
Digital Intervention for Problematic Smartphone Use


 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
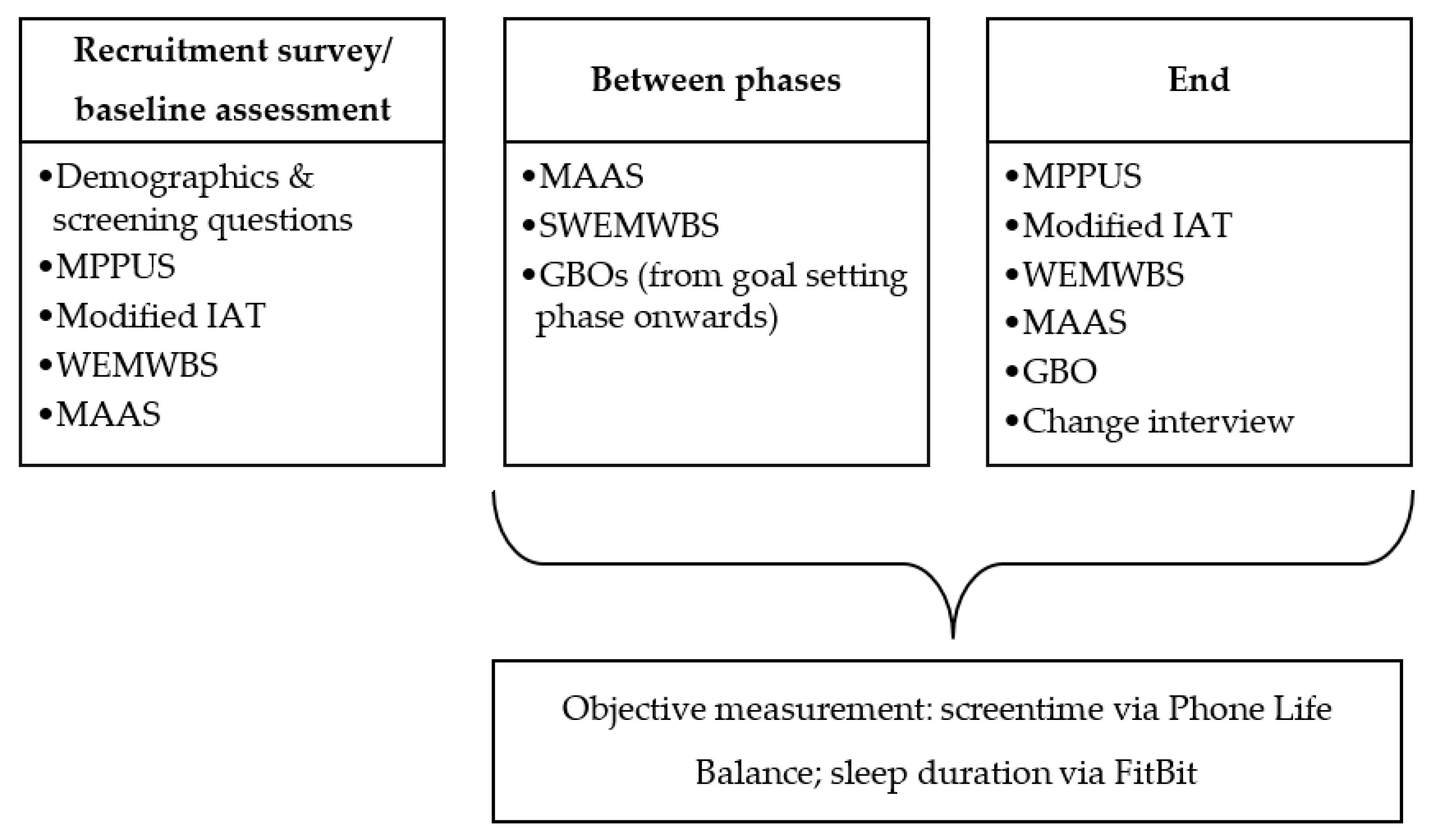
2.1. Design
2.2. Participants
2.3. Measures
2.3.1. Technology Use
Phone Life Balance
Mobile Phone Problem Use Scale (MPPUS)
Modified Internet Addiction Test (IAT)
2.3.2. Wellbeing and Related Constructs
The Warwick Edinburgh Mental Wellbeing Scale (WEMWBS)
The Short Warwick Edinburgh Mental Wellbeing Scale (SWEMWBS)
The Mindful Attention Awareness Scale (MAAS)
FitBit Charge 2
