
Modulating the Gut Microbiome in Multiple Sclerosis Management: A Systematic Review of Current Interventions

 , , ,
, , ,  ,
,  ,
, 
Abstract
1. Introduction
Gut-Microbiome-Based Therapeutic Interventions in MS
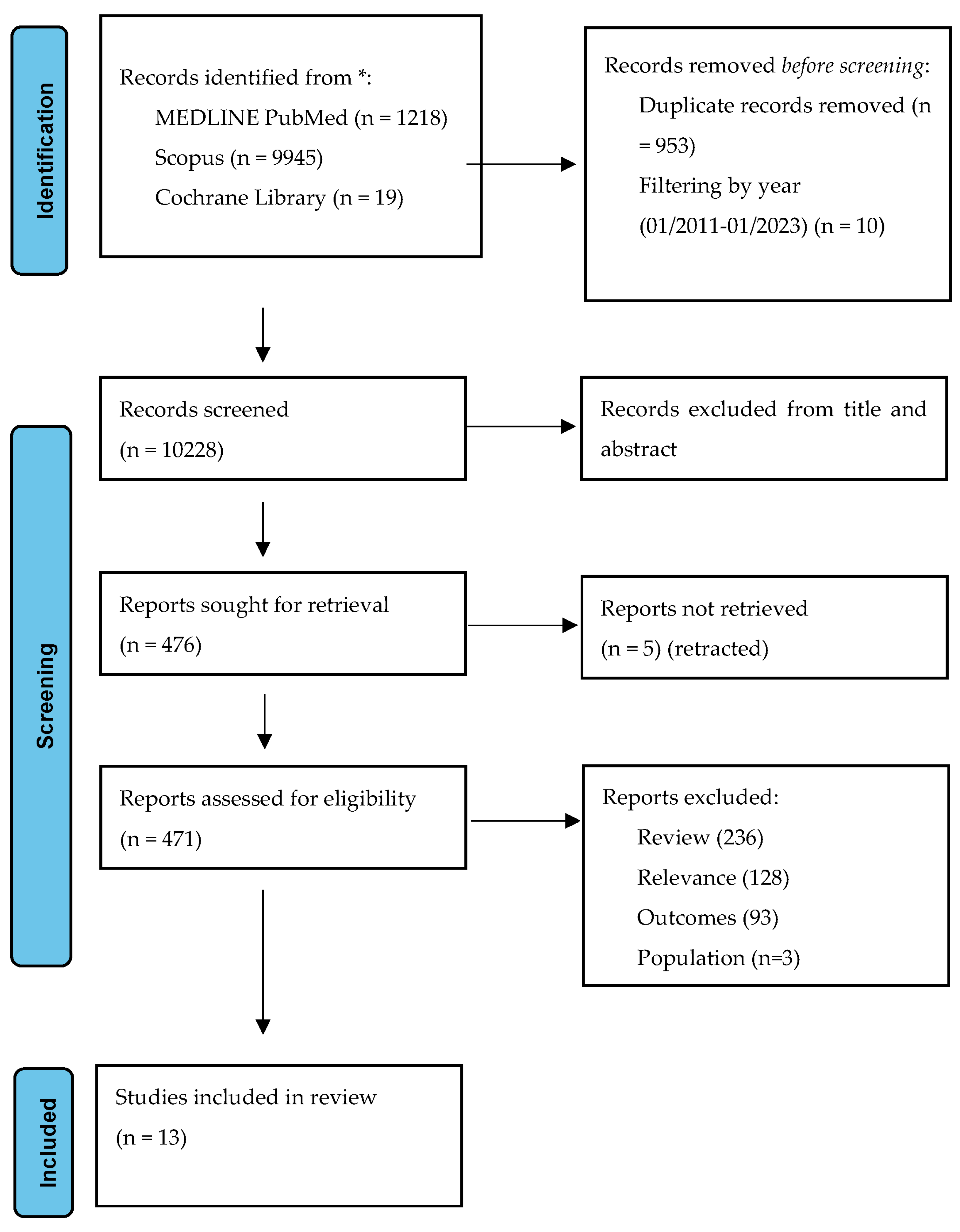
2. Methods
3. Results
3.1. Systematic Analysis
3.2. Dietary Modifications
3.3. Probiotic Nutritional Mixtures
3.4. Fecal Microbiota Transplantation
3.5. Intermittent Fasting
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nicol, B.; Salou, M.; Laplaud, D.; Wekerle, H. The autoimmune concept of multiple sclerosis. La Presse Médicale 2015, 44, e103–e112. [Google Scholar] [CrossRef]
- Ebringer, A.; Hughes, L.; Rashid, T.; Wilson, C. Acinetobacter Immune Responses in Multiple Sclerosis. Arch. Neurol. 2005, 62, 33–36. [Google Scholar] [CrossRef][Green Version]
- Kirby, T.; Ochoa-Repáraz, J. The Gut Microbiome in Multiple Sclerosis: A Potential Therapeutic Avenue. Med. Sci. 2018, 6, 69. [Google Scholar] [CrossRef]
- Adamczyk-Sowa, M.; Medrek, A.; Madej, P.; Michlicka, W.; Dobrakowski, P. Does the Gut Microbiota Influence Immunity and Inflammation in Multiple Sclerosis Pathophysiology? J. Immunol. Res. 2017, 2017, 7904821. [Google Scholar] [CrossRef]
- Esmaeil Amini, M.; Shomali, N.; Bakhshi, A.; Rezaei, S.; Hemmatzadeh, M.; Hosseinzadeh, R.; Eslami, S.; Babaie, F.; Aslani, S.; Torkamandi, S.; et al. Gut microbiome and multiple sclerosis: New insights and perspective. Int. Immunopharmacol. 2020, 88, 107024. [Google Scholar] [CrossRef]
- Chu, F.; Shi, M.; Lang, Y.; Shen, D.; Jin, T.; Zhu, J.; Cui, L. Gut Microbiota in Multiple Sclerosis and Experimental Autoimmune Encephalomyelitis: Current Applications and Future Perspectives. Mediat. Inflamm. 2018, 2018, 8168717. [Google Scholar] [CrossRef]
- Wang, Y.; Kasper, L.H. The role of microbiome in central nervous system disorders. Brain Behav. Immun. 2014, 38, 1–12. [Google Scholar] [CrossRef]
- Engelenburg, H.J.; Lucassen, P.J.; Sarafian, J.T.; Parker, W.; Laman, J.D. Multiple sclerosis and the microbiota: Progress in understanding the contribution of the gut microbiome to disease. Evol. Med. Public Health 2022, 10, 277–294. [Google Scholar] [CrossRef] [PubMed]
- Bronzini, M.; Maglione, A.; Rosso, R.; Matta, M.; Masuzzo, F.; Rolla, S.; Clerico, M. Feeding the gut microbiome: Impact on multiple sclerosis. Front. Immunol. 2023, 14, 1176016. [Google Scholar] [CrossRef]
- Fitzgerald, K.C.; Bhargava, P.; Smith, M.D.; Vizthum, D.; Henry-Barron, B.; Kornberg, M.D.; Cassard, S.D.; Kapogiannis, D.; Sullivan, P.; Baer, D.J.; et al. Intermittent calorie restriction alters T cell subsets and metabolic markers in people with multiple sclerosis. eBioMedicine 2022, 82, 104124. [Google Scholar] [CrossRef]
- Kohl, H.M.; Castillo, A.R.; Ochoa-Repáraz, J. The Microbiome as a Therapeutic Target for Multiple Sclerosis: Can Genetically Engineered Probiotics Treat the Disease? Diseases 2020, 8, 33. [Google Scholar] [CrossRef]
