
Coffee Consumption and Risk of Hypertension in Adults: Systematic Review and Meta-Analysis

 , ,
, ,  , , , and
, , , and 
Abstract
1. Introduction
2. Methods
Statistical Analysis
3. Results
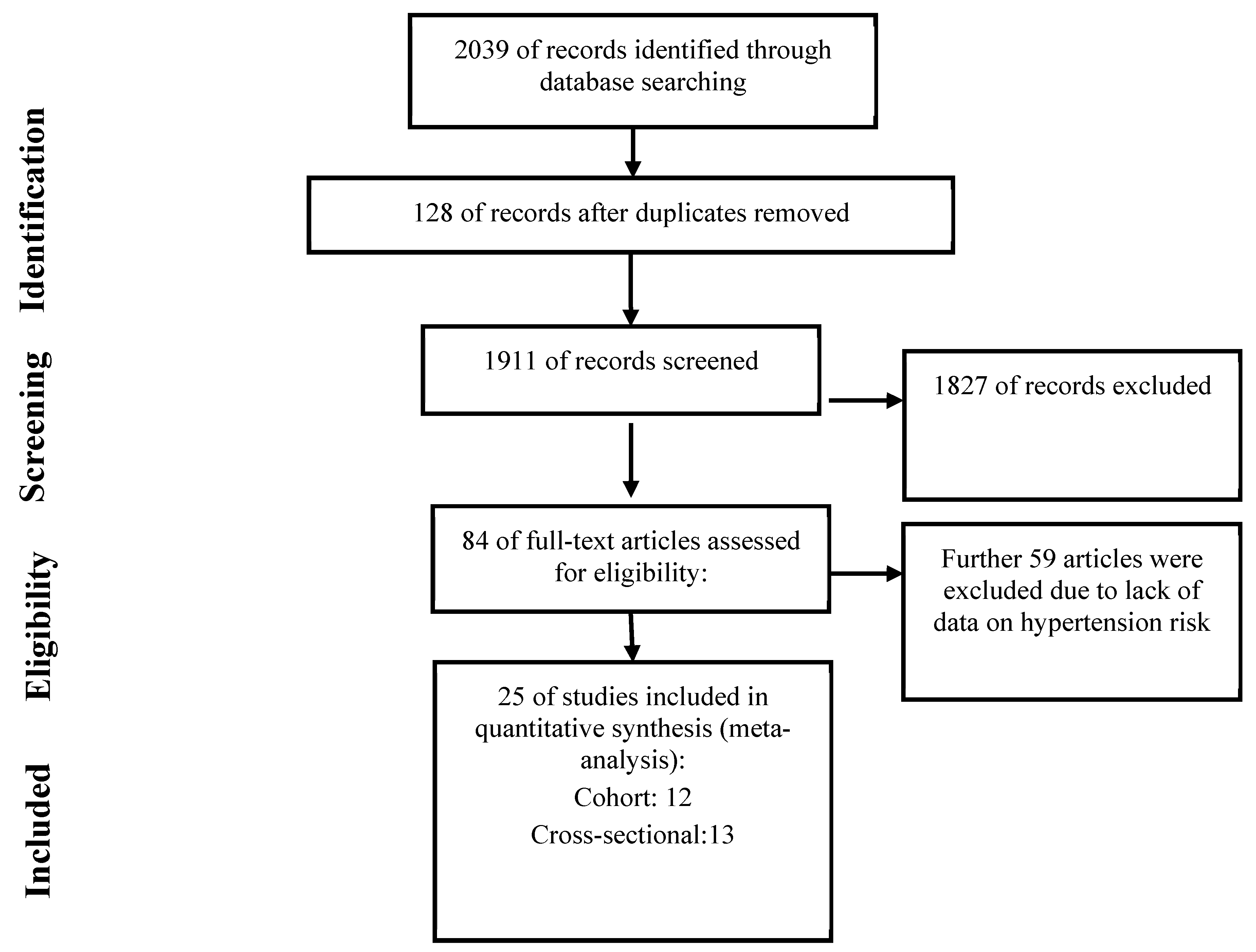
3.1. Search Results
3.2. Characteristics of Studies Included in the Meta-Analysis
3.3. Results of Meta-Analysis
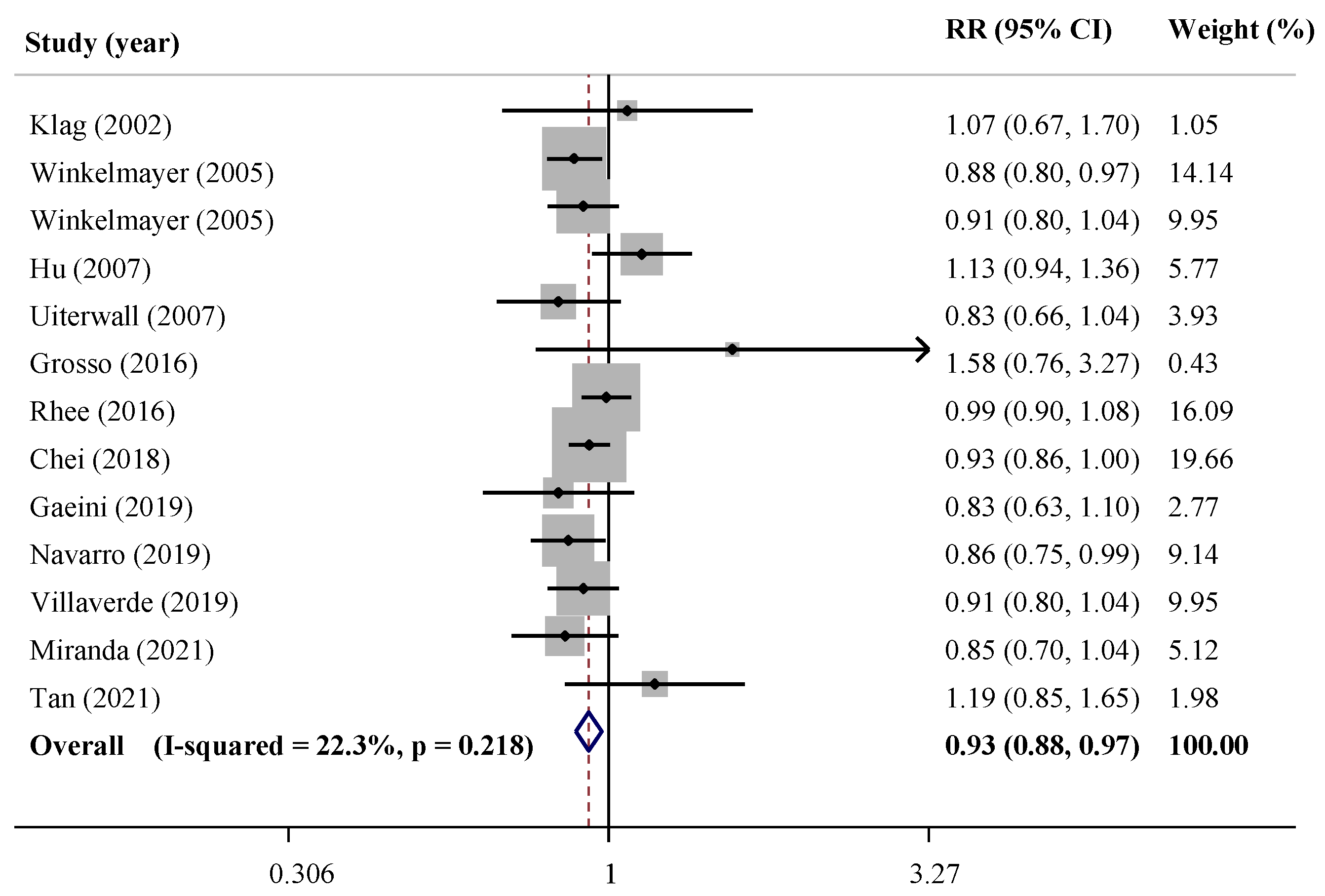
3.3.1. Cohort Studies
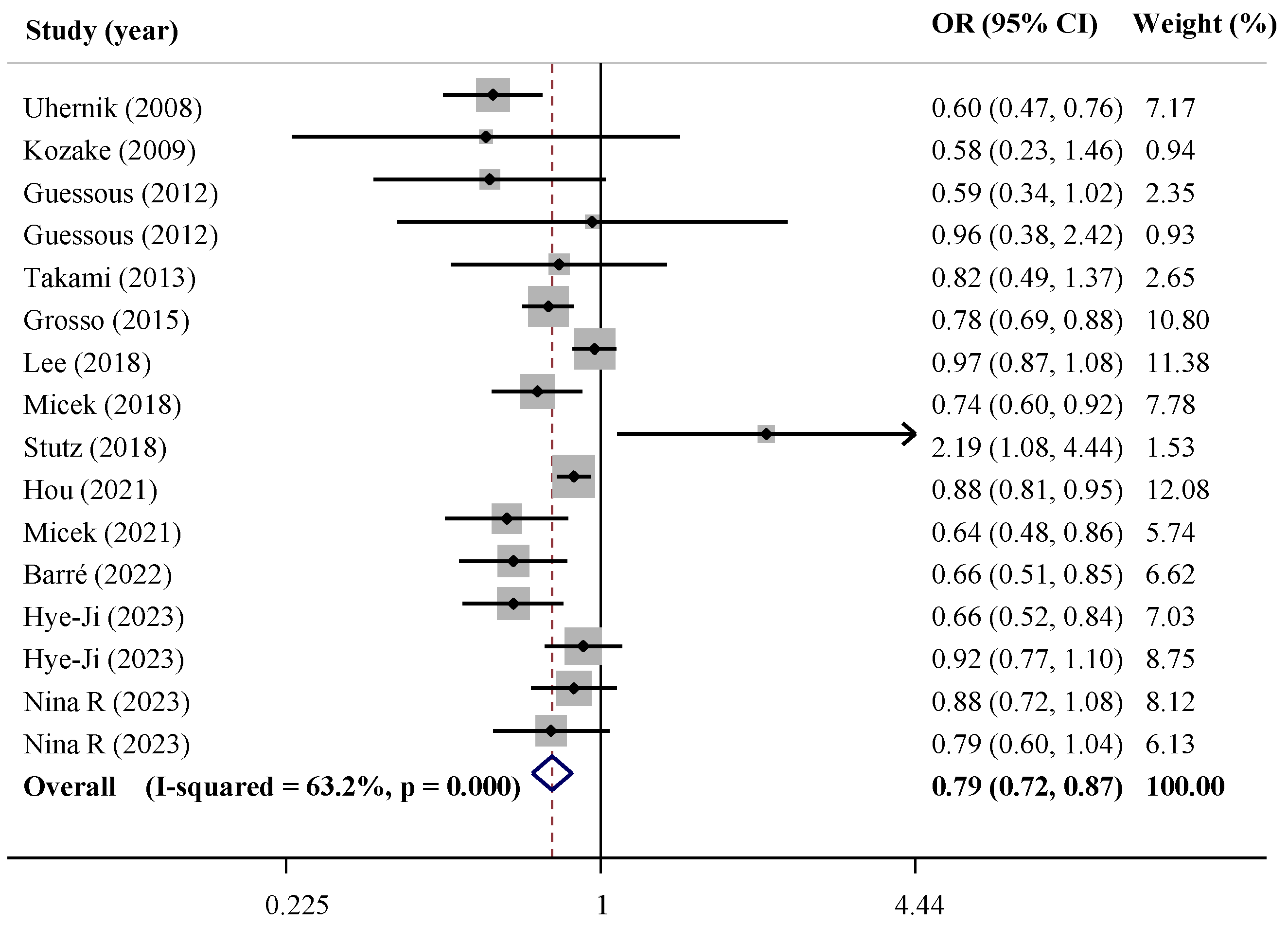
3.3.2. Cross-Sectional Studies
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mills, K.T.; Stefanescu, A.; He, J. The global epidemiology of hypertension. Nat. Rev. Nephrol. 2020, 16, 223–237. [Google Scholar] [CrossRef] [PubMed]
- Zhou, B.; Carrillo-Larco, R.M.; Danaei, G.; Riley, L.M.; Paciorek, C.J.; Stevens, G.A.; Gregg, E.W.; Bennett, J.E.; Solomon, B.; Singleton, R.K.; et al. Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: A pooled analysis of 1201 population-representative studies with 104 million participants. Lancet 2021, 398, 957–980. [Google Scholar] [CrossRef]
- Mills, K.T.; Bundy, J.D.; Kelly, T.N.; Reed, J.; Kearney, P.M.; Reynolds, K.; Chen, J.; He, J. Abstract 16828: Global Disparities of Hypertension Prevalence and Control: A Systematic Analysis of Population-based Studies From 90 Countries. Circulation 2016, 132, 441–450. [Google Scholar] [CrossRef] [PubMed]
- Morze, J.; Danielewicz, A.; Hoffmann, G.; Schwingshackl, L. Diet Quality as Assessed by the Healthy Eating Index, Alternate Healthy Eating Index, Dietary Approaches to Stop Hypertension Score, and Health Outcomes: A Second Update of a Systematic Review and Meta-Analysis of Cohort Studies. J. Acad. Nutr. Diet. 2020, 120, 1998–2031.e15. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Schwedhelm, C.; Hoffmann, G.; Knüppel, S.; Iqbal, K.; Andriolo, V.; Bechthold, A.; Schlesinger, S.; Boeing, H. Food Groups and Risk of Hypertension: A Systematic Review and Dose-Response Meta-Analysis of Prospective Studies. Adv. Nutr. 2017, 8, 793–803. [Google Scholar] [CrossRef]
- Voskoboinik, A.; Koh, Y.; Kistler, P.M. Cardiovascular effects of caffeinated beverages. Trends Cardiovasc. Med. 2019, 29, 345–350. [Google Scholar] [CrossRef] [PubMed]
- Turnbull, D.; Rodricks, J.V.; Mariano, G.F.; Chowdhury, F. Caffeine and cardiovascular health. Regul. Toxicol. Pharmacol. 2017, 89, 165–185. [Google Scholar] [CrossRef]
- Rodríguez-Artalejo, F.; López-García, E. Coffee Consumption and Cardiovascular Disease: A Condensed Review of Epi-demiological Evidence and Mechanisms. J. Agric. Food Chem. 2018, 66, 5257–5263. [Google Scholar] [CrossRef] [PubMed]
- O’Keefe, J.H.; Bhatti, S.K.; Patil, H.R.; DiNicolantonio, J.J.; Lucan, S.C.; Lavie, C.J. Effects of Habitual Coffee Consumption on Cardiometabolic Disease, Cardiovascular Health, and All-Cause Mortality. J. Am. Coll. Cardiol. 2013, 62, 1043–1051. [Google Scholar] [CrossRef]
- Surma, S.; Oparil, S. Coffee and Arterial Hypertension. Curr. Hypertens. Rep. 2021, 23, 38. [Google Scholar] [CrossRef]
- Steffen, M.; Kuhle, C.; Hensrud, D.; Erwin, P.J.; Murad, M.H. The effect of coffee consumption on blood pressure and the development of hypertension: A systematic review and meta-analysis. J. Hypertens. 2012, 30, 2245–2254. [Google Scholar] [CrossRef] [PubMed]
- D’elia, L.; La Fata, E.; Galletti, F.; Scalfi, L.; Strazzullo, P. Coffee consumption and risk of hypertension: A dose–response meta-analysis of prospective studies. Eur. J. Nutr. 2019, 58, 271–280. [Google Scholar] [CrossRef]
- Zhang, Z.; Hu, G.; Caballero, B.; Appel, L.; Chen, L. Habitual coffee consumption and risk of hypertension: A systematic review and meta-analysis of prospective observational studies. Am. J. Clin. Nutr. 2011, 93, 1212–1219. [Google Scholar] [CrossRef] [PubMed]
