The Environmental and Bitter Taste Endophenotype Determinants of Picky Eating in Australian School-Aged Children 7–12 years—A Cross-Sectional Pilot Study Protocol

 , , , and
, , , and 
Abstract
1. Introduction
2. Materials and Methods
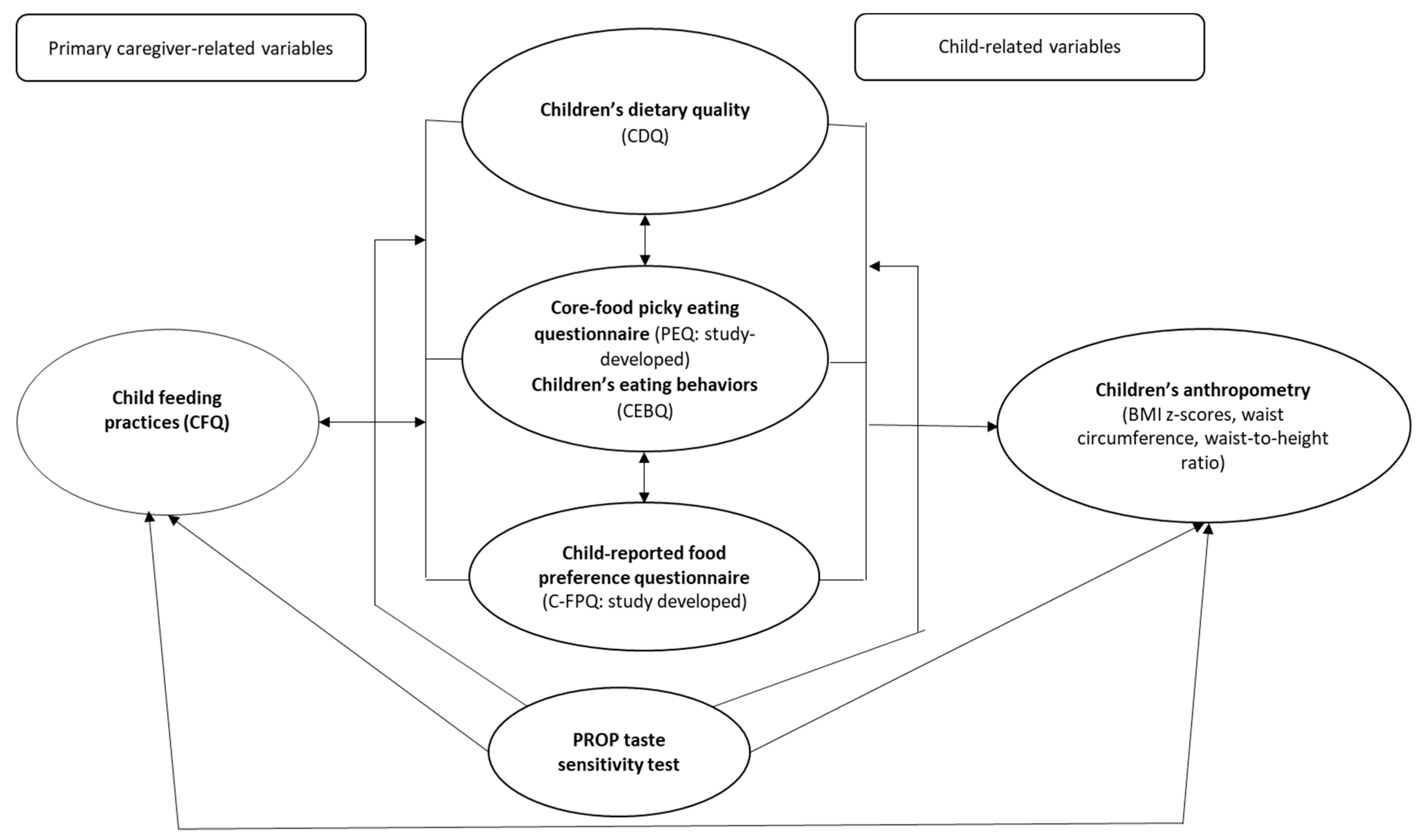
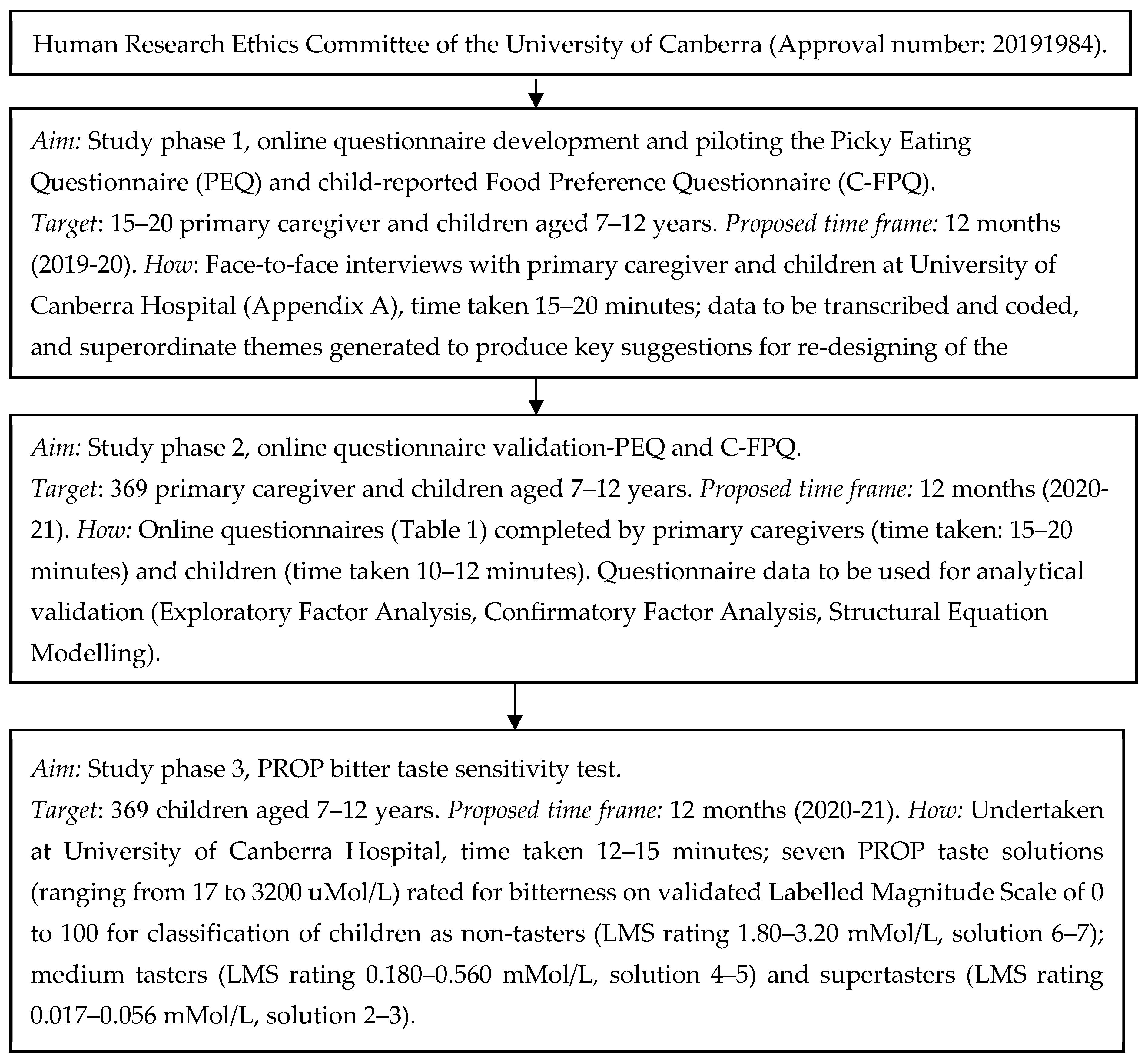
2.1. Study Design and Ethics
2.2. Participant Eligibility Criteria
2.3. Participant Recruitment
2.4. Sample Size
2.5. Data Collection
2.6. Data Analysis
3. Discussions
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
- Did the questionnaire link open and was it functional?