2.3.3. Idiosyncratic Measurement
Goal-Based Outcomes (GBOs)
Client Change Interview
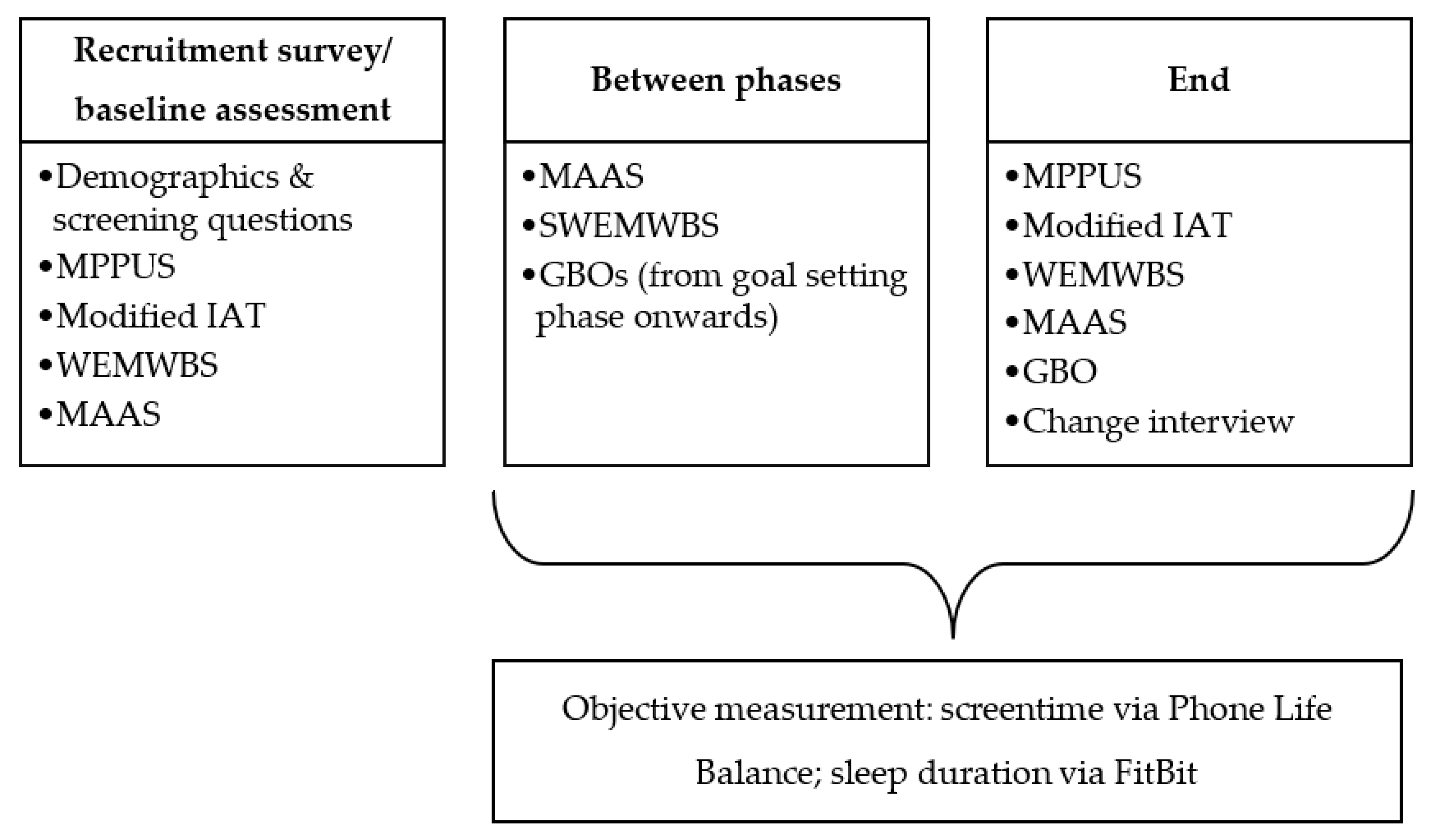
2.4. Procedure
2.4.1. Baseline
2.4.2. Intervention
2.5. Final Assessment and Change Interview
2.6. Analysis
3. Results
3.1. Overall Engagement and Change
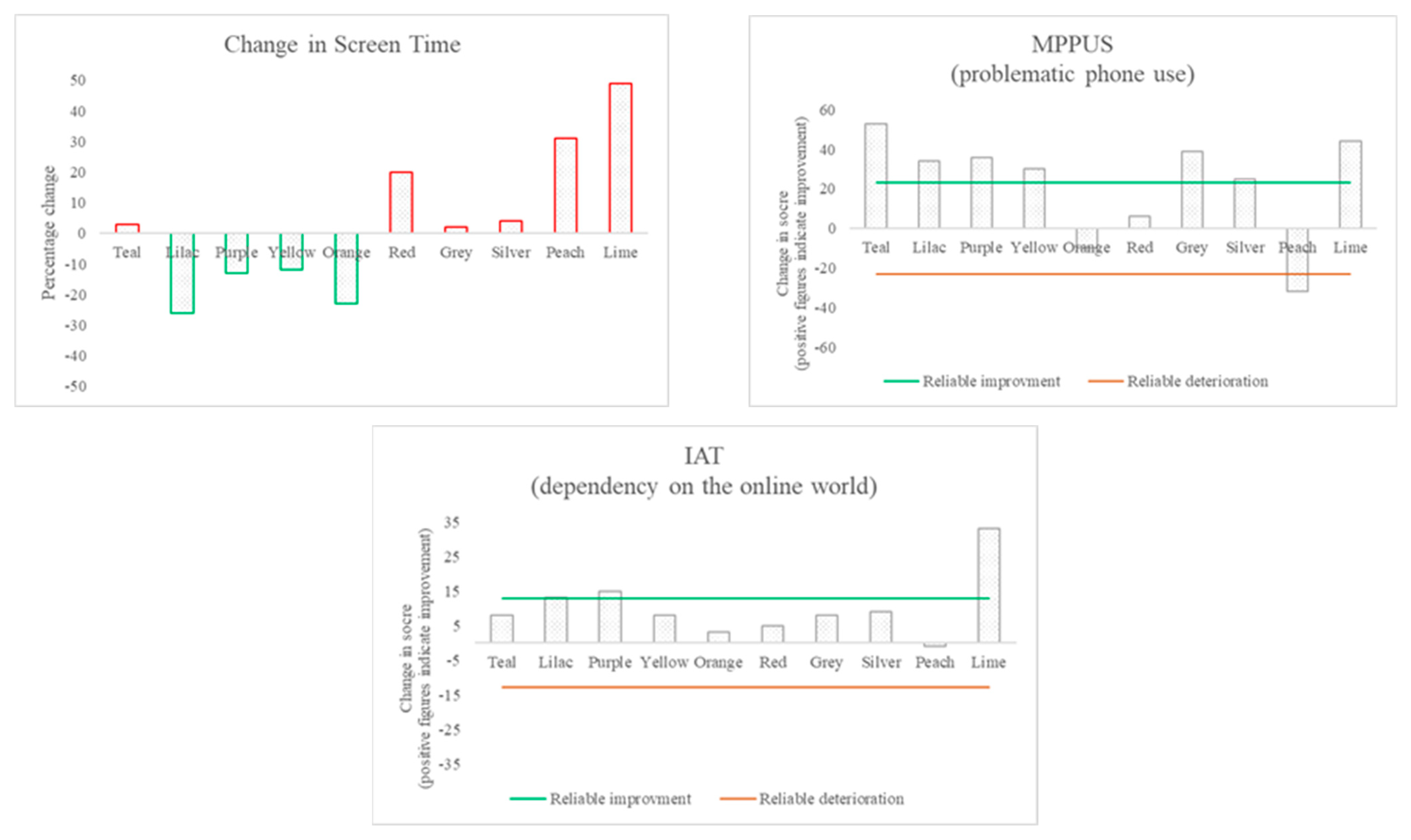
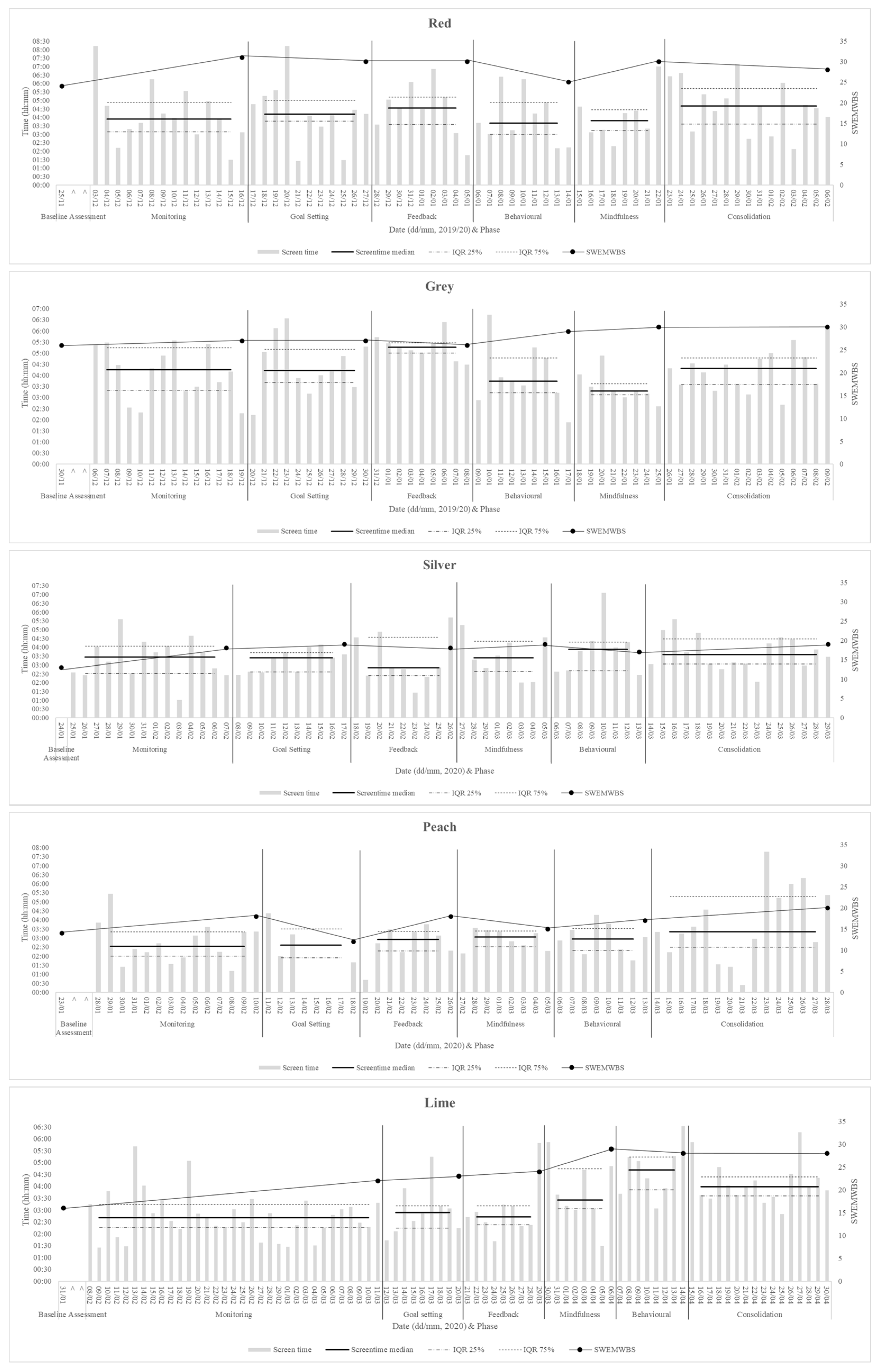
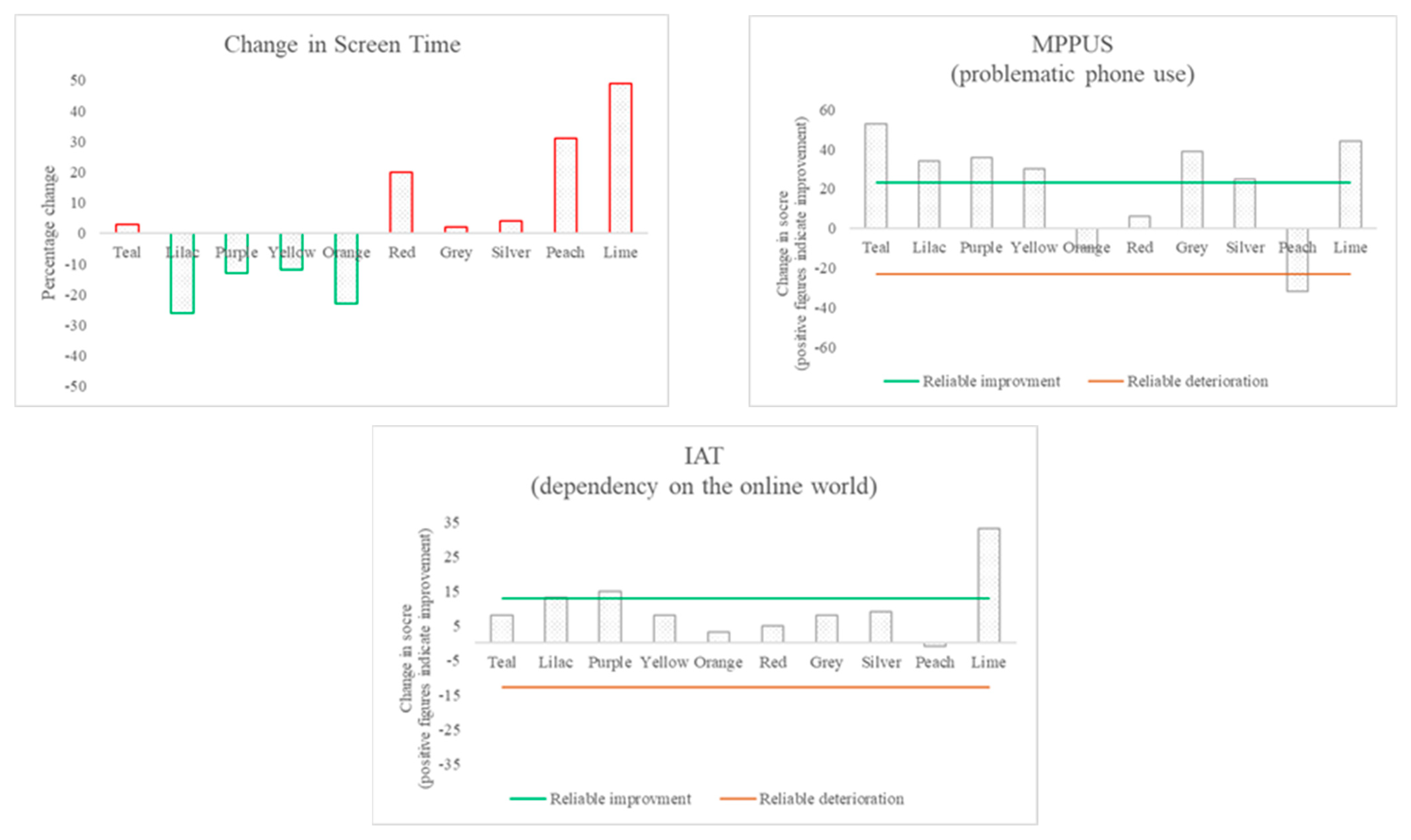
3.2. Changes in Technology Use
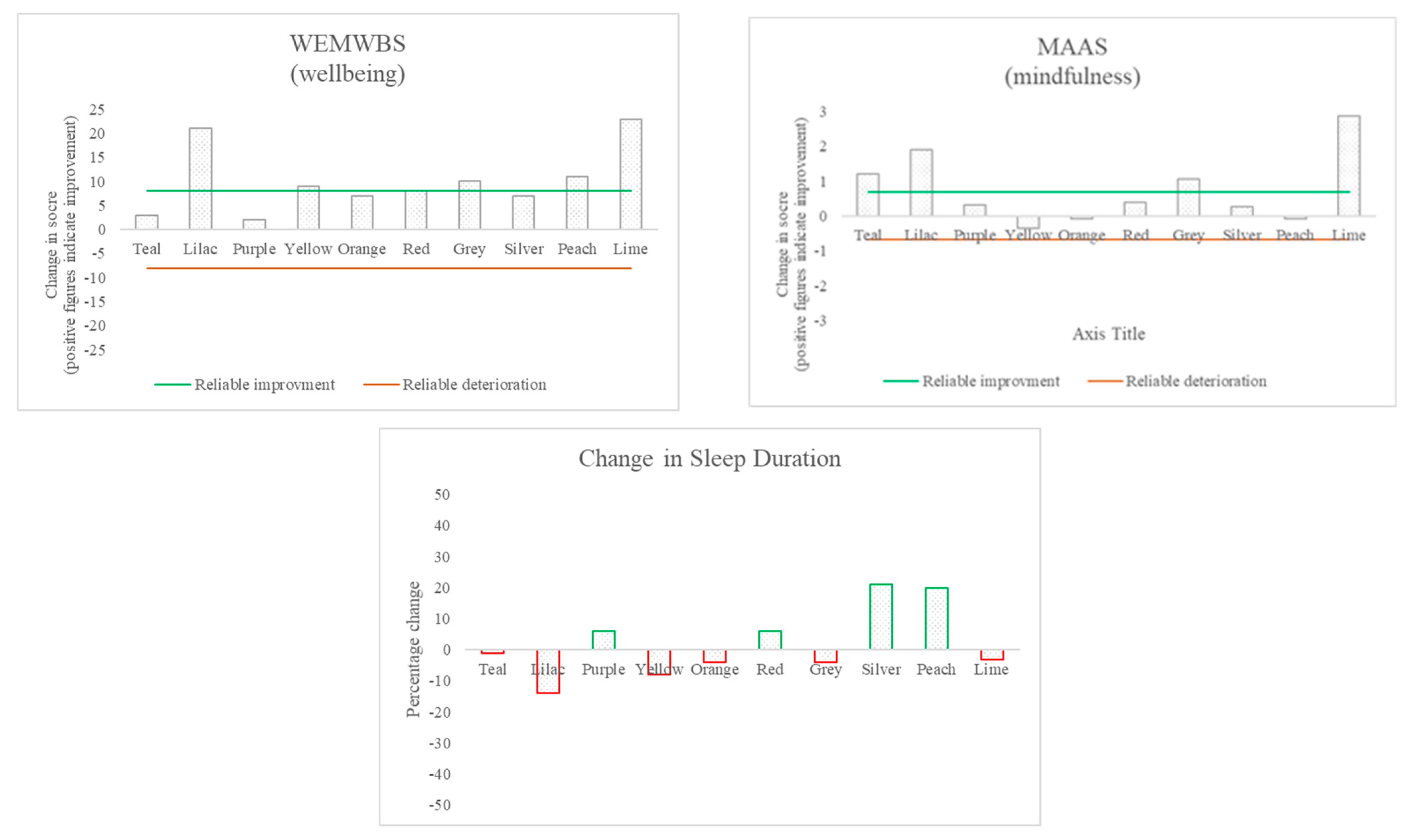
3.3. Changes in Wellbeing and Related Constructs
