Abstract
Contemporary estimates of the association between functional impairment and health costs among United States (US) older adults who documented having pain are unavailable. We used a retrospective database design and developed unadjusted and adjusted linear regression models to assess total, office, outpatient, emergency department, inpatient, and prescribed drug costs between older US adults with and without functional impairment. We included US adults aged ≥ 50 in the 2020 Medical Expenditure Panel Survey dataset who documented having pain in the past month. We also included only those who had positive health costs. Among the 40,092,210 US adults aged ≥ 50 who documented having pain in the past month, we found 37% had functional impairment. In adjusted linear regression models, we found adults with functional impairment (versus adults without functional impairment) had 57.2% higher total health costs and 54.1% higher prescribed drug costs. We did not observe any statistical differences between groups for office, outpatient, emergency department, or inpatient costs. In conclusion, the higher total and prescribed drug costs we found among US older adults with pain and a functional impairment draws attention to the financial burden of functional impairment among these individuals, which needs to be addressed.
1. Introduction
Pain is a prevalent condition that affected over 125 million United States (US) adults in 2012 according to one study [1]. Data from the 2011 National Health and Aging Trends Study found that approximately 53% of US adults aged ≥ 65 years of age had bothersome pain in the past month [2]. It can be managed using a variety of strategies, yet the amount of time and number of strategies used to manage pain is often burdensome for patients [3,4]. Pain is attributed to substantial economic consequences for patients both directly and indirectly, for healthcare payers (e.g., health insurance companies and government programs such as Medicare and Medicaid), and from a societal perspective. For example, one study using 2008 MEPS data calculated the overall costs of pain varied between $560 billion and to $630 billion [5]. The same study found individuals with pain had approximately $300 billion per year higher health costs than those without pain. Furthermore, pain was attributable to approximately $335 billion in lost productivity [5].
Pain is related to functional impairment and disabilities such as activities of daily living impairment and mobility issues [6,7,8,9]. For instance, a nationally representative survey of older adults found that pain in the past month was associated with lower physical functioning [2]. Previous research has suggested modest declines in the proportion of US adults aged ≥ 85 years old in recent years, although data for this population are somewhat limited in national surveys. However, the same research observed a stagnation in the prevalence of various limitations among older adults aged 65–84 years, and concerningly a slight increase in limitations for those aged 55–64 years [10]. Meanwhile, another study reported that the prevalence of functional limitations among community-dwelling older adults did not change between 2000 and 2005 [11]. Research has repeatedly indicated that healthcare expenditures are increasing [12] and that these expenditures increase substantially as the number of health conditions an individual has increases [13]. Recent research has reported that several characteristics, including sex, ethnicity or race, work status, marriage status, pain severity, health condition status, exercise status, and comorbidities, were also related to functional impairment among US adults aged ≥ 50 with pain [14].
Individuals with functional impairment typically experience greater health costs than those without functional impairment. For example, a study that used 2006 MEPS data reported individuals with chronic conditions and functional impairment ($11,284) spent on average over three times more on health costs each year than individuals with chronic conditions, but no functional impairment ($3641) [15].
The number of US older adults has been growing substantially in recent years. For instance, there were 10.5 million more US adults aged ≥ 50 in the five years from 2011 to 2016, reaching a total of 112 million [16]. As a result, 55% of households are now headed by someone aged ≥ 50 years [16]. Previous research using 1997 Medicare Current Beneficiary Survey data found total median health costs increased with the number of activity impairments. These increased costs were attributed to an increase in the frequency of health service use, rather than the intensity or cost of each event [17]. Data on functional impairment can be used as a determinant of health costs given the established association between activity impairment and health costs [18].
In 2019, US health costs increased by 4.6% [19]. Approximately 31% of this cost was attributed to hospital services, while 15% was attributed to physician services, and 10% to prescription medications [19]. Given the rising older adult population and ever-rising health costs, it is prudent to investigate the association between the presence of functional impairment and contemporary health costs among US older adults. The rationale for this study, therefore, was to assess health costs between US older (≥50 years) adults who documented having pain and functional impairment to those with no functional impairment.
