
Effect of Different Surface Treatment Methods on Bond Strength of Dental Ceramics to Dental Hard Tissues: A Systematic Review

 ,
, 
Abstract
1. Introduction
2. Results
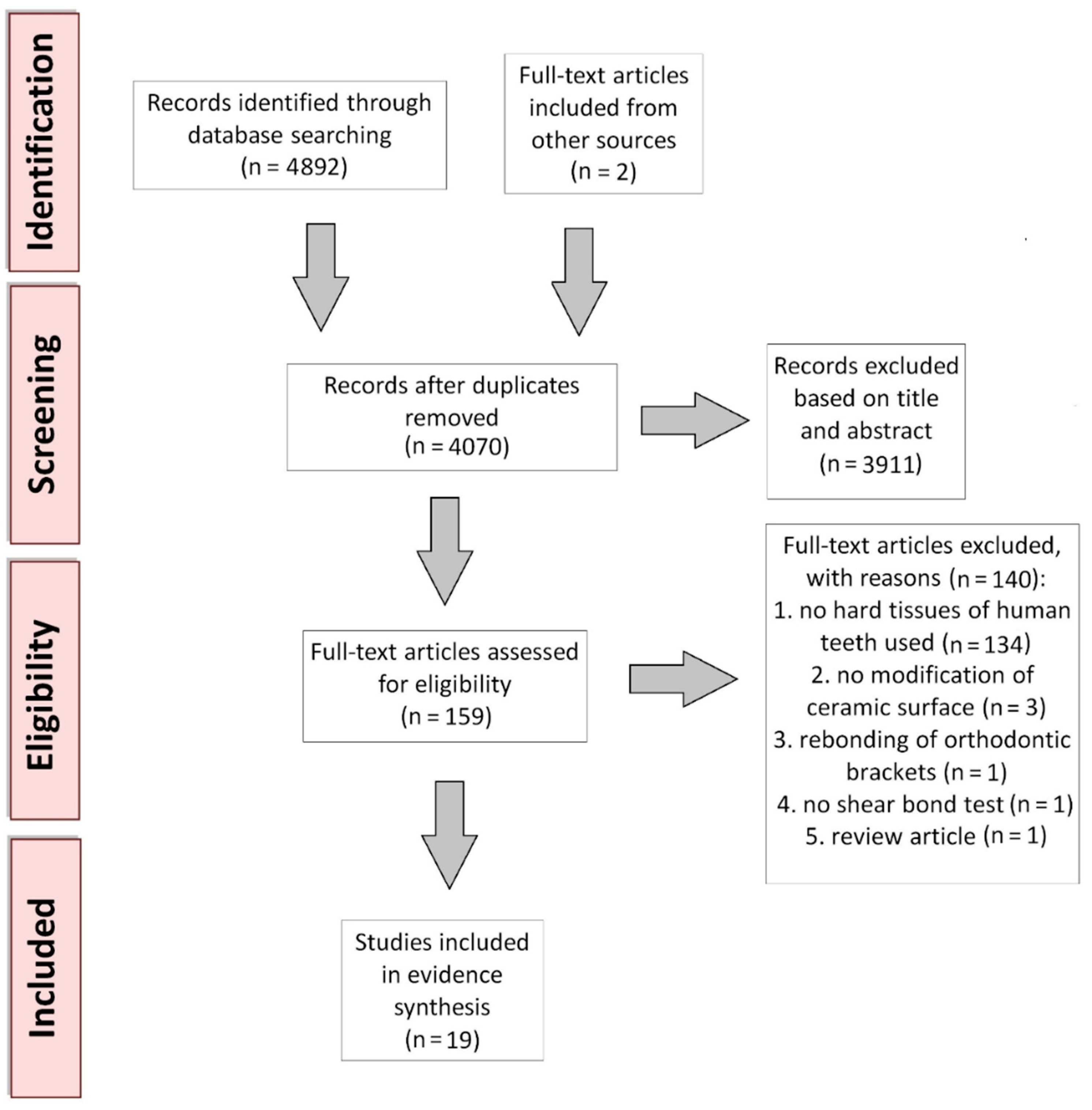
2.1. Study Selection
2.2. Material Characterization and Specimen Preparation
2.3. Methodology of the Selected Studies: Surface Treatment, Artificial Aging, and Bond Strength Evaluation
2.4. Outcomes
2.5. Evidence Synthesis
3. Discussion
4. Materials and Methods
4.1. Search Strategy
4.1.1. Data Sources and Searches
4.1.2. Eligibility Criteria for Initial Study Selection
4.2. Data Extraction
4.3. Data Synthesis and Analysis and Quality Assessment
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Tanaka, S.; Takaba, M.; Ishiura, Y.; Kamimura, E.; Baba, K. A 3-year follow-up of ceria-stabilized zirconia/alumina nanocomposite (Ce-TZP/A) frameworks for fixed dental prostheses. J. Prosthodont. Res. 2015, 59, 55–61. [Google Scholar] [CrossRef]
- Philipp, A.; Fischer, J.; Hämmerle, C.H.; Sailer, I. Novel ceriastabilized tetragonal zirconia/alumina nanocomposite as framework material for posterior fixed dental prostheses: Preliminary results of a prospective case series at 1 year of function. Quintessence Int. 2010, 41, 313–319. [Google Scholar] [PubMed]
- Blatz, M.B.; Sadan, A.; Kern, M. Resin-ceramic bonding: A review of the literature. J. Prosthet. Dent. 2003, 89, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Blatz, M.B.; Sadan, A.; Arch, G.H.; Lang, B.R. In vitro evaluation of long-term bonding of procera all ceram alumina restorations with modified resin luting agent. J. Prosthet. Dent. 2003, 89, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Lung, C.Y.; Matinlinna, J.P. Aspects of silane coupling agents and surface conditioning in dentistry: An overview. Dent. Mater. 2012, 28, 467–777. [Google Scholar] [CrossRef] [PubMed]
- Bielen, V.; Inokoshi, M.; Munck, J.D.; Zhang, F.; Vanmeensel, K.; Minakuchi, S.; Vleugels, J.; Naert, I.; Van Meerbeek, B. Bonding effectiveness to differently sandblasted dental zirconia. J. Adhes. Dent. 2015, 17, 235–242. [Google Scholar] [PubMed]
- Park, J.H.; Choi, Y.S. Microtensile bond strength and micromorphologic analysis of surface-treated resin nanoceramics. J. Adv. Prosthodont. 2016, 8, 275–284. [Google Scholar] [CrossRef] [PubMed]
- Mattiello, R.D.L.; Coelho, T.M.K.; Insaurralde, E.; Coelho, A.A.K.; Terra, G.P.; Kasuya, A.V.B.; Favarao, I.N.; Goncalves, L.S.; Fonseca, R.B. A review of surface treatment methods to improve the adhesive cementation of zirconia-based ceramics. Int. Sch. Res. Not. Biomater. 2013, 2013, 185376. [Google Scholar] [CrossRef]
- Griffin, J.D.; Suh, B.; Chen, L.; Brown, D.J. Surface treatments for zirconia bonding: A clinical perspective. Can. J. Restor. Dent. Prosthodont. 2010, 3, 23–29. [Google Scholar]
- Anami, L.C.; Lima, J.; Valandro, L.F.; Kleverlaan, C.J.; Feilzer, A.J.; Bottino, M.A. Fatigue resistance of Y-TZP/porcelain crowns is not influenced by the conditioning of the intaglio surface. Oper. Dent. 2016, 41, E1–E12. [Google Scholar] [CrossRef]
