Abstract
Background: The flexor digitorum brevis tendon to the fifth digit is frequently absent, and this absence is typically an incidental discovery during dissection or surgical studies. This study aimed to assess the frequency of a missing flexor digitorum brevis tendon in a Hispanic population for the first time, the association between the absence of the flexor digitorum brevis tendon, variables such as sex and ethnicity, and the functional implications of an absent tendon. Methods: Our sample consists of 30 cadavers whose feet were dissected and examined for the presence or absence of the digiti minimi tendon. Results: We found no significant relationship between the presence or absence of the tendon to sex or ethnicity. However, due to a lack of significant effects on human ambulation from the absence of this tendon, and the ability of adjacent muscles to adapt to its absence, the absence of this tendon might become increasingly prevalent over time. Conclusions: Knowledge of the frequency of flexor digitorum brevis variations concerning the demographic characteristics of patients would be of clinical importance for tendon repair, tendon transfer to correct deformities such as claw toe or hammer toe, or soft tissue reconstruction in foot surgery.
1. Introduction
Variations in the ankle and foot muscles are well-known [1,2,3,4,5]. The flexor digitorum brevis (FDB) belongs to the superficial layer of muscles of the plantar surface of the foot and serves to flex digits II-V at the proximal interphalangeal joint (Figure 1). The FDB tendons are typically inserted on the sides of the lateral four digits middle phalanx [1]. They are potentially clinically significant as the flexor tendons are often used for tendon transfers to correct deformities such as hammer toe [6]. Paralysis of the FDB results in distortion of the foot’s arch [7].
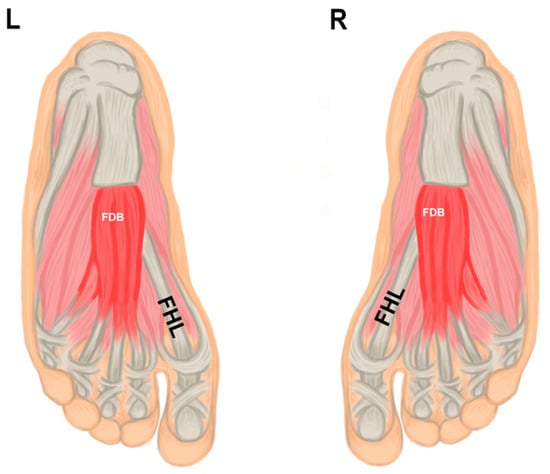
Figure 1.
Illustration showing the anatomy of plantar muscles; the flexor digitorum brevis muscle (FDB); the tendon of the flexor hallucis longus (FHL) of the left (L) and right (R) feet.
Clinical and cadaveric studies reported the incidence of the absence of the FDB’s of one of its tendons of 72% [6] and 74% [8], respectively. Nathan and Gloobe reported that in 23% of their cases, a part of muscle and tendon inserting the fifth toe was absent, and in 3% of cases inserting in the fourth and fifth toe was absent [9]. Standard descriptions mention that the tendon to the fifth digit is often degenerated or lacking [1,9,10,11,12]. In addition, Bergmann established that the FDB muscle sometimes has a small fifth tendon which replaces the missing flexor digitorum brevis tendon to the fifth toe [1]. Other reports also indicate that anatomical variations often accompany an absent FDB tendon and are sometimes replaced or compensated by other muscles. For instance, studies found that the missing tendon was replaced by an extra muscle originating from the calcaneal tuberosity with connections extending to the tendinous plate of the flexor digitorum longus and the quadratus plantae in a 75-year-old male cadaver [13].
Previous studies have shown that, although there are no significant differences in peak pressure or contact time during walking in males and females, the contact area of the foot in males is consistently larger [14]. This foot surface area distinction may suggest a difference in the underlying anatomy of the foot in males and females, which may extend to the presence or absence of flexor tendons. Retrospective studies reported the absence of one of the tendons of the FDB as a common occurrence [1,6,8,9,10,11].
