1. Introduction
Tuberculosis (TB) is a communicable disease that imposes a global public health burden, with over 10 million new cases and over a million TB-related deaths annually. Despite the active measures and treatments developed to tackle it, TB remains the top cause of deaths due to a communicable disease [
1]. While TB can be symptomatic, referred to as active TB, patients with TB could be in a state of persistent immune response to TB without evidence of clinical manifestations, referred to as latent TB [
2]. In Saudi Arabia, it is estimated that latent TB infections range between 10% and just over 30% of studied cohorts [
3], with an incidence of 14 per 100,000 inhabitants [
4].
Since the beginning of the coronavirus disease 2019 (COVID-19) pandemic, countries were in a race to implement measures to tackle it. Saudi Arabia was one of the earliest countries to implement progressive measures that significantly reduced the forecasted mortality [
5]. Additionally, Saudi Arabia continued to apply protective measures despite being one of the earliest countries to approve both COVID-19 vaccines, Pfizer/BioNTech and AstraZeneca, and use them in a mass vaccination program. Additionally, precautionary measures were introduced, such as mandatory face masks in public and compulsory temperature measurement of anyone entering a closed place such as shops, airports or governmental buildings. These measures continued even after the beginning of mass vaccination, as the first dose was not enough to prevent the spread of infection [
6]. Although these measures were aimed directly at detecting COVID-19, they can be used to detect other conditions, e.g., TB.
In this study, we present four different scenarios in which the implementation of these measures assisted in detecting cases of TB. The detection of these cases would not be possible without the use of these measures. These case scenarios make a case for the continuous implementation of COVID-19 measures, even after the resolution of the ongoing COVID-19 pandemic.
3. Results
3.1. Case 1: A Traveling Salesman
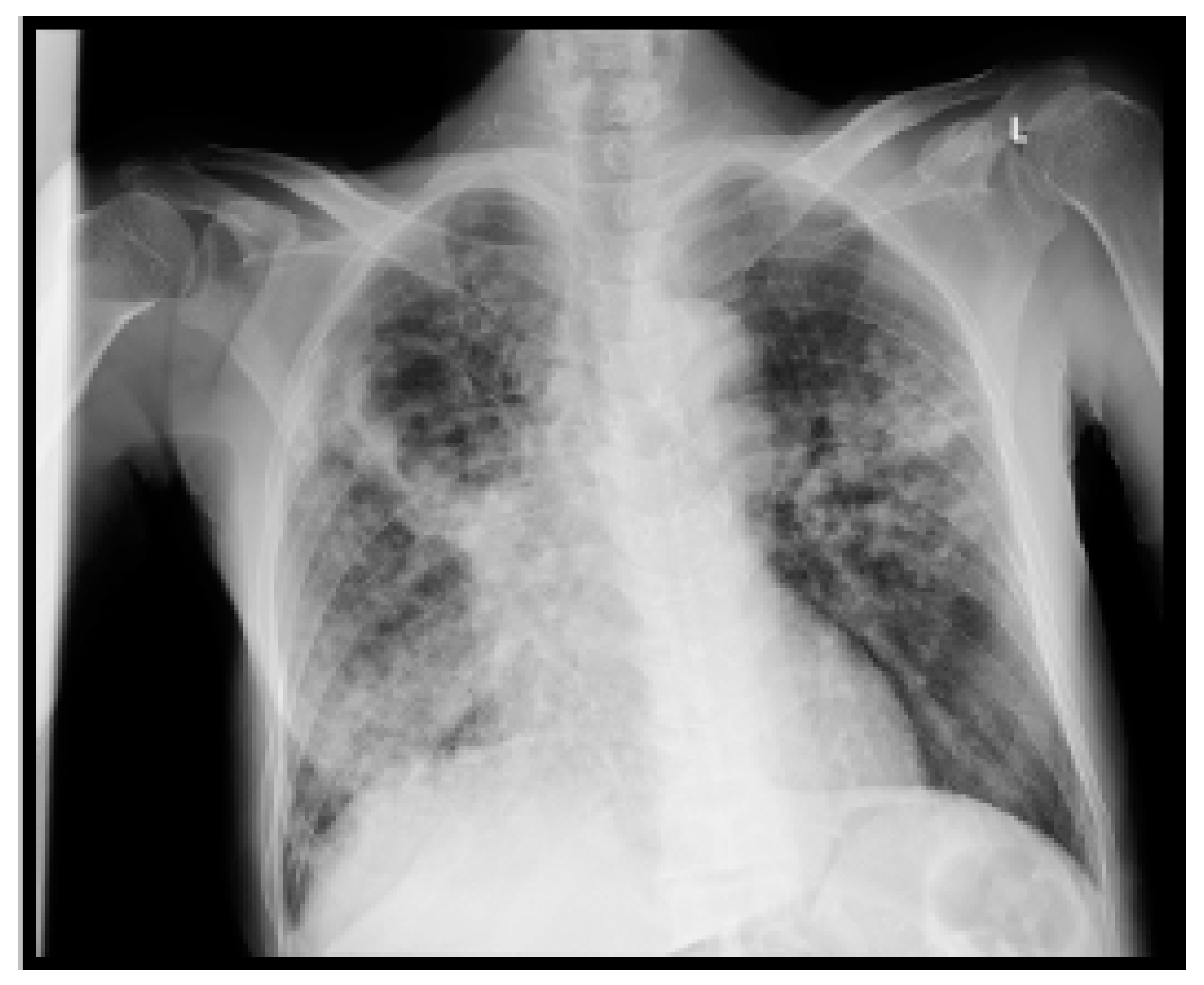
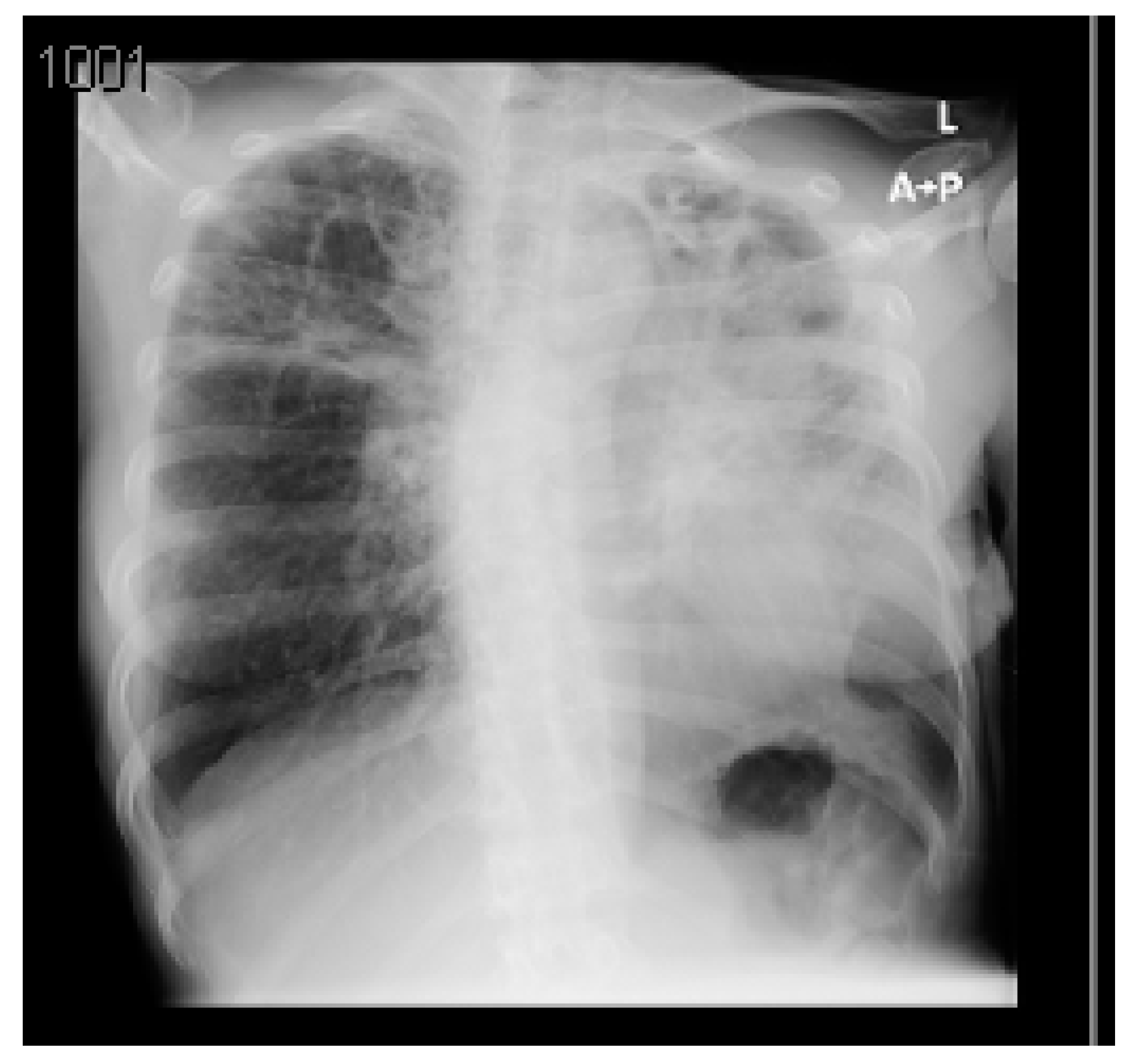
Case 1 is a 51-year-old male with a history of hypertension and diabetes for the last 2 years, who is not compliant with medications. He was brought by the emergency medical services from King Khalid International Airport, with hemoptysis and suffering from shortness of breath and chest pain. He arrived at the KAAUH ED, coughing blood.
