
Antihypertensive and Vasorelaxant Effects of Citric Acid and Lemon Juice in Spontaneously Hypertensive Rats: In Vivo and Ex Vivo Studies

Abstract
:1. Introduction
2. Materials and Methods
2.1. Reagents and Materials
2.2. Animals and Ethics Statement
2.3. Single Oral Administration Test
2.3.1. Administration Test for Citric Acid and Lemon Juice
2.3.2. Administration Test for AFR-Lemon Juice
2.3.3. Citric Acid Hemodynamics in SHRs
2.4. Aorta Assay
2.5. Statistical Analysis
3. Results
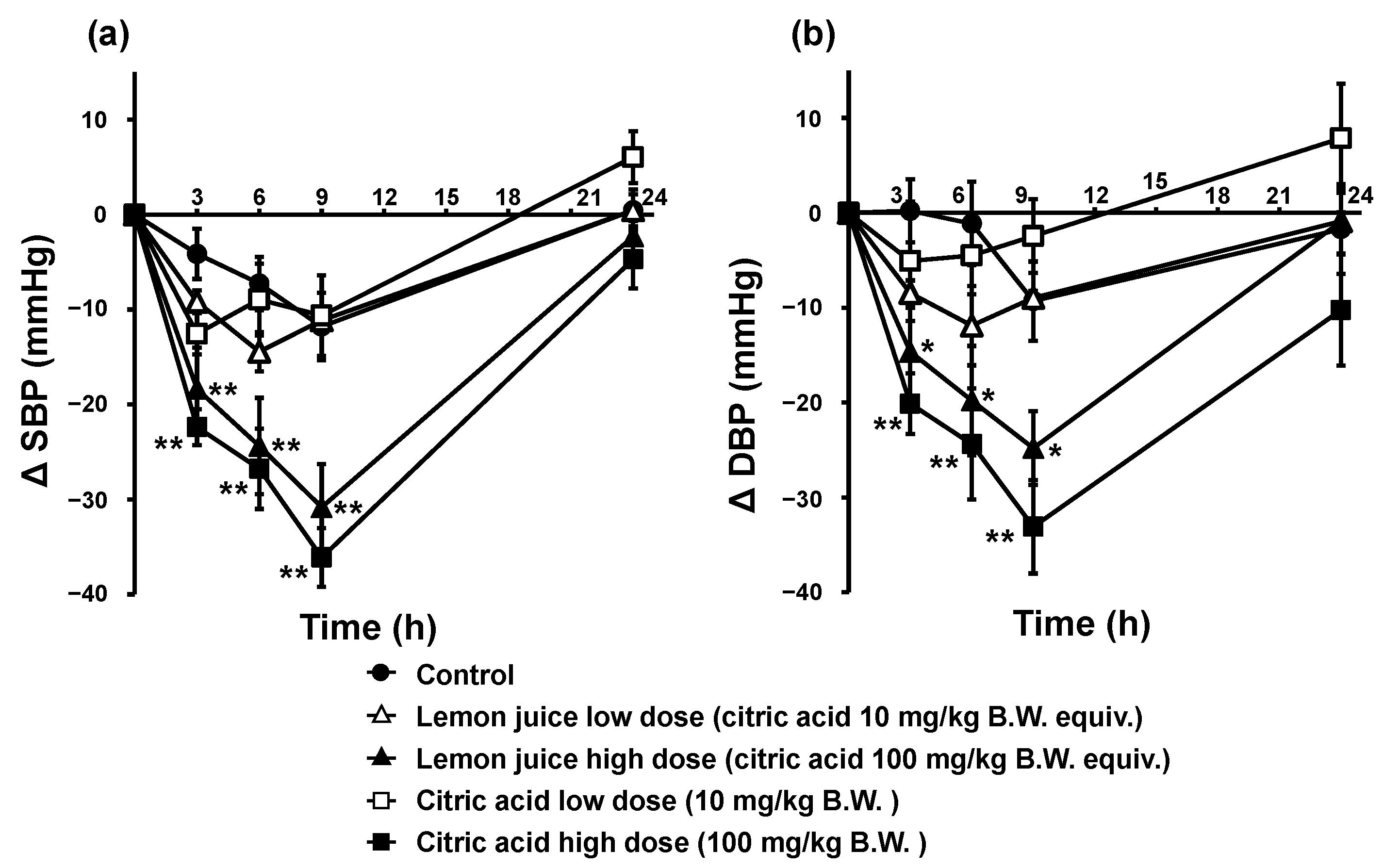
3.1. Antihypertensive Effects of Citric Acid and Lemon Juice
3.1.1. Blood Pressure-Lowering Effects of a Single Oral Administration of Citric Acid and Lemon Juice
3.1.2. Citric Acid Hemodynamics
