
The Effect of Perioperative Administration of Probiotics on Colorectal Cancer Surgery Outcomes

 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
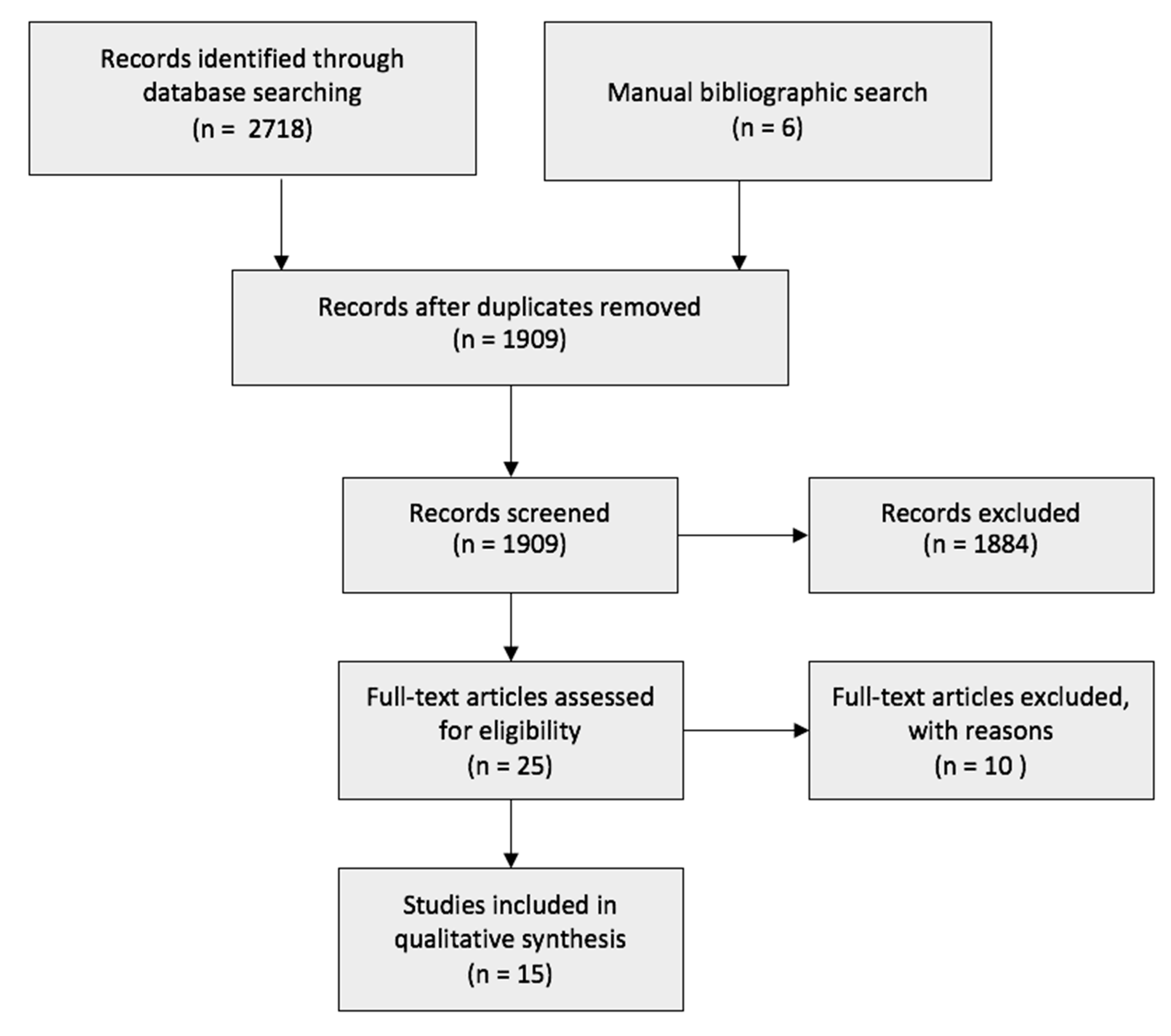
2.1. Search Strategy
2.2. Study Selection and Quality Assesment
2.3. Data Extraction and Analysis
3. Results
3.1. Postoperative Infectious Complications
3.2. Postoperative Non-Infectious Complications and Outcomes
3.3. Bacterial Translocation and Intestinal Permeability
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CRC | Colorectal Cancer |
| BT | Bacterial Translocation |
| HRP | Horseradish Peroxidase |
| IBD | Inflammatory Bowel Diseases |
| L/M | Lactulose/Mannitol |
| MeSH | Medical Sub Headings |
| MLN | Mesenteric Lymph Node |
| RCT | Randomised Controlled Trial |
| SSIs | Surgical Site Infections |
| TER | Trans-Epithelial Resistance |
| TJs | Tight Junction |
| UC | Ulcerative Colitis |
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Arnold, M.; Sierra, M.S.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global patterns and trends in colorectal cancer incidence and mortality. Gut 2017, 66, 683–691. [Google Scholar] [CrossRef] [PubMed]
- WHO Surgical Site Infection Guidelines. Web Appendix 6. Summary of a Systemic Review on Mechanical Bowel Preparation and the Use of Oral Antibiotics. Available online: https://www.who.int/gpsc/appendix6.pdf?ua=1 (accessed on 23 March 2020).