His condition started 3 days before with hemoptysis, followed by exertional dyspnea with minimal activity, and was associated with chest pain on the day of travel. According to him, he had no previous episodes of vomiting blood, having a fever or being in contact with a sick person and had no weight loss or night sweats.
Upon examination, the patient looked ill, coughing blood. His vitals were as follows: blood pressure was 130/82 mmHg, mean arterial pressure was 98, heart rate was 116 beats per minute (bpm), respiratory rate was 30 breaths/minute, temperature was 37 °C, and O2 saturation was 96% on 7 L of O2.
His chest examination revealed scattered crepitation all over his lung fields, more pronounced on the left side. The rest of the physical examination was unremarkable. His ECG showed sinus tachycardia with an ST depression in the anterior leads.
A summary of his laboratory and radiological investigations are described in
Table 1 and
Figure 1, respectively.
A CT chest with contrast was completed to confirm the CXR findings and was reported as: ‘Bilateral multiple patchy cavitating consolidations larger at the apical posterior segment of left upper lobe, differential diagnosis includes cavitating pneumonia, fungal infection or TB, especially with the involvement of the the apicoposterior segment and less likely to represent septic emboli’. The patient was admitted to the intensive care unit (ICU) with the impression of COVID-19 or TB pneumonia and acute coronary syndrome. The patient was examined by the Cardiology and Gastroenterology teams, who ruled out any significant conditions and placed him on conservative therapy.
The patient was placed in a negative-pressure airborne isolation room, and three samples were sent for, acid-fast bacilli (AFB), smear and cultures and TB PCR testing. The AFB and PCR tests were positive for TB, and the patient received first-line anti-TB medications (REF): Isoniazid (INH) 300 mg OD, Ethambutol 1200 mg OD, Pyrazinamide 1500 mg OD, Rifampicin 600 mg OD and Pyridoxine 40 mg OD. The patient was kept in isolation until his AFB sample was negative. He was discharged with instructions to continue Rifampicin, INH, Pyrazinamide and Ethambutol for eight weeks, followed by Rifampicin, INH and Pyridoxine for seven months.