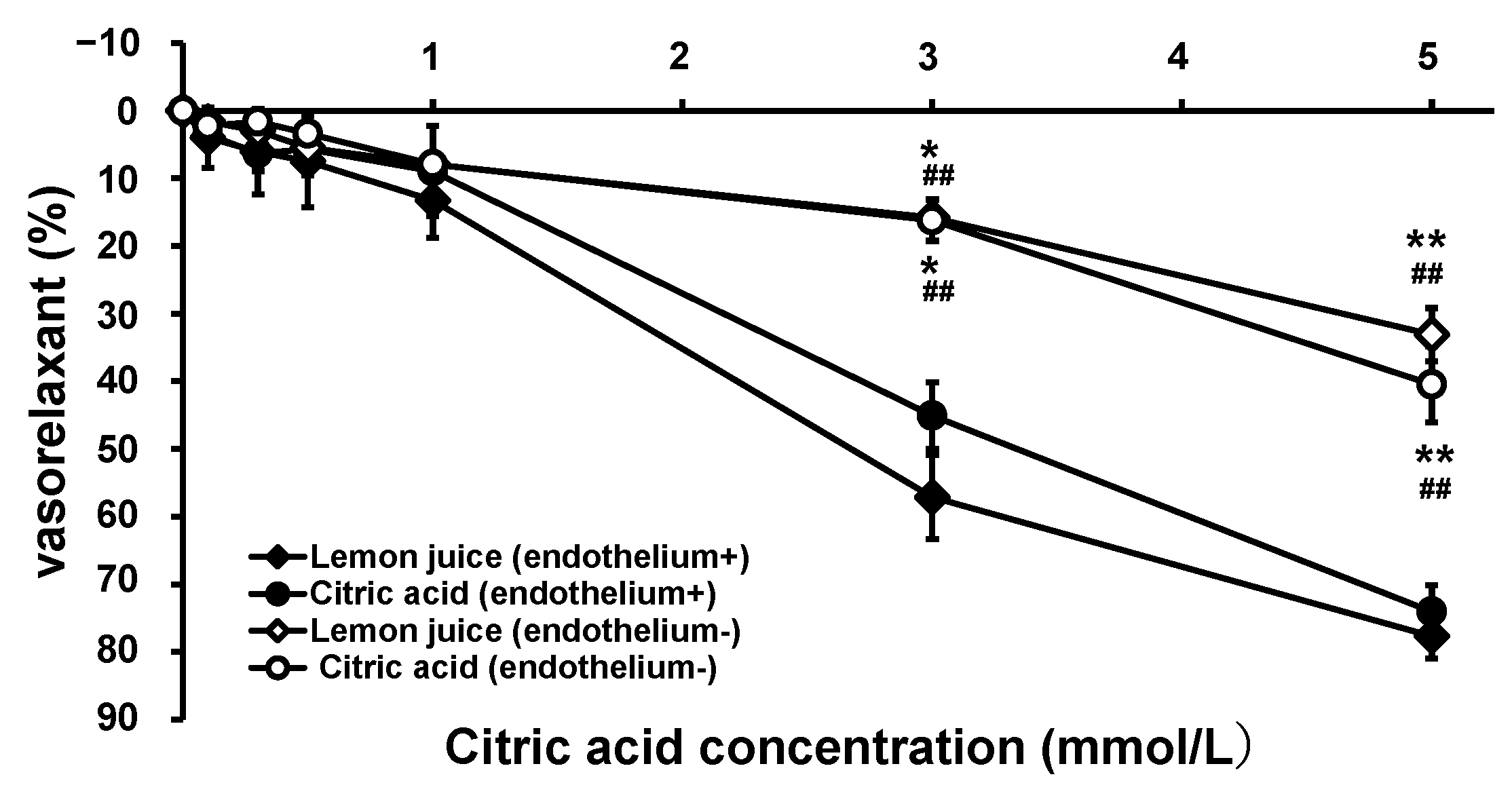
3.2. Vascular Effects of Citric Acid and Lemon Juice
3.2.1. Vasorelaxation Effects of Citric Acid and Lemon Juice in Endothelium-Intact and -Removed Aorta
3.2.2. Effect of pH on Vasorelaxation
3.2.3. Vasorelaxation with Citric Acid and Lemon Juice in KCl-Contracted Aortae from SHRs
3.3. Single Oral Administration Tests and Aorta Assay for Testing the Effects of AFR-Lemon Juice
4. Discussion
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO). Guideline for the Pharmacological Treatment of Hypertension in Adults. WHO. 2021. Available online: https://apps.who.int/iris/bitstream/handle/10665/344424/9789240033986-eng.pdf (accessed on 27 July 2023).