3.4. The Relationship between Changes in Technology Use and Other Changes
3.5. Participants’ Perspectives on Change
4. Discussion
4.1. Discussion of Findings
4.2. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Deloitte. Global Mobile Consumer Survey: UK Cut Plateauing at the Peak the State of the Smartphone. 2019. Available online: https://www2.deloitte.com/content/dam/Deloitte/uk/Documents/technology-media-telecommunications/deloitte-uk-plateauing-at-the-peak-the-state-of-the-smartphone.pdf (accessed on 29 May 2020).
- Thorsteinsson, G.; Page, T. User attachment to smartphones and design guidelines. Int. J. Mob. Learn. Organ. 2014, 8, 201–215. [Google Scholar] [CrossRef] [Green Version]
- Billieux, J.; Philippot, P.; Schmid, C.; Maurage, P.; De Mol, J.; Van Der Linden, M. Is Dysfunctional Use of the Mobile Phone a Behavioural Addiction? Confronting Symptom-Based Versus Process-Based Approaches. Clin. Psychol. Psychother. 2015, 22, 460–468. [Google Scholar] [CrossRef] [Green Version]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar] [CrossRef]
- Lortie, C.L.; Guitton, M.J. Internet addiction assessment tools: Dimensional structure and methodological status. Addiction 2013, 108, 1207–1216. [Google Scholar] [CrossRef]
- Brand, M.; Laier, C.; Young, K.S. Internet addiction: Coping styles, expectancies, and treatment implications. Front. Psychol. 2014, 5, 1256. [Google Scholar] [CrossRef] [Green Version]
- Ofcom. Digital Day 2016 Media and Communications Diary Aged 16–34 in the UK. 2016. Available online: http://www.digitaldayresearch.co.uk/media/1087/aged-16-34-in-the-uk.pdf (accessed on 29 May 2020).