2. Methods
We utilized a retrospective database design for this study. We used the 2020 Medical Expenditure Panel Survey (MEPS) data, which are gathered from individuals over five panels of consultations during a two-year timeframe using the 2019 National Health Interview Survey sampling framework. MEPS data contains weighting variables than can be employed in analysis to provide weighted estimations of the non-institutionalized US population. One core aspect is the MEPS household component, which holds demographic, health status, health conditions, health insurance, and various health cost data for each person surveyed. Cost data from the Medical Provider Component of MEPS are used by MEPS staff to supplement the cost data to enhance data quality [20]. We used the 2020 Full Year Consolidated Data File released in August 2022 for this study [21,22].
We included US adults aged ≥ 50 who were living in 2020 and documented having pain in the past month, and had positive total health costs. Pain in the past month was qualified based off answers from the question: “During the past four weeks, pain interfered with normal work (including both work outside the home and housework).” Participants that answered: “a little bit”, “moderately”, “quite a bite”, or “extremely” were deemed to have pain. Participants that answered “not at all” on the question, who died during 2020, were younger than 50 years of age, or did not have positive total health costs were considered ineligible for the study [21,22].
Our independent variable for this study was functional impairment (coded dichotomously as “yes” or “no”), which was determined based off answers from the question: “Does anybody in the family have difficulties walking, climbing stairs, grasping objects, reaching overhead, lifting, bending or stooping, or standing for long periods of time?” Participants who had any of these impairments were identified and deemed to have functional impairment [21,22].
We controlled the following variables in the adjusted analysis: age in years (50–64 or ≥65), gender (male or female), education attained (up to and including high school or higher than high school), employment status (employed or unemployed), poverty level (poor to low income or middle to high income), health insurance coverage (private, public, or uninsured), marital status (married or other), number of chronic conditions (≥3 or <3), frequent exercise (yes or no), pain level (quite a bit to extreme or little to moderate), general health state (excellent to good or fair to poor), mental health state (excellent to good or fair to poor), and smoking status (smoker or non-smoker) [21,22].
Six categories of health costs were assessed between participants with a functional impairment and participants with no functional impairment: (1) total cost, (2) office cost, (3) outpatient cost, (4) emergency department cost, (5) inpatient cost, and (6) prescribed drug cost. MEPS health costs are characterized as the total amount of payments made directly for services provided in 2020 and include out-of-pocket, private insurance, and public insurance payments (e.g., payments from Medicaid or Medicare services). Indirect payments and over-the-counter medications are not included. Total costs included costs for all health services for 2020. Office and outpatient costs included visits to physicians and non-physician health professionals. Inpatient costs included costs for hospital admissions. Outpatient, emergency department, and inpatient costs included facility costs and separately billing doctor costs (i.e., payments for services that were billed separately). Prescribed drug costs constituted all costs for initial and refill prescriptions by insurance providers or out-of-pocket [21,22].
To compare differences between participants with functional impairment and participants without functional impairment, we used chi-square tests for nominal variables and a t-tests for cost variables. Variables that had a significant difference between functional impairment groups were controlled for in adjusted models. Cost data were logarithmically transformed (to improve the distribution of the non-linear cost data) in all regression models. The reference group in all instances was the no functional impairment group. We tested the linear regression model assumptions that were determined to be acceptable. We calculated variance estimates using the Taylor-series linearization methodology. We calculated the percent difference between the functional impairment group and no functional impairment group using semi-logarithmic equations. We accounted for the complex MEPS survey design and weighted the analysis accordingly. We used SAS Studio (SAS Institute Inc., Cary, NC, USA) for all analyses.
