
Cope or Perish? Managing Tipping Points in Developing Coping Strategies for Emergency Response during the First Wave of the COVID-19 Outbreak in Europe



Abstract
:1. Introduction
2. Materials and Methods
2.1. A Typology of Emergency Strategies
- If R0 < 1, each existing infection causes less than one new infection. In this case, the disease will decline and eventually cease to exist.
- If R0 equals 1, each existing infection causes at least one new infection. The disease remains stable, without causing an outbreak or an epidemic.
- If R0 > 1, each existing infection causes more than one new infection. The disease will rapidly spread, causing an outbreak or epidemic.
2.2. Research Methodology
2.2.1. Case Study Selection and Case Characteristics
- Mediterranean style: once the seriousness of the virus is recognized, drastic measures are to be taken to remedy the situation. This involves a full lockdown of (nearly) all business and public activity, a closing of the airports and borders, serious bureaucratic administration for people applying for permission to travel, active enforcement of the use of facemasks and heavy penalties for those who violate any of the above policy measures. This response style is typically reflected in the more severe suppression paradigm (see strategy 4 in Table 1) adopted by Italy, Spain and France.
- Continental style: upon the breakout and the apparent undeniability of its severe consequences, policy instruments at the curative end of the spectrum are applied. Light or partial lockdown is announced, social distancing is encouraged, traveling is discouraged and hospital capacity stepped up to the extent possible. On the other hand, some flights are kept in operation, borders are kept open, people maneuver around if they wish to and fines imposed for violations are comparatively low. Germany and Austria are the most notable examples of this style, which is reflected in the modest suppression paradigm adopted by them (see strategy 3 in Table 1). There is variety in this group to the extent that Germany and Austria tend to be a bit stricter than The Netherlands, and therefore can be considered a bridge to the third and last response style.
- Liberal style: in spite of the fact that infection and even death rates in surrounding countries begin their remarkable increase, national and local authorities worry little and brush aside the urge to act. Belief in the possible working of herd immunity is expressed and the idea that the national population is used as a medical testbed for the virus is not found to be an objectionable idea. In the UK and The Netherlands, this idea was firmly expressed and later revoked by the government upon public outcry, although policies remained remarkably carefree until a (comparatively) light lockdown became unavoidable. Sweden was the most extreme case in point, with no lockdown announced at any point, soft advice issued by the public authorities to citizens to “act responsibly” and overwhelming national pride in the government and the population at large for being more tolerant and relaxed than the rest of Europe and incurring less damage. When, further down the road, no other European countries seemed to comprehend and respect the Swedish position, active diplomatic action was undertaken to clarify the approach to neighbors. The style of the UK and The Netherlands resonates with the modest mitigation paradigm (see strategy 2 in Table 1), whereas the Swedish style corresponds to the severe mitigation paradigm (see strategy 1 in Table 1).
2.2.2. Data Analysis and Sources
3. Results
3.1. Italy
3.2. Spain
3.3. France
3.4. The Netherlands
3.5. Germany
3.6. Austria
3.7. United Kingdom
3.8. Sweden
3.9. Case Comparison
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Report of the Who-China Joint Mission on Coronavirus Disease 2019 (COVID-19); World Helath Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Zhou, P.; Yang, X.-L.; Wang, X.-G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.-R.; Zhu, Y.; Li, B.; Huang, C.-L.; et al. A Pneumonia Outbreak Associated with a New Coronavirus of Probable Bat Origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leung, K.; Wu, J.T.; Liu, D.; Leung, G. First-Wave COVID-19 Transmissibility and Severity in China Outside Hubei after Control Measures, and Second-Wave Scenario Planning: A Modelling Impact Assessment. Lancet 2020, 395, 1382–1393. [Google Scholar] [CrossRef]
- Okell, L.C.; Verity, R.; Watson, O.J.; Mishra, S.; Walker, P.; Whittaker, C.; Katzourakis, A.; Donnelly, C.A.; Riley, S.; Ghani, A.C.; et al. Have Deaths from COVID-19 in Europe Plateaued Due to Herd Immunity? Lancet 2020, 395, e110–e111. [Google Scholar] [CrossRef]
- Eades, S.; Eades, F.; McCaullay, D.; Nelson, L.; Phelan, P.; Stanley, F. Australia’s First Nations’ Response to the COVID-19 Pandemic. Lancet 2020, 396, 237–238. [Google Scholar] [CrossRef]
- Salyer, S.J.; Maeda, J.; Sembuche, S.; Kebede, Y.; Tshangela, A.; Moussif, M.; Ihekweazu, C.; Mayet, N.; Abate, E.; Ouma, A.O.; et al. The First and Second Waves of the COVID-19 Pandemic in Africa: A Cross-Sectional Study. Lancet 2021, 397, 1265–1275. [Google Scholar] [CrossRef]
- The Lancet. COVID-19 in the USA: A Question of Time. Lancet 2020, 395, 1229. [Google Scholar]
- Day, M. COVID-19: Italy Confirms 11 Deaths as Cases Spread from North. BMJ 2020, 368, m757. [Google Scholar] [CrossRef] [Green Version]
- ECDC. Novel Coronavirus Disease 2019 (COVID-19) Pandemic: Increased Transmission in the EU/EEA and the UK—Sixth Update—12 March 2020; European Centre for Disease Prevention and Control: Stockholm, Sweden, 2020.
- Kwok, K.O.; Lai, F.; Wei, W.I.; Wong, S.Y.S.; Tang, J.W.T. Herd Immunity—Estimating the Level Required to Halt the COVID-19 Epidemics in Affected Countries. J. Infect. 2020, 80, e32–e33. [Google Scholar] [CrossRef]
- Poljanšek, K.; Marin Ferrer, M.; De Groeve, T.; Clark, I. (Eds.) Science for Disaster Risk Management 2017: Knowing Better and Losing Less; European Commission: Luxembourg, 2017. [Google Scholar]
- Tàbara, J.D.; Frantzeskaki, N.; Hölscher, K.; Pedde, S.; Kok, K.; Lamperti, F.; Christensen, J.H.; Jäger, J.; Berry, P. Positive Tipping Points in a Rapidly Warming World. Curr. Opin. Environ. Sustain. 2018, 31, 120–129. [Google Scholar] [CrossRef]
- Haasnoot, M.; Kwakkel, J.H.; Walker, W.E.; ter Maat, J. Dynamic Adaptive Policy Pathways: A Method for Crafting Robust Decisions for a Deeply Uncertain World. Glob. Environ. Chang. 2013, 23, 485–498. [Google Scholar] [CrossRef] [Green Version]
- Werners, S.E.; Pfenninger, S.; van Slobbe, E.; Haasnoot, M.; Kwakkel, J.H.; Swart, R.J. Thresholds, Tipping and Turning Points for Sustainability under Climate Change. Curr. Opin. Environ. Sustain. 2013, 5, 334–340. [Google Scholar] [CrossRef]
- Paul, L.D.; Street, E.J.; Leslie, T.F.; Yang, Y.T.; Jacobsen, K.H. Complexity of the Basic Reproduction Number (R(0)). Emerg. Infect. Dis. 2019, 25, 1–4. [Google Scholar]
- Gillespie, C. Coronavirus Experts Want to ‘Flatten the Curve’ to Fight the Pandemic—Here’s What That Means. Available online: https://www.health.com/condition/infectious-diseases/coronavirus/flatten-the-curve-meaning (accessed on 13 March 2020).
- Hofstede, G.; Hofstede, G.-J.; Minkov, M. Cultures and Organizations—Software of the Mind: Intercultural Cooperation and Its Importance for Survival; Mc Graw-Hill: New York, NY, USA, 2010. [Google Scholar]
- Andrea, R.; Remuzzi, G. COVID-19 and Italy: What Next? Lancet 2020, 395, 1225–1228. [Google Scholar]
- El País. Coronavirus Deaths Continue to Rise in Spain, with a Record 838 in 24 Hours. Available online: https://english.elpais.com/society/2020-03-29/coronavirus-deaths-continue-to-rise-in-spain-with-new-record-838-in-last-24-hours.html (accessed on 29 March 2020).
