
Hybrid Orthodontics for Aesthetic Deep Bite Correction—Case Series and General Clinical Considerations



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Methods
Patient Selection
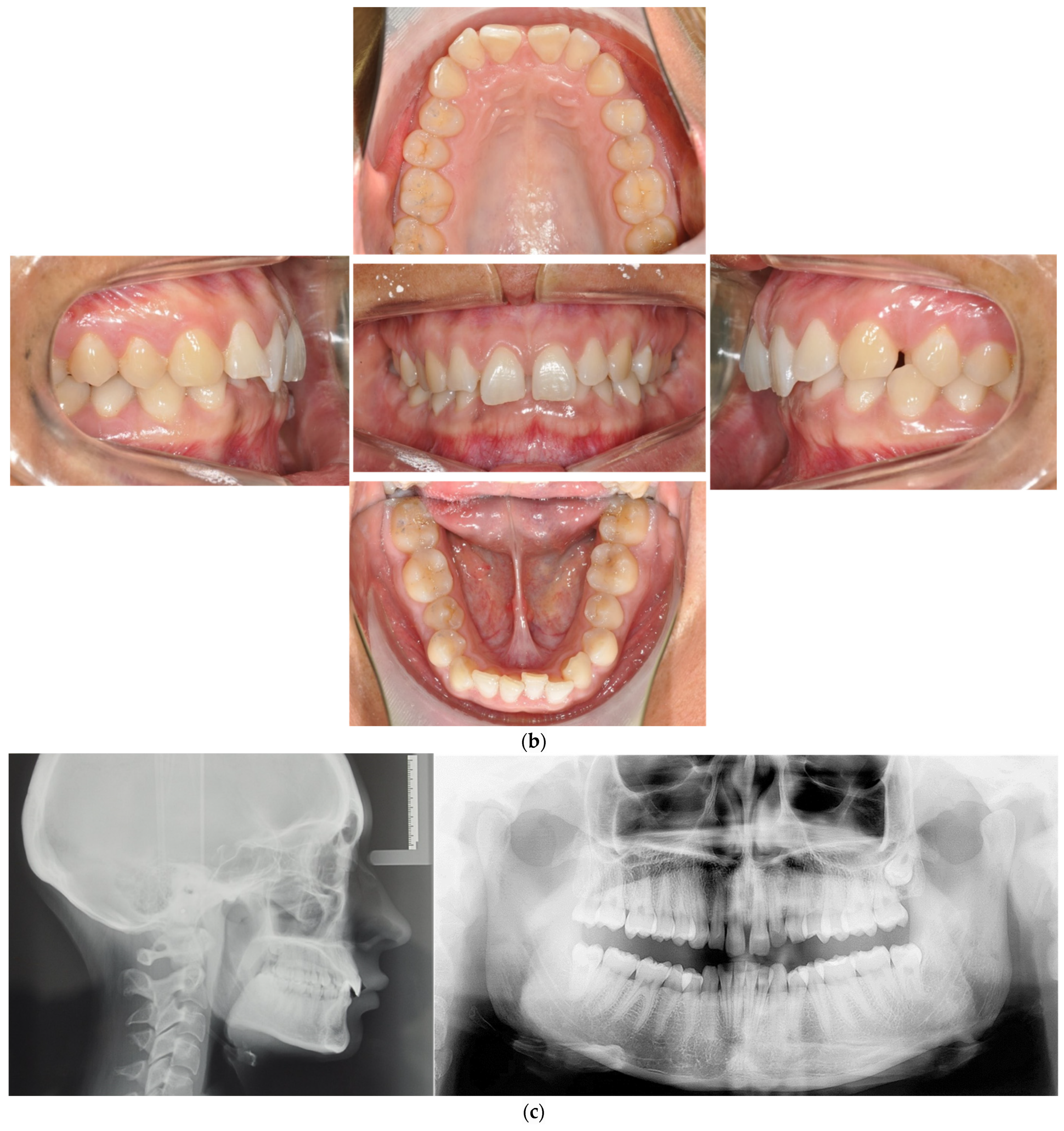
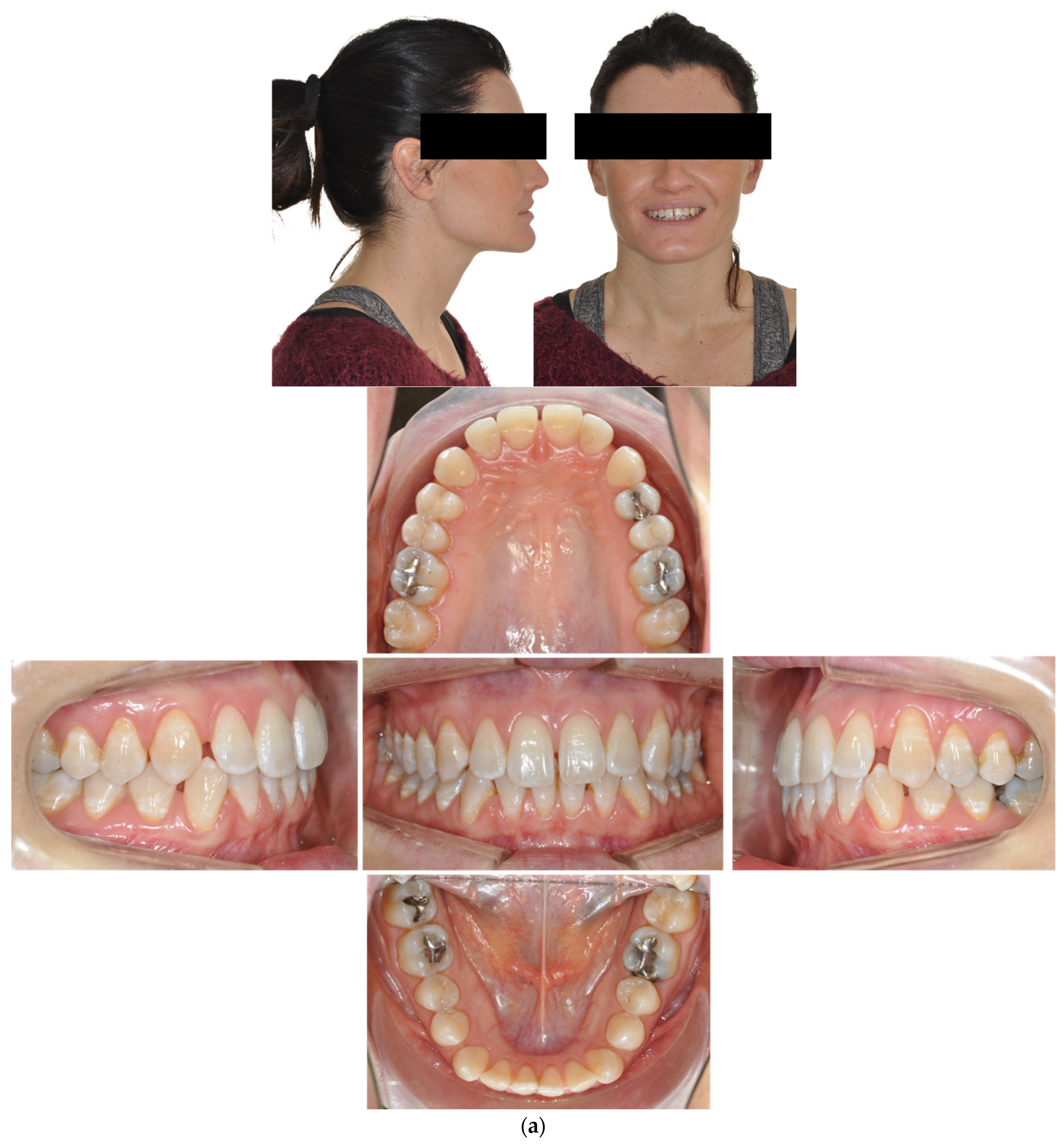
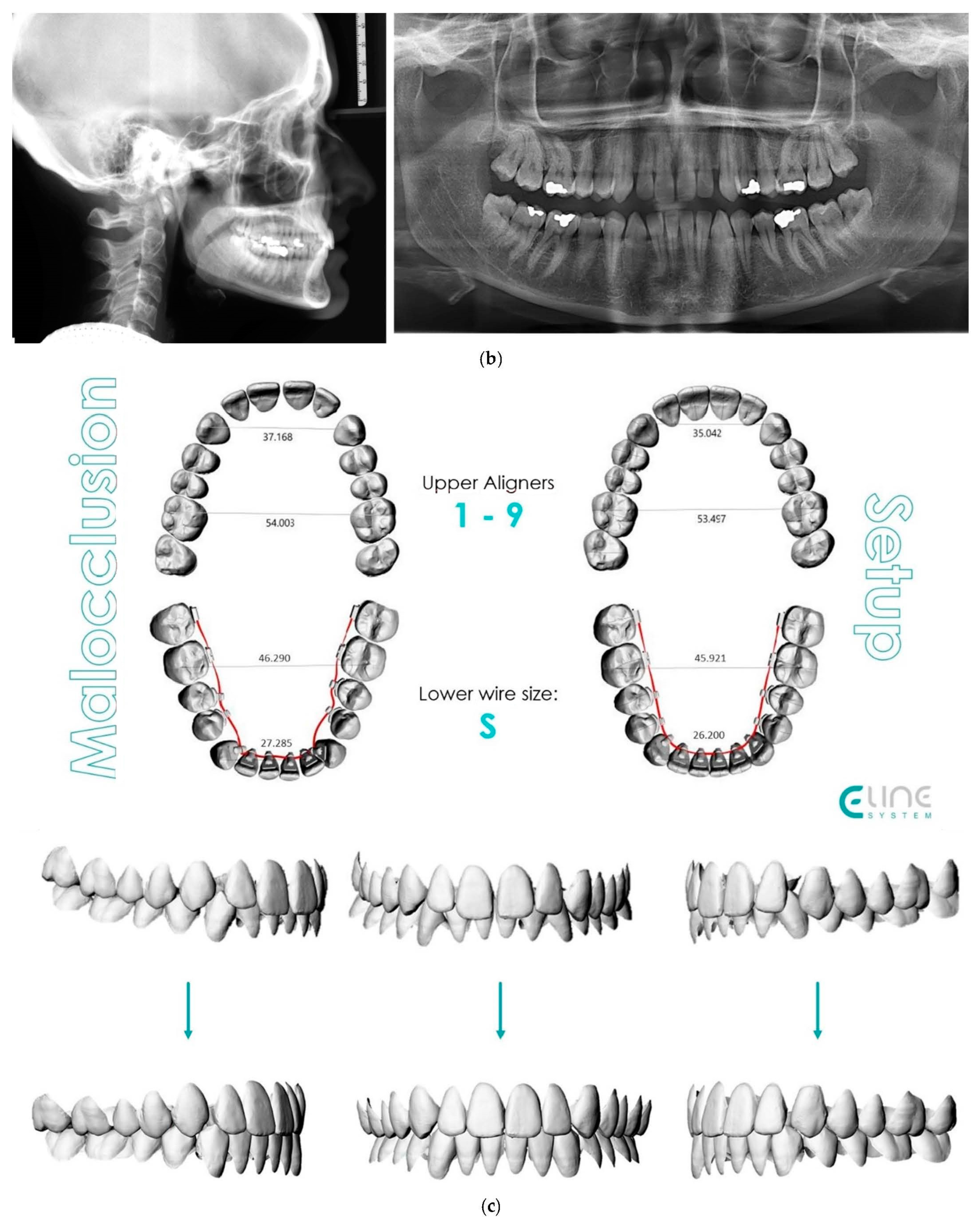
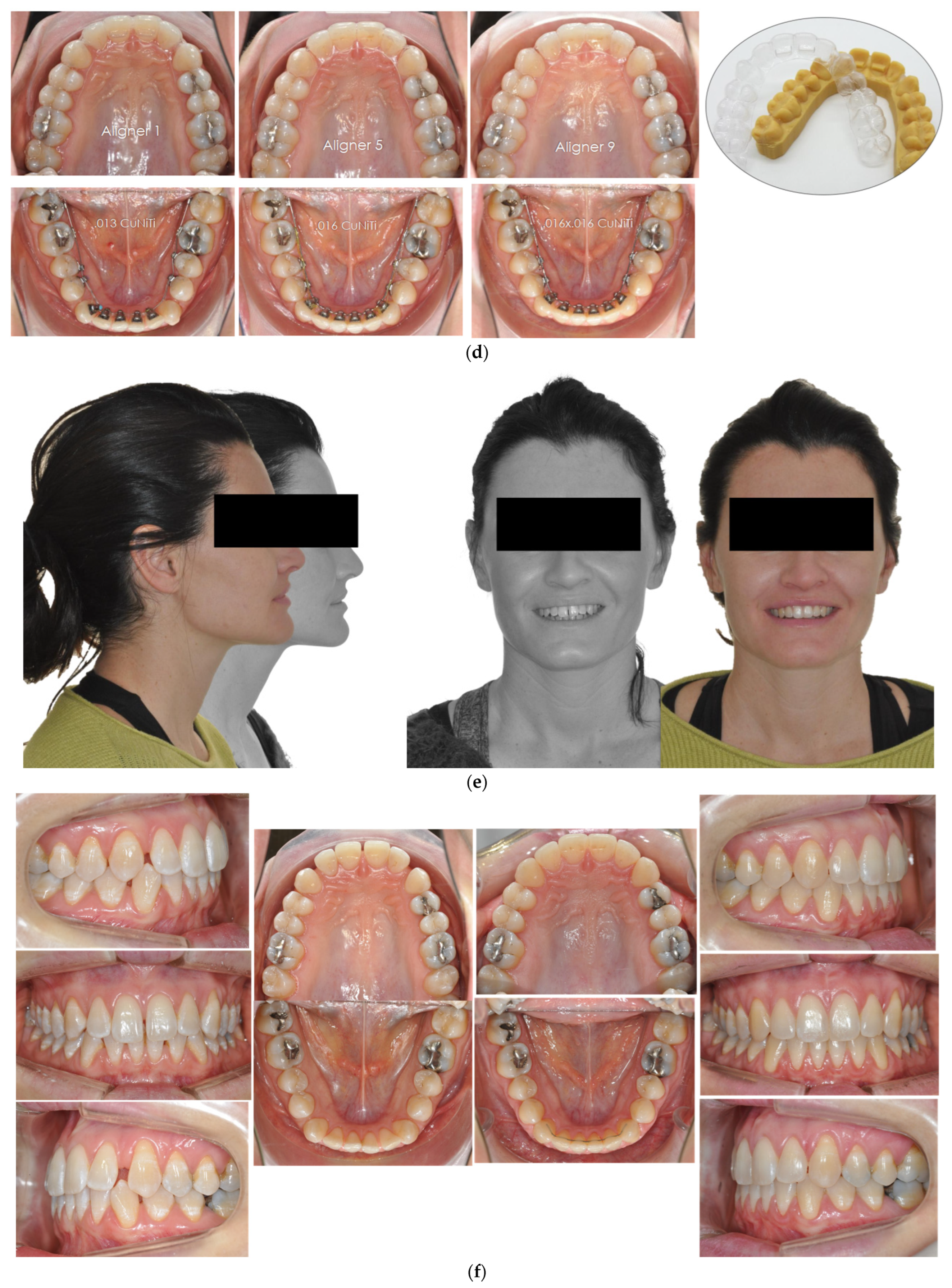
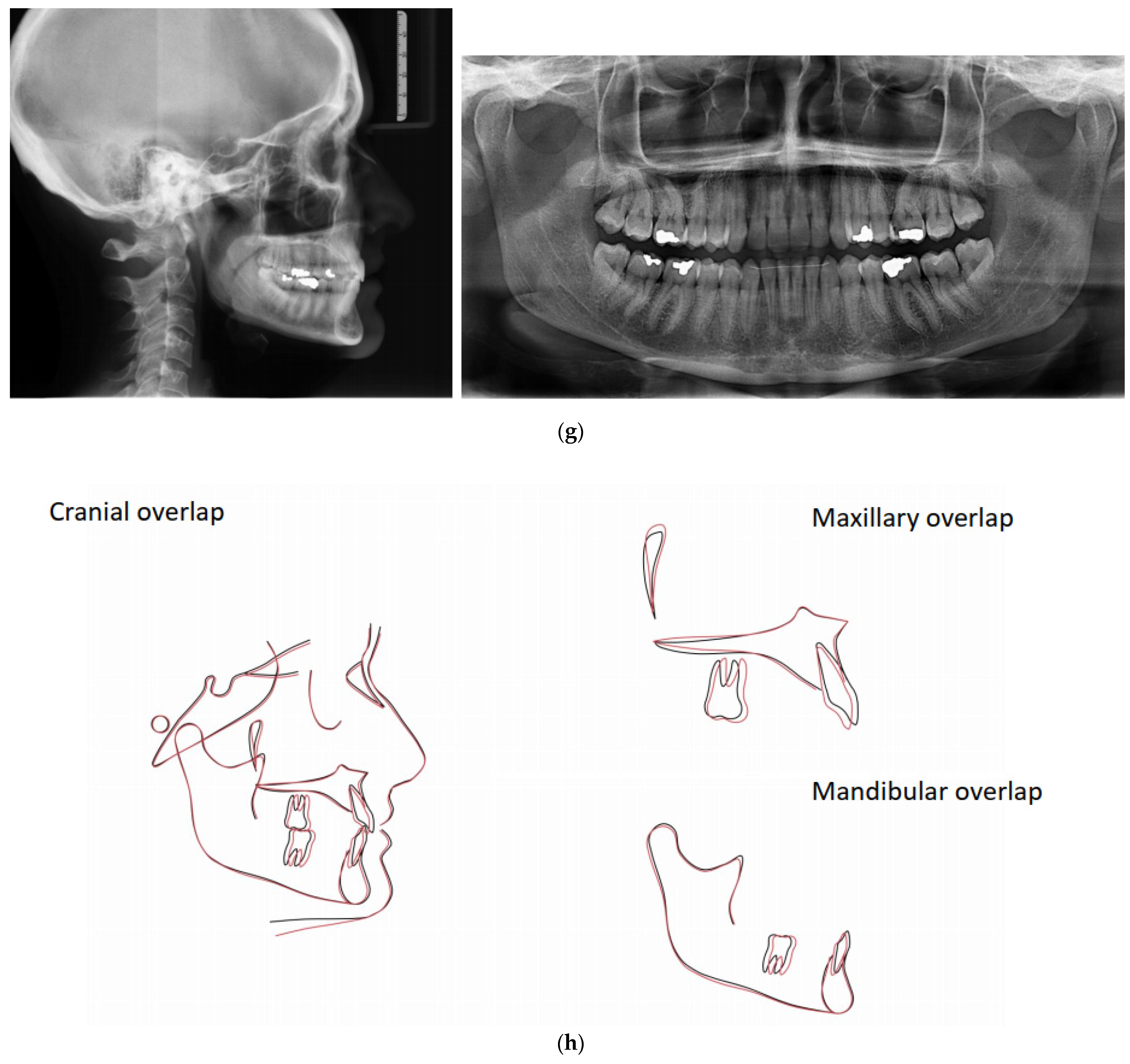
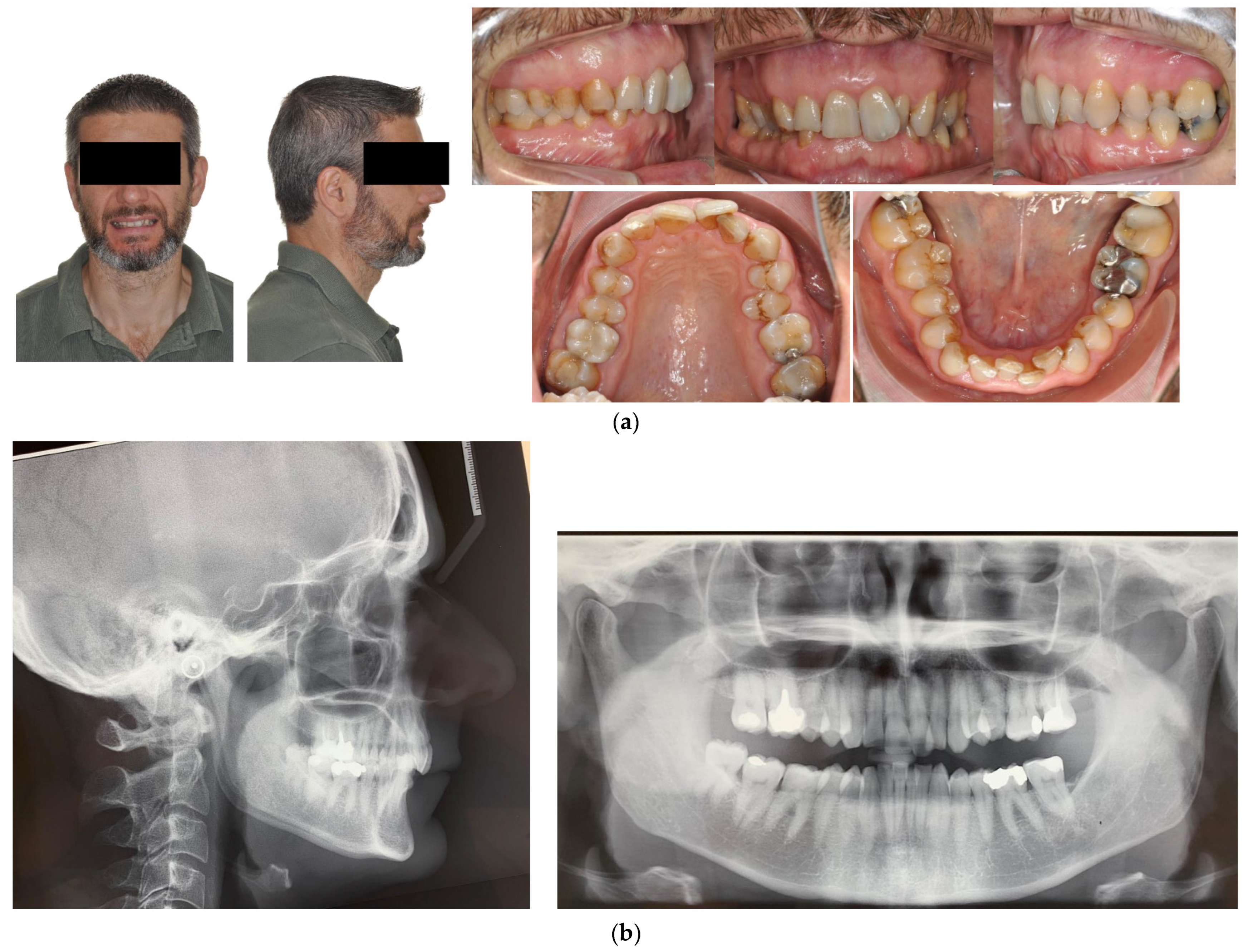
- Case 1: Class II division 2 with deep bite
- Case 2: Class III with deep bite
- Case 3: Class II subdivision with deep bite
3. Materials
4. Treatment Protocol
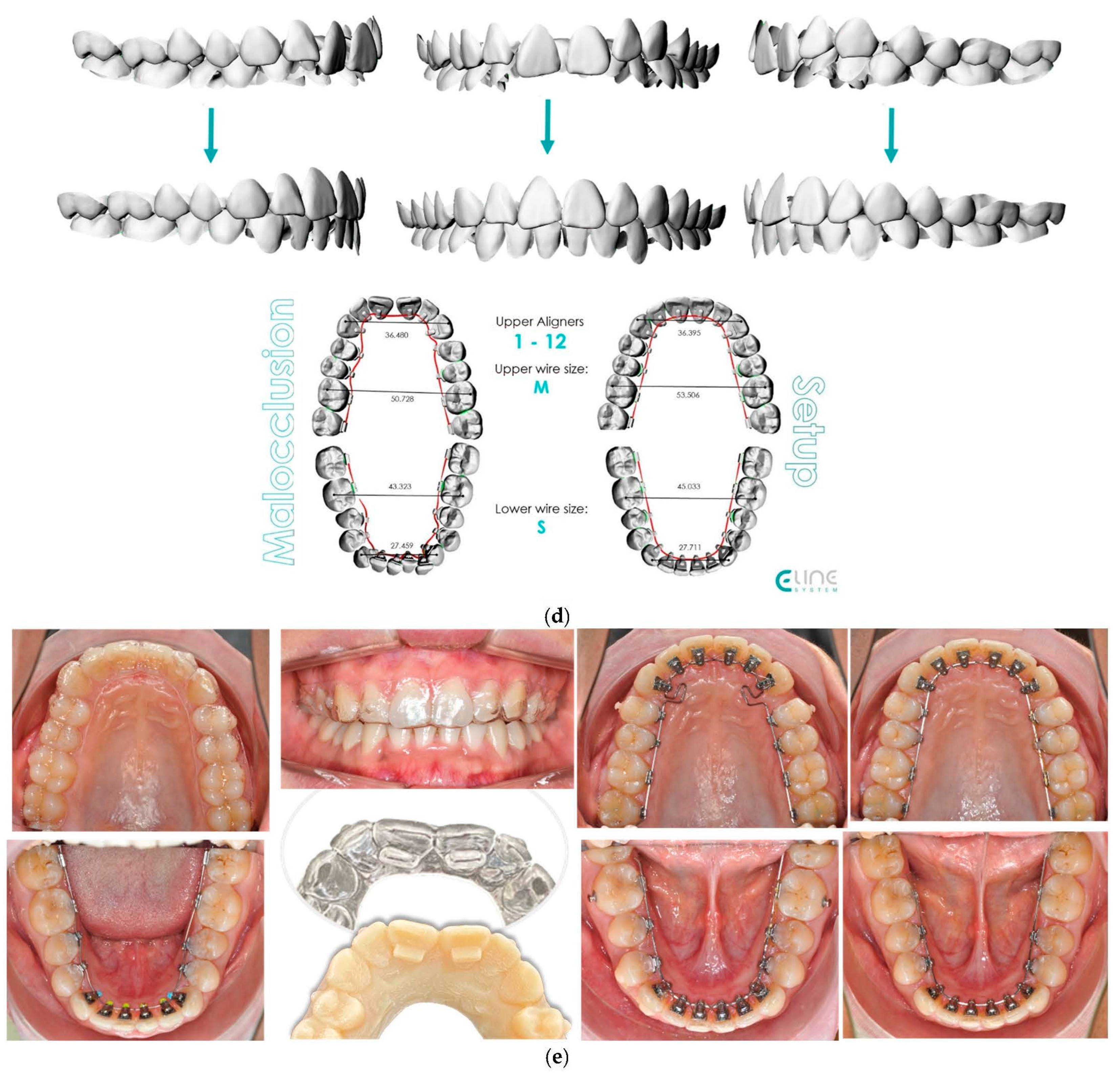
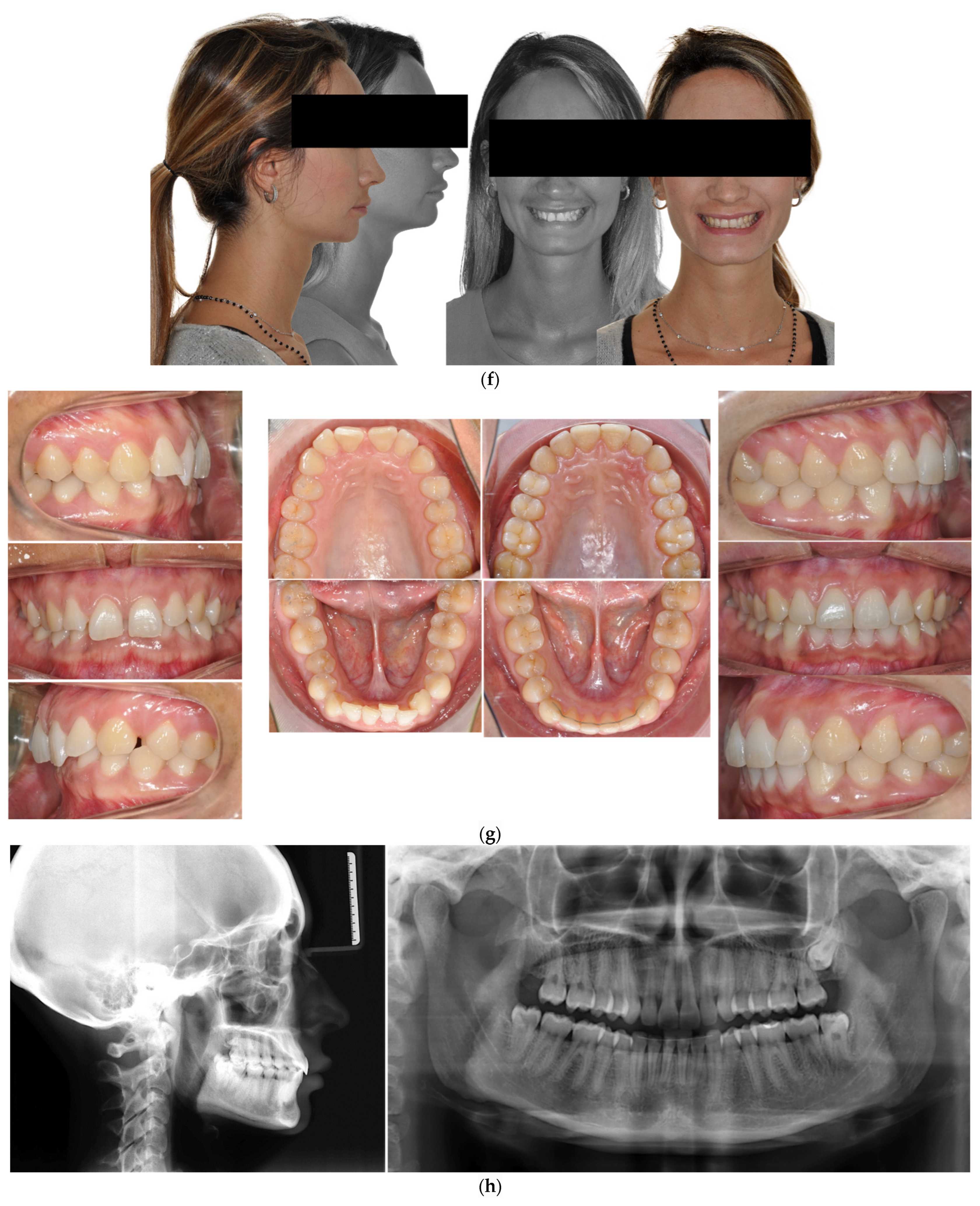
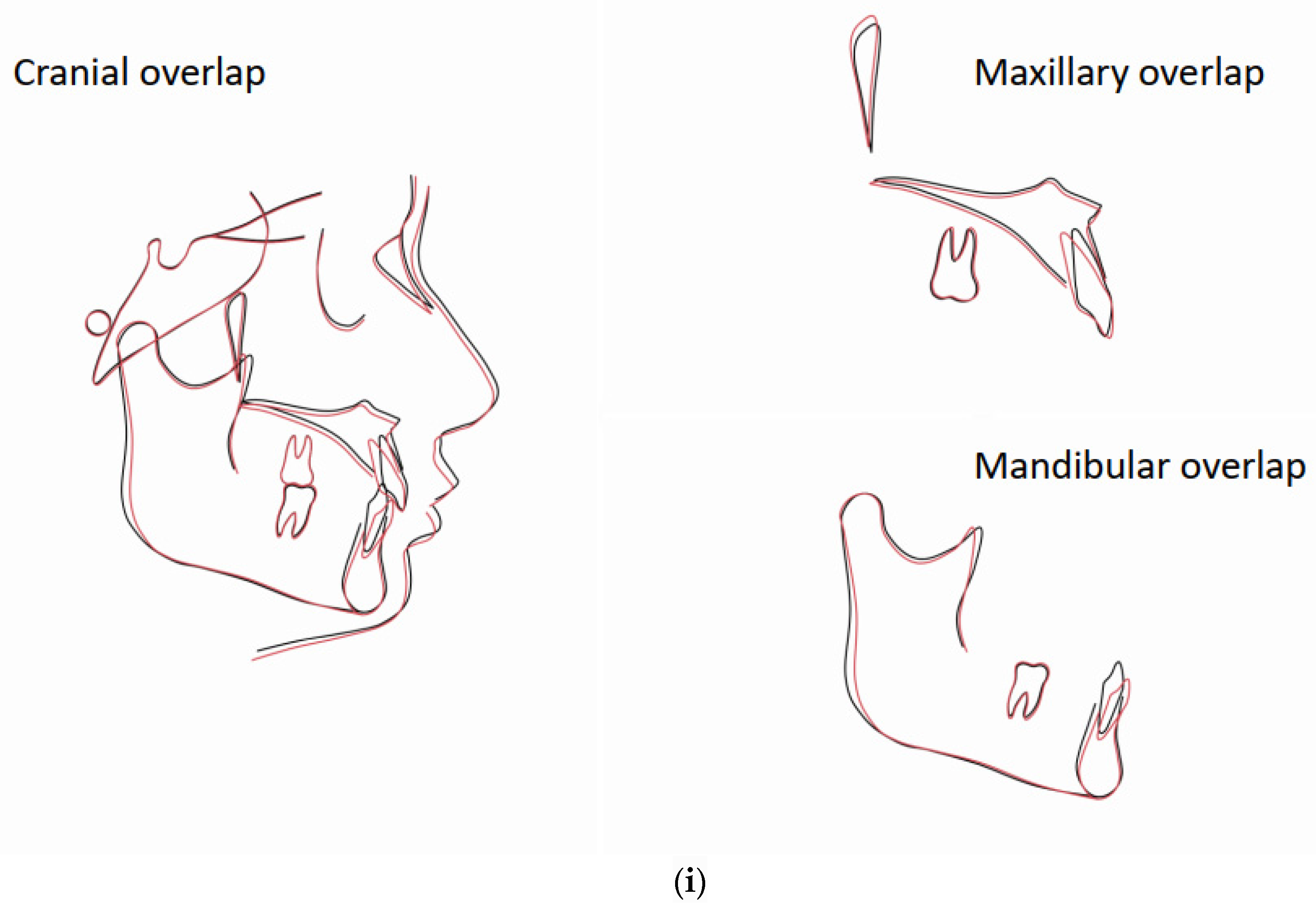
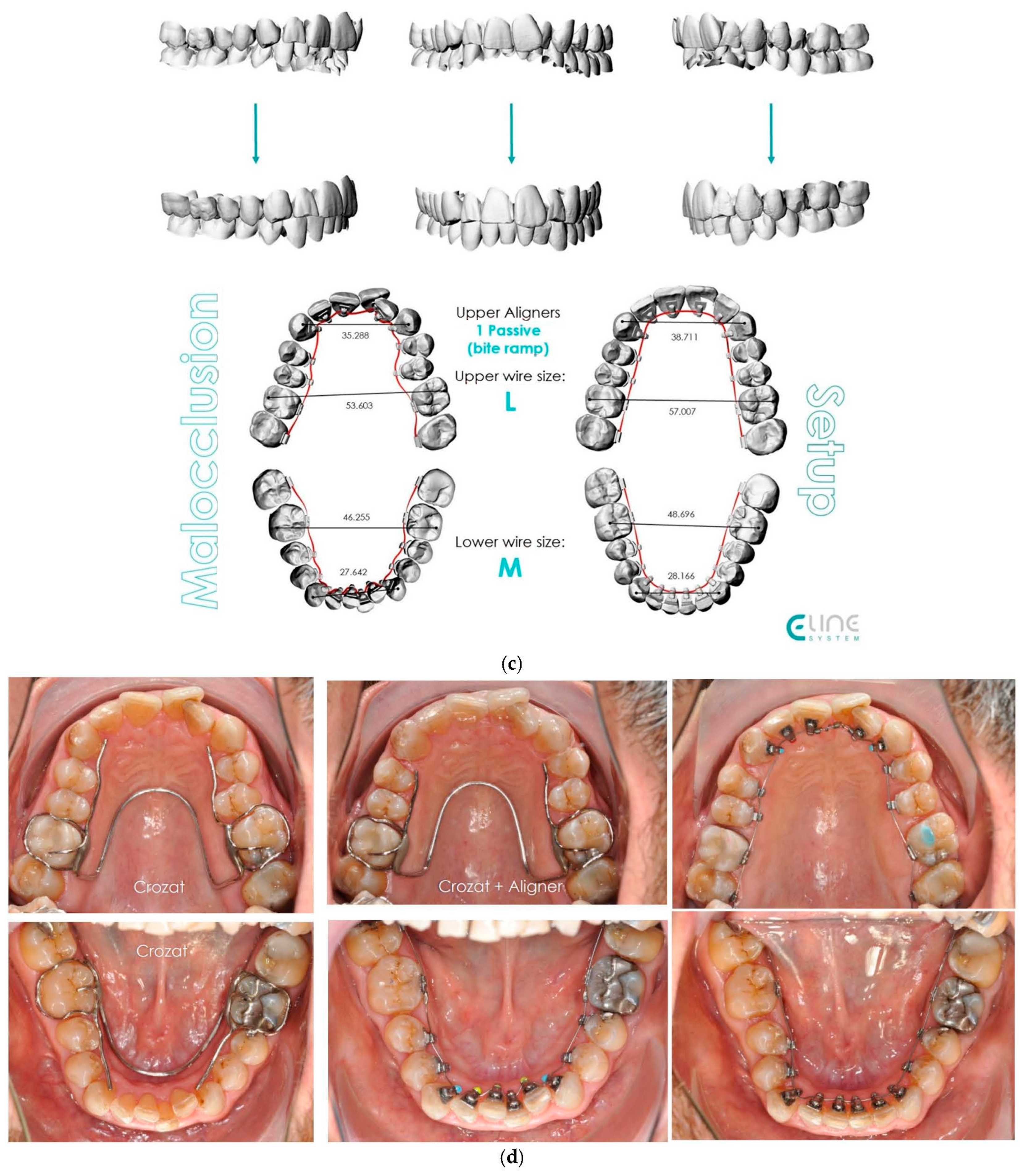
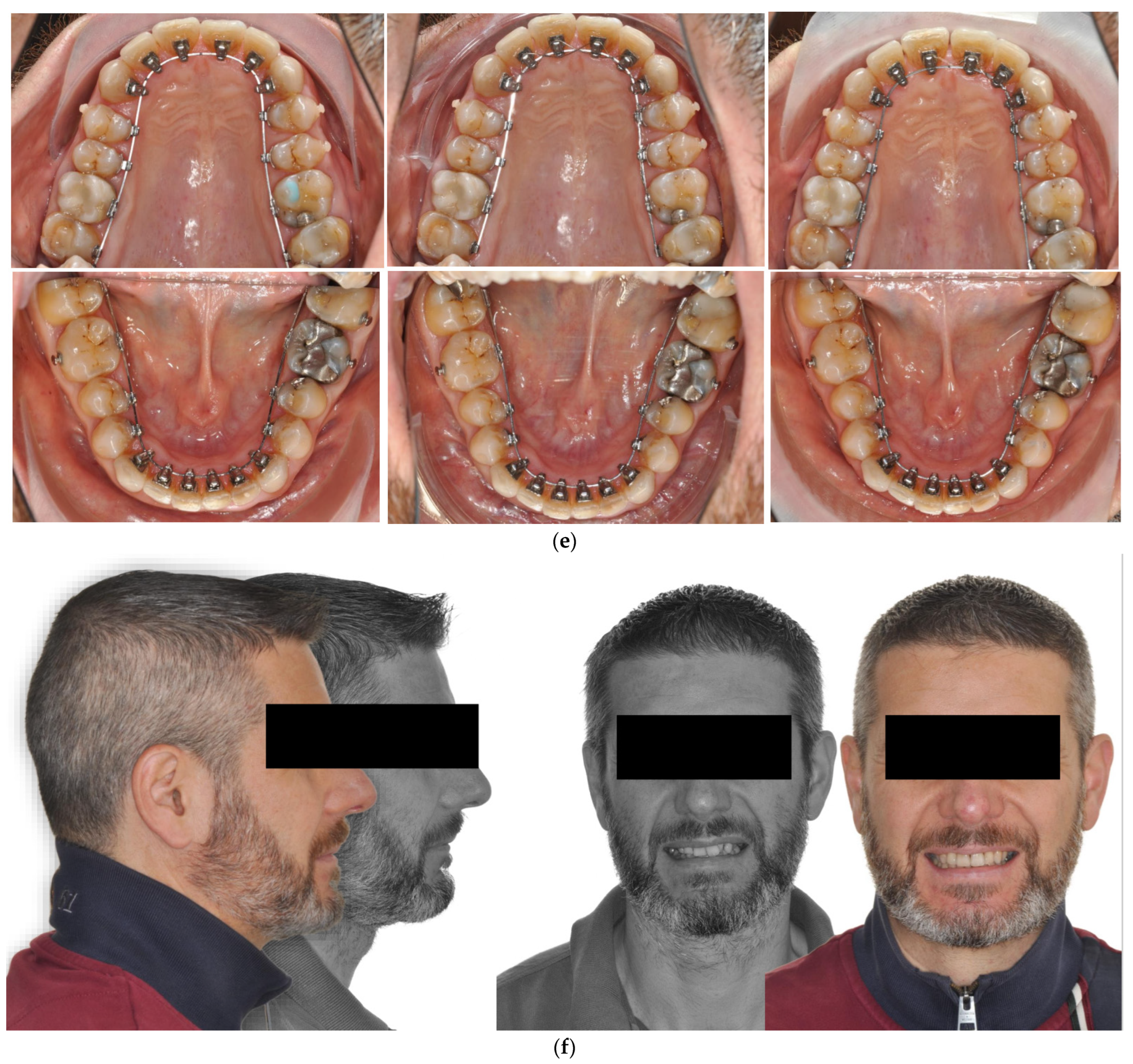
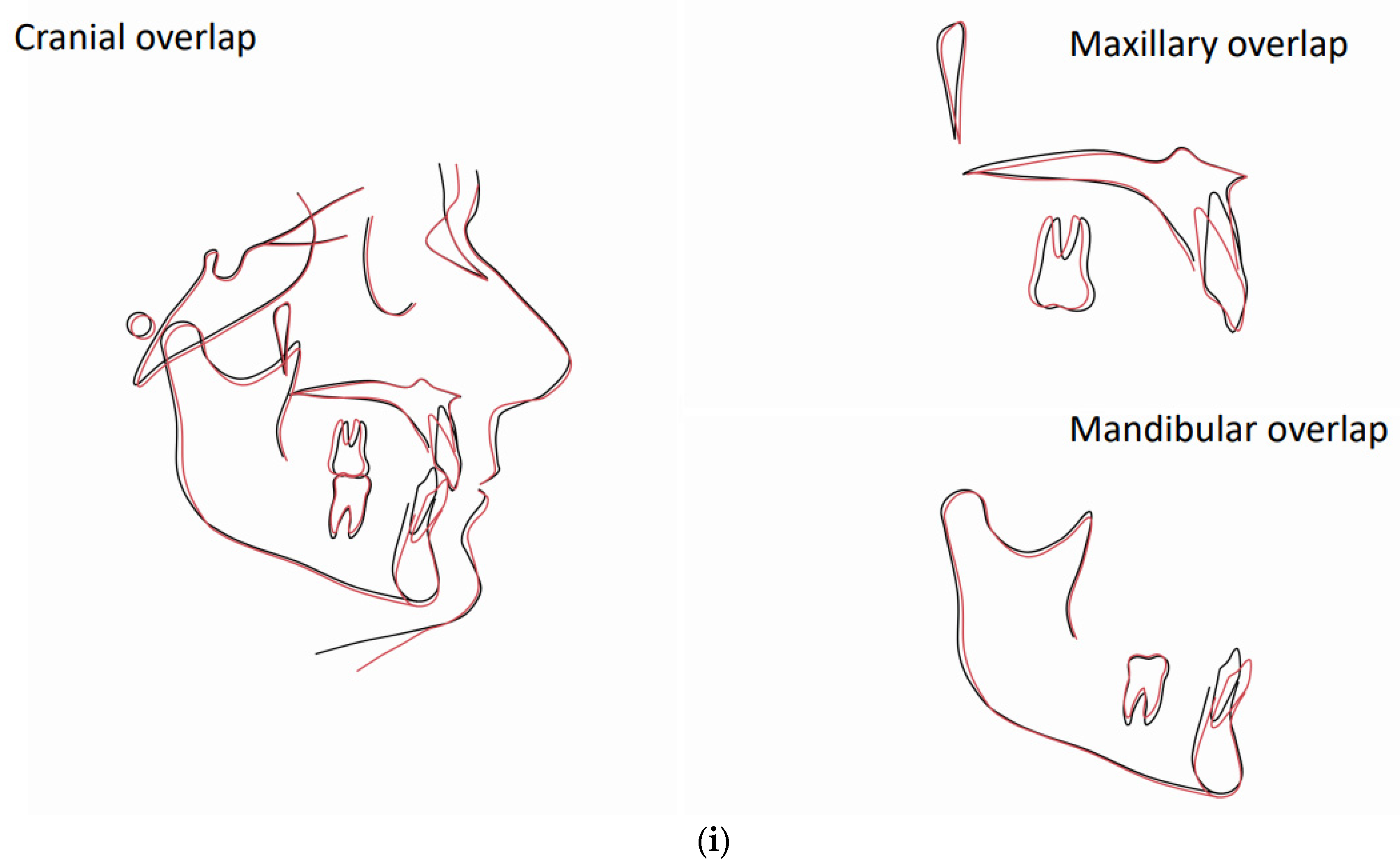
4.1. Case 1: Class II Division 2 with a Deep Bite
4.2. Case 2: Class III with a Deep Bite
4.3. Case 3: Class II Subdivision with a Deep Bite
5. Results and Discussion
- relatively reduced total treatment time compared to clear aligner therapy alone
- substantially improved quality of results with respect to those achievable via aligners alone
- the clear aligners used initially offered comfort, practicality and better dental hygiene while the bite was opened, and smaller movements could be easily achieved using aligners during bite opening while lingual fixed appliances were used for the more complex rotation and torque control