- Soares, C.J.; Soares, P.V.; Pereira, J.C.; Fonseca, R.B. Surface treatment protocols in the cementation process of ceramic and laboratory-processed composite restorations: A literature review. J. Esthet. Rest. Dent. 2005, 17, 224–235. [Google Scholar] [CrossRef] [PubMed]
- Atsu, S.S.; Kilicarslan, M.A.; Kucukesmen, H.C.; Aka, P.S. Effect of zirconium-oxide ceramic surface treatments on the bond strength to adhesive resin. J. Prosthet. Dent. 2006, 95, 430–436. [Google Scholar] [CrossRef]
- Blatz, M.B.; Chiche, G.; Holst, S.; Sadan, A. Influence of surface treatment and simulated aging on bond strengths of luting agents to zirconia. Quintessence Int. 2007, 38, 745–753. [Google Scholar]
- Lindgren, J.; Smeds, J.; Sjogren, G. Effect of surface treatments and aging in water on bond strength to zirconia. Oper. Dent. 2008, 33, 675–681. [Google Scholar] [CrossRef] [PubMed]
- Carrilho, E.; Cardoso, M.; Marques Ferreira, M.; Marto, C.M.; Paula, A.; Coelho, A.S. 10-MDP Based Dental Adhesives: Adhesive Interface Characterization and Adhesive Stability—A Systematic Review. Materials 2019, 12, 790. [Google Scholar] [CrossRef] [PubMed]
- Qeblawi, D.M.; Munoz, C.A.; Brewer, J.D.; Monaco, E.A. The effect of zirconia surface treatment on flexural strength and shear bond strength to a resin cement. J. Prosthet. Dent. 2010, 103, 210–220. [Google Scholar] [CrossRef]
- Madina, M.M.; Ozcan, M.; Badawi, M.F. Effect of surface conditioning and taper angle on the retention of IPS e.max Press crowns. J. Prosthodont. 2010, 19, 200–204. [Google Scholar] [CrossRef]
- Shahin, R.; Kern, M. Effect of air-abrasion on the retention of zirconia ceramic crowns luted with different cements before and after artificial aging. Dent. Mater. 2010, 26, 922–928. [Google Scholar] [CrossRef]
- Chai, J.; Chu, F.C.; Chow, T.W. Effect of surface treatment on shear bond strength of zirconia to human dentin. J. Prosthodont. 2011, 20, 173–179. [Google Scholar] [CrossRef]
- Reddy, S.M.; Vijitha, D.; Deepak, T.; Balasubramanian, R.; Satish, A. Evaluation of shear bond strength of zirconia bonded to dentin after various surface treatments of zirconia. J. Indian Prosthodont. Soc. 2014, 14, 38–41. [Google Scholar] [CrossRef]
- de Castro, H.L.; Corazza, P.H.; de Paes-Júnior, T.A.; Bona, A.D. Influence of Y-TZP ceramic treatment and different resin cements on bond strength to dentin. Dent. Mater. 2012, 28, 1191–1197. [Google Scholar] [CrossRef] [PubMed]
- Bottino, M.A.; Bergoli, C.; Lima, E.G.; Marocho, S.M.; Souza, R.O.; Valandro, L.F. Bonding of Y-TZP to dentin: Effects of Y-TZP surface conditioning, resin cement type, and aging. Oper. Dent. 2014, 39, 291–300. [Google Scholar] [CrossRef] [PubMed]
- Feng, X.L.; Liu, R.Y.; Znag, Y.L.; Chen, L.J. Effect of Surface Treatment and Resin Cement on Microtensile Bond Strength of Zirconia to Dentin. Key Eng. Mater. 2014, 602, 602–605. [Google Scholar] [CrossRef]
- Alves, M.; Campos, F.; Bergoli, C.D.; Bottino, M.A.; Özcan, M.; Souza, R. Effect of Adhesive Cementation Strategies on the Bonding of Y-TZP to Human Dentin. Oper. Dent. 2016, 41, 276–283. [Google Scholar] [CrossRef] [PubMed]
- Jetti, R.R.; Balasubramaniam, M.; Chidambaranathan, A.S.; Srinivasan, S. Evaluation of Shear Bond Strength of Feldspathic CAD/CAM Ceramic with Dentin using 2 Bonding Agents and 2 Surface Treatments-An Invitro Study. J. Clin. Diagn. Res. 2015, 9, 36–39. [Google Scholar] [CrossRef] [PubMed]