- Clément, M.; Roux, J.; Crépey, P. COVID-19: Forecasting Short Term Hospital Needs in France. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Van Nederland, H. Tekort Aan Ic-Bedden Dreigt: Nog Maar Een Paar Plekken Vrij Voor Coronapatiënten. Available online: https://www.hartvannederland.nl/nieuws/2020/nog-maar-paar-ic-bedden-vrij/ (accessed on 28 March 2020).
- AFP. Germany Ramps up Intensive Care and Hospital Capacity in Coronavirus Fight. Available online: https://www.thelocal.de/20200318/germany-ramps-up-intensive-care-and-hospital-capacity-in-coronavirus-fight (accessed on 18 March 2020).
- Wolf, B. The Coronavirus in Austria & Vienna|A New Normality. Available online: https://metropole.at/coronavirus-in-austria/ (accessed on 7 April 2020).
- The Coronavirus in Austria & Vienna|What Happened in March. Available online: https://metropole.at/coronavirus-in-austria-march/ (accessed on 31 March 2020).
- Aftonbladet. Tabell: Här Finns Alla Platser På Intensiven. Available online: https://www.aftonbladet.se/nyheter/a/AdMPyr/sa-manga-platser-pa-intensiven-har-ditt-sjukhus (accessed on 1 May 2020).
- ECDC. Data on Testing for Covid-19 by Week and Country. Available online: https://www.stelios67pi.eu/older/20210604.html (accessed on 2 February 2021).
- Worldbank. Gdp (Current Us$). 2020. Available online: https://data.worldbank.org/indicator/SP.POP.TOTL (accessed on 2 February 2021).
- Worldbank. Gdp Growth (Annual %). 2020. Available online: https://data.worldbank.org/indicator/SP.POP.TOTL (accessed on 2 February 2021).
- Worldbank. Current Health Expenditure (% of Gdp). 2020. Available online: https://data.worldbank.org/indicator/SP.POP.TOTL (accessed on 2 February 2021).
- Worldbank. Total Population Database. 2020. Available online: https://data.worldbank.org/indicator/SP.POP.TOTL (accessed on 2 February 2021).
- Worldbank. Population Ages 65 and above, Total. 2020. Available online: https://data.worldbank.org/indicator/SP.POP.TOTL (accessed on 2 February 2021).
- Worldbank. Population Density (People Per Sq. Km of Land Area). 2020. Available online: https://data.worldbank.org/indicator/SP.POP.TOTL (accessed on 2 February 2021).
- Worldbank. Urban Population (% of Total Population). 2020. Available online: https://data.worldbank.org/indicator/SP.POP.TOTL (accessed on 2 February 2021).
- Paul, C.; Brown, B.; Majomi, P. Professional Identity in Community Mental Health Nursing: A Thematic Analysis. Int. J. Nurs. Stud. 2008, 45, 1055–1063. [Google Scholar]
- Valerie, M.; Theuns, P.; Erstad, I.; Bernheim, J. The Best and Worst Times of Life: Narratives and Assessments of Subjective Well-Being by Anamnestic Comparative Self Assessment (Acsa) in the Eastern Cape, South Africa. Soc. Indic. Res. 2008, 89, 1–22. [Google Scholar]
- Langellier, K.M.; Peterson, E.E. Performing Narrative: The Communicative Practice of Storytelling; Temple University Press: Philadelphia, PA, USA, 2004; pp. 7–31. [Google Scholar]
- Van der Voorn, T.; Quist, J. Analysing the Role of Visions, Agency, and Niches in Historical Transitions in Watershed Management in the Lower Mississippi River. Water 2018, 10, 1845. [Google Scholar] [CrossRef] [Green Version]
- Nicholas, P. Rational Choice, Structural Context, and Increasing Returns:A Strategy for Analytic Narrative in Historical Sociology. Sociol. Methods Res. 2005, 33, 349–382. [Google Scholar]
- Denzin, N.K. The Research Act in Sociology; Aldine: Chicago, IL, USA, 1970. [Google Scholar]
- Bryman, A. Social Research Methods; Oxford University Press: Oxford, UK, 2001. [Google Scholar]
- Chiara, S. Coronavirus: Primi Due Casi in Italia. Available online: https://www.corriere.it/cronache/20_gennaio_30/coronavirus-italia-corona-9d6dc436-4343-11ea-bdc8-faf1f56f19b7.shtml?refresh_ce-cp (accessed on 6 April 2020).
- Anzolin, E.; Amante, A. First Italian Dies of Coronavirus as Outbreak Flares in North. Available online: https://www.reuters.com/article/us-china-health-italy-idUSKBN20F0UI (accessed on 21 February 2020).
- Coronavirus Outbreak Grows in Northern Italy, 16 Cases Reported in One Day. Available online: https://www.reuters.com/article/us-china-health-italy/coronavirus-outbreak-grows-in-northern-italy-16-cases-reported-in-one-day-idUSKBN20F0UI (accessed on 21 February 2020).
- Ravizza, S. Coronavirus: Primi Casi a Milano. Cosa Sappiamo Dei Nuovi Contagi in Lombardia, Veneto E Piemonte [Coronavirus: First Case in Milan. What We Know About New Infections in Lombardy, Veneto and Piemont]. Available online: https://www.corriere.it/cronache/20_febbraio_22/coronavirus-italia-nuovi-contagi-lombardia-veneto-245e72d4-5540-11ea-8418-2150c9ca483e.shtml (accessed on 6 April 2020).
- Ananasso, A.; de Stabile, E.; Gagliardi, G.; Matteucci, P. Coronavirus in Italia: Aggiornamento Ora Per Ora. La Repubblica (in Italian). 22 February 2020. Available online: https://www.repubblica.it/cronaca/2020/02/22/news/coronavirus_in_italia_aggiornamento_ora_per_ora-249241616/ (accessed on 6 April 2020).
- Riccioni, L.; Bertolini, G.; Giannini, A.; Vergano, M.; Gristina, G.; Livigni, S.; Petrini, F. Raccomandazioni di etica clinica per l’ammissione a trattamenti intensivi e per la loro sospensione, in condizioni eccezionali di squilibrio tra necessità e risorse disponibili. Recenti Progress. Med. 2020, 111, 207–211. [Google Scholar]
- BBC. Coronavirus: Northern Italy Quarantines 16 Million People. Available online: https://www.bbc.com/news/world-middle-east-51787238 (accessed on 8 March 2020).
- News BBC. All of Italy to Be Placed on Coronavirus Lockdown. Available online: https://www.bbc.com/news/world-europe-51810673 (accessed on 9 March 2020).
- Chico, H.; Loveday, M. Italy Ramps up Coronavirus Lockdown, Merkel Warns Virus Could Infect Two-Thirds of Germany. Available online: https://www.washingtonpost.com/world/europe/merkel-coronavirus-germany/2020/03/11/e276252a-6399-11ea-8a8e-5c5336b32760_story.html (accessed on 6 April 2020).
- Safi, M.; Giuffrida, A.; Farrer, M. Coronavirus: Italy Bans Any Movement inside Country as Toll Nears 5500. Available online: https://www.theguardian.com/world/2020/mar/22/italian-pm-warns-of-worst-crisis-since-ww2-as-coronavirus-deaths-leap-by-almost-800 (accessed on 6 April 2020).
- Fortuna, G. Pm Conte Dismisses Idea That Italy Will Resort to Eurozone Bailout Fund. Available online: https://www.euractiv.com/section/health-consumers/short_news/italy-update-covid-19/1441629/ (accessed on 13 March 2020).