- both devices were customised and digitally programmed, which increased their predictability
- If the movements required are simple, such as uncontrolled tipping of the anterior and posterior teeth, small rotations of the incisors and posterior intrusion, aligner therapy is likely suitable; however, a hybrid approach may be more appropriate if multiple tooth movements are needed, as it enhances predictability and reduces treatment duration.
- Evaluation of the entity of the required moment and rotation is required. In our experience, if more than fifteen degrees of rotation are needed on premolars and molars, bodily movement of the teeth is greater than three mm and/or angular movements are greater than five degrees, a hybrid approach may be more efficient and predictable.
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pabari, S.; Moles, D.R.; Cunningham, S.J. Assessment of motivation and psychological characteristics of adult orthodontic patients. Am. J. Orthod. Dentofac. Orthop. 2011, 140, e263–e272. [Google Scholar] [CrossRef] [PubMed]
- Melzack, R. The McGill Pain Questionnaire: Major properties and scoring methods. Pain 1975, 1, 277–299. [Google Scholar] [CrossRef] [PubMed]
- Shaw, W.; Rees, G.; Dawe, M.; Charles, C. The influence of dentofacial appearance on the social attractiveness of young adults. Am. J. Orthod. 1985, 87, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Yavan, M.A.; Gökçe, G. YouTube as a source of information on adult orthodontics: A video analysis study. J. World Fed. Orthod. 2022, 11, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Weir, T. Clear aligners in orthodontic treatment. Aust. Dent. J. 2017, 62 (Suppl. S1), 58–62. [Google Scholar] [CrossRef] [PubMed]
- Papadimitriou, A.; Mousoulea, S.; Gkantidis, N.; Kloukos, D. Clinical effectiveness of Invisalign® orthodontic treatment: A systematic review. Prog. Orthod. 2018, 19, 37. [Google Scholar] [CrossRef] [PubMed]
- Boyd, R.L. Esthetic orthodontic treatment using the invisalign appliance for moderate to complex malocclusions. J. Dent. Educ. 2008, 72, 948–967. [Google Scholar] [CrossRef] [PubMed]
- Takemoto, K.; Scuzzo, G.; Lombardo, L.U.; Takemoto, Y.U. Lingual straight wire method. Int. Orthod. 2009, 7, 335–353. [Google Scholar] [CrossRef] [PubMed]
- Scuzzo, G.; Takemoto, K.; Takemoto, Y.; Takemoto, A.; Lombardo, L. A new lingual straight-wire technique. J. Clin. Orthod. 2010, 44, 114–123, quiz 106. [Google Scholar]
- Ravera, S.; Castroflorio, T.; Garino, F.; Daher, S.; Cugliari, G.; Deregibus, A. Maxillary molar distalization with aligners in adult patients: A multicenter retrospective study. Prog. Orthod. 2016, 17, 12. [Google Scholar] [CrossRef]
