
Cardiac Arrest Occurring in High-Rise Buildings: A Scoping Review


 , ,
, ,  and
and 
Abstract
:
1. Introduction
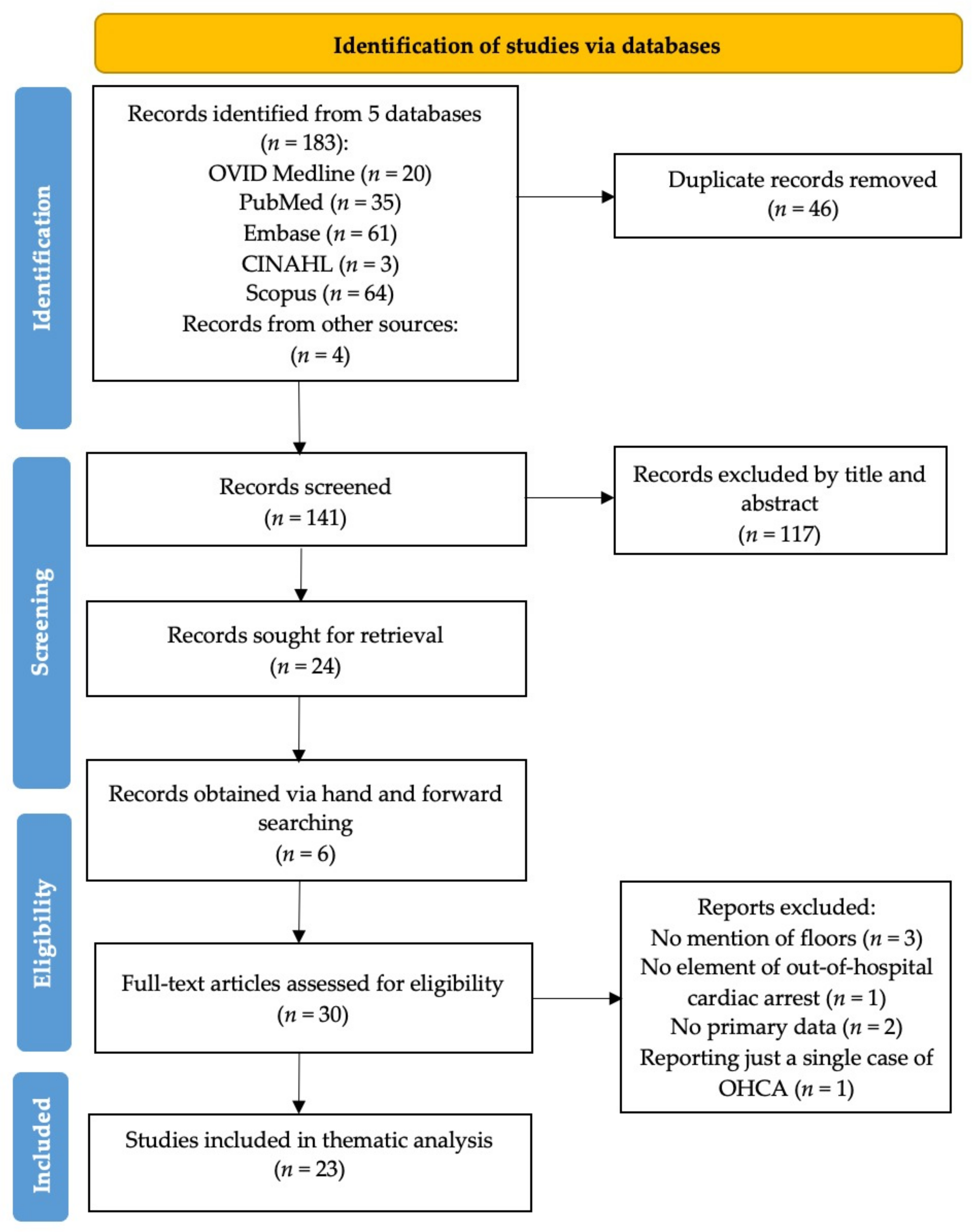
2. Materials and Methods
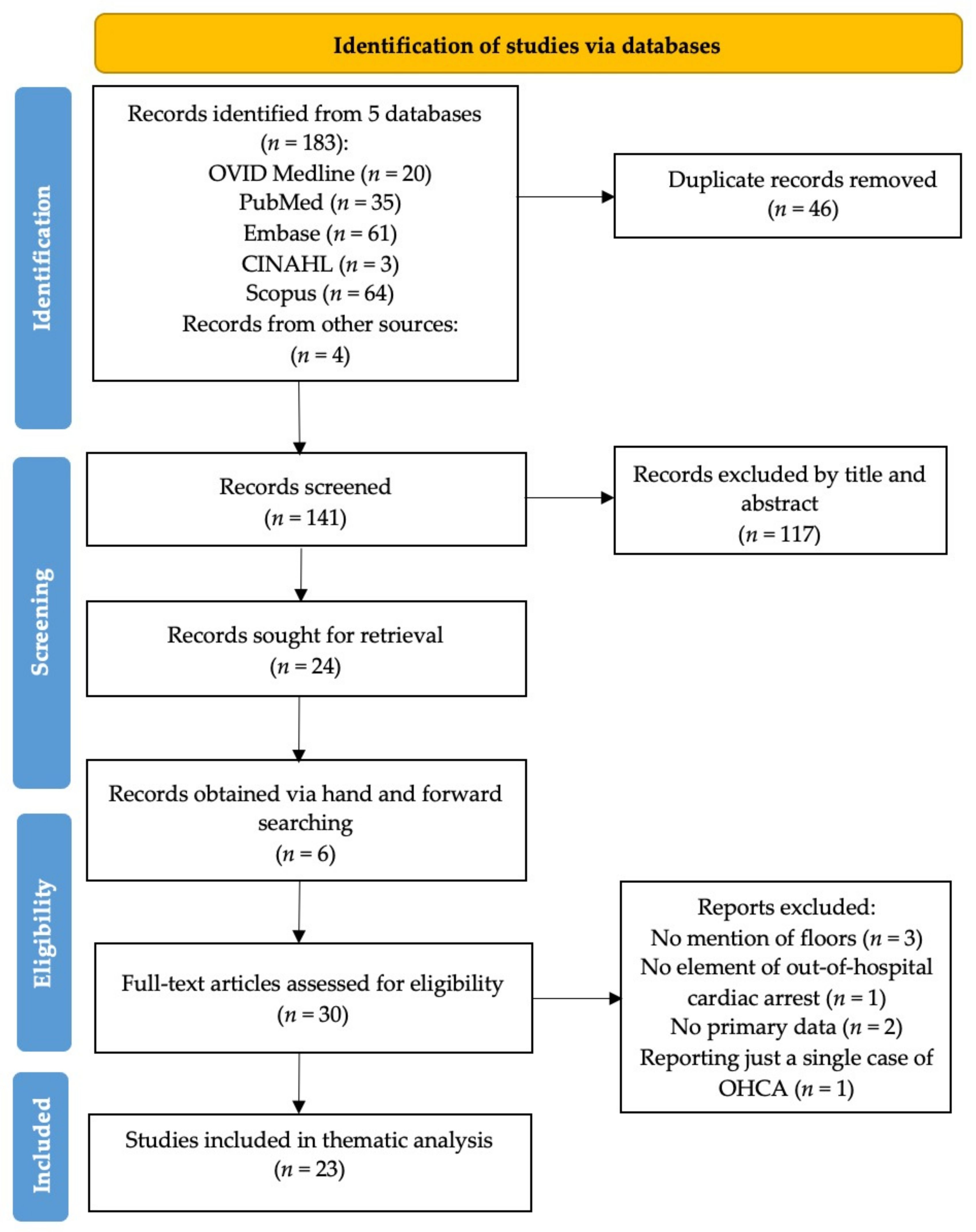
2.1. Search Strategy
2.2. Selection Criteria
2.3. Data Extraction
2.4. Ethical Considerations
3. Results
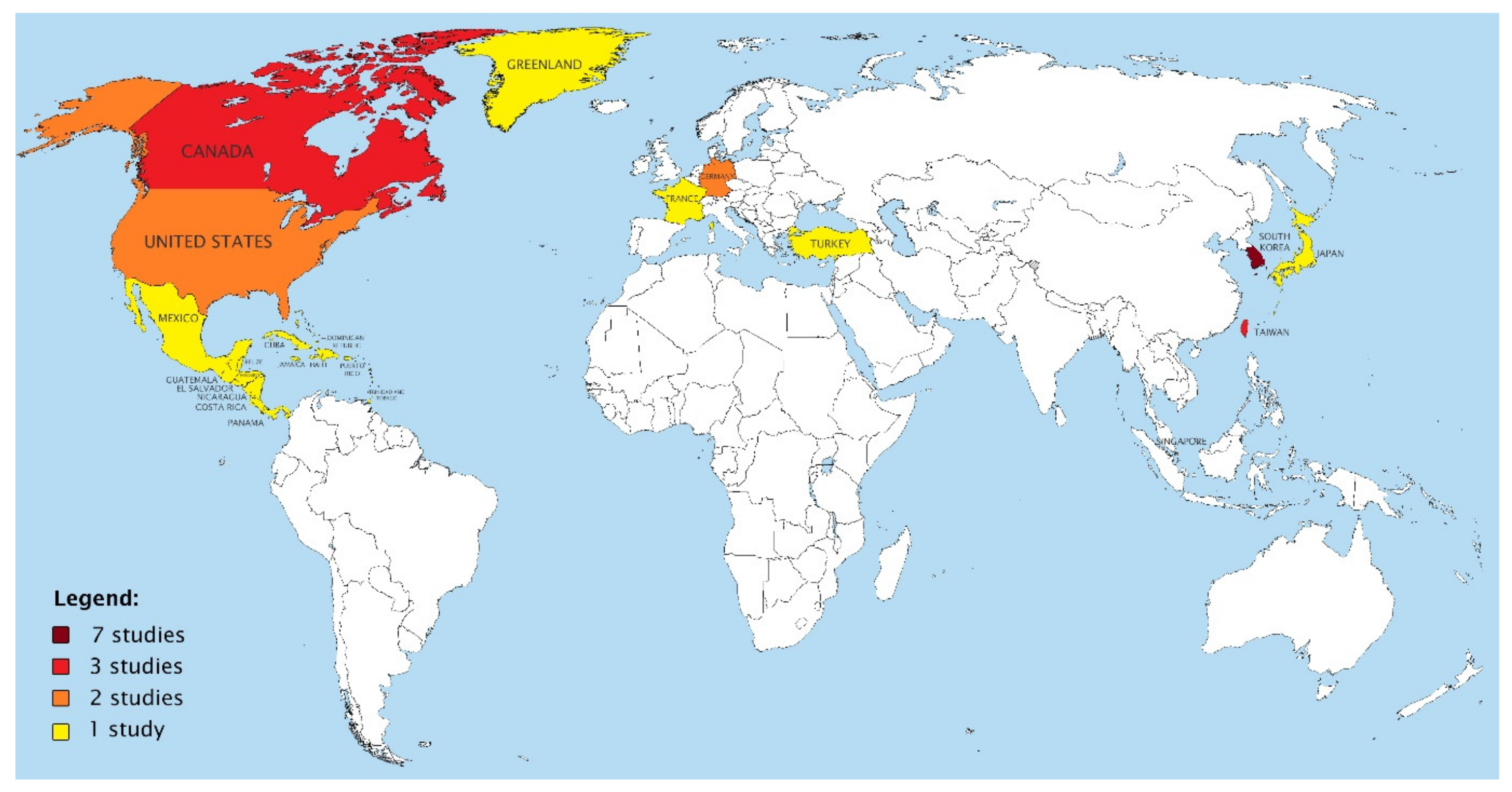
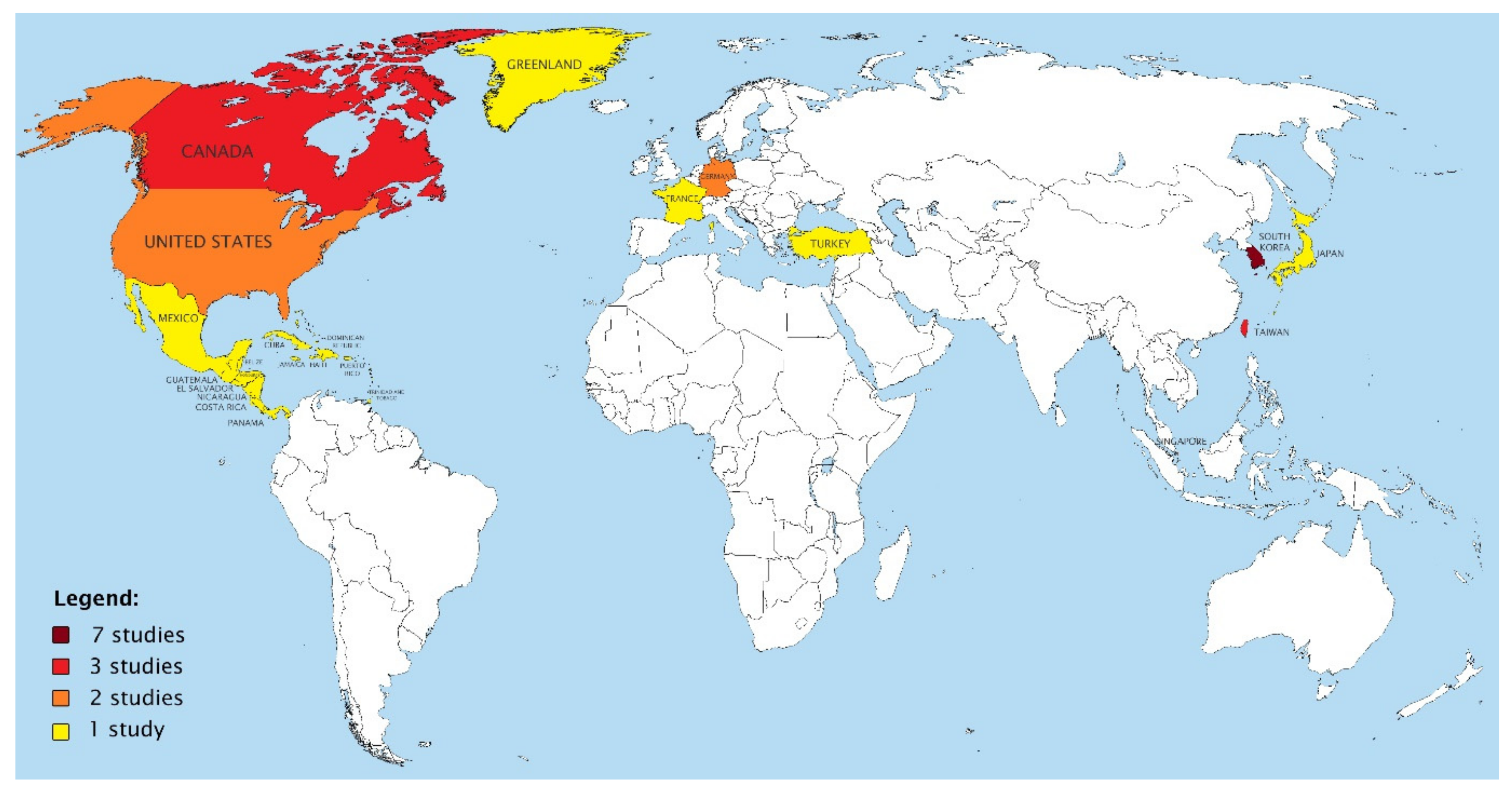
3.1. Geographical Distribution of Studies
3.2. Unique Challenges of High-Rise Settings
3.3. Prognosis and Outcomes
3.4. Approaches and Solutions
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Berdowski, J.; Berg, R.A.; Tijssen, J.G.; Koster, R.W. Global incidences of out-of-hospital cardiac arrest and survival rates: Systematic review of 67 prospective studies. Resuscitation 2010, 81, 1479–1487. [Google Scholar] [CrossRef] [PubMed]
- Cummins, R.O.; Ornato, J.P.; Thies, W.H.; Pepe, P.E. Improving survival from sudden cardiac arrest: The “chain of survival” concept. A statement for health professionals from the Advanced Cardiac Life Support Subcommittee and the Emergency Cardiac Care Committee, American Heart Association. Circulation 1991, 83, 1832–1847. [Google Scholar] [CrossRef] [Green Version]
- Deakin, C.D. The chain of survival: Not all links are equal. Resuscitation 2018, 126, 80–82. [Google Scholar] [CrossRef] [PubMed]
- Silverman, R.A.; Galea, S.; Blaney, S.; Freese, J.; Prezant, D.J.; Park, R.; Pahk, R.; Caron, D.; Yoon, S.; Epstein, J.; et al. The “vertical response time”: Barriers to ambulance response in an urban area. Acad. Emerg. Med. 2007, 14, 772–778. [Google Scholar] [PubMed]
- Morrison, L.J.; Angelini, M.P.; Vermeulen, M.J.; Schwartz, B. Measuring the EMS patient access time interval andthe impact of responding to high-rise buildings. Prehosp. Emerg. Care 2005, 9, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Chan, T.C. Rise and shock: Optimal defibrillator placement in a high-rise building. Prehosp. Emerg. Care 2017, 21, 309–314. [Google Scholar] [CrossRef]
- Lian, T.W.; Allen, J.C.; Ho, A.F.; Lim, S.H.; Shahidah, N.; Ng, Y.Y.; Doctor, N.; Leong, B.S.; Gan, H.N.; Mao, D.R.; et al. Effect of vertical location on survival outcomes for out-of-hospital cardiac arrest in Singapore. Resuscitation 2019, 139, 24–32. [Google Scholar] [CrossRef]
- Park, J.S.; Chang, W.J.; Kim, H.J.; Choi, K.J.; Lee, B.C. Delays in the EMS Response Time and the Evacuation of Patients in High-Rise Buildings in a New Town in Korea. J. Korean Soc. Emerg. Med. 2010, 21, 119–124. [Google Scholar]
- Zhang, X.Q. The trends, promises and challenges of urbanisation in the world. Habitat Int. 2016, 54, 241–252. [Google Scholar] [CrossRef]
- United Nations, Department of Economic and Social Affairs, Population Division (2018). World Urbanization Prospects: The 2018 Revision, Online Edition. Available online: https://esa.un.org/unpd/wup/ (accessed on 10 July 2021).
