
Objective and Measurable Biomarkers in Chronic Subjective Tinnitus



Abstract
1. Introduction
2. Aims
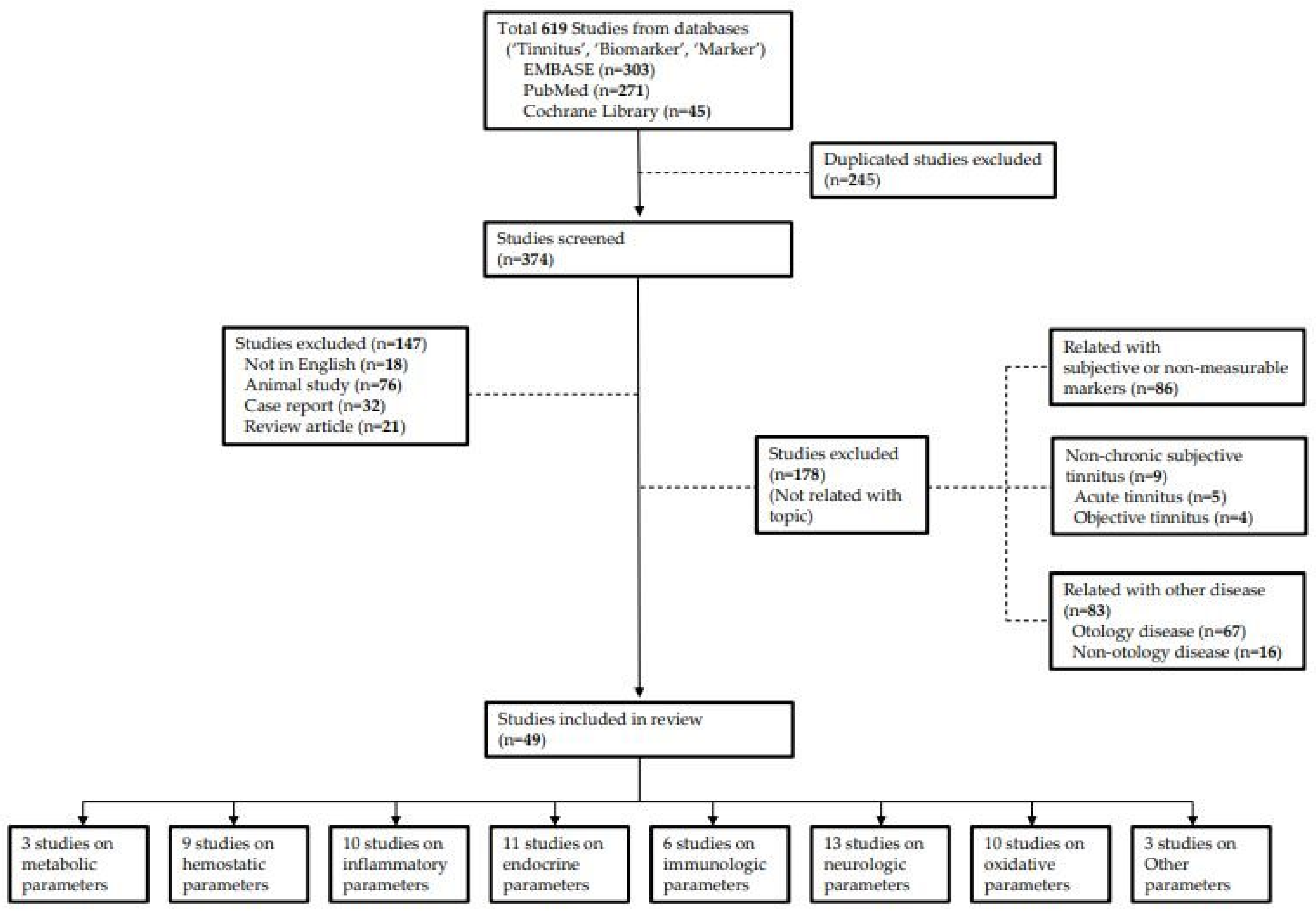
3. Review Methods
4. Biomarkers in Chronic Subjective Tinnitus
4.1. Metabolic Parameters
4.2. Hemostatic Parameters
4.3. Inflammatory Parameters
4.4. Endocrine Parameters
4.5. Immunologic Parameters
4.6. Neurologic Parameters
4.7. Oxidative Parameters
4.8. Other Markers
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Park, K.H.; Lee, S.H.; Koo, J.W.; Park, H.Y.; Lee, K.Y.; Choi, Y.S.; Oh, K.W.; Lee, A.; Yang, J.E.; Woo, S.Y. Prevalence and associated factors of tinnitus: Data from the Korean national health and nutrition examination survey 2009–2011. J. Epidemiol. 2014, 24, 417–426. [Google Scholar] [CrossRef] [PubMed]
- Cederroth, C.R.; Canlon, B.; Langguth, B. Hearing loss and tinnitus-are funders and industry listening? Nat. Biotechnol. 2013, 31, 972–974. [Google Scholar] [CrossRef] [PubMed]
- Vio, M.M.; Holme, R.H. Hearing loss and tinnitus: 250 million people and a US$10 billion potential market. Drug Discov. Today 2005, 10, 1263–1265. [Google Scholar] [CrossRef]
- Stockdale, D.; McFerran, D.; Brazier, P.; Pritchard, C.; Kay, T.; Dowrick, C.; Hoare, D.J. An economic evaluation of the healthcare cost of tinnitus management in the UK. BMC Health Serv. Res. 2017, 17, 577. [Google Scholar] [CrossRef]
- Mattox, D.E.; Hudgins, P. Algorithm for evaluation of pulsatile tinnitus. Acta Otolaryngol. 2008, 128, 427–431. [Google Scholar] [CrossRef]
- Sindhusake, D.; Golding, M.; Newall, P.; Rubin, G.; Jakobsen, K.; Mitchell, P. Risk factors for tinnitus in a population of older adults: The blue mountains hearing study. Ear Hear. 2003, 24, 501–507. [Google Scholar] [CrossRef]
- Tunkel, D.E.; Bauer, C.A.; Sun, G.H.; Rosenfeld, R.M.; Chandrasekhar, S.S.; Cunningham, E.R., Jr.; Archer, S.M.; Blakley, B.W.; Carter, J.M.; Granieri, E.C.; et al. Clinical practice guideline: Tinnitus. Otolaryngol. Head Neck Surg. 2014, 151, S1–S40. [Google Scholar] [CrossRef]
- Henry, J.A.; Roberts, L.E.; Caspary, D.M.; Theodoroff, S.M.; Salvi, R.J. Underlying mechanisms of tinnitus: Review and clinical implications. J. Am. Acad. Audiol. 2014, 25, 5–22, quiz 126. [Google Scholar] [CrossRef]
- Shargorodsky, J.; Curhan, G.C.; Farwell, W.R. Prevalence and characteristics of tinnitus among US adults. Am. J. Med. 2010, 123, 711–718. [Google Scholar] [CrossRef]
- Goto, F.; Saruta, J.; Kanzaki, S.; To, M.; Tsutsumi, T.; Tsukinoki, K.; Ogawa, K. Various levels of plasma brain-derived neurotrophic factor in patients with tinnitus. Neurosci. Lett. 2012, 510, 73–77. [Google Scholar] [CrossRef]
- Sahley, T.L.; Nodar, R.H. A biochemical model of peripheral tinnitus. Hear. Res. 2001, 152, 43–54. [Google Scholar] [CrossRef]
- Eggermont, J.J. Pathophysiology of tinnitus. Prog. Brain Res. 2007, 166, 19–35. [Google Scholar] [CrossRef]
- Kaltenbach, J.A.; Rachel, J.D.; Mathog, T.A.; Zhang, J.; Falzarano, P.R.; Lewandowski, M. Cisplatin-induced hyperactivity in the dorsal cochlear nucleus and its relation to outer hair cell loss: Relevance to tinnitus. J. Neurophysiol. 2002, 88, 699–714. [Google Scholar] [CrossRef]
- Kaltenbach, J.A.; Zhang, J.; Afman, C.E. Plasticity of spontaneous neural activity in the dorsal cochlear nucleus after intense sound exposure. Hear. Res. 2000, 147, 282–292. [Google Scholar] [CrossRef]
- Moller, A.R. The role of neural plasticity in tinnitus. Prog. Brain Res. 2007, 166, 37–45. [Google Scholar] [CrossRef]
- Jastreboff, P.J.; Hazell, J.W. A neurophysiological approach to tinnitus: Clinical implications. Br. J. Audiol. 1993, 27, 7–17. [Google Scholar] [CrossRef]
- Eggermont, J.J.; Roberts, L.E. Tinnitus: Animal models and findings in humans. Cell Tissue Res. 2015, 361, 311–336. [Google Scholar] [CrossRef]
- Husain, F.T.; Gander, P.E.; Jansen, J.N.; Shen, S. Expectations for tinnitus treatment and outcomes: A Survey study of audiologists and patients. J. Am. Acad. Audiol. 2018, 29, 313–336. [Google Scholar] [CrossRef]
- Zarenoe, R.; Ledin, T. Quality of life in patients with tinnitus and sensorineural hearing loss. B-ENT 2014, 10, 41–51. [Google Scholar]
- Puntmann, V.O. How-to guide on biomarkers: Biomarker definitions, validation and applications with examples from cardiovascular disease. Postgrad Med. J. 2009, 85, 538–545. [Google Scholar] [CrossRef]
- Miller, J.M.; Ren, T.Y.; Nuttall, A.L. Studies of inner ear blood flow in animals and human beings. Otolaryngol. Head Neck Surg. 1995, 112, 101–113. [Google Scholar] [CrossRef]
- Norena, A.J. An integrative model of tinnitus based on a central gain controlling neural sensitivity. Neurosci. Biobehav. Rev. 2011, 35, 1089–1109. [Google Scholar] [CrossRef]
- Cai, Q.; Du, X.; Zhou, B.; Cai, C.; Kermany, M.H.; Zhang, C.; Yoo, T. Effects of simvastatin on plasma lipoproteins and hearing loss in apolipoprotein E gene-deficient mice. ORL J. Otorhinolaryngol. Relat. Spec. 2009, 71, 244–250. [Google Scholar] [CrossRef]
- Hameed, M.K.; Sheikh, Z.A.; Ahmed, A.; Najam, A. Atorvastatin in the management of tinnitus with hyperlipidemias. J. Coll. Physicians Surg. Pak. 2014, 24, 927–930. [Google Scholar]
- Pulec, J.L.; Pulec, M.B.; Ignacio, M.H. Progressive sensorineural hearing loss, subjective tinnitus and vertigo caused by elevated blood lipids. Ear Nose Throat J. 1997, 76, 716–730, 725–716, 728 passim. [Google Scholar] [CrossRef]
- Canis, M.; Olzowy, B.; Welz, C.; Suckfull, M.; Stelter, K. Simvastatin and Ginkgo biloba in the treatment of subacute tinnitus: A retrospective study of 94 patients. Am. J. Otolaryngol. 2011, 32, 19–23. [Google Scholar] [CrossRef]
- Yuksel, F.; Karatas, D.; Turkdogan, F.T.; Yuksel, O. Increased atherosclerosis correlates with subjective tinnitus severity. Indian J. Otolaryngol. Head Neck Surg. 2018, 70, 119–124. [Google Scholar] [CrossRef]