- Unal, S.M.; Nigiz, R.; Polat, Z.S.; Usumez, A. Effect of ultrashort pulsed laser on bond strength of Y-TZP zirconia ceramic to tooth surfaces. Dent. Mater. J. 2015, 34, 351–357. [Google Scholar] [CrossRef]
- Kara, O.; Ozturk, A. The effect of surface treatments on the bonding strength of ceramic inlays to dentin. J. Adhes. Sci. Technol. 2017, 31, 1–13. [Google Scholar] [CrossRef]
- Gamal, A.E.; Medioni, E.; Rocca, J.P.; Fornaini, C.; Brulat-Bouchard, N. CO2 laser dentin surface treatment most effectively increased ceramic shear bond strength. Laser Ther. 2018, 27, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Butler, S.; Linke, B.; Torrealba, Y. Effect of MDP-Based Primers on the Luting Agent Bond to Y-TZP Ceramic and to Dentin. Biomed. Res. Int. 2018, 16. [Google Scholar] [CrossRef]
- Zandparsa, R.; Talua, N.A.; Finkelman, M.D.; Schaus, S.E. An in vitro comparison of shear bond strength of zirconia to enamel using different surface treatments. J. Prosthodont. 2014, 23, 117–123. [Google Scholar] [CrossRef]
- Lv, P.; Yang, X.; Jiang, T. Influence of Hot-Etching Surface Treatment on Zirconia/Resin Shear Bond Strength. Materials 2015, 8, 8087–8096. [Google Scholar] [CrossRef]
- Menani, L.R.; Farhat, I.A.G.K.M.; Tiossi, R.; Ribeiro, R.F.; Guastaldi, A.C. Effect of surface treatment on the bond strength between yttria partially stabilized zirconia ceramics and resin cement. J. Prosthet. Dent. 2014, 112, 357–364. [Google Scholar] [CrossRef]
- Saker, S.; Ibrahim, F.; Ozcan, M. Effect of different surface treatments on adhesion of In-Ceram Zirconia to enamel and dentin substrates. J. Adhes. Dent. 2013, 15, 369–376. [Google Scholar] [PubMed]
- Russo, D.S.; Cinelli, F.; Sarti, C.; Giachetti, L. Adhesion to Zirconia: A Systematic Review of Current Conditioning Methods and Bonding Materials. Dent. J. 2019, 7, 74. [Google Scholar] [CrossRef] [PubMed]
- Luthra, R.; Kaur, P. An insight into current concepts and techniques in resin bonding to high strength ceramics. Aust. Dent. J. 2016, 61, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Ozcan, M.; Yoshida, K.; Cheng, H.; Sawase, T. Bonding to industrial indirect composite blocks: A systematic review and meta-analysis. Dent. Mater. 2020, 36, 119–134. [Google Scholar] [CrossRef] [PubMed]
- Yassen, G.H.; Platt, J.A.; Hara, A.T. Bovine teeth as substitute for human teeth in dental research: A review of literature. J. Oral Sci. 2011, 53, 273–282. [Google Scholar] [CrossRef] [PubMed]
- Soares, F.Z.; Follak, A.; da Rosa, L.S.; Montagner, A.F.; Lenzi, T.L.; Rocha, R.O. Bovine tooth is a substitute for human tooth on bond strength studies: A systematic review and meta-analysis of in vitro studies. Dent. Mater. 2016, 32, 1385–1393. [Google Scholar] [CrossRef] [PubMed]
- de Carvalho, M.F.F.; Leijôto-Lannes, A.C.N.; Rodrigues, M.C.N.; Nogueira, L.C.; Ferraz, N.K.L.; Moreira, A.N.; Yamauti, M.; Zina, L.G.; Magalhães, C.S. Viability of Bovine Teeth as a Substrate in Bond Strength Tests: A Systematic Review and Meta-analysis. J. Adhes. Dent. 2018, 20, 471–479. [Google Scholar]