- Children only: Where you able to see all the food pictures? Did they download well?
- Did you complete the questionnaire on a PC/laptop or a cell phone?
- Are the formatting and layout of the questionnaire easy to follow? (Yes/No)
- If not, what modifications might make the online questionnaire easier to follow? (Probing: colour theme, font, font size, font colour, spacing, no. of questions per page)
- Parents only: Did you understand the scale? Was it easy to use the 10-point scale?
- Children only: Did you understand the scale? Was it easy to use the 5-point smiley scale?
- What do you think the questionnaire is trying to ask from you?
- Children only: Can you tell us in one or two sentences what these questions are asking you to do?
- Parents only: Were there any questions that you did not want to answer regarding your child’s food-related picky eating or that you felt uncomfortable answering?
- Were there any food items that were unfamiliar to you?
- In your opinion, were there any food items that may be more commonly known by other names?
- Did you select the ‘never tried’ option for any food items? If so, can you please give the reason for your answer (e.g., were you unfamiliar with the food, is it too expensive, or is it not eaten within your culture/religion?)? Go through the questionnaire with the mother/child and point out the ones that were selected as never tried.
- Do you think the questionnaire should have any other food items included? And why?
- Do you think the questionnaire should have specific food items removed? And why?
- Do you think ‘dried fruit’ should be separated into sultanas, dates, apricots, etc., or remain grouped together?
- Children only: Do you dislike dried fruits in general or are there some dried fruits that you like and some you do not?
- What did you select regarding liking ‘salad leaves’? Did you have trouble choosing a response? Do you think it would be better if we had two separate groups—one for raw salad leaves (lettuce, rocket) and one for larger cooked leaves (spinach, kale, bok choy)?
- Children only: Were the food pictures clear and easy to understand? (Yes/No)
- Children only: Were you confused about any specific food picture? What was confusing about the food picture? (Probing: looked like other food, such as Brussel sprouts and cabbage)
- Children only: Do you think the questionnaire should have any other food items included (e.g., peanut butter, Nutella, mushroom, pineapple)? And why?
- How much time did it take you to complete the questionnaire?
- In your opinion, is the questionnaire too long? (Yes/No)
- If you think it is too long, which strategies do you think will be useful to make the questionnaire feel less lengthy?
- Children only: Did the ‘smiley cartoons’ motivate you to continue completing the questionnaire?
- Children only: What else do you think will make the questionnaire more interesting and exciting for children your age to answer?
- Children only: Were there any answers you were not sure about and so you guessed them? Can you tell us why you had to guess some answers? (Probing: do not remember how it tastes, only tried it once, etc.)
- Do you have any other feedback that will help to improve the questionnaire?