3.2. Case 2: A Heavy Machine Operator
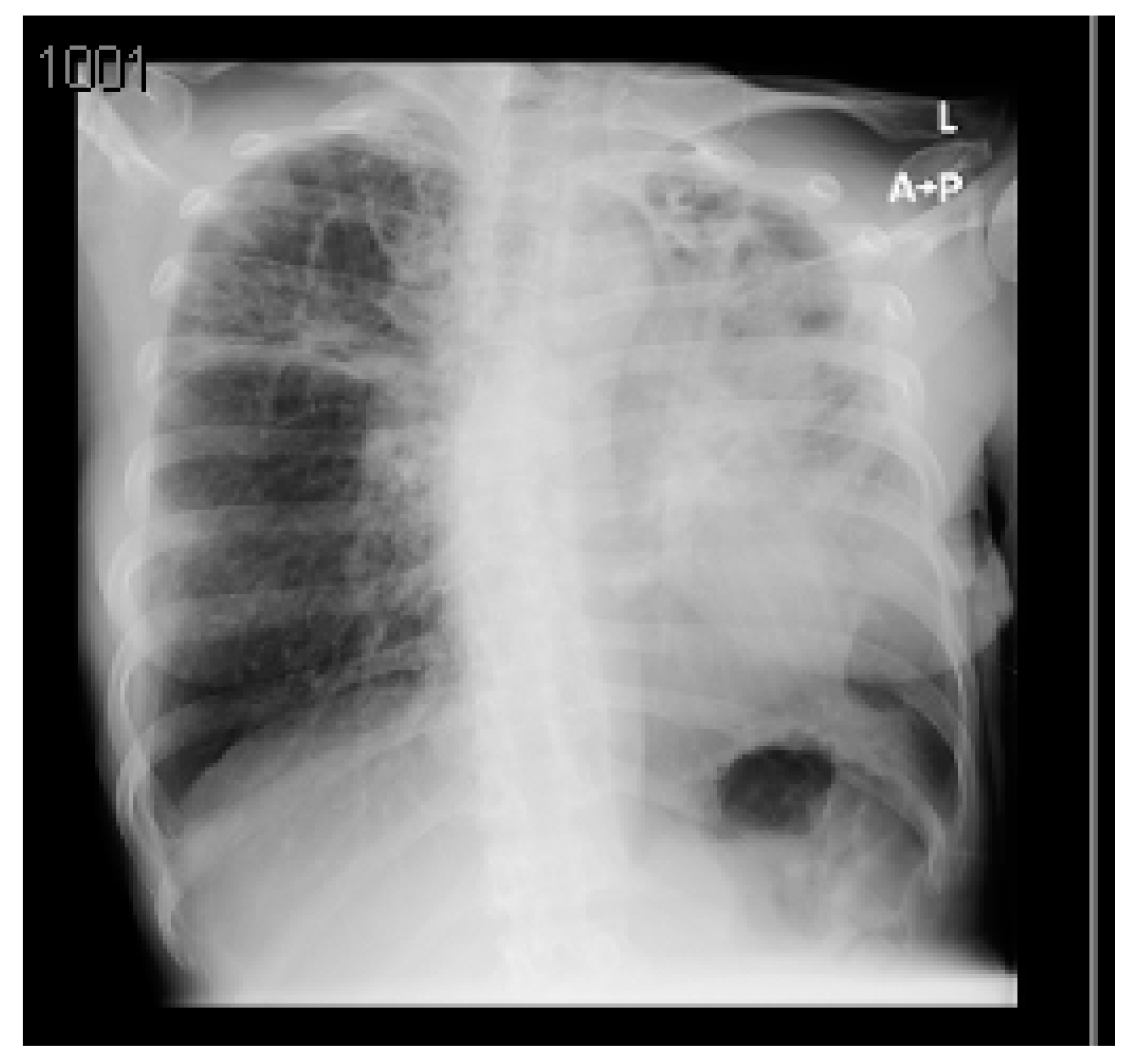
A 58-year-old Filipino male is a known case of bronchial asthma and diabetes mellitus type 2, who is on metered dose inhalers and oral hypoglycemic agents. He has worked as a heavy machine operator in an industrial area for the past 10 years. The worker was about to fly home; however, he missed his flight due to a severe coughing episode, with intermittent expectorations and exertional dyspnea at the airport. The airport emergency medical services brought him to the emergency department. Careful history-taking demonstrated that the cough started one month prior and was associated with more than 10% weight loss. The patient denied any hemoptysis, fever or gastrointestinal symptoms. The patient reported no history of COVID-19 infection or interaction with COVID-19 patients.
Upon examination, the patient was conscious and oriented, in mild respiratory distress, and his oxygen saturation was 98% on 4 L of oxygen with nasal prongs. His respiratory rate was between 18–22 breaths/minute, his heart rate was 140+ bpm, and he was afebrile. He had normal heart sounds; however, his chest examination revealed scattered crackles and rhonchi. His ECG showed sinus tachycardia, i.e., a heart rate of 140 bpm, Qs V1–V3 and T wave inversion in leads v2–v6.
A summary of the patient’s CXR and lab investigations are demonstrated in
Figure 2 and
Table 2, respectively.