From a clinical perspective, the anatomical variations of FDB reinforce the need to understand anatomical diversity to develop appropriate surgical approaches and diagnostic tools. Awareness of muscle attachments of the foot will assist in biomechanical modeling of the foot and surgical procedures, such as tendon transfer, reconstruction of the heel pad, and correction of claw and hammer toe deformity [6,12].
Despite its significance, there is a gap in knowledge regarding variations of the FDB muscle in the Puerto Rican population compared to Caucasians and African Americans. Therefore, the present study assesses the frequency of a missing flexor digitorum brevis tendon to the fifth digit from a functional standpoint, focusing on its presence or absence in different populations by ancestry and sex.
2. Materials and Methods
2.1. Data Acquisition
The present study examined 30 embalmed cadavers at the Universidad Central del Caribe School of Medicine and School of Health and Allied Sciences, the Ponce Health Sciences University, and the Texas Woman’s University’s School of Physical Therapy. Specimens were obtained from the Anatomical Donations Boards at the University of Puerto Rico School of Medicine and the Texas Woman’s University School of Physical Therapy. Fourteen males and sixteen females were included. Specimens were preserved using 10% formalin. Clinical history, family history, and cause of death are not available.
2.2. Plantar Aspect of the Foot Dissection
The feet were dissected by a medial and plantar incision, removing the plantar skin. Next, the tarsal tunnel was dissected, and all anatomical structures were identified. The plantar aponeurosis was carefully dissected from the flexor digitorum brevis (FDB) and reflected proximally. Afterward, the FDB and flexor hallucis brevis (FHB) were dissected and reflected proximally. Next, separating the FDB from other structures and separate tendons of the FDB was performed via blunt dissection to keep structures intact. We then assessed the presence or absence (Figure 2) of the flexor digitorum brevis tendon to the fifth digit.
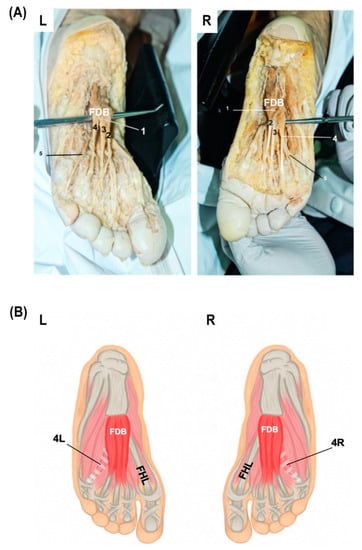
Figure 2.
(A) Dissection showing the muscle belly of the flexor digitorum brevis (FDB) of the left (L) and right (R) feet (1); tendon to second phalanx (2); tendon to third phalanx (3); tendon to fourth phalanx (4); fourth tendon from flexor digitorum longus (5). (B) Illustration showing the variation encountered during dissection of left and right feet, the bilateral absence of the fourth tendon of the flexor digitorum brevis (FDB); the tendon of the flexor hallucis longus (FHL); the missing fourth tendon from FDB on the left (4L) and right (4R).
2.3. Statistical Analysis
We used a contingency table to analyze relationships among variables. The variables used were sex, side of the body, ethnicity, and presence or absence of the tendon to the fifth digit. We performed a Chi-square test to assess the significance of associations between variables. Still, when our expected results were less than five in the contingency tables, we also conducted a Fisher’s exact test. The graphs were designed using GraphPad Prism version 9.0 (GraphPad Software, San Diego, CA, USA). The results were considered statistically significant when p ≤ 0.05.
2.4. Ethical and Bioethical Principles
This research was performed following the regulations provided by donor programs and institutions in compliance with the laws and ethical standards in the country where the research was conducted. The donors’ identifiers, family histories, clinical histories, and death certificates were unavailable for the participating medical institutions. The results provided were used solely for scientific purposes.
3. Results
3.1. Descriptive Statistics
We identified the presence or absence of the FDB muscle tendon to the digiti minimi. Eight of 30 individuals in our sample (26.7%) were missing the FDB fourth tendon to the fifth digit. In comparison, 22 of 30 individuals (73.3%) had the standard configuration. Of individuals with the variation present, 2 (25%) had a unilateral variation, and 6 (75%) had a bilateral variation. When analyzing the sex of those subjects with the variation, 3 (37.5%) were males, and 5 (62.5%) were female (Figure 3A). Regarding ancestry, 8 (100%) individuals with the variation were Puerto Ricans. Neither White Americans nor African Americans had the variation.
