
Component-Resolved Diagnosis of Hazelnut Allergy in Children

 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Selection and Data Collection
2.2. Statistical Analyses
3. Results
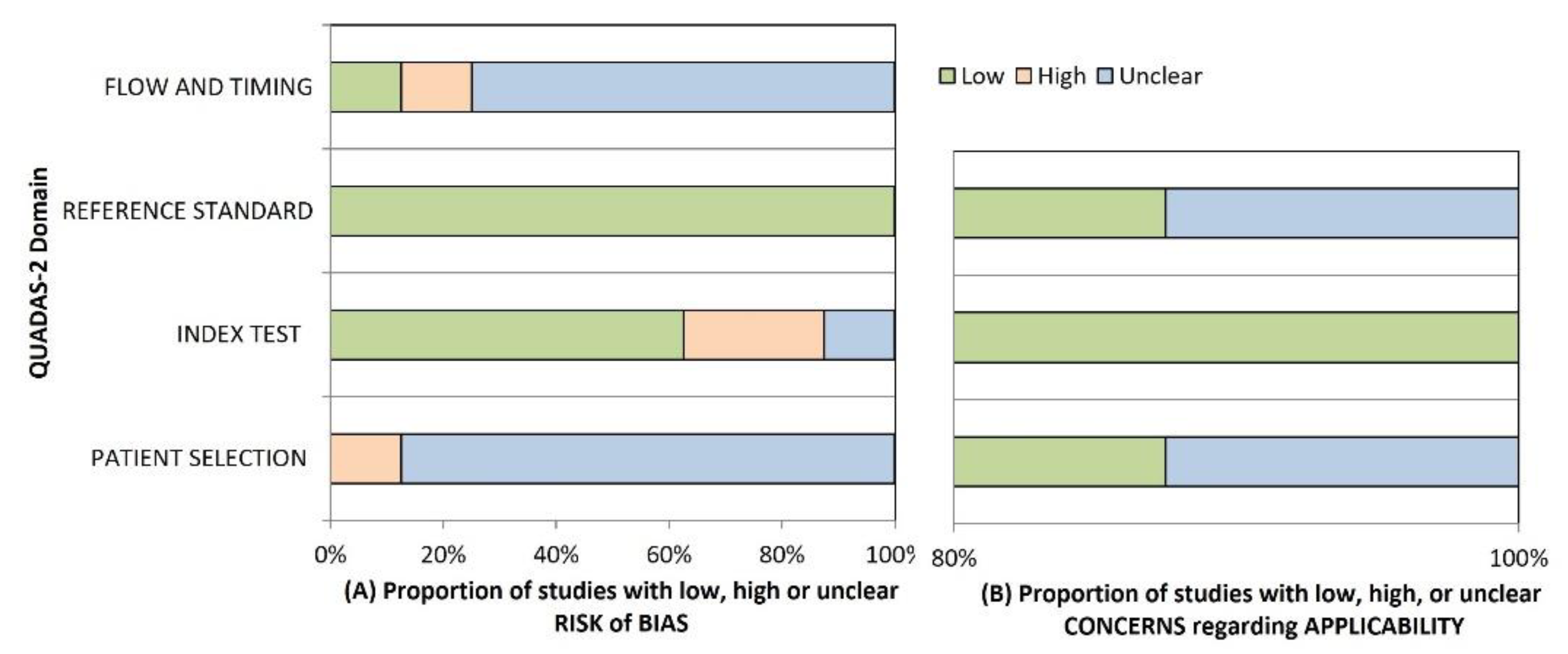
3.1. Risk of Bias
3.2. Study Characteristics
3.3. Diagnostic Accuracy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sicherer, S.H.; Muñoz-Furlong, A.; Godbold, J.H.; Sampson, H.A. US Prevalence of Self-Reported Peanut, Tree Nut, and Sesame Allergy: 11-Year Follow-Up. J. Allergy Clin. Immunol. 2010, 12, 1322–1326. [Google Scholar] [CrossRef] [PubMed]
- McWilliam, V.; Koplin, J.; Lodge, C.; Tang, M.; Dharmage, S.; Allen, K. The Prevalence of Tree Nut Allergy: A Systematic Review. Curr. Allergy Asthma Rep. 2015, 15, 54. [Google Scholar] [CrossRef]
- Fleischer, D.M.; Conover-Walker, M.K.; Matsui, E.C.; Wood, R.A. The Natural History of Tree Nut Allergy. J. Allergy Clin. Immunol. 2005, 116, 1087–1093. [Google Scholar] [CrossRef] [PubMed]
- De Knop, K.J.; Verweij, M.M.; Grimmelikhuijsen, M.; Philipse, E.; Hagendorens, M.M.; Bridts, C.H.; De Clerck, L.S.; Stevens, W.J.; Ebo, D.G. Age-Related Sensitization Profiles for Hazelnut (Corylus Avellana) in a Birch-Endemic Region. Pediatr. Allergy Immunol. 2011, 22, e139–e149. [Google Scholar] [CrossRef]
- Turner, P.J.; Gowland, M.H.; Sharma, V.; Ierodiakonou, D.; Harper, N.; Garcez, T.; Pumphrey, R.; Boyle, R.J. Increase in Anaphylaxis-Related Hospitalizations but No Increase in Fatalities: An Analysis of United Kingdom National Anaphylaxis Data, 1992-2012. J. Allergy Clin. Immunol. 2015, 135, 956–963. [Google Scholar] [CrossRef] [PubMed]
- Stiefel, G.; Anagnostou, K.; Boyle, R.J.; Brathwaite, N.; Ewan, P.; Fox, A.T.; Huber, P.; Luyt, D.; Till, S.J.; Venter, C.; et al. BSACI Guideline for the Diagnosis and Management of Peanut and Tree Nut Allergy. Clin. Exp. Allergy. 2017, 47, 719–739. [Google Scholar] [CrossRef]
- Sicherer, S.H.; Muñoz-Furlong, A.; Sampson, H.A. Prevalence of Peanut and Tree Nut Allergy in the United States Determined by Means of a Random Digit Dial Telephone Survey: A 5-Year Follow-up Study. J. Allergy Clin. Immunol. 2003, 112, 1203–1207. [Google Scholar] [CrossRef]
- Ewan, P.W.; Clark, A.T. Long-Term Prospective Observational Study of Patients with Peanut and Nut Allergy after Participation in a Management Plan. Lancet 2001, 357, 111–115. [Google Scholar] [CrossRef]
- Sampson, H.A.; Aceves, S.; Bock, S.A.; James, J.; Jones, S.; Lang, D.; Nadeau, K.; Nowak-Wegrzyn, A.; Oppenheimer, J.; Perry, T.T.; et al. Food Allergy: A Practice Parameter Update—2014. J. Allergy Clin. Immunol. 2014, 134, 1016–1025. [Google Scholar] [CrossRef]
