Brazil’s Actions and Reactions in the Fight against COVID-19 from January to March 2020

 ,
,  ,
, 

Abstract
1. Introduction
2. Methodology
3. Findings
3.1. Case Presentation
3.1.1. Brazil’s Context
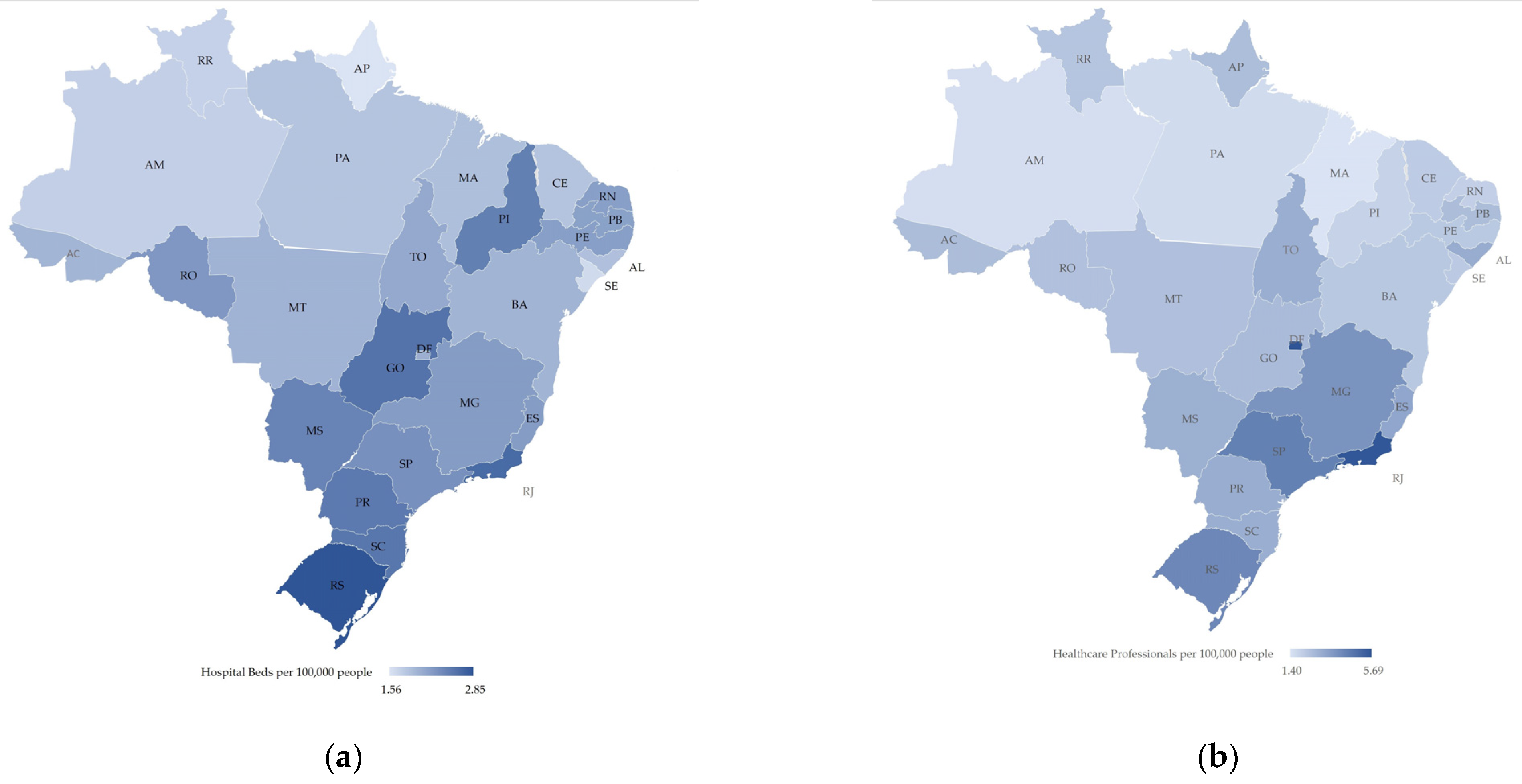
3.1.2. Brazil’s Health System
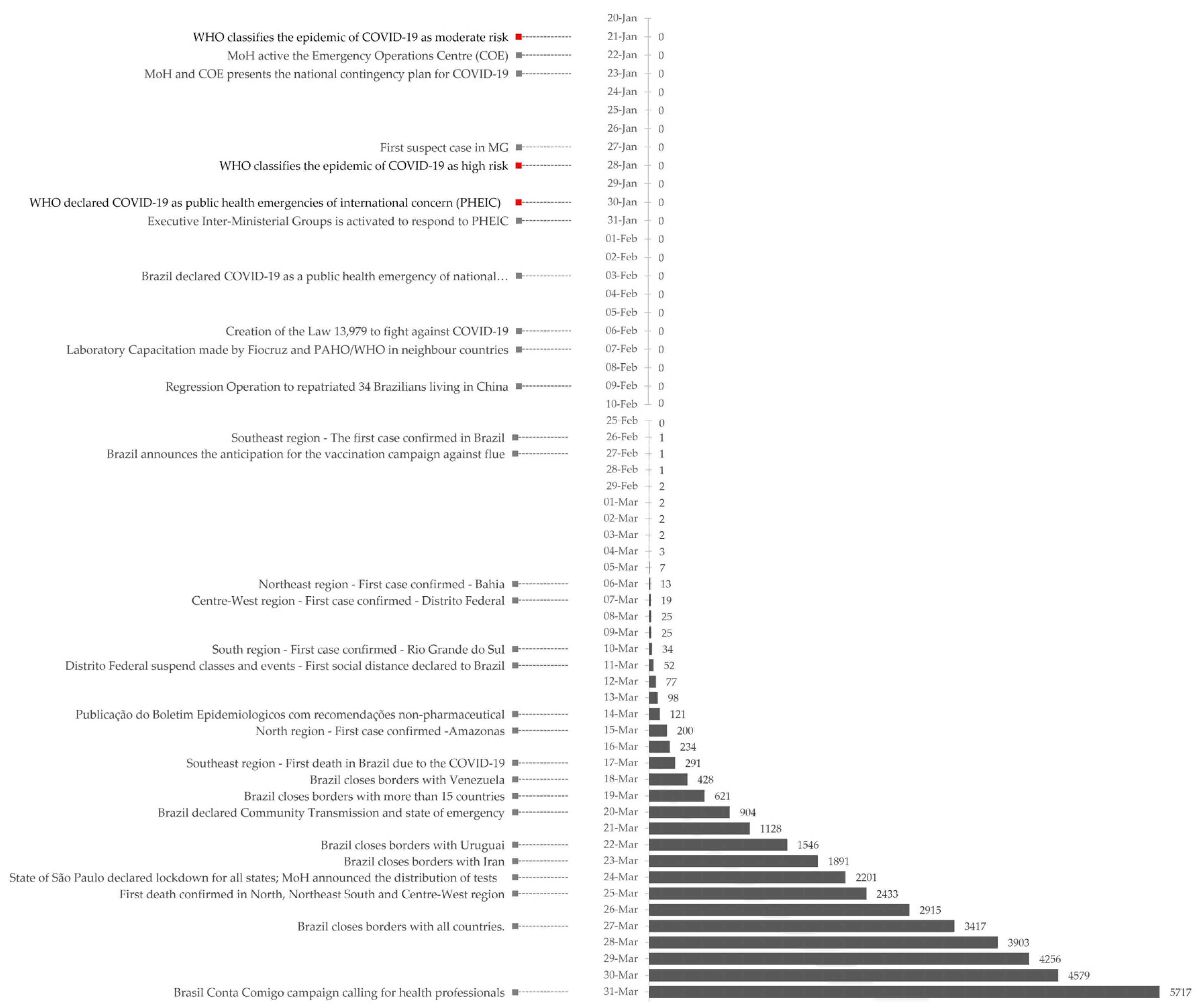
3.1.3. Epidemiological Situation
3.2. Management and Outcome
3.2.1. Non-Pharmaceutical Measures
3.2.2. Economy
3.2.3. Social and Political Disruption/Media Coverage
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization Naming the Coronavirus Disease (COVID-19) and the Virus that Causes It. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/naming-the-coronavirus-disease-(covid-2019)-and-the-virus-that-causes-it (accessed on 15 April 2020).
- World Health Organization 2019 Novel Coronavirus (2019-nCoV): Strategic Preparedness and Response Plan 2020. Available online: https://www.who.int/publications/i/item/strategic-preparedness-and-response-plan-for-the-new-coronavirus (accessed on 15 April 2020).
- World Health Organization WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19–11 March 2020. Available online: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 15 April 2020).
