
The Impact of Hospital Competition on the Quality of Care in Europe: A Systematic Review



Abstract
1. Introduction
2. Defining Key Terms
3. Overview of the Relevant Reviews
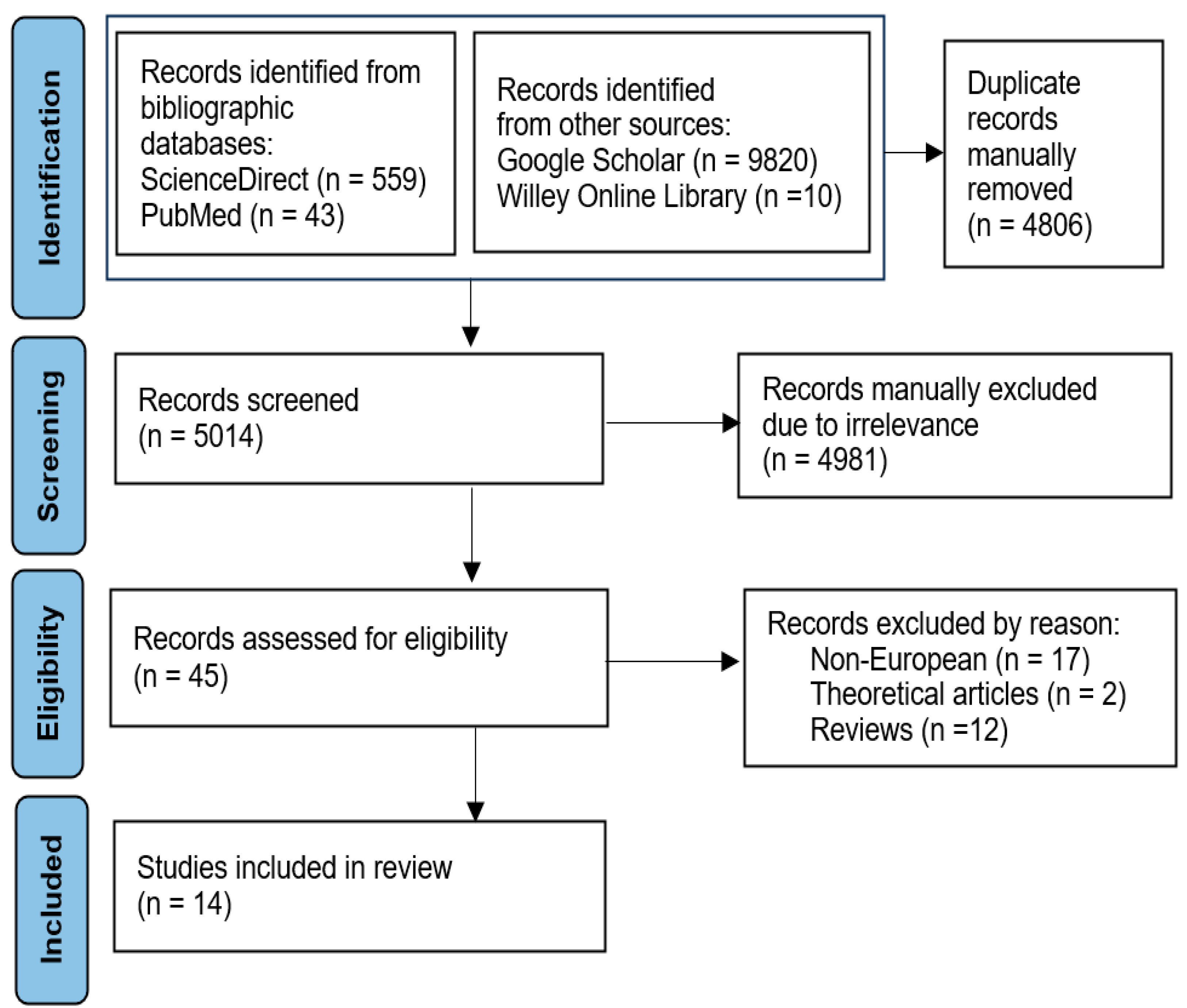
4. Methods and Data
5. Results
5.1. Descriptive Statistics
5.2. The Effects of Hospital Competition on Care Quality in Europe
5.2.1. Germany, France, the Netherlands, and Italy
5.2.2. Scandinavia
5.2.3. The United Kingdom
6. Discussion
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Bank Group. World Bank Group. World Development Report 1991: The Challenge of Development (English). In World Development Report; World Development Indicators: Washington, DC, USA, 1991; Available online: http://documents.worldbank.org/curated/en/888891468322730000/World-development-report-1991-the-challenge-of-development (accessed on 5 March 2024).
- Porter, M.E.; Teisberg, E.O. Redefining competition in health care. Harv. Bus. Rev. 2004, 82, 64–77. Available online: https://hbr.org/2004/06/redefining-competition-in-health-care (accessed on 5 March 2024). [PubMed]
- Porter, M. Competitive Strategy: Techniques for Analyzing Industries and Competitors; Free Press: New York, NY, USA, 1980. [Google Scholar]
- Porter, M.E.; Teisberg, E.O. Redefining Health Care: Creating Value-Based Competition on Results; Harvard Business Press: Boston, MA, USA, 2006. [Google Scholar]
- Grand, J.; Propper, C.; Robinson, R.V. Economics of Social Problems; Springer: London, UK, 1992; Available online: https://link.springer.com/book/10.1007/978-1-349-21930-8 (accessed on 5 March 2024).