3. Results
Figure 1 reports the number of participants who met the eligibility criteria for this study. A total of 2855 (weighted N = 40,092,210) US older adults were living throughout 2020, aged 50 years or older, documented having pain in the past month and had positive total health costs. Of these, 1148 reported a functional impairment, while 1707 did not report a functional impairment. The weighted population of participants who reported a functional impairment was 14,847,351 (37.0%, 95% confidence interval [CI] = 35.0, 39.1). Conversely, the weighted population of participants who did not report a functional impairment was 25,244,859 (63.0%, 95% CI = 60.9, 65.0).
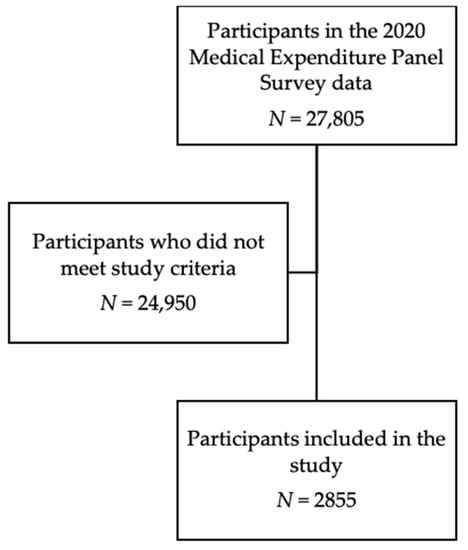
Figure 1.
Participants eligibility criteria.
We report the characteristics of the weighted population of US older adults (age ≥ 50) who documented having pain in the past month in our study in Table 1. We identified statistical differences between individuals with functional impairment and individuals with not functional impairment for all variables (p < 0.05) included in our analysis.

Table 1.
Characteristics of the weighted population of United States older adults (age ≥ 50) who documented having pain in the past month, stratified by functional impairment.
We report the descriptive statistics for the health cost of US older adults (age ≥ 50) who documented having pain in the past month in Table 2. Descriptive (unadjusted) total health and prescribed drug costs were higher among US older adults who reported a functional impairment than US older adults who did not (p < 0.05). There was no difference in the office, outpatient, emergency department, or inpatient health costs (p > 0.05).
Table 2.
Descriptive statistics for health cost of United States older adults (age ≥ 50) who documented having pain in the past month, stratified by functional impairment.
In the adjusted linear regression models, those with a functional impairment had 57.2% higher total health costs (β = 0.45, p < 0.0001) and 54.1% higher prescribed drug costs (β = 0.43, p < 0.0001). There was no difference in adjusted office, outpatient, emergency department, or inpatient health costs between groups (p > 0.05). See Table 3 for unadjusted and adjusted beta estimates and Figure 2 for the difference in percentage for health costs among those with a functional impairment compared to no functional impairment.
Table 3.
Unadjusted and adjusted intercepts and parameter estimates for functional impairment compared to no functional impairment in United States older adults (age ≥ 50) with pain in the past month, using positive logged health costs.
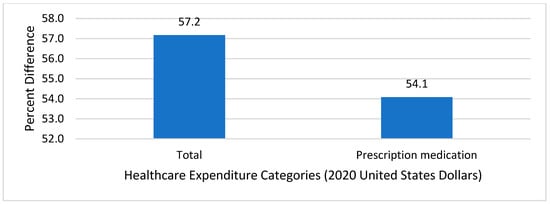
Figure 2.
Adjusted percent difference in 2020 health costs between those with functional impairment versus those without functional impairment among United States older adults with documented pain in the past month.
4. Discussion
In this study we found that US older adults with pain in the past month who also reported having a functional impairment had higher total health costs and higher prescribed drug costs in 2020 compared to US older adults who did not report a functional impairment in adjusted regression analyses. There was no difference between functional impairment groups for office costs, outpatient costs, emergency department costs, and inpatient costs. Our findings add fresh information to the literature about total health costs and prescribed drug costs using contemporary data, and are discussed in more detail below.