- Ensari, N.; Gur, O.E.; Gur, N.; Selcuk, O.T.; Renda, L.; Yilmaz, M.D.; Ozturk, M.T.; Cekin, Y. Can apelin play a role in the etiology of tinnitus? Turk. J. Med. Sci. 2019, 49, 769–773. [Google Scholar] [CrossRef]
- Avci, D. Increased serum lipid levels in patients with subjective tinnitus. Iran. J. Otorhinolaryngol. 2021, 33, 31–36. [Google Scholar] [CrossRef]
- Verdoia, M.; Camaro, C.; Barbieri, L.; Schaffer, A.; Marino, P.; Bellomo, G.; Suryapranata, H.; De Luca, G. Mean platelet volume and the risk of periprocedural myocardial infarction in patients undergoing coronary angioplasty. Atherosclerosis 2013, 228, 136–141. [Google Scholar] [CrossRef]
- Greisenegger, S.; Endler, G.; Hsieh, K.; Tentschert, S.; Mannhalter, C.; Lalouschek, W. Is elevated mean platelet volume associated with a worse outcome in patients with acute ischemic cerebrovascular events? Stroke 2004, 35, 1688–1691. [Google Scholar] [CrossRef] [PubMed]
- Yuksel, O.; Helvaci, K.; Basar, O.; Koklu, S.; Caner, S.; Helvaci, N.; Abayli, E.; Altiparmak, E. An overlooked indicator of disease activity in ulcerative colitis: Mean platelet volume. Platelets 2009, 20, 277–281. [Google Scholar] [CrossRef] [PubMed]
- Kemal, O.; Muderris, T.; Basar, F.; Kutlar, G.; Gul, F. Prognostic value of mean platelet volume on tinnitus. J. Laryngol. Otol. 2016, 130, 162–165. [Google Scholar] [CrossRef]
- Yildiz, S.; Karaca, H.; Toros, S.Z. Mean platelet volume and neutrophil to lymphocyte ratio in patients with tinnitus: A case-control study. Braz. J. Otorhinolaryngol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Demir, M. Does inflammation play a role in the pathophysiology of tinnitus? Niger. J. Clin. Pract. 2021, 24, 199–204. [Google Scholar] [CrossRef]
- Yuksel, F.; Karatas, D. Can platelet indices be new biomarkers for subjective tinnitus? J. Craniofacial Surg. 2016, 27, e420–e424. [Google Scholar] [CrossRef] [PubMed]
- Ulusoy, B.; Bozdemir, K.; Akyol, M.; Mise, H.I.; Kutluhan, A.; Korkmaz, M.H. Investigation of neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio and mean platelet volume in patients with tinnitus. J. Laryngol. Otol. 2018, 132, 129–132. [Google Scholar] [CrossRef] [PubMed]
- Sarikaya, Y.; Bayraktar, C.; Karatas, M.; Dogan, S.; Olt, S.; Kaskalan, E.; Turkbeyler, I.H. Increased mean platelet volume in patients with idiopathic subjective tinnitus. Eur. Arch. Oto-Rhino-Laryngol. 2016, 273, 3533–3536. [Google Scholar] [CrossRef]
- Chrbolka, P.; Alusik, S.; Kalatova, D.; Paluch, Z. Increased platelet activity in tinnitus patients. Neuro Endocrinol. Lett. 2020, 41, 102–106. [Google Scholar]
- Bayram, A.; Yaşar, M.; Doğan, M.; Güneri, E.; Özcan, İ. Assessment of neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio and mean platelet volume in patients with tinnitus. ENT Updates 2015, 5, 103–106. [Google Scholar] [CrossRef]
- Arruda-Olson, A.M.; Reeder, G.S.; Bell, M.R.; Weston, S.A.; Roger, V.L. Neutrophilia predicts death and heart failure after myocardial infarction: A community-based study. Circ. Cardiovasc. Qual. Outcomes 2009, 2, 656–662. [Google Scholar] [CrossRef]
- Turkmen, K.; Ozcicek, F.; Ozcicek, A.; Akbas, E.M.; Erdur, F.M.; Tonbul, H.Z. The relationship between neutrophil-to-lymphocyte ratio and vascular calcification in end-stage renal disease patients. Hemodial. Int. 2014, 18, 47–53. [Google Scholar] [CrossRef]
- Bucak, A.; Ulu, S.; Oruc, S.; Yucedag, F.; Tekin, M.S.; Karakaya, F.; Aycicek, A. Neutrophil-to-lymphocyte ratio as a novel-potential marker for predicting prognosis of Bell palsy. Laryngoscope 2014, 124, 1678–1681. [Google Scholar] [CrossRef]
- Seo, Y.J.; Jeong, J.H.; Choi, J.Y.; Moon, I.S. Neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio: Novel markers for diagnosis and prognosis in patients with idiopathic sudden sensorineural hearing loss. Dis. Markers 2014, 2014, 702807. [Google Scholar] [CrossRef]
- Ozbay, I.; Kahraman, C.; Balikci, H.H.; Kucur, C.; Kahraman, N.K.; Ozkaya, D.P.; Oghan, F. Neutrophil-to-lymphocyte ratio in patients with severe tinnitus: Prospective, controlled clinical study. J. Laryngol. Otol. 2015, 129, 544–547. [Google Scholar] [CrossRef] [PubMed]
- Bayraktar, C.; Tasolar, S. Relationship between increased carotid artery stiffness and idiopathic subjective tinnitus. Eur. Arch. Oto-Rhino-Laryngol. 2017, 274, 2125–2130. [Google Scholar] [CrossRef]
- Ami, M.; Abdullah, A.; Awang, M.A.; Liyab, B.; Saim, L. Relation of distortion product otoacoustic emission with tinnitus. Laryngoscope 2008, 118, 712–717. [Google Scholar] [CrossRef]
- Gunes, A.; Karali, E.; Ural, A.; Ruzgar, F.; Bayatkara, T. The relationship of high-frequency distortion product otoacoustic emission (DPOAE) values with hematological parameters in tinnitus patients. Eur. Arch. Oto-Rhino-Laryngol. 2019, 276, 3013–3019. [Google Scholar] [CrossRef]
- Düzenli, U.; Bozan, N.; Aslan, M.; Özkan, H.; Turan, M.; Kıroğlu, A.F. A Retrospective analysis of haemotologic parameters in patients with bilateral tinnitus. East. J. Med. 2018, 23, 264–268. [Google Scholar] [CrossRef]
- Molini, E.; Faralli, M.; Calzolaro, L.; Ricci, G. Impact of identifying factors which trigger bothersome tinnitus on the treatment outcome in tinnitus retraining therapy. ORL 2014, 76, 81–88. [Google Scholar] [CrossRef]
- Marvar, P.J.; Harrison, D.G. Stress-dependent hypertension and the role of T lymphocytes. Exp. Physiol. 2012, 97, 1161–1167. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Jin, J.; Xi, S.; Zhu, Q.; Chen, Y.; Huang, M.; He, C. Clinical efficacy of cognitive behavioral therapy for chronic subjective tinnitus. Am. J. Otolaryngol. 2019, 40, 253–256. [Google Scholar] [CrossRef] [PubMed]