- Sicherer, S.H.; Sampson, H.A. Food Allergy: A Review and Update on Epidemiology, Pathogenesis, Diagnosis, Prevention, and Management. J. Allergy Clin. Immunol. 2018, 141, 41–58. [Google Scholar] [CrossRef]
- Caffarelli, C.; Garrubba, M.; Greco, C.; Mastrorilli, C.; Dascola, C.P. Asthma and Food Allergy in Children: Is There a Connection or Interaction? Front. Pediatr. 2016, 4, 34. [Google Scholar] [CrossRef] [PubMed]
- Mastrorilli, C.; Caffarelli, C.; Hoffmann-Sommergruber, K. Food Allergy and Atopic Dermatitis: Prediction, Progression, and Prevention. Pediatr. Allergy Immunol. 2017, 28, 831–840. [Google Scholar] [CrossRef]
- Ortolani, C.; Ballmer-Weber, B.K.; Hansen, K.S.; Ispano, M.; Wüthrich, B.; Bindslev-Jensen, C.; Ansaloni, R.; Vannucci, L.; Pravettoni, V.; Scibilia, J.; et al. Hazelnut allergy: A double-blind, placebo-controlled food challenge multicenter study. J. Allergy Clin Immunol. 2000, 105, 577–581. [Google Scholar] [CrossRef]
- Hansen, K.S.; Ballmer-Weber, B.K.; Sastre, J.; Lidholm, J.; Andersson, K.; Oberhofer, H.; Lluch-Bernal, M.; Östling, J.; Mattsson, L.; Schocker, F.; et al. Component-Resolved In Vitro Diagnosis of Hazelnut Allergy in Europe. J. Allergy Clin. Immunol. 2009, 123, 1134–1141. [Google Scholar] [CrossRef]
- Schocker, F.; Lüttkopf, D.; Scheurer, S.; Petersen, A.; Cisteró-Bahima, A.; Enrique, E.; San Miguel-Moncín, M.; Akkerdaas, J.; Van Ree, R.; Vieths, S.; et al. Recombinant Lipid Transfer Protein Cor a 8 from Hazelnut: A New Tool for in Vitro Diagnosis of Potentially Severe Hazelnut Allergy. J. Allergy Clin. Immunol. 2004, 113, 141–147. [Google Scholar] [CrossRef]
- Grabenhenrich, L.; Lange, L.; Härtl, M.; Kalb, B.; Ziegert, M.; Finger, A.; Harandi, N.; Schlags, R.; Gappa, M.; Puzzo, L.; et al. The Component-Specific to Total IgE Ratios Do Not Improve Peanut and Hazelnut Allergy Diagnoses. J. Allergy Clin. Immunol. 2016, 137, 1751–1760. [Google Scholar] [CrossRef] [PubMed]
- Beyer, K.; Grishina, G.; Bardina, L.; Grishin, A.; Sampson, H.A. Identification of an 11S Globulin as a Major Hazelnut Food Allergen in Hazelnut-Induced Systemic Reactions. J. Allergy Clin. Immunol. 2002, 110, 517–523. [Google Scholar] [CrossRef]
- Clark, A.T.; Ewan, P.W. Interpretation of Tests for Nut Allergy in One Thousand Patients, in Relation to Allergy or Tolerance. Clin. Exp. Allergy 2003, 33, 1041–1045. [Google Scholar] [CrossRef]
