Abstract
Background/Objectives: Co-occurring mental health conditions affect autistic individuals at high rates, impacting their well-being and quality of life. Mental health conditions are often appropriate treatment targets that can improve the lives of autistic individuals. Because of this, there is growing interest in predictors of mental health and behavioral outcomes. Given the rapidly evolving evidence base and growing literature using longitudinal cohorts, it is unclear which predictors of symptoms of anxiety and depression are consistent, and which are not. Additionally, it is difficult to deduce which predictors of mental health symptoms at a given time also predict change over time. This can be partially due to the different statistical approaches that are implemented, including trajectory vs. non-trajectory methodologies. Methods: We conducted a systematic review to evaluate how non-trajectory and trajectory analyses inform our knowledge of how symptoms of anxiety and depression change over time. Additionally, we aimed to identify important predictors of change and later anxiety and depressive symptoms in autistic individuals. Results: There is variability in symptoms of anxiety and depression in autistic individuals. Adaptive skills arose as significant predictors of change and of later symptoms of both anxiety and depression. Peer relationships in school age seem to be particularly important in predicting later symptoms of depression. Conclusions: This review provides evidence that there are different trajectories and different patterns of mental health symptoms over the lifespan, providing further evidence that autism is a developmental condition that changes over time in different ways for different people. Implications and future directions are further discussed.
1. Introduction
Autism is a neurodevelopmental condition diagnosed based on social communication difficulties and restricted and repetitive interests and behaviors that are present early in development and significantly impact functioning []. Autism often co-occurs with other neurodevelopmental (e.g., intellectual disability, attention-deficit hyperactivity disorder [ADHD]), medical, psychological, and behavioral (e.g., aggression) conditions. For instance, an estimated 26–37.9% of autistic individuals have a co-occurring intellectual disability [,]. Higher rates of co-occurring conditions affect autistic individuals compared to the general population [] and can impact the mental health and well-being of autistic individuals throughout their lives []. This study focuses specifically on symptoms of anxiety and depression due to the high rates of their co-occurrence with autism and the significance to stakeholders. Mental health and psychological well-being have been defined in many ways in the literature. One conceptualization encompasses psychological/cognitive, emotional, and behavioral well-being.
1.1. Mental Health Disorders in Autism
Symptoms of depression and anxiety are particularly common in autistic individuals. However, identifying mental health disorders such as depression and anxiety in autistic individuals can be challenging. Many of the symptoms of autism and these psychological conditions overlap (also known as symptom over-shadowing) and can be difficult to disentangle from one another []. For example, challenges in social communication are common in both anxiety and autism []. Additionally, only a limited number of anxiety and depression measures have been validated for autistic people [,,]. Consequently, estimates of mental health issues in autistic individuals vary based on diagnostic procedures, measures, and sampling differences []. While estimates of co-occurring mental health rates vary across the literature, the rates of mental health challenges that affect autistic people are still consistently higher compared to rates in neurotypical individuals []. Estimates from two studies suggested that current anxiety prevalence estimates are 7.8% in autistic children, 21.5% in autistic adolescents, and 27% in autistic adults [,]. When considering the prevalence rates of anxiety in autistic adults who have a co-occurring intellectual disability (ID), the pooled estimates are lower (20%) []. Depression prevalence rates in autism from the same studies are 1% in autistic children, 12.7% in autistic adolescents, 23% in autistic adults without ID, and 16% in autistic adults with ID [,].
Cross-sectional designs are useful and cost-efficient tools to help researchers identify prevalence rates of co-occurring psychiatric conditions and their concurrent associations with predictors. Longitudinal designs are necessary to understand the trajectories of mental health symptoms over the lifespan, however, and to identify critical early predictors of later outcomes. Mental health outcomes are particularly important because they are associated with the overall well-being of autistic adults [,,,]. Using a large and diverse community sample (n = 194) McCauley and colleagues [] found that having high and stable anxiety levels over time predicted worse objectively defined adult outcomes that were developed using a framework from the World Health Organization (having at least one friend, living independently, having a job) for adults with IQ scores greater than 70. A similar association was seen between higher levels of depression and worse adult outcomes []. A separate study using a smaller clinical sample (n = 58) found a positive correlation between individuals’ mental health and poor social outcomes in adulthood []. These studies suggest that mental health is a significant predictor of traditional objective adult outcomes above and beyond autism symptoms. It is important to understand the mechanisms that contribute to these mental health outcomes of autistic people over their lifespan.
1.2. Longitudinal Cohort Studies
Long-term longitudinal studies in autism are particularly helpful because they are less likely to be influenced by trends and changes in diagnostic criteria over time. For example, prevalence rates of autism have changed dramatically over the last 40 years, a phenomenon most often attributed to better awareness, but also to broader interpretations of autism definitions []. Thus, cross-sectional comparisons of recently diagnosed young children with later diagnosed or early diagnosed adolescents or adults may be difficult to interpret. Though participants in longitudinal studies starting in early childhood likely represent a different population of individuals than current cross-sectional studies (with children diagnosed at younger ages likely to have substantial developmental delays), at the least the participants are compared to themselves as they grow older.