- Chrbolka, P.; Paluch, Z.; Hill, M.; Alusik, S. Circulating steroids negatively correlate with tinnitus. Steroids 2017, 123, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Hebert, S.; Lupien, S.J. The sound of stress: Blunted cortisol reactivity to psychosocial stress in tinnitus sufferers. Neurosci. Lett. 2007, 411, 138–142. [Google Scholar] [CrossRef] [PubMed]
- Yang, E.V.; Glaser, R. Stress-induced immunomodulation and the implications for health. Int. Immunopharmacol. 2002, 2, 315–324. [Google Scholar] [CrossRef]
- Savastano, M.; Aita, M.; Barlani, F. Psychological, neural, endocrine, and immune study of stress in tinnitus patients: Any correlation between psychometric and biochemical measures? Ann. Otol. Rhinol. Laryngol. 2007, 116, 100–106. [Google Scholar] [CrossRef]
- Simpson, J.J.; Davies, W.E. A review of evidence in support of a role for 5-HT in the perception of tinnitus. Hear. Res. 2000, 145, 1–7. [Google Scholar] [CrossRef]
- Kim, D.K.; Chung, D.Y.; Bae, S.C.; Park, K.H.; Yeo, S.W.; Park, S.N. Diagnostic value and clinical significance of stress hormones in patients with tinnitus. Eur. Arch. Oto-Rhino-Laryngol. 2014, 271, 2915–2921. [Google Scholar] [CrossRef]
- Kirschbaum, C.; Hellhammer, D.H. Salivary cortisol in psychoneuroendocrine research: Recent developments and applications. Psychoneuroendocrinology 1994, 19, 313–333. [Google Scholar] [CrossRef]
- Hebert, S.; Paiement, P.; Lupien, S.J. A physiological correlate for the intolerance to both internal and external sounds. Hear. Res. 2004, 190, 1–9. [Google Scholar] [CrossRef]
- de Kloet, E.R.; Schmidt, M.; Meijer, O.C. Corticosteroid receptors and HPA-axis regulation. In Techniques in the Behavioral and Neural Sciences; Elsevier: Amsterdam, The Netherlands, 2005; Volume 15, pp. 265–294. [Google Scholar]
- Simoens, V.L.; Hebert, S. Cortisol suppression and hearing thresholds in tinnitus after low-dose dexamethasone challenge. BMC Ear Nose Throat Disord. 2012, 12, 4. [Google Scholar] [CrossRef]
- Nater, U.M.; Maloney, E.; Boneva, R.S.; Gurbaxani, B.M.; Lin, J.M.; Jones, J.F.; Reeves, W.C.; Heim, C. Attenuated morning salivary cortisol concentrations in a population-based study of persons with chronic fatigue syndrome and well controls. J. Clin. Endocrinol. Metab. 2008, 93, 703–709. [Google Scholar] [CrossRef]
- Jackson, J.G. The cortisol awakening response: A feasibility study investigating the use of the area under the curve with respect to increase as an effective objective measure of tinnitus distress. Am. J. Audiol. 2019, 28, 583–596. [Google Scholar] [CrossRef]
- Alsalman, O.A.; Tucker, D.; Vanneste, S. Salivary stress-related responses in tinnitus: A preliminary study in young male subjects with tinnitus. Front. Neurosci. 2016, 10, 338. [Google Scholar] [CrossRef]
- Aydin, N.; Searchfield, G.D. Changes in tinnitus and physiological biomarkers of stress in response to short-term broadband noise and sounds of nature. Complement. Ther. Med. 2019, 46, 62–68. [Google Scholar] [CrossRef]
- Megwalu, U.C.; Finnell, J.E.; Piccirillo, J.F. The effects of melatonin on tinnitus and sleep. Otolaryngol. Head Neck Surg. 2006, 134, 210–213. [Google Scholar] [CrossRef]
- Lasisi, A.O.; Fehintola, F.A.; Lasisi, T.J. The role of plasma melatonin and vitamins C and B12 in the development of idiopathic tinnitus in the elderly. Ghana Med. J. 2012, 46, 152–157. [Google Scholar]
- Herbert, T.B.; Cohen, S. Stress and immunity in humans: A meta-analytic review. Psychosom. Med. 1993, 55, 364–379. [Google Scholar] [CrossRef]
- Maes, M.; Song, C.; Lin, A.; De Jongh, R.; Van Gastel, A.; Kenis, G.; Bosmans, E.; De Meester, I.; Benoy, I.; Neels, H.; et al. The effects of psychological stress on humans: Increased production of pro-inflammatory cytokines and a Th1-like response in stress-induced anxiety. Cytokine 1998, 10, 313–318. [Google Scholar] [CrossRef]
- Seidel, A.; Arolt, V.; Hunstiger, M.; Rink, L.; Behnisch, A.; Kirchner, H. Cytokine production and serum proteins in depression. Scand. J. Immunol. 1995, 41, 534–538. [Google Scholar] [CrossRef]
- Probert, L.; Selmaj, K. TNF and related molecules: Trends in neuroscience and clinical applications. J. Neuroimmunol. 1997, 72, 113–117. [Google Scholar] [CrossRef]
- Weber, C.; Arck, P.; Mazurek, B.; Klapp, B.F. Impact of a relaxation training on psychometric and immunologic parameters in tinnitus sufferers. J. Psychosom. Res. 2002, 52, 29–33. [Google Scholar] [CrossRef]
- Andrews, J.A.; Neises, K.D. Cells, biomarkers, and post-traumatic stress disorder: Evidence for peripheral involvement in a central disease. J. Neurochem. 2012, 120, 26–36. [Google Scholar] [CrossRef] [PubMed]
- Eyre, H.; Baune, B.T. Neuroplastic changes in depression: A role for the immune system. Psychoneuroendocrinology 2012, 37, 1397–1416. [Google Scholar] [CrossRef]
- Szczepek, A.J.; Haupt, H.; Klapp, B.F.; Olze, H.; Mazurek, B. Biological correlates of tinnitus-related distress: An exploratory study. Hear. Res. 2014, 318, 23–30. [Google Scholar] [CrossRef]
- Haider, H.F.; Ribeiro, S.F.; Martins, C.; Ribeiro, D.; Trigueiros, N.; Szczepek, A.J.; Caria, H.; Hoare, D.J.; Paco, J.; Borrego, L.M. Tinnitus, hearing loss and inflammatory processes in an older Portuguese population. Int. J. Audiol. 2020, 59, 323–332. [Google Scholar] [CrossRef]
- Breinekova, K.; Svoboda, M.; Smutna, M.; Vorlova, L. Markers of acute stress in pigs. Physiol. Res. 2007, 56, 323–329. [Google Scholar]
- Heller, M.F.; Bergman, M. VII Tinnitus aurium in normally hearing persons. Ann. Otol. Rhinol. Laryngol. 1953, 62, 73–83. [Google Scholar] [CrossRef]
- Binder, D.K.; Scharfman, H.E. Brain-derived neurotrophic factor. Growth Factors 2004, 22, 123–131. [Google Scholar] [CrossRef]
- Tan, J.; Ruttiger, L.; Panford-Walsh, R.; Singer, W.; Schulze, H.; Kilian, S.B.; Hadjab, S.; Zimmermann, U.; Kopschall, I.; Rohbock, K.; et al. Tinnitus behavior and hearing function correlate with the reciprocal expression patterns of BDNF and Arg3.1/arc in auditory neurons following acoustic trauma. Neuroscience 2007, 145, 715–726. [Google Scholar] [CrossRef]