- Bekgöz, B.; Şan, İ.; Ergin, M. Quality comparison of the manual chest compression and the mechanical chest compression during difficult transport conditions. J. Emerg. Med. 2020, 58, 432–438. [Google Scholar] [CrossRef]
- Kim, J.; Brewster, L.; Maria, S.; Moon, J. The effect of a mechanical compression device and supraglottic airway on flow time: A simulation study of out-of-hospital cardiac arrest in a high-rise building. Emerg. Med. Int. 2018, 2018, 7246964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, C.-B.; Chen, K.-F.; Chien, C.-Y.; Kuo, C.-W.; Goh, Z.N.L.; Seak, C.-K.; Seak, J.C.-Y. Shoulder strap fixation of LUCAS-2 to facilitate continuous CPR during non-supine (stair) stretcher transport of OHCAs patients. Sci. Rep. 2021, 11, 9858. [Google Scholar] [CrossRef]
- Chi, A.; Cho, Y.; Lee, H.; Lee, J.; Cho, G.C.; Kim, W.Y.; Kim, M.C. The influence of vertical location of cardiac arrest and application of mechanical cardiopulmonary resuscitation device on out of hospital cardiac arrest in a community: A retrospective observational study. J. Korean Soc. Emerg. Med. 2016, 27, 530–539. [Google Scholar]
- Chi, C.-Y.; Renhao, D.M.; Yang, C.-W.; Yang, M.-F.; Lee, H.-J.; Lee, C.-H.; Shih, F.F.-Y.; Ong, E.H.M.; Ko, P.C.-I. Comparison of Chest Compression Quality between Transfer Sheet and Stretcher Use for Transporting out-of-Hospital Cardiac Arrest Patients in a High-Rise Building-A Randomized and Open-Label Cross-over Design. Prehosp. Emerg. Care 2021, 25, 370–376. [Google Scholar] [CrossRef]
- Choi, H.J.; Moon, H.J.; Jeong, W.J.; Kim, G.W.; Woo, J.H.; Lee, K.M.; Choi, H.J.; Park, Y.J.; Lee, C.A. Effect of the Floor Level on the Probability of a Neurologically Favorable Discharge after Cardiac Arrest according to the Event Location. Emerg. Med. Int. 2019, 2019, 9761072. [Google Scholar] [CrossRef] [Green Version]
- Conway, A.B.; McDavid, A.; Emert, J.M.; Kudenchuk, P.J.; Stubbs, B.A.; Rea, T.D.; Yin, L.; Olsufka, M.; McCoy, A.M.; Sayre, M.R. Impact of building height and volume on cardiac arrest response time. Prehosp. Emerg. Care 2016, 20, 212–219. [Google Scholar] [CrossRef]
- Drennan, I.R.; Strum, R.P.; Byers, A.; Buick, J.E.; Lin, S.; Cheskes, S.; Hu, S.; Morrison, L.J. Out-of-hospital cardiac arrest in high-rise buildings: Delays to patient care and effect on survival. CMAJ 2016, 188, 413–419. [Google Scholar] [CrossRef] [Green Version]
- Drinhaus, H.; Nüsgen, S.; Adams, N.; Wetsch, W.A.; Annecke, T. Rescue under ongoing CPR from an upper floor: Evaluation of three different evacuation routes and mechanical and manual chest compressions: A manikin trial. Scand. J. Trauma Resusc. Emerg. Med. 2020, 28, 16. [Google Scholar] [CrossRef] [Green Version]
- Heidet, M.; Da Cunha, T.; Brami, E.; Mermet, E.; Dru, M.; Simonnard, B.; Lecarpentier, E.; Chollet-Xémard, C.; Bergeron, C.; Khalid, M.; et al. EMS Access Constraints And Response Time Delays For Deprived Critically Ill Patients Near Paris, France: Study examines emergency response times for critically ill patients who live in an area of low socioeconomic status near Paris, France. Health Aff. 2020, 39, 1175–1184. [Google Scholar] [CrossRef] [PubMed]