- Dranove, D. Health care markets, regulators, and certifiers. In Handbook of Health Economics; Elsevier: Amsterdam, The Netherlands, 2011; pp. 639–690. [Google Scholar]
- Gaynor, M.; Town, R.J. Competition in health care markets. In Handbook of Health Economics; Pauly, M.V., McGuire, T.G., Barros, P.P., Eds.; Elsevier: Amsterdam, The Netherlands, 2011; Volume 2, pp. 499–637. [Google Scholar] [CrossRef]
- Robinson, J.C.; Luft, H.S. The impact of hospital market structure on patient volume, average length of stay, and the cost of care. J. Health Econ. 1985, 4, 333–356. [Google Scholar] [CrossRef] [PubMed]
- Gaynor, M.; Vogt, W.B. Antitrust and competition in health care markets. In Handbook of Health Economics; Culyer, A.J., Newhouse, J.P., Eds.; Elsevier: Amsterdam, The Netherlands, 2000; Volume 1, pp. 1405–1487. [Google Scholar] [CrossRef]
- Satterthwaite, M.A. Consumer information, equilibrium industry price, and the number of sellers. Bell J. Econ. 1979, 10, 483–502. [Google Scholar] [CrossRef]
- Delamater, P.L.; Messina, J.P.; Grady, S.C.; WinklerPrins, V.; Shortridge, A.M. Do more hospital beds lead to higher hospitalization rates? A spatial examination of Roemer’s law. PLoS ONE 2013, 8, e54900. [Google Scholar] [CrossRef]
- Luft, H.S.; Robinson, J.C.; Garnick, D.W.; Maerki, S.C.; McPhee, S.J. The role of specialized clinical services in competition among hospitals. Inquiry 1986, 23, 83–94. Available online: https://www.jstor.org/stable/29771762 (accessed on 5 March 2024).
- Ikegami, K.; Onishi, K.; Wakamori, N. Competition-driven physician-induced demand. J. Health Econ. 2021, 79, 102488. [Google Scholar] [CrossRef] [PubMed]
- Pan, J.; Qin, X.; Li, Q.; Messina, J.P.; Delamater, P.L. Does hospital competition improve health care delivery in China? China Econ. Rev. 2015, 33, 179–199. [Google Scholar] [CrossRef]
- Brekke, K.R.; Canta, C.; Siciliani, L.; Straume, O.R. Hospital competition in a national health service: Evidence from a patient choice reform. J. Health Econ. 2021, 79, 102509. [Google Scholar] [CrossRef]
- Centers for Medicare and Medicaid Services (CMS). Overview Prospective Payment Systems. Available online: https://www.cms.gov/medicare/payment/prospective-payment-systems?redirect=/prospmedicarefeesvcpmtgen/ (accessed on 5 March 2024).
- Turner, S.; Wright, J.S. The corporatization of healthcare organizations internationally: A scoping review of processes, impacts, and mediators. Public Adm. 2022, 100, 308–323. [Google Scholar] [CrossRef]
- Moscelli, G.; Gravelle, H.; Siciliani, L. Hospital competition and quality for non-emergency patients in the English NHS. RAND J. Econ. 2021, 52, 382–414. [Google Scholar] [CrossRef]
- Ranabhat, C.L.; Jakovljevic, M.; Dhimal, M.; Kim, C.B. Structural factors responsible for universal health coverage in low-and middle-income countries: Results from 118 countries. Front. Public Health 2020, 7, 414. [Google Scholar] [CrossRef] [PubMed]
- Or, Z.; Rococco, E.; Touré, M.; Bonastre, J. Impact of competition versus centralisation of hospital care on process quality: A multilevel analysis of breast cancer surgery in France. Int. J. Health Policy Manag. 2022, 11, 459–469. [Google Scholar] [CrossRef] [PubMed]
- Croes, R.R.; Krabbe-Alkemade, Y.J.; Mikkers, M.C. Competition and quality indicators in the health care sector: Empirical evidence from the Dutch hospital sector. Eur. J. Health Econ. 2018, 19, 5–19. [Google Scholar] [CrossRef] [PubMed]
- Pross, C.; Averdunk, L.H.; Stjepanovic, J.; Busse, R.; Geissler, A. Health care public reporting utilization–user clusters, web trails, and usage barriers on Germany’s public reporting portal Weisse-Liste.de. BMC Med. Inform. Decis. Mak. 2017, 17, 48. [Google Scholar] [CrossRef] [PubMed]
- Park, P.W.; Dryer, R.D.; Hegeman-Dingle, R.; Mardekian, J.; Zlateva, G.; Wolff, G.G.; Lamerato, L.E. Cost burden of chronic pain patients in a large integrated delivery system in the United States. Pain Pract. 2016, 16, 1001–1011. [Google Scholar] [CrossRef]
- Sari, N. Do competition and managed care improve quality? Health Econ. 2002, 11, 571–584. [Google Scholar] [CrossRef]
- Hudson, B. Competition and Collaboration in the New NHS; Centre for Health and the Public Interest: London, UK, 2013. [Google Scholar]
- Lewis, R.Q. More reform of the English National Health Service: From competition back to planning? Int. J. Health Serv. 2019, 49, 5–16. [Google Scholar] [CrossRef]
- Leichsenring, K.; Rodrigues, R.; Winkelmann, J.; Falk, R. Integrated Care, Competition and Choice-Removing barriers to care coordination in the context of market-oriented governance in Germany and Sweden. Int. J. Integr. Care. 2016, 16, 89. [Google Scholar] [CrossRef]
- Shishkin, S. Competition in Russian Healthcare. In HSE Working Paper; HSE University: Moscow, Russia, 2024. [Google Scholar]
- Mukamel, D.B.; Zwanziger, J.; Tomaszewski, K.J. HMO penetration, competition, and risk-adjusted hospital mortality. Health Serv. Res. 2001, 36 Pt 1, 1019–1035. Available online: https://pubmed.ncbi.nlm.nih.gov/11775665/ (accessed on 5 March 2024).
