Antecedents and Consequences of Information Overload in the COVID-19 Pandemic


Abstract
1. Introduction
2. Literature Review
2.1. Health Information Overload and COVID-19
2.2. Antecedents of Information Overload
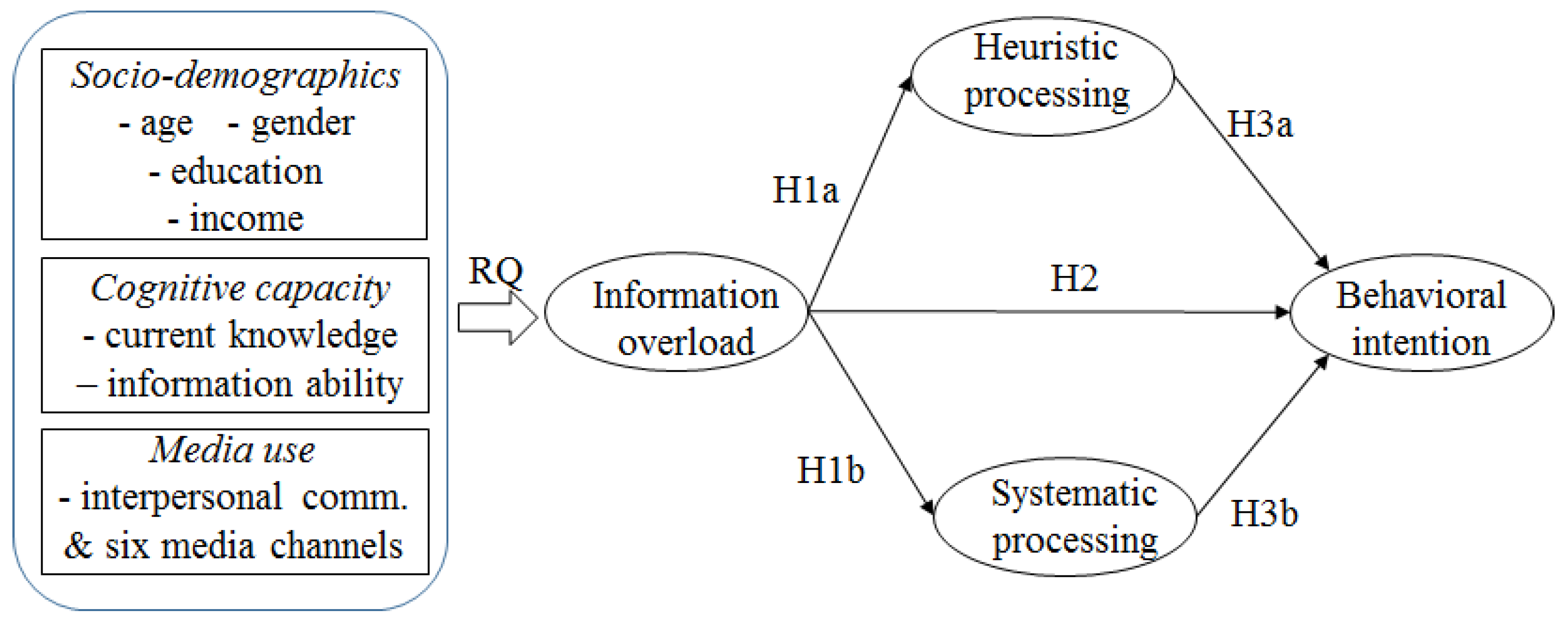
RQ: Does information overload differ across individual socio-demographic characteristics (i.e., age, gender, education level, and income level), cognitive capacity (i.e., current knowledge and information ability), and media use when obtaining COVID-19 information?
2.3. Consequences of Information Overload
2.3.1. Influence on Information Processing
2.3.2. Influence on Behavioral Intentions
3. Materials and Methods
3.1. Survey Procedure and Sample
3.2. Measurements
3.2.1. Perceived Information Overload
3.2.2. Information Processing
3.2.3. Behavioral Intentions
3.2.4. Cognitive Capacity
3.2.5. Media Use
3.2.6. Socio-Demographics
4. Results
5. Discussion
5.1. Antecedents of Information Overload
5.2. Consequences of Information Overload
5.3. Limitations of the Study and Suggestions for Future Studies
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. COVID-19 Dashboard. Available online: https://covid19.who.int/ (accessed on 10 October 2020).