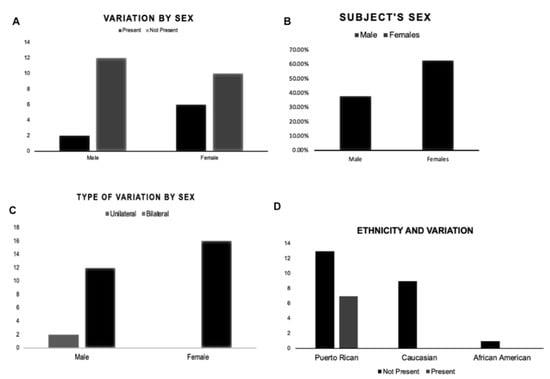
Figure 3.
Variables used to evaluate the frequency of FDB variation (A) frequency of male and female subjects with the variation; (B) presence or absence of the variation by the subject’s sex; (C) type of variation by subject’s sex; (D) presence or absence of variation by ethnicity.
3.2. Association between Sex, Ancestry, and Presence or Absence of the FDB Fourth Tendon
There is no association between the presence or absence of the variation by sex (Figure 3B) (X2 = 0.0373, p > 0.05). We also evaluated the association of sex to the type of variation specifically (Figure 3C). As before, the results indicated no significant difference between males and females and the type of variation they present (X2 = 2.61, p > 0.05). We found no association between the presence of the variation and ancestry (Figure 3D) (X2 = 4.47, p > 0.05). Therefore, based on the results, a person’s ancestry is not related to the presence or absence of the variation.
4. Discussion
Our study aimed to determine the occurrence of variations of the FDB muscle in the Hispanic population, whether variables such as sex and ancestry were associated with the absence of the FDB’s fourth tendon, and the clinical implications related to this anatomical variation.
The current study found no significant differences between females (37.5%) and males (62.5%) in the anatomical variation proportion. These percentages are similar to those reported in other studies, which report frequencies between 18% and 63% [1,9,10]. Furthermore, there were no significant differences in ancestry in our study comparing Puerto Ricans with White Americans or African Americans. However, previous studies evaluating skeletal muscle mass showed that African Americans tended to have higher skeletal muscle mass differences than White Americans and Hispanics [15].
We found a 26.7% frequency of a bilaterally missing tendon to the fifth digit. Speculation about the partial absence of the FDB tendon attributes it to degenerative changes among diverse populations or evolutionary adaptations [11,16]. Although humans rely heavily on their feet for walking and support, and the human foot has evolved to be highly efficient in bipedal walking, humans cannot oppose the first and fifth digits in the foot, unlike other primates, who use highly dexterous feet to assist with activities such as climbing [17]. Instead, in humans, the FDB is associated with postural control and longitudinal arch support [18]. The intrinsic plantar muscles contribute to stiffening the metatarsophalangeal joints in a late stance during walking or running to assist propulsive push-off [19]. Additionally, the FDB assists the flexor digitorum longus (FDL) during the flexion of the second to the fifth toe [20]. However, studies showed that plantar flexion was not affected by removing the FDB tendon for correction of claw or hammer toe deformities, and its absence does not affect the stability of the foot during gait [12].
Other studies focused on variation in the foot musculature reveal that the absence of the FDB tendon is associated with the presence of a particularly rare muscle called the flexor digiti quinti (FDQ), whose tendon extends from the common flexor digitorum longus [21]. In contrast to the FDB, which develops embryologically from anterior condensations of abaxial muscle cell precursors [22], the FDQ derives from the distal part of the crural pronator-flexor mass [21], suggesting that the FDQ is not a variant morphology of the FDB itself. Nevertheless, none of the cadavers have this associated FDQ variation and not a separate muscle belly.