- Haley, D.R.; Zhao, M.; Spaulding, A.; Hamadi, H.; Xu, J.; Yeomans, K. The influence of hospital market competition on patient mortality and total performance score. Health Care Manager. 2016, 35, 266–276. [Google Scholar] [CrossRef]
- Strumann, C.; Geissler, A.; Busse, R.; Pross, C. Can competition improve hospital quality of care? A difference-in-differences approach to evaluate the effect of increasing quality transparency on hospital quality. Eur. J. Health Econ. 2022, 23, 1229–1242. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.C. The effect of financial pressure on the quality of care in hospitals. J. Health Econ. 2003, 22, 243–269. [Google Scholar] [CrossRef]
- Van der Schors, W.; Kemp, R.; Van Hoeve, J.; Tjan-Heijnen, V.; Maduro, J.; Peeters, M.J.; Siesling, S.; Varkevisser, M. Associations of hospital volume and hospital competition with short-term, middle-term and long-term patient outcomes after breast cancer surgery: A retrospective population-based study. BMJ Open 2022, 12, e057301. [Google Scholar] [CrossRef] [PubMed]
- Jürges, H.; Pohl, V. Medical guidelines, physician density, and quality of care: Evidence from German SHARE data. Eur. J. Health Econ. 2012, 13, 635–649. [Google Scholar] [CrossRef]
- Dzampe, A.K.; Takahashi, S. Competition and quality of care under regulated fees: Evidence from Ghana. Health Econ. Rev. 2022, 12, 57. [Google Scholar] [CrossRef]
- Scott, A.; Li, J.; Gravelle, H.; McGrail, M. Physician competition and low-value health care. Am. J. Health Econ. 2022, 8, 252–274. [Google Scholar] [CrossRef]
- Lin, X.; Jian, W.; Yip, W.; Pan, J. Perceived competition and process of care in rural China. Risk Manag. Healthc. Policy 2020, 13, 1161–1173. [Google Scholar] [CrossRef]
- Bloom, N.; Propper, C.; Seiler, S.; van Reenen, J. The impact of competition on management quality: Evidence from public hospitals. Rev. Econ. Stud. 2015, 82, 457–489. [Google Scholar] [CrossRef]
- Wong, H.S.; Zhan, C.; Mutter, R. Do different measures of hospital competition matter in empirical investigations of hospital behavior. Rev. Ind. Organ. 2005, 26, 27–60. [Google Scholar] [CrossRef]
- Advin House. Types of Hospitals. Available online: https://advinhealthcare.com/types-of-hospitals (accessed on 5 March 2024).
- Dranove, D.; White, W.D. Recent theory and evidence on competition in hospital markets. J. Econ. Manag. Strategy 1994, 3, 169–209. [Google Scholar] [CrossRef]
- Lu, L.; Pan, J. Does hospital competition lead to medical equipment expansion? Evidence on the medical arms race. Health Care Manag. Sci. 2021, 24, 582–596. [Google Scholar] [CrossRef] [PubMed]
- Kessler, D.P.; McClellan, M.B. Is hospital competition socially wasteful? Q. J. Econ. 2000, 115, 577–615. [Google Scholar] [CrossRef]
- Gowrisankaran, G.; Town, R.J. Competition, payers, and hospital quality. Health Serv. Res. 2003, 38, 1403–1422. [Google Scholar] [CrossRef] [PubMed]
- Moscelli, G.; Gravelle, H.; Siciliani, L.; Santos, R. Heterogeneous effects of patient choice and hospital competition on mortality. Soc. Sci. Med. 2018, 216, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Chong, F.; Jianping, Z.; Zhenjie, L.; Wenxing, L.; Li, Y. Does competition support integrated care to improve quality? Heliyon 2024, 10, e24836. [Google Scholar] [CrossRef] [PubMed]
- Wadhera, R.K.; Maddox, K.E.; Kazi, D.; Shen, C.; Yeh, R.W. Hospital revisits within 30 days after discharge for medical conditions targeted by the Hospital Readmissions Reduction Program in the United States: National retrospective analysis. BMJ 2019, 366, I4563. [Google Scholar] [CrossRef]
- Martsolf, G.R.; Nuckols, T.K.; Fingar, K.R.; Barrett, M.L.; Stocks, C.; Owens, P.L. Nonspecific chest pain and hospital revisits within 7 days of care: Variation across emergency department, observation and inpatient visits. BMC Health Serv. Res. 2020, 20, 1–8. [Google Scholar] [CrossRef]
- Gaynor, M.; Moreno-Serra, R.; Propper, C. Death by market power: Reform, competition, and patient outcomes in the National Health Service. Am. Econ. J. Econ. Policy 2013, 5, 134–166. [Google Scholar] [CrossRef]
- Cooper, Z.; Gibbons, S.; Skellern, M. Does competition from private surgical centres improve public hospitals’ performance? Evidence from the English National Health Service. J. Public Econ. 2018, 166, 63–80. [Google Scholar] [CrossRef]
- Aggarwal, A.K.; Sujenthiran, A.; Lewis, D.; Walker, K.; Cathcart, P.; Clarke, N.; Sullivan, R.; van der Meulen, J.H. Impact of patient choice and hospital competition on patient outcomes after prostate cancer surgery: A national population-based study. Cancer 2019, 125, 1898–1907. [Google Scholar] [CrossRef]
- Cerullo, M.; Sheckter, C.C.; Canner, J.K.; Rogers, S.O.; Offodile, A.C. Is bigger better?: The effect of hospital consolidation on index hospitalization costs and outcomes among privately insured recipients of immediate breast reconstruction. Ann. Surg. 2019, 270, 681–691. [Google Scholar] [CrossRef] [PubMed]
- Brekke, K.R.; Straume, O.R. Competition policy for health care provision in Norway. Health Policy 2017, 121, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Chandler, V.; Dilmaghani, M. Competition and childcare quality: Evidence from Quebec. J. Soc. Policy 2023, 1–26. [Google Scholar] [CrossRef]
- Feng, Y.; Pistollato, M.; Charlesworth, A.; Devlin, N.; Propper, C.; Sussex, J. Association between market concentration of hospitals and patient health gain following hip replacement surgery. J. Health Serv. Res. Policy. 2015, 20, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Skellern, M. The Effect of Hospital Competition on Value-Added Indicators of Elective Surgery Quality; Centre for Economic Performance: London, UK, 2019; Available online: https://cep.lse.ac.uk/_new/publications/abstract.asp?index=5440 (accessed on 5 March 2024).