- Canbek, K.; Karbach, M.; Gottschalk, F.; Erbe, C.; Wehrbein, H. Evaluation of bovine and human teeth exposed to thermocycling for microleakage under bonded metal brackets. J. Orofac. Orthop. 2013, 74, 102–112. [Google Scholar] [CrossRef]
- Fernandes, V.V.B.; Oliani, M.G.; Nogueira, L.; Silva, J.M.F.; Araujo, R.M. Analysis and Comparison of Different Bond Strength Tests. JSM Dent. 2016, 4, 1076. [Google Scholar]
- Sirisha, K.; Rambabu, T.; Ravishankar, Y.; Ravikumar, P. Validity of bond strength tests: A critical review—Part II. J. Conserv. Dent. 2014, 17, 420–426. [Google Scholar] [CrossRef] [PubMed]
- Rungruanganunt, P.; Kelly, R.J. Insight into “bonding” of all-ceramics influenced by cement, sandblasting and water storage time. Dent. Mater. 2012, 28, 939–944. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; for the PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 349, g7647. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.; Oxman, A.D.; Akl, E.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falk-Ytter, Y.; Glasziou, P.; Debeer, H.; et al. GRADE guidelines 1. Introduction-GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author and Year | Ceramics (Commercial Name, Manufacturer) | Cement (Commercial Name, Manufacturer) |
|---|---|---|
| Madina 2010 [17] | IPS e.max PRESS (Ivoclar Vivadent) | Panavia F 2.0 (Kuraray) |
| Qeblawi 2010 [16] | IPS e.max ZirCAD (Ivoclar Vivadent) | Multilink Automix (Ivoclar Vivadent) |
| Shahin 2010 [18] | In-Ceram YZ for inLAB (Vita) | (1) Hoffmann quick setting (Hoffmann Dental) (2) Ketac Cem Maxi Cap (3M ESPE) (3) Panavia 21 TC (Kuraray) |
| Chai 2011 [19] | (1) In-Ceram Zirconia (Vita) (2) YZ Zirconia (Vita) | Panavia F 2.0 (Kuraray) |
| Reddy 2012 [20] | Incoris ZI (Sirona) | Multilink Speed (Ivoclar Vivadent) |
| De Castro 2012 [21] | In-Ceram YZ (Vita) | (1) RelyX ARC (3M ESPE) (2) RelyX U100 (3M ESPE) (3) Panavia F (Kuraray) |
| Saker 2013 [33] | In-Ceram Zirconia (Vita) | Panavia F 2.0 (Kuraray) |
| Zandparsa 2013 [30] | Zirconia (3M ESPE) | Panavia F 2.0 (Kuraray) |
| Bottino 2014 [22] | In Ceram YZ 2000 (Vita) | (1) Panavia F (Kuraray) (2) Clearfil SA Cement (Kuraray) |
| Feng 2014 [23] | Sintered zirconia blocks (3M ESPE) | (1) Panavia F (Kuraray) (2) RelyX Unicem (3M ESPE) |
| Menani 2014 [32] | Lava Frame Y-TZP (3M ESPE) | Panavia F (Kuraray) |
| Alves 2015 [24] | InCeram YZ (Vita) | (1) RelyX ARC (3M ESPE) (2) RelyX U200 (3M ESPE) |
| Jetti 2015 [25] | CEREC (Sirona) | Variolink II (Ivoclar Vivadent) |
| Lv 2015 [31] | Yttria-stabilized zirconia powder (Tosho) | (1) Superbond C and B (Sun Medical) (2) Panavia F 2.0 (Kuraray) |
| Unal 2015 [26] | ZirkonZahn (Steger) | (1) Panavia F 2.0 (Kuraray) (2) Variolink N (Ivoclar Vivadent) |
| Park 2016 [7] | Lava Ultimate (3M ESPE) | RelyX (3M ESPE) |
| Kara 2017 [27] | (1) Finesse (Ceramco) (2) IPS Empress Esthetics (Ivoclar Vivadent) (3) IPS Empress e.Max (Ivoclar Vivadent) (4) Zirkonzahn Prettau (Zirkonzahn GmBh) | Clearfil Esthetic Cement (Kuraray) |
| Gamal 2018 [28] | (1) IPS e.max CAD (Ivoclar Vivadent) (2) IPS e.max ZirCAD (Ivoclar Vivadent) | RelyX Ultimate (3M ESPE) |
| Butler 2018 [29] | NexxZr (Sagemax Bioceramic) | Duo-link (Bisco) |