References
- Samuel, T.; Musa-Veloso, K.; Ho, M.; Venditti, C.; Shahkhalili-Dulloo, Y. A Narrative Review of Childhood Picky Eating and Its Relationship to Food Intakes, Nutritional Status, and Growth. Nutrients 2018, 10, 1992. [Google Scholar] [CrossRef] [PubMed]
- Wolstenholme, H.; Kelly, C.; Hennessy, M.; Heary, C. Childhood fussy/picky eating behaviours: a systematic review and synthesis of qualitative studies. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Cole, N.C.; An, R.; Lee, S.-Y.; Donovan, S.M. Correlates of picky eating and food neophobia in young children: a systematic review and meta-analysis. Nutr. Rev. 2017, 75, 516–532. [Google Scholar] [CrossRef] [PubMed]
- Brown, C.L.; Vander Schaaf, E.B.; Cohen, G.M.; Irby, M.B.; Skelton, J.A. Association of picky eating and food neophobia with weight: a systematic review. Child. Obes. 2016, 12, 247–262. [Google Scholar] [CrossRef]
- Taylor, C.M.; Wernimont, S.M.; Northstone, K.; Emmett, P.M. Picky/fussy eating in children: Review of definitions, assessment, prevalence and dietary intakes. Appetite 2015, 95, 349–359. [Google Scholar] [CrossRef]
- Wardle, J.; Guthrie, C.A.; Sanderson, S.; Rapoport, L. Development of the children’s eating behaviour questionnaire. J. Child Psychol. Psychiatry Allied Discip. 2001, 42, 963–970. [Google Scholar] [CrossRef]
- Taylor, C.M.; Emmett, P.M. Picky eating in children: causes and consequences. Proc. Nutr. Soc. 2019, 78, 161–169. [Google Scholar] [CrossRef]
- Byrne, R.; Jansen, E.; Daniels, L. Perceived fussy eating in Australian children at 14 months of age and subsequent use of maternal feeding practices at 2 years. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 123. [Google Scholar] [CrossRef]
- Walton, K.; Kuczynski, L.; Haycraft, E.; Breen, A.; Haines, J. Time to re-think picky eating?: a relational approach to understanding picky eating. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 62. [Google Scholar] [CrossRef]
- Dubois, L.; Diasparra, M.; Bédard, B.; Kaprio, J.; Fontaine-Bisson, B.; Tremblay, R.; Boivin, M.; Pérusse, D. Genetic and environmental influences on eating behaviors in 2.5-and 9-year-old children: a longitudinal twin study. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 134. [Google Scholar] [CrossRef]
- Keller, K.L.; Reid, A.; MacDougall, M.C.; Cassano, H.; Song, J.L.; Deng, L.; Lanzano, P.; Chung, W.K.; Kissileff, H.R. Sex Differences in the Effects of Inherited Bitter Thiourea Sensitivity on Body Weight in 4–6-Year-Old Children. J. Obes. 2010, 18, 1194–1200. [Google Scholar] [CrossRef]
- Gibson, E.L.; Cooke, L. Understanding food fussiness and its implications for food choice, health, weight and interventions in young children: the impact of professor Jane Wardle. Curr. Obes. Rep 2017, 6, 46–56. [Google Scholar] [CrossRef]
- Joseph, P.V.; Reed, D.R.; Mennella, J.A. Individual differences among children in sucrose detection thresholds: relationship with age, gender, and bitter taste genotype. Nurs. Res. 2016, 65, 3. [Google Scholar] [CrossRef]
- Tepper, B.; Melis, M.; Koelliker, Y.; Gasparini, P.; Ahijevych, K.; Tomassini Barbarossa, I. Factors influencing the phenotypic characterization of the oral marker, PROP. Nutrients 2017, 9, 1275. [Google Scholar] [CrossRef]
- Jani Mehta, R.; Mallan, K.M.; Mihrshahi, S.; Mandalika, S.; Daniels, L.A. An exploratory study of associations between A ustralian-I ndian mothers’ use of controlling feeding practices, concerns and perceptions of children’s weight and children’s picky eating. Nutr. Diet. 2014, 71, 28–34. [Google Scholar] [CrossRef]
- Birch, L.L.; Fisher, J.O.; Grimm-Thomas, K.; Markey, C.N.; Sawyer, R.; Johnson, S.L. Confirmatory factor analysis of the Child Feeding Questionnaire: a measure of parental attitudes, beliefs and practices about child feeding and obesity proneness. Appetite 2001, 36, 201–210. [Google Scholar] [CrossRef]
- Birch, L.L.; McPhee, L.; Shoba, B.; Pirok, E.; Steinberg, L. What kind of exposure reduces children’s food neophobia?: Looking vs. tasting. Appetite 1987, 9, 171–178. [Google Scholar] [CrossRef]