The patient was admitted to the ICU, where cardiologists reviewed him. The patient was given antiplatelet therapy, cholesterol-lowering therapy, omeprazole and IV fluid, with serial troponin and ECG 6-hourly. The patient was started on steroids, magnesium sulphate, bronchodilators, azithromycin and tazocin, and samples were sent for a septic screen, COVID-19 testing, three AFB samples, smear and cultures and TB PCR testing.
The first AFB and TB PCR returned positive; after 1 h, the patient was started on first-line TB treatment and was shifted to the medical ward in a negative-pressure isolation room in stable condition. After 23 days of hospitalization, the patient was discharged after three negative samples of AFB and was instructed to continue on INH, Rifampicin and Pyridoxine for 7 months more, to complete 9 months of TB treatment course.
3.3. Case 3: An Infrastructure Worker in a Remote Area
A 36-year-old male Filipino male is a known case of type 2 diabetes mellitus on metformin, who is working in road infrastructure in Abha, a remote administrative region with a low population density. The patient was in transit at the airport when he developed a sudden onset of severe shortness of breath, which prompted the airport EMS team to bring him to the ED. The patient mentioned a history of cough with sputum, fatigue, excessive sweating at night and weight loss (>20 kg) in the past 2 months. The patient denied chest pain, fever and contact with sick people or COVID-19 patients.
Upon examination, the patient was alert and looked underweight and cachexic. His vital signs were as follows: blood pressure was 87/63 mmHg, temperature was 37.7 °C, pulse was 102 bpm, respiratory rate was 24 breaths/minute and O2 saturation was 97% on room air. His chest examination revealed bilateral course crepitations. His cardiovascular examination demonstrated normal heart sounds with no murmurs. His abdomen was soft and lax. ECG recording showed sinus tachycardia with a heart rate of 110 bpm, ST segment elevations in leads in V5–V6 and T wave inversion in leads V2–V3.
A summary of the patient’s CXR and lab investigations’ findings are demonstrated in
Figure 3 and
Table 3, respectively.
An ACT scan of the chest was completed to verify the findings of the CXR. The CT scan revealed large cavitary lesions with septations involving both lungs more severely at the upper lobes bilaterally. They were associated with traction bronchiectasis, bronchial wall thickening, fibrotic changes and tri in buds.
Multifocal patches of ground-glass opacities were seen involving both lower lobes, associated with a crazy-paving appearance. Mucous secretions were seen in the trachea, right main bronchus and right bronchi. Interstitial septal thickening was noted with diffuse nodular changes.
An echocardiography examination was performed, showing an ejection fraction of 35–40%, severe hypokinesis of the apex and most of the anterior wall and a trace of pericardial effusion. The echo was unremarkable otherwise. The cardiology team was consulted, which advised that the patient would not benefit from an invasive intervention, and medical therapy would be the treatment of choice.
The patient was admitted to the ICU with suspected pulmonary TB, COVID-19 and acute coronary syndrome. A septic workup, TB PCR and three AFB samples were sent for investigation. Meanwhile, the patient was initially started on tazocin and azithromycin. His TB PCR and first AFB samples, smear and cultures were positive; hence, he was started on first-line TB medications. The patient’s condition worsened, warranting an intubation, and he later developed right pneumothorax, for which he was managed correctly. He was shifted to the medical ward once he was in stable condition, after 2 months of intensive care.
He was later discharged with the instruction to continue anti-TB therapy with four drugs and pyridoxine for a total of 3 months. After that, he should continue INH, rifampicin and pyridoxine for a total of 5 months.