Moreover, different statistical methods can be implemented in longitudinal studies to understand data and trends over time in the symptoms measured. Trajectory methods can be particularly useful in elucidating change over time, since they are focused on patterns of change across multiple developmental periods. Additionally, trajectory methods assume the population is heterogeneous and subgroups follow different developmental trajectories. In contrast, non-trajectory methods assume the population is homogeneous, and unlike trajectory models, do not elicit different patterns of change. Non-trajectory methods used in longitudinal studies can provide information about the causal relationship between the average of an earlier construct and the average of a later outcome for the entire sample.
Trajectory methods help us understand how symptoms of anxiety and depression evolve over time, identifying critical periods in autistic individuals’ lives when support is especially important. For example, a study using an ongoing longitudinal sample (n = 165) collected anxiety and depressive symptom questionnaires from autistic individuals during several timepoints, including school age, adolescence, and early adulthood []. Results showed that males had higher symptoms of anxiety and depression than females during school age (entry timepoint), but females showed greater increases in symptoms of anxiety and depression over time throughout adolescence, which resulted in no significant differences in symptoms between males and females at age 21. These results provide important clinical guidance, suggesting that males with autism may experience internalizing symptoms earlier in development, while females show sharp increases in symptoms during adolescence. It may be worth screening for anxiety and depression earlier in development in order to equip all autistic individuals, but especially females, with the tools to offset symptoms of anxiety and depression prior to adolescence.
Identifying consistent predictors of long-term mental health outcomes in autistic adults is also important for several reasons. Longitudinal studies assessing predictors can help identify early clinical targets that can influence positive mental health outcomes, and overall well-being. For instance, a study using a large community sample of autism (n = 390) found a significant and positive association between caregiver depressive symptoms at age 3 and their autistic child’s depressive symptoms at age 14 []. In the same study, peer relationships at age 10 were identified as significant mediators between early childhood irritability and depression at age 14 in autistic individuals []. These findings can help to inform targeted interventions to best support youth. For example, intervening more directly on peer relationships at age 10 could protect against later mental health challenges affecting autistic adolescents, based on these study findings. Other early predictors of later mental health outcomes in autism include sociodemographic and contextual factors (i.e., gender and caregiver education [used as a proxy for SES]), peer-relationships, parental well-being, and parent–child interaction styles [,,,]).
1.3. Aims
The increasing number of large longitudinal cohorts and growing interest in predictors of mental health and behavioral outcomes is encouraging, given their importance to stakeholders, including autistic individuals and their families []. Given the rapidly evolving evidence base, it is not clear which predictors of anxiety and depression are most important, and which are not. Additionally, it is difficult to deduce which predictors of mental health symptoms at a given time also predict change over time. This can be partially due to the different statistical approaches that are implemented, including trajectory vs. non-trajectory methodologies []. Thus, the aims of this systematic review are to: (1) evaluate how non-trajectory analyses inform our knowledge of individual and contextual predictors of later symptoms of anxiety and depression, and (2) evaluate how trajectory analyses inform our knowledge of individual and contextual predictors of change in anxiety and depression symptoms in autistic individuals within longitudinal studies.
2. Methods
2.1. Search Strategy
A systematic search was carried out by searching two large databases, PsychINFO and PubMed. The search terms were entered in three layers; the first were terms related to autism (i.e., autism, Asperger, ASD, PDD-NOS, “autism spectrum disorder”), the next were related to the longitudinal nature of the relevant articles (i.e., longitudinal, long-term, change, trajectories), and the third was related to mental health and related disorders (i.e., depression, anxiety, “maladaptive behaviors”, “mood disorders”). The exact search strings with MeSH terms and indications of the search location (i.e., abstract/title) can be found in Appendix A. The parentheses in the search indicate different groups of related terms. The only additional limit added during the search was to restrict the search to articles published between 2000 and 2023. The database search took place on February of 2023. This systematic review has been registered with INPLASY (International Platform of Registered Systematic Review and Meta-analysis Protocols) and the registration number is INPLASY2024100068.
The study screening and inclusion process took place in three stages. Articles were first screened for duplicates, then for relevance to the topic and clear violations of the inclusion criteria (i.e., autism-specific, clearly longitudinal, and human subjects) by screening the title and abstract. A final and more rigorous screen was conducted to exclude any additional studies that were missed during the initial screen. During this step, relevant data from each study was extracted to track which studies met all the inclusion criteria, and to indicate why the studies that did not meet the inclusion criteria were excluded. A hand search was then conducted by searching the reference lists of the identified papers to locate additional papers that met inclusion criteria that did not come up in the original search. The search process is shown in the PRISMA flow diagram in Figure 1.
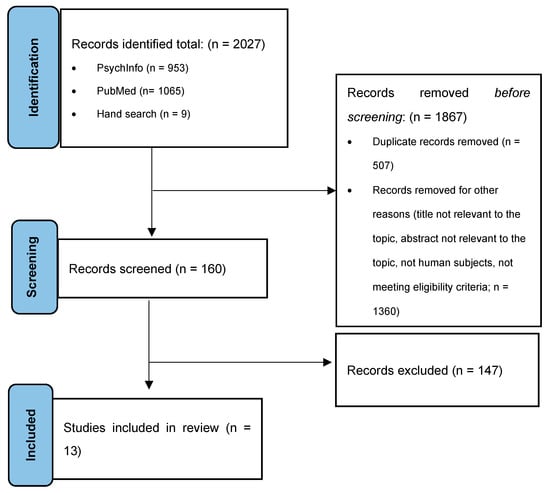
Figure 1.