- University Johns Hopkins. Coronavirus Covid-19 Global Cases by the Center for Systems Science and Engineering (Csse) at Johns Hopkins. Available online: https://gisanddata.maps.arcgis.com/apps/opsdashboard/index.html#/bda7594740fd40299423467b48e9ecf6 (accessed on 6 April 2020).
- Linde, P. Sanidad Confirma En La Gomera El Primer Caso De Coronavirus En España. Available online: https://elpais.com/sociedad/2020/01/31/actualidad/1580509404_469734.html (accessed on 6 April 2020).
- Colman, A. Spain Recorded 950 Coronavirus Deaths in a Day, the Highest Single-Day Toll of Any Country. Available online: https://www.businessinsider.com/coronavirus-spain-950-deaths-one-day-most-of-any-country-2020-4 (accessed on 6 April 2020).
- Abbonati, A. Coronavirus, Positivi Due Italiani a Tenerife. Mille Persone Nell’hotel in Quarantena. Available online: https://www.repubblica.it/esteri/2020/02/25/news/coronavirus_contagiati_in_italia-249569108/ (accessed on 6 April 2020).
- de Sanidad, M. Actualización Nº 67. Enfermedad Por El Coronavirus (COVID-19). Edited by Centro de Coordinación de Alertas y Emergencias Sanitarias. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/documentos/Actualizacion_67_COVID-19.pdf. (accessed on 20 April 2020).
- Gallardo, C. Spain Unveils €200b Package to Combat Virus Downturn. Available online: https://www.politico.eu/article/spain-200-billion-euros-package-virus-downturn/ (accessed on 17 March 2020).
- Politico. How Europe Is Responding to the Coronavirus Pandemic Politico’s Country-by-Country Guide to Health, Travel and Economic Measures. Available online: https://www.politico.eu/article/how-europe-is-responding-to-the-coronavirus-pandemic/ (accessed on 13 March 2020).
- van Landbouw, M.; en Voedselkwaliteit, N. Spanish Government Greenlights €200 Billion to Mitigate COVID-19 Impact on Economy. Available online: https://www.agroberichtenbuitenland.nl/actueel/nieuws/2020/03/19/spanish-government-greenlights-€200-billion-to-mitigate-covid-19-impact-on-economy (accessed on 19 March 2020).
- Lee, Y.N.; Ellyatt, H. Spain’s Cases Surpass 11,000; Iran Temporarily Frees 85,000 Prisoners. Available online: https://www.cnbc.com/2020/03/17/coronavirus-latest-updates.html (accessed on 16 March 2020).
- Euractiv. State of Alarm to Be Extended; Measures Appear to Be Paying Off. Available online: https://www.euractiv.com/section/coronavirus/short_news/spain-update-covid-19/ (accessed on 13 March 2020).
- Threadgould, J. Spain Passes China COVID-19 Death Toll, 2nd Behind Italy. Available online: https://www.laprensalatina.com/spain-passes-china-covid-19-death-toll-2nd-behind-italy/ (accessed on 25 March 2020).
- Gotev, G. Spanish Doctors, Nurses Demand Action after Coronavirus Cases Soar. Available online: https://www.euractiv.com/section/coronavirus/news/spanish-doctors-nurses-demand-action-after-coronavirus-cases-soar/ (accessed on 25 March 2020).
- RKI. Situation Report of the Robert Koch Institute Covid-19. 31/03/2020—Updated Status for German. Robert Koch Inst. 2020. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Situationsberichte/2020-04-06-en.pdf?__blob=publicationFile (accessed on 2 February 2021).
- Jones, S.; Kassam, A. Spain Defends Response to Coronavirus as Global Cases Exceed 500,000. Available online: https://www.theguardian.com/world/2020/mar/26/spanish-coronavirus-deaths-slow-as-world-nears-500000-cases (accessed on 26 March 2020).
- Marcos, J. Spanish Government Tightens Lockdown to Include All Non-Essential Workers. Available online: https://english.elpais.com/politics/2020-03-28/spanish-government-tightens-lockdown-to-include-all-non-essential-workers.html (accessed on 29 March 2020).
- The Straits Times. Wuhan Virus: France Confirms Fourth Case of Coronavirus in Elderly Chinese Tourist. Available online: https://www.straitstimes.com/world/europe/france-confirms-fourth-case-of-coronavirus-in-elderly-chinese-tourist (accessed on 29 January 2020).
- BBC. Coronavirus: First Death Confirmed in Europe. Available online: https://www.bbc.com/news/world-europe-51514837 (accessed on 15 February 2020).
- The Connexion. Stage 3 Covid-19 Epidemic ‘Inevitable’ in France. Available online: https://wuhanupdate.com/health/stage-3-covid-19-epidemic-inevitable-in-france-84060864 (accessed on 7 March 2020).
- Euractiv. France ‘Headed for Worst Year of Economic Recession since End of World War Ii’. Available online: https://www.euractiv.com/section/health-consumers/short_news/france-update-covid-19/ (accessed on 13 March 2020).
- The Local France. France Bans Gatherings of More Than 100 People as Coronavirus Death Toll Rises. Available online: https://www.thelocal.fr/20200313/france-bans-gatherings-of-over-100-people-to-fight-coronavirus-pandemic (accessed on 13 March 2020).
- Barbiere, C. After Declaring ‘War’ on Covid-19, France Readies Measures to Uphold Economy. Available online: https://www.euractiv.com/section/coronavirus/news/after-declaring-war-on-covid-19-france-readies-measures-to-uphold-economy/ (accessed on 18 March 2020).
- RFI. France to Step up Coronavirus Testing Methods as Death Toll Climbs. Available online: http://www.rfi.fr/en/france/20200318-france-step-up-coronavirus-new-test-methods-death-toll-climbs-covid-19-priority-risk-elderly-symptoms (accessed on 18 March 2020).
- Reuters. Twitter, “Dutch Prime Minster Mark Rutte Advised People to Not Shake Hands at a #Coronavirus Press Conference on Monday, but Went on to Do Exactly that Moments Later”. Available online: https://twitter.com/Reuters/status/1237342436533420034 (accessed on 10 March 2020).
- van Nederland, H. Geen Lockdown, Wel Scherpere Corona-Maatregelen: Boetes Voor Geen Afstand Houden. Available online: https://www.hartvannederland.nl/nieuws/2020/persconferentie-kabinet-coronacrisis/ (accessed on 7 April 2020).
- NOS. Ic-Arts Gommers: Binnen Een Week Moeten 2400 Bedden Gereed Zijn. Available online: https://nos.nl/artikel/2328827-ic-arts-gommers-binnen-een-week-moeten-2400-bedden-gereed-zijn.html (accessed on 7 April 2020).
- Pieters, J. Icu Staff Stressed and Overworked in Coronacrisis. Available online: https://nltimes.nl/2020/04/01/icu-staff-stressed-overworked-coronacrisis (accessed on 7 April 2020).
- van der Aa, E.; Bolt, R. Ic-Voorzitter Gommers Vreest ‘Italiaanse Toestanden’. Available online: https://www.ad.nl/politiek/ic-voorzitter-gommers-vreest-italiaanse-toestanden~a99030f3/ (accessed on 7 April 2020).
- Eck, D. Dutch Government Extends ‘Intelligent Lockdown’, Proposes Eu Emergency Corona-Fund without Conditions. Available online: https://www.euractiv.com/section/coronavirus/short_news/netherlands-update-covid-19/ (accessed on 7 April 2020).
- NOS. Van Dissel: Volhouden Beperkende Maatregelen Is Cruciaal. Available online: https://nos.nl/artikel/2329035-van-dissel-volhouden-beperkende-maatregelen-is-cruciaal.html (accessed on 1 April 2020).
- Spiegel, D. Bayerische Behörden Bestätigen Ersten Fall in Deutschland. 2020. Available online: https://www.spiegel.de/wissenschaft/medizin/corona-virus-erster-fall-in-deutschland-bestaetigt-a-19843b8d-8694-451f-baf7-0189d3356f99 (accessed on 7 April 2020).