3.4. Case 4: A Departing Domestic Worker in a Peripheral City
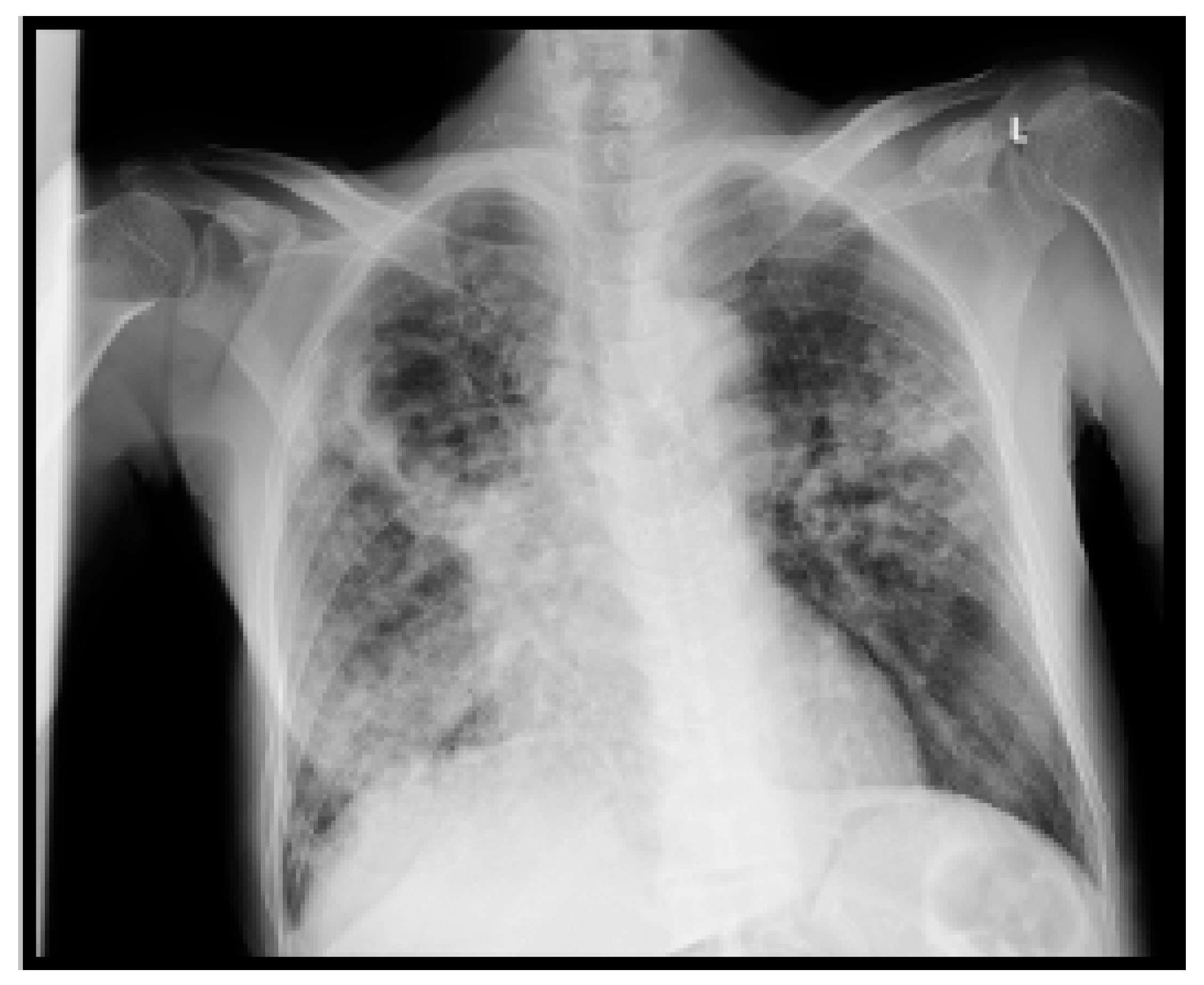
A 39-year-old female patient is a known case of primary hypertension and is on monotherapy of Nifedipine 30 mg OD. She was about to depart the country, when she was found to have a low-grade fever at the airport. Additionally, she complained of hemoptysis and shortness of breath, which warranted her dispatch to our emergency department using the airport’s emergency medical services. Upon arrival at the emergency department, her oxygen saturation was 85% initially, so she was stabilized with a 4 L oxygen through a nasal cannula.
She reported that she has worked as a domestic worker in AlMajmah, a small peripheral city, for the past 22 months. Her symptoms started almost a year ago, with a productive cough and shortness of breath, for which she did not seek medical advice. It was associated with significant unintentional weight loss from 78 kg to 43 kg over a year, in addition to poor appetite. She also admitted having a history of low-grade fever occasionally. Over the last month, she started to have sputum mixed with blood; however, no frank hemoptysis was noted. She also denied any dizziness or palpitation.
She was admitted to a local secondary hospital for 2 weeks; however, she did not have a clear idea of her diagnosis there, no discharge medications were given to the patient, and the hospital’s report was not available from her. An effort was made to contact her sponsor for further information.