- Reddy, B.S.; Gatt, M.; Sowdi, R.; MacFie, J. Surgical manipulation of the large intestine increases bacterial translocation in patients un-dergoing elective colorectal surgery. Colorectal Dis. Off. J. Assoc. Coloproctol. Great Br. Irel. 2006, 8, 596–600. [Google Scholar]
- Saadia, R.; Schein, M.; Macfarlane, C.; Boffard, K.D. Gut barrier function and the surgeon. Br. J. Surg. 1990, 77, 487–492. [Google Scholar] [CrossRef] [PubMed]
- Espín-Basany, E.; Solís-Peña, A.; Pellino, G.; Kreisler, E.; Fraccalvieri, D.; Muinelo-Lorenzo, M.; Maseda-Díaz, O.; García-González, J.M.; Santamaría-Olabarrieta, M.; Codina-Cazador, A.; et al. Preoperative oral antibiotics and surgical-site infections in colon surgery (ORALEV): A multicentre, single-blind, pragmatic, randomised controlled trial. Lancet Gastroenterol. Hepatol. 2020, 5, 729–738. [Google Scholar] [CrossRef]
- Fijan, S. Microorganisms with Claimed Probiotic Properties: An Overview of Recent Literature. Int. J. Environ. Res. Public Health 2014, 11, 4745–4767. [Google Scholar] [CrossRef]
- Bajramagic, S.; Hodzic, E.; Mulabdic, A.; Holjan, S.; Smajlovic, S.V.; Rovcanin, A. Usage of probiotics and its clinical significance at surgically treated patients suffering from colorectal carcinoma. Med. Arch. 2019, 73, 316–320. [Google Scholar] [CrossRef]
- Nomura, T.; Tsuchiya, Y.; Nashimoto, A.; Yabusaki, H.; Takii, Y.; Nakagawa, S.; Sato, N.; Kanbayashi, C.; Tanaka, O. Probiotics reduce infectious complications after pancreaticoduodenectomy. Hepatogastroenterology 2007, 54, 661–663. [Google Scholar] [PubMed]
- Sugawara, G.; Nagino, M.; Nishio, H.; Ebata, T.; Takagi, K.; Asahara, T.; Nomoto, K.; Nimura, Y. Perioperative Synbiotic Treatment to Prevent Postoperative Infectious Complications in Biliary Cancer Surgery. Ann. Surg. 2006, 244, 706–714. [Google Scholar] [CrossRef] [PubMed]
- Rayes, N.; Seehofer, D.; Müller, A.R.; Hansen, S.; Bengmark, S.; Neuhaus, P. Influence of probiotics and fibre on the incidence of bacterial infections following major abdominal surgery—Results of a prospective trial. Z. Gastroenterol. 2002, 40, 869–876. [Google Scholar] [CrossRef] [PubMed]
- Rayes, N.; Seehofer, D.; Theruvath, T.; Schiller, R.A.; Langrehr, J.M.; Jonas, S.; Bengmark, S.; Neuhaus, P. Supply of Pre- and Probiotics reduces bacterial infection rates after liver transplantation—A randomized, double-blind trial. Am. J. Transplant. 2004, 5, 125–130. [Google Scholar] [CrossRef]
- Wei, D.; Heus, P.; Van De Wetering, F.T.; Van Tienhoven, G.; Verleye, L.; Scholten, R.J. Probiotics for the prevention or treatment of chemotherapy- or radiotherapy-related diarrhoea in people with cancer. Cochrane Database Syst. Rev. 2018, 8, CD008831. [Google Scholar] [CrossRef]
- Ewaschuk, J.B.; Dieleman, L.A. Probiotics and prebiotics in chronic inflammatory bowel diseases. World J. Gastroenterol. 2006, 12, 5941–5950. [Google Scholar] [CrossRef]