- Jörgens, M.; Königer, J.; Kanz, K.-G.; Birkholz, T.; Hübner, H.; Prückner, S.; Zwissler, B.; Trentzsch, H. Testing mechanical chest compression devices of different design for their suitability for prehospital patient transport-a simulator-based study. BMC Emerg. Med. 2021, 21, 18. [Google Scholar] [CrossRef]
- Kim, T.H.; Hong, K.J.; Do, S.S.; Kim, C.H.; Song, S.W.; Song, K.J.; Ro, Y.S.; Ahn, K.O.; Jang, D.B. Quality between mechanical compression on reducible stretcher versus manual compression on standard stretcher in small elevator. Am. J. Emerg. Med. 2016, 34, 1604–1609. [Google Scholar] [CrossRef]
- Kobayashi, D.; Kitamura, T.; Kiyohara, K.; Nishiyama, C.; Hayashida, S.; Fujii, T.; Izawa, J.; Shimamoto, T.; Matsuyama, T.; Hatakeyama, T.; et al. High-rise buildings and neurologically favorable outcome after out-of-hospital cardiac arrest. Int. J. Cardiol. 2016, 224, 178–182. [Google Scholar] [CrossRef]
- Lateef, F.; Anantharaman, V. Delays in the EMS response to and the evacuation of patients in high-rise buildings in Singapore. Prehosp. Emerg. Care 2000, 4, 327–332. [Google Scholar] [CrossRef]
- Lee, D.E.; Ryoo, H.W.; Ahn, J.Y.; Moon, S.; Kim, J.K.; Kim, Y.J.; Park, J.B.; Kim, J.H.; Lee, K.W.; Jin, S.C. Does the placement of automated external defibrillators affect first responders’ willingness to perform cardiopulmonary resuscitation in high-rise residential buildings? Resuscitation 2018, 29, 557–567. [Google Scholar]
- Liao, E.C.-W.; Mao, D.R.; Yang, C.-W.; Chi, C.-Y.; Yang, M.-F.; Lee, H.-J.; Leed, C.-H.; Marcus, O.E.H.; Ko, P.C.-I. Simulation study comparing quality of conventional vs active compression-decompression vs load-distribution band CPR in a confined elevator: The MECHER trial. Resuscitation 2019, 142, e59–e60. [Google Scholar] [CrossRef]
- Sinden, S.; Heidet, M.; Scheuermeyer, F.; Kawano, T.; Helmer, J.S.; Christenson, J.; Grunau, B. The association of scene-access delay and survival with favourable neurological status in patients with out-of-hospital cardiac arrest. Resuscitation 2020, 155, 211–218. [Google Scholar] [CrossRef]
- Sohn, Y.; Cho, Y.; Cho, G.; Consortium, K.C.A. Neurological outcomes after an out-of-hospital cardiac arrest among people living in high-rise buildings in South Korea. Eur J Emerg Med. 2020, 27, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Tay, P.J.M.; Pek, P.P.; Fan, Q.; Ng, Y.Y.; Leong, B.S.-H.; Gan, H.N.; Mao, D.R.; Chia, M.Y.C.; Cheah, S.O.; Doctor, N.; et al. Effectiveness of a community based out-of-hospital cardiac arrest (OHCA) interventional bundle: Results of a pilot study. Resuscitation 2020, 146, 220–228. [Google Scholar] [CrossRef] [PubMed]
- Mason, C.J. Method of Operating Elevators during Emergency Situations. Google Patents. U.S. Patent US8230980B2, 31 July 2012. [Google Scholar]