Upon examination, the patient was conscious, oriented, alert, and cachectic and looked in respiratory distress. Her vital signs were as follows: blood pressure was 104/77 mmHg, pulse was 78 bpm, respiratory rate was 16 breaths/minute, and temperature was 36.8 °C. Her initial oxygen saturation was 85% on room air. She was given oxygen through a face mask and switched to 4 L of oxygen through a nasal cannula to maintain her saturation above 95%. Her chest examination revealed crackles all over her left side and crackles on the right side up to one-third of her right lung. Her cardiovascular, abdominal and peripheral examinations were unremarkable.
During admission, the patient’s hemoptysis caused her hemoglobin to drop from 8.9 to 6.7 g/dL, for which she received two packed RBCs.
A summary of the patient’s CXR and lab investigations’ findings are demonstrated in
Figure 4 and
Table 4, respectively.
The patient was admitted to the medical ward in a negative-pressure room with airborne/droplet precaution, with the impression of pulmonary TB or multilobar pneumonia. A COVID-19 swab, three early morning samples were collected for sputum AFB, smear and cultures, and TB PCR. A full septic work up, inflammatory markers and D-dimer were requested. Initially, the patient started on first line anti-TB medications ceftriaxone and nifedipine. After one day, her COVID-19 test came back negative; however, her AFB and TB PCR came back positive, for which TB medications continued to be given, and the patient is still under our care at the KAAUH hospital.
4. Discussion
Since the detection of the first case of COVID-19 in Saudi Arabia in March 2020, Saudi Arabia took a series of measures to tackle the spread of COVID-19 infection. These measures were progressive in nature, up to national curfews, and directly contributed to the reduced COVID-19-related mortality rates in Saudi Arabia, compared to some developed countries such as the UK and the US [
5]. Following that, the government started a national campaign called ‘We all return with caution’, which aimed to instruct a number of safety measures to ensure a safe return to how it was without COVID-19 strict measures. These measures included mandatory face masks in closed spaces, which has been determined to be an important step in tackling the spread of COVID-19 [
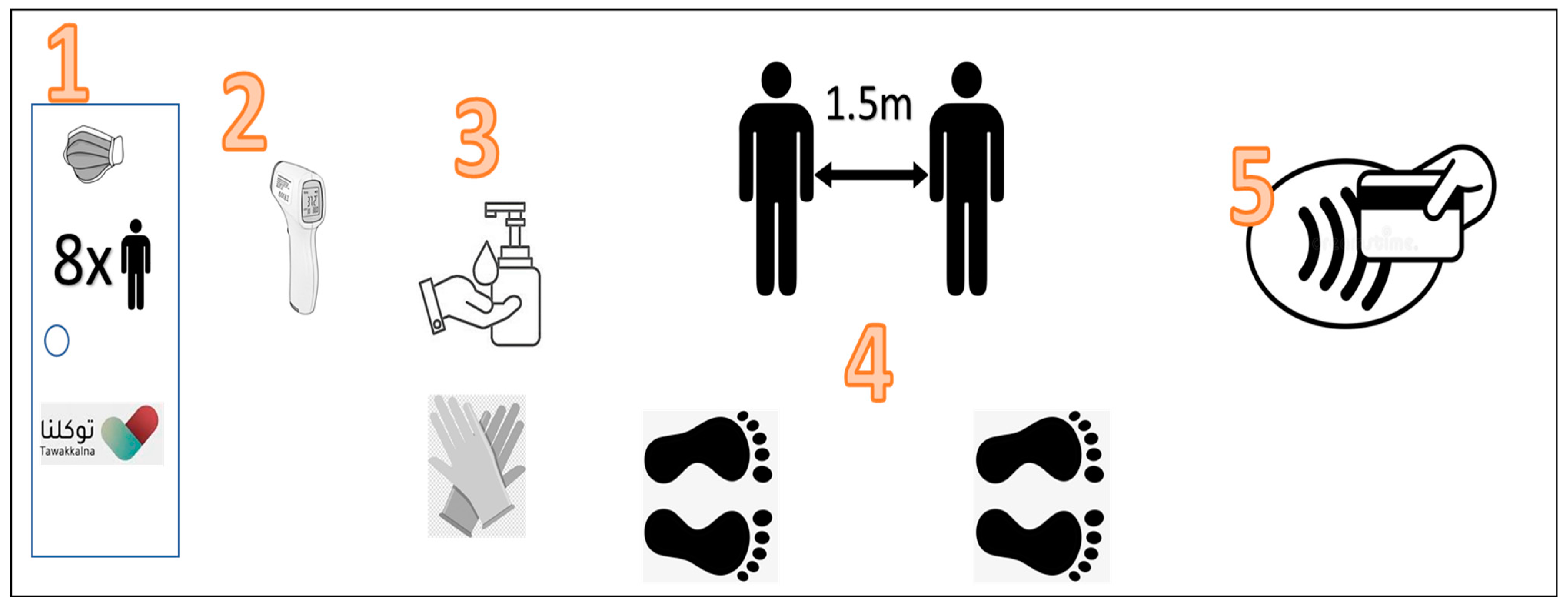
7]. Currently, every closed space such as shops and mosques currently have a predetermined capacity based on their area, which is set to avoid overcrowding. Moreover, mandatory contactless temperature checks were introduced at the entry to every closed establishment, which aim to prevent any symptomatic patient, mainly those with fever, from entering closed buildings. Other measures include the provision of hand-based sanitizers, maintaining social distancing and the wide availability of contactless payment methods, which are summarized in
Figure 5.