- Logsdon, A.F.; Erickson, M.A.; Rhea, E.M.; Salameh, T.S.; Banks, W.A. Gut reactions: How the blood–brain barrier connects the microbiome and the brain. Exp. Biol. Med. 2018, 243, 159–165. [Google Scholar] [CrossRef]
- Jayasinghe, M.; Prathiraja, O.; Kayani, A.M.A.; Jena, R.; Caldera, D.; Silva, M.S.; Singhal, M.; Pierre, J. The Role of Diet and Gut Microbiome in Multiple Sclerosis. Cureus 2022, 14, e28975. [Google Scholar] [CrossRef] [PubMed]
- Stoiloudis, P.; Kesidou, E.; Bakirtzis, C.; Sintila, S.-A.; Konstantinidou, N.; Boziki, M.; Grigoriadis, N. The Role of Diet and Interventions on Multiple Sclerosis: A Review. Nutrients 2022, 14, 1150. [Google Scholar] [CrossRef] [PubMed]
- Trentini, A.; Manfrinato, M.C.; Castellazzi, M.; Tamborino, C.; Roversi, G.; Volta, C.A.; Baldi, E.; Tola, M.R.; Granieri, E.; Dallocchio, F.; et al. TIMP-1 resistant matrix metalloproteinase-9 is the predominant serum active isoform associated with MRI activity in patients with multiple sclerosis. Mult. Scler. J. 2015, 21, 1121–1130. [Google Scholar] [CrossRef]
- Aristotelous, P.; Stefanakis, M.; Pantzaris, M.; Pattichis, C.S.; Calder, P.C.; Patrikios, I.S.; Sakkas, G.K.; Giannaki, C.D. The effects of specific omega-3 and omega-6 polyunsaturated fatty acids and antioxidant vitamins on gait and functional capacity parameters in patients with relapsing-remitting multiple sclerosis. Nutrients 2021, 13, 3661. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Mousavi-Shirazi-Fard, Z.; Mazloom, Z.; Izadi, S.; Fararouei, M. The effects of modified anti-inflammatory diet on fatigue, quality of life, and inflammatory biomarkers in relapsing-remitting multiple sclerosis patients: A randomized clinical trial. Int. J. Neurosci. 2021, 131, 657–665. [Google Scholar] [CrossRef]
- Saresella, M.; Mendozzi, L.; Rossi, V.; Mazzali, F.; Piancone, F.; LaRosa, F.; Marventano, I.; Caputo, D.; Felis, G.E.; Clerici, M. Immunological and Clinical Effect of Diet Modulation of the Gut Microbiome in Multiple Sclerosis Patients: A Pilot Study. Front. Immunol. 2017, 8, 1391. [Google Scholar] [CrossRef]
- Yadav, V.; Marracci, G.; Kim, E.; Spain, R.; Cameron, M.; Overs, S.; Riddehough, A.; Li, D.K.; McDougall, J.; Lovera, J.; et al. Low-fat, plant-based diet in multiple sclerosis: A randomized controlled trial. Mult. Scler. Relat. Disord. 2016, 9, 80–90. [Google Scholar] [CrossRef] [PubMed]
- Swidsinski, A.; Dörffel, Y.; Loening-Baucke, V.; Gille, C.; Göktas, Ö.; Reißhauer, A.; Neuhaus, J.; Weylandt, K.-H.; Guschin, A.; Bock, M. Reduced Mass and Diversity of the Colonic Microbiome in Patients with Multiple Sclerosis and Their Improvement with Ketogenic Diet. Front. Microbiol. 2017, 8, 1141. [Google Scholar] [CrossRef]
- Rahimlou, M.; Hosseini, S.A.; Majdinasab, N.; Haghighizadeh, M.H.; Husain, D. Effects of long-term administration of Multi-Strain Probiotic on circulating levels of BDNF, NGF, IL-6 and mental health in patients with multiple sclerosis: A randomized, double-blind, placebo-controlled trial. Nutr. Neurosci. 2022, 25, 411–422. [Google Scholar] [CrossRef]