Our study found that among US older adults with pain, those with functional impairment had 57.2% higher total health costs than those who did not have functional impairment. This finding corroborates an existing report that found individuals with ≥3 chronic conditions and functional impairment had higher health costs, visited their health provider more frequently, and used home health care services more often than those with ≥3 chronic conditions, but no functional impairment [23]. Previous studies have reported the costs associated with various impairment and disabilities. For instance, data from a 2008 study in Belgium found that individuals with severe activity impairment accounted for approximately 17% of total health cost, indicating the impact that functional impairment can have on health costs [18]. Another study using MEPS data and Behavioral Risk Factor Surveillance System data reported disability-associated costs equaled $397.8 billion in 2006, and that 26.7% of health costs were related to disability in the US [24]. Those who reported having a functional impairment may also be unhealthier in general or have health conditions that resulted in their functional impairment. Data from the Framingham Study found several conditions, including depression, heart disease, hip fracture, knee osteoarthritis, and stroke, were all associated with functional impairment among older adults [25]. Other studies have supported this concept in specific populations. For example, those who rated their health as poor were strongly associated with physical impairment among individuals with chronic kidney disease [26]. The current study supports this concept, given that a greater proportion of individuals who had a functional impairment had ≥3 chronic conditions, did not frequently exercise, had greater pain levels, and perceived their health and mental health to be poor, compared to those without a functional impairment. Previous research using the National Health and Nutrition Examination Survey (2005–2012) data indicated that a greater number of chronic conditions was related to a corresponding increase in functional impairment [27]. Other studies have reported associations between multiple chronic conditions and higher health costs. For example, a study that also used 2018 MEPS data found multimorbidity (≥2 comorbid conditions) was associated with 76% higher total health costs, 41% higher office costs, and 101% higher prescription medications costs among US adults aged ≥ 50 years who documented having pain [28]. The presence of functional impairment may also be related to age. The current study found those with a functional impairment were typically older than those without. Previous research using 2013–2014 MEPS data found poorer physical functioning was associated with higher health utilization and costs among adults aged ≥ 70 years [29]. The finding that total health costs are higher among US older adults with a functional impairment versus those without is therefore well explained by existing literature.
Our study also found that among older US adults with documented pain, those who reported having functional impairment had 54.1% higher prescribed drug costs than those without functional impairment. This is an expected finding as those with functional impairment are likely to need more medications. However, it is unclear whether these medications actually lead to improved outcomes. One study of community-dwelling Medicare Advantage patients found that most participants with functional limitations did not have any help managing their medications, and suggested that improved adherence and outcomes could be obtained if they received medication management support [30]. Research has also shown that although improved adherence is associated with increased prescribed drug costs in older adults taking renin–angiotensin system antagonists, statins, and oral diabetes medications, it is also associated with lower overall health costs [31]. Additional research is needed to test the hypothesis of whether adherence to pain management strategies is associated with similar findings (i.e., reduced overall health costs despite increased prescribed drug costs) among older US adults with pain and functional limitations. Individuals with pain use many different types of pain management strategies [3,4]. It may be possible that alternatives to prescription medications could be used that help maintain or even improve pain management, while simultaneously reducing the cost and potential side effects of prescription medications. Although non-pharmacological therapies can be used to help manage pain, some may be better suited for individuals with functional impairment; for example, too much exercise may be difficult, yet massage may be helpful.
Our study findings support recommendations made by other researchers in recent years. For instance, a scoping review published in 2019 concluded that interventions are required to prevent the consequences of chronic conditions and impairment associated with older adults [32], while another review called for more research into interventions to prevent functional impairment throughout the lifespan [33]. In addition, a previous study using 1992–1998 Medicare data found that the health costs from age 70 to death were similar among healthy and non-healthy adults; thus, preventive interventions to improve health and longevity among older adults are warranted [34].