- Mancia, G.; Kreutz, R.; Brunström, M.; Burnier, M.; Grassi, G.; Januszewicz, A.; Muiesan, M.L.; Tsioufis, K.; Agabiti-Rosei, E.; Algharably, E.A.E.; et al. 2023 ESH Guidelines for the management of arterial hypertension The Task Force for the management of arterial hypertension of the European Society of Hypertension Endorsed by the European Renal Association (ERA) and the International Society of Hypertension (ISH). J. Hypertens. 2023. [Google Scholar] [CrossRef]
- Appel, L.J.; Moore, T.J.; Obarzanek, E.; Vollmer, W.M.; Svetkey, L.P.; Sacks, F.M.; Bray, G.A.; Vogt, T.M.; Cutler, J.A.; Windhauser, M.M.; et al. A clinical trial of the effects of dietary patterns on blood pressure. DASH Collaborative Research Group. N. Engl. J. Med. 1997, 336, 1117–1124. [Google Scholar] [CrossRef]
- John, J.H.; Ziebland, S.; Yudkin, P.; Roe, L.S.; Neil, H.A.W.; Oxford Fruit and Vegetable Study Group. Effects of fruit and vegetable consumption on plasma antioxidant concentrations and blood pressure: A randomised controlled trial. Lancet 2002, 359, 1969–1974. [Google Scholar] [CrossRef]
- Chen, Z.Y.; Peng, C.; Jiao, R.; Wong, Y.M.; Yang, N.; Huang, Y. Anti-hypertensive nutraceuticals and functional foods. J. Agric. Food Chem. 2009, 57, 4485–4499. [Google Scholar] [CrossRef] [PubMed]
- Ström, E.; Östgren, C.J.; Nystrom, F.H.; Wijkman, M.O. Associations between fruit consumption and home blood pressure in a randomly selected sample of the general Swedish population. J. Clin. Hypertens. 2022, 24, 723–730. [Google Scholar] [CrossRef]
- Elsahoryi, N.; Neville, C.; Patterson, C.; Linden, G.; Moitry, M.; Biasch, K.; Kee, F.; Amouyel, P.; Bongard, V.; Dallongeville, J.; et al. Association between overall fruit and vegetable intake, and fruit and vegetable sub-types and blood pressure: The PRIME study (Prospective Epidemiological Study of Myocardial Infarction). Br. J. Nutr. 2021, 125, 557–567. [Google Scholar] [CrossRef]
- FAOSTAT. Crops and Livestock Products. Available online: https://www.fao.org/faostat/en/#data/QCL (accessed on 24 March 2023).