- Kouchaki, E.; Tamtaji, O.R.; Salami, M.; Bahmani, F.; Daneshvar Kakhaki, R.; Akbari, E.; Tajabadi-Ebrahimi, M.; Jafari, P.; Asemi, Z. Clinical and metabolic response to probiotic supplementation in patients with multiple sclerosis: A randomized, double-blind, placebo-controlled trial. Clin. Nutr. 2017, 36, 1245–1249. [Google Scholar] [CrossRef] [PubMed]
- Tankou, S.K.; Regev, K.; Healy, B.C.; Cox, L.M.; Tjon, E.; Kivisakk, P.; Vanande, I.P.; Cook, S.; Gandhi, R.; Glanz, B.; et al. Investigation of probiotics in multiple sclerosis. Mult. Scler. 2018, 24, 58–63. [Google Scholar] [CrossRef]
- Tankou, S.K.; Regev, K.; Healy, B.C.; Tjon, E.; Laghi, L.; Cox, L.M.; Kivisäkk, P.; Pierre, I.V.; Hrishikesh, L.; Gandhi, R.; et al. A probiotic modulates the microbiome and immunity in multiple sclerosis. Ann. Neurol. 2018, 83, 1147–1161. [Google Scholar] [CrossRef]
- Salami, M.; Kouchaki, E.; Asemi, Z.; Tamtaji, O.R. How probiotic bacteria influence the motor and mental behaviors as well as immunological and oxidative biomarkers in multiple sclerosis? A double blind clinical trial. J. Funct. Foods 2019, 52, 8–13. [Google Scholar] [CrossRef]
- Engen, P.A.; Zaferiou, A.; Rasmussen, H.; Naqib, A.; Green, S.J.; Fogg, L.F.; Forsyth, C.B.; Raeisi, S.; Hamaker, B.; Keshavarzian, A. Single-Arm, Non-randomized, Time Series, Single-Subject Study of Fecal Microbiota Transplantation in Multiple Sclerosis. Front. Neurol. 2020, 11, 978. [Google Scholar] [CrossRef]
- Borody, T.; Leis, S.; Campbell, J.; Torres, M.; Nowak, A. Fecal Microbiota Transplantation (FMT) in Multiple Sclerosis (MS): 942. Am. J. Gastroenterol. 2011, 106, S352. [Google Scholar] [CrossRef]
- Cignarella, F.; Cantoni, C.; Ghezzi, L.; Salter, A.; Dorsett, Y.; Chen, L.; Phillips, D.; Weinstock, G.M.; Fontana, L.; Cross, A.H.; et al. Intermittent Fasting Confers Protection in CNS Autoimmunity by Altering the Gut Microbiota. Cell Metab. 2018, 27, 1222–1235.e6. [Google Scholar] [CrossRef]
- Fitzgerald, K.C.; Vizthum, D.; Henry-Barron, B.; Schweitzer, A.; Cassard, S.D.; Kossoff, E.; Hartman, A.L.; Kapogiannis, D.; Sullivan, P.; Baer, D.J.; et al. Effect of intermittent vs. daily calorie restriction on changes in weight and patient-reported outcomes in people with multiple sclerosis. Mult. Scler. Relat. Disord. 2018, 23, 33–39. [Google Scholar] [CrossRef]
- Lee, Y.K.; Menezes, J.S.; Umesaki, Y.; Mazmanian, S.K. Proinflammatory T-cell responses to gut microbiota promote experimental autoimmune encephalomyelitis. Proc. Natl. Acad. Sci. USA 2011, 108 (Suppl. S1), 4615–4622. [Google Scholar] [CrossRef]
- Kwon, H.-K.; Kim, G.-C.; Kim, Y.; Hwang, W.; Jash, A.; Sahoo, A.; Kim, J.-E.; Nam, J.H.; Im, S.-H. Amelioration of experimental autoimmune encephalomyelitis by probiotic mixture is mediated by a shift in T helper cell immune response. Clin. Immunol. 2013, 146, 217–227. [Google Scholar] [CrossRef]