- Buss, P. Brazil: Structuring cooperation for health. Lancet 2011, 377, 1722–1723. [Google Scholar] [CrossRef]
- Ventura, D.d.F.L.; Ribeiro, H.; Giulio, G.M.d.; Jaime, P.C.; Nunes, J.; Bógus, C.M.; Antunes, J.L.F.; Waldman, E.A. Challenges of the COVID-19 pandemic: For a Brazilian research agenda in global health and sustainability. Cadernos Saude Publ. 2020, 36, e00040620. [Google Scholar] [CrossRef] [PubMed]
- Fiocruz. The Fiocruz Response to the COVID-19. Fiocruz. Available online: https://fiocruz.tghn.org/coronavirus/ (accessed on 15 April 2020).
- Yin, R.K. Case Study Research and Applications: Design and Methods; Sage Publishing: Thousand Oaks, CA, USA, 2017. [Google Scholar]
- Brasil Consitituição da Republica Federativa do Brasil 1988. Available online: http://www.planalto.gov.br/ccivil_03/constituicao/constituicao.htm (accessed on 15 April 2020).
- Albuquerque, M.V.d.; Viana, A.L.d.; Lima, L.D.d.; Ferreira, M.P.; Fusaro, E.R.; Iozzi, F.L. Desigualdades regionais na saúde: Mudanças observadas no Brasil de 2000 a 2016. Ciência Saúde Coletiva 2017, 22, 1055–1064. [Google Scholar] [CrossRef] [PubMed]
- IPEA; PNUD. Fundação João Pinheiro Radar IDHM: Evolução do IDHM e de Seus Índices Componentes no Período de 2012 a 2017; IPEA: Brasília, Brazil, 2019. [Google Scholar]
- Instituto Brasileiro de Geografia e Estatística (IBGE) Projeções da População. Available online: https://www.ibge.gov.br/estatisticas/sociais/populacao/9109-projecao-da-populacao.html?=&t=o-que-e (accessed on 15 April 2020).
- Instituto Brasileiro de Geografia e Estatística (IBGE) Pesquisa Nacional por Amostra de Domicílios Contínua—PNAD Contínua. Available online: https://www.ibge.gov.br/estatisticas/sociais/trabalho/9173-pesquisa-nacional-por-amostra-de-domicilios-continua-trimestral.html?t=resultados (accessed on 15 April 2020).
- Panel de Saneamento Brasil. Available online: https://www.painelsaneamento.org.br/localidade?id=0 (accessed on 15 April 2020).
- Instituto Brasileiro de Geografia e Estatística (IBGE) Balanço de Contas Nacionais. Available online: https://sidra.ibge.gov.br/tabela/1846#/n1/all/v/all/p/-1/c11255/90687,90691,90696,90705,90706,90707,93404,93405,93406,93407,93408,102880/l/v,,c11255+t+p/resultado (accessed on 15 April 2020).
- Brasil, Ministério da Saúde. Sistema Único de Saúde (SUS): Estrutura, Princiípios e Como Funciona. Available online: https://www.saude.gov.br/sistema-unico-de-saude (accessed on 15 April 2020).
- Castro, M.C.; Massuda, A.; Almeida, G.; Menezes-Filho, N.A.; Andrade, M.V.; de Souza Noronha, K.V.M.; Rocha, R.; Macinko, J.; Hone, T.; Tasca, R.; et al. Brazil’s unified health system: The first 30 years and prospects for the future. Lancet 2019, 394, 345–356. [Google Scholar] [CrossRef]
- Watts, J. Brazil’s health system woes worsen in economic crisis. Lancet 2016, 387, 1603–1604. [Google Scholar] [CrossRef]
- Associação de Medicina Intensiva Brasileira (AMIB). Censo AMIB 2016; AMIB: São Paulo, Brasil, 2016. [Google Scholar]
- Coelho, F.C.; Lana, R.M.; Cruz, O.G.; Codeco, C.T.; Villela, D.; Bastos, L.S.; Piontti, A.P.Y.; Davis, J.T.; Vespignani, A.; Gomes, M.F.C. Assessing the potential impact of COVID-19 in Brazil: Mobility, morbidity and the burden on the health care system. medRxiv 2020. [Google Scholar] [CrossRef]
- Agência Nacional de Saúde Complementar (ANS) Dados Gerais—ANS—Agência Nacional de Saúde Suplementar. Available online: https://www.ans.gov.br/perfil-do-setor/dados-gerais (accessed on 15 April 2020).