- Caffarelli, C.; Ricò, S.; Rinaldi, L.; Povesi Dascola, C.; Terzi, C.; Bernasconi, S. Blood Pressure Monitoring in Children Undergoing Food Challenge: Association With Anaphylaxis. Ann. Allergy Asthma Immunol. 2012, 108, 285–286. [Google Scholar] [CrossRef]
- Uotila, R.; Röntynen, P.; Pelkonen, A.S.; Voutilainen, H.; Kaarina Kukkonen, A.; Mäkelä, M.J. For Hazelnut Allergy, Component Testing of Cor a 9 and Cor a 14 Is Relevant Also in Birch-Endemic Areas. Allergy 2020, 75, 2977–2980. [Google Scholar] [CrossRef] [PubMed]
- Matricardi, P.M.; Kleine-Tebbe, J.; Hoffmann, H.J.; Valenta, R.; Hilger, C.; Hofmaier, S.; Aalberse, R.C.; Agache, I.; Asero, R.; Ballmer-Weber, B.; et al. EAACI Molecular Allergology User’s Guide. Pediatr. Allergy Immunol. 2016, 27, 1–250. [Google Scholar] [CrossRef] [PubMed]
- Costa, J.; Mafra, I.; Carrapatoso, I.; Oliveira, M.B.P.P. Hazelnut Allergens: Molecular Characterization, Detection, and Clinical Relevance. Crit. Rev. Food Sci. Nutr. 2016, 56, 2579–2605. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, C.; Berthold, M.; Mascialino, B.; Orme, M.; Sjölander, S.; Hamilton, R. Allergen Components in Diagnosing Childhood Hazelnut Allergy: Systematic Literature Review and Meta-Analysis. Pediatr. Allergy Immunol. 2020, 31, 186–196. [Google Scholar] [CrossRef]
- Whiting, P.F.; Rutjes, A.W.S.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.G.; Sterne, J.A.C.; Bossuyt, P.M.M. Quadas-2: A Revised Tool for the Quality Assessment of Diagnostic Accuracy Studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-Analysis in Clinical Trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Fagan, T.J.F. Nomogram for Bayes’s Theorem. N. Engl. J. Med. 1975, 293, 257. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in Meta-Analysis Detected by a Simple, Graphical Test. Br. Med. J. 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Masthoff, L.J.N.; Mattsson, L.; Zuidmeer-Jongejan, L.; Lidholm, J.; Andersson, K.; Akkerdaas, J.H.; Versteeg, S.A.; Garino, C.; Meijer, Y.; Kentie, P.; et al. Sensitization to Cor a 9 and Cor a 14 Is Highly Specific for a Hazelnut Allergy with Objective Symptoms in Dutch Children and Adults. J. Allergy Clin. Immunol. 2013, 132, 393–399. [Google Scholar] [CrossRef]
- Beyer, K.; Grabenhenrich, L.; Härtl, M.; Beder, A.; Kalb, B.; Ziegert, M.; Finger, A.; Harandi, N.; Schlags, R.; Gappa, M.; et al. Predictive Values of Component-Specific IgE for the Outcome of Peanut and Hazelnut Food Challenges in Children. Allergy 2015, 70, 90–98. [Google Scholar] [CrossRef]
- Brandström, J.; Nopp, A.; Johansson, S.G.O.; Lilja, G.; Sundqvist, A.C.; Borres, M.P.; Nilsson, C. Basophil Allergen Threshold Sensitivity and Component-Resolved Diagnostics Improve Hazelnut Allergy Diagnosis. Clin. Exp. Allergy 2015, 45, 1412–1418. [Google Scholar] [CrossRef] [PubMed]