- Sen, S.; Duman, R.; Sanacora, G. Serum brain-derived neurotrophic factor, depression, and antidepressant medications: Meta-analyses and implications. Biol. Psychiatry 2008, 64, 527–532. [Google Scholar] [CrossRef]
- Fernandes, B.S.; Gama, C.S.; Ceresér, K.M.; Yatham, L.N.; Fries, G.R.; Colpo, G.; de Lucena, D.; Kunz, M.; Gomes, F.A.; Kapczinski, F. Brain-derived neurotrophic factor as a state-marker of mood episodes in bipolar disorders: A systematic review and meta-regression analysis. J. Psychiatr. Res. 2011, 45, 995–1004. [Google Scholar] [CrossRef]
- Xiong, H.; Yang, H.; Liang, M.; Ou, Y.; Huang, X.; Cai, Y.; Lai, L.; Pang, J.; Zheng, Y. Plasma brain-derived neurotrophic factor levels are increased in patients with tinnitus and correlated with therapeutic effects. Neurosci. Lett. 2016, 622, 15–18. [Google Scholar] [CrossRef]
- Bermingham, N.; Hillermann, R.; Gilmour, F.; Martin, J.E.; Fisher, E.M. Human glial cell line-derived neurotrophic factor (GDNF) maps to chromosome 5. Hum. Genet. 1995, 96, 671–673. [Google Scholar] [CrossRef]
- Karege, F.; Perret, G.; Bondolfi, G.; Schwald, M.; Bertschy, G.; Aubry, J.M. Decreased serum brain-derived neurotrophic factor levels in major depressed patients. Psychiatry Res. 2002, 109, 143–148. [Google Scholar] [CrossRef]
- Guerini, F.; Beghi, E.; Riboldazzi, G.; Zangaglia, R.; Pianezzola, C.; Bono, G.; Casali, C.; Di Lorenzo, C.; Agliardi, C.; Nappi, G. BDNF Val66Met polymorphism is associated with cognitive impairment in Italian patients with Parkinson’s disease. Eur. J. Neurol. 2009, 16, 1240–1245. [Google Scholar] [CrossRef]
- Pivac, N.; Nikolac, M.; Nedic, G.; Mustapic, M.; Borovecki, F.; Hajnsek, S.; Presecki, P.; Pavlovic, M.; Mimica, N.; Muck Seler, D. Brain derived neurotrophic factor Val66Met polymorphism and psychotic symptoms in Alzheimer’s disease. Prog. Neuropsychopharmacol. Biol. Psychiatry 2011, 35, 356–362. [Google Scholar] [CrossRef]
- Kocabas, N.A.; Antonijevic, I.; Faghel, C.; Forray, C.; Kasper, S.; Lecrubier, Y.; Linotte, S.; Massat, I.; Mendlewicz, J.; Noro, M.; et al. Brain-derived neurotrophic factor gene polymorphisms: Influence on treatment response phenotypes of major depressive disorder. Int. Clin. Psychopharmacol. 2011, 26, 1–10. [Google Scholar] [CrossRef]
- Sand, P.G.; Langguth, B.; Schecklmann, M.; Kleinjung, T. GDNF and BDNF gene interplay in chronic tinnitus. Int. J. Mol. Epidemiol. Genet. 2012, 3, 245–251. [Google Scholar]
- Coskunoglu, A.; Orenay-Boyacioglu, S.; Deveci, A.; Bayam, M.; Onur, E.; Onan, A.; Cam, F.S. Evidence of associations between brain-derived neurotrophic factor (BDNF) serum levels and gene polymorphisms with tinnitus. Noise Health 2017, 19, 140–148. [Google Scholar] [CrossRef] [PubMed]
- Orenay-Boyacioglu, S.; Coskunoglu, A.; Caki, Z.; Cam, F.S. Relationship between chronic tinnitus and glial cell line-derived neurotrophic factor gene rs3812047, rs1110149, and rs884344 polymorphisms in a Turkish population. Biochem. Genet. 2016, 54, 552–563. [Google Scholar] [CrossRef] [PubMed]
- Stenz, L.; Zewdie, S.; Laforge-Escarra, T.; Prados, J.; La Harpe, R.; Dayer, A.; Paoloni-Giacobino, A.; Perroud, N.; Aubry, J.-M. BDNF promoter I methylation correlates between post-mortem human peripheral and brain tissues. Neurosci. Res. 2015, 91, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Orenay-Boyacioglu, S.; Caliskan, M.; Boyacioglu, O.; Coskunoglu, A.; Bozkurt, G.; Cam, F.S. Chronic tinnitus and BDNF/GDNF CpG promoter methylations: A case-control study. Mol. Biol. Rep. 2019, 46, 3929–3936. [Google Scholar] [CrossRef] [PubMed]
- Sachanska, T. Changes in blood serotonin in patients with tinnitus and other vestibular disturbances. Int. Tinnitus J. 1999, 5, 24–26. [Google Scholar] [PubMed]
- Tyler, R.S.; Coelho, C.; Noble, W. Tinnitus: Standard of care, personality differences, genetic factors. ORL J. Otorhinolaryngol. Relat. Spec. 2006, 68, 14–19; discussion 20-12. [Google Scholar] [CrossRef]
- Deniz, M.; Bayazit, Y.A.; Celenk, F.; Karabulut, H.; Yilmaz, A.; Gunduz, B.; Saridogan, C.; Dagli, M.; Erdal, E.; Menevse, A. Significance of serotonin transporter gene polymorphism in tinnitus. Otol. Neurotol. 2010, 31, 19–24. [Google Scholar] [CrossRef]
- Jeong, J.E.; Jeon, S.; Han, J.S.; Cho, E.Y.; Hong, K.S.; Park, S.N.; Kim, J.J. The mediating effect of psychological distress on the association between BDNF, 5-HTTLPR, and tinnitus severity. Psychiatry Investig. 2021, 18, 187–195. [Google Scholar] [CrossRef]
- Figueiredo, R.R.; Langguth, B.; Mello de Oliveira, P.; Aparecida de Azevedo, A. Tinnitus treatment with memantine. Otolaryngol. Head Neck Surg. 2008, 138, 492–496. [Google Scholar] [CrossRef]
- Friedman, R.A.; Van Laer, L.; Huentelman, M.J.; Sheth, S.S.; Van Eyken, E.; Corneveaux, J.J.; Tembe, W.D.; Halperin, R.F.; Thorburn, A.Q.; Thys, S.; et al. GRM7 variants confer susceptibility to age-related hearing impairment. Hum. Mol. Genet. 2009, 18, 785–796. [Google Scholar] [CrossRef]
- Haider, H.F.; Flook, M.; Aparicio, M.; Ribeiro, D.; Antunes, M.; Szczepek, A.J.; Hoare, D.J.; Fialho, G.; Paco, J.C.; Caria, H. Biomarkers of presbycusis and tinnitus in a Portuguese older population. Front. Aging Neurosci. 2017, 9, 346. [Google Scholar] [CrossRef]
- Cevette, M.J.; Vormann, J.; Franz, K. Magnesium and hearing. J. Am. Acad. Audiol. 2003, 14, 202–212. [Google Scholar] [CrossRef] [PubMed]
- Uluyol, S.; Kilicaslan, S.; Yagiz, O. Relationship between serum magnesium level and subjective tinnitus. Kulak Burun Bogaz Ihtis Derg. 2016, 26, 225–227. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Calabrese, V.; Cornelius, C.; Maiolino, L.; Luca, M.; Chiaramonte, R.; Toscano, M.A.; Serra, A. Oxidative stress, redox homeostasis and cellular stress response in Meniere’s disease: Role of vitagenes. Neurochem. Res. 2010, 35, 2208–2217. [Google Scholar] [CrossRef] [PubMed]