- Chae, J. Who avoids cancer information? Examining a psychological process leading to cancer information avoidance. J. Health Commun. 2016, 21, 837–844. [Google Scholar] [CrossRef] [PubMed]
- Chae, J.; Lee, C.J.; Kim, K. Prevalence, predictors, and psychosocial mechanism of cancer information avoidance: Findings from a national survey of U.S. adults. Health Commun. 2020, 35, 322–330. [Google Scholar] [CrossRef] [PubMed]
- Jensen, J.D.; Carcioppolo, N.; King, A.J.; Scherr, C.L.; Jones, C.L.; Niederdeppe, J. The cancer information overload (CIO) scale: Establishing predictive and discriminant validity. Patient Educ. Couns. 2014, 94, 90–96. [Google Scholar] [CrossRef]
- Niederdeppe, J.; Lee, T.; Robbins, R.; Kim, H.K.; Kresovich, A.; Kirshenblat, D.; Standridge, K.; Clarke, C.E.; Jensen, J.; Fowler, E.F. Content and effects of news stories about uncertain cancer causes and preventive behaviors. Health Commun. 2014, 29, 332–346. [Google Scholar] [CrossRef] [PubMed]
- Chae, J.; Lee, C.J.; Jensen, J.D. Correlates of cancer information overload: Focusing on individual ability and motivation. Health Commun. 2016, 31, 626–634. [Google Scholar] [CrossRef] [PubMed]
- Chan, Y.M.; Huang, H. Weight management information overload challenges in 2007 HINTS: Socioeconomic, health status and behaviors correlates. J. Consum. Health Internet 2013, 17, 151–167. [Google Scholar] [CrossRef]
- Jiang, S.; Beaudoin, C.E. Health literacy and the internet: An exploratory study on the 2013 HINTS survey. Comput. Hum. Behav. 2016, 58, 240–248. [Google Scholar] [CrossRef]
- Kim, K.; Lustria, M.L.A.; Burke, D.; Kwon, N. Predictors of cancer information overload: Findings from a national survey. Inf. Res. 2007, 12, 12–14. [Google Scholar]
- Khaleel, I.; Wimmer, B.C.; Peterson, G.M.; Zaidi, S.T.R.; Roehrer, E.; Cummings, E.; Lee, K. Health information overload among health consumers: A scoping review. Patient Educ. Couns. 2020, 103, 15–32. [Google Scholar] [CrossRef]
- We are Social. Digital in 2020. Available online: https://wearesocial.com/digital-2020 (accessed on 30 November 2020).
- Gallup. Market 70-2B Report: The Use of Media, Contents, and Social Networking Services (before the Pandemic). Available online: https://www.gallup.co.kr/gallupdb/reportContent.asp?seqNo=1113 (accessed on 30 November 2020).