- Carruth, B.R.; Skinner, J.; Houck, K.; Moran III, J.; Coletta, F.; Ott, D. The phenomenon of “picky eater”: a behavioral marker in eating patterns of toddlers. J. Am. Coll. Nutr. 1998, 17, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Carnell, S.; Wardle, J. Appetitive traits and child obesity: measurement, origins and implications for intervention: Symposium on ‘Behavioural nutrition and energy balance in the young’. Proc. Nutr. Soc. 2008, 67, 343–355. [Google Scholar] [CrossRef] [PubMed]
- Wardle, J.; Sanderson, S.; Gibson, E.L.; Rapoport, L. Factor-analytic structure of food preferences in four-year-old children in the UK. Appetite 2001, 37, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Ogden, J.; Roy-Stanley, C. How do children make food choices? Using a think-aloud method to explore the role of internal and external factors on eating behaviour. Appetite 2020, 147, 104551. [Google Scholar] [CrossRef] [PubMed]
- Guinard, J.-X. Sensory and consumer testing with children. Trends Food Sci. Technol. 2000, 11, 273–283. [Google Scholar] [CrossRef]
- Cole, N.C.; Wang, A.A.; Donovan, S.M.; Lee, S.-Y.; Teran-Garcia, M. Variants in chemosensory genes are associated with picky eating behavior in preschool-age children. J. Lifestyle Genom. 2017, 10, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A.; Kristal, A.; Cohen, J. Genetic taste responses to 6-n-propylthiouracil among adults: a screening tool for epidemiological studies. Chem. Senses 2001, 26, 483–489. [Google Scholar] [CrossRef] [PubMed]
- Mascola, A.J.; Bryson, S.W.; Agras, W.S. Picky eating during childhood: a longitudinal study to age 11 years. Eat. Behav. 2010, 11, 253–257. [Google Scholar] [CrossRef] [PubMed]
- Van Der Horst, K.; Deming, D.M.; Lesniauskas, R.; Carr, B.T.; Reidy, K.C. Picky eating: Associations with child eating characteristics and food intake. Appetite 2016, 103, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Magarey, A.; Golley, R.; Spurrier, N.; Goodwin, E.; Ong, F. Reliability and validity of the Children’s Dietary Questionnaire; a new tool to measure children’s dietary patterns. Int. J. Pediatric Obes. 2009, 4, 257–265. [Google Scholar] [CrossRef]
- Begg, M.D.; Parides, M.K. Separation of individual-level and cluster-level covariate effects in regression analysis of correlated data. J. Stat. Med. 2003, 22, 2591–2602. [Google Scholar] [CrossRef]
- Majorana, A.; Campus, G.; Anedda, S.; Piana, G.; Bossu, M.; Cagetti, M.; Conti, G.; D’Alessandro, G.; Strohmneger, L.; Polimeni, A. Development and validation of a taste sensitivity test in a group of healthy children. Eur. J. Paediatr. Dent. Off. J. Eur. Acad. Paediatr. Dent. 2012, 13, 147–150. [Google Scholar]
- Kothari, C.R. Research Methodology: Methods and Techniques; New Age International: Delhi, India, 2004. [Google Scholar]
- Dworkin, S.L. Sample Size Policy for Qualitative Studies Using in-Depth Interviews; Springer: Berlin/Heidelberg, Germany, 2012. [Google Scholar]
- Galloway, A.T.; Fiorito, L.; Lee, Y.; Birch, L.L. Parental pressure, dietary patterns, and weight status among girls who are “picky eaters”. J. Am. Diet. Assoc. 2005, 105, 541–548. [Google Scholar] [CrossRef]
- Jacobi, C.; Schmitz, G.; Agras, W.S. Is picky eating an eating disorder? Int. J. Eat. Disord. 2008, 41, 626–634. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.R.; Steer, C.D.; Rogers, I.S.; Emmett, P.M. Influences on child fruit and vegetable intake: sociodemographic, parental and child factors in a longitudinal cohort study. Public Health Nutr. 2010, 13, 1122–1130. [Google Scholar] [CrossRef] [PubMed]
- Rodenburg, G.; Kremers, S.P.; Oenema, A.; van de Mheen, D. Associations of children’s appetitive traits with weight and dietary behaviours in the context of general parenting. PLoS ONE 2012, 7, e50642. [Google Scholar] [CrossRef] [PubMed]
- Rydell, A.-M.; Dahl, M.; Sundelin, C. Characteristics of school children who are choosy eaters. J. Genet. Psychol. 1995, 156, 217–229. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. National Health Survey. First results, 2017-18. ABS Catalogue No. 4364.0.55.001; Australian Bureau of Statistics: Canberra, Australia, 2019.