- Buyuktiryaki, B.; Cavkaytar, O.; Sahiner, U.M.; Yilmaz, E.A.; Yavuz, S.T.; Soyer, O.; Sekerel, B.E.; Tuncer, A.; Sackesen, C. Cor a 14, Hazelnut-Specific IgE, and SPT as a Reliable Tool in Hazelnut Allergy Diagnosis in Eastern Mediterranean Children. J. Allergy Clin. Immunol. Pract. 2016, 4, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Eller, E.; Mortz, C.G.; Bindslev-Jensen, C. Cor a 14 Is the Superior Serological Marker for Hazelnut Allergy in Children, Independent of Concomitant Peanut Allergy. Allergy 2016, 71, 556–562. [Google Scholar] [CrossRef]
- Kattan, J.D.; Sicherer, S.H.; Sampson, H.A. Clinical Reactivity to Hazelnut May Be Better Identified by Component Testing than Traditional Testing Methods. J. Allergy Clin. Immunol. Pract. 2014, 2, 633–634. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Inoue, Y.; Sato, S.; Takahashi, K.; Yanagida, N.; Yamamoto, H.; Shimizu, N.; Ebisawa, M. Component-Resolved Diagnostics Can Be Useful for Identifying Hazelnut Allergy in Japanese Children. Allergol. Int. 2020, 69, 239–245. [Google Scholar] [CrossRef]
- Weinberger, T.; Sicherer, S. Current Perspectives on Tree Nut Allergy: A Review. J. Asthma Allergy 2018, 11, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Ebo, D.G.; Verweij, M.M.; Sabato, V.; Hagendorens, M.M.; Bridts, C.H.; De Clerck, L.S. Hazelnut Allergy: A Multi-Faced Condition with Demographic and Geographic Characteristics. Acta Clin. Belg. 2012, 67, 317–321. [Google Scholar] [CrossRef] [PubMed]
- Cipriani, F.; Mastrorilli, C.; Tripodi, S.; Ricci, G.; Perna, S.; Panetta, V.; Asero, R.; Dondi, A.; Bianchi, A.; Maiello, N.; et al. Diagnostic Relevance of IgE Sensitization Profiles to Eight Recombinant Phleum Pratense Molecules. Allergy Eur. J. Allergy Clin. Immunol. 2018, 73, 673–682. [Google Scholar] [CrossRef]
- Mastrorilli, C.; Cardinale, F.; Giannetti, A.; Caffarelli, C. Pollen-Food Allergy Syndrome: A Not so Rare Disease in Childhood. Med. 2019, 55, 641. [Google Scholar] [CrossRef]
- Cardinale, F.; Ciprandi, G.; Barberi, S.; Bernardini, R.; Caffarelli, C.; Calvani, M.; Cavagni, G.; Galli, E.; Minasi, D.; Del Giudice, M.M.; et al. Consensus Statement of the Italian Society of Pediatric Allergy and Immunology for the Pragmatic Management of Children and Adolescents with Allergic or Immunological Diseases during the COVID-19 Pandemic. Ital. J. Pediatr. 2020, 46, 84. [Google Scholar] [CrossRef]