- Nehme, Z.; Ball, J.; Stephenson, M.; Walker, T.; Stub, D.; Smith, K. Effect of a resuscitation quality improvement programme on outcomes from out-of-hospital cardiac arrest. Resuscitation 2021, 162, 236–244. [Google Scholar] [CrossRef]
- Ryu, H.H.; Moore, J.C.; Yannopoulos, D.; Lick, M.; McKnite, S.; Shin, S.D.; Kim, T.Y.; Metzger, A.; Rees, J.; Tsangaris, A.; et al. The Effect of Head Up Cardiopulmonary Resuscitation on Cerebral and Systemic Hemodynamics. Resuscitation 2016, 102, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Pepe, P.E.; Scheppke, K.A.; Antevy, P.M.; Crowe, R.P.; Millstone, D.; Coyle, C.; Prusansky, C.; Garay, S.; Ellis, R.; Fowler, R.L.; et al. Confirming the Clinical Safety and Feasibility of a Bundled Methodology to Improve Cardiopulmonary Resuscitation Involving a Head-Up/Torso-Up Chest Compression Technique. Crit., Care Med. 2019, 47, 449–455. [Google Scholar] [CrossRef] [PubMed]
- Pepe, P.E.; Aufderheide, T.P.; Lamhaut, L.; Davis, D.P.; Lick, C.J.; Polderman, K.H.; Scheppke, K.A.; Deakin, C.D.; O’Neil, B.J.; van Schuppen, H.; et al. Rationale and Strategies for Development of an Optimal Bundle of Management for Cardiac Arrest. Crit Care Explor. 2020, 2, e0214. [Google Scholar] [CrossRef] [PubMed]
- Aufderheide, T.P.; Frascone, R.J.; Wayne, M.A.; Mahoney, B.D.; Swor, R.A.; Domeier, R.M.; Olinger, M.L.; Holcomb, R.G.; Tupper, D.E.; Yannopoulos, D.; et al. Standard cardiopulmonary resuscitation versus active compression-decompression cardiopulmonary resuscitation with augmentation of negative intrathoracic pressure for out-of-hospital cardiac arrest: A randomised trial. Lancet 2011, 377, 301–311. [Google Scholar] [CrossRef] [Green Version]
- Ng, W.M.; De Souza, C.R.; Pek, P.P.; Shahidah, N.; Ng, Y.Y.; Arulanandam, S.; White, A.E.; Leong, B.S.-H.; Ong, M.E.H. myResponder smartphone application to crowdsource basic life support for out-of-hospital cardiac arrest: The Singapore experience. Prehosp. Emerg. Care 2021, 25, 388–396. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.M.; Wilson, M.H.; Ghorbangholi, A.; Hartley-Sharpe, C.; Gwinnutt, C.; Dicker, B.; Perkins, G. The use of trained volunteers in the response to out-of-hospital cardiac arrest–the GoodSAM experience. Resuscitation 2017, 121, 123–126. [Google Scholar] [CrossRef] [Green Version]
- Greif, R.; Perkins, G.; Semeraro, F.; Soar, J.; Truhlář, A.; Georgiou, M.; Nolan, J.; Böttiger, B.; Grünfeld, M.; Van De Voorde, P.; et al. Kids Save Lives–ERC position statement on school children education in CPR.:“Hands that help–Training children is training for life”. Resuscitation 2016, 105, A1–A3. [Google Scholar]
- Kok, Y. SCDF-Grab Tie-Up Has 64 Drivers Trained as Lifesavers, 50 Private-Hire Vehicles Fitted with AEDs [Internet]. The Straits Times. 2021. Available online: https://www.straitstimes.com/singapore/50-grab-vehicles-fitted-with-aeds-to-respond-to-cardiac-arrests-with-drivers-trained-as (accessed on 19 August 2021).