- Lavasani, S.; Dzhambazov, B.; Nouri, M.; Fåk, F.; Buske, S.; Molin, G.; Thorlacius, H.; Alenfall, J.; Jeppsson, B.; Weström, B. A Novel Probiotic Mixture Exerts a Therapeutic Effect on Experimental Autoimmune Encephalomyelitis Mediated by IL-10 Producing Regulatory T Cells. PLoS ONE 2010, 5, e9009. [Google Scholar] [CrossRef]
- Budhram, A.; Parvathy, S.; Kremenchutzky, M.; Silverman, M. Breaking down the gut microbiome composition in multiple sclerosis. Mult. Scler. J. 2017, 23, 628–636. [Google Scholar] [CrossRef]
- Braniste, V.; Al-Asmakh, M.; Kowal, C.; Anuar, F.; Abbaspour, A.; Tóth, M.; Korecka, A.; Bakocevic, N.; Ng, L.G.; Kundu, P.; et al. The gut microbiota influences blood-brain barrier permeability in mice. Sci. Transl. Med. 2014, 6, 263ra158. [Google Scholar] [CrossRef]
- Farrokhi, V.; Nemati, R.; Nichols, F.C.; Yao, X.; Anstadt, E.; Fujiwara, M.; Grady, J.; Wakefield, D.; Castro, W.; Donaldson, J.; et al. Bacterial lipodipeptide, Lipid 654, is a microbiome-associated biomarker for multiple sclerosis. Clin. Transl. Immunol. 2013, 2, e8. [Google Scholar] [CrossRef] [PubMed]
- Joscelyn, J.; Kasper, L.H. Digesting the emerging role for the gut microbiome in central nervous system demyelination. Mult. Scler. J. 2014, 20, 1553–1559. [Google Scholar] [CrossRef] [PubMed]
- Piccio, L.; Stark, J.L.; Cross, A.H. Chronic calorie restriction attenuates experimental autoimmune encephalomyelitis. J. Leukoc. Biol. 2008, 84, 940–948. [Google Scholar] [CrossRef] [PubMed]
- Riccio, P.; Rossano, R. Nutrition Facts in Multiple Sclerosis. ASN Neuro 2015, 7, 175909141456818. [Google Scholar] [CrossRef] [PubMed]
- Yokote, H.; Miyake, S.; Croxford, J.L.; Oki, S.; Mizusawa, H.; Yamamura, T. NKT Cell-Dependent Amelioration of a Mouse Model of Multiple Sclerosis by Altering Gut Flora. Am. J. Pathol. 2008, 173, 1714–1723. [Google Scholar] [CrossRef]
- Reynolds, A.N.; Akerman, A.; Kumar, S.; Diep Pham, H.T.; Coffey, S.; Mann, J. Dietary fibre in hypertension and cardiovascular disease management: Systematic review and meta-analyses. BMC Med. 2022, 20, 139. [Google Scholar] [CrossRef] [PubMed]
- Racke, M.K.; Frohman, E.M.; Frohman, T. Pain in Multiple Sclerosis: Understanding Pathophysiology, Diagnosis, and Management Through Clinical Vignettes. Front. Neurol. 2022, 12, 799698. [Google Scholar] [CrossRef] [PubMed]
- Lopez, J.; Grinspan, A. Fecal Microbiota Transplantation for Inflammatory Bowel Disease. Gastroenterol. Hepatol. (N. Y.) 2016, 12, 374–379. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Author | Year | Region | Study Type | MS/Intervention | Control | Intervention Type |
|---|---|---|---|---|---|---|
| Borody | 2011 | USA | CR | 3 | FMT | |
| Salami | 2015 | Iran | RCT | 24 | 24 | PNM |
| Yadav | 2016 | USA | RCT | 32 | 29 | DP |
| Saresella | 2017 | Italy | RCT | 10 | 10 | DP |
| Swidsinski | 2017 | Germany | CC | 25 | 14 | DP |
| Kouchaki | 2017 | Iran | RCT | 30 | 30 | PNM |
| Tankou | 2018 | USA | CC | 9 | 13 | PNM |
| Tankou | 2018 | USA | CC | 9 | 13 | PNM |