Study limitations include recall bias from the self-reported Medical Expenditure Panel Survey data (a secondary data source), whereby individuals may not have accurately recalled their responses to survey questions. Pain and functional impairment are conditions that may be interpreted subjectively by each individual. This makes them difficult to measure and compare to existing knowledge in the literature. The nature of this retrospective database study design was not able to establish a causal relationship between functional impairment status and health costs. Rather, only statistical associations can be ascertained. Given that the study was representative of the non-institutionalized civilian US older adult population, the findings in this study likely underestimate the health cost associated with functional impairment among US older adults. That is, individuals with severe functional impairment may be institutionalized due to their condition and their costs would not be captured in this study. Given that this study used data collected during the coronavirus disease-19 (COVID-19) pandemic, future research may be warranted to investigate these costs post-COVID-19 when data become available, to determine if they are similar or different to the 2020 data.
5. Conclusions
Our study found total health costs and prescribed drug costs were higher among US older adults (≥50 years) with pain in the past four weeks who reported having a functional impairment compared to those who did not report having a functional impairment. Yet, this was not the case in other categories of health costs, such as office, outpatient, emergency department, or inpatient health costs where there was no difference between those with and without a functional impairment. Further research is warranted to investigate why these health costs were associated with functional impairment, yet others were not, and to establish if a causal relationship exists between functional impairment status and health costs using a prospective study design. Further research could also investigate if these findings are similar post-COVID-19.
Author Contributions
Conceptualization, D.R.A.; methodology, D.R.A.; software, D.R.A.; validation, D.R.A. and H.U.; formal analysis, D.R.A.; investigation, D.R.A.; resources, D.R.A.; data curation, D.R.A.; writing—original draft preparation, D.R.A. and H.U.; writing—review and editing, D.R.A.; visualization, D.R.A.; supervision, D.R.A.; project administration, D.R.A.; funding acquisition, D.R.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of The University of Arizona (protocol code #2006721124, 12 June 2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data are available from the corresponding author upon reasonable request.
Conflicts of Interest
David R. Axon reports grant funding from the American Association of Colleges of Pharmacy, Arizona Department of Health, Merck & Co., National Council for Prescription Drug Programs, Pharmacy Quality Alliance, and Tabula Rasa HealthCare Group, outside of this study. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Nahin, R.L. Estimates of pain prevalence and severity in adults: United States, 2012. J. Pain 2015, 16, 769–780. [Google Scholar] [CrossRef] [PubMed]
- Patel, K.V.; Guralnik, J.M.; Dansie, E.J.; Turk, D.C. Prevalence and impact of pain among older adults in the United States: Findings from the 2011 National Health and Aging Trends Study. Pain 2013, 154, 2649–2657. [Google Scholar] [CrossRef]
- Axon, D.R.; Patel, M.J.; Martin, J.R.; Slack, M.K. Use of multidomain management strategies by community dwelling adults with chronic pain: Evidence from a systematic review. Scand. J. Pain 2019, 19, 9–23. [Google Scholar] [CrossRef]
- Axon, D.R.; Bhattacharjee, S.; Warholak, T.L.; Slack, M.K. Xm2 scores for estimating total exposure to multimodal strategies identified by pharmacists for managing pain: Validity testing and clinical relevance. Pain Res. Manag. 2018, 2018, 2530286. [Google Scholar] [CrossRef]
