Abstract
Hereditary spastic paraplegia (HSP) is characterized by progressive lower limb spasticity. There is no disease-modifying treatment currently available. Therefore, standardized, validated outcome measures to facilitate clinical trials are urgently needed. We performed a scoping review of outcome measures and biomarkers for HSP to provide recommendations for future studies and identify areas for further research. We searched Embase, Medline, Scopus, Web of Science, and the Central Cochrane database. Seventy studies met the inclusion criteria, and eighty-three outcome measures were identified. The Spastic Paraplegia Rating Scale (SPRS) was the most widely used (27 studies), followed by the modified Ashworth Scale (18 studies) and magnetic resonance imaging (17 studies). Patient-reported outcome measures (PROMs) were infrequently used to assess treatment outcomes (28% of interventional studies). Diffusion tensor imaging, gait analysis and neurofilament light chain levels were the most promising biomarkers in terms of being able to differentiate patients from controls and correlate with clinical disease severity. Overall, we found variability and inconsistencies in use of outcome measures with a paucity of longitudinal data. We highlight the need for (1) a standardized set of core outcome measures, (2) validation of existing biomarkers, and (3) inclusion of PROMs in HSP clinical trials.
1. Introduction
Hereditary Spastic Paraplegia (HSP) refers to a group of inherited neurodegenerative conditions characterized by lower limb spasticity and weakness. HSP is rare, with a prevalence of 0.3 to 5.5 per 100,000 people, depending on country [1,2,3,4]. HSP is associated with significant disability and a negative impact on quality of life [5]. There are over 80 recognized HSP-associated genes with broad phenotypic variability [6,7,8]. Clinically, HSP can be categorized into pure HSP—symptoms limited to weakness, spasticity, impaired vibration sense in the lower limbs, and bladder dysfunction; and complex HSP—where there are additional neurological and non-neurological manifestations [9]. The phenotypic and genotypic heterogeneity of HSP and the rarity of the condition pose a challenge to the development of suitable outcome measures and biomarkers.
Advances in genetic testing have led to the rapid discovery of genes associated with HSP [10], accelerating the discovery of therapeutic targets. Patient-derived stem cell and animal models have identified potential drug treatment candidates targeting underlying pathogenesis for specific HSP genotypes, such as noscapine for HSP-SPAST [11,12,13,14,15]. Currently, the rate of drug discovery is far outpaced by the rate of gene discovery for HSP and a shift in HSP research to developing treatment options is required [10,16,17]. Outcome measures and biomarkers that can measure the efficacy of therapeutic interventions in clinical trials are needed to facilitate this.
The choice of appropriate outcome measures in interventional trials is critical to demonstrating a meaningful treatment effect [18]. Initiatives such as COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) and Core Outcome Measures in Effectiveness Trials (COMET) aim to guide the selection of appropriate outcome measures [19]. There is currently a lack of standardized outcome measures used in HSP clinical trials, with recent reviews of interventional trials in HSP showing heterogeneity of outcome measures [17,20]. Inconsistency of outcome measures leads to an increased risk of reporting bias due to post hoc selection of outcomes based on results rather than the use of pre-specified primary outcomes [21]. Furthermore, use of different outcome measures limits comparison and meta-analysis of results from different studies [21].
There are no current consensus guidelines for outcome measures in HSP clinical trials. To address this, we performed a scoping review of outcome measures and biomarkers in HSP to identify suitable outcome measures, provide recommendations for future HSP clinical trials, and identify areas for further research.
2. Materials and Methods
2.1. Search Strategy
This study was conducted according to published guidelines for conducting a systematic scoping review [22,23]. Under the guidance of an academic librarian, we performed a search in Embase, Medline, Scopus, Web of Science and the Central Cochrane databases using the search terms “Hereditary Spastic Paraplegia”, “biomarker”, “outcome measure”, and “patient reported outcome measure” (Appendix A). Additional studies were identified by searching the references of the included articles and relevant review articles.
2.2. Selection Criteria
We kept the selection criteria broad to capture all possible outcome measures and biomarkers. The inclusion criteria included studies involving patients with HSP of any age and gender, and that included a description of the outcome measures or biomarkers for HSP. Abstracts were included if novel outcome measures or biomarkers were described.
We excluded review articles, single-case reports, trial protocols with no published results, abstracts with no novel outcome measures/biomarkers, and articles that did not involve humans or human samples, did not include outcome measures/biomarkers, or were not in English.
2.3. Screening of Search Results
The screening and data extraction process was conducted using Covidence, a web-based collaboration software platform that streamlines the production of systematic and other literature reviews [24]. The first author (S.F.S.) excluded all irrelevant results—studies unrelated to HSP or not in English and duplicate studies. Authors S.F.S. and D.Y. independently reviewed the abstracts according to the selection criteria for the first 50 results. Authors S.F.S. and D.Y. independently reviewed the remaining abstracts, applying the finalized exclusion criteria.
2.4. Data Extraction and Analysis
Authors S.F.S., D.Y., L.R., and F.J. reviewed two full texts each to test the data extraction template. The template was modified by discussion at a team meeting. The team then reviewed six full texts, each with each author reviewing the same three articles as two other authors (~30% overlap) and met to resolve any discrepancies and standardize the extraction process. The rest of the studies were reviewed by one reviewer (D.Y., L.R., or F.J.) and verified by a second reviewer (S.F.S.). At each stage, discrepancies were resolved through a team meeting. The data were extracted using a standardized data extraction template, including information on study characteristics, aim of study, participant characteristics, characteristics of interventions, outcome measures, and ability of outcome measure to (i) distinguish patients versus controls, (ii) demonstrate change over time; (iii) show response to the intervention; and (iv) correlate with other measures. Study quality analysis was not performed, as is usual for scoping reviews [22].
Data were analyzed descriptively to provide an overview of study characteristics and outcome measures. Outcome measures were grouped according to the types of clinical outcome assessments as defined by the U.S. Food and Drug Administration [25]:
- Clinician-reported outcome measures (CROM): measurement of clinical signs or findings performed by a health professional.
- Performance outcome measures (PerfOM): measurement with a standardized task, either administered by a trained individual or undertaken by the patient without assistance.
- Patient-reported outcome measures (PROM): measurement of patient-reported health status.
Biomarkers were grouped according to the assessed modality:
- Laboratory-based biomarkers;
- Neuroimaging biomarkers;
- Neurophysiology biomarkers;
- Other biomarkers.
As other groups have previously published reviews of non-randomized interventional clinical trials [17,20], we chose to perform further analysis of randomized controlled trials (RCTs) to compare the outcome measures used, as RCTs are the study type with the highest level of evidence for treatment effectiveness [26].
3. Results
3.1. Search Results
A total of 1930 search results were identified, and 1437 abstracts were screened after duplicates were removed, of which 1222 were identified as irrelevant. The full texts of the remaining results (n = 215) were assessed according to inclusion criteria. Ten more studies were identified by searching the references of the included articles (Figure 1).
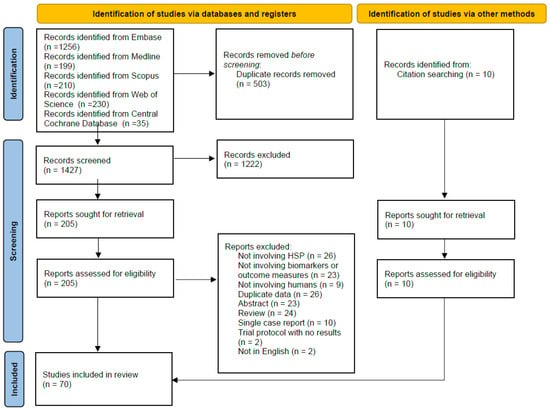
Figure 1.
PRISMA flow chart [27].
3.2. Study Characteristics
A total of 70 studies that met the inclusion criteria were identified. These studies were published between 1991 and 2022; date limits were not set to include as many studies as possible.
The majority (78.6%) of the included studies were observational studies, and only a quarter (25.7%) of studies were interventional studies. Most studies did not include longitudinal data (75.7%), and over half did not include a control group (51.4%). Participant genotype was predominantly mixed or unknown (65.7%), and sample sizes were small (mean of 36.99 participants) (Table 1). A list of all studies with relevant details is included as Supplementary Material S1.

Table 1.
Descriptive findings.