- Klerings, I.; Weinhandl, A.S.; Thaler, K.J. Information overload in healthcare: Too much of a good thing? Z. Evidenz Fortbild. Qual. Gesundh. 2015, 109, 285–290. [Google Scholar] [CrossRef]
- Jensen, J.D.; Pokharel, M.; Carcioppolo, N.; Upshaw, S.; John, K.K.; Katz, R.A. Cancer information overload: Discriminant validity and relationship to sun safe behaviors. Patient Educ. Couns. 2020, 103, 309–314. [Google Scholar] [CrossRef] [PubMed]
- Bawden, D.; Robinson, L. The dark side of information: Overload, anxiety and other paradoxes and pathologies. J. Inf. Sci. 2009, 35, 180–191. [Google Scholar] [CrossRef]
- Eppler, M.J.; Mengis, J. The concept of information overload: A review of literature from organization science, accounting, marketing, MIS, and related disciplines. Inf. Soc. 2004, 20, 325–344. [Google Scholar] [CrossRef]
- Schommer, J.C.; Doucette, W.R.; Worley, M.M. Processing prescription drug information under different conditions of presentation. Patient Educ. Couns. 2001, 43, 49–59. [Google Scholar] [CrossRef]
- Ji, Q.; Ha, L.; Sypher, U. The role of news media use and demographic characteristics in the possibility of information overload prediction. Int. J. Commun. 2014, 8, 16. [Google Scholar]
- Jensen, J.D.; Carcioppolo, N.; King, A.J.; Bernat, J.K.; Davis, L.; Yale, R.; Smith, J. Including limitations in news coverage of cancer research: Effects of news hedging on fatalism, medical skepticism, patient trust, and backlash. J. Health Commun. 2011, 16, 486–503. [Google Scholar] [CrossRef] [PubMed]
- Jensen, J.D.; Liu, M.; Carcioppolo, N.; John, K.K.; Krakow, M.; Sun, Y. Health information seeking and scanning among US adults aged 50–75 years: Testing a key postulate of the information overload model. Health Inform. J. 2017, 23, 96–108. [Google Scholar] [CrossRef]
- Lang, A. Using the limited capacity model of motivated mediated message processing to design effective cancer communication messages. J. Commun. 2006, 56, S57–S80. [Google Scholar] [CrossRef]
- Obamiro, K.; Lee, K. Information overload in patients with atrial fibrillation: Can the cancer information overload (CIO) scale be used? Patient Educ. Couns. 2019, 102, 550–554. [Google Scholar] [CrossRef]
- Ramírez, A.S.; Arellano Carmona, K. Beyond fatalism: Information overload as a mechanism to understand health disparities. Soc. Sci. Med. 2018, 219, 11–18. [Google Scholar] [CrossRef]
- Swar, B.; Hameed, T.; Reychav, I. Information overload, psychological ill-being, and behavioral intention to continue online healthcare information search. Comput. Hum. Behav. 2017, 70, 416–425. [Google Scholar] [CrossRef]
- Jensen, J.D.; King, A.J.; Carcioppolo, N.; Krakow, M.; Samadder, N.J.; Morgan, S. Comparing tailored and narrative worksite interventions at increasing colonoscopy adherence in adults 50–75: A randomized controlled trial. Soc. Sci. Med. 2014, 104, 31–40. [Google Scholar] [CrossRef] [PubMed]
- Chaiken, S.; Ledgerwood, A. A theory of heuristic and systematic information processing. In Handbook of Theories of Social Psychology; Van Lange, P.A.M., Kruglanski, A.W., Higgins, E.T., Eds.; Sage Publications Ltd.: Thousand Oaks, CA, USA, 2012; Volume 1, pp. 246–266. [Google Scholar]
- Chaiken, S.; Liberman, A.; Eagly, A.H. Heuristic and systematic information processing within and beyond the persuasion context. In Unintended Thought; The Guilford Press: New York, NY, USA, 1989; pp. 212–252. [Google Scholar]
- Eagly, A.H.; Chaiken, S. Process theories of attitude formation and change: The elaboration likelihood and heuristic-systematic models. In The Psychology of Attitudes; Eagly, A.H., Chaiken, S., Eds.; Harcourt Brace: Orlando, FL, USA, 1993; pp. 303–350. [Google Scholar]
- Han, P.K.J.; Moser, R.P.; Klein, W.M.P. Perceived ambiguity about cancer prevention recommendations: Associations with cancer-related perceptions and behaviours in a US population survey. Health Expect. 2007, 10, 321–336. [Google Scholar] [CrossRef] [PubMed]
- Jimenez, T.; Restar, A.; Helm, P.J.; Cross, R.I.; Barath, D.; Arndt, J. Fatalism in the context of COVID-19: Perceiving coronavirus as a death sentence predicts reluctance to perform recommended preventive behaviors. SSM-Popul. Health 2020, 11, 100615. [Google Scholar] [CrossRef]
- Ryu, Y.; Kim, S. Testing the heuristic/systematic information-processing model (HSM) on the perception of risk after the Fukushima nuclear accidents. J. Risk Res. 2015, 18, 840–859. [Google Scholar] [CrossRef]
- Trumbo, C.W. Information processing and risk perception: An adaptation of the heuristic-systematic model. J. Commun. 2002, 52, 367–382. [Google Scholar] [CrossRef]
- Embrain. Introduction to Online Research in Micromill-Embrain. Available online: https://embrain.com/upload/data/embrain_online.pdf (accessed on 30 November 2020).