Preferred reporting items for systematic reviews and meta-analysis (PRISMA) flowchart.
2.2. Inclusion Criteria
Studies that met the following inclusion criteria were included in this study:
- Equal to or longer than a three-year follow-up between the first and final timepoint;
- Prospective study;
- Sample size larger than 50 participants;
- Included participants with a confirmed professional diagnosis (use of observational measures, interviews or evidence of a medical diagnosis given by a professional) of ASD, autism, Asperger’s syndrome, or pervasive developmental disorder–not otherwise specified (PDD-NOS);
- Included measures of symptoms of anxiety or depression as the outcome;
- Included behavioral or environmental (e.g., sociodemographic and contextual) predictors.
2.3. Exclusion Criteria
Studies that met the following exclusion criteria were excluded from this study:
- Treatment study;
- Only included prenatal or genetic data as predictors;
- Publications not written in English.
Only studies that had a follow-up period of at least three years were included to ensure that we were capturing a sufficiently long interval to see developmental changes. Only studies that included more than 50 participants were included to ensure that the research was appropriately powered to find associations between predictors and the outcomes of interest, given the heterogeneity within autism []. Additionally, we excluded studies that only included prenatal data as predictors of outcomes because we were mainly interested in participant behavioral and contextual predictors.
2.4. Data Extraction
Data from each article was extracted using a series of questions created for the purposes of this study, including the following: (1) longitudinal sample name and study citation; (2) sample size; (3) mean and standard deviation of age and/or age range; (4) diagnoses were reported for the sample (in addition to autism); (5) mean length of follow-up after the initial timepoint; (6) IQ data, if available; (7) predictors included in the study; (8) construct of interest measured in the study (anxiety and/or depression); (9) outcome measures; (10) trajectory vs. non-trajectory statistical methods; and (11) result summaries.
Many of the studies that were included in the systematic review were secondary data analyses from larger longitudinal samples. As a result, information about the full sample demographics from all the longitudinal cohorts represented in the articles that met eligibility criteria were extracted from the parent studies. Information regarding the original cohort included the following: (1) name of cohort, (2) principal investigators leading the cohort, (3) sample size, (4) diagnoses included, (5) mean age and/or range at entry, (6) average age at the final timepoint, (7) length of study, (8) country of origin, (9) type of sample (e.g., community sample, population-based cohort, etc.), (10) gender ratio, (11) IQ, (12) caregiver education, and (13) participant race.
3. Results
3.1. Search Results and Study Inclusion
The initial search resulted in the identification of 2027 studies (PsychInfo = 953, PubMed = 1065, hand search = 9). After the first screen, 1867 studies were excluded (duplicates = 507, not meeting inclusion criteria based on title/abstract = 1360). Of the 160 studies that were left, 147 were excluded for the following reasons: treatment study (n = 18), not longitudinal (n = 20), prenatal study (n = 4), genetic study (n = 8), insufficient follow-up period (n = 29), no confirmed autism diagnosis (n = 29), autistic participants not the focus (n = 7), and no outcomes of interest (n = 28). Additionally, four studies were excluded because they used very general constructs of “emotional problems”, which included symptoms of depression, anxiety, OCD, and additional mental health conditions. While these papers are valuable to the autism and mental health literature, they were excluded in order to focus on symptoms of anxiety and depression as separate outcomes. A total of 13 studies met eligibility criteria and were included in the review. Of the 13 studies, three measured both anxiety and depression using the same participants. The demographic information for all included studies is shown in Table 1.

Table 1.
Demographic information of included articles.
3.2. Characteristics of Longitudinal Cohorts
Seven longitudinal cohorts were represented across the 13 studies that met eligibility criteria. All samples included participants with diagnoses of autism, and some reported on the presence of co-occurring ID and other developmental delays within the sample. Most cohorts began data collection when participants were in early childhood, with only a few beginning in late childhood, adolescence, and adulthood. A wide range of ages are represented in the seven cohorts, and follow-up times within the studies ranged from about 3 to 30 years. The cohorts were primarily based in the United States (n = 2), United Kingdom (n = 2), and Canada (n = 2) but also included samples from Australia (n = 1) and Israel (n = 1). One of the studies was based in both the United States and Canada and is represented in each country in the previous count (see Table 2). The cohorts include community samples, population-based cohorts, and clinical samples. As expected, each of the cohorts included primarily male participants (from 70 to 90%). A large percentage of caregivers had education levels of a high school diploma or more. Three of the seven cohorts did not report race and/or ethnicity demographics, but the majority of participants in the other studies identified as White. Characteristics of the longitudinal cohorts are shown in Table 2.
Table 2.
Characteristics of the longitudinal cohorts.
3.3. Characteristics of Included Studies
For the studies included in this review, sample sizes ranged from 65 to 6,091 participants, the larger samples being population-based cohort studies. The 13 studies that met eligibility criteria used data from the following cohorts: four came from the Pathways in ASD study, three from the Early Diagnosis of ASD (EDX) cohort, one from the Special Needs and Autism Project (SNAP) cohort, one from the Avon Longitudinal Study of Parents and Children (ALSPAC), two from a cohort followed by Zachor and Ben-Itzchak, one from the Autism Treatment Network (ATN) Call-Back study, and one from the Australian Child to Adult cohort. Outcomes of anxiety and depression were measured during childhood, adolescence, and adulthood. Multiple outcomes of interest were sometimes included in a single study. Follow-up times within the studies ranged from 4–23 years. Cognitive abilities varied across studies as shown by the wide ranges of IQ scores. Characteristics of the included studies are highlighted in Table 2. A summary of predictors, outcomes of interest, outcome measures, respondents, and results of all studies that met eligibility criteria are described in Table 3 and Table 4.