{kind=link}
{kind=link}
{kind=link}
| Author, Year | Country and Study Setting | Study Design (Sample Size) | Study Outcomes | Interventions and Control Groups for Comparison | Results | Conclusions |
|---|---|---|---|---|---|---|
| Bekgoz et al., 2020 [11] | Ankara, capital of Turkey Training centre # floors = 3 Starting floor: 3rd Ending floor: 1st | Manikin trial (n = 10 female and 10 male paramedics) | Compression rate (compressions/min) Compression depth (mm) Hands-on time (%) | Manual CPR and manual chest compression device (MCCD) | Median chest compression rate: Higher for manual CPR at 142 compressions/min than the MCCD at 102.3 compressions/min (p < 0.01) Median chest compression depth: More shallow for manual CPR at 25.2 mm than MCCD at 52.0 mm (p < 0.001) Hands-on time: 92.0% for manual CPR vs. 100% for MCCD (p = 0.09) | While transporting the patient simulator manikin to the lower floor, it was found that MCCD achieved high-quality CPR targets recommended by resuscitation guidelines in terms of compression rate, depth, and hands-on time. |
| Chan, 2017 [6] | Toronto, Canada | Mathematical model of a high-rise building (n floors, single elevator and single AED) OHCA occurrences modelled using independent Poisson processes on each floor | Average override-to-arrival response distance, E(DOA) Maximum response distance, max(DOA) | Elevator-based AED vs. lobby-based AED Arrest floor I = 0 vs. arrest floor I ≠ 0. | Average response distance was shorter for elevator-based AED if the number of floors exceeded ¾ of the ratio of ground-floor OHCA risk to above-ground floor risk plus 0.5. If not, a lobby-based AED had a shorter response distance. If the risk of OHCA was equal for each floor, an elevator-based AED would have a shorter average response distance. | Cardiac arrests in a tall building may experience faster response from an elevator-based AED, whereas a building with much higher risk on the ground floor compared to any above-ground floor would be better off with a lobby-based AED. |
| Chen et al., 2021 [15] | Taoyuan, Taiwan Environmental conditions: 5-storey building without an elevator. Start: 3rd floor End: 1st/ground floor | Nonrandomised manikin simulation trial (n = 20 EMTs placed in 10 pairs) 2 simulation runs per experimental arm with Resusci Anne First Aid full body manikin (60 kg) | CPR quality | Experimental group: mechanical compressions with adapted LUCAS-2 device strapped to manikin before transport down the stairs on a stair stretcher Control group: manual chest compressions with manikin strapped directly to stair stretcher | There were no statistically significant differences in CPR quality between experimental and control groups for the overall resuscitation period. Chest compression fraction: Statistically significantly higher in LUCAS-2 experimental group at 0.76 (0.75, 0.78) vs. 0.63 (0.62, 0.66) for the control group | LUCAS-2 mechanical CPR provides better chest compression fractions than manual CPR in stairwells. |
| Chi et al., 2016 [16] | Gangdong-gu, Seoul, South Korea | Retrospective observational study (n = 119 rescue records) Qualitative survey (n = 54 paramedics) | ROSC rate Survival to hospital admission | Vertical location of arrest Manual CPR vs. mechanical CPR | ROSC: Significantly lower likelihood of ROSC in a vertical location of cardiac arrest (OR: 0.40, 95% CI 0.17–0.98, p = 0.044) Survival to hospital admission: No statistically significant differences between OHCA patients from ground floors vs. nonground floors Qualitative survey: 85.2% felt there was a lower quality of chest compressions for patients above ground floor, and 93.1% felt that mechanical CPR devices could circumvent this | Vertical location of cardiac arrest scene independently affects ROSC rates in OHCA. |
| Chi et al., 2020 [17] | Taipei, Taiwan Conventional passenger elevator: Length = 1.6 m Width = 1.5 m Height = 2.2 m Start: 13th floor End: 1st/ground floor | Randomised open-label cross-over manikin trial (n = 72 simulation runs with EMTs in 12 3-person crews) | Primary outcomes: mean compression depth, chest compression fraction (CCF) Secondary outcomes: Percentage of fully released compressions, compressions with adequate rate, hand position | Before entering elevator: Chest compressions and defibrillation on scene Intervention group: Move manikin to transfer sheet (TS) and enter elevator Stretcher groups: Move manikin to stretcher and adjust to either 45 or 90 degree incline | Mean compression depth: Significantly deeper for TS (54.4 ± 4.2) compared to stretcher groups at 45 degrees (39.6 ± 7.2) and at 90 degrees (40.6 ± 8.3) Chest compression fraction: No significant differences between intervention and control groups Compressions with adequate recoil: No significant differences between intervention and control groups Compressions with adequate depth: Significantly higher for TS at 51% (23.8–74.8) compared to stretcher groups at 45 degrees (19.5, 5.8–29.5) and 90 degrees (25.5, 20.0–34.3) Time interval for moving patient from scene to elevator: Significantly shorter for TS at 22.5 s (18.7–26.8) compared to stretcher groups at 45 degrees (45.3 s, 39.9–52.1) and 90 degrees (47.7 s, 42.1–65.0) | TS is better than stretcher with regards to chest compression depth and transport time. TS should be used for high-rise building transport of OHCA patients. Rescuers need to be aware to allow full chest recoil. |
| Choi et al., 2019 [18] | Korea, 18 urban and suburban areas Home = apartment, condominium, house, townhouse. Public place = everything else High floor ≥3rd Low floor = 2nd and lower | Retrospective cohort study (n = 6355 OHCA cases) | Primary outcome: Neurologically favourable outcome after a high-floor OHCA, measured at hospital discharge (CPC 1 or 2) Secondary outcomes: ROSC, call-to-scene time and call-to-patient time | High-floor vs. low-floor groups | Neurologically favourable discharge: Significantly lower for high-floor OHCA if the incident occurred in a public place (aOR, 0.58; 95% CI: 0.37–0.89) Significantly higher for high floor OHCA if incident occurred at home (aOR, 1.40; 95% CI: 0.96–2.03) ROSC:Significantly higher for home OHCAs occurring at high floors (551, 25.39%) compared to lower floors (421, 21.22%), p = 0.002 Time intervals: The call-to-scene time was a median of 7 min, which was shorter on a high floor for events in both homes and public places. Call-to-patient time for home events was significantly longer on a high floor (a median of 9 min). | Nature of setting (home vs. public) affects EMS response times to OHCA in high-rise buildings. Patient’s prognosis is more likely to be affected by the structure and use of the building, rather than the floor height where the CA event occurred. |