- Adibelli, Z.; Dilek, M.; Akpolat, T. Lemon juice as an alternative therapy in hypertension in Turkey. Int. J. Cardiol. 2009, 135, e58–e59. [Google Scholar] [CrossRef]
- Kato, Y.; Domoto, T.; Hiramitsu, M.; Katagiri, T.; Sato, K.; Miyake, Y.; Aoi, S.; Ishihara, K.; Ikeda, H.; Umei, N.; et al. Effect on blood pressure of daily lemon ingestion and walking. J. Nutr. Metab. 2014, 2014, 912684. [Google Scholar] [CrossRef] [PubMed]
- Miyake, Y.; Kuzuya, K.; Ueno, C.; Katayama, N.i; Hayakawa, T.; Tsuge, H.; Osawa, T. Suppressive effect of components in lemon juice on blood pressure in spontaneously hypertensive rats. Food Sci. Tech. Int. 1998, 4, 29–32. [Google Scholar] [CrossRef]
- Ministry of Education, Culture, Sports, Science and Technology. Food Composition Database. Available online: https://fooddb.mext.go.jp/index.pl (accessed on 14 July 2023).
- Ministry of Education, Culture, Sports, Science and Technology. The Standard Tables of Food Composition in Japan 2020 (8th revision). Available online: https://www.mext.go.jp/a_menu/syokuhinseibun/mext_01110.html (accessed on 14 July 2023).
- Abdel-Salam, O.M.; Youness, E.R.; Mohammed, N.A.; Morsy, S.M.; Omara, E.A.; Sleem, A.A. Citric acid effects on brain and liver oxidative stress in lipopolysaccharide-treated mice. J. Med. Food. 2014, 17, 588–598. [Google Scholar] [CrossRef]
- Hamm, L.L.; Hering-Smith, K.S. Pathophysiology of hypocitraturic nephrolithiasis. Endocrinol. Metab. Clin. North Am. 2002, 31, 885–893. [Google Scholar] [CrossRef]
- He, F.J.; Markandu, N.D.; Coltart, R.; Barron, J.; MacGregor, G.A. Effect of short-term supplementation of potassium chloride and potassium citrate on blood pressure in hypertensives. Hypertension 2005, 45, 571–574. [Google Scholar] [CrossRef] [PubMed]
- Braschi, A.; Naismith, D. The effect of a dietary supplement of potassium chloride or potassium citrate on blood pressure in predominantly normotensive volunteers. Br. J. Nutr. 2008, 99, 1284–1292. [Google Scholar] [CrossRef]
- González-Molina, E.; Domínguez-Perles, R.; Moreno, D.A.; García-Viguera, C. Natural bioactive compounds of Citrus limon for food and health. J. Pharm. Biomed. Anal. 2010, 51, 327–345. [Google Scholar] [CrossRef]
- Whelton, P.K.; He, J.; Cutler, J.A.; Brancati, F.L.; Appel, L.J.; Follmann, D.; Klag, M.J. Effects of oral potassium on blood pressure, meta-analysis of randomised controlled clinical trials. JAMA 1997, 277, 1624–1632. [Google Scholar] [CrossRef] [PubMed]
- Cappuccio, F.P.; MacGregor, G.A. Does potassium supplementation lower blood pressure? A meta-analysis of published trials. J. Hypertens. 1991, 9, 465–473. [Google Scholar] [CrossRef] [PubMed]
- Sacks, F.M.; Svetkey, L.P.; Vollmer, W.M.; Appel, L.J.; Bray, G.A.; Harsha, D.; Obarzanek, E.; Conlin, P.R.; Miller, E.R., 3rd; Simons-Morton, D.G.; et al. Effects on blood pressure of reduced dietary sodium and the Dietary Approaches to Stop Hypertension (DASH) diet. N. Engl. J. Med. 2001, 344, 3–10. [Google Scholar] [CrossRef]
- Lin, P.H.; Aickin, M.; Champagne, C.; Craddick, S.; Sacks, F.M.; McCarron, P.; Most-Windhauser, M.M.; Rukenbrod, F.; Haworth, L.; Dash-Sodium Collaborative Research Group. Food group sources of nutrients in the dietary patterns of the DASH-Sodium trial. J. Am. Diet Assoc. 2003, 103, 488–496. [Google Scholar] [CrossRef] [PubMed]