Table 3.
Predictors and results of included articles on anxiety.
Table 4.
Predictors and results of included articles on depression.
3.4. Anxiety
3.4.1. Results from Studies Using Trajectory Methods
Of the 13 studies, 10 included anxiety as a primary outcome. Four of the ten studies used trajectory analyses, focusing on changes in symptoms of anxiety over time in participants. Of those studies, one showed that symptoms of anxiety decreased from school age to adulthood []. Other studies showed variable trajectories with multiple trends of stability, including increases and decreases in anxiety over time within the samples [,,]. For example, one study identified a group with low symptoms of anxiety in childhood that remained low into adulthood, and a group that started with higher levels of anxiety that remained high over time [].
A number of predictors of trajectories and changes in anxiety were identified across the studies. One study showed that higher levels of executive functioning challenges in childhood were related to increasing levels of anxiety over time into early adulthood []. Similarly, a separate study found that children with better adaptive skills at age 9 were less likely to belong in the high anxiety trajectory group from late childhood to adulthood []. Other significant predictors of higher anxiety trajectories throughout childhood and from childhood to adulthood included early insistence on sameness [], caregiver mental health [], lower parental education [], and higher IQ scores [,]. Being female was associated with higher levels of later childhood anxiety in one sample [], greater increases in anxiety over time from school age to adulthood but no overall higher levels of anxiety in adulthood compared to males [], or no associations with any trajectories from childhood to adulthood [].
3.4.2. Results from Studies Using Non-Trajectory Methods
The remaining six studies used non-trajectory methods, focusing on the association between earlier factors and later symptoms of anxiety, on average, for the entire sample. Earlier psychopathology including high levels of anxiety were reliable predictors of later high levels of anxiety in autistic school age-children []. In one large community sample, higher levels of insistence on sameness and RRBs in early childhood predicted later anxiety symptoms in middle childhood [,], although in a different sample, they did not predict diagnoses of social or separation anxiety in adolescence []. Sleep difficulties in early childhood did not predict later anxiety in school-age children [].
The association between earlier adaptive functioning and anxiety symptoms found in adolescence in one study was not significant []. However, significant associations between higher adaptive functioning in childhood and lower anxiety symptoms in adulthood were found [], further supporting the findings by Gotham and colleagues [] and McCauley and colleagues []. Findings on the relationship between childhood IQ and later anxiety symptoms were mixed. One study found that higher IQ was associated with higher levels of anxiety symptoms in adolescence [], while two others found that higher IQ was associated with lower scores of anxiety symptoms in adolescence [] and adulthood []. Of caregiver predictors, earlier symptoms of caregiver mental health were associated with later symptoms of anxiety in adults with autism in one study [], but no other studies tested this association [,,,].
3.5. Depression
3.5.1. Results from Studies Using Trajectory Methods
Only six studies assessed symptoms of depression as a primary outcome. Half of these studies used non-trajectory analyses. Children with confirmed diagnoses of autism and children without official diagnoses with high autistic traits (determined using measures of social affect and RRBs) had higher depressive symptoms than the general population at age 10, and depressive symptoms continued to increase until age 18 []. Additionally, children with autism and high autistic traits who reported being bullied had the highest depressive symptom scores at age 10, which remained elevated throughout adolescence []. Autism diagnosis (compared to other developmental delays) showed consistently higher symptoms of depression over time in one study []. Similarly, higher social communication autism severity scores (CSS Social Affect score) at age 9 were associated with greater odds of being part of the high depressive symptoms class instead of the low depressive symptom class [] using the same sample.
Depressive symptoms increased with age for females, similar to anxiety symptoms, but there were no significant gender differences in symptoms of depression between males and females in adulthood [,]. The associations between IQ and depressive symptoms were unclear; higher IQ at age 5 was found to be associated with higher odds of belonging to the high depression group in adulthood in one study [], while no significant associations were found in another that used the same longitudinal cohort but slightly different sample and different longitudinal methods []. One study found that lower caregiver education predicted increasing depressive symptoms in adults, but only for those with IQ scores of less than 70 []. More severe ADHD and anxiety symptoms at age 9 were positively associated with the high depressive symptoms class compared to the low depressive symptoms class []. In one study, more severe executive functioning difficulties (EF) were associated with higher symptoms of depression during school age, but with slower-growing depressive symptoms over time in this group compared to those with less severely affected EF skills []. Similarly, worse adaptive skills at age 9 predicted an increased risk of belonging to the class that had high depressive symptoms over time from childhood to adulthood [].