- Yang, Z.J.; Rickard, L.N.; Harrison, T.M.; Seo, M. Applying the risk information seeking and processing model to examine support for climate change mitigation policy. Sci. Commun. 2014, 36, 296–324. [Google Scholar] [CrossRef]
- Yang, Z.J.; Kahlor, L. What, me worry? The role of affect in information seeking and avoidance. Sci. Commun. 2012, 35, 189–212. [Google Scholar] [CrossRef]
- Huerta, T.R.; Walker, D.M.; Johnson, T.; Ford, E.W. A time series analysis of cancer-related information seeking: Hints from the Health Information National Trends Survey (HINTS) 2003–2014. J. Health Commun. 2016, 21, 1031–1038. [Google Scholar] [CrossRef]
- Yang, Y.; Liu, K.; Li, S.; Shu, M. Social media activities, emotion regulation strategies, and their interactions on people’s mental health in COVID-19 pandemic. Int. J. Environ. Res. Public Health 2020, 17, 8931. [Google Scholar] [CrossRef]
- Chon, M.-G.; Park, H. Predicting public support for government actions in a public health crisis: Testing fear, organization-public relationship, and behavioral intention in the framework of the situational theory of problem solving. Health Commun. 2019, in press. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.L. COVID-19 information seeking on digital media and preventive behaviors: The mediation role of worry. Cyberpsychol. Behav. Soc. Netw. 2020, 23, 677–682. [Google Scholar] [CrossRef] [PubMed]
- Anwar, A.; Malik, M.; Raees, V.; Anwar, A. Role of mass media and public health communications in the COVID-19 pandemic. Cureus 2020, 12, e10453. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Infodemic Management: A Key Component of the COVID-19 Global Response. Wkly. Epidemiol. Rec. 2020, 95, 145–148. Available online: https://apps.who.int/iris/handle/10665/331775 (accessed on 30 November 2020).
- Iglesias-Sánchez, P.P.; Witt, G.F.V.; Cabrera, F.E.; Jambrino-Maldonado, C. The contagion of sentiments during the COVID-19 pandemic crisis: The case of isolation in Spain. Int. J. Environ. Res. Public Health 2020, 17, 5918. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Liu, Y. Media exposure and anxiety during COVID-19: The mediation effect of media vicarious traumatization. Int. J. Environ. Res. Public Health 2020, 17, 4720. [Google Scholar] [CrossRef]