- Berta, P.; Martini, G.; Moscone, F.; Vittadini, G. The association between asymmetric information, hospital competition and quality of healthcare: Evidence from Italy. J. R. Stat. Soc. A Stat. Soc. 2016, 179, 907–926. [Google Scholar] [CrossRef]
- Tay, A. Assessing competition in hospital care markets: The importance of accounting for quality differentiation. RAND J. Econ. 2003, 34, 786–814. Available online: https://www.jstor.org/stable/1593788 (accessed on 5 March 2024). [CrossRef]
- Propper, C.; Burgess, S.; Green, K. Does competition between hospitals improve the quality of care?: Hospital death rates and the NHS internal market. J. Pub. Econ. 2004, 88, 1247–1272. [Google Scholar] [CrossRef]
- Gaynor, M.; Propper, C.; Seiler, S. Free to choose: Reform and demand response in the British National Health Service. In CEP Discussion Paper No 1179; Centre for Economic Performance: London, UK, 2012; Available online: https://cep.lse.ac.uk/pubs/download/dp1179.pdf (accessed on 5 March 2024).
- Dranove, D.; Kessler, D.; McClellan, M.; Satterthwaite, M. Is more information better? The effects of “report cards” on health care providers. J. Polit. Econ. 2003, 111, 555–588. [Google Scholar] [CrossRef]
- Dranove, D.; Sfekas, A. Start spreading the news: A structural estimate of the effects of New York hospital report cards. J. Health Econ. 2008, 27, 1201–1207. [Google Scholar] [CrossRef]
- Luft, H.S.; Garnick, D.W.; Mark, D.H.; Peltzman, D.J.; Phibbs, C.S.; Lichtenberg, E.; McPhee, S.J. Does quality influence choice of hospital? JAMA 1990, 263, 2899–2906. [Google Scholar] [CrossRef]
- Howard, D.H. Quality and consumer choice in healthcare: Evidence from kidney transplantation. B.E. J. Econ. Anal. Policy 2006, 5, 0000101515153806531349. [Google Scholar] [CrossRef]
- Cooper, Z.; Gibbons, S.; Jones, S.; McGuire, A. Does hospital competition save lives? Evidence from the English NHS patient choice reforms. Econ. J. 2011, 121, F228–F260. [Google Scholar] [CrossRef] [PubMed]
- Beckert, W.; Christensen, M.; Collyer, K. Choice of NHS-Funded hospital services in England. Econ. J. 2012, 122, 400–417. [Google Scholar] [CrossRef]
- Varkevisser, M.; van der Geest, S.A.; Schut, F.T. Do patients choose hospitals with high quality ratings? Empirical evidence from the market for angioplasty in the Netherlands. J. Health Econ. 2012, 31, 371–378. [Google Scholar] [CrossRef]
- Ghiasi, A.; Zengul, F.D.; Ozaydin, B.; Oner, N.; Breland, B.K. The impact of hospital competition on strategies and outcomes of hospitals: A systematic review of the US hospitals 1996–2016. J. Health Care Finance 2018, 44, 22–42. Available online: https://healthfinancejournal.com/index.php/johcf/article/view/142 (accessed on 5 March 2024).