3.5.2. Results from Studies Using Non-Trajectory Methods
Similar to findings from the trajectory analyses by Gotham and colleagues [] and McCauley and colleagues [], in non-trajectory analyses, higher adaptive skills predicted lower symptoms of depression in adulthood []. In a separate study by Forbes and colleagues [] using the same sample, depressive symptoms in adulthood were not related to autism severity, adaptive skills, IQ, irritability, or hyperactivity in childhood and adolescence, including teacher reports of behavioral and emotional problems at ages 14 or 17. In another sample, higher irritability and lower peer relationship scores in preschool age were associated with higher symptoms of depression in adolescence []. Finally, of the sociodemographic and contextual factors, maternal mental health and neighborhood deprivation were significant predictors of later symptoms of depression in autistic adolescents and adults. Higher maternal symptoms of depression measured when children were three were a significant predictor of higher symptoms of depression in autistic adolescents []. Furthermore, worse maternal mental health measured in childhood predicted higher symptoms of depression in adults []. One study found that greater neighborhood deprivation in childhood was related to lower depressive symptoms in adulthood, but the association was weak [].
4. Discussion
Higher rates of co-occurring psychological conditions in autistic people compared to the general population have been well-established in the literature [,]. Furthermore, these co-occurring psychological conditions are linked to individuals’ quality of life and well-being [,,]. We undertook a systematic review to evaluate the unique contributions of trajectory and non-trajectory analyses to our understanding of symptoms of anxiety and depression in autistic individuals across their lifespan and to identify unique predictors of those outcomes. These aims are critical for identifying developmental periods where increased support and targeted interventions may be beneficial.
4.1. Trajectory Analyses in Autism Research
The analytic methods used were quite variable across the included studies, even within trajectory and non-trajectory models. Some studies used growth curve modeling, group-based trajectory modeling and structural equation modeling followed by regression analyses, while other studies analyzed their data using simple correlations between entry and exit variables. There is support for the statistical equivalence of the various approaches []. However, different methods used to model data can influence the interpretation of the relationships between variables and our ability to see patterns of change in behaviors over time []. A strength of trajectory models is that they allow us to understand whether overall levels and changes in anxiety and depressive symptoms are homogeneous across time in the population of interest or whether there is variability in the development of symptoms. Based on the trajectory studies included in this review, it is clear that there are a range of different trajectories (identified as multiple groups with varying levels of anxiety and depression) that change differently over time in autistic populations. Despite this, trajectory-based analytical methods are used less often than expected in longitudinal autism research, likely due to the large sample sizes that are required to secure enough statistical power [].
4.2. Predictors of Mental Health Outcomes
One clear pattern that emerged from the included studies was that early mental health challenges are strong predictors of trajectories of later mental health challenges. Earlier symptoms of anxiety or depression are consistently associated with higher symptoms of anxiety and depression later in life. There was some inconsistency in the relationship between adaptive skills and later symptoms of anxiety in adolescence [], but overall, worse adaptive skills predict worse symptoms of anxiety and depression trajectories and outcomes in adulthood [,,]. Targeting adaptive skills early in development could be a way to support mental health outcomes in adulthood. There are few interventions specifically targeted at improving adaptive skills in children with autism; most interventions are focused on increasing adaptive skills in adulthood []. It is possible that there is a window to support both adaptive skills and symptoms of anxiety and depression in late school age or early adolescence before mental health challenges become clinically significant. Learning more about the effects of intervention on adaptive skills in childhood and the mediating effects of improving adaptive skills on later mental health outcomes is an area of research that requires further exploration.
IQ has consistently been identified as a strong predictor of many more positive adult outcomes on average []. The varying results across studies using both trajectory and non-trajectory methods suggest that the relationships between IQ and symptoms of anxiety and between IQ and symptoms of depression remain less clear. The inconsistent relationships between IQ and mental health challenges could be due to several reasons, including but not limited to differences in respondents (self vs caregiver report) and/or low rates of inclusion of individuals who are less cognitively able in longitudinal samples.
The relationship between gender and mental health symptoms needs further exploration as well. Variability in rates of anxiety and depressive symptoms across males and females in the literature could be attributed to ascertainment differences, including oversampling of males in general and oversampling of females with lower IQs in face-to-face research studies [,]. Furthermore, females identified in adulthood are clinically different on average compared to those that are identified in childhood (e.g., higher IQ and levels of anxiety) []. While it is costly and time intensive, matched samples for gender, IQ, and age are needed to systematically assess whether there are gender differences in mental health symptoms and additional clinical factors that influence these relationships (e.g., age, IQ, adaptive skills, etc.).
Autistic individuals have higher symptoms of depression over time than the general population, while insistence on sameness and RRBs (as opposed to an autism diagnosis) in childhood predicts later anxiety symptoms. Additionally, having positive peer relationships during school age seems to protect against symptoms of depression later in life in autistic adolescents [,,]. Studies should assess whether social skill interventions that target social skills in children and adolescents [] indirectly influence symptoms of depression later in life through the mediating role of social relationships. An additional predictor of depressive symptoms in autistic adolescents and adults was earlier maternal mental health. This highlights the potential bidirectional relationship between parent and child mental health outcomes and the need to support family units.
4.3. Limitations
The results presented here should be considered with a few limitations. The included studies covered a wide range of development (i.e., childhood, adolescence, and adulthood) and specific periods of development varied across studies. It may be more appropriate to compare studies within a particular age range. This is difficult to do, however, given the relatively few longitudinal studies available. Additionally, the studies used different measures for their predictors and outcomes, and varied in reporters (e.g., teacher, parent or self-report). For example, one study by Ben-Itzchak and colleagues [] used SCARED to identify symptoms of separation anxiety and social anxiety, while the majority of studies relied primarily on the anxiety subscale of the CBCL and ABCL. Moreover, there is still little evidence that different measures and different reporters of these outcomes tap into the same constructs. Future work is needed to link and validate the use of common measures of anxiety and depression for autistic people [,]. Additionally, the majority of the included literature used questionnaire data to measure changes in symptoms of anxiety and depression, as opposed to using professionally provided diagnoses.