- Torres, J.; Ellul, P.; Langhorst, J.; Mikocka-Walus, A.; Barreiro-de, A.M.; Basnayake, C.; Sheng Ding, N.; Gilardi, D.; Katsanos, K.; Moser, G.; et al. European Crohn’s and Colitis Organisation Topical Review on Complementary Medicine and Psychotherapy in Inflammatory Bowel Disease. J. Crohns Colitis. 2019, 27, 673–685. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Horan, T.C.; Gaynes, R.P.; Martone, W.J.; Jarvis, W.R.; Emori, T.G. CDC definitions of nosocomial surgical site infections. Infect. Control. Hosp. Epidemiol. 1992, 13, 606–608. [Google Scholar] [CrossRef]
- Aisu, N.; Tanimura, S.; Yamashita, Y.; Yamashita, K.; Maki, K.; Yoshida, Y.; Sasaki, T.; Takeno, S.; Hoshino, S. Impact of perioperative probiotic treatment for surgical site infections in patients with colorectal cancer. Exp. Ther. Med. 2015, 10, 966–972. [Google Scholar] [CrossRef]
- Kotzampassi, K.; Stavrou, G.; Damoraki, G.; Georgitsi, M.; Basdanis, G.; Tsaousi, G.; Giamarellos-Bourboulis, E.J. A four-probiotic regimen reduces postoperative complications after colorectal surgery: A randomized, double-blind, placebo-controlled study. World J. Surg. 2015, 39, 2276–2783. [Google Scholar] [CrossRef] [PubMed]
- Kakaei, F.; Shahrasbi, M.; Kermani, T.A.; Taheri, S.; Tarvirdizade, K. Assessment of probiotic effects on colorectal surgery complications: A double blinded, randomized clinical trial. Biomed. Res. Ther. 2019, 6, 3067–3072. [Google Scholar] [CrossRef]
- Tan, C.K.; Said, S.; Rajandram, R.; Wang, Z.; Roslani, A.C.; Kin Fah, C. Pre-surgical administration of microbial cell preparation in colorectal cancer patients: A ran-domized controlled trial. World J. Surg. 2016, 40, 1985–1992. [Google Scholar] [CrossRef]
- Liu, Z.; Qin, H.; Yang, Z.; Xia, Y.; Liu, W.; Yang, J.; Jiang, Y.; Zhang, H.; Yang, Z.; Wang, Y.; et al. Randomised clinical trial: The effects of perioperative probiotic treatment on barrier function and post-operative infectious complications in colorectal cancer surgery—A double-blind study. Aliment. Pharmacol. Ther. 2011, 33, 50–63. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.-W.; Du, P.; Yang, B.-R.; Gao, J.; Fang, W.-J.; Ying, C.-M. Preoperative Probiotics Decrease Postoperative Infectious Complications of Colorectal Cancer. Am. J. Med. Sci. 2012, 343, 199–205. [Google Scholar] [CrossRef]
- Mangell, P.; Henrik, T.; Syk, I.; Ahrné, S.; Molin, G.; Olsson, C.; Jeppsson, B. Lactobacillus plantarum 299v does not reduce enteric bacteria or bacterial translocation in patients undergoing colon resection. Dig. Dis. Sci. 2012, 57, 1915–1924. [Google Scholar] [CrossRef] [PubMed]
- Sadahiro, S.; Suzuki, T.; Tanaka, A.; Okada, K.; Kamata, H.; Ozaki, T.; Koga, Y. Comparison between oral antibiotics and probiotics as bowel preparation for elective colon cancer surgery to prevent infection: Prospective randomized trial. Surgery 2014, 155, 493–503. [Google Scholar] [CrossRef] [PubMed]