- Anderl, S. Fallsterblichkeitsrate: Wie Tödlich Ist Covid-19 in Deutschland? Available online: https://www.faz.net/aktuell/politik/inland/wie-toedlich-ist-das-coronavirus-in-deutschland-16711071.html (accessed on 4 April 2020).
- Die Rheinpfalz. Corona-Virus: Bundesregierung Hält Risiko Für Deutschland Sehr Gering. Available online: https://www.rheinpfalz.de/panorama_artikel,-corona-virus-bundesregierung-hält-risiko-für-deutschland-sehr-gering-_arid,1579340.html (accessed on 27 January 2020).
- O’Brien, C. Us Commander: Coronavirus Could Restrict Troop Travel in Germany. Available online: https://www.politico.eu/article/us-commander-says-troop-travel-in-germany-could-be-restricted-amid-coronavirus-outbreak/ (accessed on 25 February 2020).
- Heinsberg, K. Aktuelles Aus Dem Kreishaus. Available online: https://www.kreis-heinsberg.de/aktuelles/aktuelles/?pid=5136 (accessed on 29 February 2020).
- Abendblatt, H. Coronavirus: Zwei Tote in Deutschland–Italien Sperrt Das Ganze Land. Available online: https://www.abendblatt.de/vermischtes/article228637475/Coronavirus-Corona-News-Live-Ticker-Covid-19-Tote-in-Deutschland-1164-Infektionen.html (accessed on 9 March 2020).
- Die Welt. Bundesregierung Legt Krisen-Leitlinien Fest–Merkel Für Vorgehen Mit Maß Und Mitte. Available online: https://www.welt.de/vermischtes/article206221797/Coronavirus-Bundesregierung-legt-Krisen-Leitlinien-fest-Merkel-fuer-Vorgehen-mit-Mass-und-Mitte.html (accessed on 29 February 2020).
- RKI. Sars-Cov-2: Fallzahlen in Deutschland, China Und Weltweit. Available online: http://web.archive.org/web/20200303083152/https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Fallzahlen.html (accessed on 2 March 2020).
- ARD. Jeder Muss Seinen Beitrag Leisten. Available online: https://www.tagesschau.de/inland/coronavirus-spahn-rki-105.html (accessed on 9 March 2020).
- Financial Times. Germany Wields ‘Bazooka’ in Fight against Coronavirus. Available online: https://www.ft.com/content/1b0f0324-6530-11ea-b3f3-fe4680ea68b5 (accessed on 13 March 2020).
- Carrel, P. Germany Discussing Its Medical Export Restrictions with Eu Partners. Available online: https://www.reuters.com/article/us-health-coronavirus-germany-ventilator/germany-discussing-its-medical-export-restrictions-with-eu-partners-idUSKBN2101IU (accessed on 13 March 2020).
- Bartsch, M.; Blech, J.; Bruhns, A.; Eberle, L.; Elger, K.; Feldenkirchen, M.; Gnirke, K.; Großbongardt, A.; Gude, H.; Hackenbroch, V.; et al. Are Hospitals Ready for the Coming Wave of Corona Cases? Available online: https://www.spiegel.de/international/germany/the-big-wave-of-corona-cases-will-hit-german-hospitals-in-10-to-14-days-a-45cd754c-e179-4dbb-8caf-8f6074e641cf (accessed on 21 March 2020).
- BBC. Coronavirus: Germany to Impose Border Controls over Coronavirus. Available online: https://www.bbc.com/news/world-europe-51897069 (accessed on 15 March 2020).
- Mappes, F.W. Erster Fall Im Landkreis Bad Dürkheim: Corona-Virus in Wachenheim Bestätigt. Available online: https://www.wochenblatt-reporter.de/bad-duerkheim/c-lokales/corona-virus-in-wachenheim-bestaetigt_a176479 (accessed on 4 March 2020).
- ARD. Bundesweite Ausgangssperre Rückt Näher. Available online: https://www.tagesschau.de/inland/corona-lockdown-nach-weihnachten-101.html (accessed on 20 March 2020).
- Marcus, I. Germany Steps up Fight against Coronavirus. Available online: https://berlinspectator.com/2020/03/11/germany-steps-up-fight-against-coronavirus/ (accessed on 11 March 2020).
- Stam, C.; Grüll, P.; Lawton, S. Progress in Germany as the Number of New Infections Decrease. Available online: https://www.euractiv.com/section/health-consumers/short_news/germany-coronavirus-update/ (accessed on 13 March 2020).
- von Lars, W. Ischgl War Die Heimliche Virus-Drehscheibe in Europa. Available online: https://www.t-online.de/nachrichten/panorama/id_87525436/coronavirus-von-ischgl-verbreitete-sich-covid-19-in-ganz-europa.html (accessed on 4 December 2020).
- Grüll, P. How an Austrian Ski Paradise Became a Covid-19 Hotspot. Available online: https://www.euractiv.com/section/coronavirus/news/ischgl-oesterreichisches-skiparadies-als-corona-hotspot/ (accessed on 20 March 2020).
- Bazaraa, D. Coronavirus: Ibiza of the Alps’ Ski Village Blamed for Hundreds of Cases in Europe. Available online: https://www.mirror.co.uk/news/world-news/coronavirus-ibiza-alps-ski-village-21739316 (accessed on 23 March 2020).
- Groendahl, B. Austria Closes Passage from Italy without Health Clearance. Available online: https://www.bloomberg.com/news/articles/2020-03-10/austria-closes-border-for-italians-without-health-clearance (accessed on 10 March 2020).
- Sebastiankurz. Mein Appell Ist in Der Derzeitigen Situation Klar: Nehmen Sie Die Situation Ernst Und Glauben Sie Den Beschwichtigungen Nicht! Nur Gemeinsam Können Wir Die Ausbreitung Des Coronavirus Verlangsamen. 2020. Available online: https://www.wienerzeitung.at/nachrichten/politik/oesterreich/2054402-Coronavirus-Parlament-beschliesst-Gesetze-fuer-Massnahmen.html (accessed on 4 March 2020).
- Grüll, P. Austria’s Government Presents Covid-19 Exit Schedule. Available online: https://www.euractiv.com/section/coronavirus/news/austrias-government-presents-covid-19-exit-schedule/ (accessed on 6 April 2020).
- Grüll, P.; Lawton, S. Government Presents First Steps of Exit Strategy, Wants to Ease Lockdown Ahead of Others. Available online: https://www.euractiv.com/section/health-consumers/short_news/austria-update-covid-19/1441621/ (accessed on 13 March 2020).
- Knolle, K. Austria Bets on Mass Testing to Manage Coronavirus Spread. Available online: https://www.reuters.com/article/us-health-coronavirus-austria/austria-bets-on-mass-testing-to-manage-coronavirus-spread-idUSKBN21B1DH (accessed on 24 March 2020).
- Boseley, S.; Campbell, D.; Murphy, S. First British National to Contract Coronavirus Had Been in Singapore. Patient Diagnosed in Brighton and Taken to London Is Third Confirmed Case in the UK. Available online: https://www.theguardian.com/world/2020/feb/06/third-person-in-uk-confirmed-as-having-coronavirus (accessed on 6 February 2020).
- Mohdin, K.; Willsher, A.; Madrid, A.; Jones, S. Coronavirus: British Nine-Year-Old in Hospital in France. Available online: https://www.theguardian.com/world/2020/feb/08/coronavirus-five-new-cases-in-france-are-british-nationals (accessed on 26 February 2020).
- BBC. Coronavirus: Brighton Gp Practice Closes after Staff Member Tests Positive. Available online: https://www.bbc.com/news/uk-51447761 (accessed on 11 February 2020).