- Elliott, P.; Stamler, J.; Nichols, R.; Dyer, A.R.; Stamler, R.; Kesteloot, H.; Marmot, M. Intersalt revisited: Further analyses of 24 hour sodium excretion and blood pressure within and across populations. BMJ 1996, 312, 1249–1253. [Google Scholar] [CrossRef]
- Tsai, C.C.; Lin, L.Y.; Chou, L.-C. The effects of lactic acid bacteria-fermented lemon juice on blood pressure regulation and allergic responses in rodents. ScienceAsia 2022, 48, 181–187. [Google Scholar] [CrossRef]
- Juraschek, S.P.; Guallar, E.; Appel, L.J.; Miller III, E.R. Effects of vitamin C supplementation on blood pressure: A meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2012, 95, 1079–1088. [Google Scholar] [CrossRef] [PubMed]
- Valls, R.M.; Pedret, A.; Calderon-Perez, L.; Llaurado, E.; Pla-Paga, L.; Companys, J.; Moragas, A.; Martin-Lujan, F.; Ortega, Y.; Giralt, M.; et al. Effects of hesperidin in orange juice on blood and pulse pressures in mildly hypertensive individuals: A randomized controlled trial (Citrus study). Eur. J. Nutr. 2021, 60, 1277–1288. [Google Scholar] [CrossRef] [PubMed]
- Inoue, K.; Shirai, T.; Ochiai, H.; Kasao, M.; Hayakawa, K.; Kimura, M.; Sansawa, H. Blood-pressure-lowering effect of a novel fermented milk containing γ-aminobutyric acid (GABA) in mild hypertensives. Eur. J. Clin. Nutr. 2003, 57, 490–495. [Google Scholar] [CrossRef]
- Yamaguchi, S.; Hayasaka, Y.; Suzuki, M.; Wang, W.; Koyama, M.; Nagasaka, Y.; Nakamura, K. Antihypertensive Mechanism of Orally Administered Acetylcholine in Spontaneously Hypertensive Rats. Nutrients 2022, 14, 905. [Google Scholar] [CrossRef]
- Yamaguchi, S.; Matsumoto, K.; Koyama, M.; Tian, S.; Watanabe, M.; Takahashi, A.; Miyatake, K.; Nakamura, K. Antihypertensive effects of orally administered eggplant (Solanum melongena) rich in acetylcholine on spontaneously hypertensive rats. Food Chem. 2019, 276, 376–382. [Google Scholar] [CrossRef]
- Sasahara, T.; Yayama, K.; Okamoto, H. Role of NO and K-V channels in the acidic pH-induced vasorelaxation in rat aorta (meeting abstract). J. Pharmacol. Sci. 2012, 118, 86. [Google Scholar]
- Kleiber, M. The Fire of Life. An Introduction to Animal Energetics; Wiley: New York, NY, USA, 1961. [Google Scholar]
- Yamamoto, M.; Suzuki, A.; Hase, T. Short-term effects of glucosyl hesperidin and hesperetin on blood pressure and vascular endothelial function in spontaneously hypertensive rats. J. Nutr. Sci. Vitaminol. 2008, 54, 95–98. [Google Scholar] [CrossRef]
- Yamaguchi, S.; Matsumoto, K.; Wang, W.; Nakamura, K. Differential antihypertensive effects of oral doses of acetylcholine between spontaneously hypertensive rats and normotensive rats. Foods 2021, 10, 2107. [Google Scholar] [CrossRef]
- Hayakawa, K.; Kimura, M.; Kasaha, K.; Matsumoto, K.; Sansawa, H.; Yamori, Y. Effect of a gamma-aminobutyric acid-enriched dairy product on the blood pressure of spontaneously hypertensive and normotensive Wistar-Kyoto rats. Br. J. Nutr. 2004, 92, 411–417. [Google Scholar] [CrossRef]
- Hara, Y.; Kume, S.; Kataoka, Y.; Watanabe, N. Changes in TCA cycle and TCA cycle-related metabolites in plasma upon citric acid administration in rats. Heliyon 2021, 7, e08501. [Google Scholar] [CrossRef] [PubMed]
- Quiñones, M.; Guerrero, L.; Fernández-Vallinas, S.; Pons, Z.; Arola, L.; Aleixandre, A.; Muguerza, B. Involvement of nitric oxide and prostacyclin in the antihypertensive effect of low-molecular-weight procyanidin rich grape seed extract in male spontaneously hypertensive rats. J. Funct. Foods 2014, 6, 419–427. [Google Scholar] [CrossRef]