- Consoli, M.L.; Steinberg, R.; Steinberg da Silva, R.; Robert Nicoli, J.; Bruña-Romero, O.; Gomes da Silva, R.; Generoso, S.d.V.; TD Correia, M.I. Randomized Clinical Trial: Impact of Oral Administration of Saccharomyces Boulardii on gene expression of intestinal cytokines in patients undergoing colon resection. J. Parenter. Enter. Nutr. 2016, 40, 1114–1121. [Google Scholar] [CrossRef]
- Yang, Y.; Xia, Y.; Chenzhang, S.; Hong, L.; Feng, J.; Yang, J.; Yang, Z.; Shi, C.; Wu, W.; Gao, R.; et al. The effect of perioperative probiotics treatment for colorectal cancer: Short-term outcomes of a randomized controlled trial. Oncotarget 2016, 7, 8432–8440. [Google Scholar] [CrossRef] [PubMed]
- Mizuta, M.; Endo, I.; Yamamoto, S.; Inokawa, H.; Kubo, M.; Udaka, T.; Sogabe, O.; Maeda, H.; Shirakawa, K.; Okazaki, E.; et al. Perioperative supplementation with bifidobacteria improves postoperative nutritional re-covery inflammatory response, and faecal microbiota in patients undergoing colorectal surgery: A prospective, randomized clinical trial. Biosci. Microbiota. 2016, 35, 77–87. [Google Scholar]
- Liu, Z.H.; Huan, M.J.; Zhang, X.w.; Wang, L.; Huang, N.Q.; Peng, H.; Lan, P.; Peng, J.S.; Yang, Z.; Xia, Y.; et al. The effects of perioperative probiotic treatment on serum zonulin concentration and subse-quent postoperative infectious complications after colorectal cancer surgery: A double-center and double-blind randomized clinical trial. Am. J. Clin. Nutr. 2013, 97, 117–126. [Google Scholar] [CrossRef]
- Pellino, G.; Sciaudone, G.; Candilio, G.; Camerlingo, A.; Marcellinaro, R.; De Fatico, S.; Rocco, F.; Canonico, S.; Riegler, G.; Selvaggi, F. Early postoperative administration of probiotics versus placebo in elderly patients undergoing elective colorectal surgery: A double-blind randomized controlled trial. BMC Surg. 2013, 13, S57. [Google Scholar] [CrossRef]
- Stephens, J.H.; Hewett, P.J. Clinical trial assessing VSL#3 for the treatment of anterior resection syndrome. ANZ J. Surg. 2012, 82, 420–427. [Google Scholar] [CrossRef]
- Kirkland, K.B.; Briggs, J.P.; Trivette, S.L.; Wilkinson, W.E.; Sexton, D.J. The Impact of Surgical-Site Infections in the 1990s: Attributable Mortality, Excess Length of Hospitalization, And Extra Costs. Infect. Control. Hosp. Epidemiol. 1999, 20, 725–730. [Google Scholar] [CrossRef] [PubMed]
- Kingham, P.T.; Pachter, L.H. Colonic anastomotic leaks: Risk factors, Diagnosis and treatment. J. Am. Coll. Surg. 2009, 208, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Eguchi, S.; Takatsuki, M.; Hidaka, M.; Soyama, A.; Ichikawa, T.; Kanematsu, T. Perioperative synbiotic treatment to prevent infectious complications in patients after elective living donor liver transplantation: A prospective randomized study. Am. J. Surg. 2011, 201, 498–502. [Google Scholar] [CrossRef]