We assessed each outcome measure for (1) the ability to differentiate patients versus controls if a control group was included, (2) the ability to demonstrate disease progression if longitudinal data were included, (3) the ability to demonstrate response to the intervention if an intervention was assessed, and (4) any correlation with other biomarkers or outcome measures. Although we report the number of studies that fulfilled the criteria for (1), (2) and (3) to illustrate the available evidence for each outcome measure, it is important to note that (1) in studies with multiple outcome measures, the control group was compared to the patient group for some but not all outcome measures, (2) not all longitudinal studies were designed to assess the ability of an outcome measure to measure disease progression, (3) an outcome measure may not demonstrate a response to the intervention for many reasons including efficacy of intervention, duration of trial, and timing of the outcome measure relative to the intervention.
3.3. Clinical Outcome Assessments
3.3.1. Clinician Reported Outcome Measures
The Spastic Paraplegia Rating Scale (SPRS) was the most widely used CROM, reported in twenty-seven studies (Table 2). Although 12/27 included studies control groups, a comparison of SPRS scores in patients versus controls was performed in only two studies, both showing significant differences [28,29]. It is important to note that SPRS values from healthy controls are most relevant when comparing to pre-symptomatic HSP carriers rather than for comparison to individuals with symptomatic HSP. 8/27 studies were longitudinal, and only six of those studies showed disease progression over time with the SPRS (median follow-up time 12–31 months) [30,31,32,33,34,35]. The SPRS was used as an outcome measure in 4/18 interventional studies and showed a response to the intervention in only one of the four studies [36]. The SPRS was commonly used to correlate with other biomarkers or outcome measures (21/27 studies) (see Supplementary Material S2).
Table 2.
Clinician-reported outcome measures.
The SPATAX-EUROSPA disability score, another HSP-specific CROM, was less commonly used than the SPRS (Table 2). There were no control data and change over time was studied in only one study showing disease progression in 3/31 patients included in the study [32]. It was used in one interventional study [37] and did not show any significant change with intervention.
CROMs developed for other neurological conditions and generic functional CROMs were also used to assess patients with HSP. The Scale for Assessment and Rating of Ataxia (SARA) was used in three studies and showed a difference between patient versus controls in 1/3 studies [38] and longitudinal change in 1/3 studies [39]. The Amyotrophic Lateral Sclerosis rating scale revised (ALSFRS-R) was used in two studies [40,41], showing disease progression in one but not the other, and was shown to correlate with serum and CSF neurofilament heavy chain [40,41], though one paper included patients with ALS in their analysis (Supplementary Material S2).
3.3.2. Performance Outcome Measures
PerfOMs assessing motor function were widely used in the included studies, with twenty-one different outcome measures identified. The most commonly reported motor PerfOMs were the modified Ashworth Scale (MAS) (18 studies) and the 10 m walk test (10MWT), 6 min walk test (6MWT) and their variations (14 studies) (Table 3). Compared to CROMs, motor PerfOMs were more commonly used as outcome measures for interventional studies—MAS in 13/18 interventional studies, 10MWT/6MWT/variations in 9/18 interventional studies. Conversely, motor PerfOMs were less commonly used to correlate with other outcome measures or biomarkers, 2/18 studies for MAS and 3/14 studies for 10MWT and its variations (Supplementary Materials S2). Similar to the CROMs, there were very little longitudinal data—3/18 for MAS, 1/14 for 10MWT and variations.
Table 3.
Performance outcome measures.
PerfOMs measuring cognition were used in ten studies for descriptive purposes only rather than to measure outcomes in interventional studies.
3.3.3. Patient Reported Outcome Measures
Most PROMs used assessed quality of life (12/17), while others assessed fatigue, pain, and autonomic symptoms (Table 4). The most used PROM was the Short Form Health Survey-36 (SF-36) and its derivative, SF-12, in seven studies, followed by EuroQoL-5 Dimensions (EQ-5D) in three studies. PROMs were not commonly used in interventional studies (5/18 interventional studies). There was no longitudinal data for PROMs in the included studies. The SF-36 and its derivatives, EQ-5D, Becks Depression Inventory (BDI-V), Zung depression score, Brief Pain inventory, Modified Fatigue Impact Scale and multidimensional fatigue inventory showed differences between patients and controls in some but not all studies.
Table 4.
Patient-Reported Outcome Measures.
3.4. Biomarkers
3.4.1. Laboratory-Based Biomarkers
Serum and cerebrospinal fluid (CSF) neurofilament light chain (NfL) levels, and serum and CSF 25- and 27-hydroxycholesterol (25- and 27-OHC) levels were the two most studied biochemical biomarkers—included in six and four studies, respectively (Table 5). Serum and CSF NfL levels were able to differentiate patient vs. control groups or historical control values in all studies. Serum and CSF NfL levels were shown to correlate with SPRS scores in two studies [29,42] but this correlation was not present in the other two studies [32,43] (Supplementary Material S2). Plasma and CSF 25- and 27-OHC were significantly elevated in individuals with HSP-CYP7B1 (SPG5) compared to controls or reported normative values in all four studies [35,43,44,45]. In the few longitudinal studies, there was no change over time in NfL levels [32] or 25- and 27-OHC levels [35,44]. NfL levels were not used as outcome measures in any interventional studies; however, 25- and 27-OHC levels showed a response to treatment with statins in interventional studies [35,44]. Other biochemical markers reported, such as lipidomics, amino acid levels, mitochondrial DNA levels and cell morphomics, were more commonly used as diagnostic biomarkers rather than to measure disease progression or response to the intervention.
Table 5.
Biochemical Biomarkers.
3.4.2. Neuroimaging Biomarkers
Magnetic resonance imaging (MRI) of the brain and spine, with or without volumetric analysis, was used in seventeen studies, diffusion tensor imaging (DTI) in seven studies and magnetic resonance spectroscopy (MRS) in four studies (Table 6). MRI brain and spine differentiated patients vs. controls in six studies and showed longitudinal change in only one study [46]. No imaging parameters were used as outcome measures for interventional studies. MRI findings were found to correlate with SPRS scores in 3/4 of the studies, and DTI findings correlated with SPRS scores in 2/3 of the studies (Supplementary Materials S2).
Table 6.
Neuroimaging Biomarkers.
3.4.3. Neurophysiology Biomarkers
Motor evoked potentials (MEPs) and nerve conduction studies/electromyography (NCS/EMG) were the most widely used neurophysiological markers, being used in ten and nine studies, respectively (Table 7). Although MEPs were used as outcome measures in three interventional studies, no changes in MEP results were demonstrated in response to any of the interventions. NCS/EMG, somatosensory evoked potentials (SSEPs), visual evoked potentials (VEPs) and brainstem auditory evoked potentials (BAEPs) were mostly used as descriptive measures with few studies using these measures to compare patients versus controls, study longitudinal cohorts, or to evaluate interventions.
Table 7.
Neurophysiology Biomarkers.
3.4.4. Other Biomarkers
We identified eight studies that utilized gait analysis—seven were laboratory-based, and one was a mobile system [34] (Table 8). Four studies described the use of an infrared multi-camera motion analysis system [28,47,48,49], one used pressure sensors [50], and another two did not provide details of the gait analysis system used [51,52] (Supplementary Material S1). Four interventional studies used gait analysis as an outcome measure, with only two of those studies showing a response to the intervention [49,50]. Gait analysis was able to differentiate patients with HSP from patients with spastic diplegia [47], healthy controls [34,48] and pre-symptomatic HSP-SPAST carriers [28]. Gait parameters also correlate with SPRS scores [28,34] (Supplementary Table S2).
Table 8.
Other Biomarkers.
SD-OCT was investigated in four studies, with one study showing statistically significant retinal nerve fiber layer (RNFL) thinning in patients compared to normative values but no change over time (Table 8).
Video-oculography and rotational chair testing and speech assessment showed differences between patients vs. controls [53,54].
3.4.5. Genotype-Specific Biomarkers in HSP
We identified biomarkers that were specific to particular HSP genotypes (Table 9). The most widely studied were serum and CSF oxysterols, 25- and 27-hydroxycholesterol (25- and 27-OHC) levels, in HSP-CYP7B1 or SPG5. 25- and 27-OHC levels were significantly elevated in the serum and CSF of patients compared to healthy controls. Plasma and serum oxysterol levels were used as outcome measures in two clinical trials showing reduced levels with atorvastatin treatment but no clinical correlation [35,44]. Most genotype-specific biomarkers were reported in single studies, with some studies (citrulline, lipidomics, glycosylceramide profile, and scanning electron microscopy of hair shafts) having small patient numbers (n ≤ 5).
Table 9.