- Castroflorio, T.; Sedran, A.; Parrini, S.; Garino, F.; Reverdito, M.; Capuozzo, R.; Mutinelli, S.; Grybauskas, S.; Vaitiekūnas, M.; Deregibus, A. Predictability of orthodontic tooth movement with aligners: Effect of treatment design. Prog. Orthod. 2023, 24, 2. [Google Scholar] [CrossRef] [PubMed]
- Papageorgiou, S.N.; Koletsi, D.; Iliadi, A.; Peltomaki, T.; Eliades, T. Treatment outcome with orthodontic aligners and fixed appliances: A systematic review with meta-analyses. Eur. J. Orthod. 2020, 42, 331–343. [Google Scholar] [CrossRef] [PubMed]
- Papageorgiou, S.N.; Gölz, L.; Jäger, A.; Eliades, T.; Bourauel, C. Lingual vs. labial fixed orthodontic appliances: Systematic review and meta-analysis of treatment effects. Eur. J. Oral Sci. 2016, 124, 105–118. [Google Scholar] [CrossRef] [PubMed]
- Houle, J.-P.; Piedade, L.; Todescan, R.; Pinheiro, F.H.S.L. The predictability of transverse changes with Invisalign. Angle Orthod. 2017, 87, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Galan-Lopez, L.; Barcia-Gonzalez, J.; Plasencia, E. A systematic review of the accuracy and efficiency of dental movements with Invisalign®. Korean J. Orthod. 2019, 49, 140–149. [Google Scholar] [CrossRef] [PubMed]
- Charalampakis, O.; Iliadi, A.; Ueno, H.; Oliver, D.R.; Kim, K.B. Accuracy of clear aligners: A retrospective study of patients who needed refinement. Am. J. Orthod. Dentofac. Orthop. 2018, 154, 47–54. [Google Scholar] [CrossRef]