- Brazil, Ministério da Saúde TabNet Win32 3.0: E.1 Número de Profissionais de Saúde por Habitante. Available online: http://tabnet.datasus.gov.br/cgi/tabcgi.exe?idb2012/e01.def (accessed on 4 December 2020).
- Brazil, Ministério da Saúde, Painel Coronavírus. Available online: https://covid.saude.gov.br/ (accessed on 15 April 2020).
- Centro de Operações de Emergência em Saúde Pública (COE). Boletim Epidemiológico 06–Doença pelo Coronavírus 2019. Available online: https://portalarquivos.saude.gov.br/images/pdf/2020/April/03/BE6-Boletim-Especial-do-COE.pdf (accessed on 15 April 2020).
- Universidade Federal de Pelotas (UFPel Gráfico da Evolução Temporal do Coronavírus. Available online: http://ccs2.ufpel.edu.br/wp/2020/03/26/grafico-da-evolucao-temporal-do-coronavirus-atualizacao-de-25-03-2020/ (accessed on 15 April 2020).
- Cota, W.; Ferreira, S.C. Risk map of COVID-19—Brazil. Available online: https://covid-19-risk.github.io/map/brazil/en/ (accessed on 26 March 2020).
- Arenas, A.; Cota, W.; Gomez-Gardenes, J.; Gómez, S.; Granell, C.; Matamalas, J.T.; Soriano-Panos, D.; Steinegger, B. A Mathematical Model for the Spatiotemporal Epidemic Spreading of COVID19. medRxiv 2020. [Google Scholar] [CrossRef]
- São Paulo. Vigilância em Saúde. Boletins Epidemiológicos. Available online: https://www.prefeitura.sp.gov.br/cidade/secretarias/saude/vigilancia_em_saude/index.php?p=295572 (accessed on 26 March 2020).
- Aquino, V. Campanha de Vacinação Contra a Gripe Será Antecipada. Available online: https://www.saude.gov.br/noticias/agencia-saude/46449-campanha-de-vacinacao-contra-a-gripe-sera-antecipada (accessed on 15 April 2020).
- Centro de Operações de Emergência em Saúde Pública (COE). Boletim Epidemiológico 05–Doença pelo Coronavírus 2019. Available online: https://portalarquivos.saude.gov.br/images/pdf/2020/marco/24/03--ERRATA---Boletim-Epidemiologico-05.pdf (accessed on 15 April 2020).
- Rio’s State of Emergency Closes Christ Statue. Available online: https://www.smh.com.au/world/south-america/rio-s-state-of-emergency-closes-christ-statue-20200318-p54bge.html (accessed on 15 April 2020).
- G1 Rio. Rio e Outros 5 Municípios do Estado Declaram Situação de Emergência Para Conter o Coronavírus. Available online: https://g1.globo.com/rj/rio-de-janeiro/noticia/2020/03/18/prefeitura-do-rio-declara-situacao-de-emergencia.ghtml (accessed on 15 April 2020).
- G1 RS. Governo do RS Decreta Situação de Calamidade Pública Devido ao Coronavírus. Available online: https://g1.globo.com/rs/rio-grande-do-sul/noticia/2020/03/19/governo-decreta-situacao-de-calamidade-publica-no-rs-devido-ao-coronavirus.ghtml (accessed on 15 April 2020).
- Brasil, Regimento Interno do Senado Federal. Decreto Legislativo n° 6, de 2020. Available online: http://www.planalto.gov.br/ccivil_03/portaria/DLG6-2020.htm#:~:text=DECRETO%20LEGISLATIVO%20N%C2%BA%206%2C%20DE,Art. (accessed on 15 April 2020).
- Brasil, Ministério da Saúde/Gabinete do Ministro. Portaria n° 454, de 20 de Março de 2020. Available online: https://www.in.gov.br/en/web/dou/-/portaria-n-454-de-20-de-marco-de-2020-249091587 (accessed on 15 April 2020).
- Brasil, Presidência da República/Casa Civil. Portaria n° 120, de 17 de Março de 2020. Available online: https://www.in.gov.br/en/web/dou/-/portaria-n-120-de-17-de-marco-de-2020-248564454 (accessed on 15 April 2020).
- Brasil, Presidência da República/Casa Civil. Portaria n° 125, de 19 de Março de 2020. Available online: https://www.in.gov.br/en/web/dou/-/portaria-n-125-de-19-de-marco-de-2020-248881224 (accessed on 15 April 2020).
- Brasil, Casa Civil. Portaria n° 126, de 19 de Março de 2020. Available online: https://www.in.gov.br/en/web/dou/-/portaria-n-126-de-19-de-marco-de-2020-248881688 (accessed on 15 April 2020).