Together, these findings suggest that, although compensatory variations are frequently associated with a missing flexor digitorum brevis tendon, there may ultimately be little functional effect on individuals with an absent tendon. Recent studies suggest that oxidative stress can influence cell signaling pathways that regulate muscle protein breakdown and synthesis during a prolonged period of disuse [23]. Thus, the anatomical variation presented in this study may be a result of skeletal muscle inactivity causing muscle fiber atrophy function [24,25]. Although the full functional consequences of this variation relative to individuals with a normal flexor digitorum brevis are unknown, we suggest that there might be a more significant clinical indication.
From a clinical standpoint, knowledge about the anatomical variations of flexor digitorum brevis has several implications [26,27]. Deformities of the lesser toes are recurrently encountered with significant morbidity [28]. Hammer and claw toe are deformities that affect the proximal interphalangeal joint, the metatarsophalangeal joint, and the distal interphalangeal joint, if present. Claw toe instability at the proximal interphalangeal joint may be corrected by an FDB tenotomy [28]. In procedures like the Valtin approach, as described by [29], the FDB is used to replace the function of an FDL tendon that has been shortened due to ischemic muscle contracture. With this technique, the FDB muscle was successfully used to restore flexion in these sets of patients [29,30]. Also, the FDB muscle is used as one of the three intrinsic foot muscles to cover diabetic foot wounds through local flaps for foot reconstruction [31]. This surgical intervention can be used for coverage of minor foot defects such as calcaneal defects. In addition, tendon variation can impact the viability of these procedures since the FDB can no longer be used as a graft, assuming the patient in question has a variation or atrophy of the tendon or muscle belly. One of the potential limitations of this study was the limited quantity of specimens used for the observations and quantitative analysis. Therefore, increasing anatomical studies may provide further insight into long-term clinical outcomes regarding the availability of specific procedures.
5. Conclusions
The incidental discovery of the absence of the flexor digitorum brevis tendon during dissections or surgical procedures has been noted for many years. Here, we assessed the prevalence of this variation in a Hispanic population and whether there were any links between sex, ancestry, and the presence of this variation. There was no significant association between the presence or absence of the tendon and sex or ancestry in our 30-cadaver sample. Future directions will include greater samples and completed foot anatomy and function variation analyses.
Author Contributions
Conceptualization, J.I.Q.-R., C.M.-R., F.R. and C.I.V.; methodology and collected data, J.I.Q.-R., C.M.-R., F.R., C.I.V., J.F., M.G.-S. and M.G.R.; data analysis: C.T.-T. and J.I.Q.-R.; writing—original draft preparation, J.I.Q.-R., C.M.-R., F.R. and C.I.V.; review and editing, J.I.Q.-R., C.M.-R., F.R., C.I.V., J.F., M.G.-S., C.T.-T. and M.G.R.; project administration, J.I.Q.-R. Authors have critically reviewed and approved the final draft and are responsible for the content and similarity index of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This research was performed following the regulations provided by donor programs and institutions in compliance with the laws and ethical standards in the country where the research was conducted. No additional approval from an ethics board was required for this study.
Informed Consent Statement
Patient consent was waived due to the donors’ identifiers, family histories, clinical histories, and death certificates being unavailable for the participating medical institutions. The results provided were used solely for scientific purposes.
Data Availability Statement
Not applicable.