- Gaskin, D.J.; Richard, P. The economic costs of pain in the United States. J. Pain 2012, 13, 715–724. [Google Scholar] [CrossRef]
- Stamm, T.A.; Pieber, K.; Crevenna, R.; Dorner, T.E. Impairment in the activities of daily living in older adults with and without osteoporosis; osteoarthritis and chronic back pain: A secondary analysis of population-based health survey data. BMC Musculoskelet. Disord. 2016, 17, 139. [Google Scholar] [CrossRef]
- Valderrama-Hinds, L.M.; Al Snih, S.; Rodriguez, M.A.; Wong, R. Association of arthritis and vitamin D insufficiency with physical disability in Mexican older adults: Findings from the Mexican Health and Aging Study. Rheumatol. Int. 2017, 37, 607–616. [Google Scholar] [CrossRef]
- Makris, U.E.; Fraenkel, L.; Han, L.; Leo-Summers, L.; Gill, T.M. Restricting back pain and subsequent mobility disability in community-living older persons. J. Am. Geriatr. Soc. 2014, 62, 2142–2147. [Google Scholar] [CrossRef]
- Eggermont, L.H.P.; Leveille, S.G.; Shi, L.; Kiely, D.K.; Shmerling, R.H.; Jones, R.N.; Guralnik, J.M.; Bean, J.F. Pain characteristics associated with the onset of disability in older adults: The maintenance of balance, independent living, intellect, and zest in the elderly Boston study. J. Am. Geriatr. Soc. 2014, 62, 1007–1016. [Google Scholar] [CrossRef]
- Freedman, V.A.; Spillman, B.C.; Andreski, P.M.; Cornman, J.C.; Crimmins, E.M.; Kramarow, E.; Lubitz, J.; Martin, L.G.; Merkin, S.S.; Schoeni, R.F.; et al. Trends in late-life activity limitations in the United States: An update from five national surveys. Demography 2013, 50, 661–671. [Google Scholar] [CrossRef]
- Fuller-Thomson, E.; Yu, B.; Nuru-Jeter, A.; Guralnik, J.M.; Minkler, M. Basic ADL disability and functional limitation rates among older AMERICANS from 2000-2005: The end of the decline? The Journals of Gerontology. Ser. A Biol. Sci. Med. Sci. 2009, 64, 1333–1336. [Google Scholar] [CrossRef]
- Dieleman, J.L.; Cao, J.; Chapin, A.; Chen, C.; Li, Z.; Liu, A.; Horst, C.; Kaldjian, A.; Matyasz, T.; Scott, K.W.; et al. US health care spending by payer and health condition, 1996–2016. JAMA 2020, 323, 863–884. [Google Scholar] [CrossRef]
- Wolff, J.L.; Starfield, B.; Anderson, G. Prevalence, expenditures, and complications of multiple chronic conditions in the elderly. Arch. Intern. Med. 2002, 162, 2269–2276. [Google Scholar] [CrossRef]
- Axon, D.R.; Le, D. Association of self-reported functional limitations among a national community-based sample of older United States adults with pain: A cross-sectional study. J. Clin. Med. 2021, 10, 1836. [Google Scholar] [CrossRef]
- Individuals Living in the Community with Chronic Conditions and Functional Limitations: A Closer Look. Available online: https://aspe.hhs.gov/sites/default/files/private/pdf/75961/closerlook.pdf (accessed on 3 April 2023).
- Housing America’s Older Adults. Available online: https://www.jchs.harvard.edu/sites/default/files/media/imp/Harvard_JCHS_Housing_Americas_Older_Adults_2018.pdf (accessed on 3 April 2023).
- Chan, L.; Beaver, S.; Maclehose, R.F.; Jha, A.; Maciejewski, M.; Doctor, J.N. Disability and health care costs in the Medicare population. Arch. Phys. Med. Rehabil. 2002, 83, 1196–1201. [Google Scholar] [CrossRef]
- Van der Heyden, J.; Van Oyen, G.H.; Berger, N.; De Bacquer, D.; Van Herck, K. Activity limitations predict health care expenditures in the general population in Belgium. BMC Public Health 2015, 15, 267. [Google Scholar] [CrossRef]
- National Health Expenditures; 2019: Steady Spending Growth Despite Increases in Personal Health Care Expenditures in Advance of the Pandemic. Available online: https://www.ama-assn.org/system/files/2021-05/prp-annual-spending-2019.pdf (accessed on 3 April 2023).