- D’Auria, E.; Anania, C.; Cuomo, B.; Decimo, F.; Cosimo Indirli, G.; Mastrorilli, V.; Santoro, A.; Sartorio, M.U.A.; Veronelli, E.; Caffarelli, C.; et al. COVID-19 and Food Allergy in Children. Acta Biomed. 2020, 91, 204–206. [Google Scholar] [CrossRef] [PubMed]
- Caffarelli, C.; Coscia, A.; Ridolo, E.; Povesi Dascola, C.; Gelmett, C.; Raggi, V.; Volta, E.; Vanell, M.; Dall’Aglio, P.P. Parents’ Estimate of Food Allergy Prevalence and Management in Italian School-Aged Children. Pediatr. Int. 2011, 53, 505–510. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Summary of the Included Studies | |||||
|---|---|---|---|---|---|
| Oral Food Challenge | |||||
| Author, Country, Year | Study Population | Age (years) M/F | Lower limit IgE Positive Test (kUA/L) | Participants (%) | Number Positive (%) |
| Beyer, Germany, 2015 [30] | 143 children with suspected hazelnut allergy | Age (median, quartile) Tolerant 4.7 (2.1–8.1) Allergic 4.3 (2.2–6.1) −98/45 | 0.10 | 143 (100%) of which 46/143 (32%) DBPCFCF | 99 (69%) |
| Brandström, Sweden, 2015 [31] | 40 children referred for oral challenge for hazelnut allergy suspicion | Age (median, range) 11 (6–18) 23/17 | 0.10 | 40 (100%) DBPCFC | 8 (20%) |
| Buyuktiryaki, Turkey, 2016 [32] | 64 children with hazelnut allergy to determine resolution of hazelnut allergy | Age (median, interquartile) 3.4 (2.1–7.2) 45/19 | 0.10 | 56 (87.5%) DBPCFC 8 not performed because of anaphylaxis within the last 12 months | 24 (42%) |
| Eller, Denmark, 2016 [33] | 155 children with suspected hazelnut allergy | Age 5.1 (0.7–15.5) 100/55 | 0.35 | 140 (90%) open challenge 15 DBPCFC | 65 (41%) |
| Grabenhenrich, Germany, 2016 [16] | 142 children with suspected hazelnut allergy | Age (median, interquartile) 4.5 (2.1–7.6) 97/45 | >0 | 142 (100%) open, single blind, double blind challenge. | 44 (31%) |
| Inoue, Japan, 2019 [35] | 91 children sensitized to hazelnut | Age (median, interquartile) 7.3 (5.9–10.5) 63/28 | 0.35 | 91 (100%) open food challenge | 9 (9%) |
| Kattan, US, 2014 [34] | 33 children with clinical impression of hazelnut allergy 9 children with history of objective symptoms with hazelnut ingestion | - | 0.10 | 33 (78%) open challenge 9 not performed because of a history of objective symptoms with ingestion of hazelnut | 4 (12%) |
| Masthoff, Netherlands, 2013 [29] | 81 children Retrospective equally powered groups with positive/negative challenge | Age (median, interquartile) 8 (7–12) 54/27 | 0.35 | 81 (100%) DBPCFC | 40 (49%) |
| Author | Sensitivity (%) | (95%CI) | Specificity (%) | (95%CI) | DOR | (95%CI) |
|---|---|---|---|---|---|---|