- Brasil, Casa Civil. Portaria n° 132, de 22 de Março de 2020. Available online: https://www.in.gov.br/en/web/dou/-/portaria-n-132-de-22-de-marco-de-2020-249098650 (accessed on 15 April 2020).
- Brasil, Presidência da República/Casa Civil. Portaria n° 47, de 26 de Março de 2020. Available online: https://www.in.gov.br/web/dou/-/portaria-n-47-de-26-de-marco-de-2020-249861855 (accessed on 15 April 2020).
- Brasil, Presidência da República/Casa Civil. Portaria n° 152, de 27 de Março de 2020. Available online: https://www.in.gov.br/en/web/dou/-/portaria-n-152-de-27-de-marco-de-2020-250060288 (accessed on 15 April 2020).
- Brasil, Ministério da Saúde. Gráfico de Insumos. Available online: https://covid-insumos.saude.gov.br/paineis/insumos/painel.php (accessed on 15 April 2020).
- Brasil, Ministério da Saúde. Portaria n° 639, de 31 de Março de 2020. Available online: https://www.in.gov.br/en/web/dou/-/portaria-n-639-de-31-de-marco-de-2020-250847738 (accessed on 15 April 2020).
- Triboli, P. Câmara Aprova Três Projetos Com Medidas de Combate ao Coronavírus. Available online: https://www.camara.leg.br/noticias/646163-camara-aprova-tres-projetos-com-medidas-de-combate-ao-coronavirus/ (accessed on 15 April 2020).
- Al Jazeera Brazil’s Health System Will Collapse by April. Available online: https://www.aljazeera.com/news/2020/03/brazil-health-system-collapse-april-health-minister-200320190048602.html (accessed on 15 April 2020).
- Lisboa, V. Hospital de Campanha Está Quase Pronto no Rio. Available online: https://agenciabrasil.ebc.com.br/saude/noticia/2020-04/hospital-de-campanha-esta-quase-pronto-no-rio (accessed on 15 April 2020).
- Bond, L. Covid-19: São Paulo Ganhará Hospital de Campanha Dia 27. Available online: https://agenciabrasil.ebc.com.br/saude/noticia/2020-03/covid-19-sao-paulo-ganhara-hospital-de-campanha-dia-27 (accessed on 15 April 2020).
- Instituto de Pesquisa Econômica Aplicada (IPEA). Carta de Conjuntura 46–1° Trimestre de 2020. Available online: https://www.ipea.gov.br/portal/index.php?option=com_content&view=article&id=35348 (accessed on 15 April 2020).
- Brasil, Banco Central. Focus—Relatório de Mercado 2019. Available online: https://www.bcb.gov.br/publicacoes/focus/27032020 (accessed on 15 April 2020).
- Instituto Brasileiro de Geografia e Estatística (IBGE) Produto Interno Bruto—PIB. Available online: https://www.ibge.gov.br/explica/pib.php (accessed on 15 April 2020).
- Brasil, Ministério da Economia. Medidas Econômicas Voltadas para a Redução dos Impactos do Covid-19. Available online: https://www.gov.br/economia/pt-br/index (accessed on 15 April 2020).
- Flaeschen, H. Coronavírus Nas Favelas: “É Difícil Falar Sobre Perigo Quando há Naturalização do Risco de Vida”—ABRASCO. Available online: https://www.abrasco.org.br/site/outras-noticias/saude-da-populacao/coronavirus-nas-favelas-e-dificil-falar-sobre-perigo-quando-ha-naturalizacao-do-risco-de-vida/46098/ (accessed on 15 April 2020).
- Carvalho, M.S.; Lima, L.D.d.; Coeli, C.M. Ciência em Tempos de Pandemia; Cadernos de Saúde Pública: Rio de Janeiro, Brazil, 2020; Volume 36. [Google Scholar] [CrossRef]
- Phillips, T. Brazilians Protest Over Bolsonaro’s Muddled Coronavirus Response. Available online: http://www.theguardian.com/world/2020/mar/22/brazilians-protest-bolsonaro-coronavirus-panelaco (accessed on 15 April 2020).
- Bevins, V. In Brazil, Bolsonaro Gambles on a Coronavirus Culture War. N. Y. Rev. Books 2020. Available online: https://www.nybooks.com/daily/2020/03/23/in-brazil-bolsonaro-gambles-on-a-coronavirus-culture-war/ (accessed on 15 April 2020).