- Goswami, B.; Tayal, D.; Gupta, N.; Mallika, V. Paraoxonase: A multifaceted biomolecule. Clin. Chim. Acta 2009, 410, 1–12. [Google Scholar] [CrossRef]
- Ciorba, A.; Bianchini, C.; Pastore, A.; Mazzoli, M. Pathogenesis of tinnitus: Any role for oxidative stress? J. Int. Adv. Otol. 2013, 9, 249. [Google Scholar]
- Baker, K.; Staecker, H. Low dose oxidative stress induces mitochondrial damage in hair cells. Anat. Rec. (Hoboken) 2012, 295, 1868–1876. [Google Scholar] [CrossRef]
- Koc, S.; Akyuz, S.; Somuk, B.T.; Soyalic, H.; Yilmaz, B.; Taskin, A.; Bilinc, H.; Aksoy, N. Paraoxonase activity and oxidative status in patients with tinnitus. J. Audiol. Otol. 2016, 20, 17–21. [Google Scholar] [CrossRef]
- Ekinci, A.; Kamasak, K. Evaluation of serum prolidase enzyme activity and oxidative stress in patients with tinnitus. Braz. J. Otorhinolaryngol. 2020, 86, 405–410. [Google Scholar] [CrossRef]
- Erel, O.; Neselioglu, S. A novel and automated assay for thiol/disulphide homeostasis. Clin. Biochem. 2014, 47, 326–332. [Google Scholar] [CrossRef]
- Celik, M.; Koyuncu, I. A comprehensive study of oxidative stress in tinnitus patients. Indian J. Otolaryngol. Head Neck Surg. 2018, 70, 521–526. [Google Scholar] [CrossRef]
- Pawlak-Osinska, K.; Kazmierczak, H.; Marzec, M.; Kupczyk, D.; Bilski, R.; Mikolajewska, E.; Mikolajewski, D.; Augustynska, B. Assessment of the state of the natural antioxidant barrier of a body in patients complaining about the presence of tinnitus. Oxid Med. Cell Longev. 2018, 2018, 1439575. [Google Scholar] [CrossRef]
- Petridou, A.I.; Zagora, E.T.; Petridis, P.; Korres, G.S.; Gazouli, M.; Xenelis, I.; Kyrodimos, E.; Kontothanasi, G.; Kaliora, A.C. The effect of antioxidant supplementation in patients with tinnitus and normal hearing or hearing loss: A randomized, double-blind, placebo controlled trial. Nutrients 2019, 11, 3037. [Google Scholar] [CrossRef]
- Savastano, M.; Brescia, G.; Marioni, G. Antioxidant therapy in idiopathic tinnitus: Preliminary outcomes. Arch. Med. Res. 2007, 38, 456–459. [Google Scholar] [CrossRef]
- Berkiten, G.; Kumral, T.L.; Yildirim, G.; Salturk, Z.; Uyar, Y.; Atar, Y. Effects of serum zinc level on tinnitus. Am. J. Otolaryngol. 2015, 36, 230–234. [Google Scholar] [CrossRef]
- Salihoğlu, M.; Güngör, A.; Özcan, Ö.; Çeşmeci, E.; Müftüoğlu, T.; Osman, M.İ. Tissue and serum prolidase activity in patients with nasal polyposis. Gülhane Tip Derg. 2014, 56, 209. [Google Scholar] [CrossRef]
- Cakmak, A.; Zeyrek, D.; Atas, A.; Celik, H.; Aksoy, N.; Erel, O. Serum prolidase activity and oxidative status in patients with bronchial asthma. J. Clin. Lab. Anal. 2009, 23, 132–138. [Google Scholar] [CrossRef]
- Lee, D.Y.; Kim, Y.H. Urine Cotinine Should Be Involved in Initial Evaluation of Tinnitus in Adolescents. Clin. Exp. Otorhinolaryngol. 2018, 11, 242–249. [Google Scholar] [CrossRef]
- Seyed Resuli, A. Can the Determination of salivary cotinine level be a new method in diagnosis and follow-up of childhood tinnitus? Iran. Red Crescent Med. J. 2020, 22. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Biomarkers | |
|---|---|
| Endocrine parameters | • Increase Saliva basal cortisol/cortisone (with blunted response to stress), 5-HIAA • Decrease Serum cortisol, Plasma melatonin level • ACTH (related with CD16NK, CD19) |
| Hemostatic parameters | • Increase MPV (related with HFHL), PDW, PC, 11-dTxB2 |
| Immunologic parameters | • Increase IL-1α (related with tonal tinnitus), IL-1β, IL-2, TNF-α • Decrease IL-10, HSP-70, Saliva neopterin • CD16NK, CD19 (related with ACTH) |
| Inflammatory parameters | • Increase NLR (related with HFHL-TN), PLR, CRP, ESR |
| Metabolic parameters | • Increase TC, TG or TRG, LDL • Decrease HDL |
| Neurologic parameters | • Increase Plasma BDNF level, Blood serotonin level • Decrease Saliva α-amylase, Serum magnesium • BDNF/GDNF SNP polymorphism, Serotonin transporter gene (SLC6A4) promoter region (5-HTTLPR) polymorphism, GRM7 gene polymorphism (relative with severity) |
| Oxidative parameters | • Increase TOS, OSI, LOOH, Nitric oxide, GST, MDA, 4-HNE, Disulphide, Disulphide/native thiol ratio, Disulphide/total thiol ratio • Decrease TAS, PON, cGPx, SOD, Native thiol, Native thiol/total thiol ratio, Vit B12, Plasma apelin level, Serum zinc • N-acetyltransferase 2 (NAT2) gene polymorphism (relative with severity) |
| Others | • Increase Saliva/Urine cotinine, ALP, Erythrocyte • Decrease Serum prolidase |
| Author (Year) | Study Design | Subjectives | Ages (years)/Hearing State | Specimen/Tissue Type | Biomarkers | Potential Application | Results/Conclusions |
|---|---|---|---|---|---|---|---|
| Deniz Avci (2021) [29] | Retrospective, case-control study | 91 patients, 65 controls (age-,sex-matched) | 18–70 years/ Normal hearing | Blood | Metabolic parameters (TC, TRG, LDL, HDL) | Diagnosis | Mean TC, TRG, and LDL levels were higher in the tinnitus group. |
| Demir M (2021) [35] | Retrospective, case-control study | 159 patients, 57 controls (age-,sex-matched) | 21–67 years/ N/A | Blood | Hemostatic parameters (MPV) Inflammatory parameters (NLR, PLR) | Diagnosis | AFHL-TN group had higher NLR than that of CNT group; HFHL-TN group had higher PLR than that of AFHL-TN, NH-TN, and CNT groups; HFHL-TN had higher MPV than that of AFHL-TN, NH-TN, and CNT groups. |
| Jeong et al. (2021) [98] | Case-control study | 86 patients, 252 controls | 22–83 years/ Normal hearing (better than 30 dB in 250 to 6000 Hz) | Blood | Neurologic parameters (BDNF gene SNP rs6265 [Val66Met], Serotonin transporter gene-linked polymorphic region 5-HTTLPR) | Prognosis | Depressive symptom in tinnitus is associated with the 5-HTTLPR S/S genotype and the severity of tinnitus. |