| Cor a 1 | ||||||
| Brandström [31] | 50 | (5.7–84.4) | 12.5 | (3.5–29.0) | 0.14 | (0.03–0.81) |
| Eller [33] | 49.2 | (36.6–61.9) | 58.9 | (48.0–69.2) | 1.39 | (0.73–2.64) |
| Masthoff [29] | 70.0 | (53.5–83.4) | 9.8 | (2.7–23.1) | 0.25 | (0.07–0.87) |
| Pooled | 56.6 | (47.0–65.9) | 37.4 | (30.0–45.3) | 0.42 | (0.09–1.89) |
| Heterogeneity, Chi2 | 4.60 p = 0.100 | 43.3 p = 0.000 | 9.9 p = 0.007 | |||
| Cor a 9 | ||||||
| Brandstrom [31] | 100 | (63.1–100) | 56.3 | (37.7–73.6) | 21.69 | (1.15–407.76) |
| Eller [33] | 74.2 | (61.5–84.0) | 67.9 | (57.1–77.3) | 5.94 | (2.93–12.06) |
| Kattan [34] | 84.6 | (54.6–98.1) | 65.5 | (45.7–82.1) | 10.45 | (1.93–56.64) |
| Masthoff [29] | 83.0 | (67.2–92.7) | 80.0 | (65.1–91.2) | 19.43 | (6.32–59.75) |
| Pooled | 79.5 | (71.5–86.2) | 68.1 | (60.9–74.6) | 9.45 | (4.92–18.13) |
| Heterogeneity, Chi2 | 5.4 p = 0.145 | 4.9 p = 0.180 | 3.5 p = 0.320 | |||
| Cor a 14 | ||||||
| Beyer [30] | 84.1 | (69.9–93.4) | 80.8 | (71.7–88.0) | 22.26 | (8.61–57.56) |
| Brandstrom [31] | 100 | (63.1–100) | 84.6 | (67.2–94.7) | 85.00 | (4.25–1699.61) |
| Buyuktiryaki [32] | 84.6 | (65.1–95.6) | 88.0 | (68.8–97.5) | 49.00 | (11.14–215.60) |
| Eller [33] | 80 | (68.2–88.9) | 84.4 | (75.3–91.2) | 21.71 | (9.44–49.96) |
| Kattan [34] | 69.2 | (38.6–90.9) | 82.8 | (64.2–94.2) | 10.80 | (2.36–49.46) |
| Masthoff [29] | 70 | (53.85–83.4) | 75.6 | (59.7–87.6) | 7.23 | (2.71–19.32) |
| Pooled | 80.2 | (74.0–85.5) | 82.4 | (77.7–86.4) | 18.27 | (10.24–32.59) |
| Heterogeneity, Chi2 | 8.4 p = 0.135 | 2.35 p = 0.799 | 6.92 p = 0.227 |
| Author | AUC | 95%CI |
|---|---|---|
| Cor a1 Masthoff [29] | 0.43 | 0.3–0.55 |
| Beyer [30] | 0.56 | 0.46–0.66 |
| Grabenhenrich [16] | 0.55 | 0.46–0.65 |
| Inoue [35] | 0.72 | 0.55–0.9 |
| Pooled | 0.55 | 0.46–0.64 |
| Cor a8 Masthoff [29] | 0.51 | 0.39–0.64 |
| Beyer [30] | 0.63 | 0.53–0.73 |
| Grabenhenrich [16] | 0.62 | 0.52–0.72 |
| Inoue [35] | 0.58 | 0.39–0.78 |
| Pooled | 0.59 | 0.54–0.65 |
| Cor a9 Masthoff [29] | 0.87 | 0.79–0.96 |
| Beyer [30] | 0.8 | 0.72–0.88 |
| Eller [33] | 0.78 | 0.7–0.85 |
| Grabenhenrich [16] | 0.8 | 0.72–0.88 |
| Inoue [35] | 0.71 | 0.52–0.89 |
| Pooled | 0.81 | 0.77–0.84 |
| Cor a14 Masthoff [29] | 0.8 | 0.7–0.9 |
| Beyer [30] | 0.89 | 0.83–0.95 |
| Eller [33] | 0.85 | 0.77–0.94 |
| Grabenhenrich [16] | 0.89 | 0.83–0.95 |
| Buyuktiryaki [32] | 0.93 | 0.85–1 |
| Inoue [35] | 0.65 | 0.44–0.86 |
| Pooled | 0.87 | 0.82–0.92 |
| PPV (%) | (95%CI) | NPV (%) | (95%CI) | LR+ | (95%CI) | LR− | (95%CI) | |
|---|---|---|---|---|---|---|---|---|
| Cor a 1 | ||||||||