- Daniels, L.A.; Magarey, A.; Battistutta, D.; Nicholson, J.M.; Farrell, A.; Davidson, G.; Cleghorn, G. The NOURISH randomised control trial: positive feeding practices and food preferences in early childhood-a primary prevention program for childhood obesity. BMC Public Health 2009, 9, 387. [Google Scholar] [CrossRef]
- Vennerød, F.F.F.; Hersleth, M.; Nicklaus, S.; Almli, V.L. The magic water test. An affective paired comparison approach to evaluate taste sensitivity in pre-schoolers. Food Qual. Prefer. 2017, 58, 61–70. [Google Scholar] [CrossRef][Green Version]
- Anliker, J.A.; Bartoshuk, L.; Ferris, A.M.; Hooks, L.D. Children’s food preferences and genetic sensitivity to the bitter taste of 6-n-propylthiouracil (PROP). Am. J. Clin. Nutr. 1991, 54, 316–320. [Google Scholar] [CrossRef]
- Baranowski, J.C.; Baranowski, T.; Beltran, A.; Watson, K.B.; Jago, R.; Callie, M.; Missaghian, M.; Tepper, B.J. 6-n-Propylthiouracil sensitivity and obesity status among ethnically diverse children. Public Health Nutr. 2010, 13, 1587–1592. [Google Scholar] [CrossRef]
- Green, B.G.; Shaffer, G.S.; Gilmore, M.M. Derivation and evaluation of a semantic scale of oral sensation magnitude with apparent ratio properties. Chem. Senses 1993, 18, 683–702. [Google Scholar] [CrossRef]
- Öter, B.; Ulukapı, I.; Ulukapı, H.; Topçuoğlu, N.; Çıldır, Ş. The relation between 6-n-propylthiouracil sensitivity and caries activity in schoolchildren. Caries Res. 2011, 45, 556–560. [Google Scholar] [CrossRef]
- Drewnowski, A.; Henderson, S.A.; Shore, A.B.; Barratt-Fornell. Nontasters, tasters, and supertasters of 6-n-propylthiouracil (PROP) and hedonic response to sweet. J. Physiol. Behav. 1997, 62, 649–655. [Google Scholar] [CrossRef]
- Drewnowski, A.; Henderson, S.A.; Shore, A.B. Taste responses to naringin, a flavonoid, and the acceptance of grapefruit juice are related to genetic sensitivity to 6-n-propylthiouracil. Am. J. Clin. Nutr. 1997, 66, 391–397. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Child Growth Standards based on length/height, weight and age. J. Acta Paediatr. 2006, 450, 76. [Google Scholar]
- World Health Organization. Waist Circumference and Waist-Hip Ratio: Report of a WHO Expert Consultation; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- Chamoun, E.; Mutch, D.M.; Allen-Vercoe, E.; Buchholz, A.C.; Duncan, A.M.; Spriet, L.L.; Haines, J.; Ma, D.W.; Study, G.F.H. A review of the associations between single nucleotide polymorphisms in taste receptors, eating behaviors, and health. Crit. Rev. Food Sci. Nutr. 2018, 58, 194–207. [Google Scholar] [CrossRef]
- Stoner, L.; Castro, N.; Kucharska-Newton, A.; Smith-Ryan, A.E.; Lark, S.; Williams, M.A.; Faulkner, J.; Skidmore, P. Food Consumption Patterns and Body Composition in Children: Moderating Effects of Prop Taster Status. Nutrients 2019, 11, 2037. [Google Scholar] [CrossRef]
- Keller, K.L.; Adise, S. Variation in the ability to taste bitter thiourea compounds: implications for food acceptance, dietary intake, and obesity risk in children. Annu. Rev. Nutr. 2016, 36, 157–182. [Google Scholar] [CrossRef]
- Sharafi, M.; Hayes, J.E.; Duffy, V.B. Masking vegetable bitterness to improve palatability depends on vegetable type and taste phenotype. Chemosens. Percept. 2013, 6, 8–19. [Google Scholar] [CrossRef]