- Rossini, G.; Parrini, S.; Castroflorio, T.; Deregibus, A.; Debernardi, C.L. Efficacy of clear aligners in controlling orthodontic tooth movement: A systematic review. Angle Orthod. 2015, 85, 881–889. [Google Scholar] [CrossRef]
- Buschang, P.H.; Ross, M.; Shaw, S.G.; Crosby, D.; Campbell, P.M. Predicted and actual end-of-treatment occlusion produced with aligner therapy. Angle Orthod. 2015, 85, 723–727. [Google Scholar] [CrossRef]
- Ata-Ali, F.; Cobo, T.; De Carlos, F.; Cobo, J.; Ata-Ali, J. Are there differences in treatment effects between labial and lingual fixed orthodontic appliances? A systematic review and meta-analysis. BMC Oral Health 2017, 17, 133. [Google Scholar] [CrossRef]
- Dai, F.-F.; Xu, T.-M.; Shu, G. Comparison of achieved and predicted tooth movement of maxillary first molars and central incisors: First premolar extraction treatment with Invisalign. Angle Orthod. 2019, 89, 679–687. [Google Scholar] [CrossRef]
- Koletsi, D.; Iliadi, A.; Eliades, T. Predictability of rotational tooth movement with orthodontic aligners comparing software-based and achieved data: A systematic review and meta-analysis of observational studies. J. Orthod. 2021, 48, 277–287. [Google Scholar] [CrossRef] [PubMed]
- Ke, Y.; Zhu, Y.; Zhu, M. A comparison of treatment effectiveness between clear aligner and fixed appliance therapies. BMC Oral Health 2019, 19, 24. [Google Scholar] [CrossRef] [PubMed]