| Brandström [31] | 12.5 | (1–24) | 50.0 | (15.4–84.6) | 0.57 | (0.28–1.16) | 4.0 | (1.27–2.62) |
| Eller [33] | 46.4 | (34.6–58.1) | 61.6 | (51.4–71.9) | 1.2 | (0.84–1.7) | 0.86 | (0.64–1.16) |
| Masthoff [26] | 43.1 | (31–55.1) | 25 | (3.8–46.2) | 0.78 | (0.62–0.97) | 3.08 | (1.08–8.74) |
| Pooled | 0.85 | (0.58–1.26) | 1.99 | (0.63–6.21) | ||||
| Heterogeneity, Chi2 | 6.0 p = 0.050 | 11.5 p = 0.003 | ||||||
| Cor a 9 | ||||||||
| Brandstrom [31] | 36.4 | (16.3–56.5) | 100 | (100–100) | 2.15 | (1.42–3.26) | 0.1 | (0.07–1.5) |
| Eller [33] | 62.3 | (51.5–73.2) | 78.2 | (69–84.4) | 2.29 | (1.64–3.2) | 0.39 | (0.25–0.60) |
| Kattan [34] | 52.4 | (31–73.7) | 90.5 | (77.9–100) | 2.45 | (1.41–4.26) | 0.24 | (0.06–0.86) |
| Masthoff [29] | 80.5 | (68.4–2.6) | 82.5 | (70.7–94.3) | 4.16 | (2.20–7.83) | 0.21 | (0.11–0.43) |
| Pooled | 2.47 | (1.93–3.17) | 0.31 | (0.21–0.45) | ||||
| Heterogeneity, Chi2 | 3.6 p = 0.309 | 3.1 p = 0.377 | ||||||
| Cor a 14 | ||||||||
| Beyer [30] | 66.1 | (53.7–78.5) | 92 | (86.2–97.7) | 4.38 | (2.87–6.70) | 0.20 | (0.1–0.39) |
| Brandstrom [31] | 61.5 | (35.1–88) | 100 | (100–100) | 5.67 | (2.60–12.35) | 0,07 | (0–1) |
| Buyuktiryaki [32] | 88 | (75.3–100) | 84.6 | (70.7–98.5) | 7.00 | (2.77–17.67) | 0.14 | (0.06–0.36) |
| Eller [33] | 78.8 | (68.9–88.7) | 85.4 | (78.1–92.7) | 5.14 | (3.13–8.45) | 0.24 | (0.14–0.39) |
| Kattan [34] | 64.3 | (39.2–89.4) | 85.7 | (72.8–98.7) | 4.02 | (1.67–9.64) | 0.37 | (0.16–0.85) |
| Masthoff [29] | 73.7 | (59.7–87.7) | 72.1 | (58.7–85.5) | 2.87 | (1.61–5.1) | 0.40 | (0.24–0.66) |
| Pooled | 4.44 | (3.48–5.67) | 0.26 | (0.18–0.37) | ||||
| Heterogeneity, Chi2 | 3.9 p = 0.560 | 7.4 p =0.196 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caffarelli, C.; Mastrorilli, C.; Santoro, A.; Criscione, M.; Procaccianti, M. Component-Resolved Diagnosis of Hazelnut Allergy in Children. Nutrients 2021, 13, 640. https://doi.org/10.3390/nu13020640
Caffarelli C, Mastrorilli C, Santoro A, Criscione M, Procaccianti M. Component-Resolved Diagnosis of Hazelnut Allergy in Children. Nutrients. 2021; 13(2):640. https://doi.org/10.3390/nu13020640
Chicago/Turabian StyleCaffarelli, Carlo, Carla Mastrorilli, Angelica Santoro, Massimo Criscione, and Michela Procaccianti. 2021. "Component-Resolved Diagnosis of Hazelnut Allergy in Children" Nutrients 13, no. 2: 640. https://doi.org/10.3390/nu13020640
APA StyleCaffarelli, C., Mastrorilli, C., Santoro, A., Criscione, M., & Procaccianti, M. (2021). Component-Resolved Diagnosis of Hazelnut Allergy in Children. Nutrients, 13(2), 640. https://doi.org/10.3390/nu13020640