- Hsu, C.-H.; Lin, H.-H.; Wang, C.-C.; Jhang, S. How to defend COVID-19 in Taiwan? Talk about people’s disease awareness, attitudes, behaviors and the impact of physical and mental health. Int. J. Environ. Res. Public Health 2020, 17, 4694. [Google Scholar] [CrossRef]
- Boczkowski, P.J.; Mitchelstein, E.; Matassi, M. “News comes across when I’m in a moment of leisure”: Understanding the practices of incidental news consumption on social media. New Media Soc. 2018, 20, 3523–3539. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Factors | Model 1 | Model 2 | ||||
|---|---|---|---|---|---|---|
| β | t | p | β | t | p | |
| Socio-Demographics | ||||||
| Gender | 0.030 | 0.736 | 0.462 | 0.019 | 0.541 | 0.589 |
| Age | −0.025 | −0.633 | 0.527 | 0.024 | 0.670 | 0.503 |
| Level of Education | −0.017 | −0.405 | 0.686 | −0.034 | −0.971 | 0.332 |
| Level of Household Income | −0.001 | −0.018 | 0.985 | 0.014 | 0.404 | 0.686 |
| Cognitive Capacity | ||||||
| Current Knowledge | −0.073 | −1.976 | 0.049 | |||
| Information Ability | −0.519 | −13.753 | <0.001 | |||
| Media Use | ||||||
| Interpersonal Communication | 0.115 | 3.268 | 0.001 | |||
| Television News | 0.025 | 0.658 | 0.511 | |||
| Newspaper | 0.005 | 0.141 | 0.888 | |||
| Online News Channels | 0.100 | 2.725 | 0.007 | |||
| Social Media | 0.057 | 1.577 | 0.115 | |||
| Mobile Applications | −0.056 | −1.425 | 0.155 | |||
| Government Channels | 0.049 | 1.300 | 0.194 | |||
| F = 0.301, p = 0.878 R2 = 0.002 | F = 21.371, p < 0.001 R2 = 0.312 ΔR2 = 0.310 (p < 0.001) | |||||
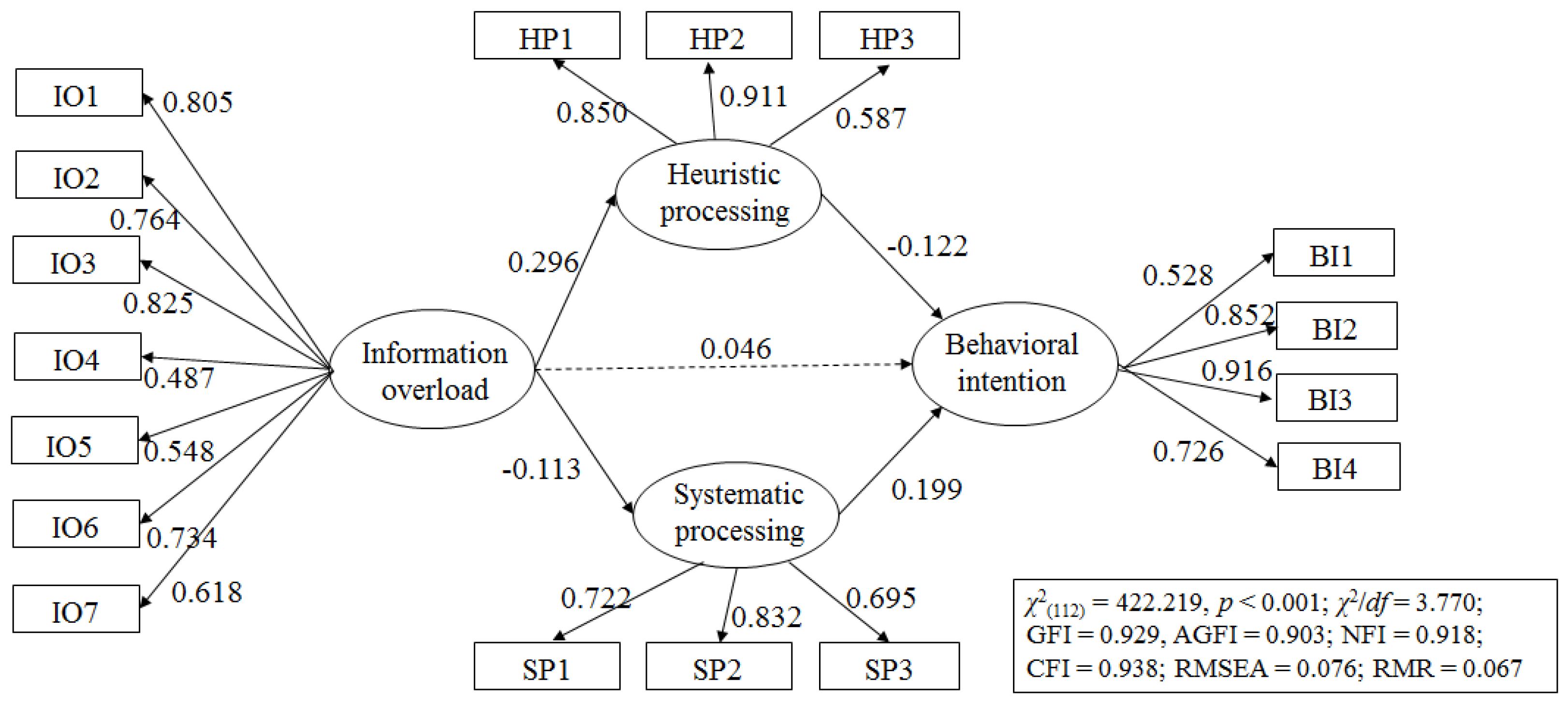
| β | B | S.E. | C.R. | p | |||
|---|---|---|---|---|---|---|---|
| Heuristic processing | ← | Information overload | 0.296 | 0.416 | 0.066 | 6.310 | <0.001 |
| Systematic processing | ← | Information overload | −0.113 | −0.117 | 0.049 | −2.373 | 0.018 |
| Behavioral intention | ← | Information overload | 0.063 | 0.046 | 0.032 | 1.445 | 0.149 |
| Behavioral intention | ← | Systematic processing | 0.285 | 0.199 | 0.041 | 4.865 | <0.001 |
| Behavioral intention | ← | Heuristic processing | −0.237 | −0.122 | 0.029 | −4.161 | <0.001 |