| Author and Year | Surface Treatment | Artificial Aging | Primary Outcome: Impact of Different Surface Treatment Methods on the Bond Strength | Secondary Outcome: Impact of the Other Studied Factors on the Bond Strength |
|---|---|---|---|---|
| Madina 2010 [17] | (1) HF acid 5% + silane (2) APA + tribochemical silica coating + silane | None | No statistically significant difference was found between the surface conditioning methods. | - |
| Qeblawi 2010 [16] | 16 groups: 4 different mechanical treatments: (1) No mechanical treatment (2) APA (3) Tribochemical silica coating (4) Wet hand grinding Combined with 4 different chemical treatments: (1) No chemical treatment (2) Acid etching + silane (3) Silane (4) Zirconia primer | (1) None (2) 90 days at 100% humidity and 37 °C; 2000 thermal cycles (5–55 °C, 10 s dwell time) every 30 days for a total of 6000 cycles | The highest SBS values were achieved for silica coating + silane. | (1) Statistically significant difference was observed between the groups (immediate/aged). (2) Artificial aging resulted in significantly lower SBS for silica coating + silane and for no mechanical treatment + zirconia primer. |
| Shahin 2010 [18] | (1) No treatment (2) APA | (1) 3 days in distilled water at 37 °C (2) 150 days in distilled water at 37 °C; 37,500 thermal cycles (5–55 °C, 30 s dwell time); after thermocycling, masticatory simulation (300,000 cycles, load of 50 N) | APA significantly increased crown retention. | (1) Artificial aging significantly reduced retention. (2) Adhesive resin cement (Panavia 21) allowed significantly higher retention than the conventional cements. |
| Chai 2011 [19] | (1) No treatment (2) Chairside tribochemical silica coating + silane (CoJet, 3M ESPE) + resin-bonding agent (Visio Bond, 3M ESPE) (3) Laboratory tribochemical silica coating + silane (Rocatec, 3M ESPE) | None | In-Ceram Zirconia treated with CoJet had a significantly higher SBS than those untreated or treated with Rocatec. | The bond strength between the two ceramic types was not significantly different. |
| Reddy 2012 [20] | (1) No treatment (2) APA (3) HF acid 4.5% (4) HF acid 4.5% + silane (5) Zirconia primer | None | (1) The highest values were obtained for zirconia primer, the second highest for APA, and the third for HF acid with silane. (2) There were no significant differences between HF acid and nontreated control. | - |
| De Castro 2012 [21] | (1) APA (2) Tribochemical silica coating | (1) No additional storage (2) 60 days in distilled water at 37 °C (3) 10,000 thermal cycles (5–55 °C, 30 s dwell time) | Statistically significant difference was found between the groups treated with different surface conditioning methods. | (1) Resin cement and artificial aging significantly affected the mean bond strength values. (2) The highest bond strength was achieved for Panavia F with APA after thermal cycling. |