- Elisabeth, M. Coronavirus: Nhs Staff Get Power to Keep Patients in Isolation as UK Declares Serious Threat. BMJ 2020, 368, 550. [Google Scholar]
- O’Regan, E.; Doyle, K.; Edwards, M.; Bray, A. Coronavirus Ireland: Passengers Who Travelled with Northern Irish Patient Traced in Bid to Prevent Outbreak. Available online: https://www.independent.ie/world-news/coronavirus/coronavirus-ireland-passengers-who-travelled-with-northern-irish-patient-traced-in-bid-to-prevent-outbreak-38997601.html (accessed on 28 March 2020).
- England Department of Health and Social Care and Public Health. Coronavirus (COVID-19): Latest Information and Advice. Available online: https://www.gov.uk/guidance/coronavirus-covid-19-information-for-the-public (accessed on 24 January 2020).
- BBC. Coronavirus Could Spread ‘Significantly’—Pm. Available online: https://www.bbc.com/news/uk-51708550 (accessed on 2 March 2020).
- Russell, P. New Coronavirus: UK Public Health Campaign Launched. Available online: https://www.medscape.com/viewarticle/924664 (accessed on 3 February 2020).
- Ross, T.; Donaldson, K.U.K. Abandons Effort to Contain Virus as 10,000 May Be Infected. Available online: https://www.bloomberg.com/news/articles/2020-03-12/u-k-abandons-effort-to-contain-virus-moves-to-delay-the-worst (accessed on 12 March 2020).
- BBC. Coronavirus: Britons Returning from Northern Italy Told to Self-Isolate. Available online: https://www.bbc.com/news/uk-51625733 (accessed on 26 February 2020).
- Rayner, G. Government Takes over Heathrow Hotel to House Quarantined Travellers as They Arrive Travellers Are Being Advised to Board Flights Back to Their Country of Origin If They Are Not Prepared to Self-Isolate. Available online: https://www.telegraph.co.uk/news/2020/03/10/government-takes-heathrow-hotel-house-quarantined-travellers/ (accessed on 10 March 2020).
- Knapton, S. Hospitals Could Run Short of Oxygen ‘within Hours’ as Coronavirus Escalates, Specialists Warn ‘Overwhelmed’ Service Also in Danger of Running out of Medication and Beds as Expected Cases Exceed One Million. Available online: https://www.telegraph.co.uk/news/2020/03/15/hospitals-could-run-short-oxygen-within-hours-pandemic-escalates/ (accessed on 15 March 2020).
- Flaxman, S.; Mishra, S.; Gandy, A. Estimating the Number of Infections and the Impact of Non-Pharmaceutical Interventions on Covid-19 in 11 European Countries. Imp. Coll. Lond. 2020, 584, 257–261. [Google Scholar] [CrossRef] [PubMed]
- Nair, A. Coronavirus: London Worst Affected by Outbreak-621 Cases, 25 Deaths. Available online: https://news.sky.com/story/uk-coronavirus-cases-reach-1-950-up-407-in-24-hours-11958875 (accessed on 18 March 2020).
- Ministry of Housing, Communities & Local Government. Coronavirus (COVID-19): Guidance for Local Government Guidance for Local Councils during the Coronavirus (COVID-19) Outbreak. Available online: https://www.gov.uk/guidance/coronavirus-covid-19-guidance-for-local-government (accessed on 17 March 2020).
- MP, HM Treasury and The Rt Hon Rishi Sunak. The Chancellor Rishi Sunak Provides an Updated Statement on Coronavirus the Chancellor Unveiled Today (20 March) a Further Series of Measures to Support People, Jobs and Businesses. Available online: https://www.gov.uk/government/speeches/the-chancellor-rishi-sunak-provides-an-updated-statement-on-coronavirus (accessed on 20 March 2020).
- BBC. Coronavirus: Tens of Thousands of Retired Medics Asked to Return to Nhs. Available online: https://www.bbc.com/news/uk-51969104 (accessed on 20 March 2020).
- Neslen, A. UK Foreign Secretary Appointed ‘Designated Survivor’ If Boris Johnson Catches COVID-19. Available online: https://www.politico.eu/article/uk-foreign-secretary-appointed-designated-survivor-if-boris-johnson-catches-covid-19/ (accessed on 22 March 2020).
- Fox, B. London–Government Seeks 250,000 Nhs Volunteer Force. Available online: https://www.euractiv.com/section/all/short_news/london-government-seeks-250000-nhs-volunteer-force/ (accessed on 25 March 2020).
- Triggle, N. Coronavirus: Is the Nhs Ready for the Surge in Cases? Available online: https://www.bbc.com/news/health-51714498 (accessed on 3 April 2020).
- Schraer, R. Coronavirus: Excel Centre Planned as Nhs Field Hospital. Available online: https://www.bbc.com/news/health-52018477 (accessed on 24 March 2020).
- BBC. Coronavirus: Thousands of Extra Hospital Beds and Staff. Available online: https://www.bbc.com/news/uk-51989183 (accessed on 21 March 2020).
- Coronavirus: UK Deaths Rise by More Than 100 in a Day. Available online: https://www.bbc.com/news/uk-52056534 (accessed on 26 March 2020).
- Zimmermann, B.; Fiske, A.; McLennan, S.; Sierawska, A.; Hangel, N.; Buyx, A. Motivations and Limits for COVID-19 Policy Compliance in Germany and Switzerland. Int. J. Health Policy Manag. 2021. [Google Scholar] [CrossRef] [PubMed]
- Gibney, E. Whose Coronavirus Strategy Worked Best? Scientists Hunt Most Effective Policies. Nature 2020, 581, 15–16. [Google Scholar] [CrossRef] [PubMed]
- Prosun, B.; Kumar, M.; Islam, M.T.; Haque, R.; Chakraborty, S.; Ahmad, A.; Niazi, N.K.; Cetecioglu, Z.; Nilsson, D.; Ijumulana, J.; et al. Prevalence of Sars-Cov-2 in Communities through Wastewater Surveillance—A Potential Approach for Estimation of Disease Burden. Curr. Pollut. Rep. 2021, 7, 160–166. [Google Scholar]
- Van der Voorn, T.; Caroline van den, B.; Prosun, B.; Jaco, Q. Never Waste a Crisis: Drawing First Lessons from the COVID-19 Pandemic to Tackle the Water Crisis. ACS EST Water 2020, 1, 8–10. [Google Scholar] [CrossRef]
- Aaron, B.; North, D.; Ahmad, A.; Ahmed, W.; Alm, E.; Been, F.; Bhattacharya, P.; Bijlsma, L.; Boehm, A.B.; Brown, J.; et al. Wastewater-Based Epidemiology: Global Collaborative to Maximize Contributions in the Fight against COVID-19. Environ. Sci. Technol. 2020, 54, 7754–7757. [Google Scholar]
- Clement, D. Estimating Economic Impact of Covid-19. Summary of Minneapolis Fed Staff Report: “What Will Be the Economic Impact of COVID-19 in the U.S? Rough Estimates of Disease Scenarios. Available online: https://www.minneapolisfed.org/article/2020/estimating-economic-impact-of-covid-19 (accessed on 19 March 2020).
- EUR. The Impact of Covid-19 on the Dutch Economy. Bas Jacobs, Sijbren Cnossen Professor of Public Economics at Erasmus School of Economics, Discusses the Impact of the Coronavirus on the Dutch Economy on Npo Radio 1 Programme Stax & Toine. NPO Radio1. Available online: https://www.eur.nl/en/news/impact-covid-19-dutch-economy (accessed on 20 March 2020).