Genotype-specific biomarkers.
3.5. Randomized Controlled Trials in HSP
We identified eight randomized controlled trials published over two decades (Supplementary Material S3). Of note, 5/8 RCTs we reviewed were not included in previously published reviews.
Six studies used a crossover design, while two studies were parallel randomized trials. Only two studies recruited patients with a single specific HSP genotype; the other six included mixed and unknown genotypes. All studies had small sample sizes (range 8–49). Two studies did not define a primary outcome measure [37,62]. Four studies showed a positive response to treatment. The outcome measures were heterogeneous, with no consistency between studies despite six studies aiming to evaluate spasticity in response to the intervention. The most common outcome measures used were the 10MWT and modified Ashworth score, with two positive studies showing a significant improvement in MAS with treatment [62,63]. Study durations were generally short—only one study had a duration of more than 6 months [64]. There was no clear association between the duration of the trial and response to the intervention.
4. Discussion
In this scoping review, we compiled a comprehensive list of outcome measures used in HSP (Figure 2) and categorized them according to construct (Table 2, Table 3, Table 4, Table 5, Table 6, Table 7 and Table 8), with information on key measurement properties. This is an important resource to inform the choice of outcome measures for future clinical trials in HSP. We identified eighty-three outcome measures highlighting the heterogeneity and inconsistency of outcome measures used. We identify a need for standardized outcome measures and recommendations for use in clinical trials, such as core outcome sets (COS) developed for other neurological conditions [19,65]. We identify common limitations of the included studies in this review (Figure 3) and list the advantages and disadvantages of commonly used outcome measures (Table 10).
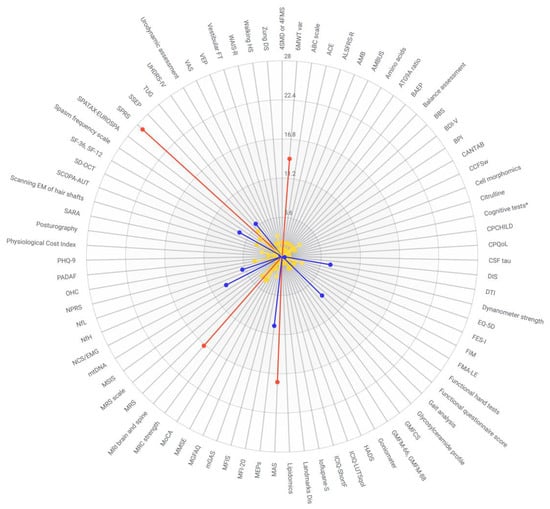
Figure 2.
Outcome measures for hereditary spastic paraplegia according to frequency reported (Yellow 1–5 studies, Blue 6–10 studies, Red >10 studies). 4SMD or 4FMS—Four-stage functional scale of motor disability; 6MWT var—Six minute walk test and variations; ABC scale—Activities-specific Balance Confidence Scale; ACE—Addenbrooke’s Cognitive Exam; ALSFRS-R—Amyotrophic Lateral Sclerosis Rating Scale Revised; AMB—Ambulatory score; AMBUS—Distance walked in meters walked in 5 s without help; ATG9A ratio—Autophagy-related protein 9A ratio; BAEP—brainstem auditory evoked potentials; BBS—Berg Balance Scale; BDI-V—Becks Depression Inventory; BPI—Brief Pain Inventory; CANTAB—CANTAB cognitive assessment; CCFSw—Composite Cerebellar Functional Severity Score; Cognitive tests*—Verbal Learning and Memory Test, Farbe-Wort-Interferenz Test, Trail Making Test Part A and B, Frontal Assessment Battery, revised d2 Test of attention, Regensburg Word Fluency Test; CPCHILD—Caregiver Priorities and Child Health Index of Life with Disabilities; CPQoL—Cerebral Palsy quality of life questionnaire; DIS—Disability score; DTI—diffusion tensor imaging; EQ-5D—EuroQoL 5 Dimensions; FES-I—Falls Efficacy Scale-International; FIM—Functional Independence Measure; FMA-LE—Lower extremity subclass of Fugl–Meyer assessment; GMFCS—Gross Motor Function Classification Score; GMFM—Gross Motor Function Measure; HADS—Hospital Anxiety and Depression Scale; ICIQ-LUTSqol—International Consultation of Incontinence Questionnaire lower urinary tract symptoms quality of life; ICIQ-ShortF—International Consultation of Incontinence Questionnaire Short Form; Ioflupane-S—Ioflupane-single photon emission computed tomography (SPECT); Landmarks Dis—Landmarks of Disability; MAS—Modified Ashworth Scale; MEPs—motor evoked potentials; MFI-20—Multidimensional Fatigue Inventory; MFIS—Modified Fatigue Impact Scale; mGAS—Modified Goal Attainment Scale; MGFAQ—Modified version of Gillette Functional Assessment Questionnaire; MMSE—Mini-Mental State Exam; MoCA—Montreal Cognitive Assessment; MRC—Medical Research Council muscle strength; MRI—magnetic resonance imaging; MRS—magnetic resonance spectroscopy; MRScale—Modified Rankin Scale; MSIS—Multiple Sclerosis Impairment Scale; mtDNA—mitochondrial DNA load; NCS/EMG—nerve conduction studies/electromyography; NfH—Neurofilament heavy chain; NfL—Neurofilament light chain; NPRS—Numeric rating scale for pain; OHC—25 and 27 hydroxycholesterol; PADAF—protocol for evaluation of acquired speech disorder; PHQ-9—Patient Health Questionnaire; SARA—Scale for Assessment and Rating of Ataxia; scanning EM of hair shafts—scanning electron microscopy of hair shafts; SCOPA-AUT—Scale for Outcomes in Parkinson’s Disease for Autonomic Symptoms; SD-OCT—spectral domain optical coherence tomography; SF-36, SF-12—Short Form 36, Short Form 12; SPRS—Spastic Paraplegia Rating Scale; SSEP—Somatosensory evoked potentials; TUG—Timed Up-and-Go test; UHDRS-IV—Unified Huntington’s Disease Rating Scale Part IV; VAS—Visual Analogue Score; VEP—visual evoked potentials; Vestibular FT—video-oculography and rotational chair testing; WAIS-R—Wechsler Adult Intelligence Scale-revisited; Walking HS—Walking Handicap Scale; Zung DS—Zung Depression Scale.
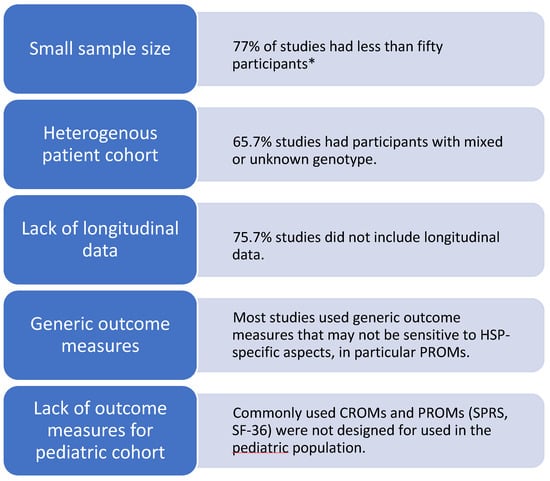
Figure 3.
Common limitations of studies of HSP outcome measures. * [66] A sample size of less than fifty participants is defined as small in the COSMIN checklist. However, a smaller sample size may be justified in the study design. For example, a randomized controlled trial of 14 patients with HSP-CYP7B1 calculated an estimate of the effect size of treatment using a pre-specified biomarker to determine the sample size required for adequate power [35].
Table 10.
Advantages and disadvantages of commonly used outcome measures for hereditary spastic paraplegia.
4.1. Recommendations for Future Research
4.1.1. Choice of Outcome Measure
This scoping review is the first comprehensive reference of outcome measures available for HSP according to outcome/construct. Based on our findings, we propose that a COS include a CROM—SPRS, PROM—SF36, and an objective biomarker—DTI, gait analysis or serum/CSF NfL.
We recommend the SPRS as it was the most commonly used CROM in HSP-related studies, has undergone psychometric testing in a cohort of individuals with HSP [67], has demonstrated cross-cultural validity [68], has been tested for responsiveness in longitudinal and interventional studies [30,33,35,62,64,69,89], and is a disease-specific outcome measure. In addition, it includes an assessment of motor function, and therefore, a performance outcome measure (PerfOM) for motor function is not required. However, we note that SPRS was not designed for use in the pediatric population, and therefore, we identify a need for a validated pediatric HSP-specific CROM.