| Saker 2013 [33] | (1) No treatment (2) APA (3) Tribochemical silica coating + silane (4) Tribochemical silica coating + metal primer-containing MDP (5) Glaze ceramic + HF acid 9.6% + silane | 5000 thermal cycles (5–55 °C, 20 s dwell time) | (1) All the surface treatment protocols significantly increased the tensile bond strength compared to control. (2) The lowest increase was achieved for APA, and the highest for glaze + HF acid (for enamel) or tribochemical silica coating + metal primer (for dentin). | Substrate type (enamel vs. dentin) had a significant influence on the bond strength. |
| Zandparsa 2013 [30] | (1) APA (2) APA + Z-PRIME Plus (3) APA + alloy primer (4) Piranha solution 7:1 (5) Piranha solution 7:1+ Z-PRIME (6) Piranha solution 7:1 + alloy primer (7) Tribochemical silica coating + silane | 500 thermal cycles (5–55 °C, 15 s dwell time) | APA + Z-PRIME Plus showed significant improvement in SBS compared to all other groups. | - |
| Bottino 2014 [22] | (1) Low-fusing porcelain glaze + HF acid 10% + silane (2) Tribochemical silica coating | 5000 thermal cycles (5–55 °C, 30 s dwell time) | No statistically significant difference was found between the groups treated with different surface conditioning methods. | Resin cement (Panavia > Clearfil) and storage conditions (nonaging > aging) significantly influenced the SBS. |
| Feng 2014 [23] | (1) No treatment (2) APA+ silane (3) APA+ tribochemical silica coating + silane | None | The bond strength of APA + silica coating + silane group was the highest, while the bond strength in the control group was the lowest. | Specimens bonded with Panavia F exhibited significantly higher bond strength than those with RelyX Unicem regardless of the surface treatments. |
| Menani 2014 [32] | (1) No treatment (2) Alloy primer (3) HF acid 40% (4) HF acid 40% + alloy primer | None | (1) The extrusion shear strength of the group etched with 40% HF acid was significantly higher than that of other groups. (2) Differences for the other groups were not statistically significant. | - |
| Alves 2015 [24] | (1) No treatment (2) Chairside tribochemical silica coating + silane (CoJet, 3M ESPE) (3) Laboratory tribochemical silica coating + silane (Rocatec + 3M ESPE) (4) Universal primer | 30 days in distilled water at 37°C | (1) Universal primer application provided the highest SBS compared to other methods. (2) Nontreated control group presented the lowest SBS. | Cement type did not significantly affect the SBS. |
| Jetti 2015 [25] | (1) HF acid <5% + Prime and Bond NT (2) HF acid <5% + silane + Prime and Bond NT (3) HF acid <5% + Xeno III (4) HF acid <5% + silane +Xeno III | None | (1) The application of silane significantly increased the SBS in both groups bonded with Prime and Bond NT and with Xeno III. (2) There were no significant differences in SBS between the groups bonded with Prime and Bond NT and with Xeno III. (3) The highest SBS was achieved using <5% HF acid + silane and Prime and Bond NT. | - |
| Lv 2015 [31] | (1) No treatment (2) APA (3) Hot-etching treatment (800 mL of methanol, 200 mL of 37% HCl and 2 g of FeCl3) for 1 h at 100 °C | 5000 thermal cycles (5–55 °C, 30 s dwell time) | The hot-etching group had significantly higher SBS than the control and APA groups. | SBS was significantly lower after thermal cycling in all groups except for the hot-etching group that was cemented with Panavia F2.0. |