- EuroSurg Collaborative; Chapman, S.J.; Blanco-Colino, R.; Pérez-Ajates, S.; Bautista, O.A.; Hodson, J.; Glasbey, J.C.; Pata, F.; Pellino, G.; Soares, A.S.; et al. Safety of hospital discharge before return of bowel function after elective colorectal surgery. BJS 2020, 107, 552–559. [Google Scholar] [CrossRef]
- EuroSurg Collaborative; Chapman, S.J.; Clerc, D.; Blanco-Colino, R.; Otto, A.; Nepogodiev, D.; Pagano, G.; Schaeff, V.; Soares, A.; Zaffaroni, G.; et al. Safety and efficacy of non-steroidal anti-inflammatory drugs to reduce ileus after colorectal surgery. BJS 2020, 107, e161–e169. [Google Scholar] [CrossRef] [PubMed]
- EuroSurg Collaborative. Ileus Management International (IMAGINE): Protocol for a multicentre, observational study of ileus after colorectal surgery. Color. Dis. 2017, 20, O17–O25. [Google Scholar] [CrossRef]
- Schietroma, M.; Pessia, B.; Carlei, F.; Cecilia, E.M.; Amicucci, G. Gut barrier function and systemic endotoxemia after laparotomy or laparoscopic re-section for colon cancer: A prospective randomized study. J. Minimal Access Surg. 2016, 12, 254–259. [Google Scholar]
- Deitch, E.A. The Role of Intestinal Barrier Failure and Bacterial Translocation in the Development of Systemic Infection and Multiple Organ Failure. Arch. Surg. 1990, 125, 403–404. [Google Scholar] [CrossRef]
- Chin, K.F.; Kallam, R.; O’Boyle, C.; MacFie, J. Bacterial Translocation May Influence the Long-Term Survival in Colorectal Cancer Patients. Dis. Colon Rectum 2007, 50, 323–330. [Google Scholar] [CrossRef] [PubMed]
- De Vrese, M.; Schrezenmeir, A.J. Probiotics, prebiotics and synbiotics. Adv. Biochem. Eng. Biotechnol. 2008, 111, 1–66. [Google Scholar]
- Stavrou, G.; Kotzampassi, K. Gut microbiome, surgical complications and probiotics. Ann. Gastroenterol. 2016, 30, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Basselink, M.G.; van Santvoort, H.C.; Renooij, W.; B de Smet, M.; Boermeester, M.A.; Fischer, K.; Timmerman, H.M.; Ali, U.A.; Cirkel, G.A.; Bollen, T.L.; et al. Intestinal barrier dysfunction in a randomised trial of a specific probiotic composition in acute pancreatitis. Ann. Surg. 2009, 250, 712–719. [Google Scholar] [CrossRef] [PubMed]
- Stearns, J.C.; Lynch, M.D.J.; Senadheera, D.B.; Tenenbaum, H.C.; Goldberg, M.B.; Cvitkovitch, D.G.; Croitoru, K.; Moreno-Hagelsieb, G.; Neufeld, J.D. Bacterial biogeography of the human digestive tract. Sci. Rep. 2011, 1, 170. [Google Scholar] [CrossRef] [PubMed]
- Donaldson, G.P.; Lee, S.M.; Mazmanian, S.K. Gut biogeography of the bacterial microbiota. Nat. Rev. Genet. 2016, 14, 20–32. [Google Scholar] [CrossRef]
- Wang, L.; Llorente, C.; Hartmann, P.; Yang, A.-M.; Chen, P.; Schnabl, B. Methods to determine intestinal permeability and bacterial translocation during liver disease. J. Immunol. Methods 2015, 421, 44–53. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Key Words | MESH Terms |
|---|---|