We recommend the SF-36 as the most suitable PROM as it was commonly used in HSP-related studies, is well-validated in healthy controls and other conditions [72], has cross-cultural validity in the HSP population [73,74], and correlates with disease severity as measured with the SPRS [75,90,91] and gait analysis [34]. However, we note that the SF-36 is a generic QoL measure and may not be sensitive to smaller changes in HSP-specific symptoms, such as spasticity and bladder function, that are likely key targets for intervention in future HSP trials [92]. Therefore, we identify a need for an HSP-specific QoL scale to address the need for more sensitive tools, particularly when evaluating small changes in response to treatment in a slowly progressive condition. These findings are echoed by a recent study of CROMs and PROMs in HSP, identifying the SPRS as a suitable CROM to measure disease progression and the need for an HSP-specific PROM [89].
Diffusion tensor imaging, gait analysis, and neurofilament light chain levels are promising objective biomarkers likely to be suitable for use in clinical trials. However, further studies are needed to establish the sensitivity and specificity of these biomarkers in HSP, including longitudinal studies. Biomarkers identified through knowledge of disease pathways in specific HSP genotypes can aid in the diagnosis and measurement of treatment response. Abnormal plasma and CSF 25- and 27-OH levels are seen in individuals with HSP-CYPB1 (SPG5) and responded to treatment with statins [35,44]. More recently, two groups used different approaches to differentiate individuals with HSP-SPAST (SPG4) from healthy controls by analyzing peripheral blood mononuclear cells. Our group demonstrated reduced levels of acetylated α-tubulin seen on flow cytometry [93], while another group showed increased distance between cell and nucleus centroids on automated image analysis [94]. Both studies used surrogate markers of microtubule dysfunction based on the known role of spastin in regulating microtubule dynamics in HSP-SPAST. These findings highlight the need for further research to identify genotype-specific biomarkers that are more likely to be sensitive and specific for particular HSP genotypes. For the evaluation of existing outcome measures or the development of new outcome measures, we recommend referring to published guidelines [19] to ensure validity and reliability. Development of a COS for HSP should be informed by published recommendations, COS-STAD, to ensure that the included outcome measures meet minimum standards [95].
4.1.2. Recommendations for Trial Design
Recommendations for HSP clinical trial design will improve the quality and consistency of reporting of evidence to strengthen conclusions drawn from clinical trials. We identify a need for larger sample sizes in HSP studies, a particular challenge when studying rare conditions. International, multi-center collaborations are a potential solution to sample size challenges and have the added benefit of cross-cultural applicability of study results. It is important for outcome measures chosen to be available in different languages, relevant in different populations, and feasible for use in low-resource settings. Biomarkers that can be collected at recruitment sites and analyzed in a central facility are ideal for multi-center trials to improve the standardization of data. Although studies of single HSP genotypes are ideal for consistency within target populations, this may not be feasible when trying to attain large sample sizes. Therefore, a grouping of HSP genotypes or other neurodegenerative disorders according to similar underlying disease pathophysiology may allow for more efficient research of targeted therapeutic agents. Clinical trials for HSP may require longer periods of treatment and follow-up to demonstrate significant treatment effects, particularly in the more slowly progressive genotypes, such as HSP-SPAST. Using a combination of multiple outcome measures and biomarkers can account for phenotypic variability, even within the same genotype. It may improve the chance of detecting a treatment effect signal in heterogeneous patient cohorts.
4.1.3. Study Limitations
A limitation of this study was the use of the search terms “outcome measure” and “biomarker”, which inevitably missed relevant studies [19]. When planning our study design, we considered the volume of search results from individual searches for each outcome, e.g., spasticity, mobility, neuroimaging, etc. and deemed that approach unfeasible.
Systematic reviews on specific outcome measures have been published previously [81,86,96,97] and provide information on the utility of these outcome measures. Due to the nature of a scoping review, we were unable to perform qualitative analysis of each outcome measure to assess validity and reliability. Therefore, a systematic review specific to an outcome measure is required to answer this question. Our review identifies outcome measures that require further validation and provides an overview of the currently available literature surrounding the identified outcome measures.
5. Conclusions
In this scoping review, we present a critical assessment of currently available outcome measures for use in HSP clinical trials. We discuss the benefits and limitations of commonly used outcome measures and propose areas for further research. Given the emergence of multiple candidate HSP therapies in recent years [35,44,98], there is an urgent need for further development of a core set of validated and standardized outcome measures for use in HSP clinical trials to test the efficacy of these therapies.
Supplementary Materials
The following supporting information can be downloaded at https://www.mdpi.com/article/10.3390/genes14091756/s1; Supplementary Material S1: List of the included studies in scoping review; Supplementary Material S2: Table of HSP outcome measures and biomarkers; Supplementary Material S3: Comparison of Randomized controlled trials in HSP.
Author Contributions
Conceptualization, S.-F.S., G.W., K.R.K. and C.M.S.; methodology, S.-F.S.; results screening, S.-F.S., D.Y. and K.R.K.; data extraction, S.-F.S., D.Y., L.I.R. and F.J.; data analysis, S.-F.S., D.Y. and G.W.; writing—original draft preparation, S.-F.S.; writing—review and editing, all authors. All authors have read and agreed to the published version of the manuscript.
Funding
S.-F.S. is the recipient of the National Health and Medical Research Council and Australian and New Zealand Association of Neurologists Postgraduate Scholarships APP113610.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
All data supporting reported materials are available in the manuscript and Supplementary Materials.
Acknowledgments
The authors would like to thank Tess Aitken, Academic Liaison Librarian at the University of Sydney, for guidance in searching the databases. K.R.K. is supported by the Paul Ainsworth Family Foundation and the Medical Research Future Fund.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
All database searches performed on 9 August 2022.
- Embase search
- Embase Classic <1947 to 1973>
- Embase <1974 to 9 August 2022>
- spastic paraplegia/or spastic para*.mp. 11219
- hereditary motor sensory neuropathy/or hereditary spastic parap*.mp. 13564
- 1 or 2 21406
- pharmacological biomarker/or biomarker*.mp. or biological marker/ 660089