| Unal 2015 [26] | (1) No treatment (2) APA (3) Tribochemical silica coating (4) YbPL laser | 5000 thermal cycles (5–55 °C, 15 s dwell time) | Laser-irradiated groups had significantly higher SBS than the other groups. | Cement type significantly affected the SBS values (Panavia F 2.0 > Variolink N). |
| Park 2016 [7] | (1) APA (2) APA + Singlebond Universal Adhesive (3) HF acid 4% + Singlebond Universal Adhesive (4) HF acid 4% + silane + Singlebond Universal Adhesive (5) Tribochemical silica coating (6) Tribochemical silica coating + Singlebond Universal Adhesive | None | (1) APA + universal adhesive resulted in the highest bond strength followed by tribochemical silica coating + universal adhesive. (2) The lowest bond strength was achieved for 4% HF acid etching + universal adhesive. (3) Universal adhesive increased the bond strength, while silane had no significant effect. | - |
| Kara 2017 [27] | (1) No treatment (2) APA (3) HF acid 9% (4) Hot acidic solution containing HCl and FeCl3 (100 °C) applied for 30 min (5) Nd:YAG laser (6) Nd:YAG laser + APA (7) Nd:YAG laser + HF acid 9% (8) Nd:YAG laser + hot acidic solution | 5000 thermal cycles (5–55 °C, 30 s dwell time) | (1) No significant differences in bond strength were seen in Finesse ceramic groups treated with different methods. (2) HF acid etching increased the bond strength of IPS Empress Esthetics. (3) APA and HF acid etching increased the bond strength of IPS Empress e-Max. (4) APA and Nd:YAG + APA increased the bond strength of Zirkonzahn Prettau. | - |
| Gamal 2018 [28] | (1) CO2 laser + HF acid 9% + silane (2) HF acid 9% + silane (3) CO2 laser + APA + silane (4) APA + silane | None | (1) Laser irradiation increased the SBS between zirconia and dentin compared with nonirradiated ceramic surfaces. (2) Laser irradiation combined with HF acid and silane did not seem to be an alternative method for improving the dentin-to-ceramic surface (lithium disilicate) bonding. | |
| Butler 2018 [29] | (1) No treatment (2) APA (3) Primer (4) APA + primer (5) APA + All-Bond Universal (6) APA + ScotchBond Universal Adhesive | None | (1) SBS was significantly influenced by the use of APA, primer, or adhesive. (2) The use of Z-Prime Plus and All-Bond Universal resulted in significantly higher bond strength. | - |
| Outcome | Outcome Significance | Author and Year | No. of Specimens per Group | Quality of the Evidence (GRADE) |
|---|---|---|---|---|
| Primary outcome | Significant correlation | Qeblawi 2010 [16] | 12 | ++++ high |
| Shahin 2010 [18] | 8 | +++− moderate due to indirectness | ||
| Chai 2011 [19] | 12 | ++−− low due to imprecision and risk of bias | ||
| Reddy 2012 [20] | 4 | +++− moderate due to imprecision | ||
| De Castro 2012 [21] | 3 | ++−− low due to imprecision and risk of bias | ||
| Saker 2013 [33] | 10 | ++++ high | ||
| Zandparsa 2013 [30] | 10 | +++− moderate due to risk of bias | ||
| Feng 2014 [23] | 10 | +++− moderate due to imprecision | ||
| Menani 2014 [32] | 7 | ++− low due to imprecision and indirectness | ||
| Alves 2015 [24] | 10 | ++++ high | ||
| Jetti 2015 [25] | 10 | ++−− low due to imprecision and risk of bias | ||
| Lv 2015 [31] | 10 | ++++ high | ||
| Unal 2015 [26] | 15 | +++− moderate due to imprecision | ||