{kind=link}
{kind=link}
{kind=link}
| Strategies for Emergency Response | (1) Mitigation without Social Restrictions | (2) Mitigation by Moderate Social Restrictions | (3) Suppression by Severe Social Restrictions | (4) Suppression by Partial Lockdown | (5) Suppression by Full Lockdown |
|---|---|---|---|---|---|
| Death and infection rate | Very high number of reported deaths Very high number of reported infections | Low number of reported deaths Low number of reported infections | Moderate number of reported deaths Moderate number of reported infections | High number of reported deaths High number of reported infections | Very high number of reported deaths Very high number of reported infections |
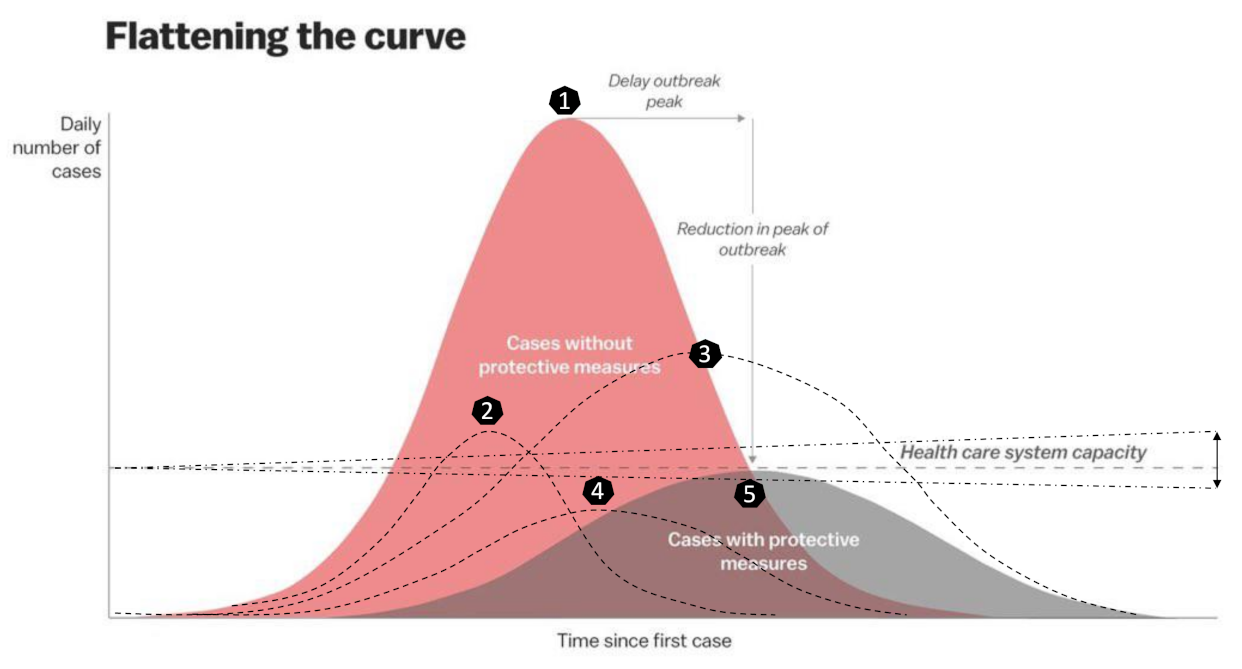
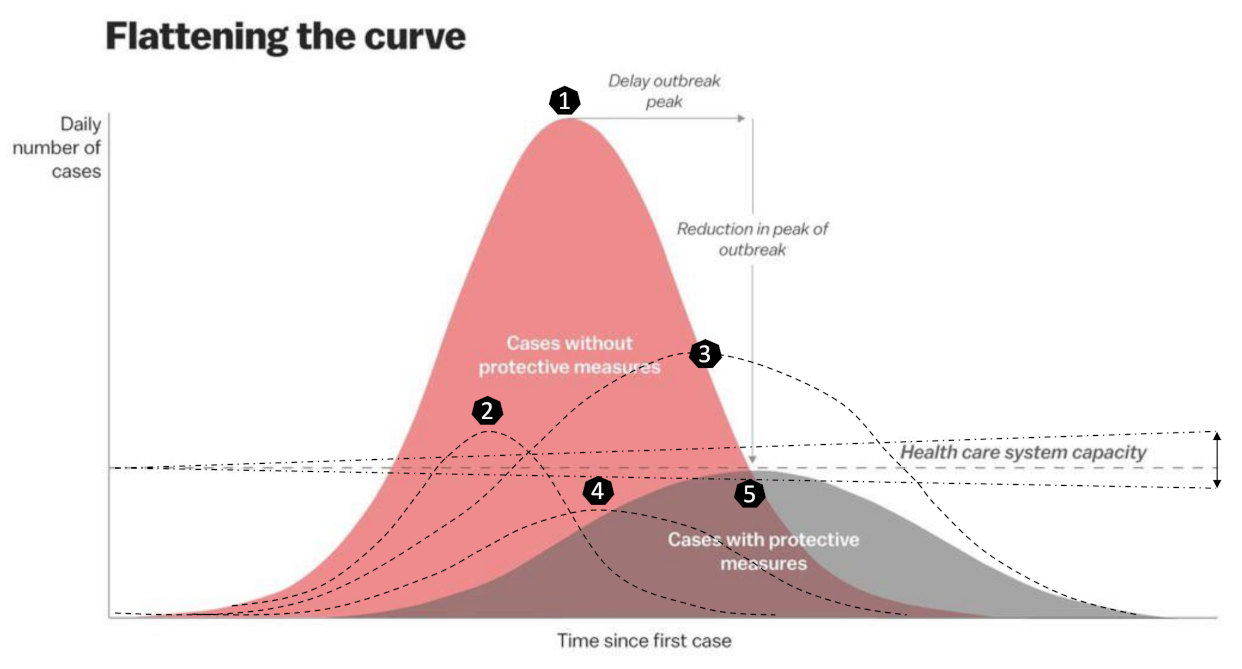
| Infection trajectory (Figure 2) | 1 R0 ≥ 3 | 4 and 5 R0 ≤ 1 | 2 1 ≤ R0 ≤ 2 | 3 2 ≤ R0 ≥ 3 | 1 R0 ≥ 3 |
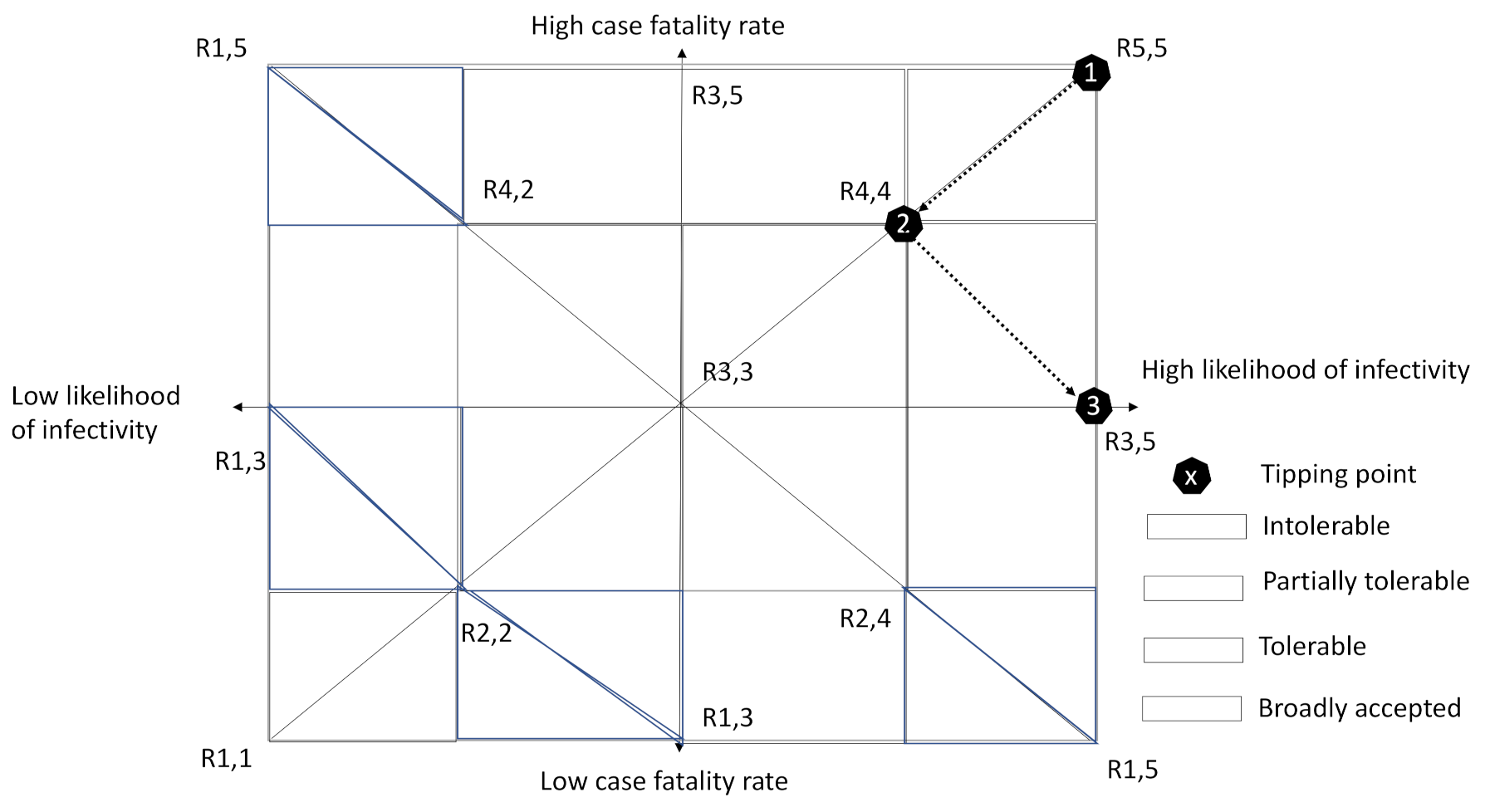
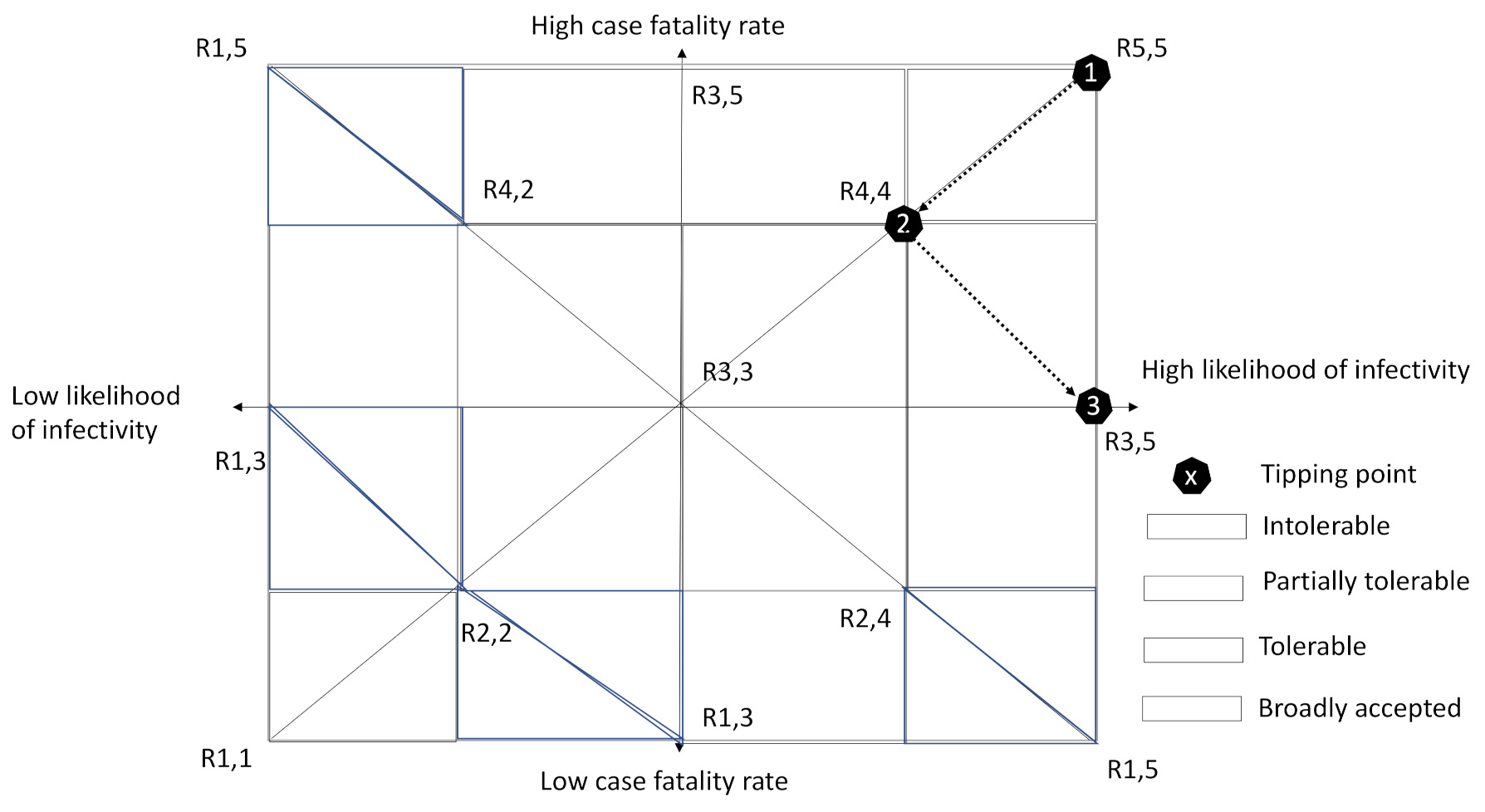
| Risk level (Figure 1) | Red | Green | Yellow | Orange | Red |
| Control Paradigm | Herd immunity | Controlled herd immunity | Targeted containment | Partial containment | Full containment |
| Measures | Business as usual | Limited border control (air, water, road) Limited travel restrictions Open public areas and events Open schools and universities Open shops, with limited access Flexible testing and tracing Self-isolation and self-quarantine No permission needed for leaving home No penalty for non-regulatory compliance | Targeted border control (air, water, road) Targeted travel restrictions Targeted closure of public areas and events Targeted closure of schools and universities Specific closure of shops, with limited access Targeted testing and tracing policy Self-isolation and quarantine Social distancing No permission needed for leaving home Penalty for non-regulatory compliance | Partial border closure (air, water, road) Partial travel restrictions Partial closure of public areas and events Partial closure of schools and universities Rigid testing and tracing policy Partial closure of shops (except for limited access to banks, supermarkets, drug stores, and petrol stations) Self-isolation and quarantine Social distancing Limited permission needed for leaving home Penalty for non-regulatory compliance | Full border closure (air, water, road) Full travel restrictions Full closure of public areas and events Full closure of schools and universities Rigid testing and tracing policy Full closure of shops (except for limited access to banks, supermarkets, drug stores, and petrol stations) Self-isolation and quarantine Permission needed for leaving home Penalty for non-regulatory compliance |
| Country | Italy | Spain | France | The Netherlands | Germany | UK | Austria | Sweden |
|---|---|---|---|---|---|---|---|---|
| Short-term coping capacity | ||||||||
| Total ICU capacity | 5.200 [18] | 4.575 [19] | 4.934 [20] | 1.050 [21] | 28.000 [22] | 4.123 [23] | 2.547 [24] | 526 [25] |
| Weekly testing rate [per 100.000] [26] 1 | 33.89 (wk9) | 0.019 (wk5) | 4.95 (wk9) | 98.83 (wk11) | 153.53 (wk11) | 102.29 (wk14) | 139.29 (wk15) | 0.11 (wk4) |
| Long-term coping capacity | ||||||||
| Gross Domestic Product (current $) [27] | 2.001 × 1012 | 1.394 × 1012 | 2.716 × 1012 | 909.07 × 109 | 3.85 × 1012 | 2.827 × 1012 | 446.315 × 109 | 530.83 × 109 |
| GDP growth (annual %) [28] | 0.3 | 2.0 | 1.5 | 1.8 | 0.6 | 1.4 | 1.6 | 1.2 |
| Current health expenditure [% of GDP] [29] | 8.84 | 8.87 | 11.31 | 10.1 | 11.25 | 9.63 | 10.4 | 11.02 |
| Social vulnerability | ||||||||