- De Giuseppe, R.; Di Napoli, I.; Granata, F.; Mottolese, A.; Cena, H. Caffeine and blood pressure: A critical review perspective. Nutr. Res. Rev. 2019, 32, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Butt, M.S.; Sultan, M.T. Coffee and its Consumption: Benefits and Risks. Crit. Rev. Food Sci. Nutr. 2011, 51, 363–373. [Google Scholar] [CrossRef]
- Chieng, D.; Kistler, P.M. Coffee and tea on cardiovascular disease (CVD) prevention. Trends Cardiovasc. Med. 2022, 32, 399–405. [Google Scholar] [CrossRef]
- Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ott. Ott. Hosp. Res. Inst. 2011, 2, 1–12. [Google Scholar]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. Newcastle-Ottawa Quality Assessment Scale Cohort Studies; University of Ottawa: Ottawa, ON, Canada, 2014. [Google Scholar]
- Zhang, J.; Yu, K.F. What’s the relative risk? A method of correcting the odds ratio in cohort studies of common outcomes. JAMA 1998, 280, 1690–1691. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Flack, J.M.; Adekola, B. Blood pressure and the new ACC/AHA hypertension guidelines. Trends Cardiovasc. Med. 2020, 30, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Smith, G.D.; Altman, D. Systematic Reviews in Health Care: Meta-Analysis in Context, 2nd ed.; BMJ Publishing Group: London, UK, 2001. [Google Scholar]
- Barré, T.; Fontaine, H.; Pol, S.; Ramier, C.; Di Beo, V.; Protopopescu, C.; Marcellin, F.; Bureau, M.; Bourlière, M.; Dorival, C.; et al. Metabolic Disorders in Patients with Chronic Hepatitis B Virus Infection: Coffee as a Panacea? (ANRS CO22 Hepather Cohort). Antioxidants 2022, 11, 379. [Google Scholar] [CrossRef]
- Miranda, A.M.; Goulart, A.C.; Benseñor, I.M.; Lotufo, P.A.; Marchioni, D.M. Coffee consumption and risk of hypertension: A prospective analysis in the cohort study. Clin. Nutr. 2021, 40, 542–549. [Google Scholar] [CrossRef]
- Micek, A.; Godos, J.; Cernigliaro, A.; Cincione, R.I.; Buscemi, S.; Libra, M.; Galvano, F.; Grosso, G. Polyphenol-Rich and Alcoholic Beverages and Metabolic Status in Adults Living in Sicily, Southern Italy. Foods 2021, 10, 383. [Google Scholar] [CrossRef]
- Hou, C.C.; Tantoh, D.M.; Lin, C.C.; Chen, P.H.; Yang, H.J.; Liaw, Y.P. Association between hypertension and coffee drinking based on CYP1A2 rs762551 single nucleotide poly-morphism in Taiwanese. Nutr. Metab. 2021, 18, 78. [Google Scholar] [CrossRef]
- Villaverde, P.; Lajous, M.; Macdonald, C.-J.; Fagherazzi, G.; Bonnet, F.; Boutron-Ruault, M.-C. High dietary total antioxidant capacity is associated with a reduced risk of hypertension in French women. Nutr. J. 2019, 18, 31. [Google Scholar] [CrossRef]
- Navarro, A.; Martinez-Gonzalez, M.; Gea, A.; Ramallal, R.; Ruiz-Canela, M.; Toledo, E. Coffee consumption and risk of hypertension in the SUN Project. Clin. Nutr. 2019, 38, 389–397. [Google Scholar] [CrossRef]
- Gaeini, Z.; Bahadoran, Z.; Mirmiran, P.; Azizi, F. Tea, coffee, caffeine intake and the risk of cardio-metabolic outcomes: Findings from a population with low coffee and high tea consumption. Nutr. Metab. 2019, 16, 28. [Google Scholar] [CrossRef]
- Stutz, B.; Ahola, A.; Harjutsalo, V.; Forsblom, C.; Groop, P.-H. Association between habitual coffee consumption and metabolic syndrome in type 1 diabetes. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 470–476. [Google Scholar] [CrossRef] [PubMed]