- National Health and Medical Research Council. Australian Dietary Guidelines; National Health and Medical Research Council: Canberra, Australia, 2013. [Google Scholar]
- Carney, E.M.; Stein, W.M.; Reigh, N.A.; Gater, F.M.; Bakke, A.J.; Hayes, J.E.; Keller, K.L. Increasing flavor variety with herbs and spices improves relative vegetable intake in children who are propylthiouracil (PROP) tasters relative to nontasters. Physiol. Behav. 2018, 188, 48–57. [Google Scholar] [CrossRef]
- Rodrigues, J.F.; da Silva Andrade, R.; Bastos, S.C.; Coelho, S.B.; Pinheiro, A.C.M. Miracle fruit: An alternative sugar substitute in sour beverages. Appetite 2016, 107, 645–653. [Google Scholar] [CrossRef]
- Schwieterman, M.L.; Colquhoun, T.A.; Jaworski, E.A.; Bartoshuk, L.M.; Gilbert, J.L.; Tieman, D.M.; Odabasi, A.Z.; Moskowitz, H.R.; Folta, K.M.; Klee, H.J. Strawberry flavor: diverse chemical compositions, a seasonal influence, and effects on sensory perception. PLoS ONE 2014, 9, e88446. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Online Questionnaire Completed by Primary Caregivers (e.g., Mothers, Fathers) | ||
|---|---|---|
| Questionnaire Sections | Items Brief Description | Source |
| Information sheet | Brief overview of the study. | NA |
| Screening questions | Assess whether primary caregiver is eligible. | NA |
| Electronic consent form | Signed by primary caregivers to participate in Study phase 2 and an optional consent for their children to participate in study phase 3. | NA |
| Section 1: Child Feeding Questionnaire (CFQ) | Feeding strategies used by the primary caregiver. Measured on a 5-point Likert scale. | [16] |
| Section 2: Core foods Picky Eating Questionnaire (PEQ) * | Measures primary caregiver’s perception of their child’s pickiness to core foods: fruits; vegetables; meat and alternatives; breads and cereals; dairy. Measured on a 5-point Likert scale. | Adapted from [20,38] |
| Section 3: Child Eating Behaviour Questionnaire (CEBQ) | Four constructs measuring ‘food approach’ appetitive traits (e.g., emotional overeating) and four constructs measuring ‘food avoidance’ appetitive traits (slowness in eating). Measured on a 5-point Likert scale. | [6] |
| Section 4: Children’s Dietary Questionnaire (CDQ) | A 28-item semi-quantitative food frequency questionnaire to measure children’s actual intake of core (fruits, vegetables, dairy) and non-core (sugary beverages and sweet and savory snacks) foods and beverages. | [27] |
| Section 5: Primary caregiver and child sociodemographic covariates | Primary caregiver covariates, e.g., age, education, occupation, income, height, weight. Child covariates, e.g., age, gender, height, weight. | Study developed questions; [37] |
| Online Questionnaire Completed by Children Aged 7–12 Years | ||
| Information Sheet | Brief overview of the study. | NA |
| Electronic consent form | Signed by primary caregivers and children. | NA |
| Section 1: Child-reported Food Preference Questionnaire (C-FPQ) ** | Child’s food preferences to core foods: Fruits, vegetables, protein-rich (meat and alternatives, breads, etc.), carbohydrate-rich (cereals, etc.), dairy and non-core sweet and savory foods and beverages. Measured on a 5-point Likert scale. | Adapted from [20,38] |