| Park 2016 [7] | 30 | ++−− low due to imprecision and risk of bias | ||
| Kara 2017 [27] | 12 | ++++ high | ||
| Gamal 2018 [28] | 6 | ++−− low due to imprecision and risk of bias | ||
| Butler 2018 [29] | 10 | ++++ high | ||
| No significant correlation | Madina 2010 [17] | 8 | ++−− low due to indirectness and risk of bias | |
| Bottino 2014 [22] | 10 | +++− moderate due to risk of bias | ||
| Secondary outcome | Significant correlation | Qeblawi 2010 [16] | 12 | +++− moderate due to risk of bias |
| Shahin 2010 [18] | 8 | +++− moderate due to indirectness and risk of bias | ||
| De Castro 2012 [21] | 3 | ++−− low due to imprecision | ||
| Saker 2013 [33] | 10 | +++− moderate due to indirectness | ||
| Bottino 2014 [22] | 10 | ++++ high | ||
| Feng 2014 [23] | 10 | +++− moderate due to imprecision | ||
| Lv 2015 [31] | 10 | ++++ high | ||
| Unal 2015 [26] | 15 | +++− moderate due to imprecision | ||
| No significant correlation | Chai 2011 [19] | 12 | ++−− low due to imprecision and risk of bias | |
| Alves 2015 [24] | 10 | ++++ high |
| PICOS | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Population | Ceramic samples luted to hard tissues of tooth (enamel or dentin) | Samples that are not made of ceramic Ceramic–cement combination without tooth tissue Ceramic luted to another material (composite, metal), without tooth tissue |
| Intervention | Any method of surface modification | No surface modification applied |
| Comparator | Nontreated control or any other method of surface modification | None |
| Outcome | Shear or tensile bond strength or retentive strength of the ceramics luted to the tooth tissue | Any other methods used for the evaluation of the quality of the bond between the ceramic and the tooth |
| Study | Only English language and full-text articles published between 1 January 2010 and 1 January 2020 | Review papers Articles not in English Articles published before 1 January 2010 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malysa, A.; Wezgowiec, J.; Orzeszek, S.; Florjanski, W.; Zietek, M.; Wieckiewicz, M. Effect of Different Surface Treatment Methods on Bond Strength of Dental Ceramics to Dental Hard Tissues: A Systematic Review. Molecules 2021, 26, 1223. https://doi.org/10.3390/molecules26051223
Malysa A, Wezgowiec J, Orzeszek S, Florjanski W, Zietek M, Wieckiewicz M. Effect of Different Surface Treatment Methods on Bond Strength of Dental Ceramics to Dental Hard Tissues: A Systematic Review. Molecules. 2021; 26(5):1223. https://doi.org/10.3390/molecules26051223
Chicago/Turabian StyleMalysa, Andrzej, Joanna Wezgowiec, Sylwia Orzeszek, Wojciech Florjanski, Marek Zietek, and Mieszko Wieckiewicz. 2021. "Effect of Different Surface Treatment Methods on Bond Strength of Dental Ceramics to Dental Hard Tissues: A Systematic Review" Molecules 26, no. 5: 1223. https://doi.org/10.3390/molecules26051223
APA StyleMalysa, A., Wezgowiec, J., Orzeszek, S., Florjanski, W., Zietek, M., & Wieckiewicz, M. (2021). Effect of Different Surface Treatment Methods on Bond Strength of Dental Ceramics to Dental Hard Tissues: A Systematic Review. Molecules, 26(5), 1223. https://doi.org/10.3390/molecules26051223