| Probiotic(s), Lactobacillus/i, Bifidobacteria/um Colorectal cancer/tumour/neoplasm/carcinoma, Rectal cancer/tumour/neoplasm/carcinoma, Colon cancer/tumour/neoplasm/carcinoma | Probiotics, Lactobacillus, Bifidobacterium, Colorectal neoplasms, Colonic neoplasms, Rectal neoplasm |
| Author (Year) | Number of Participants (Probiotics + Placebo) | SSIs Rate in Probiotics Group (%) | SSIs Rate in Placebo Group (%) | p-Value |
| Aisu (2015) [18] | 156 (75 + 81) | 6.7 | 19.7 | 0.016 * |
| Kotzampassi (2015) [19] | 164 (84 + 80) | 6.0 | 16.0 | 0.040 * |
| Bajramagic (2019) [8] | 78 (39 + 39) | 28.2 | 35.9 | 0.682 |
| Kakaei (2019) [20] | 99 (50 + 49) | 6.0 | 10.0 | 0.460 |
| Tan (2016) [21] | 40 (20 + 20) | 5.0 | 10.0 | 0.548 |
| Liu (2011) [22] | 100 (50 + 50) | 7.0 | 11.0 | >0.05 |
| Zhang (2012) [23] | 60 (30 + 30) | 3.3 | 13.3 | 0.353 |
| Mangell (2012) [24] | 72 (36 + 36) | 3.0 | 3.0 | N/A |
| Sadahiro (2014) [25] | 310 (100 + 95) (third group taking antibiotics: 99) | 18.9 | 17.9 | 1.00 |
| Author (Year) | Number of Participants (Probiotics + Placebo) | Organ/Space SSIs Rate in Probiotics Group (%) | Organ/Space SSIs Rate in Placebo Group (%) | p-Value |
| Aisu (2015) [18] | 156 (75 + 81) | 2.7 | 4.9 | 0.016 * |
| Sadahiro (2014) [25] | 310 (100 + 95) (third group taking antibiotics: 99) | 4 | 5.3 | 0.93 |
| Author (Year) | Number of Participants (Probiotics + Placebo) | Intra-Abdominal Abscess Rate in Probiotics Group (%) | Intra-Abdominal Abscess Rate in Placebo Group (%) | p-Value |
| Bajramagic (2019) [8] | 78 (39 + 39) | 12.8 | 17.9 | 0.530 |
| Consoli (2016) [26] | 33 (15 + 18) | 0 | 4.0 | >0.10 |
| Mangell (2012) [24] | 72 (36 + 36) | 0 | 3.0 | N/A |
| Zhang (2012) [23] | 60 (30 + 30) | 6.7 | 3.3 | 1.00 |
| Author (Year) | Number of Participants (Probiotics + Placebo) | Anastomotic Leaks in Probiotics Group (%) | Anastomotic Leaks IN Placebo Group (%) | p-Value |
| Kotzampassi (2015) [19] | 164 (84 + 80) | 1.2 | 8.8 | 0.031 * |
| Sadahiro (2014) [25] | 310 (100 + 95) (third group taking antibiotics, 99) | 7.4 | 12.0 | 0.560 |
| Yang (2016) [27] | 60 (30 + 30) | 3.3 | 6.7 | 1.00 |
| Mizuta (2016) [28] | 60 (31 + 29) | 9.7 | 17.2 | >0.05 |
| Tan (2016) [21] | 40 (20 + 20) | 5.0 | 10.0 | 0.548 |
| Zhang (2012) [23] | 60 (30 + 30) | 0 | 3.3 | 0.492 |
| Mangell (2012) [24] | 72 (36 + 36) | 0 | 3.0 | N/A |
| Author (Year) | Number of Participants (Probiotics + Placebo) | Mean Incidence of Fever in Probiotics Group (days ± standard deviation) | Mean Incidence of Fever in Placebo Group (days ± standard deviation) | p-Value |
| Liu (2011) [22] | 100 (50 + 50) | 6.0 ±1.9 | 7.2 ± 2.1 | <0.05 * |
| Liu (2013) [29] | 138 (70 + 68) | 5.82 ± 1.98 | 6.68 ± 2.29 | 0.015 * |
| Yang (2016) [27] | 60 (30 + 30) | 1.80 ± 2.34 | 4.77 ± 1.79 | 0.951 |
| Author (Year) | Number of Participants (Probiotics + Placebo) | Incidence of Ileus in Probiotics Group (%) | Incidence of Ileus in Placebo Group (%) | p-Value | |
| Bajramagic (2019) [8] | 78 (39 + 39) | 2.6 | 23.1 | 0.007 * | |