| Analytical Objectives | IV | DV | Analytical Approach |
|---|---|---|---|
| Develop and pilot parent-reported PEQ and child-reported C-FPQ. | PEQ C-FPQ | NA | Transcription of interview data |
| Validate study developed questionnaires (PEQ, C-FPQ). | PEQ C-FPQ | Factorial validation indicators: root mean square error of approximation; Tucker Lewis Index; non-normed fit index; Comparative Fit Index | Exploratory Factor Analysis, Confirmatory Factor Analysis, Structural Equation Modelling |
| Direct association between supertaster status and primary caregiver-reported perceptions of picky eating. | Supertasters | PEQ mean scores | Bivariate: ANOVA, correlations Multivariate: Hierarchical regression controlling for sociodemographic covariates |
| Lower preference and intake of vegetables and greater preference and intake of sweet non-core foods among children identified as supertasters (using PROP protocol) and picky eaters (primary caregiver-reported). | Supertasters Picky eaters: PEQ mean scores | Food group preference: C-FPQ mean scores Food group intake: CDQ mean scores | |
| Direct association between child-feeding practice (e.g., pressure to eat) and children identified as supertasters (using PROP protocol) and picky eaters (primary caregiver-reported). | Supertasters Picky eaters: PEQ mean scores | E.g., pressure to eat mean scores from CFQ | |
| Inverse association between children identified as supertasters (using PROP protocol) and picky eaters (primary caregiver-reported) and anthropometric indices. | Supertasters Picky eaters: PEQ mean scores | Anthropometric indices: BMI z-scores, waist circumference, waist to height ratio |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jani, R.; Byrne, R.; Love, P.; Agarwal, C.; Peng, F.; Yew, Y.W.; Panagiotakos, D.; Naumovski, N. The Environmental and Bitter Taste Endophenotype Determinants of Picky Eating in Australian School-Aged Children 7–12 years—A Cross-Sectional Pilot Study Protocol. Int. J. Environ. Res. Public Health 2020, 17, 1573. https://doi.org/10.3390/ijerph17051573
Jani R, Byrne R, Love P, Agarwal C, Peng F, Yew YW, Panagiotakos D, Naumovski N. The Environmental and Bitter Taste Endophenotype Determinants of Picky Eating in Australian School-Aged Children 7–12 years—A Cross-Sectional Pilot Study Protocol. International Journal of Environmental Research and Public Health. 2020; 17(5):1573. https://doi.org/10.3390/ijerph17051573
Chicago/Turabian StyleJani, Rati, Rebecca Byrne, Penny Love, Cathy Agarwal, Fanke Peng, Yang Wai Yew, Demosthenes Panagiotakos, and Nenad Naumovski. 2020. "The Environmental and Bitter Taste Endophenotype Determinants of Picky Eating in Australian School-Aged Children 7–12 years—A Cross-Sectional Pilot Study Protocol" International Journal of Environmental Research and Public Health 17, no. 5: 1573. https://doi.org/10.3390/ijerph17051573
APA StyleJani, R., Byrne, R., Love, P., Agarwal, C., Peng, F., Yew, Y. W., Panagiotakos, D., & Naumovski, N. (2020). The Environmental and Bitter Taste Endophenotype Determinants of Picky Eating in Australian School-Aged Children 7–12 years—A Cross-Sectional Pilot Study Protocol. International Journal of Environmental Research and Public Health, 17(5), 1573. https://doi.org/10.3390/ijerph17051573