| Population size [30] | 60.3 × 106 | 47.1 × 106 | 67.1 × 106 | 17.3 × 106 | 83.13 × 106 | 66.83 × 106 | 8.87 × 106 | 1.8 × 106 |
| Population age 65 and above [% of total population] [31] | 23 | 20 | 20 | 20 | 22 | 19 | 19 | 20 |
| Population density [people/km2] [32] | 205 | 94 | 122 | 511 | 237 | 275 | 170 | 25 |
| Urban population [% of total population] [33] | 71 | 81 | 81 | 92 | 77 | 84 | 59 | 88 |
| Country | Ground for Policy Response | Strategy | Type of Measure | Measure | Effective Date |
|---|---|---|---|---|---|
| Austria | Delaying the spread | 3 | School closure | Nationwide school closures | 14 March 2020 |
| Delaying the spread | 4 | Public events banned | Banning of gatherings of more than 5 people | 10 March 2020 | |
| Increasing reproduction number (R0 > 3) | 5 | Lockdown ordered | Banning all access to public spaces and gatherings of more than 5 people. Advice to maintain 1 m distance. | 16 March 2020 | |
| Increasing reproduction number (R0 > 3) | 5 | Social distancing encouraged | Recommendation to maintain a distance of 1 m | 16 March 2020 | |
| Increasing reproduction number (R0 > 3) | 5 | Case-based measures | Implemented at lockdown | 16 March 2020 | |
| The Netherlands | Delaying the spread | 4 | School closure | Nationwide school closures | 16 March 2020 |
| Delaying the spread | 3 | Public events banned | Bans of events > 100 people | 12 March 2020 | |
| Increased ICU occupancy/Abandoning controversial herd immunity approach | 5 | Lockdown ordered | ‘Intelligent lockdown’ | 31 March 2020 | |
| First death cases confirmed | 2 | Social distancing encouraged | No hand shaking | 9 March 2020 | |
| Delaying the spread | 2 | Case-based measures | Advice for everyone experiencing symptoms to contact a health care agency to get tested and then self-isolate | 12 March 2020 | |
| France | Following “Declaration of war” | 4 | School closure | Nationwide school closures | 14 March 2020 |
| “Declaration of war” issued | 4 | Public events banned | Bans of events >100 people | 13 March 2020 | |
| Increasing reproduction number (R0 > 3) | 5 | Lockdown ordered | Everybody has to stay at home. Need a self-authorization form to leave home | 17 March 2020 | |
| Increasing reproduction number (R0 > 3) | 5 | Social distancing encouraged | Advice at the time of lockdown | 16 March 2020 | |
| Increasing reproduction number (R0 > 3) | 5 | Case-based measures | Advice at the time of lockdown | 16 March 2020 | |
| Germany | Protection stage of national pandemic plan | 4 | School closure | Nationwide school closures | 14 March 2020 |
| Increasing reproduction number (R0 > 3) | 5 | Public events banned | No gatherings of >1000 people. Otherwise regional restrictions only until lockdown. | 22 March 2020 | |
| Increasing reproduction number (R0 > 3) | 5 | Lockdown ordered | Gatherings of > 2 people banned, 1.5 m distance | 22 March 2020 | |
| Government assured preparedness | 3 | Social distancing encouraged | Avoid social interaction wherever possible recommended by Merkel | 12 March 2020 | |
| Increased threat level by Robert Koch Institute | 3 | Case-based measures | Advice for everyone experiencing symptoms to contact a health care agency to get tested and then self-isolate | 6 March 2020 | |
| Italy | Increasing reproduction number (R0 > 4) | 4 | School closure | Nationwide school closures | 5 March 2020 |
| High ICU occupancy | 4 | Public events banned | The government bans all public events | 9 March 2020 | |
| Potential exceedance of ICU capacity | 5 | Lockdown ordered | The government closes all public places. People have to stay at home except for essential travel. | 1 March /2020 | |