- Shen, V.C.; Ward, W.J., Jr.; Chen, L.K. Systematic review and meta-analysis on the effect of hospital competition on quality of care: Implications for senior care. Arch. Gerontol. Geriatr. 2019, 83, 263–270. [Google Scholar] [CrossRef]
- Jamalabadi, S.; Winter, V.; Schreyögg, J. A systematic review of the association between hospital cost/price and the quality of care. Appl. Health Econ. Health Policy 2020, 18, 625–639. [Google Scholar] [CrossRef]
- Jiang, Q.; Tian, F.; Liu, Z.; Pan, J. Hospital competition and unplanned readmission: Evidence from a systematic review. Risk Manag. Healthc. Policy 2021, 14, 473–489. [Google Scholar] [CrossRef]
- Mariani, M.; Sisti, L.G.; Isonne, C.; Nardi, A.; Mete, R.; Ricciardi, W.; Villari, P.; De Vito, C.; Damiani, G. Impact of hospital mergers: A systematic review focusing on healthcare quality measures. Eur. J. Public Health 2022, 32, 191–199. [Google Scholar] [CrossRef]
- Mills, C.A.; Yeager, V.A.; Unroe, K.T.; Holmes, A.; Blackburn, J. The impact of rural general hospital closures on communities—A systematic review of the literature. J. Rural Health 2024, 40, 238–248. [Google Scholar] [CrossRef]
- Mullens, C.L.; Hernandez, J.A.; Murthy, J.; Hendren, S.; Zahnd, W.E.; Ibrahim, A.M.; Scott, J.W. Understanding the impacts of rural hospital closures: A scoping review. J. Rural Health 2024, 40, 227–237. [Google Scholar] [CrossRef] [PubMed]
- Stansberry, T.T.; Roberson, P.N.; Myers, C.R. US rural hospital care quality and the effects of hospital closures on the health status of rural vulnerable populations: An integrative literature review. Nurs. Forum 2023, 1, 3928966. [Google Scholar] [CrossRef]
- Zander, N.; Dukart, J.; van den Berg, N.; Augustin, J. Identifying determinants for traveled distance and bypassing in outpatient care: A scoping review. Inquiry 2019, 56, 46958019865434. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, K.; Hashim, S.; Khankhara, M.; Said, I.; Shandakumar, A.T.; Zaman, S.; Veiga, A. What drives general practitioners in the UK to improve the quality of care? A systematic literature review. BMJ Open Qual. 2021, 10, e001127. [Google Scholar] [CrossRef] [PubMed]
- Bradow, J.; Smith, S.D.; Davis, D.; Atchan, M. A systematic integrative review examining the impact of Australian rural and remote maternity unit closures. Midwifery 2021, 103, 103094. [Google Scholar] [CrossRef]
- Yang, O.; Yong, J.; Scott, A. Nursing home competition, prices, and quality: A scoping review and policy lessons. Gerontologist 2022, 62, e384–e401. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef] [PubMed]
- Jakovljevic, M.; Timofeyev, Y.; Zhuravleva, T. The impact of pandemic-driven care redesign on hospital efficiency. Risk Manag. Healthc. Policy 2024, 17, 1477–1491. [Google Scholar] [CrossRef]
- Goro, S.; Challine, A.; Lefèvre, J.H.; Epaud, S.; Lazzati, A. Impact of interhospital competition on mortality of patients operated on for colorectal cancer faced to hospital volume and rurality: A cross-sectional study. PLoS ONE 2024, 19, e0291672. [Google Scholar] [CrossRef]
- Lisi, D.; Moscone, F.; Tosetti, E.; Vinciotti, V. Hospital quality interdependence in a competitive institutional environment: Evidence from Italy. Reg. Sci. Urban Econ. 2021, 89, 103696. [Google Scholar] [CrossRef]
- Guida, P.; Iacoviello, M.; Passantino, A.; Scrutinio, D. Measures of hospital competition and their impact on early mortality for congestive heart failure, acute myocardial infarction and cardiac surgery. Int. J. Qual. Health Care 2019, 31, 598–605. [Google Scholar] [CrossRef] [PubMed]
- Goude, F.; Kittelsen, S.A.; Malchau, H.; Mohaddes, M.; Rehnberg, C. The effects of competition and bundled payment on patient reported outcome measures after hip replacement surgery. BMC Health Serv. Res. 2021, 21, 387. [Google Scholar] [CrossRef] [PubMed]
- Avdic, D. Improving efficiency or impairing access? Health care consolidation and quality of care: Evidence from emergency hospital closures in Sweden. J. Health Econ. 2016, 48, 44–60. [Google Scholar] [CrossRef] [PubMed]
- Sundmacher, L.; Busse, R. The impact of physician supply on avoidable cancer deaths in Germany. A spatial analysis. Health Policy 2011, 103, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Bijlsma, M.J.; Koning, P.W.; Shestalova, V. The effect of competition on process and outcome quality of hospital care in the Netherlands. De Econ. 2013, 161, 121–155. [Google Scholar] [CrossRef]
- Ikkersheim, D.E.; Koolman, X. Dutch healthcare reform: Did it result in better patient experiences in hospitals? A comparison of the consumer quality index over time. BMC Health Serv. Res. 2012, 12, 76. [Google Scholar] [CrossRef] [PubMed]
- Heijink, R.; Mosca, I.; Westert, G. Effects of regulated competition on key outcomes of care: Cataract surgeries in the Netherlands. Health Policy 2013, 113, 142–150. [Google Scholar] [CrossRef] [PubMed]
- Semenova, Y.; Lim, L.; Salpynov, Z.; Gaipov, A.; Jakovljevic, M. Historical evolution of healthcare systems of post-soviet Russia, Belarus, Kazakhstan, Kyrgyzstan, Tajikistan, Turkmenistan, Uzbekistan, Armenia, and Azerbaijan: A scoping review. Heliyon 2024, 10, e29550. [Google Scholar] [CrossRef]
- Cookson, R.; Laudicella, M.; Donni, P.L. Does hospital competition harm equity? Evidence from the English National Health Service. J. Health Econ. 2013, 32, 410–422. [Google Scholar] [CrossRef]
- Kim, S.J.; Park, E.C.; Kim, S.J.; Han, K.T.; Jang, S.I. How did market competition affect outpatient utilization under the diagnosis-related group-based payment system? Int. J. Qual. Health Care 2017, 29, 399–405. [Google Scholar] [CrossRef]
- Kim, S.J.; Park, E.C.; Kim, S.J.; Han, K.T.; Han, E.; Jang, S.I.; Kim, T.H. The effect of competition on the relationship between the introduction of the DRG system and quality of care in Korea. Eur. J. Public Health 2016, 26, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Lin, X.; Cai, M.; Fu, Q.; He, K.; Jiang, T.; Lu, W.; Ni, Z.; Tao, H. Does hospital competition harm inpatient quality? Empirical evidence from Shanxi, China. Int. J. Environ. Res. Public Health 2018, 15, 2283. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.H.; Lu, N.; Tang, C.H.; Chang, H.C.; Huang, K.C. Assessing the relationship between healthcare market competition and medical care quality under Taiwan’s National Health Insurance programme. Eur. J. Public Health 2018, 28, 1005–1011. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Xu, D.R.; Zhang, Y.; Fu, H.; Wang, S.; Ju, K.; Chen, C.; Yang, L.; Jian, W.; Chen, L.; et al. Development of the China’s list of ambulatory care sensitive conditions (ACSCs): A study protocol. Glob. Health Res. Policy 2024, 9, 11. [Google Scholar] [CrossRef]
- Lu, Y.; Jiang, Q.; Zhang, X.; Lin, X.; Pan, J. Heterogeneous effects of hospital competition on inpatient quality: An analysis of five common diseases in China. Health Econ. Rev. 2024, 14, 28. [Google Scholar] [CrossRef]
- European Agency for Safety and Health at Work. Impact Assessment of Occupational Safety and Health Policy; European Agency for Safety and Health at Work: Bilbao, Spain, 2012; Available online: https://oshwiki.osha.europa.eu/en/themes/impact-assessment-occupational-safety-and-health-policy (accessed on 30 October 2024).