| Cignarella | 2018 | USA | RCT | 8 | 8 | IF |
| Fitzgerald | 2018 | USA | RCT | 24 | 12 | IF |
| Fard | 2020 | Iran | RCT | 50 | 50 | DP |
| Rahimlou | 2022 | Iran | RCT | 35 | 35 | PNM |
| Engen | 2022 | USA | CR | 1 | FMT |
| Dietary Protocols | |||
|---|---|---|---|
| First Author | Sample-Duration | Results | Limitations |
| Fard et al. [19]. | 100 RRMS 50 participants on anti-inflammatory diet 50 participants in the control group—healthy diet 12 weeks | Significant improvements: MFIS scores (p = 0.001) MSQoL-54: physical component (p = 0.015) Mental component (p = 0.003) in the diet group compared to the control group (p < 0.05) significant increase in IL-4 levels (0.05). No significant changes were observed in IL-17 and hs-CRP levels (p < 0.05) |
|
| Saresella et al. [20] | 20 RRMS 10 participants on HV/LP diet 10 participants on Western diet 12 months | rr and EDSS reduced 12 m after HV/LP diet initiation |
|
| Yadav et al. [21] | 61 RRMS 32 participants on very-low-fat/plant-based diet 29 controls Patients randomized in very-low-fat/plant-based diet or placed on waitlist (control group) 1 year | Significant improvements in measures of fatigue, BMI, and metabolic biomarkers (p = 0.001) |
|
| Swidsinski et al. [22] | 25 RRMS 10 participants on Ketogenic diet 15 controls 6 months | In patients with MS, Roseburia, Bacteroides, Faecalibacterium prausnitzii probes were diminished the most. The effects of a ketogenic diet led to further reduction in bacterial concentrations and diversity. | Although the concentrations and the biodiversity of colonic microbiota are strong markers of the intensity of the microbial metabolism, the shifts in bacterial groups per se do not reveal the exact metabolic changes taking place. |
| Probiotic Nutritional Mixtures | |||
| First Author | n | Results | Limitations |
| Rahimlou et al. [23] | 70 RRMS 35 participants taking probiotic capsule (12 weeks) 35 participants taking placebo (6 months) | BDNF titer increase (0.001), IL-6 titer decrease (0.001) BDI decrease (p = 0.001) FSS decrease (0.007) | Probiotic effects of HPA axis were not taken into account. |
| Salami et al. [27] | 48 patients with MS 24 participants taking probiotics 24 participants taking placebo 16 weeks | Significant differences in EDSS, depression, anxiety, and stress levels (p = <0.001) Also, significant differences in CRP, IL-6, IL-10, NO (p = <0.001) | Difficulty in counting microbial flora on the patients with MS. |
| Kouchaki et al. [24] | 60 RRMS 30 participants taking probiotic capsule 30 participants taking placebo 12 weeks | Probiotic vs. placebo EDSS decrease (0.001) DASS decrease. (0.001) GHQ decrease (0.001) MDI decrease (0.001) Probiotic vs. placebo hs-CRP decrease (p = 0.01) MDAI decrease (p = 0.04) NO increase (p = 0.002) Serum insulin, HOMA-IR, HOMA-B, HDL/TOTAL CHOL. Ratio decrease (0.001, p = 0.001, 0.001, p = 0.02) QUICKI, HDL increase (0.001) |
|