| Author (Year) | Number of Participants (Probiotics + Placebo) | Mean day to First Flatus in Probiotics Group (days ± standard deviation) | Mean Day to First Flatus In Placebo Group (days ± standard deviation) | p-Value | |
| Aisu (2015) [18] | 156 (75 + 81) | 2.0 ± 1.1 | 2.8 ± 2 | 0.001 * | |
| Yang (2016) [27] | 60 (30 + 30) | 3.27 ± 0.58 | 3.63 ± 0.67 | 0.0274 * | |
| Mangell (2012) [24] | 72 (36 + 36) | Median day to first flatus | Median day to first flatus | N/A | |
| 2 | 3 | ||||
| Author (Year) | Number of Participants (Probiotics + Placebo) | Mean Day to First Stool in Probiotics Group (days ± standard deviation) | Mean Days to First Stool in Placebo Group (days ± standard deviation) | p-Value | |
| Kotzampassi (2015) [19] | 164 (84 + 80) | Lower a | Higher a | 0.001 * | |
| Yang (2016) [27] | 60 (30 + 30) | 3.87 ± 1.17 | 4.53 ± 1.11 | 0.0268 * | |
| Mangell (2012) [24] | 72 (36 + 36) | Median day to first stool | Median day to first stool | N/A | |
| 4 | 4 | ||||
| Author (Year) | Number of Participants (Probiotics + Placebo) | Incidence of Abdominal Distention in Probiotics Group (%) | Incidence of Abdominal Distention in Placebo Group (%) | p-Value | |
| Liu (2011) [22] | 100 (50 + 50) | 21.0 | 36.0 | <0.05 * | |
| Yang (2016) [27] | 60 (30 + 30) | 30.0 | 43.3 | <0.05 * | |
| Author (Year) | Number of participants (probiotics + study) | Incidence of Abdominal Cramps in probiotics group (%) | Incidence of Abdominal Cramps in placebo group (%) | p-Value | |
| Liu (2011) [22] | 60 (30 + 30) | 26.0 | 39.0 | <0.05 * | |
| Author (Year) | Number of participants (probiotics + placebo) | Incidence of Diarrhoea in probiotics group (%) | Incidence of Diarrhoea in placebo group (%) | p-Value | |
| Liu (2011) [22] | 100 (50 + 50) | 17.0 | 34.0 | <0.05 * | |
| Liu (2013) [29] | 128 (70 + 68) | 14.7 | 29.3 | 0.03 * | |
| Yang (2016) [27] | 60 (30 + 30) | 26.7 | 53.3 | 0.0352 * | |
| Author (Year) | Number of Participants (Probiotics + Placebo) | Mean length of Stay in Probiotics Group (days ± standard deviation) | Mean Length of Stay in Placebo Group (days ± standard deviation) | p-Value | |
| Kotzampassi (2015) [19] | 164 (75 + 81) | Median length of stay | Median length of stay | <0.0001 * | |
| 8 | 10 | ||||
| Consoli (2016) [26] | 33 (15 + 18) | 10 | 11 | >0.10 | |
| Kakaei (2019) [20] | 99 (50 + 49) | 5.96 ± 2.53 | 6.10 ± 2.44 | 0.30 | |
| Liu (2011) [22] | 100 (50 + 50) | 12.3 ± 2.3 | 12.6 ± 3.3 | >0.05 | |
| Mizuta (2016) [28] | 60 (31 + 29) | 21.4 ± 10.1 | 23.0 ± 13.8 | >0.05 | |
| Pellino (2013) [30] | 18 (10 + 8) | 12.0 ± 8.3 | 13.5 ± 4.8 | >0.05 | |
| Stephens (2012) [31] | 38 (20 + 18) | 5.60 ± 2.93 | 6.45 ± 7.50 | 0.564 | |
| Zhang (2012) [23] | 60 (30 + 30) | 12.0 ± 3.0 | 14.0 ± 3.0 | 0.109 | |
| Yang (2016) [27] | 60 (30 + 30) | 15.86 ± 4.92 | 15.0 ± 4.31 | 0.487 | |
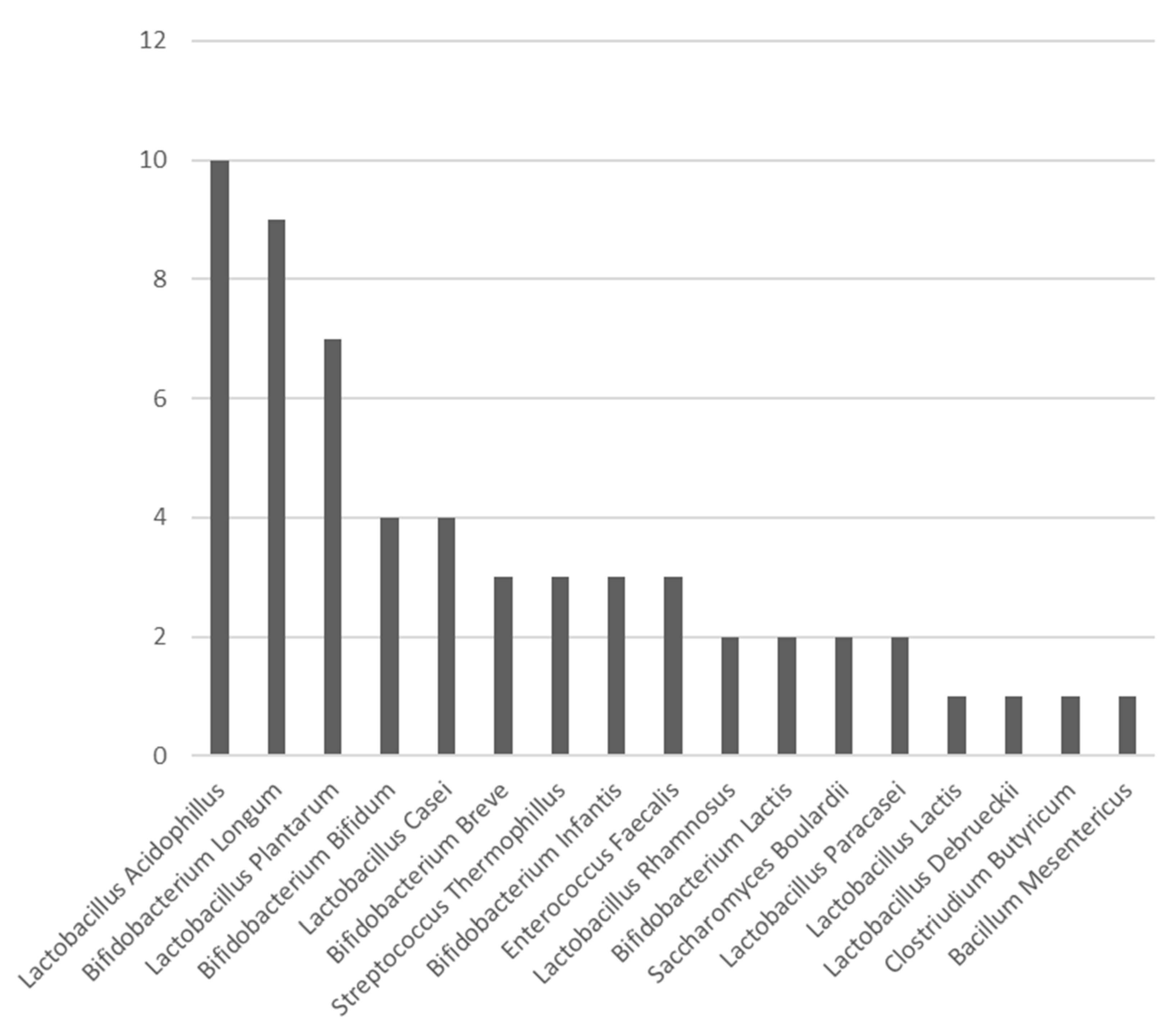
| Study | Probiotic Strains | No. of Strains | Duration of Administration |