Acknowledgments
This work was performed at Universidad Central del Caribe School of Medicine. The authors gratefully acknowledge the collaborating academic institutions for providing the cadavers for this study. Also, we thank Jose E. Quiles-Ruiz, for the graphical illustration. This research was supported by the Puerto Rico IDeA Network of Biomedical Research Excellence, an Institutional Development Award (IDeA) from the National Institute of General Medical Sciences of the National Institutes of health under the grant no. P20GM103475.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bergmann, R.A.; Thompson, S.A.; Afifi, A.K.; Saadeh, F.A. Compendium of Human Anatomic Variation; Urban & Schwarzenberg: Baltimore, MD, USA; Munich, Germany, 1988; pp. 27–28. [Google Scholar]
- Aparisi Gómez, M.P.; Aparisi, F.; Bartoloni, A.; Ferrando Fons, M.A.; Battista, G.; Guglielmi, G.; Bazzocchi, A. Anatomical variation in the ankle and foot: From incidental finding to inductor of pathology. Part II: Midfooot and forefoot. Insights Imaging 2019, 10, 69. [Google Scholar] [CrossRef] [PubMed]
- Bernhard, A.; Miller, J.; Keeler, J.; Siesel, K.; Bridges, E. Absence of the Fourth Tendon of the Flexor Digitorum Brevis Muscle: A Cadaveric Study. Foot Ankle Spec. 2013, 6, 286–289. [Google Scholar] [CrossRef] [PubMed]
- Ferreira Arquez, H. An Anatomical Study of The Musculus Flexor Digitorum Brevis. Int. Arch. Med. 2017, 10, 1–5. [Google Scholar] [CrossRef]
- Vega, J.; Redó, D.; Savín, G.; Malagelada, F.; Dalmau-Pastor, M. Anatomical variations of flexor hallucis longus tendon increase safety in hindfoot endoscopy. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 1929–1935. [Google Scholar] [CrossRef] [PubMed]
- Ilayperuma, I. On the variations of the muscle flexor digitorum brevis: Anatomical insight. Int. J. Morphol. 2012, 30, 337–340. [Google Scholar] [CrossRef][Green Version]
- Rosse, C.; Gaddum-Rosse, P. Hollinshead’s Textbook from Anatomy, 6th ed.; Lippincott–Raven: Philadelphia, PA, USA, 1997. [Google Scholar]
- Agarwal, R.; Khajuria, S.; Saini, H. Study of Absence of 4th Tendon of Flexor Digitorum Brevis Muscle. Int. J. Anat. Res. 2017, 5, 47–50. [Google Scholar] [CrossRef]
- Nathan, H.; Gloobe, H. Flexor digitorum brevis--anatomical variations. Anat. Anzeiger. 1974, 135, 295–301. [Google Scholar]
- Yalçın, B.; Ozan, H. Some variations of the musculus flexor digitorum brevis. Anat. Sci. Int. 2005, 80, 189–192. [Google Scholar] [CrossRef]
- Lobo, S.W.; Menezes, R.G.; Mamata, S.; Baral, P.; Hunnargi, S.A.; Kanchan, T.; Bhat, N.B. Phylogenetic variation in flexor digitorum brevis: A Nepalese cadaveric study. Nepal Med. Coll. J. 2008, 10, 230–232. [Google Scholar] [PubMed]
- Becerro de Bengoa Vallejo, R.; Viejo Tirado, F.; Prados Frutos, J.C.; Losa Iglesias, M.E.; Jules, K.T. Transfer of the flexor digitorum brevis tendon. J. Am. Podiatr. Med. Assoc. 2008, 98, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Claassen, H.; Wree, A. Isolated flexor muscles of the little toe in the feet of an individual with atrophied or lacking 4th head of the M. extensor digitorum brevis and lacking the 4th tendon of the M. extensor digitorum longus. Ann. Anat. 2003, 185, 81–84. [Google Scholar] [CrossRef] [PubMed]
- Putti, A.B.; Arnold, G.P.; Abboud, R.J. Foot pressure differences in men and women. Foot Ankle Surg. 2010, 16, 21–24. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.M.; Shen, W.; Heo, M.; Gallagher, D.; Wang, Z.; Sardinha, L.B.; Heymsfield, S.B. Ethnicity-related skeletal muscle differences across the lifespan. Am. J. Hum. Biol. 2010, 22, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Chaney, D.M.; Lee, M.S.; Khan, M.A.; Krueger, W.A.; Mandracchia, V.J.; Yoho, R.M. Study of ten anatomical variants of the foot and ankle. J. Amer. Podiatr. Med. Assoc. 1996, 86, 532–537. [Google Scholar] [CrossRef] [PubMed]