5. Conclusions
This is the first review to synthesize data on early predictors of later symptoms of anxiety and depression in autism using longitudinal data. There are many factors, both individual and contextual, that have been assessed as predictors of mental health outcomes, both cross-sectionally and longitudinally, in this population. This review provides a new perspective on the consistency, or lack thereof, of early predictors of symptoms of anxiety and depression. Some factors reliably predict later symptoms of anxiety and depression such as childhood adaptive skills and peer relationships, and others are less consistent, like IQ. Additionally, this review provides solid evidence that there are different trajectories and different patterns of mental health symptoms over the lifespan, supporting the importance of acknowledging that autism is truly a spectrum, as well as a developmental condition that changes over time in different ways for different people. Because of the heterogeneity in autism across almost all behaviors and characteristics that we measure in clinical practice and research (e.g., age, gender, IQ, adaptive skills, etc.), large and diverse longitudinal samples are necessary to appropriately capture different profiles and patterns of development across the lifespan. Understanding these outcomes is the first step to being able to implement interventions at the right time to offset the effects on anxiety and depression outcomes.
Author Contributions
Conceptualization, M.T. and C.L.; methodology, M.T.; resources, C.L.; writing—original draft preparation, M.T.; writing—review and editing, M.T. and C.L.; supervision, C.L. All authors have read and agreed to the published version of the manuscript.
Funding
This project was supported by National Institute on Aging (R01-AG080599, CL) and the Simons Foundation (624965, CL).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Search Criteria provided in Appendix A.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix A
- Search terms
- PubMed: (((“autis*”[Title/Abstract] OR “asperger*”[Title/Abstract] OR
- “asd”[Title/Abstract] OR “PDD-NOS” [Title/Abstract] OR “autism spectrum disorder”[MeSH
- Terms])))
- AND
- (((“longitudinal”[Title/Abstract] OR “long-term”[Title/Abstract] OR
- “change”[Title/Abstract] OR “trajector*”[Title/Abstract])))
- AND
- (((“depress*”[Title/Abstract] OR “anxiety”[Title/Abstract] OR “mood disorders”[MeSH
- Terms] OR “Anxiety”[MeSH Terms] OR “Depression”[MeSH Terms] OR “maladaptive
- behaviors”[Title/Abstract])))
- Psych info: (tiab(autis*) OR tiab(asperger*) OR tiab(asd) OR tiab(PDD-NOS) OR
- MAINSUBJECT.EXACT.EXPLODE(“Autism Spectrum Disorders”))
- AND
- (tiab(longitudinal) OR tiab(long-term) OR tiab(change) OR tiab(trajector*))
- AND
- (tiab(anxiety) OR tiab(depress*) OR tiab(“maladaptive behaviors”) OR
- (MAINSUBJECT.EXACT(“Anxiety”) OR MAINSUBJECT.EXACT.EXPLODE(“Anxiety”)) OR (MAINSUBJECT.EXACT.EXPLODE(“Affective Disorders”) OR
- MAINSUBJECT.EXACT(“Affective Disorders”)) OR
- (MAINSUBJECT.EXACT.EXPLODE(“Depression (Emotion)”) OR
- MAINSUBJECT.EXACT(“Depression (Emotion)”)))
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlington, VA, USA, 2013. [Google Scholar]
- Maenner, M.J.; Warren, Z.; Williams, A.R.; Amoakohene, E.; Bakian, A.V.; Bilder, D.A.; Durkin, M.S.; Fitzgerald, R.T.; Furnier, S.M.; Hughes, M.M.; et al. Prevalence and characteristics of autism spectrum disorder among children aged 8 years—Autism and Developmental Disabilities Monitoring Network, 11 sites, United States, 2020. MMWR Surveill. Summ. 2023, 72, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Mutluer, T.; Genç, H.A.; Morey, A.; Eser, H.Y.; Ertinmaz, B.; Can, M.; Munir, K. Population-Based Psychiatric Comorbidity in Children and Adolescents with Autism Spectrum Disorder: A Meta-Analysis. Front. Psychiatry 2022, 13, 856208. [Google Scholar] [CrossRef] [PubMed]
- Croen, A.L.; Zerbo, O.; Qian, Y.; Massolo, M.L.; Rich, S.; Sidney, S.; Kripke, C. The health status of adults on the autism spectrum. Autism 2015, 19, 814–823. [Google Scholar] [CrossRef] [PubMed]
- McCauley, J.B.; Elias, R.; Lord, C. Trajectories of co-occurring psychopathology symptoms in autism from late childhood to adulthood. Dev. Psychopathol. 2020, 32, 1287–1302. [Google Scholar] [CrossRef] [PubMed]