- Young, K.S. Internet Addiction: A Handbook and Guide to Evaluation and Treatment; John Wiley & Sons: Hoboken, NJ, USA, 2010. [Google Scholar] [CrossRef]
- Genova, G.P.; Bewick, B.M.; Summers, B. Student Perceptions of Digital Addiction; Society for the Study of Addiction. 2019. Available online: https://www.addiction-ssa.org/knowledge-hub/student-perceptions-of-digital-addiction/ (accessed on 10 May 2019).
- Ali, R.; Jiang, N.; Phalp, K.; Muir, S.; Mcalaney, J. The Emerging Requirement for Digital Addiction Labels. In Requirements Engineering: Foundation for Software Quality; Fricker, S., Schneider, K., Eds.; REFSQ 2015; Lecture Notes in Computer Science, Volume 9013; Springer: Cham, Switzerland, 2015. [Google Scholar] [CrossRef] [Green Version]
- Lam, L.T.; Lam, M.K. eHealth Intervention for Problematic Internet Use (PIU). Curr. Psychiatry Rep. 2016, 18, 107. [Google Scholar] [CrossRef]
- Du, Y.-S.; Jiang, W.; Vance, A. Longer Term Effect of Randomized, Controlled Group Cognitive Behavioural Therapy for Internet Addiction in Adolescent Students in Shanghai. Aust. N. Z. J. Psychiatry 2010, 44, 129–134. [Google Scholar] [CrossRef]
- Lan, Y.; Ding, J.-E.; Li, W.; Li, J.; Zhang, Y.; Liu, M.; Fu, H. A pilot study of a group mindfulness-based cognitive-behavioral intervention for smartphone addiction among university students. J. Behav. Addict. 2018, 7, 1171–1176. [Google Scholar] [CrossRef]
- Young, K.S. Internet Addiction: Symptoms, Evaluation, And Treatment. Innov. Clin. Pract. 1999, 17, 351–352. [Google Scholar]
- Bewick, B.M.; West, R.; Gill, J.; O’May, F.; Mulhern, B.; Barkham, M.; Hill, A.J. Providing Web-Based Feedback and Social Norms Information to Reduce Student Alcohol Intake: A Multisite Investigation. J. Med. Internet Res. 2010, 12, e59. [Google Scholar] [CrossRef]
- Calvete, E.; Gámez-Guadix, M.; Cortazar, N. Mindfulness facets and problematic Internet use: A six-month longitudinal study. Addict. Behav. 2017, 72, 57–63. [Google Scholar] [CrossRef]
- Dallery, J.; Cassidy, R.N.; Raiff, B. Single-Case Experimental Designs to Evaluate Novel Technology-Based Health Interventions. J. Med. Internet Res. 2013, 15, e22. [Google Scholar] [CrossRef]
- Chambless, D.L.; Hollon, S.D. Defining empirically supported therapies. J. Consult. Clin. Psychol. 1998, 66, 7–18. [Google Scholar] [CrossRef]
- Lobo, M.A.; Moeyaert, M.; Cunha, A.B.; Babik, I. Single-Case Design, Analysis, and Quality Assessment for Intervention Research. J. Neurol. Phys. Ther. 2017, 41, 187–197. [Google Scholar] [CrossRef]
- Young, K.S. Internet Addiction: The Emergence of a New Clinical Disorder. CyberPsychology Behav. 1998, 1, 237–244. [Google Scholar] [CrossRef] [Green Version]
- Young, K.S. Caught in the Net: How to Recognize the Sign of Internet Addiction and a Winning Strategy for Recovery; John Wiley & Sons: Hoboken, NJ, USA, 1998. [Google Scholar]
- Prochaska, J.O.; Norcross, J.C. Stages of change. Psychotherapy 2001, 38, 443–448. [Google Scholar] [CrossRef]
- Powell, G. The Beginning of Space. 2017. Available online: https://findyourphonelifebalance.com/news/2017/4/25/thebeginningofspace (accessed on 7 November 2021).
- Bianchi, A.; Phillips, J.G. Psychological Predictors of Problem Mobile Phone Use. CyberPsychol. Behav. 2005, 8, 39–51. [Google Scholar] [CrossRef]
- Frangos, C.C.; Frangos, C.C.; Sotiropoulos, I. A meta-analysis of the reliabilty of young’s internet addiction test. In Proceedings of the World Congress on Engineering 2012, London, UK, 4–6 July 2012; Volume 1, pp. 368–371. Available online: https://www.researchgate.net/publication/265084236 (accessed on 30 March 2020).