- Micek, A.; Grosso, G.; Polak, M.; Kozakiewicz, K.; Tykarski, A.; Walczak, A.P.; Drygas, W.; Kwaśniewska, M.; Pająk, A. Association between tea and coffee consumption and prevalence of metabolic syndrome in Poland—results from the WOBASZ II study (2013–2014). Int. J. Food Sci. Nutr. 2018, 69, 358–368. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.W.; Shin, D. A Healthy Beverage Consumption Pattern Is Inversely Associated with the Risk of Obesity and Metabolic Abnormalities in Korean Adults. J. Med. Food 2018, 21, 935–945. [Google Scholar] [CrossRef] [PubMed]
- Chei, C.-L.; Loh, J.K.; Soh, A.; Yuan, J.-M.; Koh, W.-P. Coffee, tea, caffeine, and risk of hypertension: The Singapore Chinese Health Study. Eur. J. Nutr. 2018, 57, 1333–1342. [Google Scholar] [CrossRef]
- Grosso, G.; Stepaniak, U.; Polak, M.; Micek, A.; Topor-Madry, R.; Stefler, D.; Szafraniec, K.; Pajak, A. Coffee consumption and risk of hypertension in the Polish arm of the HAPIEE cohort study. Eur. J. Clin. Nutr. 2016, 70, 109–115. [Google Scholar] [CrossRef]
- Grosso, G.; Stepaniak, U.; Micek, A.; Topor-Mądry, R.; Pikhart, H.; Szafraniec, K.; Pająk, A. Association of daily coffee and tea consumption and metabolic syndrome: Results from the Polish arm of the HAPIEE study. Eur. J. Nutr. 2015, 54, 1129–1137. [Google Scholar] [CrossRef]
- Takami, H.; Nakamoto, M.; Uemura, H.; Katsuura, S.; Yamaguchi, M.; Hiyoshi, M.; Sawachika, F.; Juta, T.; Arisawa, K. Inverse Correlation Between Coffee Consumption and Prevalence of Metabolic Syndrome: Baseline Survey of the Japan Multi-Institutional Collaborative Cohort (J-MICC) Study in Tokushima, Japan. J. Epidemiol. 2013, 23, 12–20. [Google Scholar] [CrossRef]
- Guessous, I.; Dobrinas, M.; Kutalik, Z.; Pruijm, M.; Ehret, G.; Maillard, M.; Bergmann, S.; Beckmann, J.S.; Cusi, D.; Rizzi, F.; et al. Caffeine intake and CYP1A2 variants associated with high caffeine intake protect non-smokers from hy-pertension. Hum. Mol. Genet. 2012, 21, 3283–3292. [Google Scholar] [CrossRef]
- Uhernik, A.I.; Erceg, M.; Milanović, S.M. Association of BMI and nutritional habits with hypertension in the adult popu-lation of Croatia. Public Health Nutr. 2009, 12, 97–104. [Google Scholar] [CrossRef]
- Kokaze, A.; Ishikawa, M.; Matsunaga, N.; Karita, K.; Yoshida, M.; Ohtsu, T.; Shirasawa, T.; Sekii, H.; Ito, T.; Kawamoto, T.; et al. NADH Dehydrogenase Subunit-2 237 Leu/Met Polymorphism Modulates the Effects of Coffee Consumption on the Risk of Hypertension in Middle-Aged Japanese Men. J. Epidemiol. 2009, 19, 231–236. [Google Scholar] [CrossRef]
- Uiterwaal, C.S.; Verschuren, W.M.; Bueno-De-Mesquita, H.B.; Ocké, M.; Geleijnse, J.M.; Boshuizen, H.C.; Peeters, P.H.; Feskens, E.J.; Grobbee, D.E. Coffee intake and incidence of hypertension. Am. J. Clin. Nutr. 2007, 85, 718–723. [Google Scholar] [CrossRef] [PubMed]
- Hu, G.; Jousilahti, P.; Nissinen, A.; Bidel, S.; Antikainen, R.; Tuomilehto, J. Coffee consumption and the incidence of antihypertensive drug treatment in Finnish men and women. Am. J. Clin. Nutr. 2007, 86, 457–464. [Google Scholar] [CrossRef] [PubMed]
- Winkelmayer, W.C.; Stampfer, M.J.; Willett, W.C.; Curhan, G.C. Habitual Caffeine Intake and the Risk of Hypertension in Women. JAMA 2005, 294, 2330–2335. [Google Scholar] [CrossRef] [PubMed]
- Klag, M.; Wang, N.; Meoni, L. Coffee intake and risk of hypertension. The Johns Hopkins precursors study. Arch. Intern. Med. 2002, 162, 657–662. [Google Scholar] [CrossRef]
- Tan, L.-J.; Jeon, H.J.; Park, S.; Kim, S.-A.; Lim, K.; Chung, S.; Chang, P.-S.; Lee, J.-K.; Kang, D.; Shin, S. Association of Coffee Consumption and Its Types According to Addition of Sugar and Creamer with Metabolic Syndrome Incidence in a Korean Population from the Health Examinees (HEXA) Study. Nutrients 2021, 13, 920. [Google Scholar] [CrossRef]
