 18q12.1 | Hormone binding | 15,887 | [23,30] |
| Apolipoprotein E | APOE | APOE | 19q13.32 | Lipid transport | 36,154 | [23,30] |
| Vitamin D-binding protein | VDBP | GC | 4q13.3 | Vitamin D transport | 52,918 | [23,30] |
| Protein Full Name | Entry Name | Gene Name | Locus | Protein Main Function | Theor. Mass. | References |
|---|---|---|---|---|---|---|
| Lipocalin-type prostaglandin D2 synthase | L-PGDS | PTGDS | 9q34.3 | Prostaglandin biosynthesis process | 21,029 | [23,30] |
| Uromodulin (or Tamm-Horsfall urinary glycoprotein) | UROM | UMOD | 16p12.3 | Cellular defense response | 69,761 | [21,23,30,33] |
| Alpha-1-microglobulin | AMBP | AMBP | 9q32 | Calcium channel inhibitor activity | 38,999 | [21,23,33] |
| Zinc-alpha-2-glycoprotein | ZAZG | AZGP1 | 7q22.1 | Protein binding | 34,259 | [21] |
| Inter-alpha-trypsin heavy chain H4 | ITIH4 | ITIH4 | 3p21.1 | Acute-phase response | 103,357 | [21,23,33] |
| Ig kappa chain C region | IGKC | IGKC | 2p11.2 | Complement activation | 11,765 | [21,23,33] |
| Non-secretory ribonuclease | RNAS2 | RNASE2 | 14q11.2 | Chemotaxis | 18,354 | [21] |
| Cystatin M | CYTM | CST6 | 11q13.1 | Cystein-type endopeptidase inhibitor activity | 16,511 | [21] |
| Cystatin C | CYTC | CST3 | 20p11.21 | Cystein-type endopeptidase inhibitor activity | 15,799 | [21,30,33] |
| Serum albumin | ALBU | ALB | 4q13.3 | Metal binding | 69,367 | [23,33] |
| Alpha-1-antitrypsin | A1AT | SERPINA1 | 14q32.13 | Protease inhibitor | 46,737 | [23,33] |
| Actin, cytoplasmic 1 | ACTB | ACTB | 7p22.1 | Cell junction assembly | 41,737 | [23,33] |
| Apolipoprotein H | APOH | APOH | 17q24.2 | Heparin binding | 38,298 | [23,33] |
| Serpin B3 | SPB3 | SERPINB3 | 18q21.33 | Cystein-type endopeptidase inhibitor activity | 44,565 | [23,33] |
| Annexin A1 | ANXA1 | ANXA1 | 9q21.13 | Calcium ion binding | 38,714 | [23,33] |
| Prostaglandin-H2-D-isomerase | PTGDS | PTGDS | 9q34.3 | Prostaglandin biosynthesis process | 21,029 | [23,30,33] |
| Perlecan (fragment) | PGBM | HSPG2 | 1p36.12 | Angiogenesis | 468,830 | [23,33] |
| Transthyretin | TTHY | TTR | 18q12.1 | Protein binding | 15,887 | [23,33] |
| Proactivator polypeptide | SAP | PSAP | 10q22.1 | Enzyme activator activity | 58,113 | [23,33] |
| Nuclear transport factor 2 | NTF2 | NUTF2 | 16q22.1 | Positive regulation of protein import into nucleus | 14,478 | [23,33] |
| Fatty acid-binding protein | FABP5 | FABP5 | 8q21.13 | Fatty acid binding | 15,164 | [23,33] |
| Beta-2-microglobulin | B2MG | B2M | 15q21.1 | Antigen processing and presentation of endogenous peptide antigen via MHC class I | 13,715 | [23,33] |
| Protein S100-A11 | S10AB | S100A11 | 1q21.3 | Calcium ion binding | 11,740 | [23,33] |
| Non-secretory ribonuclease | RNAS2 | RNASE2 | 14q11.2 | Chemotaxis | 18,354 | [23,33] |
| Protein S100-A8 | S10A8 | S100A8 | 1q21.3 | Calcium ion binding | 10,835 | [23,33] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shnayder, N.A.; Sharavii, V.B.; Petrova, M.M.; Moskaleva, P.V.; Pozhilenkova, E.A.; Kaskaeva, D.S.; Tutynina, O.V.; Popova, T.E.; Garganeeva, N.P.; Nasyrova, R.F. Candidate Genes and Proteomic Biomarkers of Serum and Urine in Medication-Overuse Headache. Int. J. Mol. Sci. 2021, 22, 9024. https://doi.org/10.3390/ijms22169024
Shnayder NA, Sharavii VB, Petrova MM, Moskaleva PV, Pozhilenkova EA, Kaskaeva DS, Tutynina OV, Popova TE, Garganeeva NP, Nasyrova RF. Candidate Genes and Proteomic Biomarkers of Serum and Urine in Medication-Overuse Headache. International Journal of Molecular Sciences. 2021; 22(16):9024. https://doi.org/10.3390/ijms22169024
Chicago/Turabian StyleShnayder, Natalia A., Victoria B. Sharavii, Marina M. Petrova, Polina V. Moskaleva, Elena A. Pozhilenkova, Darya S. Kaskaeva, Olga. V. Tutynina, Tatiana E. Popova, Natalia P. Garganeeva, and Regina F. Nasyrova. 2021. "Candidate Genes and Proteomic Biomarkers of Serum and Urine in Medication-Overuse Headache" International Journal of Molecular Sciences 22, no. 16: 9024. https://doi.org/10.3390/ijms22169024
APA StyleShnayder, N. A., Sharavii, V. B., Petrova, M. M., Moskaleva, P. V., Pozhilenkova, E. A., Kaskaeva, D. S., Tutynina, O. V., Popova, T. E., Garganeeva, N. P., & Nasyrova, R. F. (2021). Candidate Genes and Proteomic Biomarkers of Serum and Urine in Medication-Overuse Headache. International Journal of Molecular Sciences, 22(16), 9024. https://doi.org/10.3390/ijms22169024