- OECD. Regulatory Impact Assessment Across the European Union in Better Regulation Practices Across the European Union; OECD Publishing: Paris, France, 2019. [Google Scholar] [CrossRef]
- Mutter, R.L.; Wong, H.S.; Goldfarb, M.G. The effects of hospital competition on inpatient quality of care. Inquiry 2008, 45, 263–279. [Google Scholar] [CrossRef]
- Jakovljevic, M.; Liu, Y.; Cerda, A.; Simonyan, M.; Correia, T.; Mariita, R.M.; Kumara, A.S.; Garcia, L.; Krstic, K.; Osabohienj, R.; et al. The Global South political economy of health financing and spending landscape–history and presence. J. Med. Econ. 2021, 24 (Suppl. S1), 25–33. [Google Scholar] [CrossRef]

{kind=link}
| № | Country | Year, Authors, Journal, Link | Sample | Methods | ‘Competition’ Proxy | ‘Quality of Care’ Proxy | Quality Aspect | Main Results | Institutional Setting |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Germany | 2022, Strumann et al., Eur J Health Econ [31] | Hospital-level panel data from 947 hospitals (n = 1894); 2006–2010 | Difference-in-differences | (1) Actual HHI, (2) predicted HHI, (3) the number of hospitals in the relevant market | The 30-day risk-adjusted mortality rate for stroke treatment | Objective output | “A homogenous positive effect of competition on quality of care is found. This effect is mainly driven by the response of non-profit hospitals that have a narrow range of services and private for-profit hospitals with a medium range of services”. | German hospitals provide primarily inpatient treatment and services. These hospitals are heterogeneous in terms of type and the range of services; they have a uniform DRG-based payment system. Patients are free to choose their provider. |
| 2 | France | 2022, Or et al., Int J Health Policy Manag [20] | 804 hospitals, patient-level data from 2 years: 2005 (n = 54,904) and 2012 (n = 62,250) | Multinomial logit model and [means of] multilevel models | (1) HHI based on actual hospital volumes for breast cancer surgery and volumes of any cancer surgery and (2) the hospital count within the market area as an exogenous measure of competition | The likelihood of providing innovative surgical procedures as a proxy of ‘process quality’ at the hospital level | Objective process | “The likelihood of receiving these procedures is significantly higher in hospitals located in more competitive markets. Yet, hospital volume remains a significant indicator of quality, therefore benefits of competition appear to be sensitive to the estimates of the impact of volume on care process. In France, the centralisation policy, with minimum activity thresholds, have contributed to improving breast cancer treatment between 2005 and 2012”. | France has a universal public health insurance system, with more than 95% of the hospital expenditure covered by public funding. Hospital care is provided by a large variety of public, private non-profit, and private for-profit entities. Patients can freely choose between public and private providers without a referral. Private hospitals have contracts with the public health insurance fund and are reimbursed based on regulated prices as public hospitals [20]. |
| 3 | France | 2024, Goro et al., PloS ONE [82] | Patients operated on for colorectal cancer in a hospital in mainland France from 726 hospitals (n = 152,235), 2015–2019 | A retrospective cross-sectional study; a mixed-effect model | The number of competitors per distance | The 30-day mortality rate after colorectal cancer surgery | Objective output | “Mortality at 30 days was 3.6% and we found that the mortality decreases with increasing of the hospital activity. Using the number of competitors per distance method, our study showed that a “highly competitive” and “moderately competitive” markets decreased mortality by 31% [OR: 0.69 (0.59, 0.80); p < 0.001] and by 12% respectively [OR: 0.88 (0.79, 0.99); p < 0.03], compared to the “non-competitive” market. High hospital volume (100 > per year) was also associated to lower mortality rate [OR: 0.74 (0.63, 0.86); p < 0.001]. Conclusions: The results of our studies show that increasing hospital competition independently decreases the 30-day mortality rate after colorectal cancer surgery. Hospital caseload, patients’ characteristics and age also impact the post-operative mortality”. | |
| 4 | the Netherlands | 2018, Croes et al., Eur J Health Econ [21] | Price and production data relating to three diagnosis groups from 87 Dutch hospitals (n = 474,410 patients) in the 2008–2011 | Panel regression models | HHI of the insurers that a hospital faces | The quality indicators from the ‘Dutch Healthcare Transparency Program’: process and structural indicators (with a ratio scale) rather than outcome indicators | Objective process | “We reveal a negative relationship between market share and quality score for two of the three diagnosis groups studied, meaning that hospitals in competitive markets have better quality scores than those in concentrated markets. We therefore conclude that more competition is associated with higher quality scores”. | The healthcare system in the Netherlands represents a setting with managed competition and compulsory healthcare coverage. Data on hospitals’ quality of care have been accessible to the public since 2008. |
| 5 | the Netherlands | 2022, van der Schors et al., BMJ Open [33] | 136,958 patients who underwent surgery for invasive breast cancer; 2004–2014 | Multilevel Cox survival regression models with hospital and year of surgery random effects | Number of proximate hospitals within a fixed radius | Surgical margins, 90 days re-excision, overall survival | Objective output | “[…] treatment types as well as patient and tumour characteristics explain most of the variation in all outcomes. After adjusting for confounding variables and intrahospital correlation in multivariate logistic regressions, hospital volume and competition from neighbouring hospitals did not show significant associations with surgical margins and re-excision rates. For patients who underwent surgery in hospitals annually performing 250 surgeries or more, multilevel Cox proportional hazard models show that survival was somewhat higher (HR 0.94). Survival in hospitals with four or more (potential) competitors within 30 km was slightly higher (HR 0.97). However, this effect did not hold after changing this proxy for hospital competition”. | The Dutch market-based healthcare system might face a trade-off between hospital volume and competition in the oncological care context, where centralization and collaboration aim to enhance patient outcomes. |