|---|---|---|---|
| Bajramagic | Lactobacillus casei, Lactobacillus acidophillus, Lactobacillus plantarum, Lactobacillus rhamnosus, Bifidobacterium lactis, Bifidobacterium bifidum, Bifidobacterium Breve, Streptococcus Thermophillus | 8 | +3 to +30 |
| Pellino | Streptococcus thermophilus, Bifidobacterium longum, Bifidobacterium breve, Bifidobacterium infantis, Lactobacillus acidophillus, Lactobacillus plantarum, Lactobacillus paracasei, Lactobacillus debrueckii | 8 | +0 to +28 |
| Stephens | Streptococcus thermophilus, Bifidobacterium longum, Bifidobacterium breve, Bifidobacterium infantis, Lactobacillus acidophillus, Lactobacillus plantarum, Lactobacillus paracasei, Lactobacillus debrueckii | 8 | +0 to +28 |
| Tan | Lactobacillus acidophillus, Lactobacillus casei, Lactobacillus lactis, Bifidobacterium bifidum, Bifidobacterium longum, Bifidobacterium infantis | 6 | −7 to +0 |
| Kakaei | Lactobacillus casei, Lactobacillus acidophillus, Bifidobacterium breve, Bifidobacterium longum, Streptococcus thermophilus | 5 | −7 to +23 |
| Yang | Bifidobacterium longum, Lactobacillus acidophillus, Enterococcus faecalis | 5 | −5 to +7 |
| Kotzampassi | Lactobacillus acidophillus, Lactobacillus plantarum, Bifidobacterium lactis, Sacharomyces boulardii | 4 | −1 to +14 |
| Aisu | Enterococcus faecalis, Clostridium butyricum, Bacillum mesentericus | 3 | −15/−3 a |
| Liu 2011 | Lactobacillus plantarum, Lactobacillus acidophillus, Bifidobacterium longum | 3 | −6 to +10 |
| Liu 2013 | Lactobacillus plantarum, Lactobacillus acidophillus, Bifidobacterium longum | 3 | −6 to +10 |
| Zhang | Bifidobacterium longum, Lactobacillus acidophillus, Enterococcus faecalis | 3 | −5 to +3 |
| Sadahiro | Bifidobacterium bifidum | 1 | −8 to −2 and +5 to +15 |
| Consoli | Sachharomyces boulardii | 1 | −7 to +0 b |
| Mangell | Lactobacillus plantarum | 1 | −8 to +0 and +1 to +6 |
| Mizuta | Bifidobacterium longum BB536 | 1 | −14/−7 to +14 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pitsillides, L.; Pellino, G.; Tekkis, P.; Kontovounisios, C. The Effect of Perioperative Administration of Probiotics on Colorectal Cancer Surgery Outcomes. Nutrients 2021, 13, 1451. https://doi.org/10.3390/nu13051451
Pitsillides L, Pellino G, Tekkis P, Kontovounisios C. The Effect of Perioperative Administration of Probiotics on Colorectal Cancer Surgery Outcomes. Nutrients. 2021; 13(5):1451. https://doi.org/10.3390/nu13051451
Chicago/Turabian StylePitsillides, Louise, Gianluca Pellino, Paris Tekkis, and Christos Kontovounisios. 2021. "The Effect of Perioperative Administration of Probiotics on Colorectal Cancer Surgery Outcomes" Nutrients 13, no. 5: 1451. https://doi.org/10.3390/nu13051451
APA StylePitsillides, L., Pellino, G., Tekkis, P., & Kontovounisios, C. (2021). The Effect of Perioperative Administration of Probiotics on Colorectal Cancer Surgery Outcomes. Nutrients, 13(5), 1451. https://doi.org/10.3390/nu13051451