| Conway et al., 2016 [19] | Seattle, Washington, United States. 2-tiered EMS response system with BLS fire engine and ALS ambulance Buildings were categorised as short (<25ft), medium (26–64 ft), and tall (>64 ft)Building volumes were categorised as small (<60,000 ft3), midsize (60,000–1,202,600 ft3) and large (>1,202,600 ft3) | Retrospective observational study (n = 3065 OHCA cases that occurred indoors and without prior deployment of defibrillator) | Call-to-curb interval: call to on-scene time Curb-to-defibrillation interval: on-scene to defibrillation on time Call-to-defibrillation interval | Time-intervals against BHC Time-intervals against BVC | Median call-to-curb intervals by building height and volume: Significantly lower for tall buildings (3.96) compared to short and medium-height buildings (4.73, 4.27), p < 0.01 Significantly lower for larger-volume buildings (4.05) compared to smaller-volume buildings (4.87), p < 0.01 Median curb-to-defib intervals by building height and volume: Significantly greater for tall buildings (3.11) compared to short and medium-height buildings (1.97, 2.62), p < 0.01 Significantly greater for larger-volume buildings (3.01) compared to smaller- and medium-volume buildings (1.90, 2.58), p < 0.01 Median call-to-defib intervals by building height and volume: No significant differences between any groups | Buildings with greater height and volume have significantly longer curb-to-defib times and significantly shorter call-to-curb times. The hypothesis that taller or larger-volume buildings cause poorer outcomes was not supported by this study’s results. |
| Drennan et al., 2016 [20] | Toronto, Canada OHCAs that occurred within Toronto city and the regional municipality of Peel. Floor of patient contact: High ≥ 3rd Low ≤ 2nd Private locations: apartments, condominiums, houses, or townhouses. Others = public/other | Retrospective observational study (n = 7842 OHCA cases) | Primary outcome: Survival to hospital discharge Secondary outcomes: Delay to patient contact, use of AEDs by bystanders | Low floors (<3 floors) vs. high floors (3 floors and higher) | Survival to hospital discharge: Significantly lower for patients residing on the third floor and above (2.6%) as compared to below the third floor (4.2%), p = 0.002 Time interval between arrival and patient contact:Significantly greater for higher floors compared with lower floors (4.9 ± 2.6 vs. 3.0 ± 2.0, p = 0.01) Use of AED: No significant differences although the rate of use was very low regardless of floor level (0.3% for lower floors and 0.4% for higher floors) | OHCA on high floors had lower rates of survival to hospital discharge, and no survivors above the 25th floor. This is likely due to longer intervals from arrival of 911 responder to patient contact, and lower rates of initial shockable rhythm for high floor patients. |
| Drinhaus et al., 2020 [21] | Brühl, North Rhine-Westphalia, Germany.Test setting: apartment (5th floor), evacuated to ground floor via lift, turntable ladder, or staircase | Manikin trial (n = 40 paramedics | CPR quality measures:Compression depth and frequency | 6 experimental arms: Lift and manual CPR Lift and mechanical CPR Ladder and manual CPR Ladder and mechanical CPR Staircase and manual CPR Staircase and mechanical CPR | Percentage of guideline-compliant CPR compression depth and frequency for lift route: No significant differences for depth. For frequency, significantly lower manual CPR compared to mechanical CPR (58 ± 34 vs. 94 ± 2, p = 0.02) Percentage of guideline-compliant CPR compression depth and frequency for ladder route: Significantly lower for manual CPR compared to mechanical CPR (depth: 18 ± 21 vs. 92 ± 7, p = 0.04; frequency: 61 ± 17 vs. 96 ± 1, p = 0.04) Percentage of guideline-compliant CPR compression depth and frequency for staircase route: Significantly lower for manual CPR compared to mechanical CPR (depth: 25 ± 16 vs. 86 ± 28, p = 0.02; frequency: 22 ± 30 vs. 96 ± 2, p = 0.02) | Mechanical CPR is more effective in delivering consistent high-quality CPR regardless of floor level. Manual CPR results in inconsistent CPR quality particularly for ladder and stairs and may pose possible hazards to staff. |
| Heidet et al., 2020 [22] | Val-de-Marne, Paris, France Population (2012) of 1,365,039 inhabitants, mean population density of 5572 inhabitants per square kilometer SAMU (Service d’aide médicale urgente) dispatches 6 hospital-based physician-staffed EMS ambulances (Service mobile d’urgence et reanimation or SMUR) | Multicentre prospective cohort study n = 2298 cases of SMUR dispatch | Primary Outcome: Overall EMS response time interval (time from vehicle start to patient contact) Secondary Outcomes: Vehicle time interval Patient access time interval ROSC Survival on scene Survival to 30 days | Area-level socioeconomic status assessed at census level. SES evaluated using French version of European Deprivation Index (French-EDI) Quintile 1: least deprived Quintile 5: most deprived | There were more floors in the most deprived areas, along with more frequent access barriers and younger age of patients. EMS response times were all significantly affected by reason for dispatch, dispatch time and location, number of floors in a patient’s dwelling, among other related barriers. Dispatch time, location, number of floors, and post-ambulance stop barriers were associated with patient access time interval. Significant associations between poor OHCA outcomes were only found for the most deprived areas (Quintile 5) In Quintile 5, 28.5% had 1–3 floors while 21.7% had 4 and more floors. 33.1% were multistorey residential buildings. | The more deprived an area was, the longer EMS response times were due to the higher prevalence of EMS access constraints. |
| Jorgens et al., 2021 [23] | Munchen, Germany | Simulator-based randomised trial 9 paramedics 4 emergency physicians 4-person transport teams to carry mannequin with mCPR through a predefined 10-step transport route | Stability of device (displacement measurement, correct pressure point) Compliance to ERC cardiac massage guidelines (50–60 mm compression depth, 30:2 compression:ventilation ratio, 100–120 bpm) Questionnaire to evaluate each mCPR device using VAS (0 = totally unsuitable, 10 = ideally suited) Questionnaire to rank perceived physical effort using modified BORG CR-10 scale (0 = no exertion/breathlessness, 10 = maximum exertion/breathlessness forces stop) | Control Route: Stationary mCPR at the beginning and end of transport Experimental Route: Transport with soft stretcher and staircase Vehicular trips with turntable ladder, rescue basket Ambulance Transport Loading and Unloading 4 different mCPR devices:animax mono, AutoPulse, corpuls CPR, LUCAS 2 | Correct pressure point recorded for 2 out of 15,962 compressions (0.013%) during the application of corpuls CPR in soft stretcher transport Compliance to compression depth had greater scattering during basic resuscitation across all mCPR devices Use of all mCPR devices showed a high level of user satisfaction regardless of route category | It is crucial to check stability of mCPR devices regularly and correct connection to the patient under different transport circumstances. |