- Nina, R.; Lingling, H.; Qiushuang, L.; Honglin, G.; Liyuan, S.; Yuting, Z. Association of coffee consumption pattern and metabolic syndrome among middle-aged and older adults: A cross-sectional study. Front. Public Health 2023, 11, 1022616. [Google Scholar] [CrossRef]
- An, H.-J.; Kim, Y.; Seo, Y.-G. Relationship between Coffee, Tea, and Carbonated Beverages and Cardiovascular Risk Factors. Nutrients 2023, 15, 934. [Google Scholar] [CrossRef]
- Rhee, J.J.; Qin, F.; Hedlin, H.K.; Chang, T.I.; Bird, C.E.; Zaslavsky, O.; Manson, J.E.; Stefanick, M.L.; Winkelmayer, W.C. Coffee and caffeine consumption and the risk of hypertension in postmenopausal women. Am. J. Clin. Nutr. 2016, 103, 210–217. [Google Scholar] [CrossRef]
- Grosso, G.; Micek, A.; Godos, J.; Pajak, A.; Sciacca, S.; Bes-Rastrollo, M.; Galvano, F.; Martinez-Gonzalez, M.A. Long-Term Coffee Consumption Is Associated with Decreased Incidence of New-Onset Hypertension: A Dose–Response Meta-Analysis. Nutrients 2017, 9, 890. [Google Scholar] [CrossRef]
- Xie, C.; Cui, L.; Zhu, J.; Wang, K.; Sun, N.; Sun, C. Coffee consumption and risk of hypertension: A systematic review and dose–response meta-analysis of cohort studies. J. Hum. Hypertens. 2018, 32, 83–93. [Google Scholar] [CrossRef]
- Han, M.; Oh, Y.; Myung, S.-K. Coffee Intake and Risk of Hypertension: A Meta-Analysis of Cohort Studies. J. Korean Med. Sci. 2022, 37, e332. [Google Scholar] [CrossRef]
- Guessous, I.; Eap, C.B.; Bochud, M. Blood Pressure in Relation to Coffee and Caffeine Consumption. Curr. Hypertens. Rep. 2014, 16, 468. [Google Scholar] [CrossRef] [PubMed]
- Emami, M.R.; Safabakhsh, M.; Alizadeh, S.; Asbaghi, O.; Khosroshahi, M.Z. Effect of vitamin E supplementation on blood pressure: A systematic review and meta-analysis. J. Hum. Hypertens. 2019, 33, 499–507. [Google Scholar] [CrossRef] [PubMed]
- Zeman, M.; Vecka, M.; Perlík, F.; Staňková, B.; Hromádka, R.; Tvrzická, E.; Širc, J.; Hrib, J.; Žák, A. Pleiotropic effects of niacin: Current possibilities for its clinical use. Acta Pharm. 2016, 66, 449–469. [Google Scholar] [CrossRef]
- Santos, R.M.M.; Lima, D.R.A. Coffee consumption, obesity and type 2 diabetes: A mini-review. Eur. J. Nutr. 2016, 55, 1345–1358. [Google Scholar] [CrossRef]
- Schwartz, S.M. Smooth muscle proliferation in hypertension. State-of-the-art lecture. Hypertension 1984, 6, I56–I61. [Google Scholar] [CrossRef]
- Fisher, J.P.; Paton, J.F.R. The sympathetic nervous system and blood pressure in humans: Implications for hypertension. J. Hum. Hypertens. 2012, 26, 463–475. [Google Scholar] [CrossRef]
- Godos, J.; Pluchinotta, F.R.; Marventano, S.; Buscemi, S.; Li Volti, G.; Galvano, F.; Grosso, G. Coffee components and cardiovascular risk: Beneficial and detrimental effects. Int. J. Food Sci. Nutr. 2014, 65, 925–936. [Google Scholar] [CrossRef]
- Ardiansyah; Ohsaki, Y.; Shirakawa, H.; Koseki, T.; Komai, M. Novel effects of a single administration of ferulic acid on the regulation of blood pressure and the hepatic lipid metabolic profile in stroke-prone spontaneously hypertensive rats. J. Agric. Food Chem. 2008, 56, 2825–2830. [Google Scholar] [CrossRef]
- Suzuki, A.; Kagawa, D.; Fujii, A.; Ochiai, R.; Tokimitsu, I.; Saito, I. Short- and long-term effects of ferulic acid on blood pressure in spontaneously hypertensive rats. Am. J. Hypertens. 2002, 15, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Khaledi, M.; Haghighatdoost, F.; Feizi, A.; Aminorroaya, A. The prevalence of comorbid depression in patients with type 2 diabetes: An updated systematic review and meta-analysis on huge number of observational studies. Acta Diabetol. 2019, 56, 631–650. [Google Scholar] [CrossRef] [PubMed]