- Duarte, J.; Pérez Vizcaíno, F.; Utrilla, P.; Jiménez, J.; Tamargo, J.; Zarzuelo, A. Vasodilatory effects of flavonoids in rat aortic smooth muscle. Structure-activity relationships. Gen. Pharmacol. 1993, 24, 857–862. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Lee, K.H.; Kang, W.S.; Kim, J.S.; Kim, S. Endothelium-dependent and endothelium-independent vasorelaxant effects of unripe Rubus coreanus Miq. And Dendropanax morbiferus H. Lév. Extracts on rat aortic rings. BMC Complement. Med. Ther. 2020, 20, 190. [Google Scholar] [CrossRef] [PubMed]
- Matoba, H.; Usui, H.; Fujita, H.; Yoshikawa, M. Novel anti-hypertensive peptide derived from ovalbumin induces nitric oxide-mediated vasorelaxation in an isolated SHR mesenteric artery. FEBS Lett. 1999, 452, 181–184. [Google Scholar] [CrossRef]
- Soff, G.A.; Cornwell, T.L.; Cundiff, D.L.; Gately, S.; Lincoln, T.M. Smooth muscle cell expression of type I cyclic GMP-dependent protein kinase is suppressed by continuous exposure to nitrovasodilators, theophylline, cyclic GMP, and cyclic AMP. J. Clin. Invest. 1997, 100, 2580–2587. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.L.; Austin, C.; Crichton, C.; Wray, S. A review of the actions and control of intracellular pH in vascular smooth muscle. Cardiovasc. Res. 1998, 38, 316–331. [Google Scholar] [CrossRef]
- Hirano, K. Current Topics in the Regulatory Mechanism Underlying the Ca2+ Sensitization of the Contractile Apparatus in Vascular Smooth Muscle. J. Pharmacol. Sci. 2007, 104, 109–115. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Citric Acid | Potassium | Vitamin C | Eriocitrin | Hesperidin | GABA | |
|---|---|---|---|---|---|---|
| Lemon juice | 4506 | 164 | 38 | 2.2 | 1.3 | 9.8 |
| AFR-lemon juice | 612 | 117 | 19 | 0.034 | 0.024 | 9.6 |
| Citric Acid | HCl | Lemon Juice | HCl | |
|---|---|---|---|---|
| pH | 6.08 | 6.53 | ||
| Concentration (mmol/L) | 5.00 | 8.43 × 10−4 | 5.00 | 3.01 × 10−4 |
| Vasorelaxation (%) * | 74.1 ± 3.97 | −8.73 ± 7.26 | 77.7 ± 3.31 | −13.2 ± 9.40 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakamura, K.; Suzuki, Y.; Goto, K.; Yamaguchi, S.; Hiramitsu, M. Antihypertensive and Vasorelaxant Effects of Citric Acid and Lemon Juice in Spontaneously Hypertensive Rats: In Vivo and Ex Vivo Studies. Nutrients 2023, 15, 3849. https://doi.org/10.3390/nu15173849
Nakamura K, Suzuki Y, Goto K, Yamaguchi S, Hiramitsu M. Antihypertensive and Vasorelaxant Effects of Citric Acid and Lemon Juice in Spontaneously Hypertensive Rats: In Vivo and Ex Vivo Studies. Nutrients. 2023; 15(17):3849. https://doi.org/10.3390/nu15173849
Chicago/Turabian StyleNakamura, Kozo, Yumiko Suzuki, Kazuma Goto, Shohei Yamaguchi, and Masanori Hiramitsu. 2023. "Antihypertensive and Vasorelaxant Effects of Citric Acid and Lemon Juice in Spontaneously Hypertensive Rats: In Vivo and Ex Vivo Studies" Nutrients 15, no. 17: 3849. https://doi.org/10.3390/nu15173849
APA StyleNakamura, K., Suzuki, Y., Goto, K., Yamaguchi, S., & Hiramitsu, M. (2023). Antihypertensive and Vasorelaxant Effects of Citric Acid and Lemon Juice in Spontaneously Hypertensive Rats: In Vivo and Ex Vivo Studies. Nutrients, 15(17), 3849. https://doi.org/10.3390/nu15173849