| Ali Seyed Resuli (2020) [119] | Retrospective, case-control study | 415 children patients, 200 controls (age-matched) | 7–15 years/ Normal hearing | Blood/Saliva | Others (Saliva cotinine, ALP, Erythrocyte) | Diagnosis | Saliva cotinine level of children and their parents, serum erythrocyte and serum ALP level are associated with tinnitus. |
| Yildiz et al. (2020) [34] | Retrospective, case-control study | 287 patients, 275 controls | 18–59 years/ Normal hearing (Pure tone average lower than 20 dB) | Blood | Hemostatic parameters (MPV) Inflammatory parameters (NLR) | Diagnosis | The percentage of subjects with high MPV and mean NLR level was higher in the tinnitus group. NLR level of 2.17 and above is associated with 1.991 times higher risk of tinnitus. |
| Chrbolka et al. (2020) [39] | Prospective cohort study | 40 patients, 40 controls (age-,sex- matched) | Mean: 50.86 years/ Hearing loss (Pure tone average lower than 40 dB) | Blood | Hemostatic parameters (11-dTxB2) | Diagnosis | Tinnitus patients have higher levels of 11-dTxB2 and increased platelet activity. |
| Ekinci A et al. (2020) [109] | Case-control study | 25 patients, 25 controls | 18–65 years/ Normal hearing | Blood | Oxidative parameters(TAS, TOS, OSI) Others (Prolidase) | Diagnosis | TOS, OSI and prolidase activity level were higher in tinnitus patients. |
| James George Jackson (2019) [64] | Case-control study | 20 patients, 10 controls | Mean: 52.2 years/ N/A | Saliva | Endocrine parameters (Cortisol) | Prognosis | Changes in cortisol levels—the AUCi—were less robust in severe tinnitus and AUCi correlated negatively with tinnitus distress later the same day. |
| Aydin N et al. (2019) [66] | Prospective study | 21 patients | 22–69 years/ N/A | Saliva | Endocrine parameters (Cortisol, Cortisone) | Therapeutic response (Sound therapy) | No changes in salivary cortisol, cortisone following sound therapy. |
| Ensari N et al. (2019) [28] | Case-control study | 40 patients, 40 controls | More than 18 years/Normal hearing | Blood | Oxidative parameters (Plasma apelin) Metabolic parameters (HDL, TG) | Diagnosis/Prognosis | Mean plasma apelin level, HDL were lower, but TG level was higher in patients with tinnitus. Negative correlations between apelin and THI were found. |
| Gunes A et al. (2019) [48] | Prospective study | 52 patients | 35–50 years/ N/A | Blood | Hemostatic parameters (MPV) Inflammatory parameters (NLR) | Prognosis | Correlation was observed between high-frequency PTA, high-frequency DPOAE, and NLR. |
| Li J et al. (2019) [52] | Case-control study | 100 patients | 18–83 years/ N/A | Blood | Endocrine parameters (Serum cortisol) Immunologic parameters (IL-2) | Therapeutic response (CBT) | Serum cortisol level was decreased and IL-2 level was increased after CBT |
| Petridou A I et al. (2019) [113] | Case-control study | 70 patients | 25–75 years/ Normal hearing or up to moderate hearing loss | Blood | Oxidative parameters (TAC, SOD, oxLDL) | Therapeutic response (Antioxidant) | No changes in TAC, SOD, and oxLDL were found after antioxidant supplementation (Multivitamin, alpha-lipoic acid). |
| Haider H F et al. (2019) [77] | Case-control study | 92 patients, 22 controls | 55–75 years/ N/A | Blood | Immunologic parameters (IL-1α, IL-2, IL-10, TNF-α HSP70) | Diagnosis/Prognosis | IL-10 levels were lower in patients with tinnitus, but IL-1α was higher in tonal tinnitus. IL-2 was lower in patients with residual inhibition. Negative correlation between tinnitus duration and IL-10, and between HSP70 and tinnitus loudness. |
| Orenay-Boyacioglu S et al. (2019) [94] | Case-control study | 60 patients, 50 controls (Age-matched) | 18–55 years/ Normal hearing | Blood | Neurologic parameters (BDNF/GDNF CpG promoter methylation) | Diagnosis | BDNF CpG6 and GDNF CpG3-5-6 methylation ratios were different between controls and tinnitus group. |
| Yuksel F et al. (2018) [27] | Retrospective study | 215 patients | 18–75 years/ N/A | Blood | Metabolic parameters (TC, LDL, TG) | Prognosis | Increased IMT in tinnitus was associated with the severity of tinnitus (THI, VAS), high levels of TC, LDL, TG. |
| Lee et al. (2018) [118] | Cross-sectional study | 486 adolescents patients, 2296 controls | 12–18 years/ Normal hearing (lower than 40 dB at 500, 1000, 2000 and 3000 Hz) | Urine | Others (Cotinine) | Diagnosis | Urine cotinine level was the only parameter associated with tinnitus and the amount of smoking with tinnitus-related annoyance. Urine cotinine may be a biomarker for treatment response in adolescents with tinnitus |
| Pawlak-Osinska K et al. (2018) [112] | Case-control study | 51 patients, 19 controls | 20–62 years/ N/A | Blood | Oxidative parameters (Cp, GSH, Nitrate/nitrite, MDA, cGPx, GST, SOD-1) | Diagnosis | As antioxidants, cGPx, SOD were lower in tinnitus group, but GST activity was higher. GSH, MDA, and nitric oxide were higher in tinnitus group, but Cp showed no significant results. Antioxidants barrier system showed inefficiency in tinnitus group. |
| Celik M et al. (2018) [111] | Prospective case-control study | 35 patients, 35 controls (age-sex-BMI-matched) | 27–56 years/ Normal hearing | Blood | Oxidative parameters (LOOH, TAS, TOS, OSI, Thiol/Disulphide) | Diagnosis | In patient group, TOS and OSI levels were higher and TAS levels were lower. Disulphide and disulphide/native thiol and disulphide/total thiol ratio were higher in patient group, but native thiol levels and native thiol/total thiol ratio were lower. Also, LOOH ratio was higher |
| Düzenli U et al. (2018) [49] | Retrospective case-control study | 58 patients, 58 controls | Mean: 38.8 years/ Normal hearing | Blood | Hemostatic parameters (MPV, PC, PDW) Inflammatory parameters (NLR) | Diagnosis | PDW was higher, but NLR was lower in tinnitus group. Also, MPV values were similar between tinnitus group and controls. There were no correlation between hematologic and audiometric values. |