- Palatini, P.; Ceolotto, G.; Ragazzo, F.; Dorigatti, F.; Saladini, F.; Papparella, I.; Mos, L.; Zanata, G.; Santonastaso, M. CYP1A2 genotype modifies the association between coffee intake and the risk of hypertension. J. Hypertens. 2009, 27, 1594–1601. [Google Scholar] [CrossRef] [PubMed]
- Kang, M.; Ragan, B.G.; Park, J.-H. Issues in Outcomes Research: An Overview of Randomization Techniques for Clinical Trials. J. Athl. Train. 2008, 43, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Brezová, V.; Šlebodová, A.; Staško, A. Coffee as a source of antioxidants: An EPR study. Food Chem. 2009, 114, 859–868. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| First Author (Year) | Study Location/Setting | Sex/Age Range or Mean (Year) | Case/Total | Duration Follow-Up (Year) | Outcome Assessment/HTN Definition | Coffee Intake Assessment | Type of Coffee | Report of Coffee Intake | OR or RR or HR (95% CI) | Quality Assessment | Adjustments |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Klag (2002) [46] | USA | M/26 years | 281/1017 | 33 years | Self-report/≥160/≥95 mmHg | Questionnaire | Caffeinated | Coffee >5 vs. 0 cups/day | RR (95% CI) 1.07 (0.67–1.69) | 6 | Parental history of HTN, smoking, alcohol, physical activity, and BMI |
| Winkelmayer (2005) [45] | USA/NHS I and II | F/25–55 years | NHS I: 18,955/53,175 NHS II: 13,468/87,369 | 12 years NHS I: 1990–2002 and NSH II: 1991–2003 | Self-reported diagnosis of HTN/≥140/≥90 mmHg | FFQ | Caffeinated and decaffeinated | Caffeinated coffee ≥6 vs. <1 cup/d | Caffeinated: RR (95% CI) NHS I: 0.88 (0.80–0.98) NSH II: 0.91 (0.80–1.04) | 6 | Age, BMI, alcohol, family history of HTN, oral contraceptive use (in Nurses’ Health Study II only), physical activity, and smoking |
| Hu (2007) [44] | Finland | M/F/25–64 years | 2505/24,710 | 13.2 years | Self-reported initiation of antihypertensive drug treatment/Incidence of antihypertensive drug | FFQ/Questionnaire | NR | Coffee ≥8 vs. 0–1 cups/day | HR (95% CI) 1.13 (0.94–1.36) | 7 | Age, sex, study year, education, physical activity, smoking, alcohol, tea, frequency of vegetable, fruit, sausage, and bread consumption, BMI, history of diabetes, total cholesterol and baseline SBP |
| Uiterwall (2007) [43] | USA | M/F/Men: 40.7 ± 10.0 Women: 40.1 ± 10.3 | 956/5189 | 11 years | Measurement/≥140/≥90 mmHg | Questionnaire | Regular, decaffeinated or other | All type of coffees: >6 vs. 0 cups/day | Coffee: OR (95% CI) All: 0.83 (0.65–1.07) Men: 1.03 (0.72–1.46) Women: 0.67 (0.46–0.98) | 8 | Age, sex, BMI smoking, alcohol, tea, education level, occupational status, and total energy intake. |
| Grosso (2016) [37] | Poland/HAPIEE project | M/F/45–69 years | 1735/2725 | 5 years | Measurement/>139/>89 mmHg | FFQ | NR but mostly caffeinated | Coffee >4 vs. <1 cups/day | OR (95% CI) All: 1.58 (0.85–3.64) Men: 2.42 (0.66–8.91) Women: 1.09 (0.36–3.33) | 7 | Age, sex, education, occupation, BMI, alcohol, smoking, physical activity, history of CVD, diabetes at baseline, cholesterol therapy at baseline, total energy intake, vitamin supplement use, oral contraceptives use, sodium and potassium intakes |
| Rhee (2016) [50] | USA/The Women’s Health Initiative Observational Study | F/50–79 years | 5566/29,985 | - | Measurement/≥140/≥90 mmHg | FFQ | Caffeinated and decaffainated | Caffeinated and decaffeinated: ≥4 vs. 0 cups/day | Caffeinated: HR (95% CI) 0.99 (0.90–1.08) | 7 | Age, baseline blood pressure, BMI, physical activity, hormone replacement therapy, alcohol consumption, smoking, total caloric intake, and intakes of sodium, magnesium, calcium, potassium, and phosphorus as time-varying covariates. |