- Uribe, G.; Coletta, R.D. Bolsonaro se Nega a Mostrar Exames Que, Segundo Ele, Deram Negativo Para Coronavirus. Available online: https://www1.folha.uol.com.br/poder/2020/03/bolsonaro-se-nega-a-mostrar-exames-que-segundo-ele-deram-negativo-para-coronavirus.shtml (accessed on 15 April 2020).
- Uol SP. “Gripezinha”: Leia a Íntegra do Pronunciamento de Bolsonaro Sobre Covid-19. Available online: https://noticias.uol.com.br/politica/ultimas-noticias/2020/03/24/leia-o-pronunciamento-do-presidente-jair-bolsonaro-na-integra.htm (accessed on 15 April 2020).
- Monteiro, W.M.; Brito-Sousa, J.D.; Baía-da-Silva, D.; Melo, G.C.d.; Siqueira, A.M.; Val, F.; Daniel-Ribeiro, C.T.; Guimarães Lacerda, M.V.; Monteiro, W.M.; Brito-Sousa, J.D.; et al. Driving forces for COVID-19 clinical trials using chloroquine: The need to choose the right research questions and outcomes. Rev. Soci. Bras. Med. Trop. 2020, 53. [Google Scholar] [CrossRef] [PubMed]
- Cortegiani, A.; Ingoglia, G.; Ippolito, M.; Giarratano, A.; Einav, S. A systematic review on the efficacy and safety of chloroquine for the treatment of COVID-19. J. Crit. Care 2020. [Google Scholar] [CrossRef]
- Colbourn, T. COVID-19: Extending or relaxing distancing control measures. Lancet Publ. Health 2020, 5, S2468–S2667. [Google Scholar] [CrossRef]
- Cerioni, C. Como os Estados Brasileiros Estão Agindo Para Conter o Coronavírus. Available online: https://exame.abril.com.br/brasil/como-os-estados-brasileiros-estao-agindo-para-conter-o-coronavirus/ (accessed on 15 April 2020).
- Barroso, M.R. Medida Cautelar na Arguição de Descumprimento de Preceito Fundamental 669 Distrito Ferederal. Available online: http://www.stf.jus.br/arquivo/cms/noticiaNoticiaStf/anexo/ADPF669cautelar.pdf (accessed on 15 April 2020).
- G1 SP. Ao Menos 25 dos 27 Governadores Manterão Restrições Contra Coronavírus Mesmo Após Bolsonaro Pedir Fim de Isolamento. Available online: https://g1.globo.com/politica/noticia/2020/03/25/governadoras-reagem-ao-pronunciamento-de-bolsonaro-sobre-coronavirus.ghtml (accessed on 15 April 2020).
- Gielow, I. Majority of Brazilians Are Afraid of Coronavirus and Support Containment Measures, Says Datafolha. Available online: https://www1.folha.uol.com.br/internacional/en/brazil/2020/03/majority-of-brazilians-are-afraid-of-coronavirus-and-support-containment-measures-says-datafolha.shtml (accessed on 15 April 2020).
- Change.org “Bolsonaro acabou”, Acreditam Assinantes de Petição Pelo Impeachment—CartaCapital. Available online: https://www.cartacapital.com.br/blogs/change-org/bolsonaro-acabou-acreditam-assinantes-de-peticao-pelo-impeachment/ (accessed on 15 April 2020).
- Agostine, C. Líderes da Oposição Pedem Renúncia de Bolsonaro. Available online: https://valor.globo.com/politica/noticia/2020/03/30/lideres-da-oposicao-pedem-renuncia-de-bolsonaro.ghtml (accessed on 15 April 2020).
- G1 SP. Grupo Faz Carreata Contra Quarentena Imposta Por Doria em SP Devido ao Coronavírus. Available online: https://g1.globo.com/sp/sao-paulo/noticia/2020/03/27/grupo-faz-carreata-contra-quarentena-imposta-por-doria-em-sao-paulo.ghtml (accessed on 15 April 2020).
- Phillips, T. “Come back Monday, OK?” Hundreds of prisoners escape in Brazil amid Covid-19 anger. Available online: http://www.theguardian.com/world/2020/mar/17/come-back-monday-ok-hundreds-of-prisoners-escape-in-brazil-amid-covid-19-anger (accessed on 15 April 2020).