| Kim et al., 2016 [24] | Seoul, Korea Simulation scenarios made up of 3-personnel teams of EMTS and resuscitation manikin placed on the 6th floor of a multistorey building using a small elevator | Randomised crossover manikin simulation trial 9 EMTs in teams of three 44 simulation scenarios with at least 21 trials for each protocol | Primary outcome: No-flow fraction during simulation scenario Secondary outcome: Proportion of chest compressions with adequate compression depth Proportion of chest compressions with adequate compression rate | Preparation: Manual CPR for 3 cycles of 2 min each Standard stretcher group (SS-CPR): Movement of manikin to standard stretcher ETI with manual CPR Standard stretcher transformed to wheelchair position during elevator transport Reducible stretcher group (RS-CPR): Movement of manikin to reducible stretcher and mounting of mCPR ETI with mCPR Reducible stretcher hinged during elevator transport to accommodate head-up, leg-raised position | Median no-flow fraction (%): Higher in SS-CPR vs. RS-CPR (32.9 (31.1–34.9) vs. 31.6 (30.8–32.7), p = 0.14) Proportion of chest compressions with adequate depth (%): Significantly higher in RS-CPR vs. SS-CPR (97.8 (88.6–98.6) vs. 83.7 (81.3–84.6), p < 0.01) Proportion of chest compression with adequate rate (%): Significantly higher in RS-CPR vs. SS-CPR (95.9 (90.6–98.9) vs. 92.9 (86.1–93.9), p = 0.05) | There was significantly higher CPR quality when a reducible stretcher was used with mCPR during vertical transport in a high-rise building, specifically for nonflow fraction and proportion of adequate chest compression depth and rate. |
| Kim et al., 2018 [12] | Jeonju, South Korea Simulation environment was a residential unit located in a 42-storey (180 m) high-rise building. Elevator had a 15-person capacity and travelled at 180 m/min. Door width was 900 mm and internal area was 1600 × 1500 mm. Flexible stretcher (DA-02768 Delti medical, Taiwan) was used for transport within the building | Randomised manikin simulation trial n = 24 professional EMS providers 4 scenarios Phase 1: initiating until performing CPR according to 1 of 4 scenarios Phase 2: leaving the scene to entering elevator Phase 3: entering till exiting elevator Phase 4: exiting elevator till loading into ambulance | Average compression depth and rate Incomplete chest recoil ratio Total flow time fraction and flow time fraction by phase of trial Duration of compression pauses | Initial preparation: 5 cycles of 30 compressions and 2 ventilations with defibrillation MAB scenario: 30 manual compressions and 2 BVM ventilations MAS scenario: 30 manual compressions and 2 SGA ventilations MED scenario: continuous mCPR compressions and BVM ventilation MES scenario: continuous mCPR compressions and SGA ventilation Post-scenario:transport to elevator on flexible stretcher, loading into ambulance | No-flow time due to artificial ventilation: Significantly shorter in SGA groups (MAS 49.6 ± 6.0 and MES 52.8 ± 7.9) as compared to BVM groups (MAB 66.2 ± 12.6 and MEB 73.6 ± 9.2) Interruptions due to manikin movement: Significantly shorter in mechanical groups (MEB 3.4±4.3 and MES 3.3 ± 7.9) as compared to manual groups (MAB 76.8 ± 14.7 and MAS 70.2 ± 10.9) Flow time: Highest in MES groups through phases 2, 3 and 4 Flow time fraction by phase: Highest in MES throughout phases 1 to 4 | The quality of manual compressions can be maintained when providing CPR for cardiac arrest patients in a high-rise setting. The use of both a mechanical CPR device and a supraglottic airway increased flow time the most effectively. |
| Kobayashi et al., 2016 [25] | Osaka, Japan | Prospective cohort study (n = 2979 OHCA patients) High-floor group: n = 1094 Low-floor group: n = 1885 | Primary outcome: 1-month survival with neurologically favourable outcome (CPC 1 or 2) Secondary outcomes: Prehospital ROSCAdmission to hospital Survival to one month | High-floor group: OHCA patients residing on 3 or more floors Low-floor group: OHCA patients residing on fewer than 3 floors | Neurologically intact survival at 1-month (CPC 1 or 2): Significantly lower for high-floor group than low-floor group (30 (2.7%) vs. 91 (4.8%), p = 0.005) Prehospital ROSC: Significantly lower for high-floor group than low-floor group (77 (7.0%) vs. 188 (10.0%), p = 0.007) Hospital admission: Significantly lower in high-floor group than low-floor group (218 (19.9%) vs. 457 (24.2%), p = 0.007) One-month survival: Significantly lower in high-floor group than low-floor group (54 (4.9%) vs. 138 (7.3%), p = 0.011) | Survival at one month with neurologically favourable outcome was significantly lower for OHCA patients in the high-floor group as compared to the lower-floor group. |
| Lateef et al., 2000 [26] | Singapore A high-rise building was taken to be one that crew had to ascend at least one flight of stairs i.e., 2nd storey and higher. Ground-level building did not involve any stair climbing. | Prospective cohort study (n = 150 ambulance runs) | Arrival-to-patient contact delay | Time interval between T4 (time ambulance arrives at scene) and T5 (time at patient’s side) Time interval between T6 (time of leaving location) and T7 (time when ambulance starts journey to hospital) | Mean delay between T4 and T5: Significantly higher in high-rise group as compared to ground-level group. (2.49 ± 0.98 vs. 1.02 ± 1.41, 95% CI: 1.20, 1.75 min, p = 0.0106) Mean delay between T6 and T7: Significantly higher in high-rise group as compared to ground-level group. (3.24 ± 1.58 vs. 1.27 ± 0.71, 95% CI: 1.68, 2.04 min, p = 0.0098) Questionnaire findings:
| High-rise buildings lead to significant delays to patient access and evacuation to hospital. |
| Lee et al., 2018 [27] | Daegu, South Korea Definition of high-rise not specified | Cross-sectional survey (n = 1445 high-rise apartment managers) | Willingness of apartment managers to perform CPR and use an AED | Apartment managers who worked in apartments with AEDs vs. those who worked in apartments without AEDs | AED placement in high-rise apartments increased willingness to CPR (OR, 1.33; 95% CI: 1.04–1.71) and increased willingness to use an AED (OR, 1.39; 95% CI: 1.10–1.75). | Apartment managers will benefit from AED placement in high-rise buildings and refresher courses on CPR to maintain CPR skills. |
| Lian et al., 2019 [7] | Singapore | Retrospective cohort study (n = 5678 OHCA cases from 01 January 2011 to 31 December 2014) | Primary outcome: 30-day post-cardiac arrest survival or survival to hospital discharge | Floor/floor groups: −4 to −1, 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16–20, 21–25, >25 | Survival rates: 4.5% for 4 basement floors (−4 to −1) vs. 6.2% for ground floor 2.7% at floor 2, declining to 0.7% at floor 6 Both linear and quadratic floor effects remained significant after adjusting for other confounders (age, bystander witnessed, EMS response time). | There is a significant U-shape relationship between vertical location and OHCA survival, even after adjusting for other OHCA variables. Midrange floors had lower rates of survival to 30 days as compared to basements, ground floor and extreme upper floors. |