| Chei (2018) [36] | Singapore/The Singapore Chinese Health Study | M/F/45–74 years | 13,658/38,592 | 9.5 years | Self-report/- | FFQ | Caffeinated | Categorized Coffee ≥3 vs. 1 cups/day | HR (95% CI) 0.93 (0.86–1.00) | 7 | Age at recruitment (years), year of recruitment, sex, dialect group, BMI, education level, smoking, physical activity, sleep duration, and dietary intake of sodium, vegetables, fruits, and dairy products |
| Gaeini (2019) [32] | Iran/TLGS | M/F/≥19 years | 291/1878 | 6 years | Measuring/≥140/≥90 mmHg or self-reported usage of blood pressure lowering medications | FFQ | NR | Coffee Drinkers vs. non-drinkers | HR (95% CI) 0.83 (0.63–1.10) | 7 | Sex, age, BMI, Triglyceride to HDL-C ratio, total energy intake |
| Navarro (2019) [31] | Spain/The SUN Project | M/F/35.7 ± 10.4 | 1750/13,369 | 9.1 years | Questionnaires/≥140/≥90 mmHg | FFQ | Regular and decaffeinated coffee | Caffeinated and decaffeinated coffee: ≥2 vs. 0 cups/day | HR (95% CI) 0.86 (0.75–0.99) | 6 | Age, BMI, alcohol, smoking and package-years of smoking, family history of HTN, sodium intake, whole and low fat dairy products consumption, sugar-sweetened beverages, non-sugared carbonated beverages, physical activity, adherence to Mediterranean diet, kind of personality), time spent watching TV and fried and fast-food consumption |
| Villaverde (2019) [30] | France/E3N | F/51.6 ± 6.2 | 9350/40,567 | 12.7 years | Questionnaire/- | Diet history questionnaire | NR | TAC (mmol/day) Quantile 5 vs. quantile 1 | HR (95% CI) 0.91 (0.80; 1.04) | 7 | Age as the time scale, energy without alcohol, diabetes, treated hypercholesterolemia, education, family history of HTN, smoking, physical activity, BMI, Na, K, Mg, AGPIw3, alcohol |
| Miranda (2021) [27] | Brazil/ELSA | M/F/35–74 years | 1285/8780 | 3.9 years | Measuring/≥140/≥90 mmHg And/or taking anti-hypertensive medications | FFQ | Caffeinated coffee | Coffee >3 vs. ≤1 cups/day | RR (95% CI) 0.85 (0.70–1.04) | 6 | Age, sex, race/skin color, educational attainment, household per capita income, BMI, physical activity level, smoking, alcohol, dietary intake of fruits, vegetables, sodium, potassium, saturated fat, added sugars, total energy intake, supplement use, fasting glucose, total cholesterol, and triglycerides |
| Tan (2021) [47] | Japan/HEXA | M/F/≥40 years | 3897 | 5 | Measurement/≥130/≥80 mmHg | FFQ | NR | Coffee >3 vs. 0 cups/day | RR (95% CI) 0.85 (0.64, 1.15) | 7 | Age, BMI, energy intake, educational level, current drinking status, current smoking status, and physical activity |
| First Author (year) | Study Location/Setting | Age Range/Mean Age (year) | Case/Total | Outcome Assessment | Coffee Intake Assessment | Type of Coffee | Report of Coffee Intake | OR or RR or HR (95% CI) | Quality Assessment | Adjustments |
|---|---|---|---|---|---|---|---|---|---|---|
| Kokaze (2009) [42] | Japan | M/53.8 ± 7.8 years | 398 | Measurement/≥140/≥90 mmHg | Questionnaire | NR | Coffee > 4 vs. ≤1 cups/day | OR ≤1: 1 2–3: 0.56 (0.34–1.01) >4: 0.58 (0.23–1.45) | 6 | Age, BMI, alcohol, smoking, serum total cholesterol level, serum HDL level, fasting plasma glucose level, serum uric acid level, and green tea. |
| Uhernik (2008) [41] | Croatia | M/F/>18 years | 10,766 | Measurement/≥140/≥90 mmHg | Questionnaire | NR | Coffee ≥3 vs. 0 cups/day | OR (95% CI) All: 0.6 (0.5–0.8) Men: 0.5 (0.3–0.7) Women: 1.1 (0.8–1.6) | 6 | - |