- Hollocks, M.J.; Lerh, J.W.; Magiati, I.; Meiser-Stedman, R.; Brugha, T.S. Anxiety and depression in adults with autism spectrum disorder: A systematic review and meta-analysis. Psychol. Med. 2018, 49, 559–572. [Google Scholar] [CrossRef]
- Pickard, H.; Rijsdijk, F.; Happé, F.; Mandy, W. Are Social and Communication Difficulties a Risk Factor for the Development of Social Anxiety? J. Am. Acad. Child Adolesc. Psychiatry 2017, 56, 344–351.e3. [Google Scholar] [CrossRef]
- Moss, P.; Howlin, P.; Savage, S.; Bolton, P.; Rutter, M. Self and informant reports of mental health difficulties among adults with autism findings from a long-term follow-up study. Autism 2015, 19, 832–841. [Google Scholar] [CrossRef]
- Williams, Z.J.; Everaert, J.; Gotham, K.O. Measuring Depression in Autistic Adults: Psychometric Validation of the Beck Depression Inventory–II. Assessment 2020, 28, 858–876. [Google Scholar] [CrossRef]
- Howlin, P.; Magiati, I. Autism spectrum disorder. Curr. Opin. Psychiatry 2017, 30, 69–76. [Google Scholar] [CrossRef]
- Mason, D.; McConachie, H.; Garland, D.; Petrou, A.; Rodgers, J.; Parr, J.R. Predictors of quality of life for autistic adults. Autism Res. 2018, 11, 1138–1147. [Google Scholar] [CrossRef]
- Rosen, N.E.; Lord, C.; Volkmar, F.R. The Diagnosis of Autism: From Kanner to DSM-III to DSM-5 and Beyond. J. Autism Dev. Disord. 2021, 51, 4253–4270. [Google Scholar] [CrossRef] [PubMed]
- Gotham, K.; Brunwasser, S.M.; Lord, C. Depressive and Anxiety Symptom Trajectories from School Age Through Young Adulthood in Samples with Autism Spectrum Disorder and Developmental Delay. J. Am. Acad. Child Adolesc. Psychiatry 2015, 54, 369–376.e3. [Google Scholar] [CrossRef] [PubMed]
- Leno, V.C.; Wright, N.; Pickles, A.; Bedford, R.; Zaidman-Zait, A.; Kerns, C.; Zwaigenbaum, L.; Duku, E.; Bennett, T.; Georgiades, S.; et al. Longitudinal associations between early childhood irritability and adolescent depression symptoms in autistic children are mediated by peer relationships but not educational engagement. Dev. Psychopathol. 2023, 36, 443–453. [Google Scholar] [CrossRef] [PubMed]
- Forbes, G.; Kent, R.; Charman, T.; Baird, G.; Pickles, A.; Simonoff, E. How do autistic people fare in adult life and can we predict it from childhood? Autism Res. 2022, 16, 458–473. [Google Scholar] [CrossRef] [PubMed]
- Simonoff, E.; Jones, C.R.; Pickles, A.; Happé, F.; Baird, G.; Charman, T. Severe mood problems in adolescents with autism spectrum disorder. J. Child Psychol. Psychiatry 2012, 53, 1157–1166. [Google Scholar] [CrossRef]
- Benevides, T.W.; Shore, S.M.; Palmer, K.; Duncan, P.; Plank, A.; Andresen, M.-L.; Caplan, R.; Cook, B.; Gassner, D.; Hector, B.L.; et al. Listening to the autistic voice: Mental health priorities to guide research and practice in autism from a stakeholder-driven project. Autism 2020, 24, 822–833. [Google Scholar] [CrossRef]
- Gentles, S.J.; Ng-Cordell, E.C.; Hunsche, M.C.; McVey, A.J.; Bednar, E.D.; DeGroote, M.G.; Chen, Y.-J.; Duku, E.; Kerns, C.M.; Banfield, L.; et al. Trajectory research in children with an autism diagnosis: A scoping review. Autism 2023, 28, 540–564. [Google Scholar] [CrossRef]
- Lombardo, M.V.; Lai, M.-C.; Baron-Cohen, S. Big data approaches to decomposing heterogeneity across the autism spectrum. Mol. Psychiatry 2019, 24, 1435–1450. [Google Scholar] [CrossRef]
- Baribeau, D.A.; Vigod, S.N.; Pullenayegum, E.; Kerns, C.M.; Vaillancourt, T.; Duku, E.; Smith, I.M.; Volden, J.; Zwaigenbaum, L.; Bennett, T.; et al. Developmental cascades between insistence on sameness behaviour and anxiety symptoms in autism spectrum disorder. Eur. Child Adolesc. Psychiatry 2022, 32, 2109–2118. [Google Scholar] [CrossRef]
- Baribeau, D.A.; Vigod, S.; Pullenayegum, E.; Kerns, C.M.; Mirenda, P.; Smith, I.M.; Vaillancourt, T.; Volden, J.; Waddell, C.; Zwaigenbaum, L.; et al. Repetitive Behavior Severity as an Early Indicator of Risk for Elevated Anxiety Symptoms in Autism Spectrum Disorder. J. Am. Acad. Child Adolesc. Psychiatry 2020, 59, 890–899.e3. [Google Scholar] [CrossRef]
- Baribeau, D.A.; Vigod, S.; Pullenayegum, E.; Kerns, C.M.; Mirenda, P.; Smith, I.M.; Vaillancourt, T.; Volden, J.; Waddell, C.; Zwaigenbaum, L.; et al. Co-occurring trajectories of anxiety and insistence on sameness behaviour in autism spectrum disorder. Br. J. Psychiatry 2021, 218, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Ben-Itzchak, E.; Koller, J.; Zachor, D.A. Characterization and Prediction of Anxiety in Adolescents with Autism Spectrum Disorder: A Longitudinal Study. J. Abnorm. Child Psychol. 2020, 48, 1239–1249. [Google Scholar] [CrossRef] [PubMed]