| Ulusoy B et al. (2018) [37] | Prospective case-control study | 64 patients, 64 controls (age-matched) | 18–65 years/ N/A | Blood | Hemostatic parameters (MPV, PDW) Inflammatory parameters (WBC, NLR, PLR) | Diagnosis | WBC, MPV, and PDW levels were higher in tinnitus, but no significant results were observed for NLR and PLR. Prothrombotic condition plays a role in the pathophysiology. |
| Chrbolka P et al. (2017) [53] | Cross-sectional study | 28 patients | Mean (male 52.5, female 55.2 years)/ Normal hearing (pure tone average lower than 40dB) | Blood | Endocrine parameters (Neuroactive, neuroprotective, immunomodulatory steroids) | Prognosis | Negative correlation between tinnitus indices and intensity of steroidogenesis. Also, circulating steroids negatively correlated with degree of tinnitus because of HPA abnormality. |
| Bayraktar C et al. (2017) [46] | Prospective case-control study | 40 patients, 40 controls (age-sex-matched) | Mean 41 years/ Normal hearing | Blood | Inflammatory parameters (NLR) | Prognosis | Positive correlation between the severity of tinnitus and CCA stiffness index, YEM measurements, left CIMT, and NLR. |
| Coskunoglu A et al. (2017) [91] | Case-control study | 65 patients, 42 controls (age-matched) | 18–55 years/ N/A | Blood | Neurologic parameters (Plasma BDNF, BDNF gene SNP rs6265 [Val66Met], rs2030324, rs1491850) | Diagnosis | Serum BNDF level was lower in tinnitus group, but no correlation BDNF gene polymorphism with tinnitus. |
| Haider H F et al. (2017) [101] | Cross-sectional study | 50 patients, 28 controls | 55–75 years/ Sensory presbycusis (bilateral SNHL in downslope audiometric pattern, above 1kHz with poor speech discrimination. | Blood | Neurologic parameters (GRM7 SNP rs11928865) Oxidative parameters (NAT2 SNP) | Diagnosis/Prognosis | Patients with T/T genotype at GRM7 had 33% lower risk for tinnitus and A/T genotype had a tendency for increased severity of tinnitus. Also, the odds of developing severe tinnitus were higher in the slow acetylator phenotype of NAT2. Therefore, Genotype A/T at GRM7 and slow acetylator NAT2 are prone to developing a more severe tinnitus. |
| Koc S et al. (2016) [108] | Prospective case-control study | 54 patients, 60 controls | 18–65 years/ Normal hearing | Blood | Oxidative parameters (PON, TOS, TAS, OSI) | Diagnosis | TAS, PON were lower, but TOS, OSI were higher in tinnitus. Tinnitus group was exposed to oxidative stress. |
| Sarikaya Y et al. (2016) [38] | Prospective case-control study | 101 patients, 54 controls (age-sex-matched) | Mean 40.87 years/ Normal hearing | Blood | Hemostatic parameters (MPV) | Diagnosis | MPV level was increased in tinnitus, but no significant association between MPV level and duration or characteristics of tinnitus. |
| Uluyol S et al. (2016) [103] | Case-control study | 76 patients (severe and catastrophic tinnitus), 86 controls | 43–65 years/ Normal hearing | Blood | Neurologic parameters (Serum magnesium) | Prognosis | Serum magnesium concentration was lower in severe tinnitus group. |
| Xiong H et al. (2016) [84] | Restrospective case-control study | 82 patients, 32 controls | Mean 42.7 years/ N/A | Blood | Neurologic parameters (Plasma BDNF) | Diagnosis/ Therapeutic response (TRT) | Plasma BDNF levels were higher in tinnitus and decreased after effective TRT, but there was no correlation with tinnitus loudness and severity. |
| Yuksel F et al. (2016) [36] | Case-control study | 100 patients, 100 controls (age-sex-matched) | Mean 50.95 years/ N/A | Blood | Hemostatic parameters (MPV, PDW, PC) Inflammatory parameters (CRP, ESR) | Diagnosis | MPV was lower, but PC and PDW were higher in tinnitus. ESR and CRP did not show any significant results. |
| Alsalman O A et al. (2016) [65] | Case-control study | 10 patients (male), 10 controls | 18–35 years/ Normal hearing | Saliva | Endocrine parameters (Cortisol) Immunologic parameters (Neopterin) Neurologic parameters (sAA) | Diagnosis/Prognosis | sAA levels were lower in tinnitus group, suggesting impaired sympathetic activity, and stress measurements were negatively correlated with measures of sAA and neopterin. |
| Orenay-Boyacioglu, S et al. (2016) [92] | Case-control study | 52 patients, 42 controls (age-matched) | 18–55 years/ N/A | Blood | Neurologic parameters (GDNF gene SNP rs884344, rs3812047, rs1110149) | Diagnosis | Heterozygosity was lower for GDNF rs1110149 in tinnitus, but no correlation was observed between tinnitus and GDNF gene polymorphism. |
| Bayram A et al. (2015) [40] | Retrospective case-control study | 51 patients, 42 controls (age-sex-matched) | Mean 43.47 years/ Normal hearing | Blood | Hemostatic parameters (MPV) Inflammatory parameters (NLR, PLR) | Diagnosis | No significant differences in NLR, PLR, and MPV between tinnitus group and control group. |
| Kemal O et al. (2015) [33] | Retrospective case-control study | 86 patients, 84 controls | Under 50 years/ Normal hearing | Blood | Hemostatic parameters (MPV) | Diagnosis | MPV values were significantly higher in tinnitus group. |
| Berkiten G et al. (2015) [115] | Cross-sectional study | 100 patients | 17–78 years/ Non-presbycusis (above 65 years and symmetrical increase in hearing threshold) | Blood | Oxidative parameters (Serum Zinc) | Prognosis | Zinc levels decrease as age increases and were significantly lower in group III (patients between 61–78 years). Also, severity and loudness of tinnitus and audiologic threshold of air conduction were greater in zinc-deficient group. |
| Ozbay I et al. (2015) [45] | Prospective case-control study | 107 patients, 107 controls (age-sex-matched) | Mean 38.7 years/ Normal hearing up to mild hearing loss | Blood | Inflammatory parameters (NLR) | Diagnosis | Despite other hematologic parameters showed no significant results, NLR was higher among the patients. |