| 6 | Italy | 2021, Lisi et al., Reg Sci Urb Econ [83] | Administrative data on all patients admitted to any hospitals in Lombardy, 120,000–244,060 observations; 2008–2014 | A Conditional Auto-regressive specification (CAR) model and a Spatial Auto-regressive (SAR) model | The number of rivals within the block/within the catchment group (local competition); Between-block spatial weights (global competition) | 30-day mortality rate for AMI; 30-day mortality rate for ischaemic stroke; 30-day mortality rate for haemorrhagic stroke; 30-day mortality rate for hip fracture; 1-year readmission rate following hip replacement; 1-year readmission rate following knee replacement | Objective output | “Consistently with our micro-founded framework, our results show a significant positive degree of short- and long-range dependence, suggesting the existence of forms of local and global competition amongst hospitals with relevant implications for health care policy”. “[The] results point at the presence of small but significant hospital interdependence within catchment areas. On the other hand, we observe a marked heterogeneity among local markets and quality indicators, with the majority of areas indicating that hospital qualities are strategic complements, but also a few that are strategic substitutes. Conversely, our results on global interdependence are consistent among quality indicators, indicating that in our context hospital qualities tend to be strategic complements also outside catchment areas”. | The Italian NHS is highly decentralized. Financial resources are allocated to regions which are responsible for the organization and management of their regional healthcare [83]. |
| 7 | Italy | 2019, Guida et al., Int J Qual Health Care [84] | Patients discharged during 2015 for CHF or AMI, and between 2014 and 2015 for cardiac surgery (respectively, from 662, 395 and 91 hospitals) | Cross-sectional study; Spearman correlation tests | HHI; the number of competitors | Mortality for congestive heart failure (CHF), AMI, isolated-coronary artery bypass graft (CABG), or valve surgery | Objective output | “Indicators of competitions varied by condition and were sensitive to method used for the area definition. Hospital mortality after AMI and valve surgery increased with competition in areas identified by the variable-radius method (higher rates for a greater number of hospitals or lower HHIs). In area with fixed radius of 100–150 km, competition reduced mortality after CABG procedures (lower rates for a greater number of hospitals or smaller HHIs). Neither the number of hospitals nor HHI correlated with outcomes in CHF”. | |
| 8 | Italy | 2016, Berta et al., J Royal Stat Soc [57] | Patients who were admitted in 2012 to the cardiac surgery (n = 172,280), cardiology (n = 4,601,876), and general medicine (n = 12,700,700) wards in any public or private hospital in the Lombardy region that was financed by regional public funds | Multilevel models | HHI; Time distance from residence of patient i and hospital j (in minutes) | Hospital j 30-day mortality rate in ward w; Hospital j 30-day after discharge readmission rate in ward w; Hospital j composite index of adverse health outcomes (i.e., 30-day mortality or readmission) in ward w, Percentile rank of ward w in hospital j in the league table of the Lombardy quality evaluation programme | Objective output | “Our results show that no association exists between such adverse events and hospital competition. Our finding may be the result of asymmetric information, as well as the difficulty of building good quality health indicators”. | An environment where information on hospital quality is not publicly disclosed. |
| 9 | Norway | 2021, Brekke et al., J Health Econ [15] | Administrative data, covering the universe of hospital admissions in 64 NHS hospitals (n = 382,176 emergency patients); 1998–2005 | Difference-in-differences | Predicted HHI, computed using pre-reform market (patient) shares | AMI, stroke, or all-cause mortality | Objective output | “…hospitals in more competitive areas have a sharper reduction in AMI mortality but no effect on stroke mortality. […] competition reduces all-cause mortality, shortens length of stay, but increases readmissions, though the effects are small in magnitude. In years with high (DRG) prices, the negative effect on readmissions almost vanishes. Finally, exposure to competition tends to reduce waiting times and increase admissions, but the effects must be interpreted with care as the outcomes include elective treatments. | In 2001, non-price competition for hospitals within an NHS setting was introduced through the implementation of patient choice reform in Norway. |
| 10 | Sweden | 2021, Goude et al., BMC Health Serv Res [85] | Patient-level data on elective primary total hip replacements carried in 2008–2012, pre-reform (2008) and post-reform (2009–2012), (patient demography, the surgery and PROMs at baseline and at 1 year and 6 years’ follow-up); n = 36,627 | Difference-in-differences (in conjunction with entropy balancing) | (Quasi-experimental research design) | Patient-reported outcome measures (PROMs) of health gain (as indicated by the EQ-5D index and a visual analogue scale (VAS)), pain reduction (VAS), and patient satisfaction (VAS) 1 year and 6 years after the hip replacement surgery | Subjective output | “The entropy balancing was successful in creating balance in all covariates between treatment groups. No significant effects of the reform were found on any of the included PROMs at one- and six-years follow-up. The sensitivity analyses showed that the results were robust. Conclusions. Competition and bundled payment had no effects on the quality of hip replacement surgery as captured by post-surgery PROMs of health gain, pain reduction and patient satisfaction”. | In 2009, a pro-competitive reform was implemented, specifically targeting elective hip replacement surgeries in Stockholm. This reform centered around granting patients the autonomy to choose their healthcare provider, facilitating the establishment of new providers, and implementing a bundled payment model. |