| Tankou et al. [25] | 9 RRMS (7 GA), 13 HCs LBS probiotic mixture 2 months | LBS administration taxa changes in both MS and HCs microbiota (0.05) KEGG changes (0.05) Stool metabolomics profile changes associated with decreased expression of MS risk allele HLA.DPB1 (p = 0.078) HLA.DPA1 (p = 0.055) Anti-inflammatory PBMC immune response (p = 0.094) | Small sample size. |
| Tankou et al. [26] | 9 RRMS (7 GA), 13 HCs VSL3 probiotic mixture 2m | Increases in several species (p = 0.048); induction of anti-inflammatory IR (p = 0.08); VSL3 discontinued. Induction of pro-inflammatory IR (p = 0.033) | Small sample size. |
| Fecal Microbiota Transplantation | |||
| First Author | n | Results | Limitations |
| Engen et al. [28] | 1 active RRMS | BDNF titer increase (0.001) 12MSWS score decrease. (0.05) | Single case report. |
| Borody et al. [29] | 3 “atypical” MS cases | Case 1: 5 FMT improvement in mobility and urinary function Case 2: 10 FMT improvement in mobility and sensory function Case 3: 5 FMT improvement in bowel and mobility function | 3 case reports. |
| Intermittent Fasting | |||
| First Author | n | Results | Limitations |
| Cignarella et al. [30] | 16 RRMS (in relapse) 8 IF 8 control diet 2 weeks | EDSS score decrease. No changes in SDMT and MSFC scores (no p values provided) | Pilot trial with short duration. |
| Fitzgerald et al. [31] | 36 RRMS 12 Daily CR diet 12 IF CR diet 12 Weight-stable diet 8 weeks | FAMS total No change between groups p = 0.63 FAMS—emotional wellbeing/depression No change between groups p = 0.22 FAMS—thinking/fatigue. p = 0.53 PSQI No change between groups p = 0.38 |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsogka, A.; Kitsos, D.K.; Stavrogianni, K.; Giannopapas, V.; Chasiotis, A.; Christouli, N.; Tsivgoulis, G.; Tzartos, J.S.; Giannopoulos, S. Modulating the Gut Microbiome in Multiple Sclerosis Management: A Systematic Review of Current Interventions. J. Clin. Med. 2023, 12, 7610. https://doi.org/10.3390/jcm12247610
Tsogka A, Kitsos DK, Stavrogianni K, Giannopapas V, Chasiotis A, Christouli N, Tsivgoulis G, Tzartos JS, Giannopoulos S. Modulating the Gut Microbiome in Multiple Sclerosis Management: A Systematic Review of Current Interventions. Journal of Clinical Medicine. 2023; 12(24):7610. https://doi.org/10.3390/jcm12247610
Chicago/Turabian StyleTsogka, Anthi, Dimitrios K. Kitsos, Konstantina Stavrogianni, Vasileios Giannopapas, Athanasios Chasiotis, Niki Christouli, Georgios Tsivgoulis, John S. Tzartos, and Sotirios Giannopoulos. 2023. "Modulating the Gut Microbiome in Multiple Sclerosis Management: A Systematic Review of Current Interventions" Journal of Clinical Medicine 12, no. 24: 7610. https://doi.org/10.3390/jcm12247610
APA StyleTsogka, A., Kitsos, D. K., Stavrogianni, K., Giannopapas, V., Chasiotis, A., Christouli, N., Tsivgoulis, G., Tzartos, J. S., & Giannopoulos, S. (2023). Modulating the Gut Microbiome in Multiple Sclerosis Management: A Systematic Review of Current Interventions. Journal of Clinical Medicine, 12(24), 7610. https://doi.org/10.3390/jcm12247610