| Guessous (2012) [40] | Switzerland/The CoLaus study | M/35–75 years | 6127/ Non-smokers: 4480 Smokers: 1647 | Measurement/≥140/≥90 mmHg | Questionnaire | NR | Coffee >6 vs. 0 cups/day | OR (95% CI) Non-smokers 0.59 (0.34–1.02) Smokers: 0.96 (0.38–2.42) | 8 | Age, sex, BMI, contraceptive use, total cholesterol, triglycerides, diabetes, alcohol, CKD-EPI, CYP1A2 variants, menopause and p-value for interaction test. |
| Takami (2013) [39] | Japan/the Japan Multi-Institutional Collaborative Cohort (J-MICC) Study | M/F/35–70 years | 172/554 | Measurement/≥130/≥85 mmHg | Questionnaire | NR | Rarely <2, 3–4 and 5–6 cups/week 1–2, 3–4 and ≥5 cups/day | OR (95% CI) <1.5: 1 ≥1.5 and <3: 0.89 (0.55–1.45) ≥3: 0.82 (0.49–1.36) | 8 | Age, sex, total energy intake, physical activity, smoking and drinking habits |
| Grosso (2015) [38] | Poland/arm of the HAPPIE study | M/F/45–69 years | 8821 | Measurement/≥130/≥85 mmHg | FFQ | NR | Coffee ≥2 vs. <1 cups/day | OR (95% CI) All: 0.78 (0.69–0.88) Men: 0.88 (0.74–1.06) Women: 0.78 (0.65–0.95) | 8 | Sex, age, educational level, occupational level, physical activity, smoking, alcohol, total energy intake, and tea consumption |
| Lee (2018) [35] | Korea | M/F/19–64 years | 15,713 | Measurement/≥130/≥85 mmHg | 24-h dietary recall | NR | Coffee pattern T3 vs. T1 | OR (95% CI) 0.97 (0.87–1.09) | 7 | Sex, age, education level, income, smoking, physical activity, BMI (except for obesity and abdominal obesity), day of recalled intake; total daily energy intake. |
| Micek (2018) [34] | Poland | M/F/≥20 years | 5164 | Measurement/≥130/≥85 mmHg or treatment of previously diagnosed HTN | 24-h dietary recall | NR | Coffee >400 vs. 0 g/day | OR (95% CI) 0.74 (0.60–0.92) | 8 | Sex, age, educational and occupational status, physical activity, smoking, alcohol, total energy intake, and tea consumption |
| Stutz (2018) [33] | Finland/the Finish Diabetic Nephropathy Study | M/F/46.7 ± 0.4 | 1040 | Measurement/≥130/≥85 mmHg or use of hypertensive medication | FFQ | NR | Coffee ≥5 vs. <1 cup/d | OR (95% CI) 2.19 (1.08–4.44) | 8 | Age, sex, energy intake, alcohol, physical activity, and smoking |
| Hou (2021) [29] | Taiwan/Biobank database | M/F/30–70 years | 3411/19,133 | Questionnaire/- | Self-reports | NR | Coffee drinkers (at least thrice per week) vs. non-drinkers (habitually drank coffee less than three times per week) | OR (95% CI) 0.877(0.807–0.954) | 5 | - |
| Micek (2021) [28] | Italy/MEAL | M/F/≥18 years | 2044 | Measurement/≥140/≥90 mmHg Or medical history of taking anti-hypertensive medications | FFQ | NR | Categorized T3 (67.6 ± 39.5 mL/d) vs. T1 (47.6 ± 51.9 mL/d) | OR (95% CI) 0.64 (0.48–0.86) | 9 | Total energy intake, all beverages investigated, age, sex, educational status, smoking, physical activity level, adherence to the Mediterranean diet |
| Barré (2022) [26] | France | M/F/43 ± 14.81 | 4590 | Self-report/Self-report or receiving treatment | Questionnaire | NR | Coffee ≥3 vs. 0 cups/day | OR (95% CI) 0.66 (0.51–0.85) | 6 | Age, sex, place of birth, living in a couple, tea, cannabis use, tobacco, alcohol, living in poverty |
| Hye-Ji An (2023) [49] | Korea/Korea National Health and Nutrition Examination Surveys | M/F/Men: 41.34 ± 0.15 Women: 42.39 ± 0.15 | 42,613 (17,311 men and 25,302 women) | Measurement/≥130/≥85 mmHg or medications | FFQ | NR | Coffee ≥1 time/d vs. <1 time/wk | OR (95% CI) Men: 0.66 (0.52, 0.84) Women: 0.92 (0.77, 1.11) | 9 | Age, the frequency of intake of tea, and carbonated beverages, daily nutritional intake (total and fat), income, education, smoking, alcohol drinking, walking, BMI, and menopausal status (only in women) |