| 11 | Sweden | 2016, Avdic, J Health Econ [86] | Swedish residents (n = 817,000) who were the subject of an AMI; 1990–2010 | Regression analysis (OLS) | The geographical distance in kilometers from AMI patient i’s home to his or her home hospital | The probability of surviving an AMI | Objective output | “Exploiting policy-induced variation in hospital distance derived from emergency hospital closures and detailed Swedish mortality data over two decades, results show a drastically decreasing probability of surviving an AMI as residential distance from a hospital increases one year after a closure occurred. The effect disappears in subsequent years, however, suggesting that involved agents quickly adapted to the new environment”. | |
| 12 | The UK | 2021, Moscelli et al., RAND J Econ [18] | Non-emergency NHS-funded patients treated in financial years 2002/3 to 2010/11 in NHS hospital sites only. N = 414,433 (hip replacement); n = 463,953 (knee replacement); n = 114,291 (coronary artery bypass grafts). Pre-choice period: financial years 2002/3 to 2005/6. Post-choice period: financial years 2006/7 to 2010/11 | Difference-in-differences | HHI | Quality for elective hip and knee replacement and CABG by whether the patient had an emergency admission within 28 days of discharge after their initial elective procedure | Objective output | “Public hospitals facing more rivals reduced quality, increased waiting times, and reduced length of stay for hip and knee replacements. This is likely due to regulated prices implying larger losses on these treatments compared to coronary artery bypass grafts, where no effects were found. Our findings are robust to estimation methods and competition measures, allowing for private providers’ entry”. | In the UK, a policy reform was introduced that relaxed constraints on patient selection of hospitals on the quality of three high-volume non-emergency medical treatments. |
| 13 | The UK | 2019, Aggarwal et al., Cancer [51] | Patients underwent prostate cancer surgery (n = 12,925); 2008–2011 | Multilevel logistic regression | The number of centers (hospitals) within a threshold distance | Postoperative length of hospital stay > 3 days, 30-day emergency readmissions, and 2-year urinary complications | Objective output | “With adjustment for patient characteristics, men who underwent surgery in centers located in a stronger competitive environment were less likely to have a 30-day emergency readmission, irrespective of the type or volume of procedures performed at each center (odds ratio, 0.46; 95% confidence interval, 0.36–0.60; p = 0.005). Men who received treatment at centers that were successful competitors were less likely to have a length of hospital stay > 3 days (odds ratio, 0.49; 95% confidence interval, 0.25–0.94; p = 0.02). Conclusions. The current results suggest for the first time that hospital competition improves short-term outcomes after prostate cancer surgery. Further evaluation of the potential role of patient choice and hospital competition is required to inform health service design in contrast to the role of top-down–driven approaches, which have focused on centralization of services”. | A competitive setting determined by the number of neighboring centers within a specified distance. |
| 14 | The UK | 2018, Moscelli et al., Soc Sci Med [45] | Patient-level data: AMI (n = 288,279 patients), hip fracture (n = 91,005 patients), stroke (n = 214,103 patients); 2002–2010 | A difference-in-differences with a continuous treatment variable (market structure) | HHI | AMI, hip fracture, and stroke risk adjusted mortality | Objective output | “We find that the choice reform reduced mortality risk for hip fracture patients by 0.62% (95% CI: 1.22%, 0.01%), compared with the 2002/3–2010/11 mean of 3.5%, but had statistically insignificant negative effects for AMI and stroke. The reform also had heterogeneous effects across AMI and stroke sub-diagnoses, reducing mortality for 3% of AMI patients and 21% of stroke patients. The reduction in hip fracture mortality was greater for more deprived patients. Policies to increase competition and give patients greater choice are likely to have heterogeneous effects depending on details of patient case mix and market conditions”. | In 2006, patient choice reform was implemented within the NHS. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Timofeyev, Y.; Goldenova, V.; Mantaeva, E.; Jakovljevic, M. The Impact of Hospital Competition on the Quality of Care in Europe: A Systematic Review. Healthcare 2024, 12, 2218. https://doi.org/10.3390/healthcare12222218
Timofeyev Y, Goldenova V, Mantaeva E, Jakovljevic M. The Impact of Hospital Competition on the Quality of Care in Europe: A Systematic Review. Healthcare. 2024; 12(22):2218. https://doi.org/10.3390/healthcare12222218
Chicago/Turabian StyleTimofeyev, Yuriy, Viktoriya Goldenova, Elza Mantaeva, and Mihajlo Jakovljevic. 2024. "The Impact of Hospital Competition on the Quality of Care in Europe: A Systematic Review" Healthcare 12, no. 22: 2218. https://doi.org/10.3390/healthcare12222218
APA StyleTimofeyev, Y., Goldenova, V., Mantaeva, E., & Jakovljevic, M. (2024). The Impact of Hospital Competition on the Quality of Care in Europe: A Systematic Review. Healthcare, 12(22), 2218. https://doi.org/10.3390/healthcare12222218