| Increasing reproduction number (R0 > 3) | 4 | Social distancing encouraged | A distance of more than 1 m has to be kept and any other form of alternative aggregation is to be excluded | 9 March 2020 | |
| Increasing reproduction number (R0 > 3) | 4 | Case-based measures | Advice to self-isolate if experiencing symptoms and quarantine if tested positive | March 2020 | |
| Spain | Increasing reproduction number (R0 > 4) | 4 | School closure | Nationwide school closures | 1 March 2020 |
| State of emergency declared | 5 | Public events banned | Banning of all public events by lockdown | 14 March 2020 | |
| State of emergency declared | 5 | Lockdown ordered | Nationwide lockdown | 14 March 2020 | |
| Increasing reproduction number (R0 > 4) | 4 | Social distancing encouraged | Advice on social distancing and working remotely from home | 9 March 2020 | |
| Increasing fatality rate | 5 | Case-based measures | Advice to self-isolate for 7 days if experiencing a cough or fever symptoms | 17 March 2020 | |
| UK | Increasing reproduction number (R0 > 3) | 4 | School closure | Nationwide school closure. Childminders, nurseries and sixth forms are told to follow the guidance. | 21 March 2020 |
| Abandoning controversial herd immunity approach | 5 | Public events banned | Implemented with lockdown. | 24 March 2020 | |
| Abandoning controversial herd immunity approach | 5 | Lockdown ordered | Gatherings of more than 2 people not from the same household are banned and police enforceable | 24 March 2020 | |
| Delay phase of action plan | 3 | Social distancing encouraged | Advice to avoid pubs, clubs, theatres and other public institutions. | 16 March 2020 | |
| Delay phase of action plan | 2 | Case-based measures | Advice to self-isolate for 7 days if experiencing a cough or fever symptoms | 12 March 2020 | |
| Sweden | Increasing reproduction number (2 < R0 < 3) | 2 | School closure | Colleges and upper secondary schools shut | 18 March 2020 |
| Containing the spread | 2 | Public events banned | The government bans events >500 people | 12 March 2020 | |
| Sufficient ICU capacity | 2 | Lockdown ordered | No lockdown occurred | ||
| Focus on right behaviour and social norms | Social distancing encouraged | People even with mild symptoms are told to limit social contact, encouragement to work from home | 16 March 2020 | ||
| Increased risk level—moderate to high | 1 | Case-based measures | Advice to self-isolate if experiencing a cough or fever symptoms | 10 March 2020 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van der Voorn, T.; de Jong, M. Cope or Perish? Managing Tipping Points in Developing Coping Strategies for Emergency Response during the First Wave of the COVID-19 Outbreak in Europe. COVID 2021, 1, 39-70. https://doi.org/10.3390/covid1010005
van der Voorn T, de Jong M. Cope or Perish? Managing Tipping Points in Developing Coping Strategies for Emergency Response during the First Wave of the COVID-19 Outbreak in Europe. COVID. 2021; 1(1):39-70. https://doi.org/10.3390/covid1010005
Chicago/Turabian Stylevan der Voorn, Tom, and Martin de Jong. 2021. "Cope or Perish? Managing Tipping Points in Developing Coping Strategies for Emergency Response during the First Wave of the COVID-19 Outbreak in Europe" COVID 1, no. 1: 39-70. https://doi.org/10.3390/covid1010005
APA Stylevan der Voorn, T., & de Jong, M. (2021). Cope or Perish? Managing Tipping Points in Developing Coping Strategies for Emergency Response during the First Wave of the COVID-19 Outbreak in Europe. COVID, 1(1), 39-70. https://doi.org/10.3390/covid1010005