- Medical Expenditure Panel Survey Background. Available online: https://meps.ahrq.gov/mepsweb/about_meps/survey_back.jsp (accessed on 3 April 2023).
- MEPS HC-224 2020 Full Year Consolidated Data File. Available online: https://meps.ahrq.gov/data_stats/download_data/pufs/h224/h224doc.pdf (accessed on 3 April 2023).
- MEPS HC-224 2020 Full Year Consolidated Data Codebook. Available online: https://meps.ahrq.gov/data_stats/download_data/pufs/h224/h224cb.pdf (accessed on 3 April 2023).
- High-Need; High-Cost Patients: Who Are They and How Do They Use Health Care? Available online: https://www.commonwealthfund.org/publications/issue-briefs/2016/aug/high-need-high-cost-patients-who-are-they-and-how-do-they-use (accessed on 3 April 2023).
- Anderson, W.L.; Armour, B.S.; Finkelstein, E.A.; Wiener, J.M. Estimates of state-level health-care expenditures associated with disability. Public Health Rep. 2010, 125, 44–51. [Google Scholar] [CrossRef]
- Guccione, A.A.; Felson, D.T.; Anderson, J.J.; Anthony, J.M.; Zhang, Y.; Wilson, P.W.; Kelly-Hayes, M.; Wolf, P.A.; Kreger, B.E.; Kannel, W.B. The effects of specific medical conditions on the functional limitations of elders in the Framingham Study. Am. J. Public Health 1994, 84, 351–359. [Google Scholar] [CrossRef]
- Lee, J.; Abdel-Kader, K.; Yabes, J.G.; Cai, M.; Chang, H.-H.; Jhamb, M. Association of self-rated health with functional limitations in patients with CKD. Kidney Med. 2021, 3, 745–752. [Google Scholar] [CrossRef]
- Jindai, K.; Nielson, C.M.; Vorderstrasse, B.A.; Quinones, A.R. Multimorbidity and functional limitations among adults 65 or alder, NHANES 2005-2012. Prev. Chronic Dis. 2016, 13, E151. [Google Scholar] [CrossRef]
- Marupuru, S.; Axon, D.R. Association of multimorbidity on healthcare expenditures among older United States adults with pain. J. Aging Health 2021, 33, 741–750. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Goodin, A.J.; Pahor, M.; Manini, T.; Brown, J.D. Healthcare utilization and physical functioning in older adults in the United States. J. Am. Geriatr. Soc. 2020, 68, 266–271. [Google Scholar] [CrossRef] [PubMed]
- Whaley, C.; Reed, M.; Hsu, J.; Fung, V. Functional limitations, medication support, and responses to drug costs among Medicare beneficiaries. PLoS ONE 2015, 10, e0144236. [Google Scholar] [CrossRef] [PubMed]
- Campbell, P.J.; Axon, D.R.; Taylor, A.M.; Smith, K.; Pickering, M.; Black, H.; Warholak, T.; Chinthammit, C. Hypertension, cholesterol and diabetes medication adherence, health care utilization and expenditure in a Medicare Supplemental sample. Medicine 2021, 100, e27143. [Google Scholar] [CrossRef] [PubMed]
- Maresova, P.; Javanmardi, E.; Barakovic, S.; Husic, J.B.; Tomsone, S.; Krejcar, O.; Kuca, K. Consequences of chronic diseases and other limitations associated with old age—A scoping review. BMC Public Health 2019, 19, 1431. [Google Scholar] [CrossRef] [PubMed]
- Von Bonsdorff, M.B.; Rantanen, T. Progression of functional limitations in relation to physical activity: A life course approach. Eur. Rev. Aging Phys. Act. 2011, 8, 23–30. [Google Scholar] [CrossRef]
- Lubitz, J.; Cai, L.; Kramarow, E.; Lentzner, H. Health, life expectancy, and health care spending among the elderly. N. Engl. J. Med. 2003, 349, 1048–1055. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).