- Forbes, G.; Lord, C.; Elias, R.; Pickles, A. Predicting Uncertain Multi-Dimensional Adulthood Outcomes from Childhood and Adolescent Data in People Referred to Autism Services. Front. Psychol. 2021, 12, 594462. [Google Scholar] [CrossRef] [PubMed]
- Gray, K.; Keating, C.; Taffe, J.; Brereton, A.; Einfeld, S.; Tonge, B. Trajectory of Behavior and Emotional Problems in Autism. Am. J. Intellect. Dev. Disabil. 2012, 117, 121–133. [Google Scholar] [CrossRef] [PubMed]
- Mazurek, M.O.; Dovgan, K.; Neumeyer, A.M.; Malow, B.A. Course and Predictors of Sleep and Co-occurring Problems in Children with Autism Spectrum Disorder. J. Autism Dev. Disord. 2019, 49, 2101–2115. [Google Scholar] [CrossRef]
- Rai, D.; Culpin, I.; Heuvelman, H.; Magnusson, C.M.K.; Carpenter, P.; Jones, H.J.; Emond, A.M.; Zammit, S.; Golding, J.; Pearson, R.M. Association of Autistic Traits with Depression from Childhood to Age 18 Years. JAMA Psychiatry 2018, 75, 835–843. [Google Scholar] [CrossRef]
- Zachor, D.A.; Ben-Itzchak, E. From Toddlerhood to Adolescence, Trajectories and Predictors of Outcome: Long-Term Follow-Up Study in Autism Spectrum Disorder. Autism Res. 2020, 13, 1130–1143. [Google Scholar] [CrossRef]
- Achenbach, T.M.; Rescorla, L.A. Manual for the ASEBA School-Age Forms and Profiles; University of Vermont Research Center for Children, Youth, and Families: Burlington, VT, USA, 2001. [Google Scholar]
- Achenbach, T.M.; Rescorla, L.A. Manual for the ASEBA Adult Forms and Profiles; University of Vermont: Burlington, VT, USA, 2003. [Google Scholar]
- Vasa, R.A.; Mazurek, M.O. An update on anxiety in youth with autism spectrum disorders. Curr. Opin. Psychiatry 2015, 28, 83–90. [Google Scholar] [CrossRef]
- Chou, C.; Bentler, P.M.; Pentz, M.A. Comparisons of two statistical approaches to study growth curves: The multilevel model and the latent curve analysis. Struct. Equ. Model. A Multidiscip. J. 1998, 5, 247–266. [Google Scholar] [CrossRef]
- McNeish, D.; Matta, T. Differentiating between mixed-effects and latent-curve approaches to growth modeling. Behav. Res. Methods 2017, 50, 1398–1414. [Google Scholar] [CrossRef]
- Palmen, A.; Didden, R.; Lang, R. A systematic review of behavioral intervention research on adaptive skill building in high-functioning young adults with autism spectrum disorder. Res. Autism Spectr. Disord. 2012, 6, 602–617. [Google Scholar] [CrossRef]
- Pickles, A.; McCauley, J.B.; Pepa, L.A.; Huerta, M.; Lord, C. The adult outcome of children referred for autism: Typology and prediction from childhood. J. Child Psychol. Psychiatry 2020, 61, 760–767. [Google Scholar] [CrossRef] [PubMed]
- Frazier, T.W.; Georgiades, S.; Bishop, S.L.; Hardan, A.Y. Behavioral and Cognitive Characteristics of Females and Males with Autism in the Simons Simplex Collection. J. Am. Acad. Child Adolesc. Psychiatry 2013, 53, 329–340.e3. [Google Scholar] [CrossRef] [PubMed]
- Halladay, A.K.; Bishop, S.; Constantino, J.N.; Daniels, A.M.; Koenig, K.; Palmer, K.; Messinger, D.; Pelphrey, K.; Sanders, S.J.; Singer, A.T.; et al. Sex and gender differences in autism spectrum disorder: Summarizing evidence gaps and identifying emerging areas of priority. Mol. Autism 2015, 6, 36. [Google Scholar] [CrossRef] [PubMed]
- Jadav, N.; Bal, V.H. Associations between co-occurring conditions and age of autism diagnosis: Implications for mental health training and adult autism research. Autism Res. 2022, 15, 2112–2125. [Google Scholar] [CrossRef]
- Laugeson, E.A.; Gantman, A.; Kapp, S.K.; Orenski, K.; Ellingsen, R. A Randomized Controlled Trial to Improve Social Skills in Young Adults with Autism Spectrum Disorder: The UCLA PEERS® Program. J. Autism Dev. Disord. 2015, 45, 3978–3989. [Google Scholar] [CrossRef]
- Cassidy, S.A.; Bradley, L.; Bowen, E.; Wigham, S.; Rodgers, J. Measurement properties of tools used to assess depression in adults with and without autism spectrum conditions: A systematic review. Autism Res. 2018, 11, 738–754. [Google Scholar] [CrossRef]
- Mingins, J.E.; Tarver, J.; Waite, J.; Jones, C.; Surtees, A.D. Anxiety and intellectual functioning in autistic children: A systematic review and meta-analysis. Autism 2020, 25, 18–32. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).