| Nina R (2023) [48] | China | M/F/≥40 years | 1719 (800 men, 919 women) | Measurement/≥130/≥85 mmHg | 2-day, 24-h recall | NR | >1 serving/day vs. non-coffee drinkers | OR (95% CI) Men: 0.88 (0.72, 1.08) Women: 0.79 (0.60, 1.04) | 9 | BMI, education level, alcohol status, Physical activity |
| Number of Effects | Effect Size | 95% Confidence Interval | I2 (%) | p-for between Subgroup Heterogeneity | |
|---|---|---|---|---|---|
| Cohorts | |||||
| Region | 0.924 | ||||
| US | 6 | 0.92 | 0.87, 0.97 | 0.7 | |
| Europe | 4 | 0.97 | 0.83, 1.13 | 60.5 | |
| Asia | 3 | 0.94 | 0.83, 1.07 | 25.0 | |
| Age | 0.444 | ||||
| <50 years | 7 | 0.91 | 0.84, 0.99 | 23.8 | |
| >50 years | 6 | 0.94 | 0.89, 1.00 | 28.5 | |
| Sample size | 0.244 | ||||
| <median (n = 20,000) | 7 | 0.89 | 0.81, 0.99 | 12.6 | |
| >median (n = 20,000) | 6 | 0.94 | 0.84, 0.99 | 30.8 | |
| Number of cases | 0.967 | ||||
| <3000 | 8 | 0.94 | 0.84, 1.06 | 43.0 | |
| >3000 | 5 | 0.93 | 0.89, 0.97 | 0.0 | |
| Follow-up duration | 0.506 | ||||
| <10 years | 6 | 0.91 | 0.84, 0.99 | 22.3 | |
| >10 years | 7 | 0.94 | 0.88, 1.00 | 30.0 | |
| Sex | 0.833 | ||||
| Men | 1 | 1.07 | 0.67, 1.70 | - | |
| Women | 4 | 0.93 | 0.88, 0.98 | 4.9 | |
| Both | 8 | 0.93 | 0.85, 1.02 | 41.3 | |
| HTN stage | 0.149 | ||||
| ≥130 mmHg for SBP and/or 80 mmHg for DBP | 1 | 1.19 | 0.85, 1.65 | - | |
| ≥140 mmHg for SBP and/or 90 mmHg for DBP | 12 | 0.92 | 0.88, 0.97 | 17.7 | |
| Study quality | 0.056 | ||||
| Low | 5 | 0.88 | 0.83, 0.94 | 0.0 | |
| High | 8 | 0.96 | 0.90, 1.03 | 34.2 | |
| Cross-sectionals | |||||
| Region | <0.0001 | ||||
| Europe | 8 | 0.72 | 0.62, 0.84 | 54.6 | |
| Asia | 8 | 0.87 | 0.81, 0.95 | 33.3 | |
| Sample size | 0.078 | ||||
| <median (n = 8000) | 8 | 0.78 | 0.66, 0.91 | 48.5 | |
| >median (n = 8000) | 8 | 0.81 | 0.72, 0.90 | 70.9 | |
| Sample size | 0.733 | ||||
| <median (n = 3000) | 7 | 0.84 | 0.67, 1.04 | 47.3 | |
| >median (n = 3000) | 9 | 0.78 | 0.70, 0.87 | 72.6 | |
| Sex | 0.423 | ||||
| Men | 4 | 0.75 | 0.61, 0.93 | 31.4 | |
| Women | 2 | 0.88 | 0.75, 1.02 | 0.0 | |
| Both | 10 | 0.79 | 0.70, 0.89 | 73.4 | |
| HTN stage | 0.154 | ||||
| ≥130 mmHg for SBP and/or 80 mmHg for DBP | 5 | 0.88 | 0.73, 1.06 | 75.2 | |
| ≥140 mmHg for SBP and/or 90 mmHg for DBP | 11 | 0.76 | 0.68, 0.85 | 55.7 | |
| Study quality | 0.637 | ||||
| Low | 4 | 0.71 | 0.55, 0.91 | 77.0 | |
| High | 12 | 0.82 | 0.73, 0.91 | 59.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haghighatdoost, F.; Hajihashemi, P.; de Sousa Romeiro, A.M.; Mohammadifard, N.; Sarrafzadegan, N.; de Oliveira, C.; Silveira, E.A. Coffee Consumption and Risk of Hypertension in Adults: Systematic Review and Meta-Analysis. Nutrients 2023, 15, 3060. https://doi.org/10.3390/nu15133060
Haghighatdoost F, Hajihashemi P, de Sousa Romeiro AM, Mohammadifard N, Sarrafzadegan N, de Oliveira C, Silveira EA. Coffee Consumption and Risk of Hypertension in Adults: Systematic Review and Meta-Analysis. Nutrients. 2023; 15(13):3060. https://doi.org/10.3390/nu15133060
Chicago/Turabian StyleHaghighatdoost, Fahimeh, Parisa Hajihashemi, Amanda Maria de Sousa Romeiro, Noushin Mohammadifard, Nizal Sarrafzadegan, Cesar de Oliveira, and Erika Aparecida Silveira. 2023. "Coffee Consumption and Risk of Hypertension in Adults: Systematic Review and Meta-Analysis" Nutrients 15, no. 13: 3060. https://doi.org/10.3390/nu15133060
APA StyleHaghighatdoost, F., Hajihashemi, P., de Sousa Romeiro, A. M., Mohammadifard, N., Sarrafzadegan, N., de Oliveira, C., & Silveira, E. A. (2023). Coffee Consumption and Risk of Hypertension in Adults: Systematic Review and Meta-Analysis. Nutrients, 15(13), 3060. https://doi.org/10.3390/nu15133060