- McNutt, E.J.; Zipfel, B.; DeSilva, J.M. The evolution of the human foot. Evol. Anthropol. 2018, 27, 197–217. [Google Scholar] [CrossRef] [PubMed]
- Grogono, B.J.S.; Jowsey, J. Flexor Accessorius Longus an Unusual Muscle Anomaly. J. Bone Jt. Surg. 1965, 47, 118–119. [Google Scholar] [CrossRef]
- Farris, D.J.; Kelly, L.A.; Cresswell, A.G.; Lichtwark, G.A. The functional importance of human foot muscles for bipedal locomotion. Proc. Natl. Acad. Sci. USA 2019, 116, 1645–1650. [Google Scholar] [CrossRef] [PubMed]
- Hartrampf, C.R.; Scheflan, M.; Bowstwick, J. The flexor digitorum brevis muscle Island pedicle flap: A new in dimension heel reconstruction. Plast. Reconstr. Surg. 1980, 66, 264–270. [Google Scholar] [CrossRef]
- Stimec, B.V.; Dash, J.; Assal, M.; Stern, R.; Fasel, J.H.D. Additional muscular slip of the flexor digitorum longus muscle to the fifth toe. Surg. Radiol. Anat. 2018, 40, 533–535. [Google Scholar] [CrossRef]
- Tarpey, M.D.; Amorese, A.J.; Balestrieri, N.P.; Ryan, T.E.; Schmidt, C.A.; McClung, J.M.; Spangenburg, E.E. Characterization and utilization of the flexor digitorum brevis for assessing skeletal muscle function. Skelet. Muscle 2018, 8, 14. [Google Scholar] [CrossRef]
- Powers Scott, K.; Smuder Ashley, J.; Judge Andrew, R. Oxidative stress and disuse muscle atrophy. Curr. Opin. Clin. Nutr. Metab. Care 2012, 15, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Malavaki, C.J.; Sakkas, G.K.; Mitrou, G.I.; Kalyva, A.; Stefanidis, I.; Myburgh, K.H.; Karatzaferi, C. Skeletal muscle atrophy: Disease-induced mechanisms may mask disuse atrophy. J. Muscle Res. Cell Motil. 2015, 36, 405–421. [Google Scholar] [CrossRef] [PubMed]
- Clark, B.C. In vivo alterations in skeletal muscle form and function after disuse atrophy. Med. Sci. Sport. Exerc. 2009, 41, 1869–1875. [Google Scholar] [CrossRef] [PubMed]
- Thangarajan, R.; Bakthavatchalam, P.; Potu, B.; Huban, T. Anatomical variation of the flexor digitorum brevis muscle revisited: A case report from South Indian population. Int. J. Anat. Var. 2010, 3, 1000–1002. [Google Scholar]
- Kaissar, Y. The Fourth Slip of the Flexor Digitorum Brevis Muscle of the Human Foot: A Systematic Review and Meta-Analysis. Anat. Appl. 2015, 120, 59–70. [Google Scholar]
- Malhotra, K.; Davda, K.; Singh, D. The pathology and management of lesser toe deformities. EFORT Open Rev. 2017, 1, 409–419. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, H.; Kajetanek, C.; Graff, W.; Thiongo, M.; Laporte, C. Flexor digitorum brevis tendon transfer to the flexor digitorum longus tendon according to Valtin in posttraumatic flexible claw toe deformity due to extrinsic toe flexor shortening. Orthop. Traumatol. Surg. Res. 2015, 101, 257–260. [Google Scholar] [CrossRef][Green Version]
- García-González, A.; Bayod, J.; Prados-Frutos, J.C.; Losa-Iglesias, M.; Jules, K.T.; Becerro de Bengoa-Vallejo, R.; Doblaré, M. Finite-element simulation of flexor digitorum longus or flexor digitorum brevis tendon transfer for the treatment of claw toe deformity. J. Biomech. 2009, 42, 1697–1704. [Google Scholar] [CrossRef]
- Deldar, R.; Merle, C.; Attinger, C.E.; Evans, K.K. Soft tissue coverage of lower extremity defects: Pearls and pitfalls in the chronic wound population. Plast. Aesthet. Res. 2022, 9, 13. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).