- patient-reported outcome/or outcome assessment/or “outcome measure*”.mp. or “quality of life”/ 1469067
- 4 or 5 2095172
- 3 and 6 1267
- remove duplicates from 7 1256
- Medline search
- Ovid MEDLINE(R) ALL <1946 to 9 August 2022>
- Spastic Paraplegia, Hereditary/or “spastic para*”.mp. 6979
- Spastic Paraplegia, Hereditary/or “hereditary spastic para*”.mp. or Paraparesis, Spastic/ 2875
- biomarker*.mp. or Biomarkers, Pharmacological/or Biomarkers/ 719216
- “outcome measure”.mp. or Outcome Assessment, Health Care/ 147938
- “patient reported outcome measure”.mp. or Patient Reported Outcome Measures/ 13303
- 1 or 2 7101
- 3 or 4 or 5 873824
- 6 and 7 199
- Scopus search
- TITLE-ABS-KEY ((“hereditary spastic parap*” OR “spastic parap*”) AND (biomarker* OR “outcome measure*”))
- 210 results
- Web of Science search
- (“hereditary spastic parap*” OR “spastic parap*”) AND (biomarker* OR “outcome measure*”)
- 230 results
- Central Cochrane Database
- EBM Reviews—Cochrane Central Register of Controlled Trials <July 2022>
- “hereditary spastic paraplegia”.mp. or Spastic Paraplegia, Hereditary/ 35
References
- Ruano, L.; Melo, C.; Silva, M.C.; Coutinho, P. The Global Epidemiology of Hereditary Ataxia and Spastic Paraplegia: A Systematic Review of Prevalence Studies. Neuroepidemiology 2014, 42, 174–183. [Google Scholar] [CrossRef]
- Erichsen, A.K.; Koht, J.; Stray-Pedersen, A.; Abdelnoor, M.; Tallaksen, C.M.E. Prevalence of hereditary ataxia and spastic paraplegia in southeast Norway: A population-based study. Brain 2009, 132, 1577–1588. [Google Scholar] [CrossRef] [PubMed]
- Coutinho, P.; Ruano, L.; Loureiro, J.L.; Cruz, V.T.; Barros, J.; Tuna, A.; Barbot, C.; Guimarães, J.; Alonso, I.; Silveira, I.; et al. Hereditary ataxia and spastic paraplegia in Portugal: A population-based prevalence study. JAMA Neurol. 2013, 70, 746–755. [Google Scholar] [CrossRef]
- Vander Stichele, G.; Durr, A.; Yoon, G.; Schüle, R.; Blackstone, C.; Esposito, G.; Buffel, C.; Oliveira, I.; Freitag, C.; van Rooijen, S.; et al. An integrated modelling methodology for estimating global incidence and prevalence of hereditary spastic paraplegia subtypes SPG4, SPG7, SPG11, and SPG15. BMC Neurol. 2022, 22, 115. [Google Scholar] [CrossRef]
- Kerstens, H.C.J.W.; Lith, B.J.H.v.; Nijkrake, M.J.; Swart, B.J.M.d.; Bemd, L.A.C.v.d.; Smeets, R.; Klemens, F.; Warrenburg, B.P.C.v.d.; Wees, P.J.v.d.; Geurts, A.C.H. Healthcare needs, expectations, utilization, and experienced treatment effects in patients with hereditary spastic paraplegia: A web-based survey in the Netherlands. Orphanet J. Rare Dis. 2021, 16, 1–283. [Google Scholar] [CrossRef]
- Shribman, S.; Reid, E.; Crosby, A.H.; Houlden, H.; Warner, T.T. Hereditary spastic paraplegia: From diagnosis to emerging therapeutic approaches. Lancet Neurol. 2019, 18, 1136–1146. [Google Scholar] [CrossRef] [PubMed]
- Meyyazhagan, A.; Orlacchio, A. Hereditary Spastic Paraplegia: An Update. Int. J. Mol. Sci. 2022, 23, 1697. [Google Scholar] [CrossRef]
- Saputra, L.; Kumar, K.R. Challenges and Controversies in the Genetic Diagnosis of Hereditary Spastic Paraplegia. Curr. Neurol. Neurosci. Rep. 2021, 21, 15. [Google Scholar] [CrossRef]
- Harding, A.E. Classification of the hereditary ataxias and paraplegias. Lancet 1983, 1, 1151–1155. [Google Scholar] [CrossRef]
- Méreaux, J.-L.; Banneau, G.; Papin, M.; Coarelli, G.; Valter, R.; Raymond, L.; Kol, B.; Ariste, O.; Parodi, L.; Tissier, L.; et al. Clinical and genetic spectra of 1550 index patients with hereditary spastic paraplegia. Brain 2022, 145, 1029–1037. [Google Scholar] [CrossRef]
- Wali, G.; Sutharsan, R.; Fan, Y.; Stewart, R.; Tello Velasquez, J.; Sue, C.M.; Crane, D.I.; Mackay-Sim, A. Mechanism of impaired microtubule-dependent peroxisome trafficking and oxidative stress in SPAST-mutated cells from patients with Hereditary Spastic Paraplegia. Sci. Rep. 2016, 6, 27004. [Google Scholar] [CrossRef]
- Denton, K.R.; Lei, L.; Grenier, J.; Rodionov, V.; Blackstone, C.; Li, X.J. Loss of Spastin Function Results in Disease-Specific Axonal Defects in Human Pluripotent Stem Cell-Based Models of Hereditary Spastic Paraplegia. Stem Cells 2014, 32, 414–423. [Google Scholar] [CrossRef]
- Fassier, C.; Tarrade, A.; Peris, L.; Courageot, S.; Mailly, P.; Dalard, C.; Delga, S.; Roblot, N.; Lefèvre, J.; Job, D.; et al. Microtubule-targeting drugs rescue axonal swellings in cortical neurons from spastin knockout mice. Dis. Model. Mech. 2013, 6, 72–83. [Google Scholar] [CrossRef]
- Wali, G.; Liyanage, E.; Blair, N.F.; Sutharsan, R.; Park, J.S.; Mackay-Sim, A.; Sue, C.M. Oxidative Stress-Induced Axon Fragmentation Is a Consequence of Reduced Axonal Transport in Hereditary Spastic Paraplegia SPAST Patient Neurons. Front. Neurosci. 2020, 14, 401. [Google Scholar] [CrossRef]
- Fan, Y.; Wali, G.; Sutharsan, R.; Bellette, B.; Crane, D.I.; Sue, C.M.; Mackay-Sim, A. Low dose tubulin-binding drugs rescue peroxisome trafficking deficit in patient-derived stem cells in Hereditary Spastic Paraplegia. Biol. Open 2014, 3, 494–502. [Google Scholar] [CrossRef]
- Halley, M.C.; Smith, H.S.; Ashley, E.A.; Goldenberg, A.J.; Tabor, H.K. A call for an integrated approach to improve efficiency, equity and sustainability in rare disease research in the United States. Nat. Genet. 2022, 54, 219–222. [Google Scholar] [CrossRef] [PubMed]
- Bellofatto, M.; De Michele, G.; Iovino, A.; Filla, A.; Santorelli, F.M. Management of Hereditary Spastic Paraplegia: A Systematic Review of the Literature. Front. Neurol. 2019, 10, 3. [Google Scholar] [CrossRef]
- Chan, A.-W.; Tetzlaff, J.M.; Gøtzsche, P.C.; Altman, D.G.; Mann, H.; Berlin, J.A.; Dickersin, K.; Hróbjartsson, A.; Schulz, K.F.; Parulekar, W.R.; et al. SPIRIT 2013 explanation and elaboration: Guidance for protocols of clinical trials. BMJ 2013, 346, e7586. [Google Scholar] [CrossRef]
- Prinsen, C.A.C.; Vohra, S.; Rose, M.R.; Boers, M.; Tugwell, P.; Clarke, M.; Williamson, P.R.; Terwee, C.B. How to select outcome measurement instruments for outcomes included in a "Core Outcome Set"—A practical guideline. Curr. Control. Trials Cardiovasc. Med. 2016, 17, 449. [Google Scholar] [CrossRef]
- Trummer, B.; Haubenberger, D.; Blackstone, C. Clinical Trial Designs and Measures in Hereditary Spastic Paraplegias. Front. Neurol. 2018, 9, 1017. [Google Scholar] [CrossRef]
- Williamson, P.R.; Altman, D.G.; Blazeby, J.M.; Clarke, M.; Devane, D.; Gargon, E.; Tugwell, P. Developing core outcome sets for clinical trials: Issues to consider. Curr. Control. Trials Cardiovasc. Med. 2012, 13, 132. [Google Scholar] [CrossRef] [PubMed]
- Peters, M.D.J.; Godfrey, C.M.; Khalil, H.; McInerney, P.; Parker, D.; Soares, C.B. Guidance for conducting systematic scoping reviews. Int. J. Evid. Based Healthc. 2015, 13, 141–146. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H. Updated methodological guidance for the conduct of scoping reviews. JBI Evid. Synth. 2020, 18, 2119–2126. [Google Scholar] [CrossRef] [PubMed]
- Veritas Health Innovation, Melbourne Australia. Covidence Systematic Review Software. Available online: www.covidence.org. (accessed on 12 July 2023).
- U.S. Food and Drug Administration. Clinical Outcome Assessment (COA): Frequently Asked Questions. Available online: https://www.fda.gov/about-fda/clinical-outcome-assessment-coa-frequently-asked-questions#COADefinition (accessed on 2 June 2023).