- Yassir, Y.A.; Nabbat, S.A.; McIntyre, G.T.; Bearn, D.R. Clinical effectiveness of clear aligner treatment compared to fixed appliance treatment: An overview of systematic reviews. Clin. Oral Investig. 2022, 26, 2353–2370. [Google Scholar] [CrossRef] [PubMed]
- Haouili, N.; Kravitz, N.D.; Vaid, N.R.; Ferguson, D.J.; Makki, L. Has Invisalign improved? A prospective follow-up study on the efficacy of tooth movement with Invisalign. Am. J. Orthod. Dentofac. Orthop. 2020, 158, 420–425. [Google Scholar] [CrossRef] [PubMed]
- Wilmes, B.; Nienkemper, M.; Ludwig, B.; Kau, C.H.; Pauls, A.; Drescher, D. Esthetic Class II treatment with the Beneslider and aligners. J. Clin. Orthod. 2012, 46, 390–398, quiz 437. [Google Scholar] [PubMed]
- Ikegami, T.; Wong, R.W.-K.; Hägg, U.; Lee, W.; Hibino, K. The Hybrid Orthodontic Treatment System (HOTS). World J. Orthod. 2010, 11, 168–179. [Google Scholar]
- Lombardo, L.; Palone, M.; Carlucci, A.; Siciliani, G. Clear aligner hybrid approach: A case report. J. World Fed. Orthod. 2020, 9, 32–43. [Google Scholar] [CrossRef] [PubMed]
- Wilmes, B.; Neuschulz, J.; Safar, M.; Braumann, B.; Drescher, D. Protocols for combining the Beneslider with lingual appliances in Class II treatment. J. Clin. Orthod. 2014, 48, 744–752. [Google Scholar] [PubMed]
- Wilmes, B.; Schwarze, J.; Vasudavan, S.; Drescher, D. Combination of clear aligners and beneslider for correction of severe midline deviation. J. Clin. Orthod. 2021, 55, 675–683. [Google Scholar]