- Uol SP. Coronavírus: Madero, Havan, Giraffas: Empresários Criticam Medidas de Combate à Pandemia. Available online: https://economia.uol.com.br/noticias/redacao/2020/03/24/empresarios-coronavirus-o-que-dizem-criticas.htm?cmpid=copiaecola (accessed on 15 April 2020).
- Santana, P. Empresas anunciam doações para combate a pandemia de coronavírus no Brasil; conheça as iniciativas. InfoMoney 2020. Available online: https://www.infomoney.com.br/economia/empresas-anunciam-doacoes-para-combate-a-pandemia-de-coronavirus-no-brasil-conheca-as-iniciativas/ (accessed on 15 April 2020).
- Martins, R.M.; Demori, L. Em áudio no WhatsApp, Bolsonaro dá parabéns a manifestações que devem aumentar propagação do coronavírus. Intercept 2020. Available online: https://theintercept.com/2020/03/16/audio-bolsonaro-parabens-protestos-coronavirus/ (accessed on 15 April 2020).
- Hone, T.; Mirelman, A.J.; Rasella, D.; Paes-Sousa, R.; Barreto, M.L.; Rocha, R.; Millett, C. Effect of economic recession and impact of health and social protection expenditures on adult mortality: A longitudinal analysis of 5565 Brazilian municipalities. Lancet Glob. Health 2019, 7, e1575–e1583. [Google Scholar] [CrossRef]
- Fellet, J. “Vírus chinês”: Como Brasil se inseriu em disputa geopolítica entre EUA e China sobre pandemia. BBC News Bras. 2020. Available online: https://www.bbc.com/portuguese/brasil-51963251 (accessed on 15 April 2020).




{kind=link}
{kind=link}
{kind=link}
| State | HDI | GDP | Population | Sanitation | |||||
|---|---|---|---|---|---|---|---|---|---|
| HDI | GDP ($100,000) | % | Population | % | Density (pop/km2) | Access to Clean Water (% pop) | Access to Sewage CollectionService (% pop) | ||
| North | 0.730 | 1,061,739.73 | 5.5% | 18,430,980 | 8.8% | 4.79 | 57.0% | 10.5% | |
| RO | Rondônia | 0.725 | 123,052.05 | 0.6% | 1,777,225 | 0.8% | 7.47 | 49.4% | 4.9% |
| AC | Acre | 0.719 | 42,002.74 | 0.2% | 881,935 | 0.4% | 5.37 | 47.1% | 10.1% |
| AM | Amazonas | 0.733 | 274,271.23 | 1.4% | 4,144,597 | 2.0% | 2.66 | 81.1% | 10.0% |
| RR | Roraima | 0.752 | 36,630.14 | 0.2% | 605,761 | 0.3% | 2.70 | 81.5% | 51.7% |
| PA | Pará | 0.698 | 442,054.79 | 2.3% | 8,602,865 | 4.1% | 6.91 | 45.6% | 5.2% |
| AP | Amapá | 0.740 | 46,013.70 | 0.2% | 845,731 | 0.4% | 5.94 | 34.9% | 7.1% |
| TO | Tocantins | 0.743 | 97,715.07 | 0.5% | 1,572,866 | 0.7% | 5.66 | 79.3% | 26.4% |
| Northeast | 0.711 | 2,752,953.42 | 14.3% | 57,071,654 | 27.2% | 36.77 | 74.2% | 28.0% | |
| MA | Maranhão | 0.687 | 268,983.56 | 1.4% | 7,075,181 | 3.4% | 21.46 | 56.4% | 13.8% |
| PI | Piauí | 0.697 | 138,021.92 | 0.7% | 3,273,227 | 1.6% | 13.01 | 75.9% | 14.4% |
| CE | Ceará | 0.735 | 427,134.25 | 2.2% | 9,132,078 | 4.3% | 61.33 | 59.0% | 25.5% |
| RN | Rio Grande do Norte | 0.731 | 183,479.45 | 1.0% | 3,506,853 | 1.7% | 66.41 | 87.1% | 23.8% |
| PB | Paraíba | 0.722 | 176,367.12 | 0.9% | 4,018,127 | 1.9% | 71.16 | 74.3% | 36.1% |
| PE | Pernambuco | 0.727 | 510,553.42 | 2.7% | 9,557,071 | 4.5% | 97.45 | 80.5% | 27.5% |
| AL | Alagoas | 0.683 | 149,076.71 | 0.8% | 3,337,357 | 1.6% | 119.86 | 74.6% | 21.3% |