The global COVID-19 pandemic is significantly increasing the global burden of tuberculosis (TB) due to disruptions to health services and delays in diagnosis and treatment that may last for years [
8,
9]. Statistically, just before the pandemic, over 4000 people died daily from TB. The latest annual TB report was released in October 2022, which warned that many countries are not on track to meet targets for the ‘End TB Strategy’, which aims to cut TB deaths by 90% and reduce the TB incidence rate by 80% by 2030, compared to a 2015 baseline, thus successfully stopping the disease’s spread [
10]. Before the COVID-19 pandemic, many countries had been making steady progress against TB. Notably, a 9% reduction in incidence was seen between 2015 and 2019, and a 14% drop in deaths occurred during the same period. Interim targets for 2020 include a 20% reduction in incidence rates and a 35% reduction in fatalities [
11]. Nevertheless, there is a fear that TB cases and deaths could rise significantly in countries suffering from a stall in medical services such as India, for example; due to disruptions caused by COVID-19, India’s TB notifications fell by 25%. Regarding the emerging data, the TB disease is not known to put people at a higher risk of COVID-19 infection, but it may put someone at risk of having more severe symptoms [
12].
On the other hand, a hypothesis stated that social distancing might reduce TB incidence. Increased awareness and checkpoints, especially in hot areas such as airports, malls and emergency department, may play a significant role in early detection not only of SARS-CoV-2 but also of other similar droplet/airborne-transmitted pathogens, such as TB [
13]. Accordingly, following the widespread adoption of community mitigation measures to reduce the transmission of SARS-CoV-2, the percentage of US respiratory specimens submitted for positive influenza testing decreased from >20% to 2.3% and has remained historically low regarding interseasonal levels (0.2% versus 1–2%). This season, seasonal influenza (flu) has increased drastically in the US, leading to 15 million illnesses, 150,000 hospitalizations and 9300 deaths [
14]. Data from countries in the Southern Hemisphere also indicate little influenza activity, in spite of other factors such as the sharp reductions in global travel and increased vaccine use, which might have played a role in decreasing the spread.
The COVID-19 pandemic has introduced advanced technological methods to track symptoms (mainly fever) through health observation methods. These methods have linked the symptoms to the people’s health records [
15,
16]. These methods were tested and encouraged for use by public health authorities, such as in South Korea, Singapore and Germany [
17,
18]. In Saudi Arabia, a new application called Tawakkalna was introduced, which is linked to the Ministry of Health’s records. More specifically, it shows the COVID-19 status of a person (healthy, active case of COVID-19, recovered, vaccinated or came in contact with an active case). Such a status is based on the use of COVID-19 PCR test results [
19,
20,
21]. A healthy or vaccinated status in this application has become a prerequisite to entering closed spaces such as mosques and shops (
Figure 5). These novel methods were developed primarily to detect potential COVID-19 cases, especially for people who do not experience severe symptoms, which, thus, prevent its spread to others. However, such measures could be used for other infections besides COVID-19, such as TB.


 ,
, 


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}