- Group OCfE-BMLoEW. The Oxford 2011 Levels of Evidence. Available online: http://www.cebm.net/index.aspx?o=56532011 (accessed on 12 July 2023).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Lassmann, C.; Ilg, W.; Schneider, M.; Volker, M.; Haeufle, D.F.B.; Schule, R.; Giese, M.; Schols, L.; Rattay, T.W. Specific gait changes in prodromal hereditary spastic paraplegia type 4—preSPG4 study. Medrxiv 2022, 21. [Google Scholar] [CrossRef]
- Rattay, T.W.; Volker, M.; Rautenberg, M.; Kessler, C.; Wurster, I.; Winter, N.; Haack, T.B.; Lindig, T.; Hengel, H.; Synofzik, M.; et al. The prodromal phase of hereditary spastic paraplegia type 4: The preSPG4 cohort study. Brain 2023, 146, 1093–1102. [Google Scholar] [CrossRef] [PubMed]
- Cubillos-Arcila, D.M.; Machado, G.D.; Sehnem, L.; Burguez, D.; Zanardi, A.P.J.; Martins, V.F.; Peyre-Tartaruga, L.A.; Saute, J.A.M. Progression of Functional Gait in Hereditary Spastic Paraplegias. Cerebellum 2022, 21, 350–357. [Google Scholar] [CrossRef] [PubMed]
- Faber, I.; Martinez, A.R.M.; de Rezende, T.J.R.; Martins, C.R.; Martins, M.P.; Lourenço, C.M.; Marques, W.; Montecchiani, C.; Orlacchio, A.; Pedroso, J.L.; et al. SPG11 mutations cause widespread white matter and basal ganglia abnormalities, but restricted cortical damage. NeuroImage Clin. 2018, 19, 848–857. [Google Scholar] [CrossRef]
- Kessler, C.; Serna-Higuita, L.M.; Wilke, C.; Rattay, T.W.; Hengel, H.; Reichbauer, J.; Stransky, E.; Leyva-Gutierrez, A.; Mengel, D.; Synofzik, M.; et al. Characteristics of serum neurofilament light chain as a biomarker in hereditary spastic paraplegia type 4. Ann. Clin. Transl. Neurol. 2022, 9, 326–338. [Google Scholar] [CrossRef]
- Musacchio, T.; Nohl, K.; Boelmans, K.; Maltese, V.; Zeller, D.; Isaias, I.; Volkmann, J.; Klebe, S. Biological course and natural history of hereditary spastic paraplegia type 11 (SPG11). Mov. Disord. 2018, 33 (Suppl. 2), S225. [Google Scholar]
- Regensburger, M.; Spatz, I.T.; Ollenschlager, M.; Martindale, C.F.; Lindeburg, P.; Kohl, Z.; Eskofier, B.; Klucken, J.; Schule, R.; Klebe, S.; et al. Inertial Gait Sensors to Measure Mobility and Functioning in Hereditary Spastic Paraplegia: A Cross-Sectional Multicenter Clinical Study. Neurology 2022, 99, e1079–e1089. [Google Scholar] [CrossRef] [PubMed]
- Schols, L.; Rattay, T.W.; Martus, P.; Meisner, C.; Baets, J.; Fischer, I.; Jagle, C.; Fraidakis, M.J.; Martinuzzi, A.; Saute, J.A.; et al. Hereditary spastic paraplegia type 5: Natural history, biomarkers and a randomized controlled trial. Brain 2017, 140, 3112–3127. [Google Scholar] [CrossRef] [PubMed]
- Paparella, G.; Vavla, M.; Bernardi, L.; Girardi, G.; Stefan, C.; Martinuzzi, A. Efficacy of a Combined Treatment of Botulinum Toxin and Intensive Physiotherapy in Hereditary Spastic Paraplegia. Front. Neurosci. 2020, 14, 111. [Google Scholar] [CrossRef] [PubMed]
- Scheuer, K.H.; Svenstrup, K.; Jennum, P.; Rogvi-Hansen, B.; Werdelin, L.; Fenger, K.; Nielsen, J.E. Double-blind crossover trial of gabapentin in SPG4-linked hereditary spastic paraplegia. Eur. J. Neurol. 2007, 14, 663–666. [Google Scholar] [CrossRef]
- Du Montcel, S.T.; Charles, P.; Ribai, P.; Goizet, C.; Le Bayon, A.; Labauge, P.; Guyant-Marechal, L.; Forlani, S.; Jauffret, C.; Vandenberghe, N.; et al. Composite cerebellar functional severity score: Validation of a quantitative score of cerebellar impairment. Brain 2008, 131, 1352–1361. [Google Scholar] [CrossRef]
- Du Montcel, S.T.; Charles, P.; Goizet, C.; Marelli, C.; Ribai, P.; Vincitorio, C.; Anheim, M.; Guyant-Marechal, L.; Le Bayon, A.; Vandenberghe, N.; et al. Factors influencing disease progression in autosomal dominant cerebellar ataxia and spastic paraplegia. Arch. Neurol. 2012, 69, 500–508. [Google Scholar] [CrossRef]
- Simonini, C.; Zucchi, E.; Bedin, R.; Martinelli, I.; Gianferrari, G.; Fini, N.; Sorau, G.; Liguori, R.; Vacchiano, V.; Mandrioli, J. CSF Heavy Neurofilament May Discriminate and Predict Motor Neuron Diseases with Upper Motor Neuron Involvement. Biomedicines 2021, 9, 1623. [Google Scholar] [CrossRef]
- Zucchi, E.; Bedin, R.; Fasano, A.; Fini, N.; Gessani, A.; Vinceti, M.; Mandrioli, J. Cerebrospinal Fluid Neurofilaments May Discriminate Upper Motor Neuron Syndromes: A Pilot Study. Neurodegener. Dis. 2018, 18, 255–261. [Google Scholar] [CrossRef]
- Wilke, C.; Rattay, T.W.; Hengel, H.; Zimmermann, M.; Brockmann, K.; Schols, L.; Jens, K.A.; Schule, R.; Synofzik, M. Serum neurofilament light chain is increased in hereditary spastic paraplegias. Ann. Clin. Transl. Neurol. 2018, 5, 876–882. [Google Scholar] [CrossRef]
- Lin, Q.; Liu, Y.; Ye, Z.; Hu, J.; Cai, W.; Weng, Q.; Chen, W.J.; Wang, N.; Cao, D.; Lin, Y.; et al. Potential markers for sample size estimations in hereditary spastic paraplegia type 5. Orphanet J. Rare Dis. 2021, 16, 1–9. [Google Scholar] [CrossRef]
- Marelli, C.; Lamari, F.; Rainteau, D.; Lafourcade, A.; Banneau, G.; Humbert, L.; Monin, M.L.; Petit, E.; Debs, R.; Castelnovo, G.; et al. Plasma oxysterols: Biomarkers for diagnosis and treatment in spastic paraplegia type 5. Brain 2018, 141, 72–84. [Google Scholar] [CrossRef] [PubMed]
- Prestsaeter, S.; Koht, J.; Lamari, F.; Tallaksen, C.M.E.; Hoven, S.T.J.; Vigeland, M.D.; Selmer, K.K.; Rydning, S.L. Elevated hydroxycholesterols in Norwegian patients with hereditary spastic paraplegia SPG5. J. Neurol. Sci. 2020, 419, 117211. [Google Scholar] [CrossRef] [PubMed]
- Sarret, C.; Lemaire, J.J.; Tonduti, D.; Sontheimer, A.; Coste, J.; Pereira, B.; Feschet, F.; Roche, B.; Boespflug-Tanguy, O. Time-course of myelination and atrophy on cerebral imaging in 35 patients with PLP1-related disorders. Dev. Med. Child Neurol. 2016, 58, 706–713. [Google Scholar] [CrossRef] [PubMed]
- Bonnefoy-Mazure, A.; Turcot, K.; Kaelin, A.; De Coulon, G.; Armand, S. Full body gait analysis may improve diagnostic discrimination between hereditary spastic paraplegia and spastic diplegia: A preliminary study. Res. Dev. Disabil. 2013, 34, 495–504. [Google Scholar] [CrossRef]
- Adair, B.; Rodda, J.; McGinley, J.L.; Graham, H.K.; Morris, M.E. Kinematic gait deficits at the trunk and pelvis: Characteristic features in children with hereditary spastic paraplegia. Dev. Med. Child Neurol. 2016, 58, 829–835. [Google Scholar] [CrossRef]
- Zhang, Y.; Roxburgh, R.; Huang, L.; Parsons, J.; Davies, T.C. The effect of hydrotherapy treatment on gait characteristics of hereditary spastic paraparesis patients. Gait Posture 2014, 39, 1074–1079. [Google Scholar] [CrossRef]
- Lith, B.J.H.v.; Boer, J.J.d.; Warrenburg, B.P.C.v.d.; Weerdesteyn, V.G.M.; Geurts, A.C.H. Functional effects of botulinum toxin type a in the hip adductors and subsequent stretching in patients with hereditary spastic paraplegia. J. Rehabil. Med. 2019, 51, 434–441. [Google Scholar] [CrossRef]