| Szczepek A J et al. (2014) [76] | Prospective study | 30 patients | 18–67 years/ N/A | Blood | Neurologic parameters (Plasma BDNF level) Immunologic parameters (IL-1β, IL-6, TNF-α) | Prognosis | A positive correlation was observed between TNF-α, tinnitus loudness, total perceived stress, tension, and depression, but a negative correlation with a psychometric score ‘joy’. IL-1β concentration was correlated with awareness grade of tinnitus. No correlation was found between plasma BDNF level and psychometric scores. |
| Kim et al. (2013) [58] | Case-control study | 344 patients, 89 controls | Mean 53.8 years/ N/A | Blood | Endocrine parameters (Cortisol) Neurologic parameters (NE, Epi, 5-HIAA) | Prognosis | The percentage of patients with high 5-HIAA level was higher in tinnitus group, and 5-HIAA levels showed correlation with duration of tinnitus, NE, and cortisol. Elevation of stress-related hormones as well as BDI and BEPSI were the related factors with tinnitus. |
| Sand et al. (2012) [90] | Cross-sectional study | 240 patients | Mean 50.3 years/ N/A | Blood | Neurologic parameters (BDNF gene SNP rs6265 [Val66Met], rs2049046, GDNF gene SNP rs884344, rs1110149, rs3812047) | Prognosis | No significant allelic association but, GDNF and BDNF genotypes jointly predicted tinnitus severity in women. |
| Simoen V L et al. (2012) [62] | Prospective case-control study | 21 patients, 21 controls | Mean 65.7 years/ N/A | Saliva | Endocrine parameters (Cortisol) | Diagnosis/Prognosis | Basal cortisol level was similar, but stronger and longer-lasting cortisol suppression was observed after DEX administration in patients with tinnitus. And discomfort threshold was lower after cortisol suppression. |
| Goto et al. (2012) [10] | Case-control study | 43 patients, 30 controls | Mean 57.1 years/ N/A | Blood | Neurologic parameters (Plasma BDNF level) | Prognosis | Plasma BDNF level was higher in mildly handicapped tinnitus group. Patients with HADS scores ≤14 had lower THI and higher BDNF levels. |
| Lasisi A O et al. (2012 [68] | Prospective case-control study | 81 patients, 58 controls | 60–98 years/ N/A | Blood | Endocrine parameters (Plasma melatonin) Oxidative parameters (Ascorbic acid, Vit B12) | Diagnosis | Low plasma melatonin and Vitamin B12 have correlation with tinnitus in elderly, but no significant results were observed with Vitamin C. |
| Deniz M et al. (2009) [97] | Case-control study | 54 patients, 174 controls | 20–51 years/ Normal hearing (Pure tone average lower than 30dB at 250Hz to 6kHz) | Blood | Neurologic parameters (Serotonin transporter gene polymorphism [5-HTTLPR, VNTR]) | Prognosis | ‘ll’ genotype of the SLC6A4 polymorphic promoter region was associated with the VAS score, but not with psycho-acoustic parameters in tinnitus. |
| Hebert S et al. (2007) [54] | Prospective case-control study | 18 patients, 18 controls (age-matched) | Mean 68.8 years/ N/A | Saliva | Endocrine parameters (Cortisol) | Diagnosis/Prognosis | There was a blunted cortisol response to psychological stress in tinnitus group compared to that of controls. |
| Savastano M et al. (2007) [56] | Cross-sectional study | 85 patients | 18–65 years/ Normal hearing | Blood | Endocrine parameters (Cortisol, ACTH, β-endorphin, prolactin, urinary catecholamine) Immunologic parameters (CD19, CD16NK) | Diagnosis | There was no significant correlation between endocrine parameters and psychological test scores, but lymphocyte CD19 and CD16NK showed correlation with ACTH. |
| Savastano M et al. (2007) [114] | Cross-sectional study | 31 patients | 37–72 years/ N/A | Blood | Oxidative parameters (MDA, 4-HNE) | Therapeutic response (Antioxidant) | ROS, including MDA and 4-HNE were reduced following antioxidant treatment, with improvement of VAS and decrease in loudness. |
| Hebert S et al. (2004) [60] | Case-control study | 18 patients, 18 controls | Mean 65.5 years/ N/A | Saliva | Endocrine parameters (Cortisol) | Prognosis | High tinnitus-distress group has elevated chronic cortisol levels, and greater intolerance to external sound. |
| Weber C et al. (2002) [73] | Case-control study | 26 patients, 13 non-tinnitus, 18 controls | 20–65 years/ N/A | Blood | Immunologic parameters (IL-6, IL-10, TNF-α) | Therapeutic response (Relaxation program) | TNF-α was reduced after the relaxation program with stress perception, anxiety, anger, and disturbance, but no significant results were observed for IL-6 and IL-10. |
| Sachanska T. (1999) [95] | Case-control study | 24 patients, 75 controls | N/A | Blood | Neurologic parameters (Serotonin) | Diagnosis | 67% of patients with tinnitus had increased blood serotonin levels compared to the reference value. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, D.-W.; Kim, S.-S.; Park, D.-C.; Kim, S.-H.; Yeo, S.-G. Objective and Measurable Biomarkers in Chronic Subjective Tinnitus. Int. J. Mol. Sci. 2021, 22, 6619. https://doi.org/10.3390/ijms22126619
Kang D-W, Kim S-S, Park D-C, Kim S-H, Yeo S-G. Objective and Measurable Biomarkers in Chronic Subjective Tinnitus. International Journal of Molecular Sciences. 2021; 22(12):6619. https://doi.org/10.3390/ijms22126619
Chicago/Turabian StyleKang, Dae-Woong, Sung-Soo Kim, Dong-Choon Park, Sang-Hoon Kim, and Seung-Geun Yeo. 2021. "Objective and Measurable Biomarkers in Chronic Subjective Tinnitus" International Journal of Molecular Sciences 22, no. 12: 6619. https://doi.org/10.3390/ijms22126619
APA StyleKang, D.-W., Kim, S.-S., Park, D.-C., Kim, S.-H., & Yeo, S.-G. (2021). Objective and Measurable Biomarkers in Chronic Subjective Tinnitus. International Journal of Molecular Sciences, 22(12), 6619. https://doi.org/10.3390/ijms22126619