- Kassam, S.K.; Stoops, F.R. Are clear aligners as effective as conventional fixed appliances? Evid. Based Dent. 2020, 21, 30–31. [Google Scholar] [CrossRef]
- Bilello, G.; Fazio, M.; Amato, E.; Crivello, L.; Galvano, A.; Currò, G. Accuracy evaluation of orthodontic movements with aligners: A prospective observational study. Prog. Orthod. 2022, 23, 12. [Google Scholar] [CrossRef] [PubMed]
- Scuzzo, G.; Takemoto, K.; Takemoto, Y.; Lombardo, L. A new self-ligating lingual bracket with square slots. J. Clin. Orthod. 2011, 45, 682–690, quiz 692. [Google Scholar] [PubMed]
- Upadhyay, M.; Arqub, S.A. Biomechanics of clear aligners: Hidden truths & first principles. J. World Fed. Orthod. 2022, 11, 12–21. [Google Scholar] [PubMed]
- Kravitz, N.D.; Kusnoto, B.; BeGole, E.; Obrez, A.; Agran, B. How well does Invisalign work? A prospective clinical study evaluating the efficacy of tooth movement with Invisalign. Am. J. Orthod. Dentofac. Orthop. 2009, 135, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Kravitz, N.D.; Kusnoto, B.; Agran, B.; Viana, G. Influence of attachments and interproximal reduction on the accuracy of canine rotation with Invisalign. A prospective clinical study. Angle Orthod. 2008, 78, 682–687. [Google Scholar] [CrossRef] [PubMed]
- Grünheid, T.; Loh, C.; Larson, B.E. How accurate is Invisalign in nonextraction cases? Are predicted tooth positions achieved? Angle Orthod. 2017; 87, 809–815. [Google Scholar]