- Tennant, R.; Hiller, L.; Fishwick, R.; Platt, S.; Joseph, S.; Weich, S.; Parkinson, J.; Secker, J.; Stewart-Brown, S. The Warwick-Edinburgh Mental Well-being Scale (WEMWBS): Development and UK validation. Health Qual. Life Outcomes 2007, 5, 63. [Google Scholar] [CrossRef] [Green Version]
- Stewart-Brown, S.; Tennant, A.; Tennant, R.; Platt, S.; Parkinson, J.; Weich, S. Internal construct validity of the Warwick-Edinburgh Mental Well-being Scale (WEMWBS): A Rasch analysis using data from the Scottish Health Education Population Survey. Health Qual. Life Outcomes 2009, 7, 15. [Google Scholar] [CrossRef] [Green Version]
- Brown, K.W.; Ryan, R.M. The benefits of being present: Mindfulness and its role in psychological well-being. J. Pers. Soc. Psychol. 2003, 84, 822–848. [Google Scholar] [CrossRef] [Green Version]
- MacKillop, J.; Anderson, E.J. Further Psychometric Validation of the Mindful Attention Awareness Scale (MAAS). J. Psychopathol. Behav. Assess. 2007, 29, 289–293. [Google Scholar] [CrossRef]
- Law, D.; Jacob, J. Goals and Goal Based Outcomes (GBOS). 2015. Available online: https://www.corc.uk.net/media/1219/goalsandgbos-thirdedition.pdf (accessed on 22 August 2018).
- Elliott, R. Client change interview protocol. In Network for Research on Experiential Therapies; Elliott: New York, NY, USA, 1999; Available online: http://www.drbrianrodgers.com/research/client-change-interview (accessed on 23 October 2018).
- Morley, S. Single-Case Methods in Clinical Psychology: A Practical Guide; Masterson, C., Main, C.J., Eds.; Routledge: Oxon, UK, 2018. [Google Scholar]
- Loid, K.; Täht, K.; Rozgonjuk, D. Do pop-up notifications regarding smartphone use decrease screen time, phone checking behavior, and self-reported problematic smartphone use? Evidence from a two-month experimental study. Comput. Hum. Behav. 2020, 102, 22–30. [Google Scholar] [CrossRef]
- Rozgonjuk, D.; Levine, J.C.; Hall, B.J.; Elhai, J.D. The association between problematic smartphone use, depression and anxiety symptom severity, and objectively measured smartphone use over one week. Comput. Hum. Behav. 2018, 87, 10–17. [Google Scholar] [CrossRef]
- Lee, H.; Ahn, H.; Choi, S.; Choi, W. The SAMS: Smartphone Addiction Management System and Verification. J. Med. Syst. 2014, 38, 1–10. [Google Scholar] [CrossRef]
- Lin, Y.-H.; Lee, Y.-H.; Lin, P.-H.; Lin, S.-H.; Chang, L.-R.; Tseng, H.-W.; Yen, L.-Y.; Yang, C.C.; Kuo, T.B. Time distortion associated with smartphone addiction: Identifying smartphone addiction via a mobile application (App). J. Psychiatr. Res. 2015, 65, 139–145. [Google Scholar] [CrossRef]
- Lee, P. Mobile Consumer Survey 2018: The UK Cut. Deloitte. 2018. Available online: https://www2.deloitte.com/uk/en/pages/technology-media-and-telecommunications/articles/mobile-consumer-survey.html (accessed on 24 January 2019).
- Turner, L.; Bewick, B.M.; Kent, S.; Khyabani, A.; Bryant, L.; Summers, B. When Does a Lot Become Too Much? A Q Methodological Investigation of UK Student Perceptions of Digital Addiction. Int. J. Environ. Res. Public Health 2021, 18, 11149. [Google Scholar] [CrossRef]
- Prochaska, J.O.; DiClemente, C.C.; Norcross, J.C. In search of how people change: Applications to addictive behaviors. Am. Psychol. 1992, 47, 1102–1114. [Google Scholar] [CrossRef]
- Young, K.S. Treatment outcomes using CBT-IA with Internet-addicted patients. J. Behav. Addict. 2013, 2, 209–215. [Google Scholar] [CrossRef] [Green Version]
- Wollburg, E.; Braukhaus, C. Goal setting in psychotherapy: The relevance of approach and avoidance goals for treatment outcome. Psychother. Res. 2010, 20, 488–494. [Google Scholar] [CrossRef]
- Oulasvirta, A.; Rattenbury, T.; Ma, L.; Raita, E. Habits make smartphone use more pervasive. Pers. Ubiquit. Comput. 2011, 16, 105–114. [Google Scholar] [CrossRef]
- Elliott, R. Hermeneutic Single-Case Efficacy Design. Psychother. Res. 2002, 12, 1–21. [Google Scholar] [CrossRef]
- Bewick, B.M.; West, R.M.; Barkham, M.; Mulhern, B.; Marlow, R.; Traviss, G.; Hill, A.J.; Blankers, M.; Cunningham, J. The Effectiveness of a Web-Based Personalized Feedback and Social Norms Alcohol Intervention on United Kingdom University Students: Randomized Controlled Trial. J. Med. Internet Res. 2013, 15, e137. [Google Scholar] [CrossRef]