- Pointon, R.; Whelan, H.; Raza, R.; Peacock, S.; Wilsmore, C.; Mulkeen, A.; Goodden, J.; Lodh, R. The use of intrathecal baclofen for management of spasticity in hereditary spastic paraparesis: A case series. Eur. J. Paediatr. Neurol. 2022, 36, 14–18. [Google Scholar] [CrossRef]
- Henderson, G.; De Gheldere, A.; Gilman, J.; Hewart, P.; Clements, P.; Bliss, W.; Henman, P. A service evaluation of gait correction surgery for patients with hereditary spastic paraplegia. Gait Posture 2019, 73 (Suppl. 1), 251–252. [Google Scholar] [CrossRef]
- Milenkovic, I.; Klotz, S.; Zulehner, G.; Sycha, T.; Wiest, G. Slowed vertical saccades as a hallmark of hereditary spastic paraplegia type 7. Ann. Clin. Transl. Neurol. 2019, 6, 2127–2132. [Google Scholar] [CrossRef]
- Olchik, M.; Scudeiro, L.; Dos Santos, V.; Ayres, A.; Rech, R.; Burguez, D.; Machado, G.; Gonzalez-Salazar, C.; Padovani, M.; Franca, M.; et al. Speech biomarkers in hereditary spastic paraplegia. Mov. Disord. 2021, 36 (Suppl. 1), S490. [Google Scholar] [CrossRef]
- Marelli, C.; Badiou, S.; Genestet, S.; Larrieu, L.; Damier, P.; Camu, W.; Planes, M.; Koenig, M.; Guissart, C. Autosomal dominant SPG9: Intrafamilial variability and onset during pregnancy. Neurol. Sci. 2020, 41, 1931–1933. [Google Scholar] [CrossRef] [PubMed]
- Coutelier, M.; Goizet, C.; Durr, A.; Habarou, F.; Morais, S.; Dionne-Laporte, A.; Tao, F.; Konop, J.; Stoll, M.; Charles, P.; et al. Alteration of ornithine metabolism leads to dominant and recessive hereditary spastic paraplegia. Brain 2015, 138, 2191–2205. [Google Scholar] [CrossRef]
- Vaz, F.M.; McDermott, J.H.; Alders, M.; Wortmann, S.B.; Kolker, S.; Pras-Raves, M.L.; Vervaart, M.A.T.; van Lenthe, H.; Luyf, A.C.M.; Elfrink, H.L.; et al. Mutations in PCYT2 disrupt etherlipid biosynthesis and cause a complex hereditary spastic paraplegia. Brain 2019, 142, 3382–3397. [Google Scholar] [CrossRef] [PubMed]
- Kloth, K.; Cozma, C.; Bester, M.; Gerloff, C.; Biskup, S.; Zittel, S. Dystonia as initial presentation of compound heterozygous GBA2 mutations: Expanding the phenotypic spectrum of SPG46. Eur. J. Med. Genet. 2020, 63, 5. [Google Scholar] [CrossRef]
- Ebrahimi-Fakhari, D.; Alecu, J.E.; Brechmann, B.; Ziegler, M.; Eberhardt, K.; Jumo, H.; D’Amore, A.; Habibzadeh, P.; Faghihi, M.A.; De Bleecker, J.L.; et al. High-throughput imaging of ATG9A distribution as a diagnostic functional assay for adaptor protein complex 4-associated hereditary spastic paraplegia. Brain Commun. 2021, 3, fcab221. [Google Scholar] [CrossRef]
- De la Casa-Fages, B.; Fernandez-Eulate, G.; Gamez, J.; Barahona-Hernando, R.; Moris, G.; Garcia-Barcina, M.; Infante, J.; Zulaica, M.; Fernandez-Pelayo, U.; Munoz-Oreja, M.; et al. Parkinsonism and spastic paraplegia type 7: Expanding the spectrum of mitochondrial Parkinsonism. Mov. Disord. 2019, 34, 1547–1561. [Google Scholar] [CrossRef]
- Rattay, T.W.; Lindig, T.; Baets, J.; Smets, K.; Deconinck, T.; Sohn, A.S.; Hortnagel, K.; Eckstein, K.N.; Wiethoff, S.; Reichbauer, J.; et al. FAHN/SPG35: A narrow phenotypic spectrum across disease classifications. Brain 2019, 142, 1561–1572. [Google Scholar] [CrossRef]
- Ardolino, G.; Bocci, T.; Nigro, M.; Vergari, M.; Di Fonzo, A.; Bonato, S.; Cogiamanian, F.; Cortese, F.; Cova, I.; Barbieri, S.; et al. Spinal direct current stimulation (tsDCS) in hereditary spastic paraplegias (HSP): A sham-controlled crossover study. J. Spinal Cord. Med. 2021, 44, 46–53. [Google Scholar] [CrossRef]
- Bastani, P.B.; Kordjazi, M.; Oveisgharan, S.; Abdi, S. A Randomized Controlled Trial of the Effect of Repetitive Transcranial Magnetic Stimulation of the Motor Cortex on Lower Extremity Spasticity in Hereditary Spastic Paraplegia. J. Clin. Neurophysiol. Off. Publ. Am. Electroencephalogr. Soc. 2021, 40, 173–179. [Google Scholar] [CrossRef]
- de Lima, F.D.; Faber, I.; Servelhere, K.R.; Bittar, M.F.R.; Martinez, A.R.M.; Piovesana, L.G.; Martins, M.P.; Martins, C.R.; Benaglia, T.; Carvalho, B.D.; et al. Randomized Trial of Botulinum Toxin Type A in Hereditary Spastic Paraplegia—The SPASTOX Trial. Mov. Disord. 2021, 36, 1654–1663. [Google Scholar] [CrossRef]
- Mitchell, J.W.; Noble, A.; Baker, G.; Batchelor, R.; Brigo, F.; Christensen, J.; French, J.; Gil-Nagel, A.; Guekht, A.; Jette, N.; et al. Protocol for the development of an international Core Outcome Set for treatment trials in adults with epilepsy: The EPilepsy outcome Set for Effectiveness Trials Project (EPSET). Trials 2022, 23, 943. [Google Scholar] [CrossRef] [PubMed]
- Mokkink, L.B.; de Vet, H.C.W.; Prinsen, C.A.C.; Patrick, D.L.; Alonso, J.; Bouter, L.M.; Terwee, C.B. COSMIN Risk of Bias checklist for systematic reviews of Patient-Reported Outcome Measures. Qual. Life Res. 2018, 27, 1171–1179. [Google Scholar] [CrossRef] [PubMed]
- SchÜLe, R.; Holland-Letz, T.; Klimpe, S.; Kassubek, J.; Klopstock, T.; Mall, V.; Otto, S.; Winner, B.; Schols, L. The Spastic Paraplegia Rating Scale (SPRS): A reliable and valid measure of disease severity. Neurology 2006, 67, 430–434. [Google Scholar] [CrossRef]
- Servelhere, K.R.; Faber, I.; Coan, A.C.; França, J.M. Translation and validation into Brazilian Portuguese of the Spastic Paraplegia Rating Scale (SPRS). Arq. De Neuro-Psiquiatr. 2016, 74, 489–494. [Google Scholar] [CrossRef][Green Version]
- Montanaro, D.; Vavla, M.; Frijia, F.; Aghakhanyan, G.; Baratto, A.; Coi, A.; Stefan, C. Multimodal MRI Longitudinal Assessment of White and Gray Matter in Different SPG Types of Hereditary Spastic Paraparesis. Front. Neurosci. 2020, 14, 325. [Google Scholar] [CrossRef]
- Meseguer-Henarejos, A.B.; Sánchez-Meca, J.; López-Pina, J.A.; Carles-Hernández, R. Inter- and intra-rater reliability of the Modified Ashworth Scale: A systematic review and meta-analysis. Eur. J. Phys. Rehabil. Med. 2018, 54, 576–590. [Google Scholar] [CrossRef]
- ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [CrossRef]
- Stewart, A.; Sherbourne, C.D.; Ware, J.E.; Hays, R.D.; Wells, K.B.; Berry, S.H.; Kamberg, C.; Nelson, E.C.; Davies, A.R.; Rogers, W.H.; et al. Measuring Functioning and Well Being: The Medical Outcomes Study Approach; Duke University Press: Durham, UK; London, UK, 1992. [Google Scholar]
- Lins, L.; Carvalho, F.M. SF-36 total score as a single measure of health-related quality of life: Scoping review. SAGE Open Med. 2016, 4, 2050312116671725. [Google Scholar] [CrossRef]
- Braschinsky, M.; Rannikmae, K.; Krikmann, U.; Luus, S.M.; Raidvee, A.; Gross-Paju, K.; Haldre, S. Health-related quality of life in patients with hereditary spastic paraplegia in Estonia. Spinal Cord. 2011, 49, 175–181. [Google Scholar] [CrossRef]