| IO7 | ← | Information overload | 0.618 | 1.000 | |||
| IO6 | ← | Information overload | 0.734 | 1.216 | 0.082 | 14.777 | <0.001 |
| IO5 | ← | Information overload | 0.548 | 0.876 | 0.074 | 11.769 | <0.001 |
| IO4 | ← | Information overload | 0.487 | 0.752 | 0.071 | 10.650 | <0.001 |
| IO3 | ← | Information overload | 0.825 | 1.509 | 0.094 | 15.988 | <0.001 |
| IO2 | ← | Information overload | 0.764 | 1.260 | 0.083 | 15.207 | <0.001 |
| IO1 | ← | Information overload | 0.805 | 1.344 | 0.085 | 15.741 | <0.001 |
| HP1 | ← | Heuristic processing | 0.850 | 1.000 | |||
| HP2 | ← | Heuristic processing | 0.911 | 1.072 | 0.046 | 23.212 | <0.001 |
| HP3 | ← | Heuristic processing | 0.587 | 0.701 | 0.046 | 15.315 | <0.001 |
| SP1 | ← | Systematic processing | 0.722 | 1.000 | |||
| SP2 | ← | Systematic processing | 0.832 | 1.087 | 0.066 | 16.447 | <0.001 |
| SP3 | ← | Systematic processing | 0.695 | 0.882 | 0.058 | 15.160 | <0.001 |
| BI1 | ← | Behavioral intention | 0.538 | 1.000 | |||
| BI2 | ← | Behavioral intention | 0.852 | 1.352 | 0.098 | 13.851 | <0.001 |
| BI3 | ← | Behavioral intention | 0.916 | 1.466 | 0.105 | 13.983 | <0.001 |
| BI4 | ← | Behavioral intention | 0.726 | 1.322 | 0.078 | 16.961 | <0.001 |
| Covariances | |||||||
| esysematic | ↔ | eheuristic | −0.533 | −0.253 | 0.028 | −9.088 | <0.001 |
| eBI1 | ↔ | eBI4 | 0.478 | 0.169 | 0.018 | 9.630 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hong, H.; Kim, H.J. Antecedents and Consequences of Information Overload in the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 9305. https://doi.org/10.3390/ijerph17249305
Hong H, Kim HJ. Antecedents and Consequences of Information Overload in the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2020; 17(24):9305. https://doi.org/10.3390/ijerph17249305
Chicago/Turabian StyleHong, Hyehyun, and Hyo Jung Kim. 2020. "Antecedents and Consequences of Information Overload in the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 17, no. 24: 9305. https://doi.org/10.3390/ijerph17249305
APA StyleHong, H., & Kim, H. J. (2020). Antecedents and Consequences of Information Overload in the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 17(24), 9305. https://doi.org/10.3390/ijerph17249305