| SE | Sergipe | 0.702 | 115,117.81 | 0.6% | 2,298,696 | 1.1% | 104.83 | 86.9% | 25.5% |
| BA | Bahia | 0.714 | 784,219.18 | 4.1% | 14,873,064 | 7.1% | 26.34 | 81.6% | 39.5% |
| Centre-West | 0.790 | 1,903,865.75 | 9.9% | 16,297,074 | 7.8% | 10.15 | 89.0% | 52.9% | |
| MS | Mato Grosso do Sul | 0.766 | 293,065.75 | 1.5% | 3,484,466 | 1.7% | 9.76 | 86.4% | 49.5% |
| MT | Mato Grosso | 0.774 | 376,556.16 | 2.0% | 2,778,986 | 1.3% | 3.08 | 89.3% | 35.6% |
| GO | Goiás | 0.769 | 536,115.07 | 2.8% | 7,018,354 | 3.3% | 20.63 | 85.5% | 46.4% |
| DF | Distrito Federal | 0.850 | 698,128.77 | 3.6% | 3,015,268 | 1.4% | 523.41 | 99.0% | 89.3% |
| Southeast | 0.795 | 10,195,389.04 | 53.1% | 88,371,433 | 42.1% | 95.58 | 91.0% | 79.2% | |
| MG | Minas Gerais | 0.787 | 1,684,591.78 | 8.8% | 21,168,791 | 10.1% | 36.09 | 82.1% | 72.1% |
| ES | Espírito Santo | 0.772 | 375,397.26 | 2.0% | 4,018,650 | 1.9% | 87.22 | 81.2% | 54.9% |
| RJ | Rio de Janeiro | 0.796 | 2,079,065.75 | 10.8% | 17,264,943 | 8.2% | 394.62 | 90.5% | 65.3% |
| SP | São Paulo | 0.826 | 6,056,334.25 | 31.6% | 45,919,049 | 21.9% | 184.99 | 96.2% | 89.8% |
| South | 0.796 | 3,275,479.45 | 17.1% | 29,975,984 | 14.3% | 51.97 | 90.2% | 45.2% | |
| PR | Paraná | 0.792 | 1,205,558.90 | 6.3% | 11,433,957 | 5.4% | 57.37 | 94.4% | 71.4% |
| SC | Santa Catarina | 0.808 | 817,060.27 | 4.3% | 7,164,788 | 3.4% | 74.84 | 89.1% | 23.7% |
| RS | Rio Grande do Sul | 0.787 | 1,252,860.27 | 6.5% | 11,377,239 | 5.4% | 40.39 | 86.4% | 32.1% |
| Brazil | 0.778 | 19,189,427.40 | 100% | 210,147,125 | 100.0% | 24.69 | 83.6% | 53.1% | |
| Target Population | Value (R$ Billion) | Value (US$ Billion) |
|---|---|---|
| Elderly people | 46.0 | 9.0 |
| Workers in the formal sector | 32.8 | 6.4 |
| Workers in the informal sector | 45.0 | 8.8 |
| Companies | 77.7 | 15.2 |
| Health system | 19.9 | 3.9 |
| Cities | 50.6 | 9.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szylovec, A.; Umbelino-Walker, I.; Cain, B.N.; Ng, H.T.; Flahault, A.; Rozanova, L. Brazil’s Actions and Reactions in the Fight against COVID-19 from January to March 2020. Int. J. Environ. Res. Public Health 2021, 18, 555. https://doi.org/10.3390/ijerph18020555
Szylovec A, Umbelino-Walker I, Cain BN, Ng HT, Flahault A, Rozanova L. Brazil’s Actions and Reactions in the Fight against COVID-19 from January to March 2020. International Journal of Environmental Research and Public Health. 2021; 18(2):555. https://doi.org/10.3390/ijerph18020555
Chicago/Turabian StyleSzylovec, Ana, Isis Umbelino-Walker, Brittany Nicole Cain, Hoi Tung Ng, Antoine Flahault, and Liudmila Rozanova. 2021. "Brazil’s Actions and Reactions in the Fight against COVID-19 from January to March 2020" International Journal of Environmental Research and Public Health 18, no. 2: 555. https://doi.org/10.3390/ijerph18020555
APA StyleSzylovec, A., Umbelino-Walker, I., Cain, B. N., Ng, H. T., Flahault, A., & Rozanova, L. (2021). Brazil’s Actions and Reactions in the Fight against COVID-19 from January to March 2020. International Journal of Environmental Research and Public Health, 18(2), 555. https://doi.org/10.3390/ijerph18020555