- Andrews, L.F. The six keys to normal occlusion. Am. J. Orthod. 1972, 62, 296–309. [Google Scholar] [CrossRef]
- Kravitz, N.D.; Dalloul, B.; Zaid, Y.A.; Shah, C.; Vaid, N.R. What percentage of patients switch from Invisalign to braces? A retrospective study evaluating the conversion rate, number of refinement scans, and length of treatment. Am. J. Orthod. Dentofac. Orthop. 2022, 163, 526–530. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aiyar, A.; Scuzzo, G.; Scuzzo, G.; Verna, C. Hybrid Orthodontics for Aesthetic Deep Bite Correction—Case Series and General Clinical Considerations. Oral 2024, 4, 126-147. https://doi.org/10.3390/oral4020011
Aiyar A, Scuzzo G, Scuzzo G, Verna C. Hybrid Orthodontics for Aesthetic Deep Bite Correction—Case Series and General Clinical Considerations. Oral. 2024; 4(2):126-147. https://doi.org/10.3390/oral4020011
Chicago/Turabian StyleAiyar, Akila, Giuseppe Scuzzo, Giacomo Scuzzo, and Carlalberta Verna. 2024. "Hybrid Orthodontics for Aesthetic Deep Bite Correction—Case Series and General Clinical Considerations" Oral 4, no. 2: 126-147. https://doi.org/10.3390/oral4020011
APA StyleAiyar, A., Scuzzo, G., Scuzzo, G., & Verna, C. (2024). Hybrid Orthodontics for Aesthetic Deep Bite Correction—Case Series and General Clinical Considerations. Oral, 4(2), 126-147. https://doi.org/10.3390/oral4020011