| Liao et al., 2019 [28] | Taipei, Taiwan Elevator setting with standard stretcher | Triple-arm, prospective manikin simulation study (n = 12 paramedic teams and 44 simulation runs) | No flow-fraction Time to first shock Percentage change in compression depth between supine and head-up stretcher positions | Conventional CPR (C-CPR) Load-distributing band mCPR (LDB) mCPR with Autopulse Active compression-decompression (ACD) mCPR with LUCAS-2 | No-flow fraction: Significantly lower in ACD group (9.6%, 95%CI: 8.5–10.8%) than C-CPR group (28.6%, 95%CI: 25.9–31.4%) and LDB group (14.9%, 95%CI: 13.6–16.2%) Percentage change in compression depth during stretcher position change: Significantly lower in ACD group (2.6%, 95%CI: 1.8–3.3%) than C-CPR (31.2%, 95%CI: 25.7–36.8%) group and LDB group (7.1%, 95%CI: 5.9–8.3%), p < 0.001 | ACD-CPR is recommended for use in an elevator to improve CPR quality as it was shown to outperform other options in terms of no-flow fraction and percentage change in compression. |
| Morrison et al., 2005 [5] | Toronto, Ontario, Canada | Observational study (n = 118 EMS calls) Single third-party EMT-P observer followed on ambulance runs and recorded data. | Patient access time interval: defined as time of ambulance arrival at scene (vehicle stops) to time of physical contact with patient (at patient’s side) Barriers to paramedic movement (qualitative) | Fewer than 3 floors above or below ground compared with 3 or more floors above ground | Median patient access time interval: Significantly higher for patients located 3 or more floors above ground (2.73 (2.22, 3.03)) as compared to lower levels (1.25 (1.07, 1.55). Significantly greater when patients resided in apartments (2.12 (1.70, 2.50)) as compared with all other buildings (1.02 (0.65, 1.47)), p < 0.001. Barriers in apartment buildings (n = 40): security code entry requirements (67%), lack of directional signs (82.6%), inability to fit stretcher into elevator (67.9%) | Ambulance calls to places three or more floors above ground had significantly longer patient access time intervals, which make up a substantial part of total EMS response time. |
| Park et al., 2010 [8] | Seoul, South Korea | Prospective study n = 35 ambulance runs n = 11 for ground-level group and n = 24 for high-rise group | Time interval between T4 (time ambulance arrives at scene) and T5 (time at patient’s side) Time interval between T6 (time of leaving location) and T7 (time when ambulance starts journey to hospital) | High-rise group (more than 1 floor above ground) vs. ground-level group | Median time interval (min) between T4 and T5: Significantly higher for the high-rise group as compared to the ground-level group (2.08 vs. 0.34, p = 0.000) Median time interval (min) between T6 and T7: Significantly higher for the high-rise group as compared to the ground-level group (3.08 vs. 1.00, p = 0.000) Narrow elevators were cited as the most frequent access barrier (100%) in all of the 24 high-rise ambulance runs | There were significantly longer time delays in the access and evacuation of patients in high-rise buildings. |
| Silverman et al., 2007 [4] | New York City, United States | Prospective observational case series (n = 449 ambulance calls between July 2001 and December 2003) | Time interval from arrival on-scene to patient’s side | Different location settings: multistorey residence, private home (<4 storeys), office building, street, train station, store/mall | Time interval (min) by location: Significantly longer for multistorey residential buildings as compared to private homes or residential areas with 3 or fewer storeys (2.8 vs. 1.3, p < 0.0001) Time interval (min) by building height: Significantly longer for office, apartment or medical facilities 10 storeys and higher (3.2 (IQR, 2.7–4.2)) as compared to buildings less than 10 storeys (2.3 (IQR, 1.6–3.1)), p < 0.0001. | Patients located in multistorey buildings are subjected to longer vertical response time intervals, which accounts for a big portion of the overall EMS response time in a large metropolitan area. |
| Sinden et al., 2020 [29] | North America | Secondary analysis of the dataset from the Resuscitation Outcomes Consortium “Trial of Continuous or Interrupted Chest Compressions During CPR” 24,685 case data included in study | Primary outcome: neurologically intact survival at hospital discharge (mRS 3 or less) Secondary outcome: survival to hospital discharge | Curb-to-Care (CTC) interval quartiles (seconds) defined as time interval between EMS vehicle arrival at scene and patient’s side 63–115 116–180 ≥181 compared with ≤62 | Neurologically intact survival at hospital discharge: Lower rates of neurologically intact survival for longer CTC quartiles (63–115, 116–180 and ≥181) with adjusted ORs 0.95, (95% CI 0.83–1.09); 0.77 (95% CI 0.66–0.89); 0.66 (95% CI 0.56–0.77) respectively. Survival to hospital discharge: Lower rates of survival to hospital discharge for longer CTC quartiles (63–115, 116–180 and ≥181) with adjusted ORs 0.92, (95% CI 0.81–1.05); 0.79 (95% CI 0.68–0.89); 0.67 (95% CI 0.58–0.78) respectively. | Lower CTC intervals improve patient outcomes in out-of-hospital cardiac arrests. A 2-min CTC interval could be a quality improvement target. |
| Sohn et al., 2020 [30] | Seoul, South Korea | Retrospective study (n = 1541 OHCA patients between 1 Oct 2015 and 30 Jun 2018) | Primary outcome: Neurologically intact survival to hospital discharge (CPC 1 or 2)Secondary outcomes: prehospital ROSC, hospital admission, hospital discharge | First and second floor (n = 887) compared with third floor and above (n = 654) | Neurologically intact survival at hospital discharge: Significantly lower rate for third floor and above as compared to first and second floors (5.2% vs. 11.1%, p < 0.001) Prehospital ROSC: Significantly lower rate for third floor and above as compared to first and second floors (9.9% vs. 16.4%, p < 0.001) Median EMS on-scene time (time interval between scene arrival and leaving for hospital): Significantly longer for third floor and above as compared to first and second floors (16 min vs. 12 min, p < 0.001) | Patients residing on higher floors have less favourable outcomes in out-of-hospital cardiac arrest. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, M.X.; Yeo, A.N.W.T.; Ong, M.E.H.; Smith, K.; Lim, Y.L.; Lin, N.H.; Tan, B.; Arulanandam, S.; Ho, A.F.W.; Ng, Q.X. Cardiac Arrest Occurring in High-Rise Buildings: A Scoping Review. J. Clin. Med. 2021, 10, 4684. https://doi.org/10.3390/jcm10204684
Han MX, Yeo ANWT, Ong MEH, Smith K, Lim YL, Lin NH, Tan B, Arulanandam S, Ho AFW, Ng QX. Cardiac Arrest Occurring in High-Rise Buildings: A Scoping Review. Journal of Clinical Medicine. 2021; 10(20):4684. https://doi.org/10.3390/jcm10204684
Chicago/Turabian StyleHan, Ming Xuan, Amelia Natasha Wen Ting Yeo, Marcus Eng Hock Ong, Karen Smith, Yu Liang Lim, Norman Huangyu Lin, Bobo Tan, Shalini Arulanandam, Andrew Fu Wah Ho, and Qin Xiang Ng. 2021. "Cardiac Arrest Occurring in High-Rise Buildings: A Scoping Review" Journal of Clinical Medicine 10, no. 20: 4684. https://doi.org/10.3390/jcm10204684
APA StyleHan, M. X., Yeo, A. N. W. T., Ong, M. E. H., Smith, K., Lim, Y. L., Lin, N. H., Tan, B., Arulanandam, S., Ho, A. F. W., & Ng, Q. X. (2021). Cardiac Arrest Occurring in High-Rise Buildings: A Scoping Review. Journal of Clinical Medicine, 10(20), 4684. https://doi.org/10.3390/jcm10204684