- Cuddeback, G.; Wilson, E.; Orme, J.G.; Combs-Orme, T. Detecting and Statistically Correcting Sample Selection Bias. J. Soc. Serv. Res. 2004, 30, 19–33. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic | Value | N (n = 10) | (%) |
|---|---|---|---|
| Gender | Female | 9 | (90) |
| Male | 1 | (10) | |
| Faculty of Study | Arts, Humanities, and Cultures | 3 | (30) |
| Engineering and Physical Sciences | 4 | (40) | |
| Medicine and Health | 2 | (20) | |
| Social Sciences | 1 | (10) | |
| Age | 18–21 | 7 | (70) |
| 22–25 | 2 | (20) | |
| 26–29 | - | - | |
| 30–33 | 1 | (10) | |
| Undergraduate Year of Study | 1 | 1 | (10) |
| 2 | 2 | (20) | |
| 3 | 4 | (40) | |
| 4 | 1 | (10) | |
| 5 | 1 | (10) | |
| Other | 1 | (10) |
| Phase | Example Messages |
|---|---|
| Personalised feedback | “You spend 3 h a day on your phone, over a year this would be over 45 whole days.” Image: a bar chart showing average daily screen time for weeks 1–4 |
| Behavioural suggestions | “You said that leisure time is important to you. Plan an activity, whilst doing this set your phone to ‘do not disturb’ and place it out of sight.” |
| Mindfulness suggestions | “Pick an everyday activity and focus all of your attention on this activity while you do it. Your mind might wander but bring it back to the activity. You can use your senses like the activity yesterday.” |
| MPPUS | IAT | MAAS | WEMWBS | |||||
|---|---|---|---|---|---|---|---|---|
| Participant | Pre | Post | Pre | Post | Pre | Post | Pre | Post |
| Teal | 134 | 81 a | 40 | 32 | 4.2 | 5.4 a | 54 | 57 |
| Lilac | 138 | 104 a | 61 | 48 | 2.6 | 4.5 a | 22 | 43 a |
| Purple | 178 | 142 a | 59 | 44 a | 1.67 | 2 | 38 | 40 |
| Yellow | 171 | 141 a | 47 | 39 | 4.13 | 3.79 | 43 | 52 |
| Orange | 130 | 140 | 33 | 30 | 3.93 | 3.87 | 49 | 56 |
| Red | 149 | 143 | 57 | 52 | 3.93 | 4.33 | 48 | 56 a |
| Grey | 160 | 121 a | 50 | 42 | 4.47 | 5.53 a | 48 | 58 a |
| Silver | 144 | 119 a | 58 | 49 | 2.67 | 2.93 | 29 | 36 |
| Peach | 91 | 123 b | 35 | 36 | 3.07 | 3 b | 29 | 40 a |
| Lime | 142 | 98 a | 41 | 8 a | 1.53 | 4.4 a | 33 | 56 a |
| Participant | Goal 1 (Change in Smartphone Use) | Change in Goal 1 Achievement Rating | Goal 2 (Area of Life Wanting to Improve) | Change in Goal 2 Achievement Rating |
|---|---|---|---|---|
| Teal | Be less distracted by | +8 | Leisure time | +4 |
| Lilac | Reduce time spent overall | +8 | Relationships with family | +5 |
| Purple | Check less often | +5 | Studying | +1 |
| Yellow | Be less distracted by | +4 | Studying | +4 |
| Orange | Reduce time spent overall | +2 | Studying | +2 |
| Red | Reduce time spent on social media | +7 | Relationships with family | +4 |
| Grey | Be less distracted by | +2 | Studying | +2 |
| Silver | Reduce time spent overall | +2 | Studying | +1 |
| Peach | Be less distracted by | +1 | Studying | +1 |
| Lime | Be less distracted by | +5 | Leisure time | +6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kent, S.; Masterson, C.; Ali, R.; Parsons, C.E.; Bewick, B.M. Digital Intervention for Problematic Smartphone Use. Int. J. Environ. Res. Public Health 2021, 18, 13165. https://doi.org/10.3390/ijerph182413165
Kent S, Masterson C, Ali R, Parsons CE, Bewick BM. Digital Intervention for Problematic Smartphone Use. International Journal of Environmental Research and Public Health. 2021; 18(24):13165. https://doi.org/10.3390/ijerph182413165
Chicago/Turabian StyleKent, Sarah, Ciara Masterson, Raian Ali, Christine E. Parsons, and Bridgette M. Bewick. 2021. "Digital Intervention for Problematic Smartphone Use" International Journal of Environmental Research and Public Health 18, no. 24: 13165. https://doi.org/10.3390/ijerph182413165
APA StyleKent, S., Masterson, C., Ali, R., Parsons, C. E., & Bewick, B. M. (2021). Digital Intervention for Problematic Smartphone Use. International Journal of Environmental Research and Public Health, 18(24), 13165. https://doi.org/10.3390/ijerph182413165