- Gassner, H.; List, J.; Martindale, C.F.; Regensburger, M.; Klucken, J.; Winkler, J.; Kohl, Z. Functional gait measures correlate to fear of falling, and quality of life in patients with Hereditary Spastic Paraplegia: A cross-sectional study. Clin. Neurol. Neurosurg. 2021, 209, 106888. [Google Scholar] [CrossRef] [PubMed]
- Rabin, R.; de Charro, F. EQ-5D: A measure of health status from the EuroQol Group. Ann. Med. 2001, 33, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Kessler, C.; Serna-Higuita, L.M.; Rattay, T.W.; Maetzler, W.; Wurster, I.; Hayer, S.; Wilke, C.; Hengel, H.; Reichbauer, J.; Armbruster, M.; et al. Neurofilament light chain is a cerebrospinal fluid biomarker in hereditary spastic paraplegia. Ann. Clin. Transl. Neurol. 2021, 8, 1122–1131. [Google Scholar] [CrossRef]
- Alecu, J.E.; Saffari, A.; Ziegler, M.; Jordan, C.; Tam, A.; Kim, S.; Leung, E.; Szczaluba, K.; Mierzewska, H.; King, S.D.; et al. Plasma Neurofilament Light Chain Is Elevated in Adaptor Protein Complex 4-Related Hereditary Spastic Paraplegia. Mov. Disord. 2023. online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Gaiottino, J.; Norgren, N.; Dobson, R.; Topping, J.; Nissim, A.; Malaspina, A.; Bestwick, J.P.; Monsch, A.U.; Regeniter, A.; Lindberg, R.L.; et al. Increased neurofilament light chain blood levels in neurodegenerative neurological diseases. PLoS ONE 2013, 8, e75091. [Google Scholar] [CrossRef]
- Navas-Sanchez, F.J.; Fernandez-Pena, A.; de Blas, D.M.; Aleman-Gomez, Y.; Marcos-Vidal, L.; Guzman-de-Villoria, J.A.; Fernandez-Garcia, P.; Romero, J.; Catalina, I.; Lillo, L.; et al. Thalamic atrophy in patients with pure hereditary spastic paraplegia type 4. J. Neurol. 2021, 268, 2429–2440. [Google Scholar] [CrossRef]
- Mishra, V.; Guo, X.; Delgado, M.R.; Huang, H. Toward tract-specific fractional anisotropy (TSFA) at crossing-fiber regions with clinical diffusion MRI. Magn. Reson. Med. 2015, 74, 1768–1779. [Google Scholar] [CrossRef]
- Rezende, T.J.R.; de Albuquerque, M.; Lamas, G.M.; Martinez, A.R.M.; Campos, B.M.; Casseb, R.F.; Silva, C.B.; Branco, L.M.T.; D’Abreu, A.; Lopes-Cendes, I.; et al. Multimodal MRI-based study in patients with SPG4 mutations. PLoS ONE 2015, 10, e0117666. [Google Scholar] [CrossRef]
- Martinuzzi, A.; Montanaro, D.; Vavla, M.; Paparella, G.; Bonanni, P.; Musumeci, O.; Brighina, E.; Hlavata, H.; Rossi, G.; Aghakhanyan, G.; et al. Clinical and Paraclinical Indicators of Motor System Impairment in Hereditary Spastic Paraplegia: A Pilot Study. PLoS ONE 2016, 11, e0153283. [Google Scholar] [CrossRef]
- Groppa, S.; Oliviero, A.; Eisen, A.; Quartarone, A.; Cohen, L.G.; Mall, V.; Kaelin-Lang, A.; Mima, T.; Rossi, S.; Thickbroom, G.W.; et al. A practical guide to diagnostic transcranial magnetic stimulation: Report of an IFCN committee. Clin. Neurophysiol. 2012, 123, 858–882. [Google Scholar] [CrossRef]
- Siow, S.-F.; Smail, R.C.; Ng, K.; Kumar, K.R.; Sue, C.M. Motor Evoked Potentials in Hereditary Spastic Paraplegia—A Systematic Review. Front. Neurol. 2019, 10, 967. [Google Scholar] [CrossRef]
- Loris, E.; Ollenschläger, M.; Greinwalder, T.; Eskofier, B.; Winkler, J.; Gaßner, H.; Regensburger, M. Mobile digital gait analysis objectively measures progression in hereditary spastic paraplegia. Ann. Clin. Transl. Neurol. 2023, 10, 447–452. [Google Scholar] [CrossRef]
- Vavla, M.; Paparella, G.; Papayannis, A.; Pascuzzo, R.; Girardi, G.; Pellegrini, F.; Capello, G.; Prosdocimo, G.; Martinuzzi, A. Optical Coherence Tomography in a Cohort of Genetically Defined Hereditary Spastic Paraplegia: A Brief Research Report. Front. Neurol. 2019, 10, 1193. [Google Scholar] [CrossRef] [PubMed]
- Amprosi, M.; Indelicato, E.; Eigentler, A.; Fritz, J.; Nachbauer, W.; Boesch, S. Toward the Definition of Patient-Reported Outcome Measurements in Hereditary Spastic Paraplegia. Neurol. Genet. 2023, 9, e200052. [Google Scholar] [CrossRef] [PubMed]
- Klimpe, S.; Schule, R.; Kassubek, J.; Otto, S.; Kohl, Z.; Klebe, S.; Klopstock, T.; Ratzka, S.; Karle, K.; Schols, L. Disease severity affects quality of life of hereditary spastic paraplegia patients. Eur. J. Neurol. 2012, 19, 168–171. [Google Scholar] [CrossRef] [PubMed]
- Orsucci, D.; Petrucci, L.; Caldarazzo Ienco, E.; Chico, L.; Simi, P.; Fogli, A.; Baldinotti, F.; Simoncini, C.; Logerfo, A.; Carlesi, C.; et al. Hereditary spastic paraparesis in adults. A clinical and genetic perspective from Tuscany. Clin. Neurol. Neurosurg. 2014, 120, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Patrick, D.L.; Deyo, R.A. Generic and Disease-Specific Measures in Assessing Health Status and Quality of Life. Med. Care 1989, 27, S217–S232. [Google Scholar] [CrossRef]
- Wali, G.; Siow, S.F.; Liyanage, E.; Kumar, K.R.; Mackay-Sim, A.; Sue, C.M. Reduced acetylated α-tubulin in SPAST hereditary spastic paraplegia patient PBMCs. Front Neurosci. 2023, 17, 1073516. [Google Scholar] [CrossRef]
- Sardina, F.; Valente, D.; Fattorini, G.; Cioffi, E.; Zanna, G.D.; Tessa, A.; Trisciuoglio, D.; Soddu, S.; Santorelli, F.M.; Casali, C.; et al. New cellular imaging-based method to distinguish the SPG4 subtype of hereditary spastic paraplegia. Eur. J. Neurol. 2023, 30, 1734–1744. [Google Scholar] [CrossRef]
- Kirkham, J.J.; Davis, K.; Altman, D.G.; Blazeby, J.M.; Clarke, M.; Tunis, S.; Williamson, P.R. Core Outcome Set-STAndards for Development: The COS-STAD recommendations. PLoS Med. 2017, 14, e1002447. [Google Scholar] [CrossRef]
- da Graça, F.F.; de Rezende, T.J.R.; Vasconcellos, L.F.R.; Pedroso, J.L.; Barsottini, O.G.P.; França, J.M.C. Neuroimaging in Hereditary Spastic Paraplegias: Current Use and Future Perspectives. Front. Neurol. 2019, 9, 1117. [Google Scholar] [CrossRef]
- Vavla, M.; Montanaro, D.; Pizzighello, S.; Frijia, F.; Arrigoni, F.; Baratto, A.; Piccoli, G.; Paparella, G.; Martinuzzi, A. Brain Magnetic Spectroscopy Imaging and Hereditary Spastic Paraplegia: A Focused Systematic Review on Current Landmarks and Future Perspectives. Front. Neurol. 2020, 11, 515. [Google Scholar] [CrossRef]
- de Freitas, J.L.; Rezende Filho, F.M.; Sallum, J.M.F.; França, M.C.; Pedroso, J.L.; Barsottini, O.G.P. Ophthalmological changes in hereditary spastic paraplegia and other genetic diseases with spastic paraplegia. J. Neurol. Sci. 2020, 409, 116620. [Google Scholar] [CrossRef] [PubMed]
- Wali, G.; Berkovsky, S.; Whiten, D.R.; Mackay-Sim, A.; Sue, C.M. Single cell morphology distinguishes genotype and drug effect in Hereditary Spastic Paraplegia. Sci. Rep. 2021, 11, 16635. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).